borderline personality disorder: content and formai ... · borderline personality disorder: content...
TRANSCRIPT
Borderline Personality Disorder:Content and Formai Analysis of thè Rorschach
Franco Burla, Stefano Ferracuti, and Renato LazzariDepartment of Psyclriatn and Medicai Psychology,
Universi!}' of Rome "la Sapienza, "Rome, 7/a/v
Borderline disturbance is a controversial clinical and diagnostic entity.There are at least two ways of conceptualizing borderline psychopathol-ogy: clinical-descriptive and psychodynamic (Millon & Davis, 1996). Inthè former, thè condition is considered a specific pattern of personalityfunctioning characterized by instability of mood, interpersonal rela-tions, and self-image (AFA, 1987, 1994). In thè lattar, thè terni border-line psychopathology is used to describe a structural personality organi-zation basecl on primitive defense mechanisms. This type of psycholog-ical organizatioii can be founcl in various personality disorders sudi asschizotypal, paranoici, histrionic. antisocial, and narcissistic (Kernberg,1970). '
The Rorschach test has been recommended by Zalewski and Archer(1991) as a diagnostic instrument for assessmg borderline personalitydisorder, even ihough their review of findings identified some inconsis-tencies related to thè use of differeiit diagnostic criteria by differentauthors. Some dimensions of personality that characterize borderlinedisturbance can be formulateci from a psychopathological descriptivepoint of view and evaluatecl using Rorschach coment scales (De Vos,1952; Elizur, 1949; Enclicott, 1972; Fisher & Cleveland, 1958). Most fre-quenti}' used in this regard is thè Rorschach defense scale of Lerner(Lerner & Lerner, 1980), which identifies primitive clefenses such assplitting, devaluation, idealization, projective identification, and denial.
Research data suggest that primitive clefenses are employed more fre-quenti}1 by borderline patients than by neurotic and psychotic pcrsons,with thè exception of idealization (Lerner, Albert. & Walsh, 1987:Lerner & Lerner, 1980: Lerner, Sugarman. & Gaughran, 1981). Theseprimitive defense mechanisms also occur more commonly in borderline
149
patients than in patients with cluster C personality disturbances (Hilsen-roth, Hibbard, Nash, & Handler, 1993). Being able to distinguish border-line patients from patients with antisocial and narcissistic personalitydisorders is more controversial (Gacono, Meloy, & Berg, 1992; Hilsen-roth, et al., 1993).
Reality testing is another element of personality functioning that canbe evaluated through content analysis of thè Rorschach. Borderline pa-tients can be distinguished from normal controls and from neurotics bythè number of Confabulatici! and Fabulized Combinations responsesthey give (Edell, 1987). Some research data suggest that Fabulized Com-binations occur even more frequently in borderline Rorschach protocolsthan in thè records of schizophrenic patients (Singer & Larson, 1981;Yen, 1983).
The purpose of our study was to compare Rorschach characteristics ofborderline clisorder with characteristics found in neurotic and psychoticpatients. Both formai and content analyses of thè Rorschach data wereconducted.
Method
Sixty subjects who were referred to our service were selected during thèyears 1994-1995. These patients were diagnosed independently of ourRorschach evaluation and divided into three groups. A group of 20borderline patients (7 males and 13 females, mean age 30.5 + 2.6 years)were who had received 7 points or more on thè Diagnostic Interview forBorderline Patients (Gunderson, Singer, & Austin, 1981) and that fitDSM-II1-R criteria for Borderline Personality Disturbance (BPD). We didnot include any BPD subjects who had concurrent Axis II diagnoses ora symptomatic Axis I diagnosis. Aclditionally, because of thè overlappingsymptoms between BPD and Dissociative Identity Disorder, BPD sub-jects were given thè Dissociative Disorder Interview Scale (Ross, 1989)and excluded if they scored over 7.
A group of 20 Neurotic patients (7 males and 13 females, mean age34.6 ±2.1) fit DSM-III-R criteria for a diagnosis of somatoform disturb-ance or ari anxiety disorder. As with borderline patients, neurotic sub-jects who could be diagnosed with another Axis 1 or II condition werenot included. The third group comprised Psychotic patients (10 malesand 10 females, mean age 33.9 + 3 years) who fit DSM-III-R criteria for
150
schizophrenia or delusional disorder. None of thè psychotic patients washospitalized at thè time of our testing, although ali of them had beenhospitalized for at least 15 days during thè 2 years prior to thè testing.
The mean educational level was 10 + .7 years for thè borderline group,10.5 ± .8 for thè psychotic group, and 12.7 ± .6 for thè neurotic group.The differences between them in age were not statistically significant (byStudent i-test).
AH subjects were administered thè Rorschach in a single session by oneof thè authors, after which thè protocols were scored independently bytwo departmental colleagues trained in thè Comprehensive System(Exner, 1993) and in thè content scales usecl for this research. The per-centage of agreement between thè scorers was evaluated for each seg-ment of thè protocols. The followiiig content analysis scales were used:Fisher and Cleveland (1958) Barrier and Penetration scale; Hostilityscale (Elizur, 1949); Anxiety scale (Elizur, 1949); Depenclency scale (DeVos, 1952); Depressici! Scale (Eiidicott, 1972; Endicott & Jortner, 1966);Suspiciousness scale (Endicott, 1972; Endicott, Jortner, & Abramoff,1969); and Lerner Defense scale (Lerner & Lerner, 1980).
The incidence of confabulations as definecl by Bohm ( 1969) was usedas a measure of reality testing. We additionally scored for a more severelevel among confabulations defined by Bohm (1969) as aii "O-" responsewith a "DG-" location and movement as thè determinant. From a contentperspective these kinds of responses are a Form of hyperelaboration ofthè stimulus in which a short but very dramatic history is iiiferrecl andreality testing is completely lost.
In order to perforili statistical analysis, quantitative variables from thèvarious scales were converted to qualitative, non-parametric classifica-tion as "present" or "absent" using thè following criteria: values equal loor more than 1 were grouped in thè "present" class, aiid values equal toor less than O were grouped in thè "absent" class. The data from thèRorschach content and formai analysis were then statistically evalualedby chi-square tests using S.P.S.S. software.
Results
The interrater agreement rates for thè Rorschach scoring categorieswere as follow: location = 92%, determinants = 94.2%, forni quality =81.7%, pairs = 95%, contents = 89%, populars = 91.5%, and special scores
151
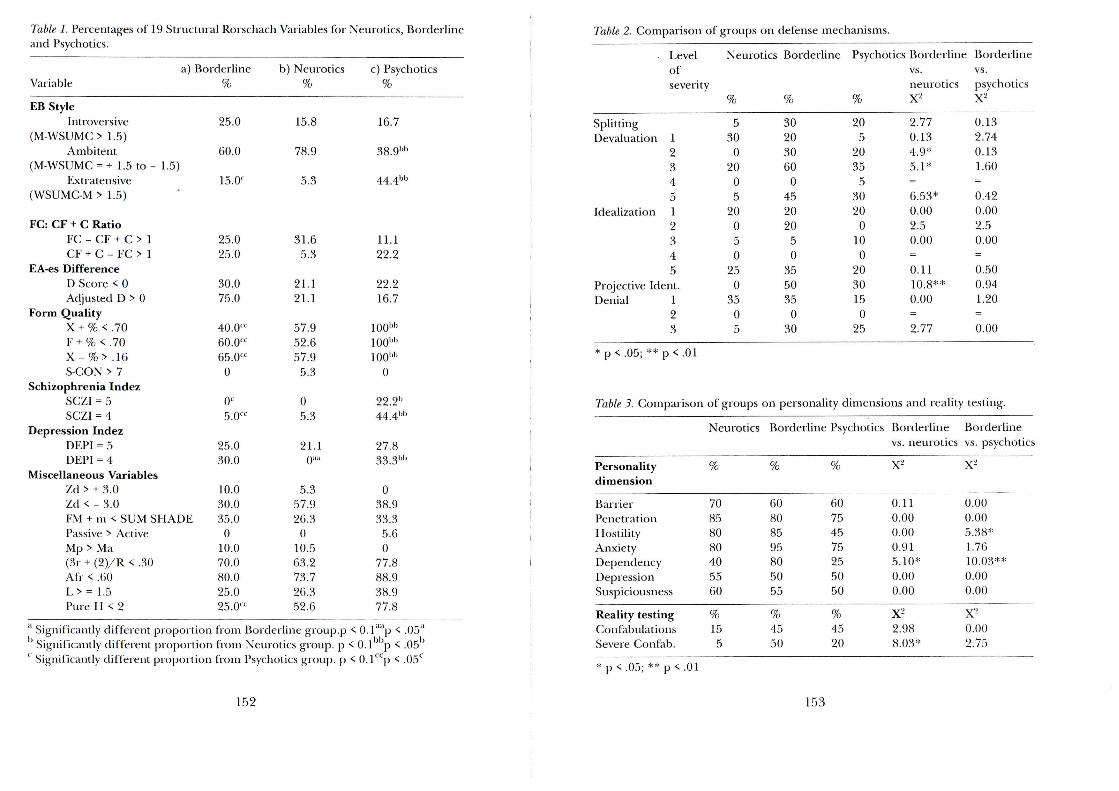
Table 1. Percemages of 19 Strnctnral Rorschach Variables for Neurotics, Bordedineand Psychotics.
a) BorclerlineVariable %
EB StyleIntroversive
(M-WSUMC > 1.5)Ambitent
(M-WSUMC = + 1.5 lo - 1.5)Extratensive
(WSUMC-M> 1.5)
FC: CF + C RatioFC - CF + C > 1CF + C - FC> 1
EA-es DifferenceI) Score < 0Adjustecl D > 0
Form QualityX + % < .70F + % < .70X-%> .16S-CON > 7
Schizophrenia IndezSCZI = 5SCZI = 4
Depression IndezDEPI = 5DEPI = 4
Miscellaneous VariablesZd > + 3.0Zd < - 3.0FM + m < SUM SHADEPassive > ActiveMp > Ma(3r + (2)/R < .30AIV < .60L>= 1.5Pure FI < 2
25.0
60.0
15. Oc
25.025.0
30.075.0
40.0"60.0"65.0"0
Oc
5.0"
25.030.0
10.030.035.0
010.070.080.025.025.0CC
b) Neurotics%
15.8
78.9
5.3
31.65.3
21.121.1
57.952.657.95.3
05.3
21.1O™
5.357.926.3
010.563.273.726.352.6
e) Psychotics%
16.7
38.9bb
44.4bb
11.122.2
22.216.7
100bb
100bb
100bb
0
22.2"44.4»
27.833. 31'1'
038.933.35.60
77.888.938.977.8
'' Significantly different proportion from Bordedine group.p < O.lilap < .05;l
' Significantly different proportion from Neurotics group. p < 0.1 bbp < .05b
Significaiuly different proportion from Psychotics group. p < O.llcp < .05°
152
Table 2. Comparisci! of groups on defense mechanisms.
. Level Neurotics Bordedine Psychotics Borclerline Bordedineof vs. vs.severi ty neurotics psychotics
SplittingDevaluation 1
2345
Idealization 12345
Projective Ident.Denial 1
23
* p < .05; ** p < .01
Table 3. Comparisco
Personalitydimension
BarrierPenetrationHostilityAnxietyDepenclencyDepressionSuspiciousness
Reality testingCon fabula tionsSevere Confab.
%
530
020
05
20050
250
3505
of groups
Neurotics
%
70858080405560
%155
%
30203060
045202050
355035
030
%
205
20355
3020
0100
2030150
25
x'-'2.770.134.9*5.1*=6.53*0.002.50.00=0.1110.8**0.00=2.77
on personality climensions and reality
Bordedine
%
60808595805055
%4550
Psychotics
%
60754575255050
%4520
Borclerlinevs. neurotics
x-
0.110.000.000.915.10*0.000.00
X2
2.988.03*
X2
0.132.740.131.60=0.420.002.50.00=0.500.941.20=0.00
testing.
Borclerlinevs. psychotics
X2
0.000.005.38*1.7610.03**0.000.00
X2
0.002.75
: p < .05; ** p < .01
153
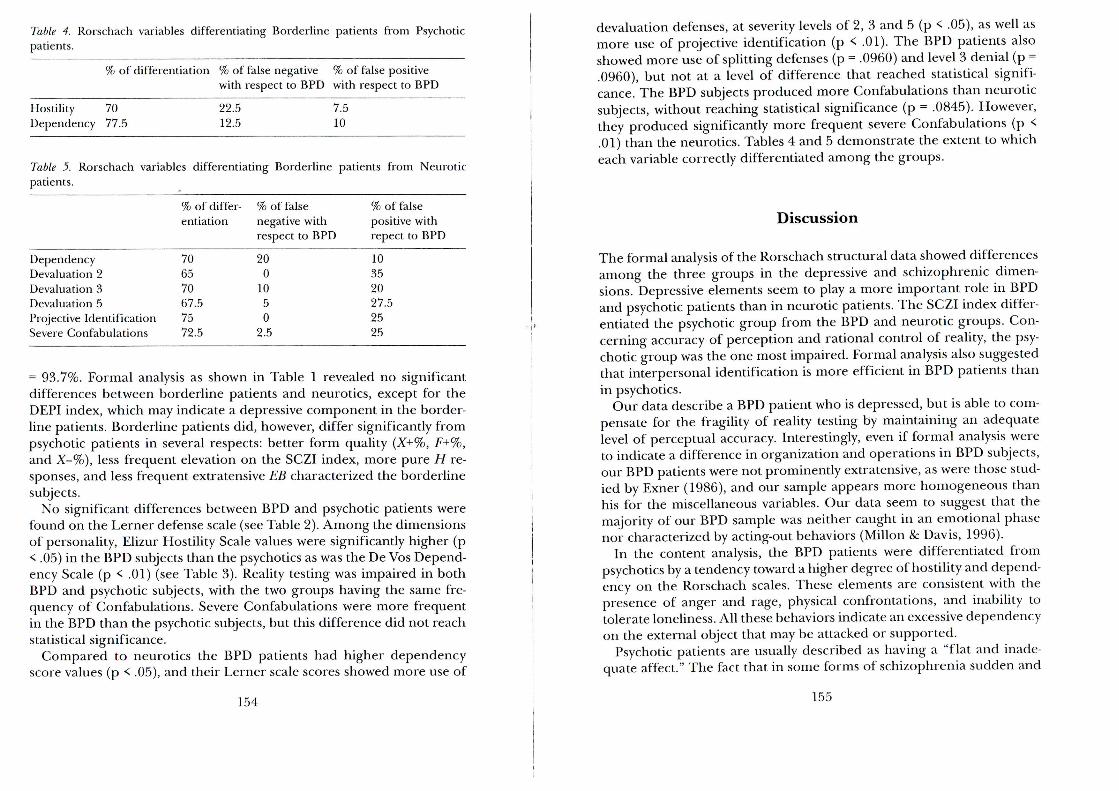
Table 4. Rorschach variables differentiating Borderline patients from Psychoticpatients.
% of differentiation % of false negative % of false positivewith respect to BPD with respect to BPD
Hostility 70Dependency 77.5
22.512.5
7.510
Table 5. Rorschach variables differentiating Borderline patients from Neuroticpatients.
DependencyDevaluation 2Devaluation 3Devaluation 5Projective IdentificationSevere Confabulations
% of differ-entiation
70657067.57572.5
% of falsenegative withrespect to BPD
200
LO50
2.5
% offa! sepositive withrepect to BPD
10352027.52525
= 93.7%. Formai analysis as shown in Table 1 revealed no significanedifferences between borderline patients and neurotics, except for thèDEPI index, which may indicate a depressive component in thè border-line patients. Borderline patients did, however, differ significantly frompsychotic patients in several respects: better form quality (X+%, F+%,and X-%), less frequent elevation on thè SCZI index, more pure H re-sponses, and less frequent extratensive EB characterized thè borderlinesubjects.
No significant differences between BPD and psychotic patients werefound on thè Lerner defense scale (see Table 2). Among thè dimensionsof personality, Elizur Hostility Scale values were significantly higher (p< .05) in thè BPD subjects than thè psychotics as was thè De Vos Depend-ency Scale (p < .01) (see Table 3). Reality testing was impaired in bothBPD and psychotic subjects, with thè two groups having thè sanie fre-quency of Confabulations. Severe Confabulations were more frequentin thè BPD than thè psychotic subjects, but this difference did not reachstatistical significance.
Compared to neurotics thè BPD patients had higher dependencyscore values (p < .05), and their Lerner scale scores showed more use of
154
devaluation defenses, at severity levels of 2, 3 and 5 (p < .05), as well asmore use of projective Identification (p < .01). The BPD patients alsoshowed more use of splitting defenses (p = .0960) and level 3 denial (p =.0960), but not at a level of difference that reached statistical signifi-cance. The BPD subjects produced more Confabulations than neuroticsubjects, without reaching statistical significance (p = .0845). However,they produced significantly more frequent severe Confabulations (p <.01) than thè neurotics. Tables 4 and 5 demonstrate thè extent to whicheach variable correctly differentiated among thè groups.
Discussioni
The formai analysis of thè Rorschach structural data showed differencesamong thè three groups in thè depressive and schizophrenic dimen-sions. Depressive elements seem to play a more important role in BPDand psychotic patients than in neurotic patients. The SCZI index differ-entiated thè psychotic group from thè BPD and neurotic groups. Con-cerning accuracy of perception and rational control of reality, thè psy-chotic group was thè one most impaired. Formai analysis also suggestedthat interpersonal Identification is more efficient in BPD patients thanin psychotics.
Our data describe a BPD patient who is clepressed, but is able to com-pensate for thè fragility of reality testing by maintaining an adequatelevel of perceptual accuracy. Interestingly, even if formai analysis wereto indicate a difference in organization and operations in BPD subjects,our BPD patients were not prominently extratensive, as were those stud-ied by Exner (1986), and our sample appears more homogeneous thanbis for thè miscellaneous variables. Our data seem to suggest that thèmajority of our BPD sample was neither caught in an emotional phasenor characterized by acting-out behaviors (Millon & Davis, 1996).
In thè content analysis, thè BPD patients were differentiated frompsychotics by a tenclency toward a higher degree of hostility and depend-ency on thè Rorschach scales. These elements are consistent with thèpresence of aiiger and rage, physical confrontations, and inability totolerate loneliness. Ali these behaviors indicate an excessive dependencyon thè external object that may be attacked or supported.
Psychotic patients are usually describecl as having a "fiat and inade-quate affect." The fact that in some forms of schizophrenia sudden aiid
155
inexplicable aggression may be present does not ref lect a Constant per-sonality trait, as does thè recurrent rage and anger of BPD patients.Furthermore, interpersonal deficit, with social retirement, "coldness,"and autistic behavior, does not permit development of adequate attach-ment, ari element necessary for promoting affective dependericy. Thefact that BPD patients produce a higher number of responses with hos-tility and dependent contents than do psychotics may be thè "Rorschachequivalent" of common clinical observations and thè DSM-III-R andDSM-IV criteria.
Affective dependency is thè only variable in our study that successfullydifferentiated BPD patients from both other groups. Gunderson (1977)has similarly suggested that BPD patients can be distinguished fromschizophrenic and neurotic subjects specifically by their dependencyand superficiality in interpersonal relations, aside from their impulsivebehaviors. Gunderson suggested further that thè core of BPD consistsof development of strong attachment, together with ambivalent fears ofdependency. Affective, behavioral, and thought disturbance in BPDwould thus be consequences of inadequate and frustrating managementof interpersonal relationships (Gunderson, 1984). This dependency traitis confirmed by thè resemblance of BPD and affective disorders (Ber-geret, 1976; Stone, 1989).
Our study did not find significant differences betweeri BPD and psy-chotics in their use of defenses. This is coritradictory to thè findings ofprevious research (Lerner & Lerner, 1981) and, more specifically, to thèstatement that BPD patients have different defensive organizations fromschizophrenics (Lerner & Lerner, 1982; Lerner, 1990). Nevertheless, ourdata are in agreement with Kernberg's hypothesis that psychotic patientscan also use thè same constellation of primitive defenses.
Our Lerner defense data on BPD and neurotics subjects are in accord-ance with previous findings (Kernberg, 1975; Lerner & Lerner, 1980;Lerner et al. 1981) and indicate that some form of linkageexistsbetweenthè groups. The Lerner scale clearly identifies in BPD patients a greateruse of medium and high levels of thè devaluation mechanism and pro-jective identification, as well as, to a lesser clegree, thè use of splittingand low level denial.
More specifically, devaluation is habitually considered thè tendency toundervalue, obscure, reduce, and finally cancel thè importance of oth-ers. Devaluation can be used with respect to feelings of envy, so that thèsubject is able to organize some forni of defense. In thè behavioralsphere devaluation can be connected to thè severe instability of personal
156
relations, so common in BPD patients, clescribed in DSM-IV as "alternat-ing between extremes of idealization and devaluation."
Projective identification is another defense mechanism that is com-mon in BPD patients and that in our data distinguished between BPDand neurotic subjects. It is defined as thè projection of unacceptableimpulses, so that thè feelings can stili be experienced and a form ofcontrol over thè projective object can be maintained (Kernberg, 1975;Lerner & Lerner, 1980; Lerner, 1990). On thè Rorschach test, projectiveidentification is usually shown by hyperelaborations with aggressivecontent.
Confabulation and aggressive contents are in accordance with thè clin-ical picture of BPD, which shows intense rage and formai thought dis-turbance in loosely structured situations (Gunderson, 1984). Reality test-ing disturbances are clearly manifested in BPD patients by thè confabu-lation phenomena. The BPD patients have thè same frequency ofBohm's Confabulation as psychotics do and show severe Confabulationsmore frequently than neurotics. These results concur with previous data(Edell, 1987; Singer & Larson, 1981; Yen, 1983), as thè Rorschach testcan be considered a "loosely structured situation" that facilitates thèemergence of thought disturbances that are not otherwise easily cle-tected during a clinical assessment.
According to Singer (1977) in this regard, primitive patterns ofthought appear in BPD Rorschach data because thè test does not pro-vide specific requirements for thè length and quality of thè answers.Arnow and Cooper (1984) have suggested that thè Rorschach, by pre-senting ambiguous stimuli that can be perceived as threatening togetherwith an examiner that presenls as "rientrai," is likely to encourage regres-sion and activation of primitive thought patterns.
The Rorschach test can be considered a useful diagnostic tool in BPDpatients, allowing display of thè weak reality testing in BPD subjects andshowing thè continuum of psychopathology among clifferent types ofpsychiatric patients (Weiner, 1986). Indeed, some of our results, both ofcontent and formai analysis, suggest possible overlap in thè cliagnosis ofBPD with other pre-psychotic conditions.
157
References
American Psychiatric Association (1987). Diagnostic and statistical manual ofmentaldisorders (3rd ed., revised). Washington, DC: Author.
American Psychiatric Association (1994). Diagnostic and statistical manual ofmentaldisorders (4th ed.). Washington, DC: Author.
Arnow, D., & Cooper, S. H. (1984). The borderline patient's regression on thè Ror-schach test: An object relation interpretation. Bulletin of thè Menninger Clinic, 48,25-36.
Bergeret,J. (1976). Depressione e stati limite. Roma, II Pensiero Scientifico Editore.Bohm, E. (1989). Manuale di psicodiagnostica di Rorschach. Firenze: Giunti-Barbera.
[Lehrbuch der Rorschach-Psychodiagnostic]. Bern: Verlag Hans Huber, 1953.De Vos, G. (1952). A quantitative approach to affective symbolism in Rorschach
responses. Journal ofProjective Techniques, 16, 133-150.Edell, W. (1987). Role of structure in disordered thinking in borderline and schizo-
phrenic disorders. Journal of Personality Assessment, 51, 23-41.Elizur, A. (1949). Content analysis in thè Rorschach with regard to anxiety and hos-
tility. Rorschach Research Exchange and Journal ofProjective Techniques, 13, 247-284.Endicott, N. A. (1972). The Hokzman Inkblot Technique content measures of de-
pression and suspiciousness./owrna^ of Personality Assessment, 36, 424-426.Endicott, N. A., &Jortner, S. (1966). Objective measures of depression. Archives of
General Psychiatry, 15, 249-255.Endicott, N. A.,Jortner, S., & Abramoff, E. (1969). Objective measure of suspicious-
ness. Journal ofAbnormal Psychology, 74, 26-32.Exner,J. E. (1986). Some Rorschach data comparìng schizophrenics with borderline
and schizotypal personality disorders. Journal of Personality Assessment, 50, 455-471.
Exner, J. E. (1993). The Rorschach: A comprehensive System. Voi. 1. Basic Foundations(3rd ed.). New York: Wiley.
Fisher, S., & Cleveland, S. E. (1958). Body image andpersonality. New York: Van Nos-trand Reinhold.
Gacono, C. B., Meloy, }. R., & Berg, J. L. (1992). Object relations, defensive opera-tions, and affective states in narcissistic, borderline, and antisocial personalitydisorders. Journal of Personality Assessment, 59, 32-49.
Gunderson, J. C. (1984). Borderline personality disorder. Washington, DC: AmericanPsychiatric Press.
Gunderson, J. C., Singer, M. T, & Austin, V. (1981). The diagnostic interview forborderline patients. American Journal of Psychialry, 138, 869-903.
Hilsenroth, M. J., Hibbard, S. R., Nash, M. R., & Handler, L. (1993). A Rorschachstudy of mircissism, defense, and aggression in borderline, narcissistic, and clusterC personality disorders. Journal of Personality Assessment, 60, 346-361.
Kernberg, O. F. (1970). A psychoanalytic classification of character pathology./owr-nal of thè American Psychoanalytic Association, 18, 800-822.
158
Kernberg, O. F. (1975). Borderline conditions and pathological narcissism. NewYork: Aronson.
Lerner, H. D., Albert, C., & Walsh, M. (1987). The Rorschach assessmeiit of border-line defenses. Journal of Personality Assessment, 51, 344-354.
Lerner, H. D., & Lerner P. M. (1980). Rorschach assessment of primitive defensesin borderline personality structure. InJ. Kwawer, H. D. Lerner, P. M. Lerner, &A. Sugarman (Eds.), Borderline phenomena and thè Rorschach test (pp. 257-274).New York: International University Press.
Lerner, H. D., & Lerner, P.M. (1982). A comparative study of defensive structure inneurotic, borderline, and schizophrenic patients. Psychoanalysis and GontemporaryThought,5,n-ll?>.
Lerner, H. D., Sugarman, A., & Gaughran, J. (1981). Borderline and schizophrenicspatients: A comparative study of defensive structure. Journal oj Nervous and MentalDisease, 169, 705-711.
Lerner, P. M. (1990). Rorschach assessment of primitive defenses: A review. Journalof Personality Assessment, 54, 30-46.
Millon T, & Davis R. D. (1996). Disorders of personality: DSM-lVand beyond. New York:Wiley.
Singer, M. T, & Larson D. G. (1981). Borderline personality and thè Rorschach test.Archives of General Psychiatry, 38, 693-698.
Stone, M. H. (1989). The course of borderline personality. In A. Tasman, R. Hales,& A. Frances (Ecls.), Review ofpsychiatry (Voi. 8). Washington, DC: American Psy-chiatric Press.
Yen, Y. (1983). Deviant verbalization in thè Rorschach test as an index of patholog-ical thinking of schizophrenics. Acta Psychologica Tawanica, 25, 13-23.
Weiner I. B. (1986). Conceptual and empirica! perspectives on thè Rorschach as-sessment of psychopathology./otrraa/ of Personality Assessment, 50, 472-479.
Zalewski C., & Archer R. P. (1991). Assessment of borderline personality disorder:A review of MMPI and Rorschach findings.yoMrwa/ of Nervous and Mental Disease,179, 338-345.
Riassunto
In questo studio sono stati confrontati venti pazienti con diagnosi DSM-III-R di disturbo borderline di personalità, con un numero eguale dinevrotici (soggetti con disturbi somatoformi o ansiosi secondo il DSM-III-R) e di psicotici (pazienti con diangosi DSM-III-R di schizofrenia odisturbo delirante). I pazienti non-differivano in forma statisticamentesignificativa per eté media.
Tutti i soggetti sono stati sottoposti al test di Rorschach, ed i protocollisono stati valutati con il sistema di Exner per quanto concerne l'analisi
159
strutturale e con analisi contenutistica. Per quanto riguarda quest'ultimasono state valutate le seguenti scale: scale di barriera e penetrazione diFisher and Cleveland (1958); scala di ostilité (Elizur, 1949); scala di an-sieté (Elizur, 1949); scala di dipendenza (De Vos, 1952); scala di depres-sione (Endicott, 1972; Endicott & Jortner, 1966); scala di sospettosité(Endicott, 1972; Endicott, Jortner, & Abramoff, 1969), scala delle difesedi Lerner (Lerner & Lerner, 1980).
Per quanto concerne l'esame di realtè sono state prese in consideraz-ione le confabulazioni e un grado di maggiore gravite delle stesse.Quest'ultime sono state tipizzate come confabulazioni nelle quali erapresente una iperelaborazione dello stimolo, con tematizzazione di unabreve storia, abitualmente drammatica, e dove il contatto con realtè ap-pariva completamente perso.
L'analisi strutturale ha indicato che i pazienti con disturbo borderlinedi personalité e i soggetti psicotici presentavano un numero maggiore disegni depressivi. L'indice SCZ1 ha differenziato esclusivamente ilgruppo degli psicotici, il quale peraltro A anche risultato come quellomaggiormente compromesso per quanto concerne l'accuratezza percet-tiva. Le capacité empatiche e di identificazione interpersonale sonorisultate migliori nei pazienti borderline.
L'analisi contenutistica ha indicato che i pazienti borderline eranodifferenziabili dagli altri due gruppi per una maggiore presenza di segnidi dipendenza affettiva. Inoltre, rispetto agli psicotici, i pazienti border-line presentavano un maggior numero di segni di ostilité, e utilizzavanoin maggior grado rispetto ai nevrotici meccanismi difensivi di svalutaz-ione ed identificazione proiettiva. I pazienti borderline presentavanoanche un maggior numero di confabulazioni gravi rispetto ai nevrotici.I dati di questo studio suggeriscono la possibilité che vi sia un discretogrado di sovrapposizione tra le categorie diagnostiche elei borderlinecon altre condizioni pre-psicotiche.
Résumé
Cette étude porte sur 20 patients aux troubles de la personnalité limites,diagnostiqués conformément aux critères du DSM III-R, que nous avonscomparés avec le meme nombre de sujets riévrotiques (DSM III-R trou-bles somatoformes et anxieux) et psychotiques (DSM III-R schizo-phrènes et troubles délirants). Les deux groupes ont passe le test du
160
Rorschach. Nous avons ensuite procède a l'analyse des données Ror-schach d'après le Système Integre d'Exner, et une analyse de contenuavec les échelles suivantes: Score Barrière et Pénétration de Fisher andCleveland; Echelle d'Hostilité d'Elizur; Echelle d'Anxiété d'Elizur;Echelle de Dépenclance de de Vos; Echelle de Dépression d'Endicotl;Echelle de Suspicion d'Endicott; et Echelle Défensive de Lerner.
Gomme mesure de l'épreuve de réalité, nous avons tenu compte eiel'incidence des Confabulations ainsi que d'une forme plus grave de con-fabulation qui consiste en une hyper-élaboration du stimulus danslaquelle le sujet raconte une histoire courte mais dramatique avec uneperle totale d'épreuve de réalité.
Les données structurales montrent plus de dignes depressiti chez lespatients limites et psychotiques que chez les névrosés. L'indice SCZI n'aidentifié que le groupe psychotique, qui était aussi le plus faible enacléquation formelle. L'identification interpersonnelle était plus impor-tante chez les patients borderline que dans les deux autres groupes.
L'analyse des contenus a mis en évidence que les patients a trouble dela personnalité limite diffèrent des deux autres groupes par une plusgrande fréquence de signes de dépendance affective. En outre, en com-paraison avec les sujets psychotiques, les patients limites ont manifesteplus de signes d'hostilité; comparés aux patients névrotiques, ils ont plusutilisé la dévalorisation, l'identification projective et des Confabulationsgraves. Les données de cette étude vont dans le sens de l'hypothèse d'unrecouvrement partici des catégories diagnostiqués limite et les autresétats pré-psychotiques.
Resumen
Veinte pacientes con trastorno de personalidad borderline seguii loscriterios del DSM-III-R fueron comparados con igual nùmero deneuróticos (sujetos con diagnòstico DSM-III-R de trastorno somato-forme y de ansiedad) y psicóticos (pacientes con diagnòstico DSM-III-Rde esquizofrenia y trastorno delirante). El anàlisis estructural de los da-tos del Rorschach fué llevado a cabo en base al Sistema Comprehensivo.Para el anàlisis de los Contenidos se utilizaron las siguientes escalas:Barrerà y Penetración de Fisher y Cleveland, LIostilidad y Ansieclad deElizur, Dependencia de De Vos, Depresión y Suspicacia de Endicott yDefensas de Lerner. Se evaluó la presencia de Confabulaciones, como
161
medida de la prueba de realidad, asì como la presencia de un nivel massevero de Confabulación, el cual incluyó la hiperelaboración delestimulo eii los casos en que se infiere una historia breve pero dramàticacon pérdida completa de la prueba de realidad.
Los datos estructurales revelaron con mayor frecuencia signos de cle-presión en los pacientes borderline y psicóticos que en los pacientesneuróticos. El indice SCZI diferenció solamente al grupo esqui-zofrénico, el cual mostrò también el mayor deterioro en la exactitudperceptiva. La identificación interpersonal se manifestò de manera masprominente en los pacientes borderline que en los otros dos grupos. Losresultados en cuanto al contenido revelaron que los pacientes con tras-torno de personalidad borderline difirieron de los otros dos grupos encuanto a una mayor incidencia de signos de dependencia afectiva. Alcompararlos con los sujetos psicóticos, los pacientes borderline desple-garon con mayor frecuencia signos de hostilidad. En comparación conlos pacientes neuróticos, los pacientes borderline dieron con mayor fre-cuencia respuestas de devaluación, identificación proyectiva y confabu-laciones severas. Los datos de este estudio apoyan la hipótesis de queprobablemente existe alguna superposición entre la categoria di-agnòstica de borderline y otras condiciones pre-psicóticas.
162
-t