bio-medical waste 1 - cpcb enviscpcbenvis.nic.in/envis_newsletter/bmw newsletter.pdf · bio-medical...
TRANSCRIPT



1 Bio-Medical Waste
1. Introduction
1.1 Background
io-medical waste is generated during the diagnosis, treatment or immunization of human beings or
animals or in research activities pertaining thereto or in the production or testing of biologicals. It include wastes like human anatomical waste, animal waste, microbiology & biotechnology waste, waste sharps, discarded medicines & cytotoxic drugs, soiled waste, solid waste, liquid waste, incineration ash, chemical wastes. These wastes are potentially hazardous because of the potentially infectious in nature as it may pose a serious threat to human health, if its management is indiscriminate and unscientific. Earlier, bio-medical waste management was not an integral part of the health care programme. The negligence on the part of health care waste management programme, in the past, was reflected in various articles in the newspapers and public litigations in various Courts including in the Hon’ble Supreme Court and this is also evident from the sporadic epidemics experienced in different parts of the Country. Realizing the gravity of the issue and to comply with the directions of the Hon’ble Supreme Court in the matter of W.P (Civil) filed by Dr. B. L. Wadhera, the Central Pollution Control Board (CPCB) took up the matter, in right earnest, with the Ministry of Environment & Forests (MoEF) and subsequently, in July, 1998, the Government of India has enacted the Bio-medical Waste (Management & Handling) Rules (BMW Rules) under
Sections 6, 8, 25 of the Environment (Protection) Act, 1986 for ensuring effective management of bio-medical waste generated from Health Care Facilities (HCFs), without causing any adverse effect on human health and the environment. Due to this legal binding, the HCFs have streamlined the process of waste segregation, collection, treatment and safe disposal of bio-medical waste in accordance with the BMW Rules. The Bio-medical Waste (Management & Handling) Rules are comprehensive and stipulates that ‘it shall be the duty of every occupier of an institution generating bio-medical waste which includes a hospital, nursing home, clinic, dispensary, veterinary institution, animal house, pathological laboratory, blood bank as well as Operator of a Common Bio-medical Waste Treatment Facility (CBWTF) to take adequate steps for environmentally sound management of such waste”. Also “Every occupier of an institution generating, collecting, receiving, storing, transporting, treating, disposing and/or handling bio-medical waste in any other manner [except such occupier of clinics, dispensaries, pathological laboratories, blood banks providing treatment/service less than 1000 (one thousand) patients per month] shall make an application in Form I to the prescribed authority for grant of authorization”. The BMW Rules classify bio-medical waste into ten categories (Figure 1) and emphasizes segregation of bio-medical waste at the source of generation, storage in accordance with the colour coding bins/bags and its labelling as stipulated under schedule –II & Schedule-III of the BMW Rules respectively, packaging and transportation of waste in accordance with
B
ENVIS Centre 01, CPCB

2 Bio-Medical Waste
Schedule-IV, submission of Annual Report in Form 2, for the preceding year, to the prescribed authority prior to 31st of January every year, constitution of an Advisory Committee by the State Government or Union Territory (UT) in the respective State or UT, maintenance of records related to generation, collection, reception, storage, transportation, treatment, disposal and/or any form of handling of bio-medical waste, accident reporting in accordance with the Rules. The BMW Rules also stipulate that the occupier is required to ensure that the bio-medical waste generated is treated and disposed of within 48 hours. The BMW Rules encourages to have captive treatment equipment like incinerator/ autoclave/ microwave and shredder, by the HCFs, for ensuring on-site treatment and disposal of waste as per provisions of the BMW Rules. These rules were further amended in the year 2000 and 2003 so as to fill the gaps experienced while implementing the BMW Rules. Through the second amendment in the year 2000, the provisions for prescribed authority i.e. State Pollution Control Board (SPCB)/ Pollution Control Committee (PCC) were stipulated for enforcement of the provisions of these Rules in the respective State/UT. Municipal Corporations, Municipalities or Urban & Local Bodies, as the case may be, made responsible for providing suitable common disposal/ incineration sites for the biomedical wastes generated in the area under their jurisdiction and in areas outside the jurisdiction of any municipal body, it shall be the responsibility of the occupier
generating bio-medical waste/ operator of a bio-medical waste treatment facility (CBWTF) to arrange for suitable sites individually or in association, so as to comply with the provisions of these rules. The Municipal body of the area shall continue to pick up and transport segregated non-bio-medical solid waste as well as duly treated bio-medical wastes for disposal at municipal sanitary landfills. The concept of CBWTF is also being widely accepted in India among the health care units, medical associations and other concerned entrepreneurs. Also, as per the amended Rules, occupier/operator wishing to use other State-of-the-art technologies shall approach the Central Pollution Control Board (CPCB) to get the standards laid down to enable the prescribed authority to consider grant of authorisation. The BMW Rules were further amended in the year 2003, whereby Director General, Armed Forces Medical Services (DGAFMS) notified as Prescribed Authority for enforcement of the BMW Rules by the Health Care Establishments (HCEs) under the Ministry of Defence. Advisory Committee for implementation of the BMW Rules by the HCEs under the Ministry of Defence is also required to be constituted under the Chairmanship of Additional Director General of Armed Force Medical Services and other members from Ministry of Defence, MoEF, Indian Society of Hospitals Waste Management, Pune. CPCB has a limited role and is required to monitor the implementation of the BMW Rules by the Armed Forces Health Care Establishments under the Ministry of Defence.
ENVIS Centre 01, CPCB

3 Bio-Medical Waste
The BMW Rules also specify standards for the bio-medical waste treatment and disposal for incineration and other environmental friendly technologies like autoclaving/ microwaving, liquid waste discharge standards as well as disposal of bio-medical waste by deep burial. Disposal of bio-medical waste by deep burial is permitted only in cities or towns where population is less than 5 lakhs and the deep burial pit is required to be followed only in consultation with the respective SPCB/PCC.
1.2 Bio-Medical Waste Segregation at Source and Characterization
BMW Rules emphasis segregation of bio-medical waste at source of generation. Segregation of wastes at source of generation helps:
I. to minimize mixing of bio-medical waste with that of the municipal solid waste generated within the HCFs ;
II. to reduce volume of waste to be handled/treated;
III. to minimize cost of treatment ;
IV. to minimize toxic emissions ; and
V. to facilitate effective recovery of
useful plastics etc. Bio- Medical waste is divided into 10 waste categories and is given in Figure 1 and the category-wise bio-medical waste treatment and disposal option is given in Table 1 and the type of colour coded container or bag to be used is given in Table 2.
1.Human and
Anatomical Waste
2.Animal Waste
3. Microbiology and
Bio-technology Waste
4.Waste Sharps
5.Discarded Medicines and Outdated Drugs
6.Soiled Waste
7. Solid Waste
8.Liquid Waste
9.Incineration ash
10. Chemical Waste
Figure 1: Categoreis of Bio-medical waste
ENVIS Centre 01, CPCB

4 Bio-Medical Waste
Table 1: Categories of Bio-medical Waste and the Treatment & Disposal Options
Waste Category Waste Class and Description Treatment and Disposal [Option]
No. 1 Human Anatomical Wastes, (Human tissues, organs, waste body parts)
Incineration @/ deep burial*
No. 2
Animal Wastes (Wastes consisting of animal tissue, organs, body parts, carcasses, body fluid, blood and blood products, items contaminated with blood and fluids, wastes from surgery treatment and autopsy and wastes of experimental animals used in research, waste generated by veterinary hospitals, colleges, animal houses and livestock farms)
Incineration @/ deep burial*
No. 3
Microbiology & Biotechnology Waste (Wastes from laboratory, culture stocks or specimens of micro-organisms, live or attenuated vaccines, human and animal cell culture used in research and infectious agents from research and industrial laboratories, wastes from production of biological dishes and devices used for transfer of cultures)
Local Autoclaving / microwaving/incineration @
No. 4
Waste Sharps (Needles, syringes, scalpels, blades, glass, etc that are capable of causing puncture and cuts. This includes both used and unused sharps)
Disinfection using chemical treatment/autoclaving/microwaving and mutilation. shredding and disposal in landfill / recycling (for PVC, plastics and glassw ares)
No. 5 Discarded Medicines (Wastes comprising of outdated, contaminated and discarded medicines)
Incineration @ or destruction and disposal in landfills
No. 6
Soiled Wastes (Wastes generated from soiled cotton, dressings, plaster casts, linens, beddings, material contaminated with blood including the packaging materials)
Incineration @ autoclaving/microwaving
No. 7
Solid Waste (Wastes generated from disposable items other than the waste sharps such as tubings, catheters, intravenous sets etc.)
Disinfection by chemical treatment@@ autoclaving/microwaving and mutilation/shredding ##
No. 8 Liquid Waste (waste generated from laboratory and washing, cleaning, house-keeping and disinfecting activities)
Disinfection by chemical treatment@@ and discharge into drains.
No. 9 Incineration Ash (ash from incineration of any bio-medical waste)
Disposal in municipal landfill
No. 10 Chemical Waste (Chemicals used in production of biologicals, chemicals used in disinfection, as insecticides, etc.)
Chemical treatment@@ and discharge into drains for liquids and secured landfill for solids
@@ Chemical treatment using at least 1% hypochlorite solution or any other equivalent chemical reagent. It must
be ensured that chemical treatment ensures disinfection.
## Mutilation/shredding must be such so as to prevent unauthorised reuse.
@ There will be no chemical pretreatment before incineration. Chlorinated plastics shall not be incinerated.
* Deep burial shall be an option available only in town with population less than five lakhs and in rural areas.
ENVIS Centre 01, CPCB

5 Bio-Medical Waste
Table 2: Colour coded container or bags to be used for segregation of bio-medical waste
1.3 Bio-Medical Waste Quantification
According to World Health Organization (WHO) report, about 85% of the hospital waste are actually non-hazardous, 10% are infectious, and 5% are non-infectious but hazardous, which is given in Figure 2.
Figure 2: Composition of BMW generated
in HCFs
Sharps represent about 1% of the total waste but they are a major source of disease transmission if not managed properly. Chemicals and pharmaceuticals account for about 3% of waste from health-care activities while genotoxic waste, radioactive matter and heavy metal account for around 1% of the total health-care waste. Based on the literature, the quantity of hospital waste generated in some developed countries are given in Table 3.
Table 3 : Quantity of Bio-medical Waste generated in few Countries
Sl. No. Name of the
Country
Quantity of Bio-medical waste (kg/bed/day)
(i). Netherlands 2.7 (ii). France 2.5 (iii). USA 4.5 (iv). Latin America 2.63 to 3.8 (v). India 0.3 to 1.0
85%
10%
5%
Bio-Medical Waste (Percentage % composition)
Non-hazardouswastesInfectious wastes
Non-infectious &hazardous
Colour Coding Type of container Waste category Treatment options
Yellow Plastic Bag
Human Anatomical Waste/Animal Waste, Microbiology and Biotechnology waste and Soiled waste
Incineration / Deep Burial
Red Disinfected container/ plastic bag
Microbiology and Biotechnology waste and Soiled waste
Autoclave/ Microwave/ Chemical Treatment
Blue Plastic Bag/ Puncture-proof container
Waste sharps, Solid waste Autoclave/Microwave/ Chemical Treatment and destruction / shredding
White (or) Translucent
Black Plastic Bag
Discarded Medicines/Cytotoxic Drugs, Incineration ash and Chemical waste
Disposal in secured landfill
ENVIS Centre 01, CPCB

6 Bio-Medical Waste
Studies carried out in India, shows generation of bio-medical waste in the range of 0.3 to 1.0 kg/bed/day of which around 50% of the wastes is collected as infectious wastes (category 1 & 2). However, effective segregation of these human & anatomical wastes in HCFs would reduce the quantity of infectious waste needing incineration/deep burial.
2. Status of Bio-medical Waste Management in the Country
2.1 Present Scenario As per the annual report information received from the State Pollution Control Boards (SPCBs)/Pollution Control Committees (PCCs) and Director General of Armed Forces Medical Services (DGAFMS) for the year 2013, the bio-medical waste management scenario in the Country is given in Table 4.
Table 4: Bio-Medical Waste Management Scenario in the Country
(As submitted by the SPCBs/PCCs & DGAFMS for the year 2013)
Items Number/ Quantity
No. of Health Care Facilities (HCFs) 1,68,869 No. of beds 17,13,816 No. of Common Bio-medical Waste Treatment Facilities (CBWTFs) 198* + 28**
No. of HCFs using CBWTFs 1,31,837 No. of HCFs having treatment & disposal facilities 22,245
No. of HCFs applied for authorization 1,06,805 No. of HCFs granted authorization 1,05,270 Total no. of on-site/captive treatment equipment
installed (excluding CBWTFs) by the HCFs: No. of incinerators i). With Air Pollution Control Device 331 ii). Without Air Pollution Control Device 217
• No. of autoclaves 3,112 • No. of microwaves 250 • No. of Hydroclaves 15 • No. of Shredders 5,179 Total no. of treatment equipment installed by the
CBWTFs: • No. of Incinerators 198 • No. of autoclaves 189 • No. of microwaves 06
Items Number/ Quantity
• No. of Hydroclaves 03 • No. of Shredders 202 Quantity of bio-medical waste generated in Tons/day 484
Quantity of bio-medical waste treated in Tons /day 447
No. of HCFs violated BMW Rules 7,894 No. of Show-cause notice/Directions issued to defaulter HCFs 4,391
Note: (i). * - CBWTFs in Operation; (ii). ** - CBWTFs under installation (iii). The information in respect of the Lakshdweep State has been included as per the Annual Report Submitted for the Year 2012.
As per the details given in Table 4, total number of Health Care Facilities (HCFs) in India have been reported as 1,68,869 (this may also contain number of HCFs which do not come under the purview of Authorization as required under BMW Rules) and 1,06,805 number of healthcare facilities applied for authorization. This certainly indicates that number of HCFs are in operation without obtaining authorization from the respective SPCB/ PCC. The number of HCFs (authorized/ unauthorized) as well as unregistered HCFs are on large number which may be involved in improper bio-medical waste management in the Country. Approximately 92.3% i.e., 447 out of 484 Tons per day bio-medical waste generated is being treated and disposed of either through 198 no. of Common Bio-medical Waste Treatment Facilities or captive treatment equipment installed by the HCFs.
548 no. of incinerators, 3112 autoclaves, 250 microwaves, 15 hydroclaves and 5179 shredders are installed by the HCFs as captive treatment equipment in the country. 198 no. of incinerators are operated by the CBWTFs. 331 (60.4%) out of 548 captive bio-medical waste Incinerators operated by HCFs are provided with air pollution control devices.
ENVIS Centre 01, CPCB

7 Bio-Medical Waste
There has been increase in number of CBWTFs over the years and at present there are 226 CBWTFs (i.e. 198 CBWTFs are in operation and 28 CBWTFs are under installation) so as to facilitate proper treatment and disposal of bio-medical waste in the Country. The state-wise no. of CBWTFs which are in operation and the no. of CBWTFs which are under construction are given in Table 5.
Table 5: State-wise Status of CBWTFs in
the Country (As submitted by the SPCBs/PCCs for the year 2013)
STATE/ UT CBWTFs
Operational Under construction
A. P. (Including Telangana) 17 02
Assam 05 0 Bihar 03 01 Chandigarh 02 0 Chhattisgarh 05 0 D & D & DNH 01 0 Delhi 03 0 Gujarat 15 09 Haryana 11 01 H. P. 02 0 J & K 04 0 Jharkhand 01 0 Karnataka 18 09 Kerala 01 0 Maharashtra 40 01 M. P. 14 0 Meghalaya 01 0 Odisha 05 0 Punjab 04 01 Puduchherry 01 0 Rajasthan 12 03 Tamil Nadu 11 01 Tripura 01 0 Uttarakhand 02 0 U. P. 14 0 W. B. 05 01
Total 198 28 (i) Data as submitted by SPCBs, PCCs (ii) No CBWTFs in A&N, Arunachal, Goa, Lakshdweep,
Manipur, Mizoram, Nagaland & Sikkim.
3. Bio-medical Waste Management Scenario since 2007
The Annual Report information provided by the SPCB/PCC & DGAFMS and the same is now available at www.cpcb.nic.in. Based on the same salient features are given in the subsequent paras:
3.1 Health Care Facilities (HCFs)
As compared to 2008, 177% growth in the number of HCFs is observed in the year 2013 in the country. This may be attributed to population growth and the concern for providing public health services. 3.2 Authorisation Status of HCFs It is observed that the SPCBs/PCCs have so far targeted only the larger occupiers of an institution generating bio-medical waste requiring authorization from them, where as it is required to bring in all the generators of bio-medical wastes irrespective of their size of operation (less than 1000 patients per month) under the purview of the rules to ensure safe disposal of bio-medical waste. The cumulative quantity of bio-medical waste generated from such facilities if considered would be significant, which needs immediate attention. Figure 3 & 4 Indicates No. of HCFs applied for Authorisation and No. of HCFs obtained Authorisation from the SPCBs/PCCs.
ENVIS Centre 01, CPCB

8 Bio-Medical Waste
Figure 3: No. of HCFs Applied for Authorization under BMW Rules during the years 2007-13
Figure 4: No. of HCFs Obtained Authorization under BMW Rules during the years 2007-13 As the number of HCFs are increasing since 2007, the applications for authorization under BMW Rules are also increasing at the same pace and accordingly, authorization granted to such HCFs by the respective SPCB/PCC is increased. However, there is still gap between number of HCFs applied for authorization to SPCBs/PCCs and number of HCFs which have been granted
authorization under BMW Rules by the respective SPCB/PCC.
3.3 HCFs utilizing Common Bio-medical Waste Treatment Facilities/ Private agencies
HCF is having option for treatment and disposal of bio-medical waste either by
47750
61293 57180
7753784396
102086 106805
0
20000
40000
60000
80000
100000
120000
2007 2008 2009 2010 2011 2012 2013
No. of HCFsapplied forAuthorisationto SPCB/PCC
4566158845 53813
7080079903
98074105270
0
20000
40000
60000
80000
100000
120000
2007 2008 2009 2010 2011 2012 2013
No. of HCFsgrantedauthorisationby SPCB/PCC
ENVIS Centre 01, CPCB

9 Bio-Medical Waste
having captive treatment equipment or it may be disposed of through a CBWTF or any other private agency authorized by the SPCB/PCC as the case may be. In order to comply with the provisions of the Rules, some of the HCFs have installed captive treatment facilities and others are availing services of Common Bio-medical Waste Treatment Facilities (CBWTFs).
In the year 2013, it is observed that 1,31,837 out of 1,68,869 HCFs are utilizing the CBWTFs/private agencies. The no. of HCFs utilizing the CBWTFs and the no. of HCFs having captive treatment facilities as observed during the years 2007-2011 are given in the Figure 5 & Figure 6.
Figure 5: No. of HCFs which are utilizing CBWTFs/Private Agencies during the years 2007-2013
Figure 6: No. of HCFs Having Captive Treatment and Disposal Facilities during
the years 2007-2013
14068
11948
20670
20228
23668
21870
22245
0 5000 10000 15000 20000 25000
2007
2008
2009
2010
2011
2012
2013
No. of HCFsHaving CaptiveTreatment AndDisposal facilities
49971
63434
95410
97764
112199
121279
131837
0 20000 40000 60000 80000 100000 120000 140000
2007
2008
2009
2010
2011
2012
2013
No. of HCFs whichare utilizingCBWTFs/ privateagencies
ENVIS Centre 01, CPCB
10 Bio-Medical Waste
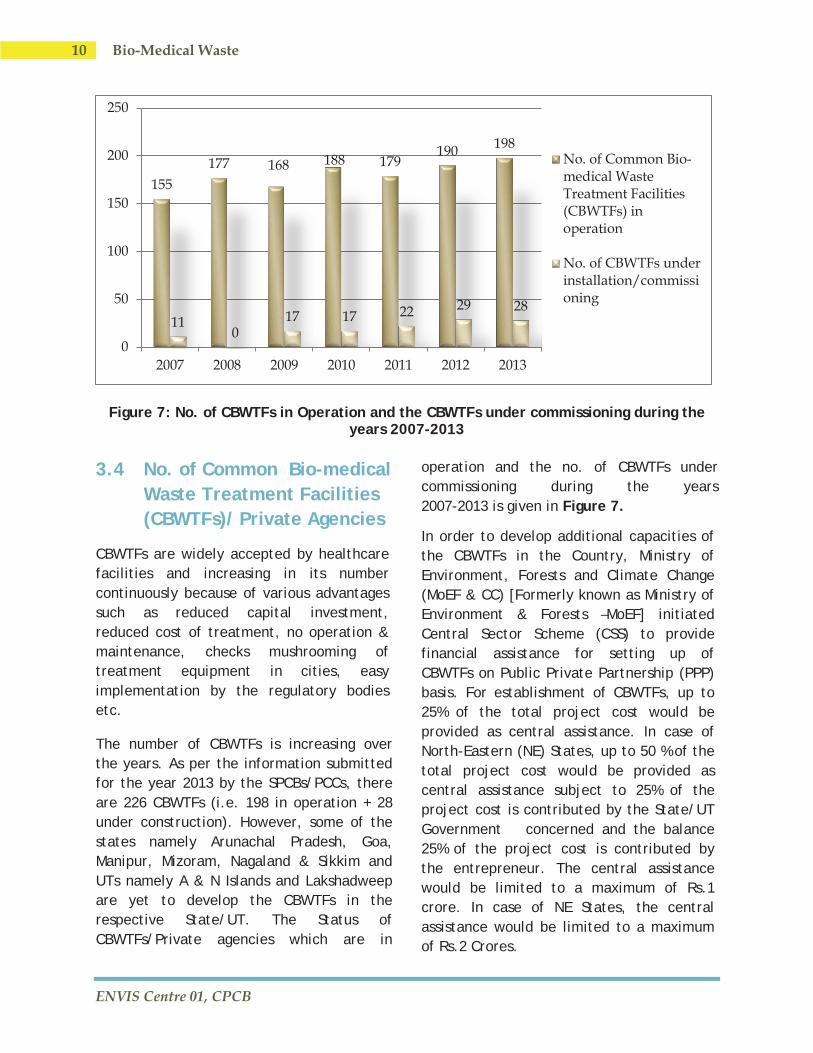
Figure 7: No. of CBWTFs in Operation and the CBWTFs under commissioning during the years 2007-2013
3.4 No. of Common Bio-medical Waste Treatment Facilities (CBWTFs)/ Private Agencies
CBWTFs are widely accepted by healthcare facilities and increasing in its number continuously because of various advantages such as reduced capital investment, reduced cost of treatment, no operation & maintenance, checks mushrooming of treatment equipment in cities, easy implementation by the regulatory bodies etc.
The number of CBWTFs is increasing over the years. As per the information submitted for the year 2013 by the SPCBs/PCCs, there are 226 CBWTFs (i.e. 198 in operation + 28 under construction). However, some of the states namely Arunachal Pradesh, Goa, Manipur, Mizoram, Nagaland & Sikkim and UTs namely A & N Islands and Lakshadweep are yet to develop the CBWTFs in the respective State/UT. The Status of CBWTFs/Private agencies which are in
operation and the no. of CBWTFs under commissioning during the years 2007-2013 is given in Figure 7.
In order to develop additional capacities of the CBWTFs in the Country, Ministry of Environment, Forests and Climate Change (MoEF & CC) [Formerly known as Ministry of Environment & Forests –MoEF] initiated Central Sector Scheme (CSS) to provide financial assistance for setting up of CBWTFs on Public Private Partnership (PPP) basis. For establishment of CBWTFs, up to 25% of the total project cost would be provided as central assistance. In case of North-Eastern (NE) States, up to 50 % of the total project cost would be provided as central assistance subject to 25% of the project cost is contributed by the State/UT Government concerned and the balance 25% of the project cost is contributed by the entrepreneur. The central assistance would be limited to a maximum of Rs.1 crore. In case of NE States, the central assistance would be limited to a maximum of Rs.2 Crores.
155177 168 188 179
190 198
110
17 17 22 29 28
0
50
100
150
200
250
2007 2008 2009 2010 2011 2012 2013
No. of Common Bio-medical WasteTreatment Facilities(CBWTFs) inoperation
No. of CBWTFs underinstallation/commissioning
ENVIS Centre 01, CPCB

11 Bio-Medical Waste
In order to ensure and to help the CBWTF operators to comply with the provisions of the Bio-medical Waste (Management & Handling) Rules and to have and uniformity in maintaining minimum requirements such as efficient treatment equipment, required infrastructure, proper transportation system, proper recording system, environmentally sound method of disposal of treated bio-medical waste etc., Central Pollution Control Board has prepared following guidelines:
i. Common Bio-medical Waste TreatmentFacilities; and
ii. Design & Construction of bio-medicalwaste incinerators
3.5 Total Quantity of Bio-medical Waste Generation & Treatment (Kg/day approx.)
CPCB is continuously pursuing and requesting all SPCBs/PCCs to take necessary steps to
ensure that Bio Medical Waste generated from various Hospitals/Nursing Homes and other Health Care Units are disposed off in an environmentally sound manner so as to prevent spread of diseases and infections. Due to regular pursuance, over the sample period (i.e. 2007 to 2013), it is observed that there is a significant decrease in total biomedical waste generation, which is due to significant improvement in segregation of bio-medical waste at the source of generation. Also, the gap between the total bio-medical waste generation and the total bio-medical waste treated is reduced significantly and is evident from the above sample period. In the year 2013, about 92% of the bio-medical waste in India is reported to be treated as per provisions of BMW Rules as compared to about 57% in the year 2007.
The Bio-medical waste generation as well as treatment & disposal scenario during the years 2007 to 2013 is given in the Figure 8.
506745
409114
414956
354992
415194
416040
484271
288204
295272
301237
303033
377876
332538
447456
0 100000 200000 300000 400000 500000 600000
2007
2008
2009
2010
2011
2012
2013
Total Quantity of BMW treated (Kg/day) Total Quantity of BMW generated (Kg/day)
Figure 8. Total Quantity of Bio-medical Generation as well as Treatment & Disposal Scenario during the years 2007-2013
ENVIS Centre 01, CPCB

12 Bio-Medical Waste
4. Standards for Treatmentand Disposal ofBio-medical Waste
Bio-medical waste shall be treated and disposed of in accordance with Schedule-I, and in compliance with the standards prescribed in Schedule-V of the BMW Rules. Standards for incineration, autoclaving, and microwaving and disposal by deep burial have been prescribed in the Rules, which are detailed below:
4.1 Standards for Incineration
A. Operating Standards
• Combustion Efficiency (CE) shallbe atleast 99.0%.
• The combustion efficiency iscomputed as follows:
%CO2 C.E. = ——————— × 100
% CO2 + % CO
• The temperature of the primarychamber shall be 800 ± 50°C.
• The secondary chamber gasresidence time shall be atleast 1(one) second at 1050 ± 50°C withthe minimum 3% oxygen in thestack gas.
B. Emission Standards
• PM 150mg/Nm3 (12% CO2 correction)• NO2 450 mg/Nm3 -do- • HCl 50 mg/Nm3 -do- • Minimum stack height shall be
30 meters above ground
• Volatile organic compounds in ashshall not be more than 0.01%.
Note : • Suitably designed air pollution
control devices shall be installed/retrofitted with the incinerator to achieve the aboveemission limits, if necessary.
• Wastes to be incinerated shall not bechemically treated with anychlorinated disinfectants.
• Chlorinated plastics shall not beincinerated.
• Toxic metals in incineration ash shallbe limited within the regulatoryquantities as defined under theHazardous Waste (Management andHandling Rules), 1989. (Now, theserules are called Hazardous WasteManagement Handling & TransboundaryMovement Rules, 2008)
• Only low sulphur fuel like L.D.O./L.S.H.S./Diesel shall be used as fuelin the incinerator.
4.2 Standards for Waste Autoclave
A. When operating a gravity flow autoclave, medical waste shall be subjected to :
• A temperature of not less than121°C and a pressure of 15 poundsper square inch gauge (psi) for anautoclave residence time of not lessthan 60 minutes;
• A temperature of not less than135°C and a pressure of 31 psi foran autoclave residence time of notless than 45 minutes; or
ENVIS Centre 01, CPCB

13 Bio-Medical Waste
• A temperature of not less than 149°C and a pressure of 52 psi for an autoclave residence time of not less than 30 minutes;
B. When operating a vacuum autoclave, medical wastes shall be subjected to a minimum of one pre-vacuum pulse to purge the autoclave of all air. The waste shall be subjected to the following:
• A temperature of not less than 121°C and a pressure of 15 psi for an autoclave residence time of not less than 45 minutes; or
• A temperature of not less than 135°C and a pressure of 31 psi for an autoclave residence time of not less than 30 minutes;
C. Medical waste shall not be considered properly treated unless all time/ temperature/ pressure indicators indicate that the required time / temperature / pressure were reached during the autoclave process. If for any reasons, time /temperature / pressure indicator indicates that the required temperature, pressure or residence time was not reached, the entire load of medical waste must be autoclaved again until the proper temperature, pressure and residence time were achieved.
D. Recording of operational parameters
Each autoclave shall have graphic or computer recording devices which will automatically and continuously monitor
and record dates, time of day, load identification number and operating parameters throughout the entire length of the autoclave cycle.
E. Validation Test
(i) Spore Testing : The autoclave shall completely and consistently kill the approved biological indicator at the maximum design capacity of each autoclave unit. Biological indicators for autoclave shall be Bacillus stearothermophilus spores using vials or
spore strips, with at least 1 × 104 spores per millilitre. Under no circumstances will an autoclave have minimum operating parameters less than a residence time of 30 minutes, regardless of temperature and pressure, a temperature less than 121°C or a pressure less than 15 psi.
(ii) Routine Test: A chemical indicator strip/tape that changes colour when a certain temperature is reached can be used to verify that a specific temperature has been achieved. It may be necessary to use more than one strip over the waste package at different location to ensure that inner content of the package has been adequately autoclaved.
4.3 Standards for Microwaving
• Microwave treatment shall not be used for cyto-toxic, hazardous or radioactive wastes, contaminated animal carcasses, body parts, and large metal items.
• The microwave system shall comply with the efficacy test/routine tests and a performance guarantee may be provided by the supplier before operation of unit.
ENVIS Centre 01, CPCB

14 Bio-Medical Waste
• The microwave should completely and consistently kill the approved biological indicator at the maximum design capacity of each microwave unit. Biological indicators for microwave shall be Bacillus Subtilis spores using vials or spore strips, with at least 1 x 104 spores per millilitre.
4.4 Liquid Waste Discharge Limits
The effluents generated from the hospital shall conform to the limits given in Table 6.
Table 6: Liquid Effluent Discharge limits for the HCFs
Parameter Permissible Limit pH 6.5 – 9.0 Suspended solids 100 mg/l Oil and grease 10 mg/l BOD 30 mg/l COD
Bio-assay test
250 mg/l 90% survival of fish after 96 hours in 100% effluent
Note: These limits are applicable to those hospitals which are either connected with sewers without sewage treatment plant or not connected to public sewers at all. For discharge into public sewers having terminal treatment facility, the general standards as notified under the Environment (Protection) Act shall be applicable.
4.5 Standards for Deep Burial
Deep burial should have the following specifications:
1. A Pit or trench should be dug about two (2) meter deep. It should be half filled with waste, then covered with lime
within 50 cm of the surface, before filling the rest of the pit with soil.
2. It must be ensured that animals do not have any access to burial. Covers of galvanized iron/wire meshes may be used.
3. On each occasion, when wastes are added to the pit, a layer of 10 cm of soil shall be added to over the wastes.
4. Burial must be performed under close and dedicated supervision.
5. The deep burial site should be relatively impermeable and no shallow well should be close to the site.
6. The pits should be distant from habitation, and sited so as to ensure that no contamination occurs of any surface water or ground water. The area should not be prone to flooding or erosion.
7. The location of the deep burial site will be authorized by the prescribed authority.
8. The institution shall maintain a record of all pits for deep burial.
A typical deep burial pit is given in Figure 9.
Figure 9: Typical deep burial pit for disposal of bio-medical waste
ENVIS Centre 01, CPCB

15 Bio-Medical Waste
5. Liquid Waste Management in HCFs
Schedule-I of the Bio-medical Waste (Management & Handling) Rules, 1998 as amended stipulates that liquid waste generated from laboratory and washing, cleaning, house-keeping and disinfecting activities of the HCF is required to be treated and disposed off either by ‘disinfection by chemical treatment (using at least 1% hypochlorite solution or any other equivalent chemical reagent) and discharge into drain. Also, schedule-V of the BMW Rules stipulates that effluent generated from the hospital should confirm to the discharge limits, which are applicable as detailed below:
(i) In case the effluent from hospitals connected with public sewers without terminal sewage treatment plant, then limits prescribed under schedule-V of the BMW Rules shall be applicable. In such case, the hospital should set up ETP of their own so as to meet the discharge norms; and
(ii) In case of effluent from hospital connected to public sewers with terminal facilities, the general standard as notified under the Environment (Protection) Act, 1986 shall be applicable.
At present, most of the HCFs are not having Effluent Treatment Plants (ETPs) in the Country. For ensuring proper treatment of wastewater generated from the HCFs, ETP should be installed. ETP should also be connected with a provision of ‘press filter’ or ‘sludge drying bed’ for drying the sludge generated from the ETP and after drying, same need to be disposed of in an
environmentally sound manner depending upon the hazardous constituents present in it.
A typical ETP installed by the HCF is given in Figure 10.
Figure 10: Typical ETP installed by the HCF
6. New Technologies for Treatment of Bio-medical Waste
As per Schedule-I of the Bio-medical Waste (Management & Handling) Rules, 1998 & as amended, any Health Care Facility (HCF) or Common Bio-medical Waste Treatment Facility (CBWTF) Operator wishing to use other Stat-of-the-art-technologies other than stipulated under Schedule-I of the said rules, shall approach the Central Pollution Control Board (CPCB) to get the standards laid down to enable the prescribed authority to consider grant of authorization. For the purpose of evaluation of new technologies for treatment of bio-medical waste and to suggest suitable standards for any such technologies, an Expert Committee was reconstituted by CPCB.
During the last five years, CPCB have granted conditional or provisional approval
ENVIS Centre 01, CPCB

16 Bio-Medical Waste
to new Technologies (other than notified under BMW Rules) for treatment of bio-medical waste, under the BMW Rules as under:
(1) Plasma Pyrolysis; (2) Waste Sharps Dry heat sterilization
and encapsulation (3) Shredding cum Chemical disinfection
(Static/Mobile)'
6.1 Plasma Pyrolysis Technology Alternate to incinerator, 'Plasma Pyrolysis' treatment technology can be adopted for treatment and disposal of bio-medical waste wherein destruction of bio-medical waste similar to the incineration can be achieved. In case of plasma pyrolysis, bio-medical waste is treated at high temperature under controlled condition to form gases like methane, hydrogen and carbon monoxide which are subjected to combustion (oxidation) in secondary chamber. In the plasma pyrolysis process waste is converted into small clinker which can be disposed in secured landfills.
CPCB granted provisional approval to the ‘Plasma Pyrolysis Technology’ as an additional option for treatment of Bio-medical waste categories 1, 2, 5 & 6 of the BMW Rules. A pilot scale plasma pyrolysis facility is given in Figure 11.
Figure 11: A Pilot Scale Plasma Pyrolysis System
6.2 Waste Sharps Dry Heat Sterilization & Encapsulation
‘Waste Sharp Dry Heat Sterilization & Encapsulation’ technology is based on 'dry heat sterilization' especially for treatment of waste category no. 04 (i.e. waste sharps) as listed under Schedule-I of the BMW Rules, 1998. Approval to this technology is accorded by CPCB under the Bio-medical Waste (Management & Handling) Rules, 1998 as amended subject to the conditions. Dry Heat Sterilization & Encapsulation of Waste Sharps treatment equipment and the canister before used for collection of waste sharps and the canister after treatment are given in the Figures 12 to 15.
Figure 12: Dry Heat Sterilisation System
ENVIS Centre 01, CPCB

17 Bio-Medical Waste
Figure 13 to 15: Canister before and after Treatment of Waste Sharps by Dry Heat Sterilization & Encapsulation
6.3 Shredding cum Chemical Disinfection of Bio-medical Waste (Static/Mobile)
This technology is based on ‘shredding followed by chemical disinfection’ of
biomedical waste. Provisional approval to this technology is accorded by CPCB for treatment of bio-medical waste on trial basis for evaluation / efficacy of the technology. This is a non-burn technology, in which bio-medical waste is shredded beyond recognition and sterilized so as to make it suitable for disposal along with municipal solid waste. The equipment (both mobile and static models) are given in the Figures 16 & 17.
Figure 16: Shredding cum Chemical Disinfection of Bio-medical Waste
Treatment Technology – Mobile Unit
Figure 17: Shredding cum Chemical Disinfection of Bio-
medical Waste Treatment Technology – Static Unit
ENVIS Centre 01, CPCB

18 Bio-Medical Waste
7. Awareness Programme on Bio-medical Waste Management
(i). CPCB developed a 40 minutes video film on bio-medical waste management in order to generate awareness about the safe management of bio-medical waste and same is available in CPCB Website at link: http://cpcb.nic.in/Bio_medical_docu.php.
(ii). During the year 2010-11, CPCB organized four one day workshops on ‘Bio-medical Waste Management’ at Goa, Lucknow, Guwahati & Bhubaneshwar for various stake holders with the financial support received from Ministry of Environment, Forests and Climate Change (MoEF & CC) and also sponsored to organize workshop on bio-medical waste management to Mizoram SPCB during the financial year 2011-12;
(iii). CPCB also organized four “Interaction meets” with the CBWTF operators and the concerned SPCBs/PCCs during the financial years 2011 to 2014 and imparted technical know-how to upgrade their existing facilities in line with the CPCB guidelines for CBWTFs and also requested to ensure strict compliance to the BMW Rules & CPCB guidelines; and
(iv). A documentary film namely
‘Bio-medical Waste Management’ under ‘Paryavaran Darshan’ in collaboration with ‘Doordarshan’ was
telecasted on March 26, 2011 & August 13, 2011 as a part of creating awareness on the BMW Management aspects to all the concerned including the general public.
Photographs relating to the workshop & interaction meet with CBWTF operators organized by CPCB are given in Figures 18 to 19.
Figure 18. Workshop Organised during June 09-10, 2011 By Mizoram SPCB with
financial support from CPCB
Figure 19. Interaction meet held with CBWTF Operators of Western Zone
* * *
For more information please refer to: http://www.cpcb.nic.in
http://www.cpcbenvis.nic.in
ENVIS Centre 01, CPCB

19 Bio-Medical Waste
In-house publications on 'Waste'
Series Publications HAZWAMS/36/2009-10 Report of the Committee on Evolve Road Map on Management Waste in India HAZWAMS/37/2009-10 Report of Hazardous Chemicals Investigation in India CUPS/41/1994-95 Management of Municipal Solid Wastes - Status and Options
CUPS/46/99-2000 Status of Solid Waste Generation, Collection, Treatment and Disposal in Metro cities
CUPS/53/2002-03 Municipal Solid Waste Processing Technologies Review and Guidelines for Local Bodies
PROBES/24/1983-84 Characteristics and Treatment of Wastewater from an Electric Bulb Manufacturing Unit : A case Study
PROBES/80/2001-02 Guidelines for Health & Safety of Workers in Wastewater Treatment Facilities PROBES/103/2005-06 Assessment of Utilisation of Industrial Waste in Cement Manufacturing
PROBES/111/2007 Bio-Methanation Potential of Agro based Solid Waste from Agro Based Industries
PROBES/113/2007 Plastic Waste Management Issues and Options
PROBES/132/2009 Assessment of Plastic Waste & Its Management at Air Port & Railway Station in Delhi
LATS/16/2002-03 Manual on Sampling, Analysis and Characterisation of Hazardous Wastes LATS/17/2004-05 Bio-Medical Waste Management – Case Study NCT – Delhi
RERES/1/1985-86 Recycling of Sewage & Industrial Waste on Land a Monitoring & Surveillance Report on Chandigarh Sewage farm
RERES/2/2001-02 Constructed Wetlands for Waste Water Treatment IMPACTS/2/99-2000 Manual on Hospital Waste Management HAZWAMS/8/1996-97 Inventorisation of Hazardous Waste Generation in Kerala State HAZWAMS/9/1996-97 Inventorisation of Hazardous Wastes Generating Industries in Orissa HAZWAMS/10/1996-97 Inventorisation of Hazardous Wastes Generation in Punjab
HAZWAMS/11/1998-99 Guidelines for Setting up of Operating Facility: Hazardous Waste Management
HAZWAMS/13/1998-99 Inventorisation & Management of Hazardous Waste in Andhra Pradesh
HAZWAMS/19/2001-02 Inventorisation and Management of Hazardous Waste Generation in West Bengal
HAZWAMS/24/2002-03 Identification of Hazardous Wastes Streams Their Characterisation and Waste Minimisation Options in Petrochemical Sector
HAZWAMS/27/2004-05 Identification of Hazardous Waste Streams their Characterisation and Waste Reduction Options in Dyes & Dye Intermediate Sector
HAZWAMS/29/2005-06 Identification of Hazardous Waste Streams their Characterisation & Management Options in Bulk Drugs & Pharmaceuticals Sectors
HAZWAMS/38/2010-11 Protocol for Performance Evaluation and Monitoring of the Common Hazardous Waste Treatment Storage and Disposal Facilities including Common Hazardous Waste Incinerators
HAZWAMS/39/2011-12 Environmentally Sound Management of Mercury Waste Generated from Health Care Facilities
Newsletters Municipal Solid Wastes Management Bio-medical Waste Wastes Hazardous Waste Management Plastic Waste Management Urban Waste Profile (ENVIS Newsletter)
ENVIS Centre 01, CPCB
20 Bio-Medical Waste
ENVIS Centre 01, CPCB

