bicuspid aortic valve 06/01/2007. bicuspid aortic valve definition: definition: –two functional...
TRANSCRIPT
Bicuspid Aortic ValveBicuspid Aortic Valve
06/01/200706/01/2007
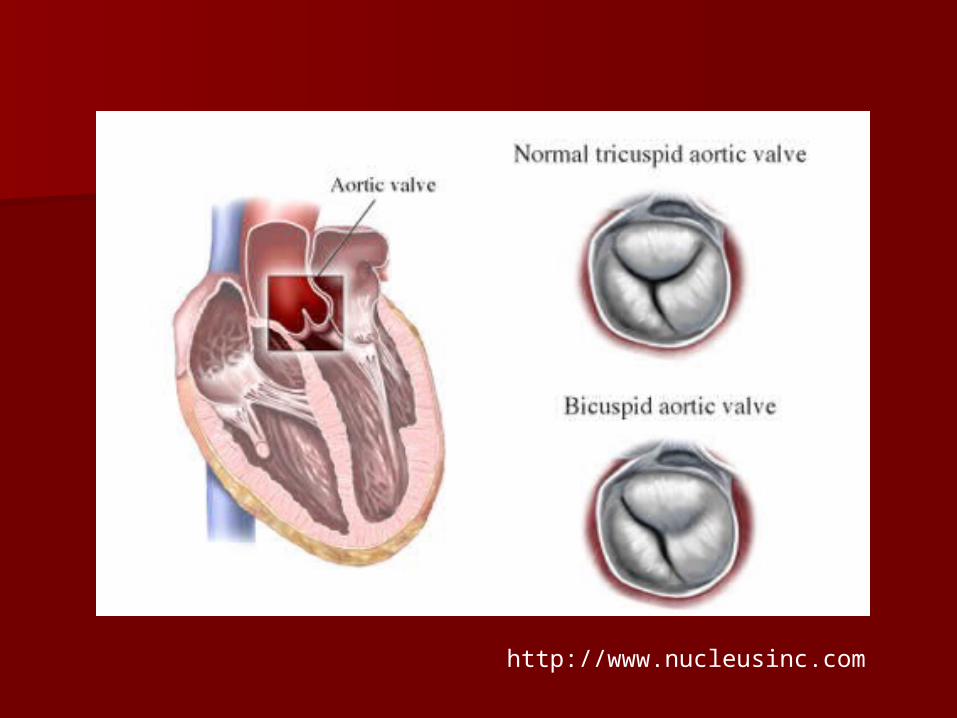
Bicuspid aortic valveBicuspid aortic valve
Definition:Definition:– Two functional aortic valve leaflets with Two functional aortic valve leaflets with
two complete commissurestwo complete commissures AKA “Bicommissural aortic valve”AKA “Bicommissural aortic valve”
Bicuspid aortic valveBicuspid aortic valve
Felt to represent a complex Felt to represent a complex continuumcontinuum– Unicommissural, Bicommissural, Unicommissural, Bicommissural,
Tricuspid, and QuadricuspidTricuspid, and Quadricuspid
Not simply a fusion of two normal Not simply a fusion of two normal cuspscusps
Bicuspid aortic valveBicuspid aortic valve
Three criteria:Three criteria:
1.) Unequally sized cusps1.) Unequally sized cusps
– Larger leaflet is the "conjoined" leafletLarger leaflet is the "conjoined" leaflet
http://www.nucleusinc.com
Bicuspid Aortic ValveBicuspid Aortic Valve
2.) Presence of a central ridge 2.) Presence of a central ridge (raphe)(raphe) – Usually in the center of the conjoined Usually in the center of the conjoined
leafletleaflet
Bicuspid Aortic ValveBicuspid Aortic Valve
3.) Smooth cusp margins3.) Smooth cusp margins
– Excludes tricuspid valves which fused Excludes tricuspid valves which fused due to inflammatory processes (eg, due to inflammatory processes (eg, rheumatic fever)rheumatic fever) Irregularity and scarring within the raphe.Irregularity and scarring within the raphe.
MorphologyMorphology
Orientation:Orientation: – Anterior-posterior Anterior-posterior
Left leaflet Left leaflet Right (conjoined) leafletRight (conjoined) leaflet
– Left-rightLeft-right Anterior (conjoined) leaflet Anterior (conjoined) leaflet Posterior leafletPosterior leaflet
PhysiologyPhysiology
Normally functioning bicuspid valveNormally functioning bicuspid valve– Abnormal folding and creasingAbnormal folding and creasing– Restricted motionRestricted motion– Turbulent flowTurbulent flow
Prolonged stress leads to valve Prolonged stress leads to valve damagedamage
StatisticsStatistics
Estimated overall incidence of 1-2%Estimated overall incidence of 1-2%
M:F at least 2:1M:F at least 2:1
Familial clustering suggests AD with Familial clustering suggests AD with variable penetrancevariable penetrance
No race or geographical predilectionNo race or geographical predilection
Associated AnomaliesAssociated Anomalies
Left dominant coronary arteryLeft dominant coronary artery– Up to 50% Up to 50%
10% with tricuspid valve10% with tricuspid valve
Short left main coronary arteryShort left main coronary artery– Less than 5mmLess than 5mm
Associated AnomaliesAssociated Anomalies
Coarctation of the aortaCoarctation of the aorta Interrupted aortic archInterrupted aortic arch
– >50% have bicuspid aortic valve>50% have bicuspid aortic valve
Associated AnomaliesAssociated Anomalies
Turner's SyndromeTurner's Syndrome– Up to 30%Up to 30%
William's SyndromeWilliam's Syndrome– Up to 10%Up to 10%
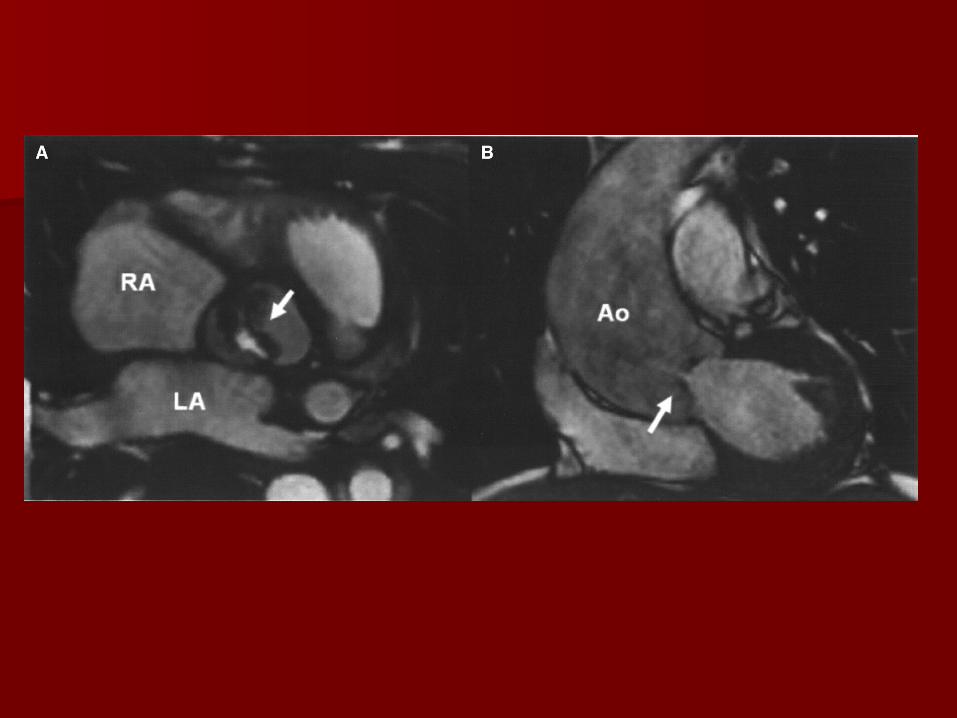
ImagingImaging
EchocardiographyEchocardiography– Modality of choiceModality of choice
Long-axis shows systolic doming due to Long-axis shows systolic doming due to limited valve openinglimited valve opening
Short-axis allows examination of the Short-axis allows examination of the commisures, leaflet morphology, and commisures, leaflet morphology, and mobility.mobility.

RadiographsRadiographs
Usually normal in pediatric Usually normal in pediatric populationpopulation
Aortic root enlargementAortic root enlargement
Left ventricular enlargementLeft ventricular enlargement
May see calcified raphe or leafletsMay see calcified raphe or leaflets
CT/MRICT/MRI
Allows for evaluation of the aorta and Allows for evaluation of the aorta and coronary arteriescoronary arteries
Functional informationFunctional information

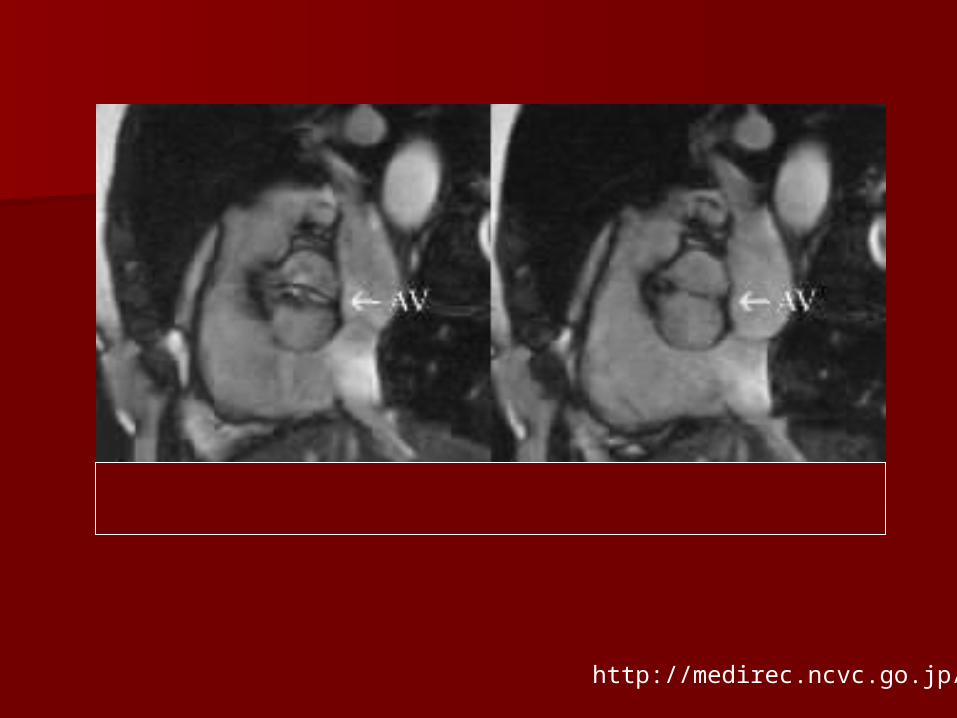
http://medirec.ncvc.go.jp/
PathologyPathology
Aortic StenosisAortic Stenosis
Aortic InsufficiencyAortic Insufficiency
Bacterial EndocarditisBacterial Endocarditis
Aortic DissectionAortic Dissection
Aortic StenosisAortic Stenosis
Poorly functioning valves may have Poorly functioning valves may have incomplete systolic openingincomplete systolic opening
Responsible for 80-95 % of aortic Responsible for 80-95 % of aortic valve disease detected in infancyvalve disease detected in infancy– May cause rapid deteriorationMay cause rapid deterioration– Progression over years is more commonProgression over years is more common
Aortic Stenosis Aortic Stenosis
Bicuspid valve may be prone to Bicuspid valve may be prone to accelerated agingaccelerated aging– Sclerosis begins in the second decade of Sclerosis begins in the second decade of
lifelife– Estimated that 50% of adults with Estimated that 50% of adults with
severe AS have bicuspid valves. severe AS have bicuspid valves.
Aortic StenosisAortic Stenosis
Cusps oriented in the AP direction Cusps oriented in the AP direction demonstrate more rapid progressiondemonstrate more rapid progression
Presence of risk factors can also Presence of risk factors can also expedite the processexpedite the process– High LDL, high lipoprotein (A) and High LDL, high lipoprotein (A) and
smokingsmoking
Aortic InsufficiencyAortic Insufficiency
Isolated AIIsolated AI
AI with aortic root dilatation AI with aortic root dilatation
Aortic InsufficiencyAortic Insufficiency
Isolated AIIsolated AI– Prolapse of redundant larger cuspProlapse of redundant larger cusp
Rarely severeRarely severe
Aortic InsufficiencyAortic Insufficiency
Disruption of the elastic tissue within Disruption of the elastic tissue within the upper aortic ring/sinotubular the upper aortic ring/sinotubular junction junction – May occur due to inherent abnormalityMay occur due to inherent abnormality– May be due to coarctation of the aorta May be due to coarctation of the aorta
or bacterial endocarditisor bacterial endocarditis Often severe with high mortalityOften severe with high mortality
Bacterial Endocarditis Bacterial Endocarditis
Estimated 10-30% of patients with Estimated 10-30% of patients with bicuspid aortic valvebicuspid aortic valve– 25% of cases of endocarditis occur on bicuspid 25% of cases of endocarditis occur on bicuspid
valvesvalves
– Tetralogy of Fallot, VSD, and MVP are the other Tetralogy of Fallot, VSD, and MVP are the other lesions associated with SBElesions associated with SBE
Prophylactic antibiotics for dental/surgical Prophylactic antibiotics for dental/surgical proceduresprocedures
Bacterial EndocarditisBacterial Endocarditis
Responsible for half of cases of Responsible for half of cases of severe AI in patients with bicuspid severe AI in patients with bicuspid valvevalve– Many due to cusp perforationMany due to cusp perforation
Unexplained systemic emboli should Unexplained systemic emboli should raise suspicionraise suspicion
Aortic Dissection Aortic Dissection
Approximately 5% of patientsApproximately 5% of patients– Etiology is unclearEtiology is unclear
Abnormal response to hemodynamic stressAbnormal response to hemodynamic stress– Cystic medial necrosis similar to Marfan’sCystic medial necrosis similar to Marfan’s– Dysfunctional microfibrillar proteins, endothelial Dysfunctional microfibrillar proteins, endothelial
nitric oxide synthetase, etc.nitric oxide synthetase, etc.
Medical Management Medical Management
LifestyleLifestyle– Exercise, heart healthy diet, no smokingExercise, heart healthy diet, no smoking
Cholesterol and hypertensive Cholesterol and hypertensive medicationmedication
Medical ManagementMedical Management
Surveillance echocardiographySurveillance echocardiography
Early surgical referralEarly surgical referral
First-degree relative screeningFirst-degree relative screening
Surgical TreatmentSurgical Treatment
Severe valvular dysfunction or aortic Severe valvular dysfunction or aortic root dilatationroot dilatation
Symptomatic patientsSymptomatic patients
Evidence of abnormal LV dimensions Evidence of abnormal LV dimensions and function and function
Surgical TreatmentSurgical Treatment
Pediatric casesPediatric cases– Balloon ValvuloplastyBalloon Valvuloplasty
Without calcified valvesWithout calcified valves Isolated Aortic InsufficiencyIsolated Aortic Insufficiency
– Valve RepairValve Repair Valve replacement Valve replacement
– With or without aortic root replacementWith or without aortic root replacement Prosthetic/Bioprosthetic/HomograftProsthetic/Bioprosthetic/Homograft Ross procedureRoss procedure
ReferencesReferences Fedak PWM, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and Fedak PWM, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and
pathophysiological implications of a bicuspid aortic valve. pathophysiological implications of a bicuspid aortic valve. Circulation. Circulation. 2002; 106: 2002; 106: 900–904 900–904
Ward, C. Clinical significance of the bicuspid aortic valve. Ward, C. Clinical significance of the bicuspid aortic valve. HeartHeart 2000 83: 81-85 2000 83: 81-85 Pediatric Cardiac SurgeryPediatric Cardiac Surgery, Mavroudis et al., 3rd edition, Mosby, St. Louis., Mavroudis et al., 3rd edition, Mosby, St. Louis. Aboulhosn, J, Child, JS. Left ventricular outflow obstruction: subaortic stenosis, Aboulhosn, J, Child, JS. Left ventricular outflow obstruction: subaortic stenosis,
bicuspid aortic valve, supravalvar aortic stenosis, and coarctation of the aorta. bicuspid aortic valve, supravalvar aortic stenosis, and coarctation of the aorta. CirculationCirculation. 2006 Nov 28;114(22):2412-22.. 2006 Nov 28;114(22):2412-22.
http://www.emedicine.com/ped/topic2486.htmhttp://www.emedicine.com/ped/topic2486.htm