bone and soft tissue neoplasms - s1.stanford.edu
TRANSCRIPT

Bone and Soft Tissue Neoplasms
Jesse K McKenney, MDAssistant Professor
Department of Pathology
Bone and Soft Tissue Neoplasms
• Essential Concepts in Lecture• Background and Definitions in syllabus
and Robbins
• PRIMARY bone tumors are RARE– Metastases to bone are common
• Soft tissue tumors are very rare

Cancer Death Rates*, for Women, US,1930-2002
*Age-adjusted to the 2000 US standard population.Source: US Mortality Public Use Data Tapes 1960-2002, US Mortality Volumes 1930-1959,National Center for Health Statistics, Centers for Disease Control and Prevention, 2005.
0
20
40
60
80
10019
30
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
Lung
Colon & rectum
Uterus
Stomach
Breast
Ovary
Pancreas
Rate Per 100,000
0.1Bone

Cancer Incidence Rates* in Children 0-14 Years, by Site, 1998-2002
*Per 100,000, age-adjusted to the 2000 US standard population.ONS = Other nervous systemSource: Surveillance, Epidemiology, and End Results Program, 1975-2002, Division of Cancer Control and Population Sciences, National Cancer Institute, 2005.
Site Male Female Total
All sites 15.6 14.3 15.0
Leukemia 4.9 4.2 4.6
Acute Lymphocytic 3.9 3.4 3.6
Brain/ONS 3.6 3.3 3.5
Soft tissue 1.1 0.9 1.0
Non-Hodgkin lymphoma 1.2 0.6 1.0
Kidney and renal pelvis 0.8 1.0 0.9
Bone and Joint 0.6 0.6 0.6
Hodgkin lymphoma 0.6 0.5 0.5

Soft Tissue/ Bone Neoplasms
• Reality Check– Many experienced pathologists are
uncomfortable diagnosing the tumors in this chapter
• Histologic differences are more subtle• Tumors are rare with hundreds of subtypes
– most have little diagnostic experience with them
• However– Many mistakes are made in the treatment of
these tumors because physicians are not aware of basic principles

Basic Principles
• Prognosis• Treatment• Diagnosis
– Clinical• Age, anatomic site, x-ray, syndrome?
– Microscope • Few basic principles for this course

Clinical Course/Prognosis
• Low-grade Sarcoma– Local recurrence– Progression to high-grade
• High-grade Sarcoma– Local recurrence– Hematogenous metastasis
• Lung

Prognosis: Location Dependent
• Sarcomas arising in a superficial location (dermis and subcutis) have a much better prognosis than deep seated sarcomas– Larger = worse prognosis
• Deep extremity sarcomas (grade-for-grade) behave better than retroperitoneal sarcomas (resectability)

General Treatment Principles
• Low-grade sarcoma– Surgical excision with wide margins
• High-grade sarcoma– Option of neoadjuvant chemo/radiation– Surgical excision with wide margins– Adjuvant chemo/radiation

Adjuvant Chemotherapy for Completely-Resected Primary
Osteosarcoma
• Metastatic sarcomas are essentially incurable (rare exceptions)
• Local control best accomplished by surgery (localized radiation for unresectable sites)
• Chemotherapy (high grade) affects systemic micrometastases and improves survival
Soft Tissue/ Bone Neoplasms

Diagnosis of Bone and Soft Tissue Tumors
• Must establish:– Histologic type– Extent of spread (stage)
• Accuracy depends on synthesis of:– Clinical findings– Radiologic findings– Pathologic findings

BONE

Presenting Signs and Symptoms
• Pain• Mass• Incidental finding on X-ray• Loss of Function
– pathologic fracture
• Prompt and accurate diagnosis improves chances of complete resection

Radiologic Findings
• Localization– part of bone
• Margin of tumor– sharp (sclerotic)– fuzzy (infiltrative)

Pathologic Findings
• Evidence of differentiation– Matrix formation
• Cartilagenous• Bone (osteoid)• None
– Fibrous
– Growth pattern– Cytologic features

Normal Anatomy
epiphysis
metaphysisdiaphysis
physis
childhood adult
cortex
medullary space
physeal scar

Anatomical Site

Tumor Border with Adjacent Bone
Patient 1 Patient 2

High Grade Osteosarcoma
• Age (2 peaks)– 75% < 20 years of age– Elderly (Paget dx)
• Site– Usually in metaphysis of long
bones (<20 yrs)• Femur• Tibia• Humerus
– In older patients, flat bones almost as common

High-grade Osteosarcoma

High Grade Osteosarcoma

High Grade Osteosarcoma

Tumor Matrix

Conventional Chondrosarcoma
• Age – >40 years of age (usually older)
• Site– Usually central skeleton
• Pelvis• Ribs• Shoulder
– Extremity much rarer

Chondrosarcoma

Chondrosarcoma

Chondrosarcoma

42 year-old man bumped kneeEnchondroma

Enchondroma Chondrosarcoma

Giant Cell Tumor of Bone
• Age– Usually 20-40 years (Skeletally mature)
• Site– Long bones (Epiphysis/Metaphysis)
• Distal femur• Proximal tibia
• Prognosis• Local recurrence rate 40-60%

Giant Cell Tumor of Bone

Giant Cell Tumor of Bone

Epiphyseal TumorsGiant Cell Tumor
of BoneChondroblastoma
Skeletally Mature?

Metastatic Carcinoma
• Most common skeletal malignancy in adults
• X-ray– Lytic – Blastic– Mixed
• In older patients, destructive bone lesions are mets until proven otherwise

Metastases
• Carcinoma– Prostate adenocarcinoma– Renal cell carcinoma– Breast adenocarcinoma
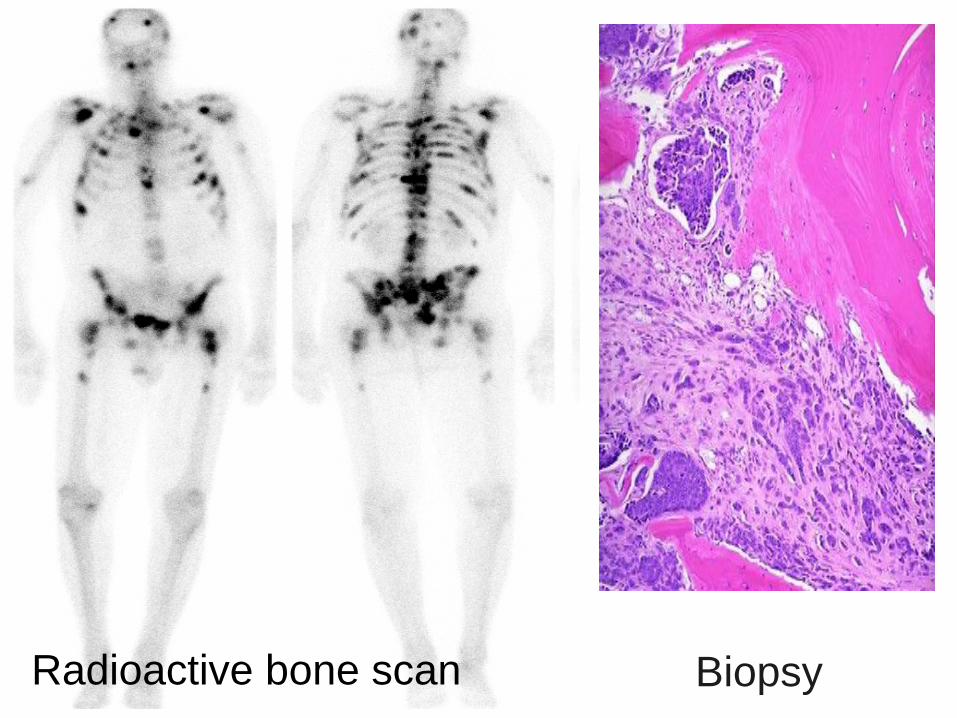
Radioactive bone scan Biopsy
Bone Tumor Syndromes
• Osteomas + Deep Fibromatosis + Adenomatous Polyposis = GARDNER SYNDROME

Bone Neoplasms
• Goals– Clinical/pathologic setting
• Child vs Adult• Anatomic Site (X-RAY)• Differential diagnosis
– Morphology• Matrix?
– Behavior/treatment

SOFT TISSUE

Soft Tissue Neoplasms
• Completely Benign– Lipoma
• Locally recurring– Fibromatosis
• Locally recurring, potential for grade progression (Low grade)– Atypical lipomatous tumor/well differentiated
liposarcoma• High metastatic potential (High grade)
– Rhabdomyosarcoma

Soft Tissue Neoplasms
• Fat• Muscle
– Smooth – Skeletal
• Fibroblast• Uncertain histogenesis

Lipoma
• Age: – Usually adults– (Most common soft tissue tumor)
• Site: – Usually superficial (any site)– Occasionally deep to superficial fascia
(intramuscular)• Prognosis
– Recurrence is very rare

Lipoma

Intramuscular Lipoma

Atypical Lipomatous Tumor/Well Differentiated Liposarcoma
• Age:– Generally a neoplasm of adults
(>40 years of age typical)• Site:
– Usually deep soft tissue (any site)
Most common adult sarcoma!

Fibrous septa and atypical stromal cells“Smudge cell” (Atypical stromal cell)
Atypical Lipomatous Tumor/ WDL

Atypical Lipomatous Tumor/ WDL
Lipoblast
De-differentiated Liposarcoma(Grade Progression)
• De-differentiation– Progression in grade to a high-grade
sarcoma• Undifferentiated pleomorphic sarcoma

Atypical Lipomatous Tumor/ WDL High-grade Sarcoma
Dedifferentiated Liposarcoma

Dedifferentiated Liposarcoma
ALT
High-grade
Sarcoma
ALT
High-grade sarcoma
Recurrence
Atypical Lipomatous Tumor/ Well Differentiated Liposarcoma
• Prognosis: – Site dependent
• Extremity– lower recurrence rate– very low-risk of de-differentiation
• Retroperitoneum– indolent course with multiple recurrences– higher risk of de-differentiation
– With de-differentiation• Metastatic potential

Malignant Fibrous Histiocytoma (MFH)
• Age– Adult
• Site– Deep soft tissue
• Prognosis– Aggressive recurrence– Metastasis

Malignant Fibrous Histiocytoma (MFH)
• A heterogeneous group of high grade pleomorphic, undifferentiated sarcomas– Ugly sarcoma without differentiation = MFH

Malignant Fibrous Histiocytoma
Nulcear pleomorphism, hyperchromasia

Deep Fibromatosis (Desmoid)
• Age:– All ages
• Site:– Extremities– Trunk– Abdominal wall– Mesentery

Deep Fibromatosis (Desmoid)
• Prognosis:– High rate of local recurrence– Does NOT metastasize– Can cause death due to infiltrative
growth• If in anatomically delicate area
(carotids)• Syndrome:
– Gardner syndrome

Fibromatosis

Fibromatosis

Soft Tissue Tumor Cytogenetics
• EWS Translocations– Ewing/ PNET– Clear cell sarcoma– Extraskeletal Myxoid Chondrosarcoma– Desmoplastic Small Round Cell Tumor
• SYT-SSX Fusion Gene– Synovial Sarcoma
• PAX-FKHR Fusion Gene– Alveolar Rhabdomyosarcoma

“The Big Picture” Bone and Soft Tissue Tumors
• Prognosis• Treatment• Diagnosis
– Clinical• Age, anatomic site, x-ray, syndrome?
– Microscope • Few basic principles