bimm118 the four cornerstones of pharmacokinetics absorption distribution metabolism elimination...
Post on 20-Dec-2015
217 views
TRANSCRIPT

BIM
M11
8
The Four Cornerstones of Pharmacokinetics
• Absorption
• Distribution
• Metabolism
• Elimination
Absorption and distribution are influenced by the formulation:
Medicinal Agent --> Formulation --> Medication
Galenic = Science of pharmaceutical formulationTinctures of natural products – opium, vegetable drugs
(Galenos of Pergamon, 129-199 AD)
2011 Updated 1/11

BIM
M11
8
Drug Administration and Absorption
• Oral
• Topical (Percutaneous)
• Rectal or Vaginal
• Pulmonal
• Parenteral
Routes of Drug Administration:
Route of administration determined by chemical properties and stability of the active substance, desired concentration needed at target tissue, sensitivity of the active agent to degradation (enzymatic) and desired duration of action.
BIM
M11
8
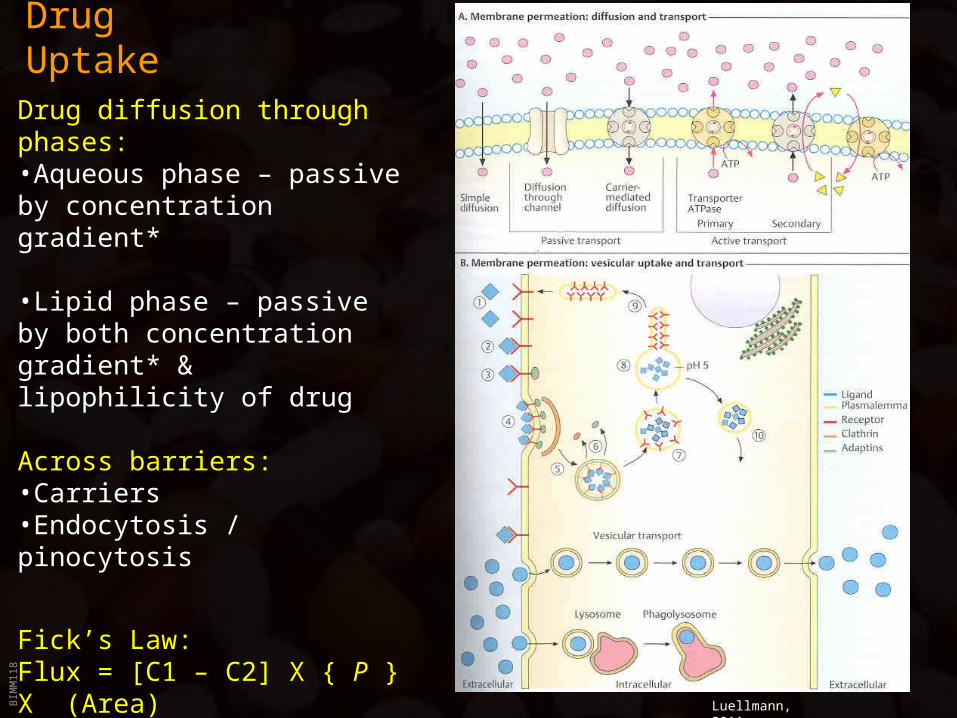
Drug Uptake
Luellmann, 2011
Drug diffusion through phases: •Aqueous phase – passive by concentration gradient*
•Lipid phase – passive by both concentration gradient* & lipophilicity of drug
Across barriers: •Carriers•Endocytosis / pinocytosis
Fick’s Law:Flux = [C1 – C2] X { P } X (Area)
P is PermeabilityP = Permeability coefficient
Thickness

BIM
M11
8
Oral Drug Administration
• Pills– Antiquated single-dose unit; round, produced by mixing
drug powder with syrup and rolling into shape
• Tablets– Oblong or disk-like shape, produced through mechanical
pressure; filler material provides mass; starch or carbonates facilitate disintegration

BIM
M11
8
Oral Drug Administration
• Coated Tablets– Tablet covered by a “shell” (wax, highly specialized polymers =
Eudragit®) to facilitate swallowing, cover bad taste or protect active ingredient from stomach acid

BIM
M11
8
Oral Drug Administration
• Matrix Tablets– Drug is embedded in inert “carrier” meshwork -->
extended or targeted (intestinal) release
• Capsules– Oblong casing (Gelatin); contains drug in liquid,
powder or granulated form
• Troches or Lozenges; Sublingual Tablets– Intended to be held in the mouth until dissolved

BIM
M11
8
Oral Drug Administration

BIM
M11
8
Oral Drug Administration
• Aequous Solutions (with Sugar=Syrup)– Mostly for pediatric use– 20 drops=1g
• Alcoholic Solutions (=Tinctures)– Often plant extracts– 40 drops=1g
• Suspensions– Insoluble drug particles in aequous or lipophilic media

BIM
M11
8
Percutaneous Drug Administration
Specific formulation determined by physician/dermatologist: • based on skin type:
– Dry vs. Oily– Young vs. Old– Intact vs. Injured
• based on drug properties:– Hydrophilic vs. Lipophilic– Soluble vs. Insoluble

BIM
M11
8
Percutaneous Drug Administration

BIM
M11
8
Percutaneous Drug Administration
• Ointment and Lipophilic Cream– Either pure lipophilic base (lanolin=wool fat; paraffin oil; petrolium jelly) or
“water-in-oil” emulsions
• Paste– Ointment with >10% pulverized solids (e.g. Zinc- or Titanium-Oxide)
• Lotion and Hydrophilic Cream– “oil-in-water” emulsions
• Gels– Either alcohol or aequous solution based (Ethanol gels --> Cooling effect)– Increased consistency due to gel-forming agents
BIM
M11
8
Percutaneous Drug Administration
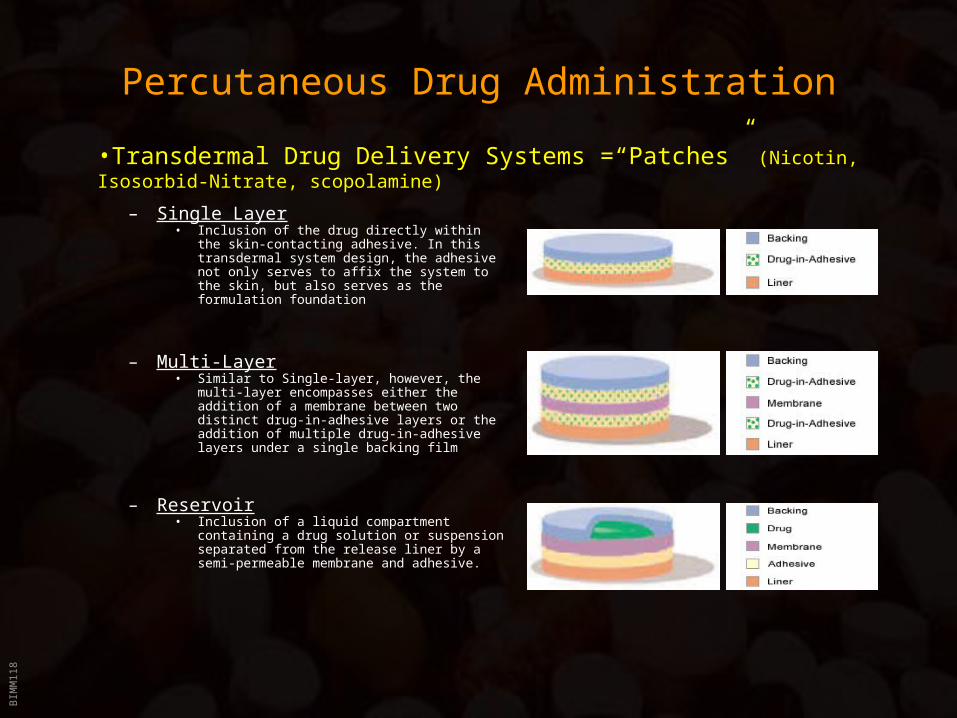
– Single Layer• Inclusion of the drug directly within the skin-
contacting adhesive. In this transdermal system design, the adhesive not only serves to affix the system to the skin, but also serves as the formulation foundation
– Multi-Layer• Similar to Single-layer, however, the multi-
layer encompasses either the addition of a membrane between two distinct drug-in-adhesive layers or the addition of multiple drug-in-adhesive layers under a single backing film
– Reservoir• Inclusion of a liquid compartment containing
a drug solution or suspension separated from the release liner by a semi-permeable membrane and adhesive.
•Transdermal Drug Delivery Systems =“Patches” (Nicotin, Isosorbid-Nitrate, scopolamine)
BIM
M11
8
Other Topical Drug Administration•Eye Drops
•Sterile; Isotonic; pH-neutral
•Nose Drops/Nasal Sprays•Viscous Solutions
•Pulmonary Formulations•Inhalation anesthetics (Hospital use only)•Nebulizers (mostly propellant operated)
•dispense defined amount of Aerosol (= dispersion of liquid or or solid particles in a gas)•Size of aerosol particles determines depth of penetration into the respiratory tract: >100 m: Nasopharynx
10-100 m: Trachea, bronchii<10 m: Bronchioli, alveoli

BIM
M11
8
Other Topical Drug Administration
•Suppositories •Drug incorporated into a fat with a melting point ~35ºC
•Rectal: Absorption mostly intended into systemic circulation (e.g. analgesics)•Vaginal: Effects intended to be confined to site of application (e.g. candidiasis)

BIM
M11
8
Parenteral Drug Administration
Sterile; iso-osmolar; pyrogen-free; pH=7.4
• Ampules– Single use (mostly with fracture ring)
• Single and Multi-dose Vials– 10-100 ml; contain preservatives
• Cartridge ampules
• Infusions– Solution administered over an extended period of time

BIM
M11
8
Parenteral Drug Administration
• Advantages:– 100% “Absorption”– Drug enters general circulation without hepatic passage -->
No first-pass hepatic elimination
– Better bioavailability of hydrophilic drugs
• Bioavailability/Speed of Absorption– Intravenous (i.v.): Fastest (infusions; cardio-vascular drugs)
– Intramuscular (i.m.): Medium (anti-inflammatory; antibiotics)
– Subcutaneous (s.c.): Slowest (vaccines; insulin; depot contraceptives)

BIM
M11
8
Drug Distribution

BIM
M11
8
Drug Distribution
• To be absorbed and distributed, drugs must cross barriers (membranes) to enter and leave the blood stream.
• Body contains two type of barriers which are made up of epithelial or endothelial cells:
– External (Absorption Barriers): Keratinized epithelium (skin), ciliated epithelium (lung), epithelium with microvilli (intestine), etc.
These epithelial cells are connected via zonulae occludens (tight junctions) to create an unbroken phospholipid bilayer. Therefore, drugs MUST cross the lipophilic membrane to enter the body (except parenteral).

BIM
M11
8
Drug Distribution
– Internal (Blood-Tissue Barriers): Drug permeation occurs mostly in the capillary bed,
which is made up of endothelial cells joined via zonulae occludens.
Blood-Tissue Barrier is developed differently in various capillary beds:
• Cardiac muscle: high endo- and transcytotic activity-> drug transport via vesicles
• Endocrine glands, gut: Fenestrations of endothelial cells (= pores closed by diaphragms)
allow for the passage of small molecules.
• Liver: Large fenestration (100 nm) without diaphragms-> drugs exchange freely between
blood and interstitium
• CNS, placenta: Endothelia lack pores and possess only little trans-cytotic activity-> drugs
must diffuse transcellularly, which requires specific physicochemical properties -> Barriers
are very restrictive, permeable only to certain types of drugs: “blood-brain barrier”

BIM
M11
8
Drug Distribution• Membrane Permeation:
– Passive Diffusion:
• Requires some degree of lipid solubility, which is in part determined by the charge of the molecule
• For weak acids or bases (which account for the vast majority of drugs), the charge of the molecule in dependence of the pH of the medium is determined by the Partition coefficient and the Henderson-Hasselbalch Equation:
Log ([H+Drug] / [Drug]) = pKa - pH
– Active Transport: Drugs “highjack” cellular transporter (e.g. L-DOPA uptake via L-amino acid carrier)
– Receptor-mediated Endocytosis: Clathrin-coated pits form endosomal vesicles; receptor gets “recycled” to the cell surface
[solute]octLog P(oct/water)=Log _________
[solute]water
Values negative = more water solubleValues positive = more octanol soluble

BIM
M11
8
Acid : HA A- + H+ Base : BH+ B + H+
Diffusible Form = HA Diffusible Form = BHenderson-Hasselbach Equation: Log [protonated form] = pKa - pH
[unprotonated form]Consider 2 compartments – with different pH values
blood pH = 7.4 urine pH = 5.4WHICH DIRECTION WILL THE DRUG MOVE, BLOOD TO URINE OR URINE TO
BLOOD?Always set X to = nondiffusible form, set the diffusible form concentration = 1.0 uMConsider weak base: Unprotonated form is readily diffusible. Assume a pKa = 7.0BLOOD: URINE:Log {X} = 7.0 – 7.4 = - 0.4 log {X} = 7.0 – 5.4 = 1.6 {1} {1}X = .398 X = 39.81Total species = 1 + .398 = 1.398uM = 1 + 39.81 = 40.81uM
As the base moves from blood into urine, it gets trapped thereConsider weak acid. Protonated form is readily diffusible; Assume a pKa = 4.4BLOOD: STOMACH:Log {1} = 4.4 – 7.4 = - 3.0 log {1} = 4.4 – 1.4 = 3.0 {X} {X}Log X = 3 X = 1000 Log X = -3.0 ; X = 0.001Total species = 1 + 1000 = 1001uM = 1 + 0.001 = 1.001uM
As the acid moves from stomach into blood, it gets trapped there

BIM
M11
8
Easy thought process for direction of drug movement“Ion Trapping”
For weak acid drugs:if compartment pH is LESS THAN pKa, less ionized, more of drug will pass bilayer membranes – increased flux across bilayerif compartment pH is MORE THAN pKa, more ionized, less of drug will pass bilayer membranes – decreased flux
For weak base drugs:if compartment pH is LESS THAN pKa, more ionized, less of drug will pass bilayer membranes – decreased fluxif compartment pH is MORE THAN pKa, less ionized, more of drug will pass bilayer membranes – increased flux

BIM
M11
8
Drug Distribution
Drug concentration is a function of absorbtion AND elimination:
Typical plasma drug concentration as function of time after a single oral dose
AUC = Area Under Curve
Plasma curve = rate entering plasma compartment – rate leaving plasma compartment

BIM
M11
8
Drug Distribution
Bioavailability (F):
the AUC of the (orally)
administered drug divided
by the AUC of the
intravenously
administered drug
NOTE: IV yields maximum plasma concentration at time = injection (0 time)

BIM
M11
8
Drug Distribution
Bioavailability:
• Intravenous 100% by definition• Intramuscular 75 to <100%• Subcutaneous 75 to <100%• Oral 5 to <100%• Rectal 30 to <100%• Inhalation 5 to <100%• Transdermal 80 to <100%

BIM
M11
8
Drug Distribution
Volume of Distribution (Vd) [ml or l]:
= Amount of drug in the body [mg] / drug concentrationplasma [mg/ml]
• Vd is an apparent volume (volume that the drug must be distributed in to produce measured plasma concentration
• Drug with near complete restriction to plasma compartment would have Vd = plasma volume (.04 L/kg) = 2.8 L/70 kg patient
– Blood volume is around 5.5L, ECF volume (sans plasma) is ~ 12 L, total body volume ~ 40 L
• But: Many drugs are highly tissue bound => large Vd. Where does it go?e.g. Chloroquine: Vd = 13,000 L

BIM
M11
8
Drug Distribution
Rate of Elimination:Drug elimination via kidney occurs by filtration => with falling blood
concentration the amount of drug filtered per time unit diminishesDrug elimination via liver occurs by metabolism, where most enzymes operate
in the quasi-linear range of their concentration-activity curve => with falling blood concentration the amount of drug metabolized per time unit diminishes
==>Vast majority of drugs follows first-order kinetics (= rate is proportional to drug concentration)
Only three drugs follow linear, zero-order (=concentration-independent) elimination characteristic: Ethanol, Aspirin and Phenytoin

BIM
M11
8
Drug Distribution (slide moved up 1)
Half-life (t1/2) [min]:
= ln 2 x Vd [ml] / CL [ml/min] (ln 2 = 0.693)
or
= ln 2 / Elimination rate constant (k) [1/min]
• Half-life is the time required for the concentration of a drug to fall by 50%
• The half-life is constant and related to (k) for drugs that follow first-order kinetics

BIM
M11
8
Clearance (New Slide)• How fast a drug is removed (cleared) from the body determines how the
drug is used therapeutically!– What will be the dose, how will it be given, what will be the rate of dosing?
• “VOLUME PER UNIT TIME”• Low: <500 ml/min; moderate: 500-1000 ml/min; high 1000-1500 ml/min• It is the sum of all separate organ clearances:
CL = CLrenal + CLliver + Clother
• Clearance is the volume of plasma cleared of all drug per unit of time (a constant for any given drug [ml/min])
• The actual quantity of drug [mg] removed per time unit [min] depends on both the clearance [ml/min] and the concentration [mg/ml].
• (Hepatic) extraction ratio = EH = 1 – [{Concentration out} / {Concentration in}]
• If EH = 0.8, only 20% of drug that enters on portal circulation leaves liver
• EH < 0.3: salicylic acid, phenobarbital, diazepam, digitoxin
• EH .3-.7: codeine, aspirin, quinidine
• EH >0.7: lidocaine, nitroglycerin, morphine, propranolol

BIM
M11
8
Drug Distribution
Clearance (CL) [ml/min]:
= Rate of Elimination [mg/min] / Drug concentrationplasma (CP) [mg/ml]
where
Rate of Elimination [mg/min] = k [1/min] x CP [mg/ml] x Vd [ml] and
Elimination rate constant (k) [1/min] = ln 2 / t1/2 (=half-life) (ln 2 = 0.693)
=> CL [ml/min] = Elimination rate constant (k) [1/min] x Vd [ml] = ln 2 x Vd / t1/2
• It is the sum of all separate organ clearances:
CL = CLrenal + CLliver + CLother
• Clearance is the volume of plasma cleared of all drug per unit of time (a constant for any given drug [ml/min])
• The actual quantity of drug [mg] removed per time unit [min] depends on both the clearance [ml/min] and the concentration [mg/ml].

BIM
M11
8
Drug Distribution
Dosage Regimens:With multiple dosing or continuous infusion, a drug will accumulate until the amount administered per time unit equals the amount eliminated per time unit. The plasma concentration at this point is called the steady-state concentration (CSS) [mg/ml]:
CSS = Infusion (dose) rate [mg/min] / Clearance [ml/min]
Typically, 90% of the CSS is reached after 3.3 half-lifes; ~100% after 5 half-lifes

BIM
M11
8
Drug Distribution
Loading Dose:
For drugs with long t1/2, 3-5 half-lifes is to long to wait for CSS
=> loading dose is used.
Loading dose must ‘fill’ the Vd to achieve the target CP:
Loading dose [mg] = {Vd [ml] x CP [mg/ml]} / bioavailability
Maintenance Dose:
Must replace the drug that is being eliminated over time:
CSS [mg/ml] = Infusion rate [mg/min] / Clearance [ml/min] =>
Infusion rate [mg/min] = Clearance [ml/min] x CSS [mg/ml] =>
Infusion rate [mg/min] = ln 2 x Vd [ml] / t1/2 [min] x CSS [mg/ml]

BIM
M11
8
Drug Distribution
• Drug Binding to Plasma Proteins:• Primarily albumin (4.6g/100ml), also -globulins and acidic glycoproteins• Other specialized plasma proteins (transcortin; thyroxin-binding globulin; etc.)
Binding to plasma proteins is instantaneous and reversible.• Of great importance, as the free (=effective) drug concentration determines
intensity of response
Drug-protein binding also influences biotransformation and elimination =>Binding to plasma proteins is equivalent to depot formulations
– Possible site for drug interactions: If two drugs bind to the same site on e.g. the albumin molecule, then drug B has the potential of displacing drug A from its binding site --> effective concentration of drug A is increased --> Toxic concentration or increased elimination
– Impaired liver function: can lead to altered pharmacokinetics of drugs that bind to albumin at
high rates due to decreased albumin concentrations in the blood
BIM
M11
8
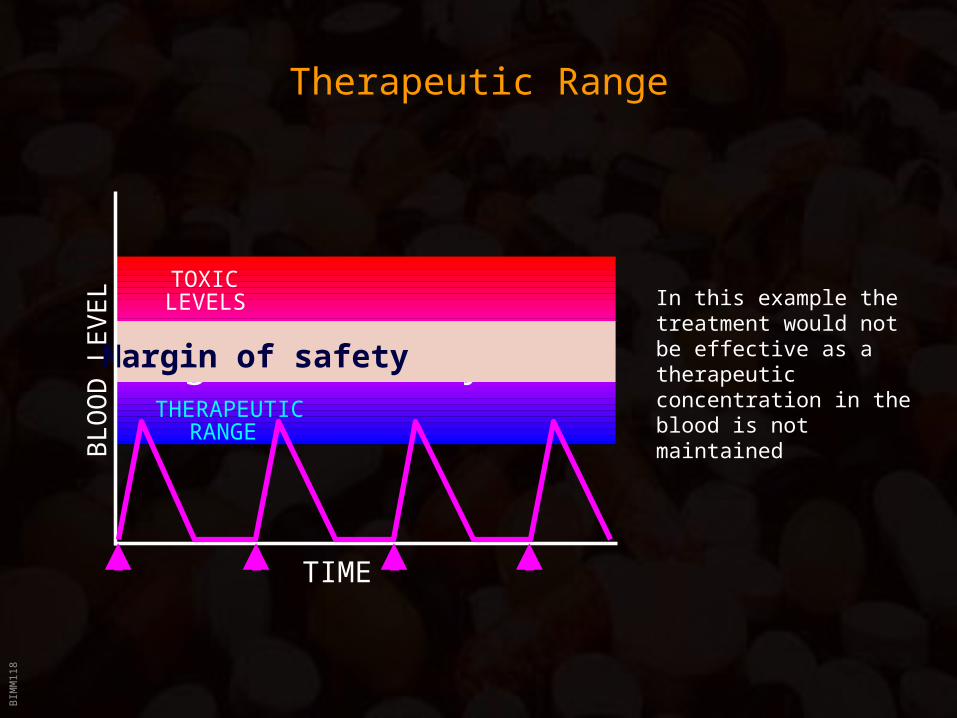
Therapeutic Range
Margin of safetyTHERAPEUTIC
RANGE
TOXICLEVELS
BL
OO
D L
EV
EL
Margin of safety
TIME
In this example the treatment would not be effective as a therapeutic concentration in the blood is not maintained

BIM
M11
8
Therapeutic Range
Margin of safetyTHERAPEUTIC
RANGE
TOXICLEVELS
BL
OO
D L
EV
EL
Margin of safety
TIME
In this example severe toxicity would occur as the therapeutic concentration in the blood is exceeded due to accumulation of the drug

BIM
M11
8
Therapeutic Range
Margin of safetyTHERAPEUTIC
RANGE
TOXICLEVELS
BL
OO
D L
EV
EL
Margin of safety
TIME
In this example the treatment would be effective as the therapeutic concentration in the blood is maintained without approaching toxic levels
BIM
M11
8
Therapeutic Range
• Therapeutic Index:= Maximum non-toxic dose / Minimum effective dose
Problem:
Does not take into account variability between individuals
=> “Improved formula”:
= LD50 / ED50
Problems:
• LD50 reflects only death, but no other toxic side effects (e.g. Ototoxicity of
aminoglycosides)
• ED50 depends on condition treated (e.g. Aspirin: Headache vs. rheumatism)
• LD50 depends on patients overall condition (e.g. Aspirin: dangerous to asthmatic patients)
==>
Therapeutic Index is not particularly useful to describe the clinical usefulness of a drug!
BIM
M11
8
Drug Metabolism and Elimination
• Elimination of drugs occurs primarily through renal mechanism– Secretion into bile also possible, but allows for re-absorption in the intestine
• Secretion into the urine requires ionized or hydrophilic molecules, but:– Most drugs are not small molecules that are highly ionized at body pH
– Most drugs are poorly ionized and lipophilic
=> This decreases renal excretion and facilitates renal tubular reabsorption
– Many drugs are highly protein bound, and therefore not efficiently filtered in the kidney
– Most drugs would have a long duration of action if termination of their effects
depended only on renal excretion
Solution: Drug Metabolism