bone grafts used in nasal reconstruction
TRANSCRIPT

Presenter – Dr. Pulkit Agarwal

INTRODUCTION Nasal surgery involves a wide spectrum of
procedures ranging from cosmetic rhinoplasty to
total nasal reconstruction.
Reconstruction of the nasal skeletal framework
is frequently necessary in patients like with
congenital or traumatic deformities.
This support is best obtained using bone or
cartilage.

HISTORY VON WALTER (1821) – Autogenous Bone Graft
Autogenous corticocancellous bone grafts to
reconstruct lost parts of the maxillofacial
skeleton.
These grafts can be used to augment the
severely atrophic edentulous alveolar ridges,
to reconstruct alveolar defects in cleft palate
patients, or to bridge defects that are the result
of ablative surgery or trauma.

Autogenous bone grafts, when adequately fixed,usually adapt to the recipient site and incorporatewell into the defects.
A layer of connective tissue will cover the graftswhile from the interface between the recipient boneand the graft revascularization takes place ultimatelyleading to the formation of new bone.
Fresh autografts contain surviving cells andinductive proteins, which can stimulate osteogenesis.
Autogenous grafts considered best as :
Nonimmunogenic
Partially retains its viability immediately aftertransplantation

WHY ALTERNATIVES ????
Limited availability
The sometimes unpredictable resorption
The need for a second operation site
The time consuming procedure
Donor site morbidity
The quantity of bone available
Increased costs of hospitalization

MECHANISMS OF BONE GRAFT HEALING
Many factors influence healing process, which mayalso be considered as a kind of bone regeneration.
Factors like :
Bone metabolism
Changes in hormonal balance
External influences that are present for a prolongedtime.
Revascularization is mandatory for graft healing asnewly formed blood vessels enable nutrients andhumoral substances to be brought into the graft.

MECHANISMS OF BONE HEALING

If revascularization is successful new bone is formedaround the transformed osteocytes at the margins of thegraft and the old bone is slowly replaced.
This process is called ‘Creeping Substitution’
WHICH TYPE OF BONE IS SUPERIOR ???
Cancellous bone – Easy capillary penetration.
Cortical bone – Volumetric maintainence.
So Corticocancellous bone is best.
Differences in healing between severalcorticocancellous donor sites are related to the 3Dosseous architecture ( The Cortical / Cancellous ratio)

TYPES OF GRAFT MATERIAL Per definition there are five types of grafts, i.e.
1. Autografts
2. Isografts
3. Allografts
4. Alloplasts
5. Xenografts
The term autograft refers to tissue transplanted from
one site to another within the same individual.
It can be cortical, cancellous or corticocancellous.
Most common sites for corticocancellous grafts areTypical donor sites are rib, iliac crest, fibula or radius,elbow, mastoid whereas oral sites include chin,retromolar area and mandibular body.
Allografts are obtained from cadavers or livingindividuals from the same species. In human medicinethey can be obtained from tissue banks (KÜBLER1997).
There are three types of bone allograft available:
Fresh or fresh-frozen bone
Freeze-dried bone allograft (FDBA)
Demineralized Freeze Dried Bone Allograft (DFDBA)
The most commonly used allograft is DFDBA.
Demineralized bone matrix minimises antigenicity.
Because allografts are not osteogenic, bone formation
takes longer and results in less volume compared to
autogenous grafts .
They revascularize quickly but the risk of an antigen
transmission, especially in a high vascular area as the
facial skeleton, increases the risk of rejection of the
graft.
So in oral and maxillofacial area demineralized bone
grafts can be used after irradiation.
Alloplasts are synthetic materials consisting of
biological inert substances. (eg Tricalciumphosphate
and Hydroxyapatite, Bovine Bone Mineral (BBM),
Coralline, Active glass ceramics).
Xenografts are composed of tissue taken from another
species (i.e. from an animal source, usually bovine).
The term ‘composite graft’ refers to grafts that are
composed of materials from different origins,
usually autogenous bone mixed with other
materials

CHARACTERISTICS OF THE IDEAL GRAFT MATERIAL
Nonimmunogenic
The shape and size of material is stable over time.
The material is reasonably malleable to carve or mold
into the desired shape.
The material does not cause discoloration or
transillumination of the intervening tissue.
The material is pliable.
The material is easily obtainable.
An adequate supply of the material is available.
Minimum donor site morbidity
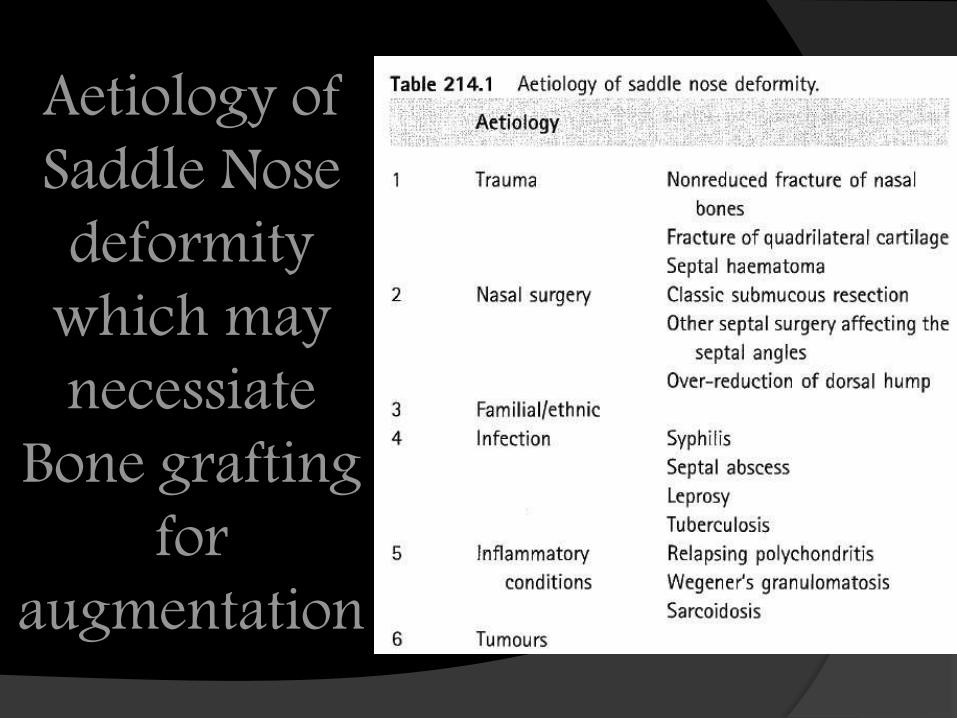
Aetiology of Saddle Nose deformity
which may necessiate
Bone grafting for
augmentation

BONE GRAFTS USED FOR NASAL RECONSTRUCTION
NASAL BONE :
Small pieces of nasal bone may be removed during the
course of traditional rhinoplasty and can be re
implanted as a graft.
A particularly good use for this bone is as a graft to
bone gaps at the lateral osteotomies.
HIP BONE GRAFTS :
Less popular as bone tends to shrink (due to lack of
density of bone which inturn is helpful in carving it).
Other problem being painful donor site.

CALVARIAL BONE GRAFTS :
Very Dense
Used most commonly for nasal reconstruction.
The skull is formed from two layers of bone which are
separated by a type of marrow.
The outer layer may be removed and used for grafting.
It is possible to cause a fracture of the skull and there
is a remote chance of damage to the underlying brain.
Not recommended after 50 yrs age as outer layer fuses
with inner due to disappearance of marrow.
RIB BONE :
Commonly used.
Hard outer cortical layer used for grafting.

Problems include :
Ribs are curved.
Painful donor site
Scar on chest.
OLECRANON BONE GRAFT :
The bone is not particularly dense but the small
quantity that would be harvested is likely to persist in
the nose longer than a block of very porous
(cancellous) bone from within the hip bone.
This scar and minor bone deformity at the elbow are
very acceptable.
RADIAL BONE GRAFT :

BONE GRAFT FROM THE JAWS :
If small amount of bone required.
Ramus Graft – from area of wisdom tooth.
Tuberosity graft – from the posterior part of the upper
jaw behind the last molars.
Chin Grafts
Bone is harvested and placed immediately to the
required site where it is secured into place using small
screws, which will be removed at a later date.
Can be done under LA or intravenous sedation.

TIBIAL BONE GRAFT
Tibial bone graft is often used for sinus lift procedures
rather than nasal augmentation.
One can expect some discomfort at the surgical site for
a period of days or sometimes a week or two, though
walking is not restricted.
This surgery can be done as an outpatient at a surgical
facility.
MASTOID BONE GRAFT
Provides adequate autologous bone in most cases of
primary or revision rhinoplasty.
The donor site carries low morbidity and a well
camouflaged scar.
It is easily accessible.


SADDLE NOSE DEFORMITY RECONSTRUCTION WITH A SPLIT CALVARIAL BONE L-SHAPED STRUT
SURGICAL TECHNIQUE :
HARVESTING AND FASHIONING OF GRAFT :
Scalp incision is made along the superior rim of the temporalis
muscle in the nondominant temporoparietal region.
A trifurcated incision is then created, extending the incision
inferiorly within the hairline to the preauricular sulcus.
Dissection in the subgaleal plane is performed, and the
periosteum is incised 1.5 cm inferior to the scalp incision.
The periosteum is then elevated off the calvarial bone in this
region. A 6-mm round cutting bur is used to circumferentially
isolate a piece of outer table cortex.

Drilling is continued down to the level of the diploic bone.
A curved sagittal saw and curved osteotome are used to lift
the outer cortex free from the intact calvarium.
Bone wax is applied as necessary for hemostasis. The
periosteum is then closed using polyglactin 910 (Vicryl)
sutures, and the scalp is closed using subdermal 4-0
polyglactin 910 sutures and 4-0 chromic locking skin
sutures.
A suction drain is placed in the subgaleal layer and is
removed on postoperative day 1. The bone graft is divided
into 2 pieces that are used to construct a dorsal onlay graft
and columellar strut. The dimensions of each are based on
the ideal nasal length and projection.5,6 The dorsal piece is
contoured using 3- and 4-mm coarse and fine diamond burs
to recreate the concavity of the natural dorsum.

The cortical side is placed superficially, and the cancellous
side is placed deep.
The cephalic- most portion of the dorsal piece is thinned
and beveled to enable a smooth transition with the patient’s
intact bony nasal bridge. In addition, the dorsal piece is
beveled laterally to prevent a noticeable ridge.
The 2 pieces are fastened together using a 1-mm titanium
screw, in contrast to previously described tongue-in-groove
techniques. The L-shaped strut is then ready for
implantation

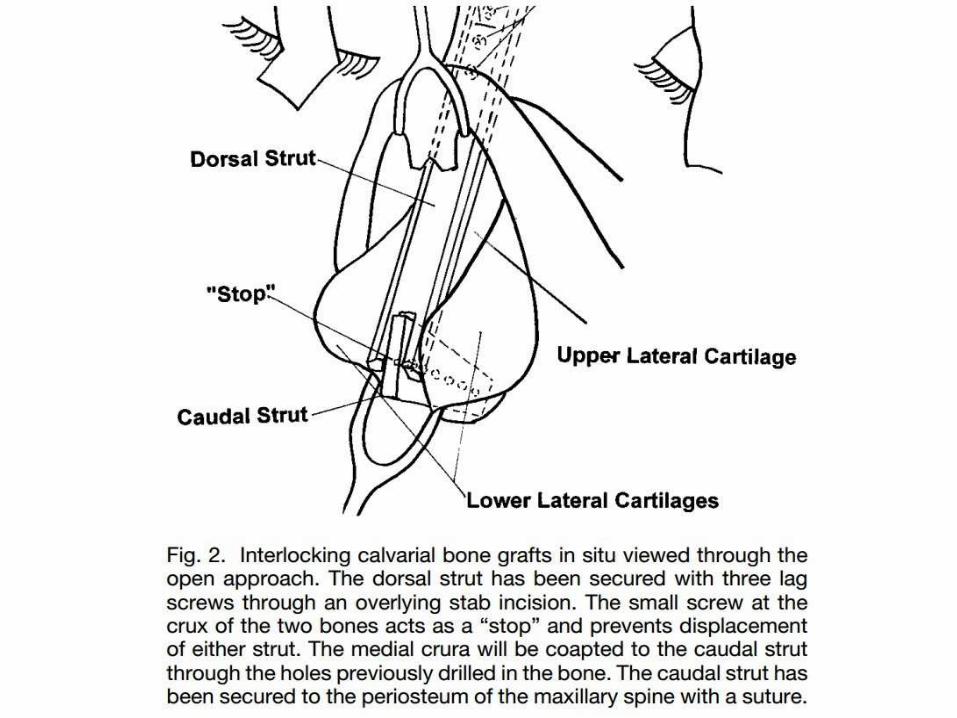
PLACEMENT OF THE L-SHAPED STRUT
The nasal skeleton is exposed using an external
rhinoplasty approach through an inverted-V columellar
incision with intravestibular marginal incisions.
Dissection is carried cephalically to the nasal dorsum. A
small portion of the nasal root is filed down to enable
smoother placement of the dorsal portion of the L-shaped
strut.
This also creates a “raw” bony surface for direct bone-to
bone contact, which hypothetically would enhance
osseous integration and fusion of the bone graft.

The medial crura of the lower lateral cartilages are
separated to enable placement of the caudal portion of the
graft into a secure pocket. In a manner akin to the
placement of a columellar strut, the bone graft is placed
into a secure pocket between the medial crura.
The base of the L shaped strut rests on the pre maxilla and
is secured with a transcrural suture. Once the L-shaped strut
is positioned in place, the lower lateral cartilages are
advanced over the caudal portion and vertex of the L-
shaped strut using intradomal sutures.
Two wire-pass drill holes are made in the dorsal bone to
place anchoring sutures to fix the lower lateral cartilages in
position and maintain the midline position of the graft. The
skin and soft-tissue nasal envelope is then closed.

CREATION OF OSTEOTOMIES
If osteotomies are necessary, a No. 11 blade is used to
create stab incisions in the cheek-nose junction bilaterally
to access the lateral rim of the bony nasal pyramid.
Medial and lateral osteotomies are then created near the
nasal bone midline and the nasofacial groove, respectively.
DRESSING
Contour taping is placed immediately after closure to shape
the external structure of the nose. A 1-piece standard porous
cast (ThermaSplint; Whitehall Manufacturing, City of
Industry, California) is placed superficial to the tape. The
cast and tape are removed 1 week postoperatively.


RADIAL BONE GRAFT FOR SEPTAL CORRECTION
Anaesthesia preferred – GA.
After local anaesthetic infiltration the nasal structures wereexposed through an open rhinoplasty approach.
Following hump resection, the septum was dissectedsubperichondrially and resected leaving a 0.8 to 1-cmdorsal and caudal L-strut.
Deviated caudal segment of the septal cartilage wasstraightened medialized and secured to the periosteum ofthe anterior nasal spine.
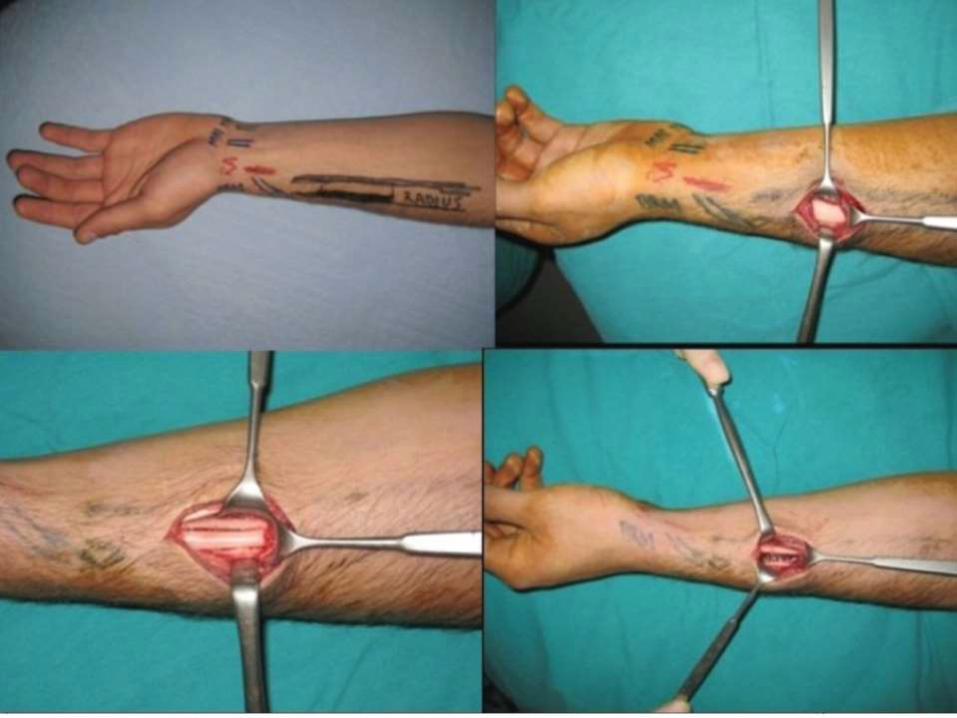
Radial bone graft was accessed from the lateral antecubitalregion, and bone graft was harvested from the lateral sideof radial bone.

Radial bone is triangular in cross section. The anterior and
posterior surfaces of the radius are generally smooth, whereas an
oval roughening for the attachment of pronator teres marks
approximatelly the middle of the lateral surface of the radius.
Bone graft was harvested a segment (about 5×1 cm) located
between the insertion of the pronator teres and the
brachioradialis muscles.
Lateral antecubital nerve, flexor and extensor muscles were
protected during bone graft harvesting procedure.
Bone graft was thinned by bone filing and shaped in the form of
a L-strut as "key in the keyhole pattern”.
The dorsal strut was placed by tongue in groove technique on the anterior nasal spine. L-strut frame was sutured under the upper lateral cartilage remnants and between the domes of two lower lateral cartilages to hide palpable edges and secure it in place.
Lateral and median osteotomies were also performed if
bony pyramid was also deviated.
Any residual irregularities on the dorsum were camouflaged
with Erol's Turkish delight.
Tipplasty was performed if necessary. Following closure,
nasal packing and plaster cast were applied. A plaster cast
was also applied on the forearm and removed 1 week later.
The packing and the nasal splint were removed at 4th and
7th days, respectively.


OLECRANON BONE GRAFT
SURGICAL PROCEDURE FOR GRAFT REMOVAL
The non-dominant forearm was chosen for removal of the
olecranon bone graft.
The proximal third of the posterior face was infiltrated followed
by a longitudinal incision and dissection of the planes.
The cortex of the olecranon was measured according to the
nasal defect for repair and the graft was removed with a bone
saw or a simple chisel.
Upon removal, the olecranon was placed in a container with
saline solution and the donor area was covered with bone wax.

Synthesis was carried out by planes, with absorbable sutures and
of skin with 4.0 nylon intradermal threads.
Finally, the limb was covered with a crepe bandage. A tourniquet
was not necessary. The graft was transferred into the recipient
area with external anchoring with micropore tape for 21 days;
rigid fixation was not used.
Possible graft resorption was monitored by anthropometric
measurements of the nose with photographic documentation and
graft radiological control.
Patients reported temporary paresthesia in the forearm scar
(donor area), with a complete recovery within 1 year.
The olecranon bone graft proved to be a good option for primary
or secondary rhinoplasty for the treatment of “saddle-back”
nose. Long-term resorption or morbidity of the donor area has
not been observed so far. This procedure ensures satisfactory,
predictable, and long-lasting aesthetic results


AUGMENTATION OF NASAL TIP PROJECTION USING
THE INFERIOR TURBINATE
GRAFT HARVEST AND PREPARATION
Inferior partial turbinectomy is performed in standard fashion,
following decongestion.
After careful infracture with a freer elevator, a right-angled
scissor is used to resect the anterior head or two-thirds of the
turbinate, including bone and soft tissue. After careful extraction
from the nose, the soft tissue covering the turbinate bone is
removed using iris scissors or a No. 15 blade, taking care to
avoid trauma to the turbinate bone.
The size of the implant will vary depending on the patient's
degree of bony inferior turbinate hypertrophy. The graft is then
shaped using a Mayo scissor. Hemostasis of the cut end of the
turbinate is achieved using suction electrocautery.

PLACEMENT
Placement of the graft can be done either Endonasally or using
an open approach.
If an endonasal approach is used, it is important for the surgeon
to carry the marginal incision almost to the medial crural
footplate and then to dissect the lower lateral cartilage free along
its length.
This allows direct placement of the strut, which will not bend
significantly, and minimizes the risk of fracturing the implant.
The marginal and transfixion sutures are closed with 4-0
chromic gut.
The nose is then taped and cast in standard fashion. A stabilizing
suture can be placed in a septal-columellar fashion. Because
driving a needle through the implant risks fracture, place the
suture just posterior to the implant in the membranous septum.
Recent AdvanceMASTOID BONE A NEW GRAFT MATERIAL IN
RHINOPLASTY
The mastoid bone graft provides adequate autologous bone
in most cases of primary or revision rhinoplasty.
The donor site carries low morbidity and a well
camouflaged scar.
It is easily accessible especially for the otolaryngologist
who is accustomed to operating on the mastoid bone

Referemces :Scott Brown 7th Edition
Barone CM, Jimenez DF and Goodrich JT (2008).
Exorbitism. In: Goodrich JT (ed.), Neurosurgical
Operative Atlas. Paediatric Neurosurgery, 2nd edn. New York: Thieme, pp. 76-82.
Chait LA, Becker H and Cort A (1980). The versatile costal osteochondral graft in nasal reconstruction.
Br J Plast Surg, 33(2): 179-184.
David DJ and Moore MH (1989). Cantilever nasal bone grafting with miniscrew fixation. Plast Reconstr Surg, 83(4): 728-732.
Farina R and Villano JB (1971). Follow-up of bone grafts to the nose. Plast Reconstr Surg, 48(3):251-255.
Gewalli F, Berlanga F, Ortiz-Monasterio F and Holmström H (2008). Nasomaxillary reconstruction in Binder Syndrome: bone versus cartilage grafts. A long-term intercenter comparison between Sweden and Mexico. J Craniofac Surg, 19(5): 1225-1236.



External Rhinoplasty The elephant trunk incision, the trans columellar incision, The
decortication technique, the external approach and open or
external rhinoplasty.
INDICATIONS
Congenital deformities, such as the cleft lip nose
Extensive revision surgery
Severe nasal trauma
Elaborate reduction and augmentation procedures
Marked tip deformities
The need for extra tip rotation
The correction of extreme overprojection
Situations where assessment of the exact pathology is difficult.

PRINCIPLES OF EXTERNAL RHINOPLASTY Conservation of the structural support of the nose by
exposing the pathology and allowing open access for
corrective surgical manoeuvres.
Correct incision placement and meticulous wound closure
are essential.
Lower and upper lateral cartilages together with the bony
dorsum can be exposed to the nasofrontal angle in their
undisturbed positions.
By dividing the upper laterals from the quadrilateral
cartilage, the whole of the septum is accessible from the
cephalic as well as the caudal aspect.
Other benefits include
Binocular vision
Use of both hands
Control of bleeding with diathermy
Precise placement and suturing of struts, Battens and shield
grafts
A very useful teaching tool.
It is important to appreciate that whilst the major tip support
mechanisms are respected in the external approach, the
disruption of the skin soft tissue envelope from the lower
lateral cartilages and the division of the medial intercrural
ligamentous fibrous tissue leads to loss of some of the minor
tip support mechanisms, and therefore some tip ptosis should
be anticipated in all cases.

SURGICAL TECHNIQUE
Incisions
The broken trans columellar incision is most commonly
used and variations include the step, gullwing and inverted
'V' configurations.
The mid-columella incision should be situated above the
level of the medial crural footplates to ensure adequate
support, thus preventing a depressed scar
The vertical columellar parts of the marginal incisions are
then placed 1.5-2 mm inside the vestibule and joined by
careful undermining with scissors of the columella skin.

SURGICAL TECHNIQUE
Dissection of the soft tissue envelope
This starts in the subperichondrial plane in the domal area.
It can be helpful to vertically incise the perichondrium at
the caudal end of the cartilaginous vault in the midline, after
which subperichondrial dissection can proceed from medial
to lateral and in a cephalic direction.
Dissection of the soft tissue of the bony pyramid in a
subperiosteal plane should start 2-3 mm parallel to and above
the caudal end of both nasal bones.
In the case of grafting procedures for augmentation, care
should be taken that the overlying soft tissue has sufficient
viability.

SURGICAL TECHNIQUE
Blanching of the skin over an augmentation graft is a
warning sign which should not be neglected.
A slight reduction of the graft size will prevent
possible skin necrosis.
A Meticulous closure of incision is done following
completion of surgery.