bone replacement of fast-absorbing
TRANSCRIPT
Bone Replacement of Fast-AbsorbingBiocomposite Anchors in ArthroscopicShoulder Labral Repairs
Matthew D. Milewski,* MD, David R. Diduch,y MD, Joseph M. Hart,y ATC, PhD,Marc Tompkins,z MD, Shen-Ying Ma,y MD, and Cree M. Gaskin,y§|| MDInvestigation performed at the University of Virginia, Charlottesville, Virginia
Background: Newer generation biocomposite anchors are hypothesized to resorb more reliably and faster, while allowing forbone ingrowth and replacement.
Purpose: The purposes of this study were to (1) assess anchor resorption and bone ingrowth over time, (2) identify tunnel wid-ening or potential reactions to the implants, (3) compare imaging findings for different sites of labral repair, and (4) determinepatient subjective outcomes with the use of biocomposite anchors in glenoid labral repair.
Study Design: Case series; Level of evidence, 4.
Methods: We enrolled 22 patients to participate in a 24-month outcomes study that included subjective and objective outcomeassessments after glenoid labrum repair surgery. Magnetic resonance imaging (MRI) was performed at 6 and 12 months to iden-tify any potential reactions to implants. Computed tomography (CT) scans were performed at 12 and 24 months to determineanchor resorption and bone ingrowth. Sixteen patients and 47 anchors were available for follow-up at 24 months. An indepen-dent, fellowship-trained musculoskeletal radiologist read the scans. Subjective outcome scores measured at 24 months post-operatively included Simple Shoulder Test, Tegner activity scale, American Shoulder and Elbow Surgeons (ASES), andUniversity of California, Los Angeles (UCLA) shoulder scores.
Results: No adverse events were reported with the use of biocomposite anchors at the end of the study period. At 12 and 24months, respectively, CT scans demonstrated that an estimated 68% and 98% of combined anchor material had been absorbed,56% and 78% of the anchor material had been replaced by soft tissue of variable density, and 9% and 20% of total anchor vol-ume was replaced by bone. No obvious mechanical failure of the labral repairs was detected on nonarthrogram MRI. Three of the47 anchors showed bone cyst formation. Tunnel widening (expansion beyond tunnel diameter of 3 mm; 2.9-mm drill hole utilized)was seen in 55% of the anchors but decreased between 12 and 24 months, consistent with bone replacement. Tunnel wideningwas seen more in anteroinferior and posterior glenoid anchor locations (84% and 57%, respectively) than in superior labral an-chors (13%). Subjective outcome scores at 24 months for ASES and UCLA shoulder scores averaged 88 and 30, respectively. Allbut one patient were satisfied with their outcome at 24 months.
Conclusion: Our imaging evaluation indicates resorption of newer generation biocomposite anchors with progressive bonereplacement at 12 and 24 months while maintaining acceptable subjective outcomes.
Keywords: biocomposite; suture anchor; labral repair; shoulder; arthroscopy
The use of suture anchors for soft tissue to bone fixationhas facilitated the movement from open surgery to arthro-scopic techniques for a variety of glenohumeral conditionsincluding Bankart and superior labrum anterior posterior(SLAP) lesion repairs.16,25,27 Success of these arthroscopicprocedures depends on multiple factors including tissuequality, patient selection, and compliance with postopera-tive rehabilitation.26,38 Technique and technology-relatedfactors including anchor and suture material, knot secu-rity, anchor geometry, and anchor biomechanics also playa role.11,12,25,37 The first-generation suture anchors weremetallic devices that provided excellent fixation but wereassociated with failures including loosening and breakagethat led to chondral damage.{ Metallic artifact also
||Address correspondence to Cree M. Gaskin, MD, University of Vir-ginia Health System, Department of Radiology and Medical Imaging,PO Box 800170, Charlottesville, VA 22908 (e-mail: [email protected]).
*Elite Sports Medicine / Connecticut Children’s Medical Center;Farmington, Connecticut.
yDepartment of Orthopaedic Surgery, University of Virginia, Charlot-tesville, Virginia.
zDepartment of Orthopaedics, University of Minnesota, Minneapolis,Minnesota.
§Department of Radiology and Medical Imaging, University of Virginia,Charlottesville, Virginia.
One or more of the authors has declared the following potential con-flict of interest or source of funding: Dr Gaskin is a consultant for DePuyMitek. This study was funded, in part, by a research grant from DePuyMitek.
The American Journal of Sports Medicine, Vol. XX, No. XDOI: 10.1177/0363546512441589� 2012 The Author(s) {References 4, 6, 10, 11, 13, 19, 30, 39.
1
AJSM PreView, published on April 20, 2012 as doi:10.1177/0363546512441589

distorted postoperative imaging by computed tomography(CT) and magnetic resonance imaging (MRI) in revisionscenarios.29 Bioabsorbable alternatives were thereforedeveloped to help address some of the disadvantages ofmetallic anchors while providing appropriate soft tissuefixation.2,9,24
Speer and Warren31 described 4 criteria for bioabsorbableimplants in the shoulder: (1) the bioabsorbable implant musthave adequate initial fixation strength to coapt the soft tis-sues to bone, (2) the implant’s bioabsorption profile mustenable it to retain satisfactory strength while the healing tis-sues are regaining mechanical integrity, (3) the implantmust not bioabsorb too slowly or it will behave like its metalcounterpart with breakage and migration, and (4) theimplant must be made of materials that are completelysafe: no toxicity, antigenicity, pyrogenicity, or carcinogeni-city. One might consider adding a fifth criterion to Speerand Warren’s criteria31 for bioabsorbable implants in theshoulder: bioabsorbable implant replacement by bone.
Biocomposite anchors, which combine biodegradable co-polymer and poly(lactic-co-glycolic acid) (PLGA) osteoconduc-tive bioceramics such as b-tricalcium phosphate (TCP) orhydroxyapatite, were developed to help bridge the gapbetween adequate initial fixation and eventual bone replace-ment without osteolysis or synovitis.21 We sought to investi-gate one such biocomposite, Biocryl Rapide (BR) (DePuyMitek, Raynham, Massachusetts), which is used in 2 differentlabral suture anchors, the Lupine BR anchor (DePuy Mitek)and the Bioknotless BR anchor (DePuy Mitek).
We hypothesized that patients undergoing glenoid labralrepair with these new biocomposite anchors would demon-strate radiographic evidence of labral healing with progres-sive anchor resorption and replacement by bone whilemaintaining good clinical outcomes based on subjective out-come scores and minimizing adverse reactions such asintra-articular inflammatory response and cyst formation.
MATERIALS AND METHODS
This longitudinal case series involving patients who hadundergone shoulder arthroscopy and labral repair by 3senior surgeons at our academic sports medicine centerwas approved by our institutional review board. Inclusioncriteria were patients between 18 and 60 years of agewho underwent arthroscopic capsulolabral repair usinganchors composed of this particular biocomposite andwho were willing to undergo postoperative MRI and CTat the established time points. Anchors used included theLupine BR anchor and the Bioknotless BR anchor. Bothanchors were included in this study, focusing on anchorbioabsorption and bioreplacement, because they have iden-tical body types by both geometry and composition. Theyboth have suture loops and differ only in that one is knot-less and the other allows suture tying of a suture attachedto the suture loop. Biocryl Rapide is made of 70% PLGAand 30% TCP.
Exclusion criteria were previous shoulder surgery; chronicor acute medical illness that may interfere with healing, suchas a neurological, collagenous, or circulatory disease; existing
pathological conditions or degenerative joint diseases includ-ing rheumatoid arthritis, extensive osteoarthritis, or otherprogressive collagen or bone conditions that would hinderadequate anatomic visualization and prevent secure tissuefixation; and women who were pregnant or lactating orplanned to become pregnant during the study. Sixteenpatients and 47 anchors were available for follow-up at 24months. Enrollment and follow-up flow are shown in Figure 1.
Computed tomography was performed without intrave-nous or intra-articular contrast at 12 6 1 months and 24 6
1 months utilizing multidetector CT scanners from GEMedical Systems (Lightspeed 16, Lightspeed Pro 32, orLightspeed VCT 64, Little Chalfont, United Kingdom).Patients were scanned with a 0.625-mm detector configu-ration, with bone and soft tissue algorithms utilizing140 kV and automatic mAs. Images were constructed pro-spectively at 0.625 mm with 50% slice overlap. These directaxial images were reviewed together with multiplanarreformats at the radiologist’s workstation.
Magnetic resonance imaging was performed withoutintravenous or intra-articular contrast at 6 6 1 monthsand 12 6 1 months utilizing a 1.5-T scanner from SiemensMedical Systems (Avanto, Erlangen, Germany). A dedi-cated shoulder coil was utilized. Scan protocol includedaxial, oblique coronal, and oblique sagittal conventionalspin echo T1 (repetition time [TR]/echo time [TE] =625/16 msec); axial and oblique sagittal turbo inversionrecovery (TR/TE = 6350/25; inversion time = 160 msec);and oblique coronal dual echo fast spin echo T2 and protondensity with fat saturation (TR/TE = 4130/102 and 4130/37).A matrix of 512 3 512 was utilized.
Radiographic outcomes were based on postoperativeMRI scans obtained at 6 and 12 months to identify anypotential reactions to the implants and CT scans obtained
12 month MRI n=3 12 month CT scans n=3
6 month MRI scans: n=19
Initial Enrollment
12 month MRI scans: n=17 12 month CT scans: n=17
Lost to follow-up
n=2 Supplemental Enrollment
Lost to follow-up
n=4 24 month CT scans: n=13
24 month Evaluations: n=13
Lost to follow-up
n=024 month CT scans: n=3
24 month Evaluations: n=3
Total 6 month MRI scans: N=19 Total 12 month MRI scans: N=20 Total 12 month CT scans: N=20 Total 24 month CT scans: N=16 Total 24 month Evaluations: N=16
Serial assessments:Total 6+12+24 month scans on same patients: N=13Total 6+12 month MRI: N=17 Total 12+24 month CT scans: N=16
Figure 1. CONSORT flowchart for study enrollment andfollow-up.
2 Milewski et al The American Journal of Sports Medicine

at 12 and 24 months to determine anchor resorption andbone ingrowth. An independent and fellowship-trainedmusculoskeletal radiologist with over 10 years of experi-ence (C.M.G.) reviewed all scans. Nonarthrogram MRIscans were examined for adequacy and integrity of labralrepair and to assess in vivo biological safety based on thepresence or absence of undesirable host responses includ-ing joint effusion, synovitis, solid mass from foreign bodyreaction, lymphadenopathy, edema, and/or cyst formation.The CT scans were examined to determine anchor resorp-tion, replacement by bone or soft tissue density, intraoss-eous cyst formation, and anchor tunnel widening.
Data Analysis
A picture archiving and communication system (PACS) wasused for digital image review. Digital tools imbedded in ourPACS (version 10.2, Carestream, Rochester, New York)were used to standardize measurements across patientsand scan dates. Specifically, we measured tunnel diameter,cyst size (if present), and density of the tissue replacing theanchors to support the determination of bone versus softtissue bioreplacement at each time point. Because of thesmall size and complicated geometry of the anchors, preciseassessment or quantification of percentage of anchor resorp-tion was not possible. The radiologist estimated the percent-age of resorption by comparing the anchors acrossexaminations over 24 months and by referencing theappearance of new (not yet absorbed) anchors. A similarprocess was used for estimating quantity of anchor replace-ment by bone or soft tissue density. Precise measurementswere again not possible, so the radiologist estimated the por-tion of the anchor replaced. Although this technique of esti-mation has limitations, it was considered satisfactory tocapture a general trend of progressive resorption.
To determine whether the tissue replacing the anchor wasbone or soft tissue, a semiquantitative or partially subjectiveapproach was employed. For the tissue replacing the anchorto be considered as bone, it required 2 criteria to be met:(1) the radiologist’s subjective interpretation of the densityand texture of the tissue needed to be consistent with bone,and (2) the tissue density as objectively measured must besimilar to that of bone in Hounsfield units (HU). The use ofHU measurements to confirm bone replacement of bioabsorb-able implants has been reported previously with interferencescrews.7,8 The HU scale is based on linear attenuation coeffi-cients and is a scale of relative radiodensity where, by defini-tion, the radiodensity of distilled water under standardpressure and temperature is 0 HU and the radiodensity ofair is –1000 HU. Typical HU measurements from the humanbody are as follows: –120 for fat, 0 to 10 for simple fluid, 40for muscle, over 150 for light trabecular bone, and 1000 forcortical bone. The HU measurements were taken from thetissue replacing the absorbed anchors, and these measure-ments were considered additional support for the subjectivedetermination of whether a resorbed anchor had beenreplaced by bone or soft tissue.
The MRI scans were reviewed for labral repair integrity,with an intact repair defined as the experienced musculoskel-etal radiologist’s subjective interpretation along with objective
criteria of labral tissue found in situ without linear increasedsignal undercutting or coursing through it. Repair failure orlabral retear was defined as displaced labral tissue or insitu labral tissue with linear high signal undercutting orcoursing through it. Indeterminate labrum was defined asnot being able to fit the definitions of intact or torn mentionedabove. Reasons for lack of clarity included patient motion andpostoperative related artifacts such as subtle signal changesthat were ambiguous for subtle retear versus normal postop-erative changes of repaired tear. The authors emphasize,however, that the primary imaging objective was focused onthe biological behavior of the implant with regard to biore-sorption, host response, and bioreplacement.
Tunnel widening was defined as 3 mm or greater inmaximal cross-sectional diameter obtained orthogonal tothe long axis of the tunnel. This definition was based onthe geometry or size of the anchors and the pilot hole.The anchors were 3 mm wide over much of their lengthbut varied from 2 mm (at deep tip) to 4 mm (near joint sur-face) in width. The drill holes had a diameter of 2.9 mm forboth types of BR anchors as they had identical body types.
The radiologist was not specifically blinded to the timeinterval between surgery and scanning. The studies wereread in 4 batches at different time points in the study,and generally, the 6- and 12-month scans appeared inthe first and second groups, and 24-month scans appearedin the third and fourth groups.
Follow-up clinical data included history and physicalexamination as well as patient demographics. Subjectiveoutcome measures were recorded at 24 months postopera-tively, which included Tegner activity scale, Simple Shoul-der Test, American Shoulder and Elbow Surgeons (ASES),and University of California, Los Angeles (UCLA) shoulderscores.
Statistical Analyses
Percentage of resorption and percentage of replacement bybone were compared among the 3 anchor locations (ante-rior, posterior, and superior) at the 12- and 24-monthtime points with a univariate analysis of variance(ANOVA). Tukey least significant difference was used forpost hoc analyses. A test was considered statistically sig-nificant if the P value was .05 or less. The data involvingthe percentage of anchor resorption, percentage of anchorreplaced by bone, and the comparisons of these variablesbetween anchors of different locations were not normallydistributed. Kruskal-Wallis nonparametric analysis wasalso completed and reported along with median values.Both parametric and nonparametric analyses includingmean and median values were reported as the parametricanalysis and mean values may be easier to interpret bothscientifically and clinically.
RESULTS
A total of 22 patients were enrolled in our study, with 16patients completing the clinical assessment, subjective out-comes, and follow-up imaging at 24 months. Enrollment
Vol. XX, No. X, XXXX Biocomposite Anchors in Arthroscopic Shoulder Labral Repairs 3

and follow-up flow are delineated in Figure 1. There was73% patient follow-up at 24 months, with 6 patients havingwithdrawn from the study or lost to follow-up. Threepatients were enrolled in a period of additional enrollmentafter 2 patients were lost during early enrollment aftertheir 6-month follow-up scans. Four patients completedMRI and CT scans at 12 months but were lost to follow-up before 24 months. There were 11 male and 5 femalepatients in our cohort, with a mean age of 35 years andan age range of 18 to 60 years. A total of 48 BR anchors,all composed of the same material, were utilized in these16 patients’ labral repairs. One of these anchors couldnot be evaluated on 24-month CT as it was obscured byrevision surgery that occurred between the 12- and 24-month scans, leaving 47 anchors for 24-month analysisby imaging. A total of 32 Bioknotless BR anchors and 16Lupine BR anchors were utilized with an average of 3.0suture anchors used per patient. Anchor type and numberutilized per patient were based on the surgeon’s prefer-ence. Of the 47 anchors available for 24-month analysis,25 anchors were placed for anteroinferior labral repairs(19 Bioknotless BR and 6 Lupine BR anchors), 15 anchorswere placed for superior labral repairs (8 Bioknotless BRand 7 Lupine BR anchors), and 7 anchors were placed forposterior labral repairs (4 Bioknotless BR and 3 LupineBR anchors).
Thirteen of 16 patients (81%) underwent their MRIexaminations at 6 months, and 15 of 16 patients (94%)completed their MRI examinations at 12 months. All 16patients completed their CT scans at 12 months and 24
months along with their clinical examinations at 24months.
The MRI scans performed at 12 months confirmed all 15patients had no signs of effusion, synovitis, lymphadenopa-thy, intra-articular masses, or soft tissue edema (Figure 2).When assessed for labral integrity, 11 of 15 patients’ labralrepairs were deemed intact at the 12-month MRI examina-tion. Three of the 15 labral repairs were deemed ‘‘indetermi-nate’’ at the 12-month MRI examination. One of the 15labral repairs was deemed ‘‘indeterminate’’ at 6 monthsand was shown subsequently to be retorn intraoperativelyat 8 months.
The CT scan assessments at 12 and 24 months were usedto assess resorption of BR anchor material (Figures 3 and 4).At 12-month follow-up, an estimated average of 68% 6 25%resorption of BR anchor material was observed across the 47anchors in 16 patients (median value of 70% resorption at12 months). At 24-month follow-up, an estimated averageof 98% 6 10% resorption of BR anchor material wasobserved, with 45 of 47 anchors having 100% resorption(median value of 100% resorption at 24 months).
In terms of bone ingrowth, an estimated average of 9% oftotal BR anchor material across all anchors was replaced bybone at 12-month follow-up (median value of 0%) as deter-mined from CT (mean, 423 HU; range, 250-800 HU). Elevenof the 47 BR anchors (23%) exhibited replacement by bone,and within this group of 11 anchors, an estimated averageof 39% 6 20% of BR anchor material was replaced bybone. At 24 months, total bone replacement of anchorshad increased to an estimated average of 20% of the BR
Figure 2. Six-month postoperative axial inversion recovery magnetic resonance imaging (MRI) scan (A) and axial T1 MRI scan(B) of a posterior labral repair utilizing a Lupine BR anchor (DePuy Mitek, Raynham, Massachusetts). Linear signal changesare seen at the site of the anchor (long, thin white arrows) without adjacent bone or soft tissue changes. Twelve-month post-operative axial inversion recovery MRI scan (C) and axial T1 MRI scan (D) show the anchor and tunnel (short, thick white arrows)to be less perceptible over time. Axial and oblique sagittal reformat computed tomography images at 12 months (long, thin blackarrows) and 24 months (short, thick black arrows) postoperatively (E-H) show progressive bone replacement and less obvioustunnel visualization in the midposterior labrum.
4 Milewski et al The American Journal of Sports Medicine

anchor material (median value of 0%). Twenty-two of the 47BR anchors (47%) exhibited some replacement by bone at 24months, and within this group of 22 anchors, bone replace-ment averaged 42% 6 26%.
At 12-month CT scan evaluation, an estimated 56% ofBR anchor material in the 48 anchors was replaced bysoft tissue density (mean, 65 HU; range, 25-120 HU), andthis increased to 78% of BR anchor material in the 47anchors at 24-month follow-up. The progression of percent-age of anchor resorption and percentage of bone replace-ment for anteriorly, posteriorly, and superiorly placedanchors from 12-month and 24-month CT scan evaluationsare shown in Figure 5.
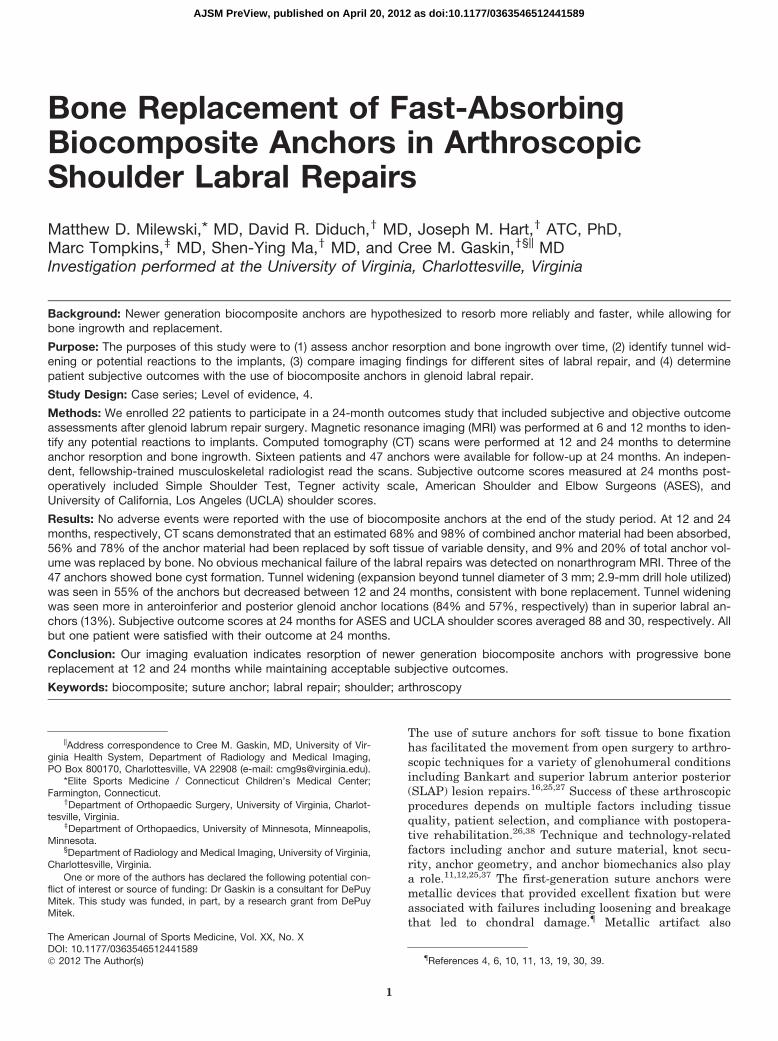
Our primary imaging focus was on overall anchor behav-ior, and thus, we did not specifically power the study to per-form subgroup analysis by anchor location or patient age;however, we did perform such analyses to contribute toour observations. Percentage of resorption was significantlydifferent among anchor locations at 12 months but not at 24months after implantation (Figure 6). Specifically, at 12months, the posterior anchors had a significantly higherpercentage of resorption than the superior (P = .03) andanterior (P = .01) anchors. The percentage of resorptionwas not different between the anterior and superior anchors(P = .72). Percentage of replacement by bone was also signif-icantly different among the anchor locations at both 12months and 24 months after implantation (Figure 6). Theaverage percentage of replacement by bone was highestfor the superior anchors at 12 and 24 months. Percentageof replacement by bone was significantly higher in the supe-rior anchors compared with the anterior anchors at 12months (P = .002) and 24 months (P = .01) after implanta-tion but not significantly higher than the posterior anchors.Kruskal-Wallis nonparametric analysis revealed a signifi-cantly greater percentage of resorption of posterior anchorsat 12 months compared with anterior anchors (P = .04) anda significantly greater percentage of replacement by bone ofsuperior anchors at 12 months compared with anterior
anchors (P = .01). Kruskal-Wallis nonparametric analysisdid not reveal significant differences in percentage of anchorresorption and percentage of replacement by bone betweenanchor locations at 24 months (P = .41 and P = .07, respec-tively). Correlations were done to compare age and percent-age of resorption and percentage of replacement by bone. At12 months, age was related to percentage of resorption (r =.30, P = .04) and percentage of replacement by bone (r =–.04, P = .005), but these correlations were not significantat 24 months (percentage of resorption: r = .15, P = .31; per-centage of replacement by bone: r = .19, P = .19).
Bone cysts that communicated with the BR anchor tun-nel were associated with 3 of the 47 BR anchors (6%). All 3cysts were seen in anchors used for superior labral repair(2 Bioknotless BR and 1 Lupine BR anchors). One wasa small cyst (\5 mm in diameter) at the deep aspect ofthe tunnel that developed between 12- and 24-monthfollow-up CT scans even though the associated tunneldecreased in size during that time period (Figure 4). Thesecond cyst was a 5-mm cyst present at 12-month follow-up that enlarged to 8 mm at 24-month follow-up. This
Figure 3. Twelve- and 24-month postoperative axial com-puted tomography images (A, B) of a superior labral repairutilizing 2 Bioknotless BR anchors (DePuy Mitek, Raynham,Massachusetts). Both anchor sites show interval anchorresorption, tunnel width narrowing, and replacement bybone between 12 months (black arrows) and 24 months(white arrows).
Figure 4. Twelve-month postoperative axial (A) and obliquesagittal reformat (B) computed tomography (CT) images ofan anteroinferior labral repair utilizing Bioknotless BR anchors(DePuy Mitek, Raynham, Massachusetts). An enlarged cysticcavity in the anterior glenoid is visualized surroundinga vaguely linear calcific density thought to reflect partiallyresorbed anchor material (black arrows). The oblique sagittalreformat CT image (B) also shows a portion of a smaller tunnelfrom another anchor (black arrowhead). Twenty-four-monthpostoperative axial (C) and oblique sagittal reformat (D) CTimages show an interval decrease in the size of the cavity(white arrows) with complete resorption of the anchor and par-tial bone replacement. The oblique sagittal reformat image(D) shows a more modest interval decrease in size of the tun-nel from the other anchor (white arrowhead).
Vol. XX, No. X, XXXX Biocomposite Anchors in Arthroscopic Shoulder Labral Repairs 5

patient also had some degree of glenohumeral osteoarthri-tis (although still within inclusion criteria), which wasa confounding factor. The third cyst was 4 mm in sizeand located at the deep aspect of the tunnel. It was presenton the 12-month CT scan, but it remained stable at 24-month follow-up.
Tunnel widening, as defined as maximal tunnel widthgreater than 3.0 mm, was associated with 26 of the 47BR anchors (55%). The average diameter of the widenedtunnels was 4.4 mm at 12 months (range, 3.25-6.0 mm),and this decreased to an average of 3.9 mm at 24 months(range, 3.0-5.0 mm). Widening affected 2 of the 15 superiorlabral BR anchors (13%) (1 Bioknotless BR and 1 LupineBR anchor). Widening affected 4 of the 7 posterior labralBR anchors (57%) (1 Bioknotless BR and 3 Lupine BRanchors). Widening affected 21 of the 25 anteroinferior lab-ral BR anchors (84%) (14 Bioknotless BR and 7 Lupine BRanchors).
Subjective outcome and clinical assessment data werecollected on 16 patients at a minimum of 24-month follow-up. Clinical data were not available on the 6 patients lost
to follow-up because this was collected only at 24-monthfollow-up. All but one patient were satisfied with their out-come at 24 months (15/16 patients, 94%). One patientsustained a repeat dislocation event at 8 months postopera-tively and required a revision surgery. This patient was sat-isfied with their outcome at most recent follow-up. TheASES scores at most recent follow-up averaged 88 6 20.The UCLA shoulder scores at most recent follow-up aver-aged 30 6 6.7. Visual analog scale scores at most recentfollow-up averaged 1.5 6 1.8. Simple Shoulder Test scoresat most recent follow-up averaged 10 6 3.3 of a possible12. Tegner activity scale scores preoperatively averaged6.4 6 2.5 and postoperatively averaged 5.0 6 2.8.
Our primary focus was on the patients who completedthe 24-month clinical and imaging follow-up. However,we did evaluate the 6- and 12-month imaging of thosepatients who were lost to follow-up. For the sake of com-plete reporting, we are providing a brief summary of datafrom this group. These data are presented separatelyfrom the data of the patients who completed the studybecause patients dropped out at varying time points.
Figure 5. Top row graphs showing percentage of anchor resorption between 12 and 24 months (12-24M % Resorption) by com-puted tomography (CT) scan evaluations for each superior, posterior, and anterior anchor. Bottom row graphs showing percent-age of anchor replacement by bone between 12 and 24 months (12-24M % Bone) by CT scan evaluations for each superior,posterior, and anterior anchor.
6 Milewski et al The American Journal of Sports Medicine
Overall, this small group demonstrated similar results tothose who completed the study. The 6 patients lost to fol-low-up had 19 anchors placed. One of these 6 patientscould not be evaluated by MRI because of artifact froma nearby metal foreign body. Fifteen anchors in 5 patientswere evaluated by MRI at 6 months, and 10 anchors in 3patients were evaluated by MRI at 12 months. The find-ings from the studies were negative for joint effusion,edema, lymphadenopathy, soft tissue mass, or fluid collec-tion. Only one anchor of 15 (7%) was associated with cystformation, and this 4-mm intraosseous cyst was stablebetween 6 and 12 months. The repairs appeared intact in3 of 5 patients. The integrity of repair was uncertain in 2patients, although there was no overt evidence of failureor retear in this group. Fourteen anchors in 4 patientswere evaluated by CT at 12 months. Six of 14 anchors(43%) showed no evidence of tunnel widening, while 8 of14 anchors (57%) were associated with tunnel widening(mean, 4.3 mm; range, 3.6-4.6 mm). At 12-month CT, anoverall estimated 84% of anchor material was resorbedand replaced by bone (9% of anchor material) and soft tis-sue (75% of anchor material).
DISCUSSION
Bioabsorbable suture anchors are rapidly evolving andsupplanting metallic anchors in arthroscopic shoulder
surgery. These anchors offer some distinct advantagesfrom their metallic counterparts, particularly in cases offailed tissue repairs. During revision cases, the need toremove permanent implants is also avoided with biode-gradable implants because they can often be drilled outor through.
Bioabsorbable anchors also improve the quality of post-operative imaging relative to metallic anchors. Bioabsorb-able anchors cause less beam-hardening artifact on CTscans, and more importantly, they minimize distortion onpostoperative MRI, which is often the study of choice toevaluate the status of the repair.
In spite of these advantages, earlier generation bioab-sorbable anchors have generated causes for concern. Multi-ple different types and combinations of polymers have beendeveloped and utilized for anchors including polyglycolicacid (PGA), poly-L-lactic acid (PLLA), and poly-D-L-lacticacid copolymer polyglycolic acid (PDLLA-co-PGA). Earlybioabsorbable anchors and fixation devices such as theSuretac (Smith & Nephew, Andover, Massachusetts) weremade of a synthetic copolymer of 67.5% polyglyconic acidand 32.5% trimethylene carbonate.31 However, the degrada-tion time reported with the PGA anchors was only 3 to 4months, and they were associated with early loss of fixation,osteolysis, loose body formation, and glenohumeral synovi-tis.10,31,32 The PLLA anchors were developed to have a lon-ger degradation time, between 10 and 30 months, butconcerns were raised as to whether this was an excessively
Figure 6. A, Percentage of anchor resorption by anchor location (superior, posterior, and anterior). Percentage of resorption washighest in the posterior anchors at 12 months after implantation. B, Percentage of replacement by bone was highest for the supe-rior anchors at 12 and 24 months after implantation.
Vol. XX, No. X, XXXX Biocomposite Anchors in Arthroscopic Shoulder Labral Repairs 7

long degradation time, which may result in similar prob-lems as metallic anchors with chondral damage from loosen-ing as well as the fact that the anchors might not bereplaced by bone.4,6,22,23,36 The PLLA tack anchors havebeen shown to have more radiographic evidence of persis-tent drill holes at 7-year follow-up than PGA tack anchors.14
Also, there have been concerns raised over intra-articularinflammatory response and cyst formation with PLLAanchors.21,22,29,31 In one study, 55% of patients who hadanterior labral repairs with 3 polylactic acid (PLA) anchors(Panalok, Mitek Ethicon, Somerville, New Jersey) showedanchor tunnel enlargement greater than the mean plusone standard deviation.34
The literature has also documented some unique com-plications associated with use of bioabsorbable anchors.Several case reports have identified a hyperinflammatoryresponse to bioabsorbable anchors, leading to synovitis,bone osteolysis, cartilage damage, and adverse clinical out-comes.# These complications have been associated withboth PGA and PLLA implants alike, contributing to theimpetus to develop better implant materials.
Biocomposite anchors are composed of newer generationmaterials with potential for improved performance overearlier generation anchors. Biocomposites include a mix-ture of biodegradable material, such as PLGA or PLA,and osteoconductive bioceramics, such as TCP. BiocrylRapide (DePuy Mitek) is a composite between fast-absorbing PLGA (70%) and osteoconductive TCP (30%).The proposed advantages of the new material includemore timely and reliable resorption of the anchor with sub-sequent replacement by bone at the site of the anchor.Anchor resorption with bone replacement was hypothe-sized to occur by 24 months. While cadaveric experimentshave demonstrated similar load-to-failure propertiesbetween biodegradable anchors and more traditionalanchor materials, concern is still raised as to whether sim-ilar results can be found in vivo.5 While suture anchorsmade of newer generation biocomposite materials such asBiocryl Rapide have found increasing utility in shoulderarthroscopy, concern remains about the long-term effectsthese materials have in the glenohumeral joint includingthe effects that material resorption may have on repairintegrity and cyst formation and whether the material orits resorption may induce an inflammatory responsewithin the glenohumeral joint that could lead to synovitis.Also, there are little data in the literature regarding thepotential for bone replacement or remodeling as the bio-composite material is resorbed.
We believe this is the first clinical study with 24-monthfollow-up that radiographically demonstrates the extent ofbone replacement of biocomposite labral anchors. Barberand Dockery7 have previously shown bone replacement ofTCP PLLA interference screws. On 24-month follow-upwith CT scans, our anchors appear to be largely resorbedwith some progressive replacement by bone. The replace-ment of the rest of the anchor material by tissue not consti-tuting bone was called ‘‘soft tissue density’’ because it
matched the density of noncalcified, nonfatty soft tissueboth subjectively and by HU density measurements butwas otherwise nonspecific. Without tissue samples, theauthors do not know whether this ‘‘soft tissue density’’material represents immature osteoid, giant cell reaction,fibrous tissue, or granulation tissue. Further long-termstudies will be needed to determine whether this materialcontinues to ossify.
Tunnel widening was seen in 55% of the anchors, butthis actually decreased between the 12- and 24-monthfollow-up CT scans. The tunnel widening was not associ-ated with clinical failures in this group and, as mentioned,tunnel widening decreased as the anchors were resorbedand partially replaced by bone. Tunnel widening is likelymultifactorial and may relate to implant material, implantgeometry and biomechanics, surgical technique, and gle-noid location. The anchors used in this study were com-posed of Biocryl Rapide but were also of a specific designand geometry. Both anchors (Lupine BR anchor [DePuyMitek] and Bioknotless BR anchor [DePuy Mitek]) usedin this study have similar anchor body geometry, withthe Lupine BR anchor having a suture attached to itssuture loop for tying. These anchors can be described asa toggle type of anchor and are triangular in shape, relyingin part on subcortical fixation with potential for spacearound the distal aspect of the anchor within the drillhole. We hypothesize that micromotion around the anchorcould occur during shoulder motion and result in pumpingof joint fluid in and around the anchor. Thus, anchordesign may also contribute to tunnel widening and cyst for-mation. Changes in subsequent anchor designs and geom-etry, such as with a cylindrical anchor that completely fillsthe bone hole, may address these concerns. Tunnel widen-ing was seen more in anteroinferior and posterior glenoidanchor locations (84% and 57%, respectively) but wasonly seen in 13% of the superior labral anchors. Identicalanchors examined at identical time points, while only dif-fering in anchor position and having different wideningpatterns, would support the idea that tunnel widening islikely related to the forces across these anchors in situ atdifferent areas of the labrum.
Cyst formation reported with earlier generation bioab-sorbable anchors has generated concern. We documented3 cysts in our study or 6% of all anchors used. All 3 cystswere seen with anchors used for superior labral repairs(2 Bioknotless BR anchors and 1 Lupine BR anchor).None of these 3 cysts were associated with anchor failure,but rather they were associated with excellent clinical out-comes. While cyst formation with these new biocompositeanchors remains a concern, there have been few investiga-tional studies documenting the clinical results of gleno-humeral surgery utilizing this new generation ofmaterial.7 Previous reports of cyst formation with PGAand PLLA were usually associated with bioabsorbablescrews used for interference screw fixation in anterior cru-ciate ligament reconstruction.18 Given the paucity of datawithin the literature on biocomposite anchors, concerntherefore remains about the long-term performance ofthese materials in the glenohumeral joint including theeffects of material resorption on repair integrity and cyst#References 1, 3, 15, 17, 20, 23, 25, 28, 33-35.
8 Milewski et al The American Journal of Sports Medicine

formation and whether the material or its resorption mayinduce an inflammatory response within the glenohumeraljoint.
The strengths of this prospective study include the min-imum 24-month follow-up including both CT and MRIevaluations. In addition to the imaging findings, the BRanchors were associated with good clinical outcomes, asshown by ASES, UCLA shoulder, and Simple ShoulderTest scores, with only one unsatisfied patient and onerepeat dislocation. We also had a broad age range ofpatients and anchor location. We believe that a diversepatient population including age range and anchor locationbetter characterizes the overall resorption profile of theimplant rather than a narrow patient population and loca-tion. This allows us to make more broad and generalizedconclusions.
Weaknesses of this study include the lack of a controlgroup by which to compare these anchors directly. A con-trol group would have required the use of another type ofanchor, which would have likely meant differences inboth anchor composition along with anchor geometry andsuture type. Subjective data were obtained in follow-upbut were not obtained preoperatively, which can limit theconclusions drawn from the study in terms of subjectiveimprovement. We were not able to precisely quantify vol-ume of anchor resorption or replacement because of smallanchor size and complex geometry, so we sought estima-tions, which introduced some intrinsic bias. In addition,we had a single fellowship-trained musculoskeletal radiol-ogist read all of the scans, but he was not blinded to thetime points. While a single reader eliminates some vari-ability, it does introduce potential bias especially whenhe was not blinded to the time points of follow-up. Whilewe used a fairly wide age range of patients, we foundthat age was not correlated at 24 months with anchorresorption or bone replacement.
We had a 9% lost to follow-up rate at 12 months anda 27% lost to follow-up rate at 24 months. The cause behindthese rates is likely multifactorial. This study was carriedout at an academic institution that is a large tertiary refer-ral center attracting patients from several hours away.Because of logistical issues, many of these patients wereunable to return for each follow-up time point. In addition,many of these represent mobile patients, such as univer-sity students, who were no longer in the area at the timeof follow-up. Lastly, during our study, there was heavypublic and media scrutiny on radiation risk associatedwith CT, which may have affected patients’ willingnessto return for CT scans at 12 and 24 months after surgery.
In conclusion, this study documents good radiographicand subjective outcomes following labral repairs usinga biocomposite anchor. We believe this study is the firstto document bone replacement of absorbed anchor materialand the first to determine the progression of absorption ofnew-generation biocomposite anchors in humans. Compli-cations related to biocomposite anchor resorption, includ-ing cyst formation and tunnel widening, were mild andnot clinically important in this study. Cyst formation wasassociated with only a small percentage of anchors, and
the cysts were small in size. Tunnel widening was common,although mild, and improved during the time course ofradiographic follow-up as the anchors were resorbed andpartially replaced by bone. There was no evidence of syno-vitis or intra-articular mass formation with absorption ofthese anchors. Good clinical outcomes can be expectedusing these new biocomposite faster absorbing sutureanchors. The residual soft tissue density at the anchorsites at 2 years may contain nonmineralized osteoidmatrix, so there is theoretical potential for further boneformation in time. Longer term CT follow-up will beneeded to examine this potential for further progressionof bone replacement of the resorbed anchors beyond 2years.
ACKNOWLEDGMENT
The authors thank Christopher M. Kuenze, MA, ATC, forhis assistance in patient recruitment and data collection.
REFERENCES
1. Athwal GS, Shridharani SM, O’Driscoll SW. Osteolysis and arthropa-
thy of the shoulder after use of bioabsorbable knotless suture
anchors: a report of four cases. J Bone Joint Surg Am. 2006;88(8):
1840-1845.
2. Balch OK, Collier MA, DeBault LE, Johnson LL. Bioabsorbable suture
anchor (co-polymer 85/15 D,L lactide/glycolide) implanted in bone:
correlation of physical/mechanical properties, magnetic resonance
imaging, and histological response. Arthroscopy. 1999;15(7):691-
708.
3. Barber FA. Biodegradable shoulder anchors have unique modes of
failure. Arthroscopy. 2007;23(3):316-320.
4. Barber FA. Poly-D,L-lactide interference screws for anterior cruciate
ligament reconstruction. Arthroscopy. 2005;21(7):804-808.
5. Barber FA, Coons DA, Ruiz-Suarez M. Cyclic load testing and ulti-
mate failure strength of biodegradable glenoid anchors. Arthroscopy.
2008;24(2):224-228.
6. Barber FA, Deck MA. The in vivo histology of an absorbable suture
anchor: a preliminary report. Arthroscopy. 1995;11(1):77-81.
7. Barber FA, Dockery WD. Long-term absorption of beta-tricalcium
phosphate poly-L-lactic acid interference screws. Arthroscopy.
2008;24(4):441-447.
8. Barber FA, Dockery WD. Long-term absorption of poly-L-lactic acid
interference screws. Arthroscopy. 2006;22(8):820-826.
9. Barber FA, Snyder SJ, Abrams JS, Fanelli GC, Savoie FH 3rd. Arthro-
scopic Bankart reconstruction with a bioabsorbable anchor. J Shoul-
der Elbow Surg. 2003;12(6):535-538.
10. Burkart A, Imhoff AB, Roscher E. Foreign-body reaction to the bioab-
sorbable Suretac device. Arthroscopy. 2000;16(1):91-95.
11. Cole BJ, Provencher MT. Safety profile of bioabsorbable shoulder
anchors. Arthroscopy. 2007;23(8):912-913, author reply 913-914.
12. Diduch DR, Tadje JP, Ferguson RE Jr, Edlich RF. Modern concepts
in arthroscopic Bankart repair. J Long Term Eff Med Implants.
1999;9(4):377-393.
13. Ekelund A. Cartilage injuries in the shoulder joint caused by migration
of suture anchors or mini screw. J Shoulder Elbow Surg. 1998;
7(5):537-539.
14. Elmlund AO, Kartus J, Rostgard-Christensen L, Sernert N, Magnus-
son L, Ejerhed L. A 7-year prospective, randomized, clinical, and
radiographic study after arthroscopic Bankart reconstruction using
2 different types of absorbable tack. Am J Sports Med.
2009;37(10):1930-1937.
Vol. XX, No. X, XXXX Biocomposite Anchors in Arthroscopic Shoulder Labral Repairs 9

15. Freehill MQ, Harms DJ, Huber SM, Atlihan D, Buss DD. Poly-L-lactic
acid tack synovitis after arthroscopic stabilization of the shoulder.
Am J Sports Med. 2003;31(5):643-647.
16. Friel NA, Karas V, Slabaugh MA, Cole BJ. Outcomes of type II supe-
rior labrum, anterior to posterior (SLAP) repair: prospective evalua-
tion at a minimum two-year follow-up. J Shoulder Elbow Surg.
2010;19(6):859-867.
17. Glueck D, Wilson TC, Johnson DL. Extensive osteolysis after rotator
cuff repair with a bioabsorbable suture anchor: a case report. Am J
Sports Med. 2005;33(5):742-744.
18. Gonzalez-Lomas G, Cassilly RT, Remotti F, Levine WN. Is the etiol-
ogy of pretibial cyst formation after absorbable interference screw
use related to a foreign body reaction? Clin Orthop Relat Res.
2011;469(4):1082-1088.
19. Jeong JH, Shin SJ. Arthroscopic removal of proud metallic suture
anchors after Bankart repair. Arch Orthop Trauma Surg. 2009;
129(8):1109-1115.
20. Kelly JD 2nd. Disintegration of an absorbable rotator cuff anchor six
weeks after implantation. Arthroscopy. 2005;21(4):495-497.
21. LeGeros RZ. Properties of osteoconductive biomaterials: calcium
phosphates. Clin Orthop Relat Res. 2002;395:81-98.
22. McGuire DA, Barber FA, Elrod BF, Paulos LE. Bioabsorbable interfer-
ence screws for graft fixation in anterior cruciate ligament recon-
struction. Arthroscopy. 1999;15(5):463-473.
23. Muller M, Kaab MJ, Villiger C, Holzach P. Osteolysis after open
shoulder stabilization using a new bio-resorbable bone anchor: a pro-
spective, non-randomized clinical trial. Injury. 2002;33 Suppl 2:
B30-B36.
24. Nho SJ, Provencher MT, Seroyer ST, Romeo AA. Bioabsorbable
anchors in glenohumeral shoulder surgery. Arthroscopy. 2009;25(7):
788-793.
25. Park MJ, Hsu JE, Harper C, Sennett BJ, Huffman GR. Poly-L/D-lactic
acid anchors are associated with reoperation and failure of SLAP
repairs. Arthroscopy. 2011;27(10):1335-1340.
26. Poukalova M, Yakacki CM, Guldberg RE, et al. Pullout strength of
suture anchors: effect of mechanical properties of trabecular bone.
J Biomech. 2010;43(6):1138-1145.
27. Rhee YG, Lee DH, Lim CT. Unstable isolated SLAP lesion: clinical
presentation and outcome of arthroscopic fixation. Arthroscopy.
2005;21(9):1099.
28. Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-
L-lactic acid bioabsorbable tacks in patients after SLAP lesion sur-
gery. Arthroscopy. 2006;22(6):615-619.
29. Shellock FG, Mink JH, Curtin S, Friedman MJ. MR imaging and
metallic implants for anterior cruciate ligament reconstruction:
assessment of ferromagnetism and artifact. J Magn Reson Imaging.
1992;2(2):225-228.
30. Silver MD, Daigneault JP. Symptomatic interarticular migration of
glenoid suture anchors. Arthroscopy. 2000;16(1):102-105.
31. Speer KP, Warren RF. Arthroscopic shoulder stabilization: a role for
biodegradable materials. Clin Orthop Relat Res. 1993;291:67-74.
32. Speer KP, Warren RF, Pagnani M, Warner JJ. An arthroscopic tech-
nique for anterior stabilization of the shoulder with a bioabsorbable
tack. J Bone Joint Surg Am. 1996;78(12):1801-1807.
33. Spoliti M. Glenoid osteolysis after arthroscopic labrum repair with
a bioabsorbable suture anchor. Acta Orthop Belg. 2007;73(1):
107-110.
34. Take Y, Yoneda M, Hayashida K, Nakagawa S, Mizuno N. Enlarge-
ment of drill holes after use of a biodegradable suture anchor: quanti-
tative study on consecutive postoperative radiographs. Arthroscopy.
2008;24(3):251-257.
35. Takubo Y, Morihara T, Namura T, et al. Anchor hole enlargement
after arthroscopic Bankart repair using absorbable suture anchors:
a report of three cases. J Shoulder Elbow Surg. 2008;17(6):e16-e18.
36. Ticker JB, Lippe RJ, Barkin DE, Carroll MP. Infected suture anchors
in the shoulder. Arthroscopy. 1996;12(5):613-615.
37. Weber SC. Surgical management of the failed SLAP repair. Sports
Med Arthrosc. 2010;18(3):162-166.
38. Yakacki CM, Poukalova M, Guldberg RE, et al. The effect of the tra-
becular microstructure on the pullout strength of suture anchors.
J Biomech. 2010;43(10):1953-1959.
39. Zuckerman JD, Matsen FA 3rd. Complications about the glenohum-
eral joint related to the use of screws and staples. J Bone Joint Surg
Am. 1984;66(2):175-180.
For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav
10 Milewski et al The American Journal of Sports Medicine