best practice instruction in cognitive rehabilitation
DESCRIPTION
Best Practice Instruction in Cognitive Rehabilitation. Laurie Ehlhardt, PhD, CCC/SLP Teaching Research Institute-Eugene Rik Lemoncello, MS, CCC/SLP University of Oregon September 30, 2005. Advanced Organizer. Part I: Background Discuss rationale, theory & research Part II: Practice - PowerPoint PPT PresentationTRANSCRIPT
Best Practice Instruction in Cognitive
Rehabilitation
Laurie Ehlhardt, PhD, CCC/SLP
Teaching Research Institute-Eugene
Rik Lemoncello, MS, CCC/SLPUniversity of Oregon
September 30, 2005
Advanced OrganizerPart I: Background
Discuss rationale, theory & research
Part II: Practice Evidence from E-Mail trainingVideo analysis
Part III: Clinical ApplicationWrap-up video analysisConcluding Remarks & Questions
Learning Outcomes
As a result of this workshop training, participants will be able to:
1. Demonstrate an understanding of evidence-based practice
2. List one empirical study related to improved outcomes and instruction
3. Describe features of the TEACH-M instructional package
4. Apply the TEACH-M instructional package to clinical examples
Instruction Defined
Teaching (i.e., therapy, training, coaching, mentoring, etc.)Sharing knowledge/skills with othersIn this course…
Explicit, systematic instructionSevere brain injuryNew learning IS possible!
Rationale: Why focus on instruction?Focus of rehabilitation on training/teaching
Regardless of the treatment domain, we are all instructors
Maximizes client success/goal achievementNot all university training programs provide coursework dedicated to instructionHave to “do more with less”
e.g., less money, treatment time, etc.
Why focus on instruction?
Example: “Do more with less”Outpatient for TBIAverage # of visits 2005:
30-60 visits/calendar year, combining physical, occupational, and speech therapiesMinimal # of sessions with Oregon Health Plan (i.e., 1-2 per year for SLP)
Why focus on instruction?
“…in particular [the field of cognitive rehabilitation] has neglected for over two decades the accumulated wisdom in educational psychology, special education, etc. This neglect has cost billions of dollars and yielded countless hours of largely unsuccessful intervention for people with TBI. We have an opportunity to turn this around.”
Mark Ylvisaker, personal communication, 2003
Why focus on instruction?Teaching is complex
Teaching IS rocket science (Moats, 1999)
Information CAN be taught Instructor is responsible for learning
Frame problems around what instructor can control/manipulate*** Incorrect response is learner’s best attempt to be intelligent
More carefully taught = More easily learned
Rationale:Evidence-Based PracticeWhat is Evidence-Based Practice (EBP)?
“the conscientious, explicit, and judicious use of the current best evidence in making decisions about the care of individual patients”
Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence-based medicine: What it is and what it isn’t. British Journal of Medicine, 312, 71-2.
“the integration of best research evidence with clinical expertise and client values”
Sackett, D. L., Straus, S. E., Richardson, W. S., Rosenberg, W., & Haynes, R. B. (2000). Evidence-Based Medicine: How to Practice and Teach EBM. New York: Churchill Livingstone.
Evidence-Based Practice
Not a new phenomenonThink of “Efficacy” and “Accountability”
Focus on improving client outcomesMakes us better cliniciansRemember science of rehabilitation
Clinical scientist and Research scientistClinical work as a marriage between art and science (Apel & Self, 2003)
Evidence-Based Practice
EBP is a process for decision making
1. Identify need for clinical information2. Ask a searchable clinical question3. Search for the evidence4. Critically evaluate the evidence5. Integrate evidence with clinical
expertise and client values6. Evaluate effectiveness of treatment
Evidence-Based Practice
FREE Databases:
PubMed (MEDLINE) - Link to Full Text of:Journal of Head Trauma Rehabilitation (1998-2005)Brain Injury (1996-2005)
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=PubMed
National Guideline Clearinghouse:http://www.guideline.gov
ASHA Website for full text journals:http://www.asha.org
*See Web-Based Resources handout
Evidence-Based PracticeCritical Appraisal: “Is this a good study?”
Levels of Evidence:I. Well-designed Randomized Controlled TrialII.Well-designed Quasi-ExperimentIII. Non-Experimental StudiesIV. Expert opinion
For more information: http://www.cebm.net/levels_of_evidence.asp#levels
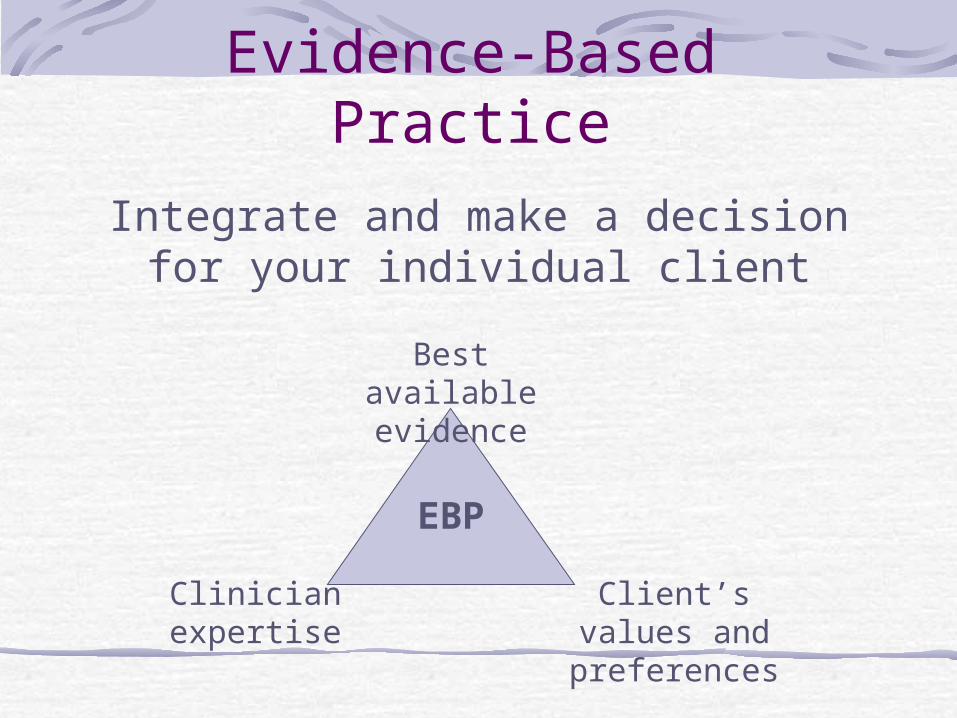
Evidence-Based Practice
Integrate and make a decision for your individual client
Best available evidence
Client’s values and preferences
Clinician expertise
EBP
Evidence-Based Practice:Insufficient Research
Evidence
Focus: Provide a rationale for your decisionsTreatment should at least be theoretically groundedClinicians have a responsibility to track outcomes and document changesBottom Line:
Take data, Measure progress, and Document gains!
Review & RecapInstruction definedRationale for instruction
Do more with lessWhat can we learn from the educational literature
Coming up…Types of instruction/Memory systems backgroundRational decision making – EBP
Integrate research evidence with clinical expertise and client’s values
Instruction
Common Types of InstructionTrial and errorMentorship/experiential learningExplicit, systematic instruction
Exchange of knowledge/skills from the instructor to the learner
Involves learning
Learning and Memory
Learning requires memoryTypes of memory
Short-term memory “Working” memory
Long-term memory“Fact” memory“Event” memory “Procedural” memory
Types of Long-Term Memory
”Fact-Event” memory (or “Explicit” memory): acquisition and intentional recollection of facts, concepts & events
“Procedural” memory: knowledge of procedures/skills or tasks without intentionally remembering the experience of learning
(Baddeley, 1995; Brandt & Rich, 1995; Tranel & Damasio, 1995)
Errorless Learning (EL)Brain injury generally does NOT affect “procedural” memory, but does affect “explicit” memory.Impaired “explicit” memory makes it difficult to remember and correct errors. Errors stick: “Trial and error” learning is therefore risky!
Goal of EL:Avoid errors while learning something new!!!
How do we achieve EL?
Errorless learning works by using high amounts of correct practice.Distributed practice (e.g., spaced retrieval) also facilitates EL.Target skill therefore becomes “routine”, “firm”, “solid”.
(Evans, et al., 2000; Wilson, Baddeley, Evans, & Shiel, 1994)
Direct InstructionDirect Instruction (DI):
well-established, systematic instructional methodology used across many different populations, particularly individuals with learning disabilitiesused across many different subject areas (e.g., reading, math, social skills)
Errorless learning is a key component of DI
DI components:* See Direct Instruction Strategies handout
Examples:Evidence in Support of DI/Errorless
Learning for Individuals with Cognitive Impairment
Wilson, et al. (1994) Errorless Learning in the Rehabilitation of Memory Impaired People; Levels 2 & 3 evidence
Evans, et al. (2000) A comparison of "errorless" and "trial and error" learning methods for teaching individuals with acquired memory deficits; Level 2 evidence
Kern, et al., (2002) Applications of Errorless Learning for Improving Work Performance in Persons with Schizophrenia; Level 1 evidence
Swanson, H., & Hoskyn, M. (1998). A synthesis of experimental intervention literature for students with learning disabilities: A meta-analysis of treatment outcomes. Review of Educational Research, 68, 277-321. Level 1 evidence

Research: Mozzoni & Bailey (1996) Improving training methods in brain injury
rehabilitation
Research Goal: To evaluate and improve the teaching effectiveness of therapists in an in-patient rehabilitation settingParticipants: Six therapists (speech, OT, recreation, nurse, cognitive rehab.) and five patients with severe TBI (Rancho Levels 5-6)Intervention: Daily feedback on therapists teaching skills using a checklist of specific behaviors Outcome measure: Patient performance on Functional Independence Measure (FIM)Level of Evidence: Level 2
Mozzoni & Bailey: Skills Checklist
Is the cuing clear?Is the patient attending to the therapist?Is the therapist using a task analysis?Is treatment consistent between sessions?Is therapist prompting systematically?Is the patient practicing the skill more than once?
*See Clinician’s Skills Checklist (#1) handout
Break
When we return…Research evidence to support DI for training individuals with severe cognitive impairments to use adapted E-MailVideotape analysis of teaching examplesPractical applications of new skills!!
Welcome BackReview Part I
What is instruction?Evidence-Based practice Research evidence to support systematic instruction for individuals with severe cognitive impairments
In this hour…Evidence from training E-MailVideotape examples for practical application
Research:An instructional package
TEACH-MEvaluation of an instructional
sequence for persons with impaired memory and executive functions
(Ehlhardt, Sohlberg, Glang, & Albin, 2005)
Level 2 Evidence

TEACH-M!Task analysis: Know your content. What is the target skill?
Break it into small steps. Chain steps together.
Errorless learning: Keep errors to a minimum during the acquisition phase. Model target step(s) BEFORE client attempts a new skill/step. Carefully fade support. Don’t let an error sneak by! Demonstrate the correct skill/step right away and ask client to do it again.
Assess performance: (initial)-assess skills before treatment; (on-going) - probe performance at the beginning of teaching session and/or before introducing a new step.
Cumulative review: Regularly review previously learned skills.
High rates of correct practice trials: 5 trials is not enough! 30-50 or more is like it!
Metacognitive strategy training: self-evaluation of one’s own performance
Research QuestionsIs there a functional relationship between implementation of the E-Steps program and:
1. The percentage of e-mail steps learned, in sequence?
2. Are treatment effects maintained at one month following the cessation of treatment?
3. Do treatment effects generalize to use of a similar e-mail interface with added features (i.e., altered interface) and/or a computer game with no shared features?
4. How many training sessions are required to reach the criterion for mastery?
Methods:Materials & Task Analysis
Simple email systemNot a “live” system for this studyHypothetical partners (e.g., counselor)
Task Analysis1. Click on start2. Click on inbox3. Click on picture4. Read message/click on reply5. Click on answer (yes or no)6. Click on send7. Click on quit
Methods: E-Steps program (IV)Phase 1: review - model - practice Phase 2: metacognitive strategy training
(reflection-prediction using screenshots)“Which step(s) will be easy? Which step(s)will be difficult?”
Phase 3: spaced retrieval (immediate recall, 30 seconds, 1 minute, 2 minutes)
Phase 4: metacognitive strategy (reflection using screenshots)“Which step was easy? Which step was difficult?”
Program implemented 4-5x weekly
MethodsDependent Variables
Number of correct email steps completed in sequence (out of 7)Whole task probe - Participants asked to perform email task (“Read and respond to the new message, then quit the program when through”); stopped when unable to go any further
Number of sessions to reach criterion for mastery (100% steps correct for 3 consecutive sessions)
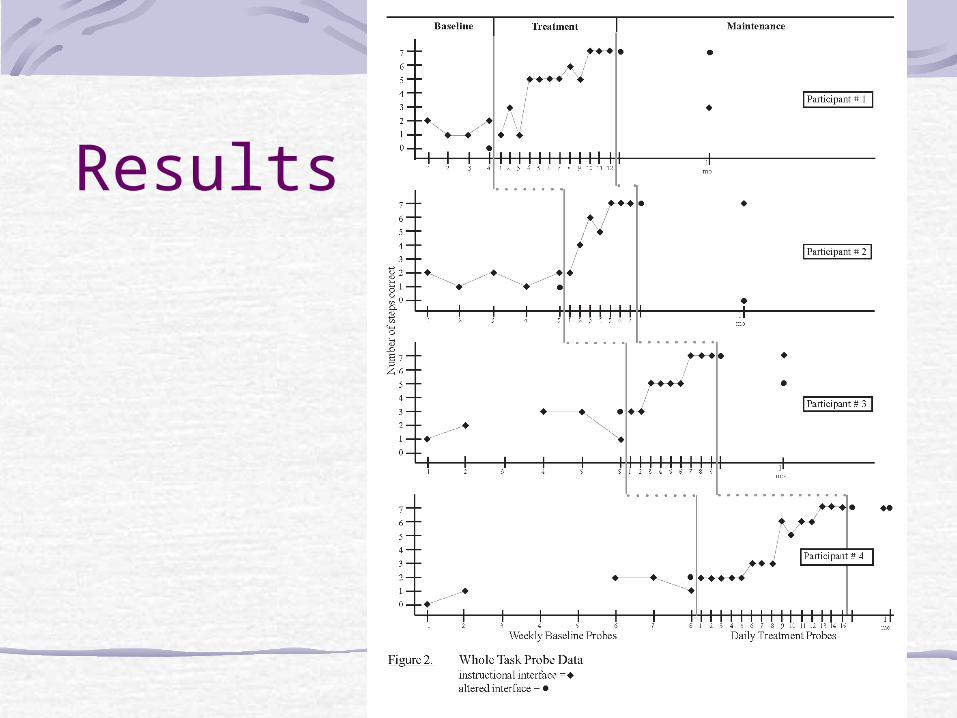
Results
Results:Additional participant performance
data
Total instruction time: 4 to 9 hours
Relatively high number of mouse activations per session (73-88 activations) when compared to the average number of minutes per session (37 minutes)
High accuracy - averaged 99% accuracy across all treatment trials/activations
Video Analysis: Part I
See Handouts(Task Analysis Forms)(Clinician Checklists)
Welcome Back
The continuing saga…Video Analysis: Part 2Concluding remarksQuestions and Answers
Learning Outcomes
As a result of this workshop training, participants will be able to:1. Describe process of evidence-based practice2. List one empirical study related to outcomes
and instruction3. Describe features of TEACH-M instructional
package4. Apply TEACH-M instructional package to
clinical examples
Final Thoughts
“What is it about my instruction that makes this client unable to learn?”
&“Nothing succeeds like success!”
Have fun and thank you!!!