bicuspid aortic valve and associated aortopathy …bicuspid aortic valve and associated aortopathy:...
TRANSCRIPT
STATE OF THE ART
Bicuspid Aortic Valve and AssociatedAortopathy: An UpdateEvaldas Girdauskas, MD, PhD* and Michael A. Borger, MD, PhD†
Bicuspid aortic valve (BAV) is the most common form of congenital heart disease and most suchpatients develop cardiovascular complications over time. Recent studies have shed light on one ofthe most common of these complications, BAV-associated aortopathy. Two distinct BAVphenotypes have been identified, which may have different causes of their associated aortopathy.Increasing evidence suggests that the BAV stenosis phenotype is predominantly secondary tohemodynamic perturbances in transvalvular flow and is associated with a more benign long-termprognosis once the stenotic BAV is replaced. In contrast, the root phenotype—which is associatedwith aortic insufficiency—appears to have a genetic origin and may be associated with a higher riskof adverse aortic complications, irrespective of the extent of valvular disease. Such observationsmay have implications for patient decision making. Future studies should be performed so as tobetter define phenotypes and risk factors for BAV-associated aortopathy.
Semin Thoracic Surg 25:310–316 I 2014 Elsevier Inc. All rights reserved.
Keywords bicuspid aortic valve, bicuspid aortopathy, aortic aneurysm, aortic surgery, aorta
EPIDEMIOLOGY AND NATURAL HISTORY predominantly derived from necropsy studies from
OF BICUSPID AORTIC VALVEBicuspid aortic valve (BAV) disease is known to bethe most common congenital anomaly of the humanheart.1,2 Taking into account all complicationsassociated with BAV disease, it accounts for moremorbidity and mortality than that of all the othercongenital cardiac lesions combined.3 A broadspectrum of complications associated with BAV hasbeen described, including aortic valve stenosis (ie,the most common form of symptomatic BAV dis-ease), aortic valve insufficiency, infective endocardi-tis, and ascending aortic complications.
There is adequate evidence that BAV is a heritabledisorder with an autosomal dominant inheritancepattern and reduced penetrance.4 The prevalence ofBAV historically quoted in the literature has beenbetween 1% and 2% with an obvious male prepon-derance. However, these estimates are
*Department of Cardiac Surgery, Central Hospital BadBerka, Bad Berka, Germany.†Department of Cardiac Surgery, Heart Center Leipzig,Leipzig, Germany.
Dr Borger reports receiving lecture fees from EdwardsLifesciences, St. Jude Medical, and Sorin. Dr Girdauskashas no commercial interests to disclose.
Address reprint requests to Evaldas Girdauskas, MD, PhD,Department of Cardiac Surgery, Central Clinic Bad Berka,Robert-Koch-Allee 9, 99437 Bad Berka, Germany. E-mail:[email protected]
310
an earlier era.5,6 As emphasized by the authors ofthese early studies, the incidence of BAV determinedby necropsy reports is unreliable because thisanomaly may be easily overlooked.5
The development of echocardiography screening hasa significant potential to increase our understanding ofthe prevalence of BAV in the general population.However, there are only limited population-basedechocardiographic data on the prevalence of BAV inthe pediatric and adult population.7-9 These echocar-diographic surveys quote a BAV frequency of 0.5% inunselected healthy populations, which is significantlylower than previously expected. However, the sensi-tivity of transthoracic echocardiography to identifyBAV has been reported in the range of only 60%.10
Therefore, at least one-third of BAV cases may remainundetected by means of transthoracic echocardio-graphic screening. Moreover, as BAV is a heritabledisorder, some familial and endemic clustering may beencountered with a potential of accumulation ofpatients with BAV in certain geographic areas.11
Therefore, the true incidence of BAV in the generalpopulation may be underestimated. An underesti-mation of the true BAV incidence may have clinicalconsequences because the reported increased risk ofaortic complications in these patients is based on theassumption that BAV prevalence is in the range of1%-2% in the general population. If the trueprevalence of BAV is higher, then the increasedaortic complication risk may be exaggerated.
1043-0679/$-see front matter ª 2014 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1053/j.semtcvs.2014.01.004
BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
Seminars in Thorac
MORPHOLOGY OF BAV—WHAT ISIMPORTANT FOR FUNCTIONAL ANALYSIS?
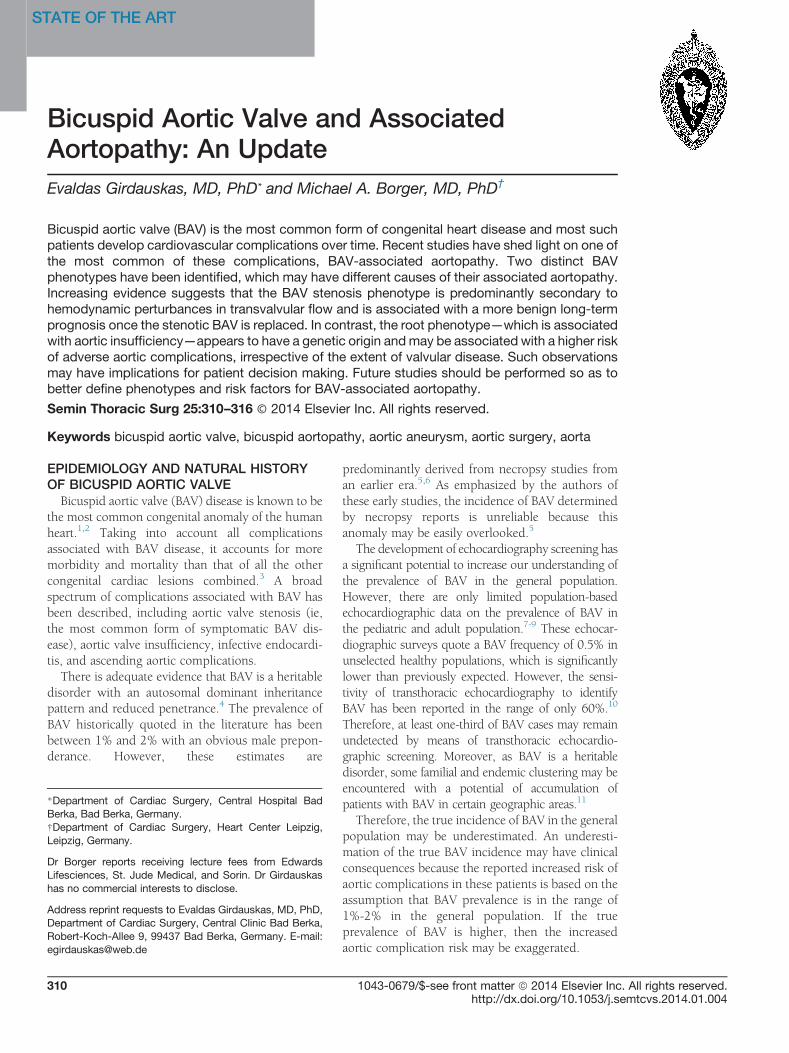
There are several morphologic aspects that predis-pose to specific functioning patterns of bicuspid valves.One structural feature that influences transvalvularflow characteristics is the cusp fusion pattern. The 2most common patterns of cusp fusion in BAV diseaseare fusion of the left and right coronary cusps, whichoccurs in 70%-85% of cases, and fusion of the rightand noncoronary cusp, which occurs in 15%-30% ofpatients with BAV (Fig. 1). There is sufficient evidencein the literature demonstrating an association betweenBAV cusp fusion pattern and specifically orientedtransvalvular systolic flow.13,14 Moreover, “cusp open-ing angle” (ie, degree of fused cusp alignment to theaortic outflow axis in systole) has been describedrecently by Della Corte et al15 to demonstrate theeffect of fused cusp motility on transvalvular systolicflow deflection. These investigators were also able todemonstrate a prognostic correlation of this parameterwith yearly rate of aortic growth.
Another structural parameter that is important inthe functional analysis of BAV is the angulationbetween the left ventricular outflow tract and theaortic root, as described previously by den Reijeret al.16 A significant correlation has been demon-strated between this angle, the degree of eccentricityof the systolic transvalvular flow, and the severity ofthe proximal aortic dilatation in a pediatric BAVpopulation (ie, the larger the angle of misdirectedflow with the aortic outflow axis, the larger theproximal aortic diameter).16
We recently examined transvalvular flow patterns,as determined by magnetic resonance imaging(MRI), in a prospective study on patients with BAVundergoing aortic valve replacement (AVR) surgery.We found variations in transvalvular flow patternseven in patients with the same cusp fusion pattern.17
We hypothesized that the exact geometric orienta-tion of residual aortic valve orifice in patients with
Figure 1. Cusp fusion patterns in BAV disease. (
ic and Cardiovascular Surgery � Volume 25, Numbe
BAV stenosis may be responsible for these variationsin transvalvular flow patterns.This overview is aimed to illustrate the complex
interaction between morphologic characteristics ofBAV and functional alterations in blood flow, whichis a crucial step in the understanding of pathogenesisof bicuspid aortopathy.
RHEOLOGICAL CHARACTERISTICS OFCLINICALLY “NORMAL” BAV: EVIDENCEFROM RECENT STUDIESThe asymmetric and dome-shaped opening of
clinically “normal” aortic valves in patients withBAV has been demonstrated experimentally byRobicsek et al18 in their pioneering in vitro study.The resultant perturbations in transvalvular flowthrough the clinically “normal”—but morphologi-cally stenotic—BAV orifice have been shown to beeccentric and directed toward the proximal aorticwall rather than toward the aortic lumen as in patientswith normal tricuspid aortic valves (TAV). The effectof transvalvular flow eccentricity on the diameter ofthe proximal aorta (ie, degree of aortopathy) has beendemonstrated in the pediatric BAV population.16
Barker et al19 evaluated wall shear stress along thelumen circumference of the ascending aorta inpatients with BAV using phase-contrast MRI. Thespatial distribution and magnitude of systolic wallshear stress in patients with BAV was shown to besignificantly different from that in patients withTAV.19 In addition, the values of turbulent kineticenergy and shear stress were significantly higher inBAV than TAV models using finite element analysis20
and particle image velocimetry.21
The most recent contributions in this field14,22
compared flow and wall shear stress patterns inindividuals with clinically “normal” bicuspid andTAV, using sophisticated 4-dimensional cardiovas-cular MRI. Similar to the findings of previous studies,BAV aortas were exposed to significantly higher
Adapted with permission from Sabet et al.12)
r 4 311
BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
transvalvular flow-induced wall shear forces thanTAV aortas were. These flow abnormalities may havea major effect on the development of BAV-associatedaortopathy in patients with clinically “normal” BAV.
BAV-ASSOCIATED AORTOPATHY: ALWAYSTHE SAME DISEASE?
Most of the literature on BAV disease consideredproximal aortic involvement as a homogeneous clin-ical entity, which may lead one to conclude that moreaggressive surgical treatment is justified. The contro-versy regarding optimal treatment of BAV-associatedaortopathy was primarily triggered by inconsistency ofpublished follow-up data on long-term outcomes afterAVR in patients with BAV.23 Such a high variability inthe prevalence of late aortic events (ie, 5%-30% over amean of 13 years) may be explained by substantialdifferences in the patient population between studies(ie, heterogeneous characteristics of the includedpatients). The concept of heterogeneity in BAV diseasebecame accepted in the last few years, which wasfollowed by identification of separate anatomical-clinical forms—so-called BAV phenotypes.24,25
BAV Stenosis and Associated AortopathyPure or predominant calcific stenosis is the most
common dysfunctional state of BAV (ie, 85% ofsurgically treated cases).12 The common associationbetween BAV stenosis and asymmetric dilatation of
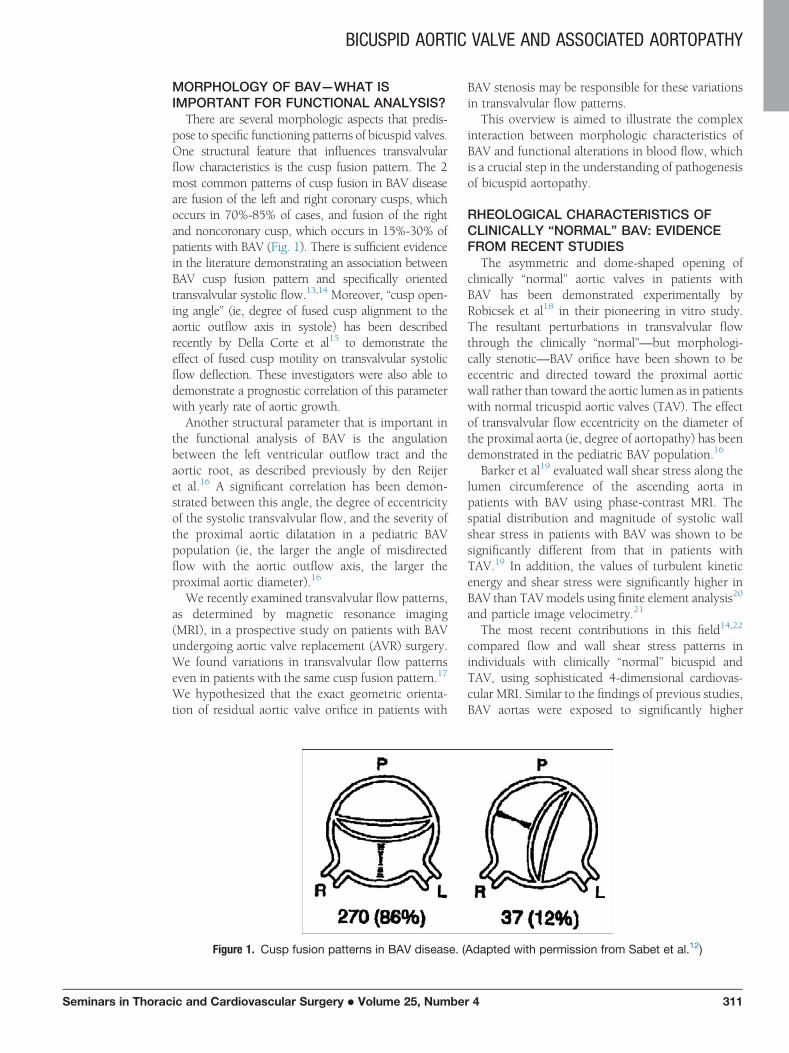
Figure 2. Magnetic resonance imaging (A) and intraoperaphenotype with concomitant asymmetric midascendingonline at http://www.semthorcardiovascsurg.com.)
312 Semin
the tubular aorta, starting from the sinotubularjunction and predominantly involving the convexityof the vessel, has been identified as “BAD MATE”syndrome by Cotrufo et al and Della Corte et al24,25
(Fig. 2). This association has been proposed to be ofpathogenetic origin and a result of an eccentrictransvalvular flow jet through the stenotic BAV.The high-velocity turbulent jet propagates towardthe greater curvature of the tubular ascending aorta,thus leading to its subsequent wall thinning andenlargement (ie, previously so-called poststenoticdilatation).24 Hemodynamic factors (ie, flow-induced vascular remodeling) have been proposedto play a major role in the development of such anaortopathy in patients with BAV stenosis.8,13 Untilrecently, this hemodynamic hypothesis has beenmostly based on indirect observational data.If abnormal transvalvular flow is the major deter-
minant of coexistent aortopathy in patients withsevere BAV stenosis, isolated AVR surgery should besufficient in patients with mild to moderate con-comitant ascending aortic dilatation. To test thishypothesis, we retrospectively examined a relativelylarge group of consecutive patients (n = 153) whounderwent isolated AVR surgery for BAV stenosiswith concomitant mild to moderate proximal aorticdilatation (ie, 40-50 mm) over a prolonged period offollow-up (mean = 11.5 years).26 Our analysisdemonstrated a considerably low risk of adverseaortic events during follow-up, with a freedom from
tive findings (B) of a patient with typical BAV stenosisaortic aneurysm. (Color version of figure is available
ars in Thoracic and Cardiovascular Surgery � Volume 25, Number 4

BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
Seminars in Thorac
adverse aortic events of 93% at 15 years.26 Nodocumented aortic dissection or rupture occurredin this patient group, supporting the hypothesis thataortopathy in patients with BAV stenosis is predom-inantly a secondary hemodynamic effect.
To further test this hypothesis, we recently exam-ined the long-term prognosis of moderate ascendingaortic dilation after isolated AVR in patients withBAV vs that in patients with TAV stenosis.27 Weobserved a low risk of adverse aortic events duringfollow-up in both groups, with 15-year freedomfrom adverse aortic event rates of 93% vs 82% in theBAV vs TAV groups (P ¼ 0.2).27
We also hypothesized that a significant correlationmay be anticipated between rheological character-istics of transvalvular blood flow and microstructuralchanges in the proximal aortic wall in patients withBAV stenosis and associated aortopathy.17 Usingpreoperative MRI examinations and intraoperativeaortic tissue samples, we were able to demonstrate astrong correlation between the systolic pattern oftransvalvular flow jet and asymmetric proximalaortic wall changes in patients undergoing AVR forBAV stenosis. The histologic sum score was signifi-cantly higher in the jet sample (ie, area of maximalflow-induced stress in the proximal aorta as deter-mined by preoperative MRI) vs control sample(ie, opposite aortic wall) in these patients.17
In summary, there is a growing body of evidencethat BAV-associated aortopathy in patients with BAVstenosis represents a predominantly hemodynamic-induced phenomenon. Concomitant mild to mod-erate dilatation of the ascending aorta in thesepatients is not associated with an increased riskof adverse aortic events up to 15 years afterisolated AVR.
Such observations may have important implica-tions for clinical decision making in patients pre-senting with BAV-associated aortopathy. However,we do not suggest that ascending aorta replacementis contraindicated in patients with BAV stenosis andmild to moderate dilation of the ascending aorta.Concomitant replacement of the supracoronary aortais a safe procedure that can be performed with lowadditional surgical risk, and it may be indicated inspecific situations (eg, in patients with a thin aorticwall so as to prevent catastrophic bleeding at the endof the operation; in patients with a family history ofadverse aortic events; and in patients with poorlycontrolled hypertension). However, it is possible toconclude from our data that very aggressiveapproaches to the aorta in patients with BAV stenosis(eg, prophylactic replacement of the aorta in patientswithout other indications for cardiac surgery andreplacement of the aortic root, ascending aorta, and
ic and Cardiovascular Surgery � Volume 25, Numbe
proximal aortic arch in patients requiring AVRsurgery) are not justified in the absence of amarkedly dilated aorta.
BAV Root PhenotypeA relatively small cohort of patients with BAV
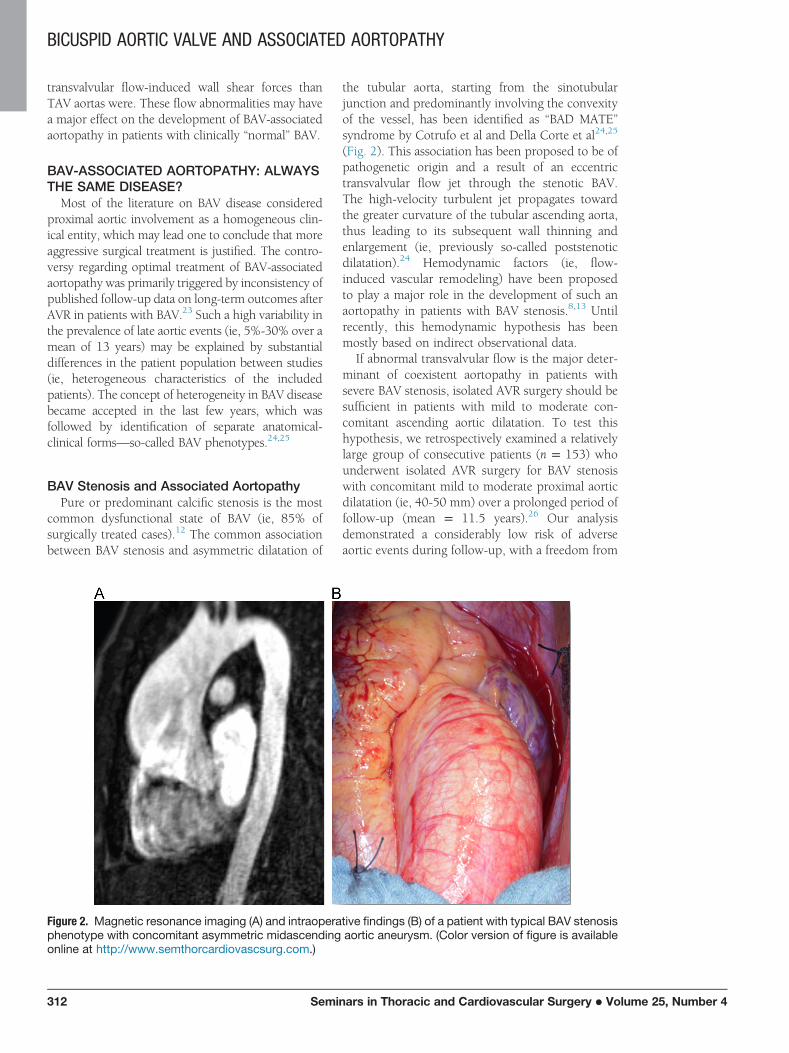
(approximately 10%) present with the second com-mon phenotype, that is, predominant aortic dilata-tion at the level of the aortic annulus and the sinusesof Valsalva with varying degrees of accompanyingaortic valve insufficiency (Fig. 3). This anatomical-clinical form of BAV disease has been described inthe literature as “root phenotype.”25 Root phenotypeoccurs primarily in the young BAV population, andmale sex has a strong predisposition for thecondition.There are some data in the literature that support
the predominantly genetic origin of BAV rootphenotype. A subgroup of young male patients withBAV who present with a varying degree of aorticvalve insufficiency and dilatation of the aortic root,which occur independent of age and body size, hasbeen identified by Nistri et al.28 Biner et al29 wereable to demonstrate the congenital pattern of aort-opathy in the first-degree relatives of patients withBAV who presented with aortic root dilatation. Wereported on a patient with familial BAV disease androot dilatation phenotype, in whom the geneticorigin was demonstrated to be a TGFBR2 genemutation.30
The BAV root phenotype seems to have a differentprognosis for aortic complications when comparedwith that of the BAV stenosis phenotype. We recentlydemonstrated a considerably higher prevalence ofadverse aortic events during follow-up in a BAVcohort with aortic insufficiency.31 The freedom fromaortic complications 15 years postoperatively was 78� 9% in patients with BAV root phenotype com-pared with 93 � 3% in patients with BAV stenosis(P ¼ 0.02).31
The aforementioned data suggest that BAV rootphenotype may be a genetic, connective tissuedisorder–like form of aortic disease that is independ-ent of transvalvular flow perturbations. One couldtherefore recommend a more aggressive surgicalapproach to the aorta in this subgroup of patientswith BAV. In addition, a distinction should be madebetween patients with root phenotype and patientswith BAV stenosis in future studies of BAV-associated aortopathy.
Biomolecular Studies on BAV AortopathyOne of the traditional arguments for a genetic
origin of BAV-associated aortopathy has been data
r 4 313
Figure 3. Transthoracic echocardiography (A) and intraoperative findings (B) in a patient with BAV rootphenotype. (Color version of figure is available online at http://www.semthorcardiovascsurg.com.)
BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
from multiple biomolecular series demonstratingmore severe microstructural lesions in the proximalaortic wall of patients with BAV when comparedwith that of matched TAV controls.32-34 Unfortu-nately, most of these studies share 2 inherentlimitations, which may have led to a misinterpreta-tion of the results. The first limitation is the lumpingof patients with BAV stenosis and patients with BAVroot phenotype together, which is probably inappro-priate for the reasons addressed earlier. Recently,some investigators have found more severe biomo-lecular lesions in patients with BAV insufficiency ascompared with those in patients with BAV stenosis,further supporting the concept that these are 2separate clinical entities.35-37 Another recent study,which included a high proportion of patients with
314 Semin
BAV insufficiency (ie, 60% of the total study cohort),showed a high prevalence of moderate or severehistologic alterations in the aortic media even in theabsence of clinically relevant proximal aortic dilata-tion.38 In their multivariate analysis, these authorsdemonstrated a significant association betweenaortic media alterations and diameter of the aorticannulus, which is in turn an indicator of aortic rootdisease (ie, BAV root phenotype).38
The second major limitation of previous biomo-lecular studies is the inability to differentiate betweenprimary congenital changes in the aortic wall archi-tecture and secondary hemodynamically inducedvascular lesions. Indeed, one may question whetherthis differentiation is possible at all. As previouslymentioned by Robicsek,39 a study demonstrating the
ars in Thoracic and Cardiovascular Surgery � Volume 25, Number 4

BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
Seminars in Thorac
primary nature of biomolecular changes by examin-ing the aortic wall in the newborns would berequired to definitely answer this question.
INTERACTION OF MORPHOLOGY,FUNCTION, AND DISEASE PROCESS:FUTURE DIRECTIONS IN BAV RESEARCH
Despite the fact that progress has been made inunderstanding BAV disease and its associated aort-opathy in the last decade, major questions remain tobe answered. Although we are aware of 2 distinctphenotypes of BAV disease, we are unable to assignevery single patient with BAV to one of these entities.Other questions to be answered include the follow-ing: (1) Why does the aorta never dilate in 20%-30%of patients with BAV? (2) What is the cutoff value ofaortic diameter that may be left untreated at the timeof cardiac surgery in patients with BAV stenosis vspatients with BAV insufficiency vs patients withfunctionally normal BAV? (3) What will be the roleof transcatheter valve technology in patients withBAV disease and associated aortopathy? (4) What arethe diagnostic tools that will help us to distinguishthe more aggressive from the more benign forms ofBAV-associated aortopathy? Future research in BAVdisease should focus on the ability to integrateinformation on the morphologic features and func-tional characteristics of the aortic valve and proximalthoracic aorta, preferably obtained by means ofnoninvasive imaging. Such information may allowus to correlate specific morphologic variants of BAV
ic and Cardiovascular Surgery � Volume 25, Numbe
with functional alterations so as to better defineindividual BAV phenotypes and future risk patterns.Noninvasive image-based assessment of aortic wallqualities may be required to better understand thedevelopment and progression of aortopathy. Suchinformation may eventually replace the nonspecificsize-based criteria that are currently used for aorticsurgery. Moreover, further genetic studies arerequired so as to better define the congenital basisof separate BAV phenotypes.
SUMMARYBAV is a common congenital disorder and a
significant proportion of such patients developcardiovascular complications over time. Associatedaortopathy is an important—but still poorly under-stood—lesion that is frequently found in patientswith BAV. Two distinct clinical-pathologic BAVphenotypes can be identified. Patients presentingwith BAV stenosis seem to have a more benign formof associated aortopathy, and aggressive manage-ment of the condition in such patients may not bejustified. By contrast, more aggressive managementof concomitant aortic dilation may be required inpatients presenting with root phenotype BAV dis-ease. Future studies should focus on better character-ization of BAV subgroups, preferably based onnoninvasive imaging or genetic testing, and theeffects of these phenotypes on outcomes and patientmanagement.
1. Wauchope G: The clinical importance of varia-tions in the number of cusps forming the aorticand pulmonary valves. Q J Med 21:383-399, 1928
2. Friedman T, Mani A, Elefteriades JA: Bicuspidaortic valve: Clinical approach and scientificreview of a common clinical entity. Expert RevCardiovasc Ther 6:235-248, 2008
3. Ward C: Clinical significance of the bicuspidaortic valve. Heart 83:81-85, 2000
4. Cripe L, Andelfinger G, Martin LJ, et al: Bicus-pid aortic valve is heritable. J Am Coll Cardiol44:138-143, 2004
5. Roberts WC: The congenitally bicuspid aorticvalve. A study of 85 autopsy cases. Am J Cardiol26:72-83, 1970
6. Pomerance A: Pathogenesis of aortic stenosisand its relation to age. Br Heart J 34:569-574, 1972
7. Movahed MR, Hepner AD, Ahmadi-Kashani M:Echocardiographic prevalence of bicuspidaortic valve in the population. Heart Lung Circ15:297-299, 2006
8. Tutar E, Ekici F, Atalay S, et al: The prevalenceof bicuspid aortic valve in newborns by
echocardiographic screening. Am Heart J 150:513-515, 2005
9. Basso C, Boschello M, Perrone C, et al: Anechocardiographic survey of primary schoolchildren for bicuspid aortic valve. Am J Cardiol93:661-663, 2004
10. Alegret JM, Palazón O, Duran I, et al: Aorticvalve morphology definition with transthoraciccombined with transesophageal echocardiogra-phy in a population with high prevalence ofbicuspid aortic valve. Int J Cardiovasc Imaging21(2-3):213-217, 2005
11. Huntington K, Hunter A, Chan K: A prospec-tive study to assess the frequency of familialclustering of congenital bicuspid aortic valve.J Am Coll Cardiol 30:1809-1812, 1997
12. Sabet HY, Edwards WD, Tazelaar HD, et al:Congenitally bicuspid aortic valves: A surgicalpathology study of 542 cases (1991 through1996) and a literature review of 2715 additionalcases. Mayo Clin Proc 74:14-26, 1999
13. Hope MD, Hope TA, Meadows AK, et al:Bicuspid aortic valve: Four-dimensional MRevaluation of ascending aortic systolic flowpatterns. Radiology 255:53-61, 2010
r 4
14. Bissell MM, Hess AT, Biasiolli L, et al: Aorticdilation in bicuspid aortic valve disease: Flowpattern is a major contributor and differs withvalve fusion type. Circ Cardiovasc Imaging 6:499-507, 2013
15. Della Corte A, Bancone C, Conti CA, et al:Restricted cusp motion in right-left type of bicus-pid aortic valves: A new riskmarker for aortopathy.J Thorac Cardiovasc Surg 144(2):360-369, 2012
16. den Reijer PM, Sallee 3rd D, van der Velden P,et al: Hemodynamic predictors of aortic dilata-tion in bicuspid aortic valve by velocity-encoded cardiovascular magnetic resonance.J Cardiovasc Magn Reson 12:4, 2010
17. Girdauskas E, Rouman M, Disha K, et al:Correlation between systolic transvalvular flowand proximal aortic wall changes in bicuspidaortic valve stenosis. Eur J Cardiothorac Surg(in press) 2014
18. Robicsek F, Thubrikar MJ, Cook JW, et al: Thecongenitally bicuspid aortic valve: How does itfunction?Why does it fail? Ann Thorac Surg 77:177-185, 2004
19. Barker AJ, Lanning C, Shandas R: Quantifica-tion of hemodynamic wall shear stress in
315
BICUSPID AORTIC VALVE AND ASSOCIATED AORTOPATHY
patients with bicuspid aortic valve using phase-contrast MRI. Ann Biomed Eng 38:788-800,2010
20. Nathan DP, Xu C, Plappert T, et al: Increasedascending aortic wall stress in patients withbicuspid aortic valves. Ann Thorac Surg 92:1384-1389, 2011
21. Saikrishnan N, Yap CH, Milligan NC, et al: Invitro characterization of bicuspid aortic valvehemodynamics using particle image velocime-try. Ann Biomed Eng 40(8):1760-1775, 2012
22. Meierhofer C, Schneider EP, Lyko C, et al: Wallshear stress and flow patterns in the ascendingaorta in patients with bicuspid aortic valvesdiffer significantly from tricuspid aortic valves:A prospective study. Eur Heart J CardiovascImaging 14:797-804, 2013
23. Girdauskas E, Borger MA, Secknus MA, et al: Isaortopathy in bicuspid aortic valve disease acongenital defect or a result of abnormalhemodynamics? A critical reappraisal of a one-sided argument. Eur J Cardiothorac Surg 39:809-814, 2011
24. Cotrufo M, Della Corte A: The association ofbicuspid aortic valve disease with asymmetricdilatation of the tubular ascending aorta: Iden-tification of a definite syndrome. J CardiovascMed (Hagerstown) 10:291-297, 2009
25. Della Corte A, Bancone C, Quarto C, et al:Predictors of ascending aortic dilatation withbicuspid aortic valve: A wide spectrum ofdisease expression. Eur J Cardiothorac Surg 31:397-404, 2007
26. Girdauskas E, Disha K, Raisin HH, et al: Risk oflate aortic events after isolated aortic valvereplacement for bicuspid aortic valve stenosis
316
with concomitant ascending aortic dilation. EurJ Cardiothorac Surg 42:832-838, 2012
27. Girdauskas E, Disha K, Borger MA, et al: Long-term prognosis of ascending aortic aneurysmafter aortic valve replacement for bicuspidversus tricuspid aortic valve stenosis. J ThoracCardiovasc Surg
28. Nistri S, Sorbo MD, Marin M, et al: Aortic rootdilatation in young men with normally func-tioning bicuspid aortic valves. Heart 82:19-22, 1999
29. Biner S, Rafique AM, Ray I, et al: Aortopathy isprevalent in relatives of bicuspid aortic valvepatients. J Am Coll Cardiol 53:2288-2295,2009
30. Girdauskas E, Schulz S, Borger MA, et al:Transforming growth factor-beta receptor typeII mutation in a patient with bicuspid aorticvalve disease and intraoperative aortic dissec-tion. Ann Thorac Surg 91:e70-e71, 2011
31. Girdauskas E, Disha K, Secknus MA, et al:Increased risk of late aortic events after isolatedaortic valve replacement in patients with bicus-pid aortic valve insufficiency versus stenosis.J Cardiovasc Surg (Torino) 54:653-659, 2013
32. Tadros TM, Klein MD, Shapira OM: Ascendingaortic dilatation associated with bicuspid aorticvalve. Pathophysiology, molecular biology,and clinical implications. Circulation 119:880-890, 2009
33. Wågsäter D, Paloschi V, Hanemaaijer R, et al:Impaired collagen biosynthesis and cross-linking in aorta of patients with bicuspid aorticvalve. J Am Heart Assoc 2(1):e000034, http://dx.doi.org/10.1161/JAHA.112.000034
Seminars in Thoracic and Cardiova
34. Kjellqvist S, Maleki S, Olsson T, et al: Acombined proteomic and transcriptomicapproach shows diverging molecular mecha-nisms in thoracic aortic aneurysm developmentin patients with tricuspid- and bicuspid aorticvalve. Mol Cell Proteomics 12(2):407-425, http://dx.doi.org/10.1074/mcp.M112.021873
35. Roberts WC, Vowels TJ, Ko JM, et al: Compar-ison of the structure of the aortic valve andascending aorta in adults having aortic valvereplacement for aortic stenosis versus for pureaortic regurgitation and resection of the ascend-ing aorta for aneurysm. Circulation 123:896-903, 2011
36. Girdauskas E, Rouman M, Borger MA, et al:Comparison of aortic media changes in patientswith bicuspid aortic valve stenosis vs bicuspidvalve insufficiency and proximal aortic aneur-ysm. Interact Cardiovasc Thorac Surg 17:931-936, 2013
37. Benedik J, Pilarzcyk K, Wendt D, et al: Is thereany difference in aortic wall quality betweenpatients with aortic stenosis and those withregurgitation? Eur J Cardiothorac Surg 44:754-759, 2013
38. Leone O, Biagini E, Pacini D, et al: Theelusive link between aortic wall histologyand echocardiographic anatomy in bicuspidaortic valve: Implications for prophylacticsurgery. Eur J Cardiothorac Surg 41:322-327, 2012
39. Robicsek F: Aortic media in bicuspid valvedisease. Ann Thorac Surg 76:337-338, 2003
scular Surgery � Volume 25, Number 4