bobic vladimir - stem cells & orthobiologics - chester nuffield seminar 060517
TRANSCRIPT

Knee OrthoBiologics New developments which may delay or avoid more
invasive surgical treatments? The future of orthopaedics? Basically, less carpentry, more biology?
Prof. Vladimir Bobić, MD FRCS Ed Chester Knee Clinic www.kneeclinic.info [email protected] @ChesterKnee
Nuffield Health, The Grosvenor Hospital Chester Seminars St. David’s Park Hotel, Ewloe, 6th May 2017

Osteochondral Repair and OA: Surgical Options
ACI BioPoly
UKR & TKR
OATS
Microfracture
Chondroplasty

Less (orthopaedic) carpentry - more biology?


• Mainly because we still do not seem to understand complex biological and mechanical interaction of articulating surface and subchondral bone.
• This is probably the reason why all mainstream cartilage repair technologies suffer from two major problems:
• insufficient peripheral chondral integration (biomechanical problem?) • insufficient longitudinal subchondral integration (nutritional and biomechanical problem?).
• We may have to accept that this is as good as it gets, at this point in time.
• However, finding a biological solution for cartilage regeneration is one of the fastest growing areas of research and development in orthopaedics and regenerative medicine in general.
So, Why is Cartilage Repair Still a Problem?

Biotechnologies - Stem Cell Technologies already here and as important as Artificial Intelligence, Robotics, Micro and Nano satellites, Biofuels, Additive
manufacturing…
1st Orthopaedic Stem Cell Seminar in the UK:
Guest Speaker:
Dr Fabio Valerio Sciarretta
Head of Department of Orthopeadic Surgery at Mercede Clinic, Rome, Italy.
A specialist knee surgeon and arthroscopist, whose special interests are articular cartilage repair in the knee and the ankle, ligament reconstruction, meniscal repair/transplantation and minimally-invasive knee replacement.
Dr Sciarretta is a member of numerous national and international orthopaedic associations, the editor of Italian editions of numerous american and international textbooks and has published over 50 articles.
www.fabiosciarretta.it


Regenerative Medicine - Stem Cell Technologies





What are Mesenchymal Stem Cells?
• Adult stem cells can help regenerate many tissues
• The best source is the autologous tissue
• Many different tissues can be used to process biologically powerful stem cells
• It seems that the best tissue to extract MSC is SVF (stromal vascular fraction) adipose tissue, which is the best source of cells and regenerative factors

Cell Senescence Exists but ...





Stem Cells No Better Than Placebo … So Far (Editor of Arthroscopy Journal re JBJSA September 2016 Article)



“The first great advancement in sports medicine was the arthroscope, the second is going to be this (stem cells).” James Andrews, MD, “The Athlete’s Surgeon”, Birmingham, Alabama, USA


OJSM 2017


From Chondral Damage to Advanced OA
... to Advanced Medial OA?From Small MFC Chondral Lesion ...

OsteoArthritis or OsteoArthrosis? or just wear and tear?

JBJSA March 1974

The Subchondral Unit: A New Frontier
re-drawn from Imhof et al. 1999
Henning Madry, Saarland University, Homburg/Saar, Germany
Imhof H, Breitenseher M, Kainberger F, Rand T, Trattnig S. (1999): Importance of subchondral bone to articular cartilage in health and disease. Top Magn Reson Imaging 10:180–192
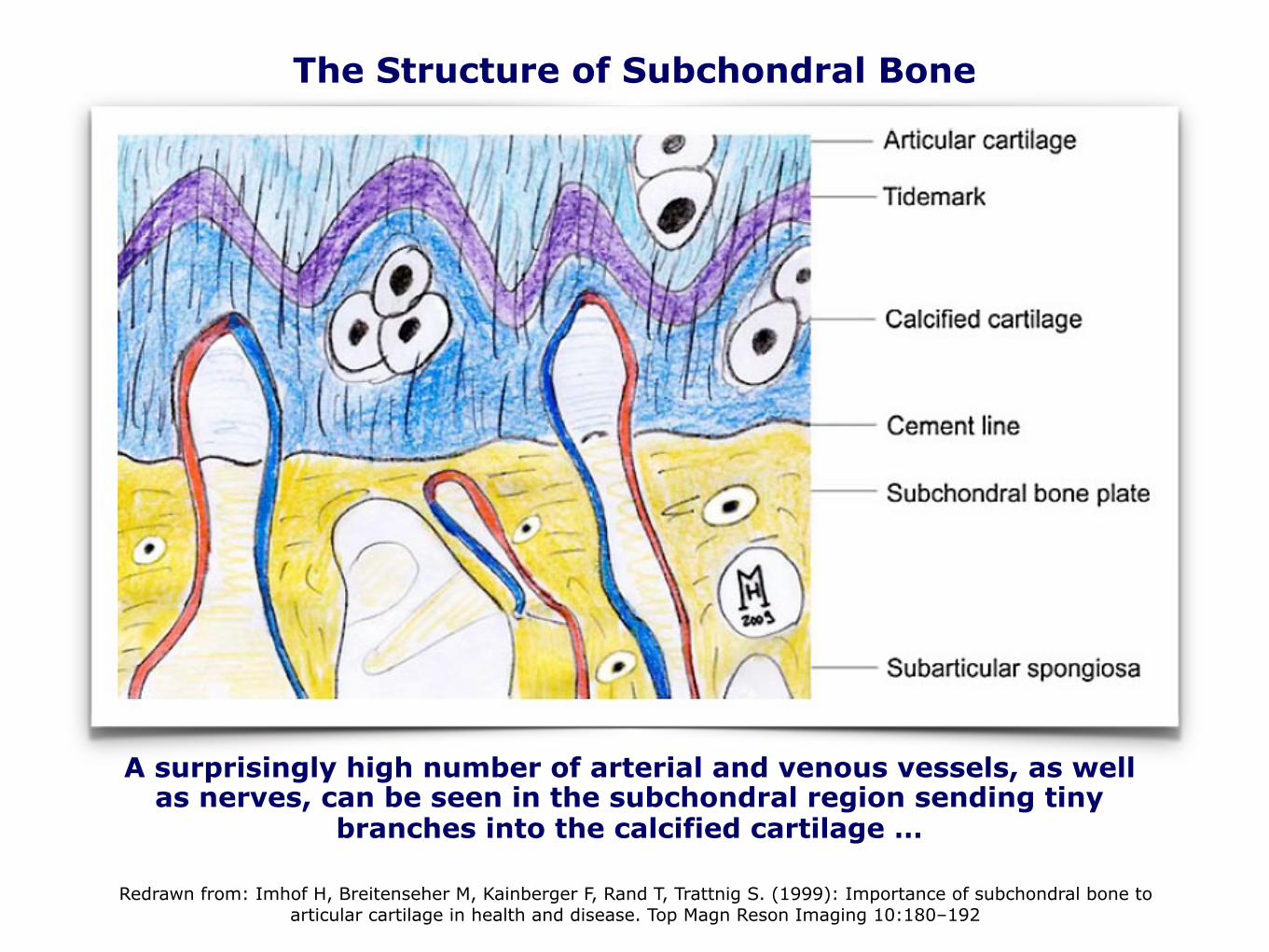
The Structure of Subchondral Bone
Redrawn from: Imhof H, Breitenseher M, Kainberger F, Rand T, Trattnig S. (1999): Importance of subchondral bone to articular cartilage in health and disease. Top Magn Reson Imaging 10:180–192
A surprisingly high number of arterial and venous vessels, as well as nerves, can be seen in the subchondral region sending tiny
branches into the calcified cartilage …

The Structure of Subchondral Bone
• This is extremely important for cartilage repair: the tidemark is crossed by collagen fibrils extending from the articular cartilage into the calcified cartilage, while no collagen fibrils connect the calcified cartilage to the subchondral bone plate.
• Blood vessels from the subchondral region can extend into the overlying calcified cartilage through canals in the subchondral bone plate.
• Therefore, nutrients can reach chondrocytes in the calcified zone via these perforations.
• Unsurprisingly, the perforations are grouped together in the regions of subchondral plate where the stress is greatest.
CKC UK
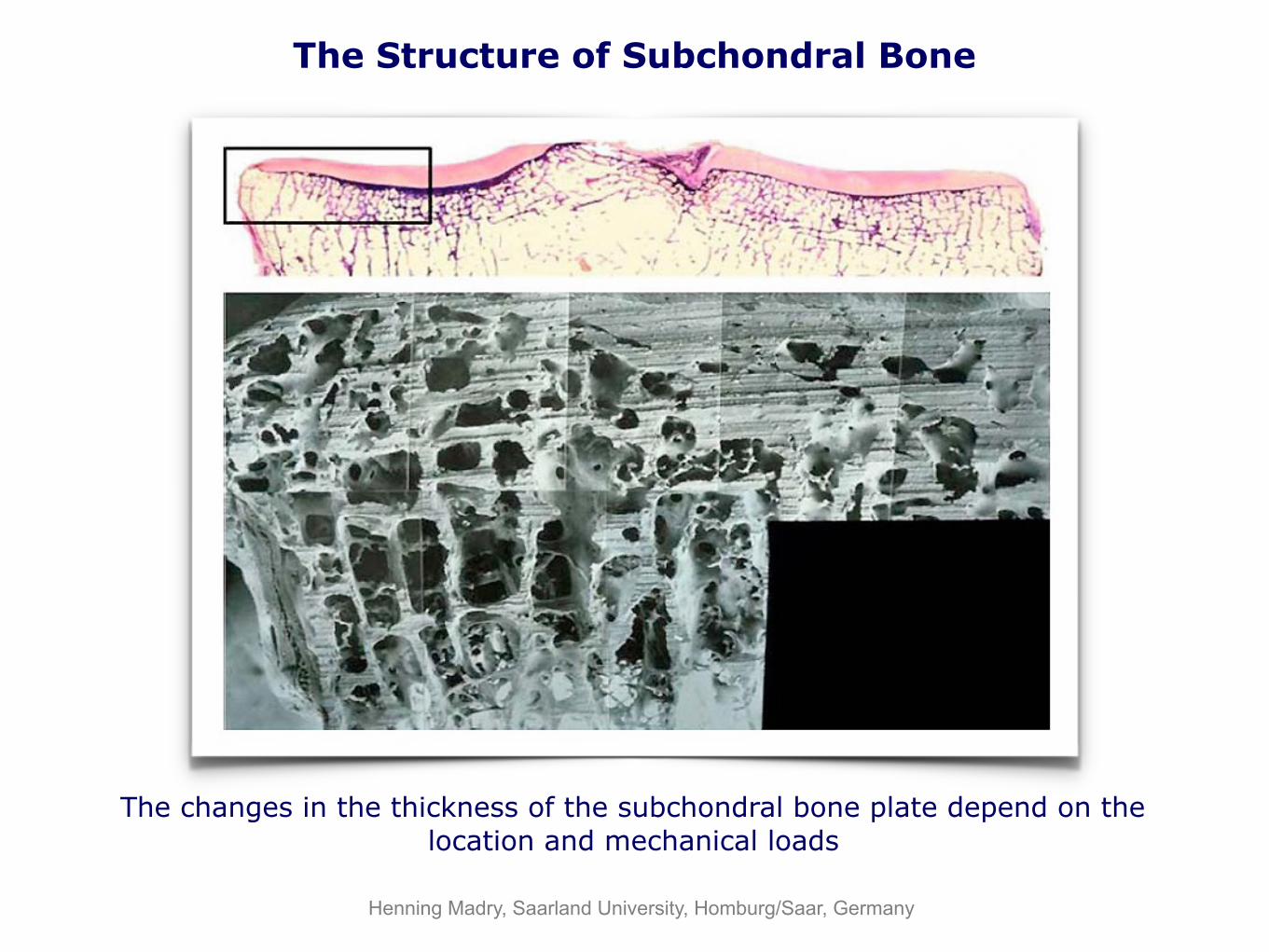
The Structure of Subchondral Bone
The changes in the thickness of the subchondral bone plate depend on the location and mechanical loads
Henning Madry, Saarland University, Homburg/Saar, Germany



Arthroscopy Journal, article in press, 2015

Arthroscopy Journal, article in press, 2015

PRP




PRP Today

In adults, stem cells act as a repair system for
the body. They allow replacement of ageing
and damaged cells in organs.
In adults, damaged tissue is usually replaced
with scar tissue which loses most of its original
function. Stem cell therapy has the potential to
restore the original structure and function of
the damaged tissue.
Researchers believe that stem cell therapy could
dramatically improve medical treatment, espe-
cially in the field of regenerative medicine.
Adult Stem Cells
KLSMC STEM CELLS
Stem Cells
KUALA LUMPUR SPORTS MEDICINE CENTRE
INFORMATION FOR PATIENTS
7th Floor, Wisma Perintis,
47 Jalan Dungun, Damansara Heights, 50490 Kuala Lumpur, Malaysia. Tel: +603 2096 1033
Fax: +603 2096 1500
Stem Cell Enquiry: +603 2089 5239 E-mail: [email protected]
Website: www.klsmc.com
Outpatient Clinic Hours Monday to Friday ( 9am to 5pm ) Saturday ( 9am to 1pm )
KUALA LUMPUR SPORTS MEDICINE CENTRE
Location Map
Parking is available in the basement P


Saw et al.: Arthroscopy 2013


Chondrogenesis: Contained Lesion

Chondrogenesis: Uncontained Lesion

Saw et al.: Arthroscopy 2011
Gradual Regeneration of Articular Surface



13th ICRS World Congress, Sorrento September 2016

SVF Adipose Tissue MSCs

•Adipose tissue derived MSCs?
•Stem cells isolated from fat are being considered as an option for treating tissue damage and diseases because of their accessibility and lack of rejection.
•New research published in BioMed Central's open access journal Stem Cell Research & Therapy shows that this is not as straightforward as previously believed, and that fat-derived stem cells secrete VEGF (Vascular Endothelial Growth Factor) and other factors, which can inhibit cartilage regeneration.
•However pre-treating the cells with antibodies against VEGF and growing them in nutrients specifically designed to promote chondrocytes can neutralize these effects.
The Best Source of Autologous Stem
Cells?






“Vladimir, give me a brief summary …”
From: Vladimir Bobic Sent: 27 March 2011 10:33 To: Fares Haddad Subject: Re: cartilage
Hi Fares,
There is not much new on the horizon. There are quite a few scaffolds/implants, etc, but nothing really exciting. We ("the cartilage people") seem to be too focused on repairing only one layer (articular cartilage), while we have much bigger structural (and metabolic) problems with an osteochondral unit. Better understanding of subchondral activity and more 3D approach to repairing the whole (osteochondral) unit rather than just damaged articulating surface is what we need if we really want to make this work functionally. As you know from my previous email, there is still a huge unmet need in treating symptomatic chondral and osteochondral lesions as many articular cartilage procedures fail functionally even with non-impact high-level pro sports. In that respect, and looking honestly at our functional outcomes of ACI/MACI surgery the best we can do is just to plug the hole (literally) with so-called "functional repair tissue", at enormous expense (over £16,000 for Genzyme ACI/MACI and over £26,000 for TiGenix CCI!) and reduce athletic population to tears and despair with months of slow and restrictive rehabilitation. We are definitely not very successful with ACI technology when it comes to anticipated functional outcomes at almost any athletic levels, although we don't know if this technology helps biologically in the long run. I don't think that TruFit works in the long run, although the concept is good, but the biological response to biphasic materials is not. OATS is generally good in the long run, but mainly for smaller lesions and with single 10mm grafts. The surrounding cartilage often fails (years later) and things get worse circumferentially, often associated with increased subchondral activity (bone marrow oedema) and subchondral cysts (failed subchondral remodelling), which is probably a consequence of very slow but much wider osteochondral problem at the outset. I often use deep subchondral decompression through the recipient socket and implant autologous bone marrow aspirate, all of which seems to work better that OATS on its own. I saw an excellent vet paper in the JBJSA last year, looking at the same combo in horses, and they confirm that OATS + ABM is better than OATS alone. I hope this is of some help.
Regards, Vladimir
London Knee Meeting 2011London, 13 October 2011.
Articular Cartilage Repair one step forward, two steps back … (in 7 minutes)

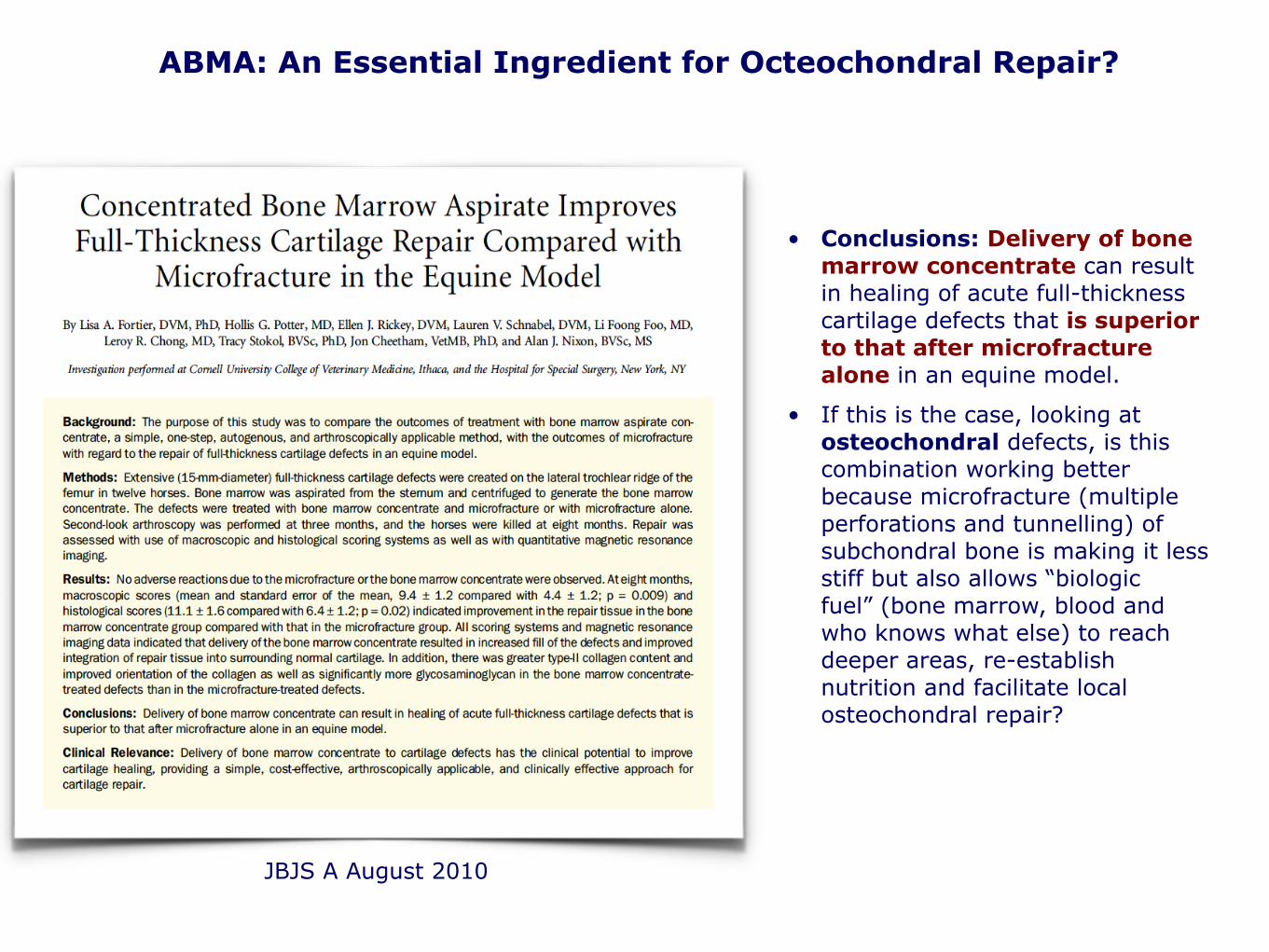
• Conclusions: Delivery of bone marrow concentrate can result in healing of acute full-thickness cartilage defects that is superior to that after microfracture alone in an equine model.
• If this is the case, looking at osteochondral defects, is this combination working better because microfracture (multiple perforations and tunnelling) of subchondral bone is making it less stiff but also allows “biologic fuel” (bone marrow, blood and who knows what else) to reach deeper areas, re-establish nutrition and facilitate local osteochondral repair?
ABMA: An Essential Ingredient for Octeochondral Repair?
JBJS A August 2010

Autologous Osteochondral Grafting (OATS)

An alternative approach to the treatment of femoral and tibial Osteonecrosis, Chronic SONK and Secondary OA:
• The knee is often not too bad (all 3 compartments) or it is too early for a partial or a full knee replacement.
• Classic Microfracture and Core Decompression are probably not deep enough.
• Looking at most MRIs it seems that we need to reach at least 15 to 20 mm deep into subchondral bone, which is where any cylindrical osteochondral harvesters are very handy.
• Effectively, this is a combination of OAT and deep core (subchondral) decompression, with a hand driven K-wire, through the bottom of the recipient socket, with
• a mixture of autologous blood + bone marrow injected into the recipient socket,
• and capped with 10 mm OATS plug, which was soaked in the same mixture of bone marrow and blood.
• This “integrated” subchondral repair concept makes sense, it gives most people quick and durable pain relief and better knee function, but it is based on huge assumptions.
• The main question is weather unprocessed (and not concentrated) autologous bone marrow, is powerful enough biologically?
CKC UK

Lateral Femoral Trochlea: a reliable source of good cancellous bone and bone marrow, even in advanced OA
CKC UK
MFC AVN

Autologous Bone Marrow Aspirate
Autologous Bone Marrow Aspirate
AANA Annual Meeting San Francisco 2011

Autologous Bone Marrow
• Red marrow has significant haematopoietic stem cell potential and still persists in adults in certain areas such as the iliac crests.
• The anterolateral trochlea (the usual OATS donor site) is often spared even in advanced OA and seems to contain reasonably good bone marrow, which can be aspirated through the donor site.
• Pluripotent haematopoietic stem cells can differentiate into any and all of the cells of circulating blood and the immune system.
• MRI studies have indicated that the conversion of red to fatty marrow occurs prematurely in some patients with avascular necrosis.
• Osteonecrosis is associated with a decrease in progenitor cells in the proximal femur. Bone marrow also contains osteogenic progenitors, with a potential for effective bone regeneration.
• It seems sensible to use core decompression but also to deliver better “biologic fuel” with pluripotent cells to the affected area.
• The quantity and quality of good autologous bone marrow is questionable, but as it seems that stem cells do not to do the actual work (they seem to go around and boss other cells and tell them where to go and what to do) a few mils of bone marrow aspirate may be good enough to kick-start the process.
CKC UK


JBJS B June 2006

SONK Before and After Subchondral Decompression
• 15/12/08: subarticular insufficiency fracture and slight flattening of the MFC and prominent subarticular marrow oedema more marked on the femoral side. Since 04/04/08, significant deterioration in the medial compartment with SONK-like process, progressive degenerative changes …
• 11/09/09: Comparison is made with the previous scan 15/12/2008. In the medial compartment, following the subchondral decompression, there is now evidence of articular irregularity, deficiency and thinning of articular cartilage, slight increase in the subarticular marrow oedema and early subarticular cyst formation in the outer aspect of the MFC …

SONK: sudden onset, severe knee pain
MRI: “In the outer weight-bearing portion of the medial femoral condyle, there is an osteochondral lesion (22mm ant-post x 10mm med-lat x 2mm deep), with fluid at the interface with parent bone, mild reactive marrow oedema and a cortical break peripherally in keeping with instability. Degenerative changes in the medial compartment with spontaneous osteonecrosis of the medial femoral condyle (SONK) and unstable fragment.”
David Ritchie, Glasgow CKC MRI 060506

FU MRI: “In the medial compartment, the graft over the central weight-bearing portion of the medial femoral condyle has incorporated with adjacent bone and the overlying articular cartilage is flush with adjacent native cartilage. A small focus of marrow oedema is noted directly beneath the graft but overall there has been a reduction in marrow oedema around the graft. A small trace of subcortical fluid in the peripheral portion of the medial femoral condyle is similar to the pre-operative scan - presumably not included in the repair.”
Dr David Ritchie, Glasgow CKC MRI 030307

The Subchondroplasty Procedure


Dear Mr Bobic,
I am writing to you to give an update of my progress and to say thanks. You carried out a Medial Subchondral Decompression, Autologous Bone Marrow Transplant and Autologous Osteochondral Grafting for me on the 7th of January 2009. I found the standard of care you supplied to be excellent. I have had numerous surgeries over the past twenty years following very poor care provided to me when I was eighteen years old. Yours was the last procedure I had. Following this my pain has been greatly reduced and my function significantly improved. To compliment your work, I have worked with a biomechanist to balance and strengthen my body with particular focus on my legs.
Last September, I completed the Yorkshire Three Peaks Challenge which, in case you are not aware, involves walking a twenty five mile circuit and climbing the highest peaks in Yorkshire. This has to be completed in less than twelve hours which basically means only two ten to fifteen minute stops. My knee was strong and pain free for the whole event and the next day provided me with only a small amount of low level aching. There were plenty of others with no surgical history who were worse off.
I would like to thank you very much for making this possible for me. I undertake regular walks in the Lake District, Yorkshire Dales and Wales and this would not of been even considered before your help.
I do understand that I will need a knee replacement in the future and I will not hesitate in coming to see you for this procedure. Of the many surgeons I have seen I feel the standard of care and expertise you provided was, by far, the best which has been born out by the excellent result I have had.
Thanks again and see you in the future
Yours sincerely
From: R... L... <[email protected]>Subject: UPDATE AND THANKSDate: 12 April 2013 16:08:18 BSTTo: Vladimir Bobic <[email protected]>

This applies to our attitudes but also to stem cell technologies …
"There are only two ways to live your life:
One is as though nothing is a miracle.
The other is as though everything is a miracle."
Albert Einstein

The Future is Cellular! Thank You
