bloodborne pathogens - texas department of insurance · bloodborne pathogens. the bloodborne...
TRANSCRIPT
HS02-037B (4/09)
Bloodborne PathogensQuestions and Answersabout Occupational Exposure
Bloodborne PathogensQuestions and Answers about Occupational Exposure
Table of Contents SECTION I 1Bloodborne Pathogens Standard 1
29 CFR 1910.1030 1SECTION II 5
Exposure Control Plans29 CFR 1910.1030(c) 5Exposure Determination29 CFR 1910.1030(c) 5
Training 629 CFR 1910.1030(G) 6
SECTION III 7Preventive Measures Hepatitis B Vaccination 29 CFR 1910.1030(f) 7Universal precautions29 CFR 1910.1030(c) 8
SECTION IV 8Methods of Control 8
Engineering controls and work practices 29 CFR 1910.1030 829 CFR 1910.1030(3)Personal protective equipment (PPE) 1029 CFR 1910.1030(4) Housekeeping 1129 CFR 1910.1030(g) Labeling 14
SECTION V 1429 CFR 1910.1030(f) Exposure Incidents 14
SECTION VI 1529 CFR 1910.1030(1) Record Keeping 15
Appendix A Statement of Declination 17Appendix B Bloodborne Pathogens Exposure Control Plan 18Engineering and WorkPractices Controls (terms) 19
Sharps containers 19Safe medical devices 19Work practices 19Personal protective equipment (PPE) 19Storage area 19PPE use & disposal 19Housekeeping 19Contaminated laundry 20
Regulated waste 20Labels and signs 20Hepatitis B vaccine 20Exposure incident & post-exposure evaluation & follow-up 20Training & training records 21Record keeping 21Plan evaluation and review 21
Example of Sharps Injury Log 22
1
THE KEY TO ACCESSIBILITY
This document was originally produced by the Department of Consumer & Business Services, Oregon Occupational Safety & Health Division (OR-OSHA). Material contained in this publication is in the public domain and may be reproduced without permission from OR-OSHA or the Texas Department of Insurance, Division of Workers’ Compensation (TDI/DWC).
INTRODUCTION
The intent of this question-and-answer manual is to help employers and employees understand the requirements for exposure to hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) and other bloodborne pathogens. Acquired immunodeficiency syndrome (AIDS) and hepatitis B merit serious concern for workers occupationally exposed to blood, other potentially infectious materials, and certain other body fluids that contain such bloodborne pathogens as HIV and HBV. According to estimates of the Occupational Safety and Health Administration (OSHA), more than 5.6 million workers in health-care and public safety occupations could be exposed to these viruses.Such workers include physicians, dentists, dental
employees, phlebotomists, nurses, morticians, paramedics, medical examiners, laboratory and blood bank technologists and technicians, housekeeping personnel in health-care institutions, laundry workers, employees in long-term-care facilities, and home-care workers. Other workers, who may be occupationally exposed to blood or other potentially infectious materials, depending on their work assignments, include research laboratory workers and public-safety personnel (fire, police, rescue, correctional officers, etc.). Exposure to bloodborne pathogens occurs in many ways. Although needlestick injuries are the most common means of exposure for health-care workers, bloodborne pathogens can also be transmitted through contact with eyes, nose, and mouth or through broken skin. TDI/DWC & OSHA recognize the need to safeguard workers from health hazards related to bloodborne pathogens. The bloodborne pathogens standard aims to reduce the risk of occupational exposure to bloodborne diseases.
SECTION IBloodborne Pathogens Standard29 CFR 1910.1030The bloodborne pathogens standard tells how to
determine who has occupational exposure and how to reduce workplace exposure to bloodborne pathogens.
Q. What are bloodborne pathogens?
A. Bloodborne pathogens are microorganisms that can cause disease when transmitted from an infected individual to another individual through blood and certain body fluids. Bloodborne pathogens are capable of causing serious illness and death. The most common illnesses caused by bloodborne pathogens are hepatitis B (HBV), hepatitis C, (HCV), and acquired immunodeficiency syndrome (AIDS) from HIV, or human immunodeficiency virus.
Q. What is HBV?
A. HBV is the virus that causes hepatitis B. Hepatitis B, formerly called “serum hepatitis,” is a life-threatening bloodborne pathogen and a major risk to employees in jobs where there is exposure to blood and other potentially infectious materials (OPIM). Hepatitis, which means “inflammation of the liver,” can be caused by drugs, toxins, autoimmune disease, and infectious agents, including viruses.
Q. What is HCV?
A. HCV is the virus that causes hepatitis C. It is the most common chronic Bloodborne infection in the United States and is primarily transmitted through large or repeated direct percutaneous (through the skin) exposure to blood. Most people who are chronically infected are not aware of their infection because they are not clinically ill. Infected persons can infect others and are at risk for chronic liver disease or other HCV-related chronic diseases. Currently there is no vaccine against hepatitis C.

2
Q. Who is covered by the bloodborne pathogens standard?
A. OSHA’s rule applies to all persons that are occupationally1 exposed to blood or other potentially infectious materials. Blood means human blood, blood products, or blood components. OPIM include the following:
• Human body fluids: semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pleural fluid, pericardial fluid, peritoneal fluid, amniotic fluid, saliva in dental procedures, any body fluid visibly contaminated with blood, and all body fluids in situations where it is difficult or impossible to differentiate between body fluids.
• Any unfixed tissue or organ (other than intact skin) from a human (living or dead).
• HIV-containing cell or tissue cultures, organ cultures, and HIV - or HBV-containing culture medium or other solutions as well as blood, organs, or other tissues from experimental animals infected with HIV or HBV.
1Occupationally exposed means exposed during the performance of job duties to blood or other potentially infectious materials through skin, eyes, mucous membranes, or broken skin by needlesticks, human bites, cuts, abrasions, splashes, or other means.
Q.Aretherespecificoccupationscovered by the standard?
A. The hazard of exposure to infectious materials affects employees in many types of jobs. The following occupations are likely to be covered by the standard, but the scope of the standard is not limited to employees in these occupations:
• Physicians, physicians’ assistants, nurses, nurse practitioners, and health-care employees in clinics and physicians’ offices
• Employees of clinical and diagnostic laboratories
• Housekeepers in health-care facilities• Workers in hospital laundries or commercial
laundries that serve health-care or public safety institutions
• Tissue bank personnel• Employees in blood banks and plasma centers
who collect, transport, and test blood
• Employees in freestanding clinics such as hemodialysis clinics, urgent-care clinics, health maintenance organization clinics, and family-planning clinics
• Employees in clinics in industrial, education, and correctional facilities (e.g., those who collect blood and clean and dress wounds)
• Employees assigned to provide emergency first aid
• Dentists, dental hygienists, dental assistants and dental laboratory technicians
• Staff of institutions for the developmentally disabled
• Hospice employees• Home health-care workers• Staff of nursing homes and long-term
care facilities• Employees of funeral homes and mortuaries• HIV and HBV research laboratory and
production facility workers• Employees handling regulated waste• Emergency medical technicians,
paramedics, and other emergency medical service providers
• Firefighters, law enforcement personnel, and correctional officers.
Q. How do employers determine if their employeesareincludedinthescopeof the standard?
A. The standard requires employers to evaluate each job task and procedure to determine which employees may be expected to be occupationally exposed to blood or other potentially infectious materials. The exposure determination is made without regard to the use of personal protective equipment (PPE), because employees are considered to be exposed even if they wear PPE. If it is determined that sufficient evidence of reasonably anticipated exposure exists, the employer will be held responsible for providing the protections of 29 CFR 1910.1030 to the employees with occupational exposure.
3
Q. If I have employees who may rarely come into contact with blood or OPIM,doalloftherulesstillapply?
A. Employers with employees who are not routinely exposed to blood or OPIM may fall under the standard, in which case the hepatitis B vaccination would not need to be offered until an incident involving the presence of blood or OPIM occurs. In order for an employer to qualify under the standard, the following conditions must be met:
• Reporting procedures must be in place under your organization’s exposure control plan to ensure that all incidents involving blood or OPIM are reported before the end of the work shift during which the incident occurred.
• Reports of incidents must include the names of all involved employees; a description of the circumstances of the incident, including the date and time; and a determination of whether an exposure incident, as defined by the standard, has occurred.
• Exposure reports must be included on a list of such incidents, be readily available to all employees, and provided to OSHA upon request.
• The specifics of the reporting procedure must be included in the bloodborne pathogens training.
• All employees who are involved in any situation involving the presence of blood or OPIM, regardless of whether a specific exposure incident occurs, must be offered the full hepatitis B vaccination series as soon as possible, but no later than 24 hours after the incident. If an exposure incident, as defined in 29 CFR1910.1030 occurs, all other post-exposure follow-up procedures in accordance with the standard must be initiated immediately, and the employer must ensure that the medical provider is familiar with and follows the recommendations for post-exposure follow-up set forth by the Centers for Disease Control.
• Bloodborne pathogens training must be provided to all affected employees.
• Appropriate personal protective equipment, clean-up materials, and equipment must be provided.
Q. Are Good Samaritan acts considered anoccupationalexposure?
A. Good Samaritan acts are not covered under the OSHA standard. If an employee has an exposure incident while acting as a Good Samaritan and that employee is not expected to render assistance as part of his or her job duties, the employer is not required by the OSHA standard to provide HBV vaccination series, post-exposure evaluation, follow-up procedures, or any other protections of the OSHA standard. However, if the employee was acting as a Good Samaritan and was injured they may be covered by workers’ compensation insurance on case-by-case bases.
Q.Docleanupactivitiesofblood orOPIMconstituteoccupationalexposure?
A. Yes. Employees who clean up and decontaminate areas or surfaces are considered to have occupational exposure. Such employees are covered under the OSHA standard.
Q.Aremotel/hotelhousekeepersincludedinthescopeoftherules?
A. Employees in the lodging industry are covered under the standard if there is a reasonable expectation that occupational exposures to blood or other potentially infectious material will occur in the performance of their job duties. The standard is a performance standard and requires the employer to determine occupational exposures without regard to personal protective clothing or equipment. Every location may have individual considerations that must be evaluated to determine exposures. If it is determined that the standard applies to the work location, action should be taken to develop an exposure control plan; provide employee training, information, and PPE; offer the hepatitis B vaccination series; and comply with the other provisions of the standard.
4
Q. Are janitorial services covered by the standard?
A. Janitorial, custodial, or maintenance staff employed in non-health-care facilities are not generally considered to have “reasonably anticipated skin, eye, mucous membrane exposures, or parenteral exposure to blood or other potentially infectious materials that may result from the performance of an employee’s duties.” It is the employer’s responsibility to determine which job classifications or specific tasks and procedures involve occupational exposure.
Q. Are chiropractors who may perform invasiveproceduresinvolvingbloodcovered by the standard?
A. Chiropractors with no paid employees and no workers’ compensation coverage would not be covered by the standard. Chiropractors with paid employees not reasonably expected to be exposed to blood or OPIM in the performance of their duties would not come under the standard. If chiropractors themselves, who are covered by workers’ compensation, perform procedures for which there is a reasonable anticipation of exposure to blood or OPIM, they fall under the scope of the standard, as would any of their employees whose job duties placed them at risk.
Q. ABC Healthcare Employment Agency has a large personnel pool providing hospitalstaffingandprivate-dutynursingservices.Theemployees are on ABC’s payroll. Who is responsible, the employment agency or the client?
A. Personnel providers who send employees to work at other facilities are considered employers whose employees may be exposed to hazards. Because ABC maintains a continuing relationship with the employees, but another employer creates and controls the hazards, there is a shared responsibility to comply with the standard. (temporary employee) would be required to provide generic training in universal precautions, ensure that employees are provided with required vaccinations, and ensure that proper follow-up evaluation is provided following any exposure
incident. The client would be responsible for providing site-specific training and PPE and for controlling potential exposure conditions. The client may specify qualifications for personnel, including vaccination status. It is in the best interest of (temporary employee) to ensure that all requirements of the standard are met by the client employer to ensure a safe and healthful workplace for the leased employees.
Q.Aretheconstruction,maritime,andagriculturalindustriescoveredbythe bloodborne pathogen standard?
A. Yes. The bloodborne pathogen standard applies to all employers at worksites where there is reasonably anticipated skin, eye, mucous membrane, or other parenteral contact with blood or OPIM that may result from the performance of an employee’s duties. It is the employer’s responsibility to determine which job classifications or specific tasks and procedures involve occupational exposure.
Q.Aredry-cleaningandlaundromatoperations covered by the standard?
A. OSHA believes that some laundry workers are at risk of exposure to bloodborne pathogens. These individuals may be employed in hospital or commercial laundries that serve health-care, public safety, or other institutions where occupational exposure to blood or OPIM occurs.
Q.Arefirst-aid-trainedemployeescovered by the standard?
A. First-aid-trained employees assigned to provide emergency first aid as part of their specific job duties are covered by the standard. Examples include occupational nurses or employees in charge of first-aid stations. Position descriptions for such employees would stipulate rendering first aid to fellow employees. Any first-aid-trained employee who has rendered first aid should receive treatment under post-exposure evaluation and followup, Section (f)(3). All first-aid-trained employees must have PPE available to them and must be informed about exposure hazards and post-exposure procedures.
5
Q.Canambulancedriversor helicopter pilots eat while transportingapatientorhuman body parts or organs?
A. Ambulance drivers or pilots can eat and drink during transportation of patients, body parts, or organs provided that the cab, compartment, or operator have not been contaminated with blood or other potentially infectious materials. The employer may implement procedures for changing contaminated clothing and washing prior to entering the vehicle and/or ensuring that patients and potentially contaminated material remain behind a separating partition.
Q.Whenisurineorfecescovered as“otherpotentiallyinfectiousmaterial”?
A. When there is visible blood. Nasal secretions and tears that have visible blood are also defined as OPIM.
SECTION IIExposure Control Plans 29 CFR 1910.1030(c)The standard requires the employer to develop a
written exposure-control plan to identify workers with occupational exposure to blood and other potentially infectious material and to specify the methods of protecting and training the employees.
Q.Whatisrequiredintheexposurecontrol plan?
A. At a minimum, the exposure control plan must include:
• The exposure determination.• The procedures for evaluating the
circumstances surrounding an exposure incident.
• The schedule and method for implementing the provisions of the standard. This schedule may be as simple as a calendar with brief notations describing the methods of implementation and an annotated copy of the standard. The plan must be reviewed and updated annually or whenever new tasks and procedures affect employees’ occupational exposure. It must be made accessible to employees in accordance with CFR 29 1910.30(c).
Q.DoesDWChaveasampleexposurecontrol plan?
A. Yes. Refer to Appendix B.
Exposure determination 29 CFR 1910.1030(C)As an element of the exposure control plan, every
employer must identify workers with occupational exposure to blood and other potentially infectious materials.
Q.HowdoIknowifanyofmyemployeeshaveoccupationalexposures?
A. Exposure determination must be based on the definition of occupational exposure without regard to personal protective clothing and equipment. Exposure determination is made by reviewing job classifications within the work environment and sorting exposures into two groups:
• The first group includes job classifications in which all of the employees have occupational exposure, such as operating room scrub nurses. Within this group, it is not necessary to list specific work tasks.
• The second group includes job classifications in which some of the employees have occupational exposure. In this group, specific tasks and procedures causing occupational exposure must be listed. An example would be hospital laundry workers if some workers were assigned the task of handling contaminated laundry.
• Once employees with occupational exposure have been identified, communicate the hazards to these employees.
Q. Do clinical or diagnostic laboratories that analyze blood or otherpotentiallyinfectiousmaterials have to comply with this section of therules?
A. Yes, but they are exempt from Section (e), which covers HIV and HBV research laboratories and production facilities. OSHA recommends that universal precaution procedures are followed in clinical or diagnostic laboratories.
6
Training29 CFR 1910.1030(G)Each occupationally exposed employee must be
given bloodborne-pathogen information and training at the time of initial assignment. The training must be conducted during working hours and at no cost to the employee. Training must be repeated at least once a year - more often if new or modified tasks involve occupational exposure to bloodborne pathogens that affect employees.
Q.Whoisqualifiedtoconducttrainingand provide information?
A. Possible trainers include a variety of health-care professionals such as infection control practitioners, nurse practitioners, physicians’ assistants, and emergency medical technicians. Non-health-care professionals such as industrial hygienists, epidemiologists, or professional trainers may conduct the training if they can demonstrate knowledge and training in the area of bloodborne pathogens. Trainers must provide information appropriate to the educational level, literacy, and language of the audience; the information must contain the following elements:
• Explanation of the regulatory text and how to get a copy of the regulatory text
• Information on the epidemiology and symptoms of bloodborne diseases
• How bloodborne pathogens are transmitted• Explanation of the exposure-control plan and
how to get a copy of it• How to recognize tasks that might result in
occupational exposure• Explanation of the use and limitations of work
practices, engineering controls, and PPE• Information on the types, selection, proper use,
location, removal, handling, decontamination, and disposal of PPE
• Information about the hepatitis B vaccination series: its safety, benefits, methods of administration, and availability
• Who to contact and what to do in an emergency
• How to report an exposure incident and conduct the post-exposure evaluation and follow-up
• Information about warning labels, signs, and color-coding
• Question-and-answer session on any aspect of the training
• Additional training in standard microbiological practices and techniques, practices and operations specific to the facility, and the proper handling of human pathogens or tissue cultures is required for employees who work in HIV and HBV laboratories and production facilities.
• Employees must receive additional training before beginning initial work assignments.
Q. Can generic training programs, “outside”trainers,orvideos/DVDs beused?
A. Yes, as long as “site specific” information and employee interaction with the trainer is also provided. OSHA evaluates training based on employee knowledge or performance. Audiovisual programs on bloodborne pathogens are available from the: TDI/DWC, Resource Center, phone number: (512) 804-4620 or select “Safety and Resources” from the Web site, www.TDI/DWC.state.tx.us.
Q.WillTDI/DWCprovidetrainingtoourouremployees?
A. Yes. TDI/DWC can conduct Bloodborne Pathogen training at your site for a minimal cost. Please call the Safety Training Team Leader at (512) 804-4626 for additional information.
Q.WillTDI/DWCreviewandapproveourexposure-controlplan,training,PPE,orotherproducts?
A. If your company does business in the state of Texas; is in private industry; and has less than 250 employees at the consultation site and no more than 500 employees at all sites controlled by the employer (limited assistance may be available for larger employers) you may receive assistance from Occupational Safety & Health
7
Q.WillTDI/DWCreviewandapproveourexposure-controlplan,training,PPE,orotherproducts?(cont.)
A (cont.) Consultation (OSHCON) Service. Employers can request OSHCON service information by calling toll-free 1-800-687-7080 or you can email OSHCON at: oshcon@TDI/DWC.state.tx.us.
SECTION IIIPreventive Measures Hepatitis B Vaccination 29 CFR 1910.1030(f)The requirements for hepatitis B vaccinations are
designed to protect employees from bloodborne pathogens caused infection by requiring employers to provide hepatitis B vaccinations and medical follow-up after an exposure incident. Early intervention, testing, counseling, and appropriate prophylaxis can reduce the risk of infection and prevent further transmission.
Q.Whoisrequiredtohave HBV vaccinations?
A. Employers must make the hepatitis B vaccination series available to all employees who have occupation exposure. They must also provide post-exposure evaluation and follow-up to all employees who experience an exposure incident. The vaccinations and all medical evaluations and follow-up must be provided at no cost to the employee, provided at a reasonable time and place, and performed by or under the supervision of a licensed physician or other licensed health-care professional. Vaccinations must be administered according to current recommendations of the U.S. Public Health Service. Employees who decline the vaccination must sign a declination form. (See Appendix A) Employees who request the vaccination series later must receive it at no cost if they continue to be exposed.
Q.WhenmusttheHBVvaccination be offered?
A. The hepatitis B vaccination series must be offered to employees who have occupational exposure to blood or other potentially infectious materials within 10 working days of initial assignment, unless the employee has previously received the series; antibody testing reveals that the employee
is immune; or, for medical reasons, the employee cannot be vaccinated. Employers are not required to provide medical pre-screening, and employees are not required to submit to pre-screening. The employer must obtain and provide the employee either a copy of the health-care professional’s written opinion stating whether a hepatitis B vaccination was indicated for the employee and whether the employee received such vaccination. Any booster doses of the hepatitis B vaccine recommended by U.S. Public Health Service also must be provided at the employer’s expense.
Q.Whatifanemployeerefuses to be vaccinated?
A. The standard requires the employer to obtain a signed declination from each employee who refuses vaccination. The declination statement used by the employer must contain the language found in Appendix A, no words may be added or subtracted. A sentence releasing the employer from liability may not be added.
Q. If an employee who wants an HBV vaccine believes he or she is allergic to the vaccine, is the employer requiredtopayforallergyteststodetermine if the employee can safely receive the vaccination?
A. It is the employer’s responsibility to bear the cost of allergy tests recommended by the physician.
Q.Ispre-screeningrequiredforhepatitisBserum?
A. No. The standard does not require pre-screening of employees for hepatitis B; neither is pre-screening prohibited. Pre-screening for immunity cannot be used in lieu of offering hepatitis B vaccination.
Q. If an employee begins the vaccination series and terminates employment before the series is complete, can he or she be charged for the remaining vaccine?
A. No. Section (f)(ii)(A) of the standard requires the employer to offer hepatitis B vaccination at no cost to the employee.
8
Q. Do my employees need to have a test for hepatitis B antibodies after they complete the vaccination series?
A. The most current CDC guideline regarding hepatitis B recommends that employees who have ongoing contact with patients or blood and are at ongoing risk for injuries with sharp instruments or needle sticks be tested for antibody to hepatitis B surface antigen one to two months after the completion of the three dose vaccination series. Employees who do not respond to the primary vaccination series must be re-vaccinated with a second three dose vaccine series and retested. A physician must evaluate employees who do not respond to the second vaccine series.
Universal precautions 29 CFR 1910.1030(c)Universal precautions must be observed. This
method of infection control requires the employer and employee to assume that all human blood and specified human body fluids are infectious for HIV, HBV, and other bloodborne pathogens. Where differentiation between types of body fluids is difficult or impossible, all body fluids are to be considered potentially infectious.
Standardprecautionsandbodysubstanceisolation
Alternative concepts in infection control are called body substance isolation (BSI) and standard precautions. These methods define blood and all body fluids (whether or not they contain blood) and mucous membranes as infectious. This method incorporates not only the fluids and materials covered by this standard but expands coverage to include all body fluids and substances. These concepts are acceptable alternatives to universal precautions, provided that facilities utilizing them adhere to all other provisions of the Bloodborne Pathogens standard.
SECTION IVMethods of ControlEngineering controls and work practices 29 CFR 1910.1030Engineering controls and work practices are the
primary methods used to prevent occupational transmission of HBV, HCV, HIV, and other
bloodborne pathogens. Personal protective clothing and equipment also are necessary when occupational exposure to bloodborne pathogens remains even after instituting these controls.Engineering controls reduce employee exposure
in the workplace by either removing or isolating the hazard or isolating the worker from exposure. Self-sheathing needles, needle systems, puncture resistant disposal containers for contaminated sharp instruments, resuscitation bags, and ventilation devices are examples of engineering controls. Engineering controls must be examined and maintained or replaced on a schedule.29 CFR 1910.10.30 also requires that every employer
with employees who use medical sharps in direct patient care must identify, evaluate, and select engineering and work-practice controls, including safer medical devices, at least annually.Evaluation of safer medical devices must involve
non-managerial front-line employees responsible for direct patient care and must be done on a facility-by-facility basis. When a facility has multiple departments with specific equipment or work practice concerns, evaluations must involve employees from those departments.Emergency departments should coordinate
appropriate medical-device selections with the emergency medical services from which they receive patients. Example of a case in which it would be useful to coordinate: an ambulance service using a needleless system not compatible with the needleless system used by personnel at a hospital can increase employee exposure potential.After a device is evaluated and selected, the
employer must decide whether or not to use that device. If a device is not purchased because of employer or employee concerns, those concerns must be documented. However, if the employer does not purchase a device that had employee support, the employer must document the employee support as well as the justification for not purchasing that device.If a device is purchased without the consent of the
employees who evaluated it, the employer must document the employees’ concerns as well as the employer’s justification for purchasing that device.Required documentation must be kept as part of the
written exposure control plan.
9
The employer must ensure that all affected employees are informed on the process for selecting safer medical devices. All employees must be trained in the use of safer medical devices before the employees use those devices.Proper work practices alter the manner in which a
task is performed. In work areas where a reasonable likelihood of occupational exposure exists, work practice controls include restricting eating, drinking, smoking, applying cosmetics or lip balm, and handling contact lenses; prohibiting mouth pipetting; preventing the storage of food and/or drink in refrigerators or other locations where blood or OPIM are kept; providing and requiring the use of hand washing facilities; and routinely checking equipment and decontaminating it prior to servicing and shipping.Washing hands when gloves are removed and as
soon as possible after skin contact with blood or other potentially infectious materials is required.The standard prohibits recapping, removing, or
bending needles unless the employer can demonstrate that no alternative is feasible or that such action is required by a specific medical procedure. When recapping, bending, or removing contaminated needles is required by a medical procedure, it must be done using a one-handed technique or by mechanical means such as the use of forceps.The standard also prohibits shearing or breaking
contaminated needles.
Q.Arecontaminatedsharpsdefined?
A. Yes. The rule defines contaminated sharps as any contaminated object that can penetrate the skin, including - but not limited to - needles, scalpels, broken glass, broken capillary tubes, and exposed ends of dental wire.
Q.WhatmustIdowithcontaminateddisposable sharps?
A. Sharps must be placed immediately (or as soon as feasible after use) in a puncture resistant, leak-proof sharps container that can be closed for handling, storage, transportation, and disposal. The container must be red and may be labeled with the “biohazard” symbol.
Q. Where are sharps containersrequired?
A. Sharps containers are considered an engineering control and must be located where sharps are used. Containers should be located in each room where sharps are used; however, containers may be placed on a tray and transported to each room for use. Disposable and reusable sharps such as large-bore needles, scalpels, and saws must be contained in a manner that eliminates or minimizes the hazard until they are disposed of or reprocessed.
Q. If I’ve never had an employee experienceaneedlestick,doIstillneedtousesaferdevices?
A Yes. OSHA standards are designed to prevent occupational injuries and illnesses. In order to most effectively avoid percutaneous injuries from contaminated sharps, employees must use engineering controls that include safer medical devices.
Q. By what date do we have to implement safer medical devices?
A. The requirement to implement safer medical devices is not new. However, the revised standard clarifies, “engineering controls” described in the original 1991 bloodborne pathogens standard by adding language to the definition section of the standard that reflects the development and availability of safer medical devices. The 1991 standard states: “engineering and work practice controls shall be used to eliminate or minimize employee exposure.” The revision defines engineering controls as “controls (e.g., sharps disposal containers, self-sheathing needles, safer medical devices, such as sharps with engineered sharps injury protections and needleless systems) that isolate or remove the bloodborne pathogens hazards from the workplace.” If you have not already evaluated and implemented appropriate and available engineering controls, you must do so now. Also, employees with occupational exposure to blood and/or OPIM must be trained regarding the proper use of all engineering and work controls.
10
Q. What if a safer option is not available forthemedicaldevicethatIuse?
A. A key element in choosing a safer medical device, other than its effectiveness and appropriateness to the procedure, is its availability on the market. If there is no safer medical device available, you are not required to use something other than the device normally used. During your annual review of devices, you must investigate new and safer options and document this fact in your written exposure control plan. If no engineering control is available, work-practice controls must be used and, if occupational exposure still remains, personal protective equipment must also be used.
Q. Is recapping needles permissible?
A. Recapping, bending, or removing needles is permissible only if there is no feasible alternative or if required for a specific medical procedure such as blood gas analysis. If recapping, bending, or removal is necessary, workers must use a mechanical device or a one-handed technique. If recapping is essential - for example, between multiple injections for the same patient - employees must avoid using both hands to recap. Recapping, using the needle itself to pick up the cap, can be done using a one-handed “scoop” technique, pushing the cap and sharp together against a hard surface to ensure a tight fit. An alternative is to hold the cap with tongs or forceps to place it on the needle.
Q. Is hand washing addressed intherules?
A. Yes. The rule requires employers to provide readily accessible hand-washing facilities, where employees are required to wash their hands immediately or as soon as feasible after removal of gloves or other PPE. Any portion of an employee’s body that has contacted blood or other potentially infectious materials, including saliva, must be washed immediately or as soon as feasible after contact. When hand-washing facilities are not feasible, such as in an ambulance, an antiseptic hand cleanser and clean towels are acceptable or the employer must provide antiseptic towelettes. The hands must be washed with soap and running water as soon as feasible after reaching hand-washing facilities.
Alternate hand-washing procedures for health-care workers can be found in the Centers for Disease Control and Prevention’s Guidelines for Hand Hygiene in Health-Care Settings.
29 CFR 1910.1030(3) Personal protective equipment (PPE)PPE must be used if engineering and work practice
controls do not eliminate the exposure hazard or if such controls are not feasible.PPE helps prevent occupational exposure to
infectious materials. Such equipment includes gloves, gowns, laboratory coats, face shields or masks, and eye protection. PPE is considered appropriate only if it prevents blood or OPIM from passing through or reaching the employee’s work clothes, street clothes, undergarments, skin, eyes, mouth, or other mucous membranes under normal conditions of use.Under the standard, employers must provide, make
accessible, and require the use of PPE at no cost to employees. PPE must be provided in appropriate sizes. Hypoallergenic gloves or similar alternatives must be made available to employees who have an allergic sensitivity to gloves. Employers must ensure that protective equipment is properly used, cleaned, laundered, repaired, or replaced, as needed.An employee may temporarily and briefly
decline to wear PPE under extraordinary (usually, life threatening) circumstances and when, in the employee’s professional judgment, it prevents the delivery of health-care or public-safety services or poses an increased hazard to workers. In general, appropriate PPE is expected to be used whenever occupational exposure may occur.The employer also must ensure that employees
observe the following precautions for safely handling and using PPE:
• Remove protective equipment when it becomes contaminated and before leaving the work area.
• Place used protective equipment in appropriately designated areas or containers for storage, washing, decontamination, or discarding.
• Wear appropriate gloves when there is a reasonable hazard of contact with blood or other potentially infectious materials, when performing vascular access procedures, and when handling or touching contaminated items or surfaces.
11
29 CFR 1910.1030(3) Personal protective equipment (PPE) (cont.)
• Replace gloves if torn, punctured, contaminated, or if they no longer function as a barrier for other reasons
• Only decontaminate utility gloves for reuse if their integrity is not compromised. Discard utility gloves when they’re punctured, cracked, peeling, torn, or deteriorated.
• Never wash or decontaminate disposable gloves for reuse.
• Wear face and eye protection such as a mask with glasses and solid side-shields or a chin-length face shield whenever splashes, sprays, spatters, or droplets of blood or OPIM may reach the eyes, nose, or mouth.
• Wear protective body coverings such as gowns, aprons, caps, and boots when occupational exposure is anticipated. The type and characteristics will depend upon the task and degree of exposure anticipated.
• Remove garments when they become saturated with blood or OPIM.
Q.Areglovesrequiredwhengivingallergyimmunotherapyinjections?
A. Gloves are not necessary if hand contact with blood or OPIM is not anticipated. If bleeding is anticipated, and the employee is required to clean the site following injection, gloves must be worn. To prevent employee hand contact with blood, the patient can be instructed to apply pressure to the injection site with an alcohol wipe or cotton ball, which the patient would then discard.
Q.AretherestandardsthatdefinesuchPPEtermsasfluid-proof,fluid-resistant, and permeability?
A. No. There are no standards defining the permeability of PPE. Paragraph (d)(3)(i) of the standard states: “Personal protective equipment will be considered ‘appropriate’ only if it does not permit blood or other potentially infectious materials to pass through to or reach the employee’s work clothes, street clothes, undergarments, skin, eyes, mouth, or other mucous membranes under normal conditions of use and for the duration of time which the protective equipment will be used.”
Q.Arelatexglovesacceptableforalltypes of jobs?
A. No. The employer has the responsibility for determining the type of glove required for each job. Vinyl or other leak-proof gloves may be required to withstand heavier work duties.
Q.Istheuseofhandorbarriercreamsacceptablewhenusinglatexgloves?
A. Yes, if the barrier cream does not cause degradation of the gloves, as petroleum-based creams can.
Q.Ifemployeeswearscrubsinworkareaswherethereareexposurestobloodandotherpotentiallyinfectiousmaterials, do they have to remove thescrubstogodownthehalltotherest room?
A. Yes. Removing contaminated scrubs prior to leaving the work area is necessary to prevent contamination of other areas. The term “contaminated” means the presence or the reasonably anticipated presence of blood or other potentially infectious materials.
29 CFR 1910.1030(4) HousekeepingUnder the standard, each place of employment must
be kept clean and sanitary. Employers must develop and implement a cleaning schedule that includes the methods of decontamination and procedures to be used. The cleaning schedule must explain which areas and surfaces are to be cleaned, the type of contamination present, and how they are to be cleaned. Employers must ensure that the following
housekeeping procedures are followed:• Cleaning and decontamination of the
environment, including equipment and work surfaces that have been contaminated with blood or OPIM.
• Decontamination of work surfaces with an appropriate disinfectant after completion of procedures; immediately, if obviously contaminated; after spills of blood or OPIM; and at the end of work shifts.
• Removal and replacing of protective coverings such as plastic wrap and aluminum foil when contaminated.
12
29 CFR 1910.1030(4) Housekeeping(cont.)• Regular inspection and decontamination of
reusable receptacles such as bins, pails, and cans that is likely to become contaminated. When contamination is visible, clean and decontaminate receptacles immediately or as soon as feasible.
• Use of mechanical means such as tongs, forceps, or a brush and a dustpan to pick up contaminated broken glass.
• Storage or processing of reusable sharps in a way that ensures safe handling.
• Placement of other regulated waste in closable, leak-proof, and labeled or color-coded containers for storage, handling, transporting, or shipping. “Other regulated waste” means liquid or semi-liquid blood or OPIM; items contaminated with blood or OPIM that would release these substances in a liquid or semi-liquid state if compressed; items caked with dried blood or OPIM capable of releasing these materials during handling; contaminated sharps; and pathological and microbiological wastes containing blood or OPIM.
• Placement of discarded contaminated sharps in labeled or color-coded containers that are closable, puncture-resistant, and leak-proof on the sides and bottom.
• Provision of sharps containers that is easily accessible to employees and as close as feasible to the area where sharps are used. Sharps containers must be kept upright during use, replaced routinely, closed when moved, and not overfilled. If cracked or punctured, sharps containers must be replaced.
• Prohibiting the manual opening, emptying, or cleaning of reusable sharps containers and other employee exposure to percutaneous injury.
• Handling contaminated laundry as little as possible and using appropriate PPE when handling it.
• Placement of wet contaminated laundry in labeled or color-coded leak-proof containers for transporting and bagging contaminated laundry without sorting or rinsing it in its area of use.
Q.Areemployeesallowedtotakegowns, lab coats, or PPE home to be laundered?
A. No. Section (d)(3)(iv) of the standard places the responsibility on the employer for cleaning, laundering, and disposal of PPE. This procedure is intended to reduce employee exposure to bloodborne pathogens.
Q. If an employee accidentally gets bloodorOPIMonhisorheruniform,is the employer responsible for cleaningthatuniform?
A. Not necessarily. The employer’s responsibility for cleaning items used in the work area is based on the intended function of those items. If a uniform is to function as PPE, then it is the employer’s responsibility to provide, clean, replace, and dispose of the uniform.
Q. Are there special handling requirementsforPPEtobelaundered?
A. Yes. Contaminated laundry, which is laundry that has been soiled with blood or OPIM, must be handled as little as possible and placed promptly into bags or containers in the area where it has been used or worn and removed. The bags or containers must prevent leakage and be red or labeled with the biohazard symbol. If the facility practices universal precautions, alternative labeling or color-coding is acceptable if it permits all employees to recognize the laundry bags or containers as requiring compliance with universal precautions. Protective gloves and other PPE must be worn when handling contaminated laundry.
Q. What disinfectants are acceptable fordecontaminatingsurfaces?
A. Products registered by the EPA as sterilants (List A), disinfectants that are effective against tuberculosis (List B), and disinfectants that are effective against Hepatitis B and HIV (List D). These lists are available from the EPA, (703) 308-0127 and at their Web site, www.epa.gov/oppad001/chemregindex.htm.
A solution of 5.25 percent sodium hypochlorite (household bleach) diluted 1:10 to 1:100 with
13
Q. What disinfectants are acceptable fordecontaminatingsurfaces?(cont.)
A. (cont.) water and prepared daily is acceptable for cleanup of contaminated items or surfaces.
Quaternary ammonia products are appropriate for general housekeeping procedures that do not involve the clean up of contaminated items or surfaces. “Contaminated” is defined as the presence or reasonably anticipated presence of blood or OPIM.
Q.Iscarpetinganacceptablefloorcoveringinmedicalexaminationrooms or other areas that may become contaminated with blood or OPIM?
A. The regulations do not address requirements for floor covering; however, the floor surface or covering must be capable of being cleaned and decontaminated. Some carpet surfaces may be difficult to decontaminate.
Q. Is there a standard reference that I can follow for decontamination procedures?
A. Yes. These procedures are found in the Centers for Disease Control’s (CDC), Guidelines for Hand Hygiene in Health-Care Setting, October 25, 2002/51 (RR16): 1-44. This publication, along with Hand Hygiene Guidelines Fact Sheet can be found on the CDC website www.cdc.gov or by calling (404) 639-3286.
Q.Whatwastesareregulated?
A. Regulated waste:
• Blood in liquid or semi-liquid form, or other potentially infectious materials, including saliva in dental procedures
• Items that would release blood or other potentially infectious materials if compressed
• Contaminated sharps• Pathological and microbiological waste
containing blood or other potentially infectious materials
• Items that are caked with dried blood or other
potentially infectious materials and that have the ability to release these materials while being handled
Q.Arefemininehygieneproductsdefinedasregulatedwaste?
A. OSHA does not generally consider discarded feminine hygiene products used to absorb menstrual flow to be regulated waste. OSHA expects the waste containers in which these products are discarded to be lined in such a way as to protect employees from physical contact with the contents.
Q.Arebandagesandvaginalspeculumsconsideredregulatedwaste?
A. Bandages that are not saturated to the point of releasing blood or OPIM if compressed are not considered regulated wastes. Similarly, vaginal speculums do not meet the criteria for regulated wastes as defined by the standard.
Q. Are there special handling proceduresforregulatedwaste?
A. Yes. Contaminated sharps must be disposed of in approved containers. Other regulated waste must be placed in properly labeled and/or red bags that contain all contents and prevent leakage. The bags or containers must be closed prior to removal. If a bag leaks or becomes contaminated on the outside, it must be placed in a second labeled and/or red bag or container.
Q.Arethererequirementsotherthanthe OSHA bloodborne pathogens standardthatgovernbiohazardousorregulatedwaste?
A. Yes. The rule requires disposal of regulated waste in accordance with state, local, or federal waste disposal standards. The Texas Department of State Health Services (DSHS) regulates storage and collection, the Texas Department of Transportation (TxDOT) regulates transportation, and the Texas Commission on Environmental Quality (TCEQ) regulates disposal of biohazardous wastes.
14
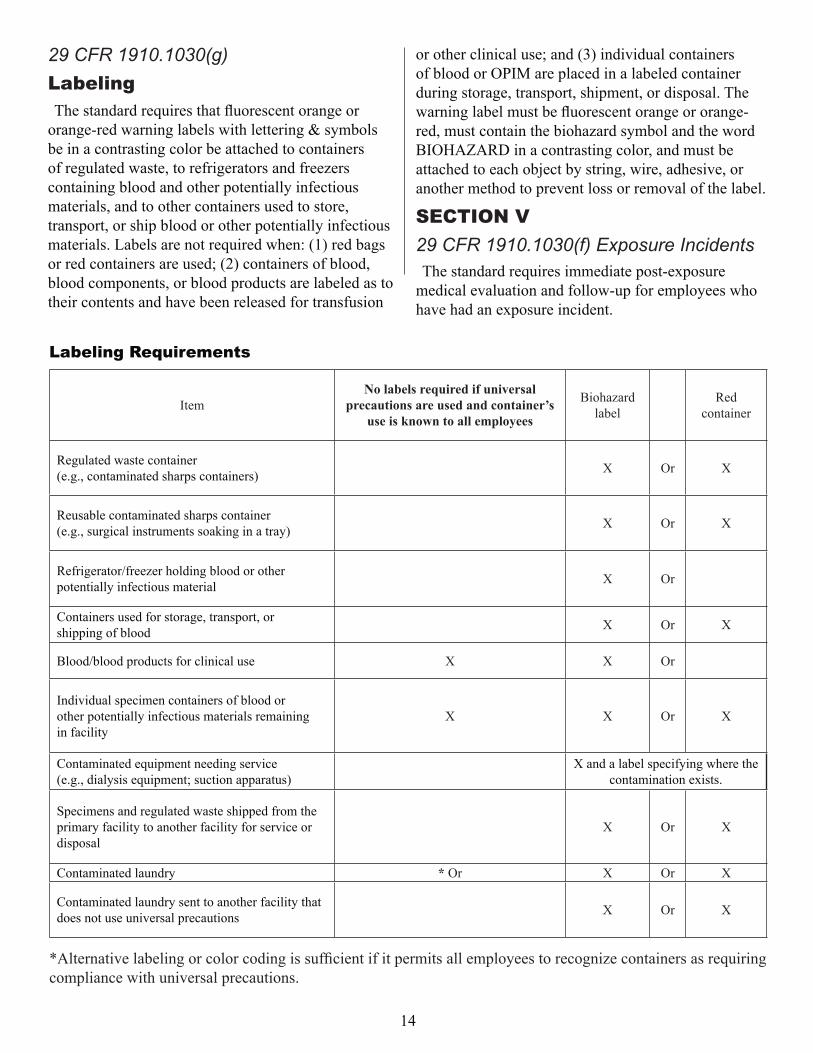
29 CFR 1910.1030(g)LabelingThe standard requires that fluorescent orange or
orange-red warning labels with lettering & symbols be in a contrasting color be attached to containers of regulated waste, to refrigerators and freezers containing blood and other potentially infectious materials, and to other containers used to store, transport, or ship blood or other potentially infectious materials. Labels are not required when: (1) red bags or red containers are used; (2) containers of blood, blood components, or blood products are labeled as to their contents and have been released for transfusion
LabelingRequirements
ItemNo labels required if universal
precautions are used and container’s use is known to all employees
Biohazard label
Red container
Regulated waste container (e.g., contaminated sharps containers) X Or X
Reusable contaminated sharps container (e.g., surgical instruments soaking in a tray) X Or X
Refrigerator/freezer holding blood or other potentially infectious material X Or
Containers used for storage, transport, or shipping of blood X Or X
Blood/blood products for clinical use X X Or
Individual specimen containers of blood or other potentially infectious materials remaining in facility
X X Or X
Contaminated equipment needing service (e.g., dialysis equipment; suction apparatus)
X and a label specifying where the contamination exists.
Specimens and regulated waste shipped from the primary facility to another facility for service or disposal
X Or X
Contaminated laundry * Or X Or X
Contaminated laundry sent to another facility that does not use universal precautions X Or X
*Alternative labeling or color coding is sufficient if it permits all employees to recognize containers as requiring compliance with universal precautions.
or other clinical use; and (3) individual containers of blood or OPIM are placed in a labeled container during storage, transport, shipment, or disposal. The warning label must be fluorescent orange or orange-red, must contain the biohazard symbol and the word BIOHAZARD in a contrasting color, and must be attached to each object by string, wire, adhesive, or another method to prevent loss or removal of the label.
SECTION V29 CFR 1910.1030(f) Exposure IncidentsThe standard requires immediate post-exposure
medical evaluation and follow-up for employees who have had an exposure incident.
15
prophylaxis according to recommendations of the U.S. Public Health Service.
The employer must give the health-care professional responsible for the employee’s hepatitis B vaccination, post-exposure evaluation, and follow-up a copy of the OSHA standard. The employer must provide the following to the health-care professional: A description of the employee’s job duties relevant to the exposure incident, documentation of the route(s) of exposure, circumstances of exposure, results of the source individual’s blood tests, if available, and all relevant employee medical records, including vaccination status.The health-care professional’s written opinion to the
employer for post-exposure evaluation must document that the employee has been informed of the results of the medical evaluation and of any medical conditions resulting from the exposure incident that may require further evaluation or treatment. Other diagnoses pertaining to the employee must remain confidential and not be included in the written report. The employer must provide a copy of this report to the employee within 15 days of the evaluation.The requirements for the medical and training records
are discussed in the next section, “Recordkeeping.”
Q.Iftheemployerisalsothehealth-care professional, how can the employermaintainpost-exposureconfidentiality?
A. The employer is required to maintain required medical records in a way that protects the employee’s identity and test results. If the employer has contracted with a clinic or other health-care facility to provide the follow-up programs, confidentiality requirements must be included in the contract.
SECTION VI29 CFR 1910.1030(1) Record KeepingEmployers must preserve and maintain for each
employee an accurate record of occupational exposure according to the OSHA standards governing access to employee exposure and medical records, 29 CFR-1910.1020.Employers who must maintain an exposure-control plan
must also maintain a log of injuries from contaminated sharps. This log must protect
Q.Whatisanoccupationalexposureincident?
A. It’s an employee’s exposure to or contact with blood or OPIM through broken skin; through the eyes, nose, or mouth; or by means of a wound such as a needlestick.
Q.Whatmustbedoneifanexposureincidentoccurs?
A. An evaluation and follow-up must be done, which must include the following elements:
• Documentation of the route of exposure and how exposure occurred.
• Identification of the source individual, unless the employer can establish that identification is infeasible or prohibited by state or local law.
• Obtain consent from the source individual. If consent is not obtained, the employer must show that legally required consent could not be obtained. Where consent is not required by law, the source individual’s blood, if available, should be tested and the results documented.
• Testing to determine HIV and HBV infectivity as soon as possible after the incident and documentation of the source individual’s blood test results. If the source individual is known to be infected with either HIV or HBV, testing need not be repeated.
• Provision of the source individual’s test results (if consent has been obtained) and information about disclosure and confidentiality laws to the exposed employee.
• Upon consent, testing of the exposed employee’s blood for HBV and HIV serological status as soon as feasible after the exposure incident.
• If the employee consents to baseline blood collection, but does not give consent at that time for HIV serologic testing, the sample shall be preserved for at least 90 days. If, within 90 days of the exposure incident, the employee elects to have the baseline sample tested, such testing shall be done as soon as feasible.
• Provision of HBV and HIV serological testing, counseling, and safe and effective post-exposure

16
another employee, a former employee, or an authorized employee representative has access to the OSHA 300 log. You must keep a separate, confidential list of the case numbers and employee names for your privacy-concern cases so you can update the cases and provide the information to the government if asked to do so.
Q. I own a janitorial company, and we haveanexposure-controlplanbecausewecleanupbloodspills.Myemployeesoccasionallyfindusedsyringes.DoIneedtokeepasharpsinjurylog?
A. Yes. The sharps injury log must be kept by all employers who must maintain an exposure-control plan, regardless of whether or not they use sharps in their normal duties.
Q.Imustalsologinjuriesfromcontaminated sharps on my OSHA 300log.CanIjustusethatasmysharpsinjurylog?
A. Yes, so long as the information required to be kept on the sharps injury log is recorded on the OSHA 300 Log. Additionally, you must be able to easily separate the sharps injury information from all of the other information on the OSHA 300 Log. For example, if you keep your 300 Log electronically in a database, you must be able to pull up a report of the sharps injuries with the required information. If you use the paper version of the OSHA 300 Log, you can comply by using a separate sheet for the sharps injuries.
Q.Howlongmustanemployermaintainmedical records?
A. Medical records must be kept confidential and maintained for at least the duration of employment plus 30 years.
The bloodborne pathogens standard also requires employers to keep accurate training records for three years. They must include training dates, contents or a summary of the training, names and qualifications of the trainer or trainers, and names and job titles of trainees.
Upon request, both medical and training records must be made available to the National Institute
29 CFR 1910.1030(1) Record Keeping (cont.)the confidentiality of the injured employee and must
include the type and brand of the device, the department or work area in which the injury occurred, and how the injury occurred. This log must be maintained for five years.
Q.Whatinformationisrequiredtoberecorded on the employee medical record?
A. Under the bloodborne pathogens standard, medical records must include the following:
• Employee’s name; social security number; hepatitis B vaccination status, including vaccination dates; and any medical records related to the employee’s ability to receive vaccinations.
• Results of examinations, medical testing, and post-exposure evaluation and follow-up procedures.
• A copy of the information provided to the health-care professional and the health-care professional’s written opinion.
Q.WhenisanemployeeexposuretobloodorOPIMrequiredtoberecorded on the OSHA 300 form?
A. All contaminated sharps injuries must be recorded on the OSHA 300 form. All other exposure incidents need only be recorded on the OSHA 300 log when medical treatment is initiated as part of the postexposure evaluation. These incidents are recorded as injuries until or unless the employee is diagnosed with an illness, such as hepatitis or HIV. If this occurs, the OSHA 300 log must be updated to reflect the incident as an illness, and the description of the incident must reflect the new diagnosis.
All of these types of incidents are recorded as privacy-concern cases, in which the name of the employee is kept confidential. If you have a “privacy-concern case,” do not enter the employee’s name on the OSHA 300 log. Instead, enter “privacy case” in the space normally used for the employee’s name. This will protect the privacy of the injured or ill employee when
17
The following statement must be signed by every employee who declines the hepatitis vaccine. The statement can only be signed by the employee after he or she has received training regarding hepatitis B, hepatitis B vaccination, and the method and benefits of vaccination. Employees must be told that the vaccine and vaccination are provided free of charge to the employee. The statement is not a waiver; employees can request and receive the hepatitis B vaccination at a later date if they remain occupationally at risk for hepatitis B.
I understand that due to my occupational exposure to blood or other potentially infectious materials I may be at risk of acquiring hepatitis B virus (HBV) infection. I have been given the opportunity to be vaccinated with hepatitis B vaccine, at no charge to myself. However, I decline hepatitis B vaccination at this time. I understand that by declining this vaccine, I continue to be at risk of acquiring hepatitis B, a serious disease. If in the future I continue to have occupational exposure to blood or other potentially infectious materials and I want to be vaccinated with hepatitis B vaccine, I can receive the vaccination series at no charge to me. Employee Signature Date
AppendixAStatement of Declination
for Occupational Safety and Health (NIOSH), the Occupational Safety & Health Administration (OSHA), the Texas Department of State Health Services (DSHS), and to the Texas Workers Compensation Commission (TDI/DWC). Training records must be available to employees or employee representatives upon request. An employee’s medical records can be obtained by that employee or anyone having that employee’s written consent.
Q.WhatmustIdoifIdecidetoclosemybusiness?
A. If an employer ceases to do business, medical and training records must be transferred to the successive employer. If there is no successive employer, the employer must notify NIOSH, and the U.S. Department of Health and Human Services, for specific directions regarding disposition of the records at least three months prior to ceasing company operations
18
AppendixBBloodborne Pathogens Exposure Control Plan
SAMPLEFacility name: Date of preparation: We, the management staff of (name of organization), are committed to the prevention of incidents or
happenings, which result in employee injury and illness, and to compliance with the OSHA bloodborne pathogens standard, 29 CFR 1910.1030. Through this written exposure control plan, we share assigned responsibility and hereby adopt this exposure control plan as an element of the (name of organization) Safety and Health Program.
A. PurposeThe purposes and goals of this exposure control plan:
1. To eliminate or minimize employee occupational exposure to blood or other potentially infectious materials (OPIM).
2. To identify employees occupationally exposed to blood in the performance of their regular job duties.3. To provide employees exposed to blood and OPIM information and training. A copy of this
plan is available to all employees at (location).4. To comply with OSHA bloodborne pathogen standard, 29 CFR 1910.1030.B. Exposure determination (Name of organization) has performed an exposure determination for all common job classifications
that may be expected to incur occupational exposures to blood or other potentially infectious materials. This exposure determination is made without regard to use of personal protective equipment (PPE). The following job classifications may be expected to incur occupational exposures to blood or other potentially infectious materials:
(List job classifications meeting the requirements in section (c)(2)).
The following is a list of job classifications in which some employees may have occupational exposures to blood or OPIM:
Job classification Task or procedure_______________________________ _____________________________________________________________ _____________________________________________________________ ______________________________
C. Compliance methods1. Universal precautions
This organization embraces “universal precautions,” which is a method of infection control that requires the employer and employee to assume that all human blood and specified human body fluids are infected with bloodborne pathogens. Where it’s difficult or impossible to identify body fluids, all are to be considered potentially infectious.The following engineering and work practice controls will be used by all employees to eliminate or minimize
occupational exposures at this facility:
19
EngineeringandWork PracticesControls(terms)
Sharps containersPlace contaminated needles, blood-contaminated
test tubes, and other sharp objects in a sharps container. Replace containers routinely and do not allow overfilling. Place reusable sharps in metal trays for decontamination. When moving containers of contaminated sharps from the area of use, close containers to prevent spillage or protrusion of contents.
Safe medical devicesPurchase and use safe medical devices whenever
possible. Evaluate devices annually to determine appropriateness of the device and to investigate new and safer options.
WorkpracticesClean-up blood spills or body fluids as soon as
possible. Use disposable absorptive materials, such as paper towels or gauze pads to soak up the fluids. Clean the area with chemical germicides or a 1:10 solution of liquid bleach. Place absorptive towels, pads, and other material used to mop up spills in plastic bags or designated, labeled containers and treat as biohazardous waste.Employees must wash their hands upon removal of
gloves and other protective gear. In an emergency, if soap and water are not immediately available, use disposable antiseptic towelettes or germicidal gel to clean hands after removing gloves.Employee must wash their hands with soap and water
as soon as possible.Employees may not eat, drink, smoke, apply
cosmetics or lip balm, or handle contact lenses where occupational exposure can occur. Do not store food or beverages in refrigerators and freezers and other sites used to store blood or other biohazardous material.Place biohazard labels on refrigerators or freezers used to store biohazardous material.
Personalprotectiveequipment(PPE)PPE is provided at no cost to employees. Employees
receive training in its use, maintenance, and disposal annually.
Storage areaThe first-aid kits are located in the following locations: In case of emergency, take the necessary first-aid kit and supplies, including PPE, to the location of the injured person. Supplies should include disposable gloves; face shields; resuscitation devices; large, heavy-duty plastic bags and ties; biohazard signs or labels; antiseptic towelettes; disposal absorptive material for cleaning up spilled blood; gloves; and bleach solutions or germicides.
PPEuseanddisposalEmployees engaging in activities that may involve
direct contact with blood, OPIM, contaminated objects, mucous membranes or open wounds must wear disposal gloves made of vinyl or latex. Use reusable rubber gloves (inspected and free of apparent defects) or disposable gloves to clean up spill areas. Disinfect reusable gloves with diluted liquid bleach or germicides after use.Wear face shields or goggles with disposable surgical
masks whenever splashes, spray, spatters of blood droplets or OPIM may be generated and eye, nose, or mouth contamination can be reasonably anticipated.Use laboratory coats or scrubs at the first-aid center
to prevent contamination of employee street clothing.Use resuscitation devices, which minimize contact
with mucous membranes, to perform cardiopulmonary resuscitation. Remove used personal protective equipment at the exposure location or as soon as feasible to avoid contamination of other work area.Place in a biohazard container or in a plastic bag with
a biohazard label. PPE must not be taken from the work site.
HousekeepingMaintain the first-aid kit in a clean and sanitary
condition. Employees who have received bloodborne pathogen training and who have been included under the exposure plan can clean up spills and work surfaces such as bench tops and blood processing areas. Clean and decontaminate all equipment and working surfaces after completion of procedures in blood processing areas.Immediately, or as soon as feasibly possible, clean
and decontaminate all equipment and working
20
Housekeeping(cont.)surfaces after completion of procedures in which
blood or body fluids contaminated with blood are handled. Clean and decontaminate the area at the end of the work shift if the surface has been contaminated since the last cleaning. Inspect all biohazardous waste receptacles and decontaminate weekly or immediately upon visible contamination.Use chemical germicides or solutions of 5.25%
sodium hyprochlorite (liquid bleach) diluted 1:10 with water for cleaning. Chemical germicides approved for use as hospital disinfectants and effective against HIV can also be used. Broken glassware or glass items must not be picked up directly with the hands. Use a mechanical means, such as a brush and dustpan, tongs, or forceps. Handle as a biohazardous waste. Decontaminate equipment used to pick up glassware with a 1:10 bleach solution or an approved germicide.
ContaminatedlaundryHandle non-disposal linen, such as laboratory coats
or scrubs, or any other clothing, visibly contaminated with blood, using disposal gloves. Minimize the time spent handling laundry by keeping as close as possible to the location where it was used. Place laundry in a bag that prevents soak-through and/or leakage of fluids to the exterior; place a biohazard label on the top of the bag.Employees are not to take contaminated items home
to launder. holds the contract to pick up, clean, and return laundered items. The laundry facility has a bloodborne pathogen program in place.
Regulatedwaste___________________________, has been
contracted to pick up regulated waste for disposal. Place regulated waste in containers that are closable, constructed to contain all contents, and prevent leakage, appropriately labeled or color-coded, and closed prior to removal to prevent spillage or protrusion of contents during handling.
Labels and signsAffix warning labels to laundry bags, containers of
regulated waste, refrigerator units and containers used to store, transport, or ship blood or OPIM. Red bags or red containers can be used instead of labels.
Hepatitis B vaccineThe hepatitis B vaccine is offered, at no cost, to
exposed employees within 10 working days of initial assignment. Employees who have potential exposure to bloodborne pathogens but decline to take the vaccination must sign a declination statement. Employees who initially decline can still receive the vaccination should they decide at a later date to accept. Previously vaccinated new hires must provide a vaccination record that includes the vaccination dates. Employees must sign a declination statement if the vaccination record is not available and revaccination is declined or not appropriate. We will coordinate with the _______________________________ to administer the vaccination and retain employee medical record files.
Exposureincidentandpost-exposureevaluationandfollow-up
An exposure incident to bloodborne pathogens is defined as an eye, mouth, or other mucous membrane, non-intact skin, or parenteral contact with blood or other potentially infectious materials that results from the performance of an employee’s duties. It is our policy to include Good Samaritan acts performed by an employee at the work site. Whenever an exposure occurs, wash the contaminated skin immediately with soap and water. Immediately flush contaminated eyes or mucous membranes with copious amounts of water.Medically evaluate exposed employees as soon as
possible after the exposure incident, if recommended, post-exposure prophylaxis can be initiated promptly.The medical evaluation is to include the route(s) of
exposure and the exposure incident circumstances; identification and documentation of the source individual, where feasible; exposed employee blood collection and testing of blood for HBV and HIV serological status, post-exposure prophylaxis, where indicated; counseling; and evaluation of reported illnesses. Source test results and identity will be disclosed to the exposed employee according to applicable state and federal laws and regulations concerning disclosure and confidentially.The provides
hepatitis B vaccinations and medical evaluations and post-exposure follow-up after an exposure incident.
21
Training and training recordsAll employees who have occupational exposure
to bloodborne pathogens receive training on the epidemiology symptoms, and mode of transmission of bloodborne-pathogen disease. In addition, the training program will include the following topics:
• An explanation of activities and tasks that may involve exposure to blood and OPIM.
• How appropriate engineering controls, work practices, and PPE will prevent or reduce exposure.
• The basis for the selection of PPE, the types, use, location, removal, handling, decontamination, and disposal procedures.
• Hepatitis B vaccine information including that the vaccine is provided at no cost; the benefits of being vaccinated, and methods of administration.
• Employer responsibilities for post-exposure evaluation and medical follow-up. How and who to contact should an exposure incident occur.
• An explanation of the signs and hazard labels.• How to review or obtain a copy of the
exposure-control plan and the OSHA standard.Employee training occurs prior to initial assignment
to tasks in which occupational exposure may occur. Training is repeated every 12 months or sooner when there are new tasks or changes to the existing procedures/tasks. Training records are maintained for three years and include the date(s) and content of the training program, name and qualifications of the trainer(s), and names and job titles of the attendees.
RecordkeepingMedical records for employees with occupational
exposure to bloodborne pathogens include the employee’s name, Social Security number, and hepatitis B vaccination status, including dates of hepatitis B vaccination and any medical records relative to the employee’s ability to receive the vaccination. Medical records are kept for the duration of employment plus 30 years in accordance with OSHA standard, 1910-1020. Medical records are confidential and are located in the office. In the event of an exposure incident, the
following records will be kept in the employee’s medical file:
• The results of any examination, medical testing, and follow-up procedures.
• A copy of the testing physician’s written opinion to the employer.
• A copy of all information provided by the employer to the health-care professional regarding the exposure incident.
Record any needle stick, mucous membrane, or skin contact with blood or body fluids contaminated with blood or OPIM requiring medical treatment (i.e. gamma globulin, hepatitis B vaccine, etc.) in the OSHA 300 log. In addition, record any contaminated sharp injuries, including needle sticks on the sharps injury log. These records are retained for five years.
PlanevaluationandreviewReview of the exposure-control plan and update will
occur annually and whenever necessary to reflect new or modified tasks and procedures that affect occupational exposure. The is responsible for the annual review.Name: Signature: Date: The following is an example of a Sharps Injury Log
form“Occupationally exposed” means exposed during the
performance of job duties to blood or OPIM through skin, eyes, mucous membranes, or broken skin by needle sticks, human bites, cuts, abrasions, splashes, or other means
22
Establishment/facility name:
Example of Sharps Injury Log; Date , 20
DateCase
report no.
Type of device(e.g., syringe, suture needle)
Brand name of device
Work area where injury occurred(e.g.. Geriatrics, Lab)
Brief description of how the incident occurred (i.e., procedure being done, action being performed, [disposal injection, etc.]
body part injured)
29 CFR 1910.1030, OSHA’s Bloodborne Pathogens Standard, in paragraph (h)(5), requires an employer to establish and maintain a sharps injury log for recording all percutaneous injuries in a facility occurring from contaminated sharps. The purpose of the log is to aid in the evaluation of devices being used in health-care and other facilities and to identify devices or procedures requiring attention or review. The employer must retain this log and the injury-and-illness log required by 29 CFR 1904. The sharps injury log should include all sharps injuries occurring in a calendar year. The log must be retained for five years following the end of the year to which it relates. The log must be kept in a manner that preserves the confidentiality of affected employees.
This publication was developed with information from the Department of Consumer and Business Services, Oregon Occupational Safety and Health Division and the Texas Department of Insurance, Division of Workers’ Compensation is considered factual at the time of development.
Remember to practice safety, don’t learn it by accident.
ExampleofSharpsInjuryLog