best evidence medical education in geriatric medicine · pdf filebest evidence medical...
TRANSCRIPT

BEST EVIDENCE MEDICAL EDUCATION
IN GERIATRIC MEDICINE
SUZAN ABOU-RAYA, MDFaculty of Medicine,
University of AlexandriaFellow, Harvard Medical School, Boston, MA

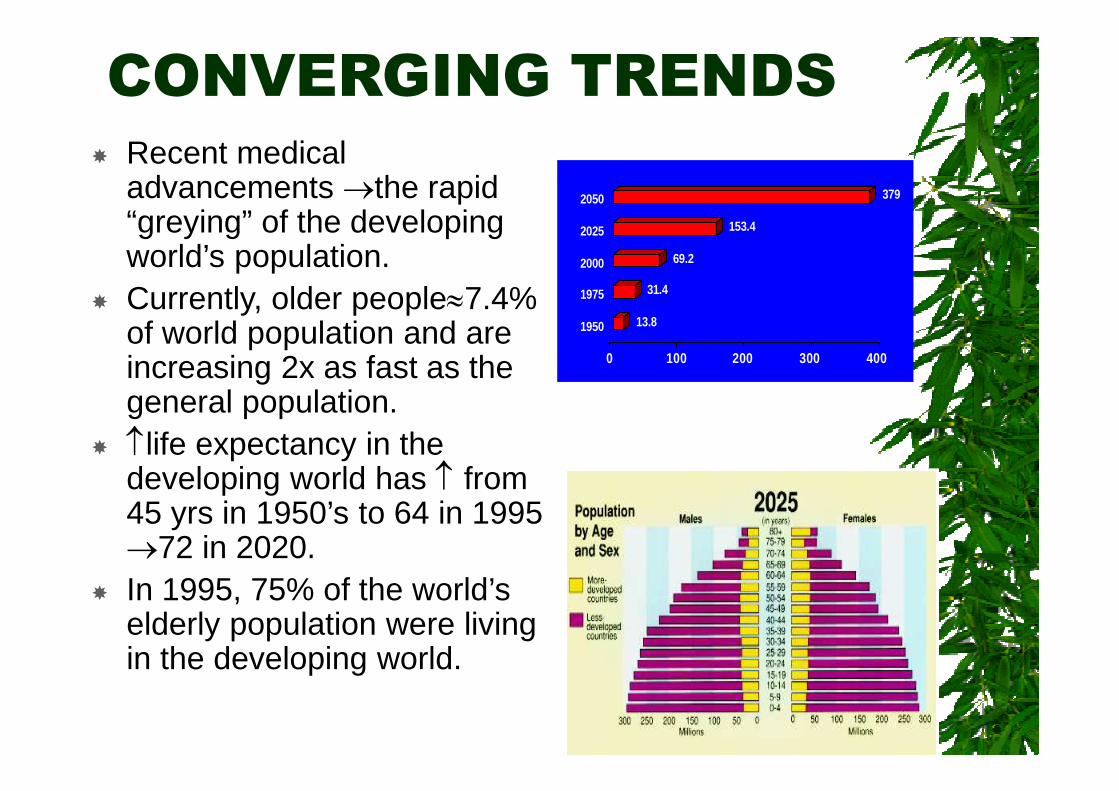
CONVERGING TRENDS Recent medical
advancements the rapid“greying” of the developingworld’s population.
Currently, older people7.4%of world population and areincreasing 2x as fast as thegeneral population.
life expectancy in thedeveloping world has from45 yrs in 1950’s to 64 in 199572 in 2020.
In 1995, 75% of the world’selderly population were livingin the developing world.
13.8
31.4
69.2
153.4
379
0 100 200 300 400
1950
1975
2000
2025
2050

Population demographics areshifting towards an increasing age.
Thus, comprehensive EBMeducation in Geriatric Medicine isvital.


Geriatric Medicine isan Integrated Medical
Practice
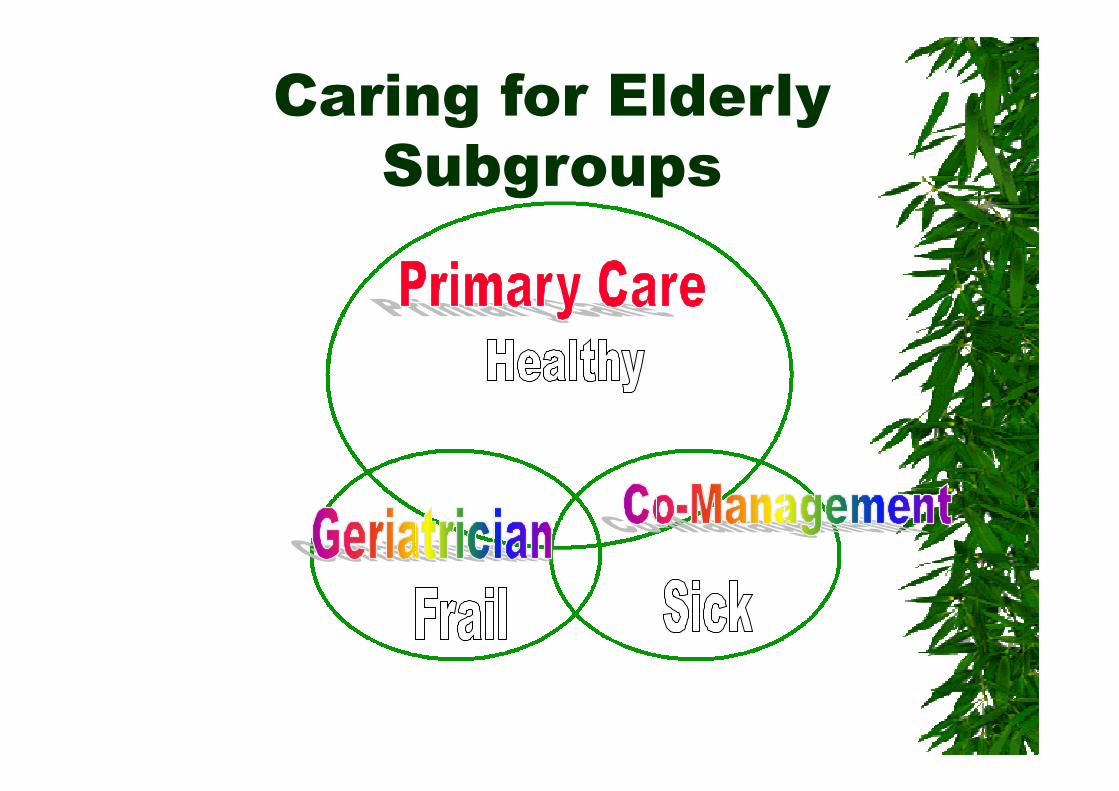
Caring for ElderlySubgroups

The "Geriatric Imperative"
IncreasingElderly
Population
Vast UnmetHealthcare
Needs

WHY DO THE ELDERLYREPRESENT ATHERAPEUTICCHALLENGE?

The Geriatrictherapeutic challenges
Impaired physiological reserve in olderpatients- “homeostenosis”.
Multiple disease and multiple drug use.
Non-specific or cryptic presentation.
Rapid deterioration if untreated(age-associated loss of adaptability).
High incidence of complications(ofdisease and treatment).

Goals of Care for Older Adults
Health-Related Quality of Life
SUCCESSFUL AGING
Prevent or reduce disability, maximize function
Manage complexity
Evidence-based treatment of disease
Anticipate and prevent clinical catastrophes
Appropriate long-term care
Palliative care
Individualized care
Care guided by patient’s preferences

Quality of HealthcarePhysician Performance - Hospital Care
“Good” performance is approximately 100%
– Flu vaccine, screened or given 27% (18)
– Pneumonia vaccine, screened or given 24% (13)
– Antibiotics within 8 hours for pneumonia 87% (85)
– Blood culture before antibiotics 82% (84)
– Fibrillators discharged on warfarin 57% (54)
– Antithrombotic for stroke at discharge 84% (82)
– No sublingual nifedipine for stroke 99% (95)

Quality of Healthcare
Physician Performance – Cardiac Care
(“Good” performance is approximately 100%)
– ASA within 24 hours 85% (82)
– ASA at discharge 86% (84)
– Beta-blocker within 24 hours 69% (63)
– Beta-blocker at discharge 79% (72)
– ACEI at discharge 74% (70)
– Counseled to quit smoking 43% (40)
– In CHF, measured ejection fraction 70% (66)
– ACEI at discharge if EF< 40% 68% (72)

Quality of HealthcarePhysician Performance - Anywhere
“Good” performance is approximately 100%
– Flu vaccination annually 72 % (66)
– Pneumovax ever 65% (55)
– Mammogram in last 2 years 60% (56)
– Diabetes Care
+ Eye exam in past year 70% (69)
+ Hemoglobin A1C annually 60% (55)
+ Lipid profile measurement for diabetics74% (58)
Why the need to change MedicalEducation ?
•The implementation of EBM has had a greatimpact on the teaching, practice and study ofmedicine.•There is a need to move from traditionalopinion-based education to evidence-basededucation.• Massive transformation in medicaleducation quantum leap from trying to be“good teachers” to making the learningprocess more readily available to students.•This is a time of great change in bothundergraduate and post -graduate medicaleducation.
Why the need for change inmedical education ??
What students now need to know isdirectly related to the informationexplosion which is evident in everyfield of study.
The goalposts have changed fromteaching facts to helping students tolearn how to find relevantinformation and how to assess itand how to organize disparateinformation into a cohesive whole.

Major pressures on healthcaresystems that lead to thedemand for an evidence-basedapproach to practice

Populationageing
Patientexpectations
Professionalexpectations
New knowledgeand technology
Industry Research
Why we need Evidence Based Medicine AND BestEvidence Medical Education


What is Best Evidence Medical
Education (BEME) ?
BEME is theimplementation byteachers in their practice,of methods andapproaches to theeducation ofphysicians/physicians-in- training based on thebest evidence available.

What is problem-basedlearning?
“ A learning methodbased on theprinciple of usingproblems as astarting point for theacquisition andintegration of newknowledge.”
H.S. Barrows 1982
What is required from atreating geriatrician throughtraditional teaching:
• Patient-Physician Relationship
• Clinical Skills
1) History taking
2) Physical examination
3) Laboratory tests
4) Imaging techniques
• Diagnosis of disease

What is required from ageriatrician through EBP:
• Caring for the patient:1) Assessing the outcome oftreatments2) Medical therapy3) Specific care for gender and agegroups4) Iatrogenic disorders5) Informed consent6) Accountability7) Practice guidelines8) Cost-effectiveness in medical care9) Research and teaching

1) Special circumstances & needs of
the older patient
2) Achieving a diagnosis and
achieving it early
3) Estimating a prognosis
4) Deciding on the best therapy
5) Determining harm
6) Providing care of the highest quality
When do you need EBM andBEME in Geriatric Medicine

Objective
The purpose of the study was to applyBEME in geriatric medicine training inrelation to the most effective method ofimparting the attitudes, skills andknowledge essential to prepare for soundand modern geriatrics practice.

Evidence-based anti-aging:

Methods
The feasibility of implementingproblem-based learning (PBL) andEBM into our traditional "lecture-based" medical curriculum by pilot-testing PBL using our 5th year internalmedicine students during their 7-weekclinical rotation was explored.

Methods
At the beginning of the round, thefundamental stages of EBM were revised.
Students were taught and proceeded togenerate specifically defined and structuredclinical questions from their clinicalencounters with older adult patients.
Students were divided into small groups andasked to tackle a geriatric clinical problem, atfirst there was a brainstorm session followedby the formulation of focused clinicalquestions.

Example
Mrs. Zenab Mourad is a 78 year old woman whohas come to the emergency room complaining ofshortness of breath and pain in her chest. She hadbeen in relatively good health until three weekspreviously.
Read theproblem
Brainstorm-hypothesize
Identify learningissues Research-
Learn(2-7 days
Return-Reread-Report-Review
Next page
EVALUATE
Methods
The participants were asked to developgeriatric patient-based searchablequestions, search for the evidence,critically appraise the retrievedliterature and finally to apply theevidence to the care of their patient.

Methods
At the last meeting of the round, theparticipants evaluated each case byanswering three questions about whetherthe process:
1) had changed the medicalmanagement of the patient during theadmission,
2) had changed the way they wouldmanage similar patients in future and
3) had informed them about thedisease process in general.
BEME teaching inGeriatric Medicine
Setting the question: A 66 yr old female suffering fromosteoarthritis of both knees as well as having Congestiveheart failure what are the best treatment options ??
Finding the evidence: Search for best availableevidence. to conduct the search need effective searchingskills and easy access to bibliographic databases = increasedaccess can be provide by ward –based computer andcomplemented by hard copies of the articles.
Appraising the evidence: Rely on the article or not=learn how to ask a few key questions about the validity of theevidence +relevance = tutorials, workshops, interactivelectures and at the bedside.
Acting on the evidence: implement the evidence todevelop team protocols or even rheumatology wardguidelines. (Best way to be learned through groupdiscussions, ward rounds, or clinical weekly meetings.
Example of Implementing BEME in Geriatric Training

Evidence-based anti-aging

RESULTS
Number of formal EBM inGeriatric Medicine questions
45
Duration of development andassessment of questions
7 weeks
Number of articles retrieved andcritically appraised
115

Evaluation Results
Percentage of participants whofelt the process had changed theactive management of elderlypatients by the team
80%
Percentage of participants whofelt that the process would affectthe care of future elderly patientswith comparable clinical problems
88%
Percentage who believe that theprocess has made them moreknowledgeable of variousdisease processes
94%

Results
The evidence-based healthcareapproach was easily implemented bythe participants. The initial results ofthe pilot experiment of PBL with ourmedical students was by and largepositive- students claimed that theywere motivated to participate activelyin the decision making andmanagement of the case and toperform an information search.

Conclusions
There is evidence to support the use ofPBL and EBM in medical educationand geriatric medicine practice.
Geriatric training could be improvedsignificantly by adopting the evidence-based advances that have been madein medical education.

Geriatric MedicineOpportunities
Geriatrics provides a uniqueeducational environment
-- Explosion of new therapies/Polypharmacy
–Wide range of presentations and atypicalpresentations
–Emphasis on decision making
–Interprofessional interactions
–-Greater incidence of side effects
Design unique educationalopportunities
Document educational outcomes
Geriatric MedicineOpportunities
Developing decision making skills
–Integrating foundational knowledge intodiagnosis of patient presentation
–Emphasis on early treatment andmanagement
-Design ways by which students/physicians-in- training will acquire expertise inelectronic information management andskills of BEME as a basic tool for life-longlearning and clinical decision-making.
BEME: Pros and Cons
Pros: For individuals: clinicians upgrade theirknowledge routinely
Improves clinicians understanding ofresearch methods
Improves computer literacy
For junior doctors: contribute to teamwork
For patients: better healthcare
Drawbacks: Time-consuming for learner andteacher.
Establish the infrastructure

Teaching Evidence BasedPractice= We should face the
challenge.
“Knowing is not enough, we must apply,Willing is not enough, we must do.”

Take Home Message
“Anyone with responsibility foreducating students, residents, andphysicians should be skilled andwell informed about medicaleducation - as preparing theselearners to provide safe, humane,and effective care for themembers of our society is a heavyresponsibility”

