bladder & urethral calculi
DESCRIPTION
blader & urethral calculiTRANSCRIPT
Bladder Calculi(Batu Buli-buli)
Rifa Roazah
Incidence
By the 19th century accounted for 80% of urolithiasis in Europe
Some historical figures : King Leopold I of Belgium, Napoleon Bonaparte, Emperor Napoleon III, Peter the Great, Louis XIV, George IV, Oliver Cromwell, Benjamin Franklin, Chief Justice John Marshall, Sir Francis Bacon, Sir Isaac Newton, the physicians Harvey and Boerhaave, and the anatomist Scarpa.
In the lower urinary tract, most calculi occur in the bladder.
Vesical calculi can be classified as migrant primary idiopathic secondary calculi
Migrant Calculi
Calculi formed in the upper tracts, pass into the bladder, and are retained there.
Most calculi <1 cm and in adults, are easily passed per urethra.
Retained upper tract stones may grow to a large size in the bladder
Primary Idiopathic (Endemic) Calculi
Form in children in the absence of obstruction, local disease, neurologic lesion, or known primary infection.
Remain common in infants and children of lower socioeconomic background (ex : North Africa)
Results from dietary and nutritional deficiencies
Children in these areas are dependent on a cereal-based diet (wheat flour, millet, and rice) that is lacking in animal proteins, especially cow's milk LOW PHOSPORUS
Leads to low urine phosphate excretion and high peaks of ammonia excretion
Most commonly composed of ammonium acid urate alone or in combination with calcium oxalate, but many also contain calcium phosphate.
Chronic dehydration,
excessive protein or oxalate
consumption, high endogenous
oxalate production, and deficiencies in vitamins A, B1,
and B6 and magnesium
associated with stone formation
Children younger than 10 years are typically affected, with the peak incidence : 3 years
Male-to-female ratio 10:1 Common symptoms :
vague abdominal pain hypogastric discomfort interruption of the urinary stream pulling and rubbing of the penis Some children complain of dysuria, frequency,
suprapubic pain, and dribbling.
Small calculi may be passed with hydration, antispasmodics, and analgesics, but most cases will require surgical intervention.
Usually solitary and rarely recur once removed.
Secondary Bladder Calculi Predominantly a disease of adults and
accounts for approximately 5% of urinary calculi in developed countries
Related to : urinary stasis recurrent urinary tract infection due to
bladder outlet obstruction or neurogenic bladder dysfunction.
foreign bodies in the urinary tract

Calculi Related to Bladder Outlet Obstruction
More than 75% of bladder calculi cases Associated with outlet obstruction Affect men older than 50 years and are
most often related to benign prostatic hyperplasia
Calculi resulting from obstruction may be composed of uric acid, calcium, or magnesium ammonium phosphate if infected.
Other causes of outlet obstruction : urethral stricture bladder neck contracture neurogenic bladder dysfunction in women, urogenital prolapse
Calculi Related to Infection or Catheterization
Residual urine from outlet obstruction predisposes to infection, and combined, these factors may result in stone formation
Most commonly with Proteus. Organisms such as Pseudomonas, Ureaplasma urealyticum, Providencia, Klebsiella, Staphylococcus, and Mycoplasma are also capable of producing bacterial urease.
The urease hydrolyzes urea, forming ammonium and carbon dioxide, which increases urine pH. Alkaline urine promotes supersaturation and precipitation of crystals of magnesium ammonium phosphate.

Long-term bladder catheterization risk for urinary infection and calculus formation.
Approximately 50% to 98% of catheter-associated calculi are composed of magnesium ammonium phosphate; the remainder are a combination of calcium oxalate and phosphate or pure calcium phosphate
Patients managed with an indwelling urethral or suprapubic catheter had a ninefold increased risk for development of a bladder stone compared with patients who were catheter free and had continent bladder control

Foreign Body Nidus Calculi
The urinary tract is the occasional repository for a wide array of foreign objects
These foreign bodies can be classified as : self-induced iatrogenic migrant
Self-induced insertion may be the result of psychological abnormalities
Calculi may develop on foreign objects in the absence of infection
Stone formation is inhibited by dilution, diuresis, and acidification of urine
Stone formation is enhanced with infection, especially with urea-splitting organisms
Calculi may form around nearly any type of suture.
Foley catheters act as foreign bodies; encrustations may form around the tip or the balloon of the catheter.
These encrustations may act as nidi for further stone growth.
Bladder calculi from migrant foreign bodies have been reported as complications of urologic and nonurologic surgical procedures.
Symptoms & Diagnosis
Most bladder calculis are asymptomatic and are found incidentally.
Patients with significant bladder outlet obstruction may : initially present with lower urinary tract symptoms or recurrent (persistent) urinary tract infections, especially with a urea-splitting organism.
Symptoms
Intermittent voiding with increase in terminal dysuria caused by lodging at the bladder neck.
Painful voiding (varying quality and exacerbated by exercise and sudden movement). The pain may be referred to the tip of the penis, the scrotum, or the perineum and on occasion to the back or the hip.
Recumbent position may alleviate the symptoms.
Hematuria
Diagnosis
Plain radiographs may be missed because of overlying bowel gas, soft tissue shadowing, and the radiolucent quality of some calculi.
Ultrasonography can be used to detect radiolucent calculi but may be limited by bowel gas.
CT Scan

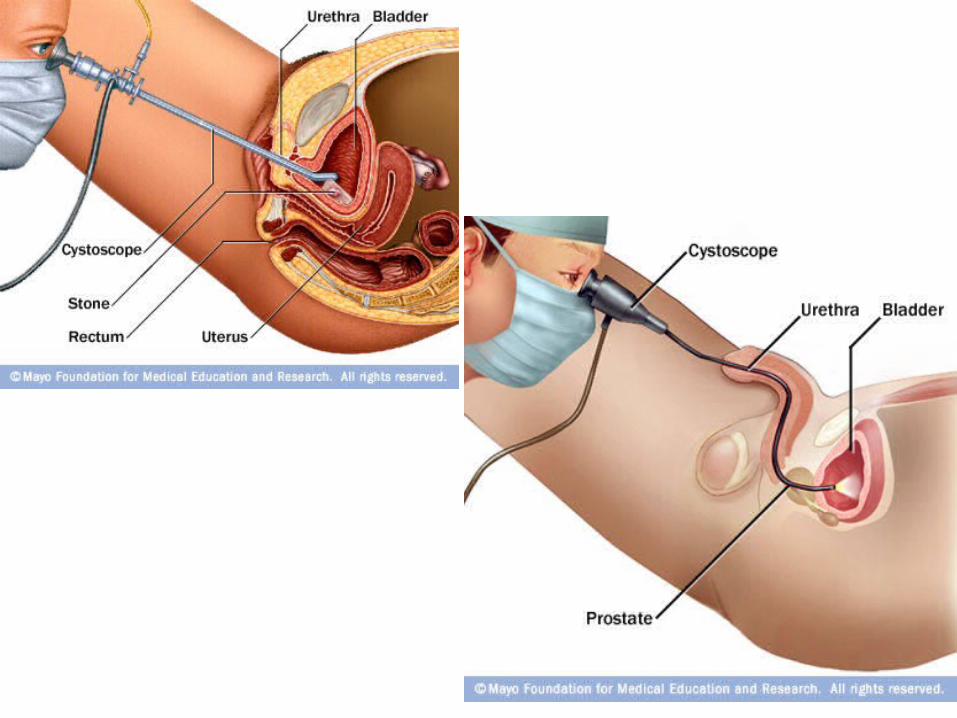
Cystoscopy is the single most accurate examination to document the presence of a bladder calculus.
Cystoscopy assists in surgical planning by identifying prostatic enlargement, urethral stricture that may need correction before or in conjunction with the treatment of the stone.
Management
The majority of bladder calculi are treated endoscopically
The approach is influenced by : patient's anatomy and comorbidities stone size, location, and composition previous stone treatment risks and complications
In addition to removal of the calculi, treatment should address predisposing factors such as bladder outlet obstruction, urinary stasis, infection, and foreign bodies to minimize recurrence.
Chemolysis
Suby solution G or hemiacidrin dissolve magnesium ammonium phosphate calculi.
Uric acid calculi oral sodium or potassium citrate.
Dissolution for primary treatment of bladder calculi is now rarely employed.
Shockwave Lithotripsy
The bladder is filled with 100 to 150 mL of normal saline through the catheter to improve visualization.
After the calculus has been localized, the bladder is drained, which minimizes stone migration.
Multiple treatments of bladder calculi with SWL may be required to achieve stone-free status
SWL may be considered for those who are unfit for surgery because of comorbid medical conditions or who refuse surgery.
Cystolitholapaxy
Cystolitholapaxy is the crushing of the calculus with irrigation of the fragments from the bladder in a single operation.
Contraindications : small-capacity bladders multiple stones or calculi larger than 2 cm hard stones bladder calculi in children small-caliber urethras
During the procedure, the bladder should be filled with about 200 mL of irrigant.
The stone is then crushed manually, and the procedure is repeated several times until fragments can no longer be caught.
Energy pneumonik, electrohydraulic, ultrasonic, laser
Percutaneous Cystolithotomy Indicated in pediatric patients with
narrow urethras and in patients with large stone burdens or multiple calculi
Contraindications : a history of bladder malignant disease prior abdominal or pelvic surgeries prior pelvic radiotherapy active urinary or abdominal wall infection pelvic prosthetic devices
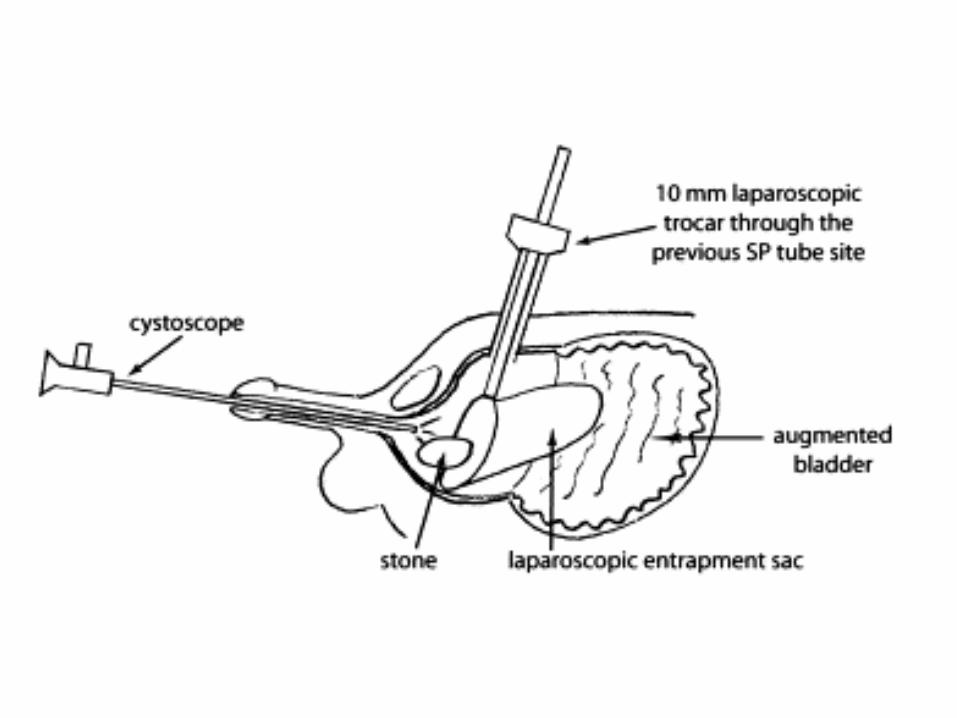
The percutaneous puncture is positioned above the symphysis or at a prior suprapubic tube site
Success rates for percutaneous cystolithotomy range from 85% to 100% with various energy sources
Cystolithotomy
Although rarely used today, open cystolithotomy for the treatment of bladder calculi is associated with a high success rate
Good for very large or hard stones Other indications :
abnormal anatomy failure of an endoscopic approach concomitant open prostatectomy
Urethral Calculi(Batu Uretra)
Rifa Roazah
Urethral calculi represent less than 2% of all urinary stone disease in the Western world
Urethral calculi in women are exceptionally rare because of low rates of bladder calculi and a short urethra that permits passage of many smaller calculi.
Urethral calculi can be classified as either native or migrant. Native urethral calculi form de novo in association with abnormalities that predispose to urinary stasis and infection. Calculi may form proximal to strictures, in congenital or acquired diverticula, with chronic infection (especially with urea-splitting organisms), with foreign bodies, in schistosomiasis, and with use of hair-bearing skin for urethroplasty. These calculi are frequently composed of struvite, calcium phosphate, or calcium carbonate.

Calculi in the female urethra are typically associated with urethral diverticulum or urethrocele
The majority of urethral calculi in men are migrant, formed in the urinary bladder or upper tract, whose passage has been impeded in the urethra
Although stones smaller than 10 mm should pass through the normal urethra, areas of possible stone impaction are the prostatic urethra, the bulb, the proximal penile urethra, the fossa navicularis, and the external meatus. A migrant stone may become impacted at the site of a urethral stricture.
Symptoms
Native urethral stones generally do not cause acute symptoms because of their slow development and growth.
Patients may present with a mass that has gradually increased in size and hardness on the undersurface of the penis or anterior wall of the vagina, urethral discharge, dyspareunia, irritative voiding symptoms, and hematuria.
Adult men with urethral calculi may present with acute retention or complaints of frequency, dysuria, poor or interrupted urinary stream, incomplete emptying, and dribbling or incontinence. Pain caused by the stone may be severe.
When the calculus is lodged in the posterior urethra, the pain is referred to the perineum or the rectum. When the calculus is lodged in the anterior urethra, the pain may be localized at the site of the impaction.

Diagnosis
Rectal examination may detect stones in the posterior urethra. Radiography can be helpful but requires proper positioning of the patient as urethral calculi are frequently overlooked on plain films and intravenous urograms.
Treatment
Treatment is contingent on the size and location of the calculus and condition of the urethra.
The objective of treatment is relief of obstruction and foreign body removal without damaging the urethra and periurethral tissues.
Urethroscopic lithotripsy and removal of stone fragments is useful in almost any situation.
Meatotomy may be used if the stone is lodged in the fossa navicularis or the external meatus.
A stone in the anterior urethra may be treated with the judicial use of forceps.
On occasion, a small stone may sometimes be gently massaged or milked outward, so that it can be expelled.
When a stricture obstructs passage of a stone, dilatation or internal urethrotomy may be necessary before the manipulation.
Calculi in the posterior urethra can be treated in situ or pushed back into the bladder and treated as vesical calculi
Referensi
Urologi Basuki Urologi Smith Urologi Campbell