bowel prep and oral antibiotics perioperative ... · bowel prep and oral antibiotics perioperative...
TRANSCRIPT

1
Preventing Surgical Site Infections
Prophylactic Antibiotics
Bowel Prep and Oral Antibiotics
Perioperative Hyperglycemia is Dangerous for both Diabetics and NONdiabetics
PreWarming and Warming for Perioperative Normothermia
Patchen Dellinger
Prophylactic Antibiotics
Antibiotics given for the purpose of preventing infection when infection is not present but the risk of postoperative infection is present
2
Prophylactic AntibioticsQuestions
• Which cases benefit?
• Which drug should you use?
• When should you start?
• How much should you give?
• How long should antibiotics be continued?
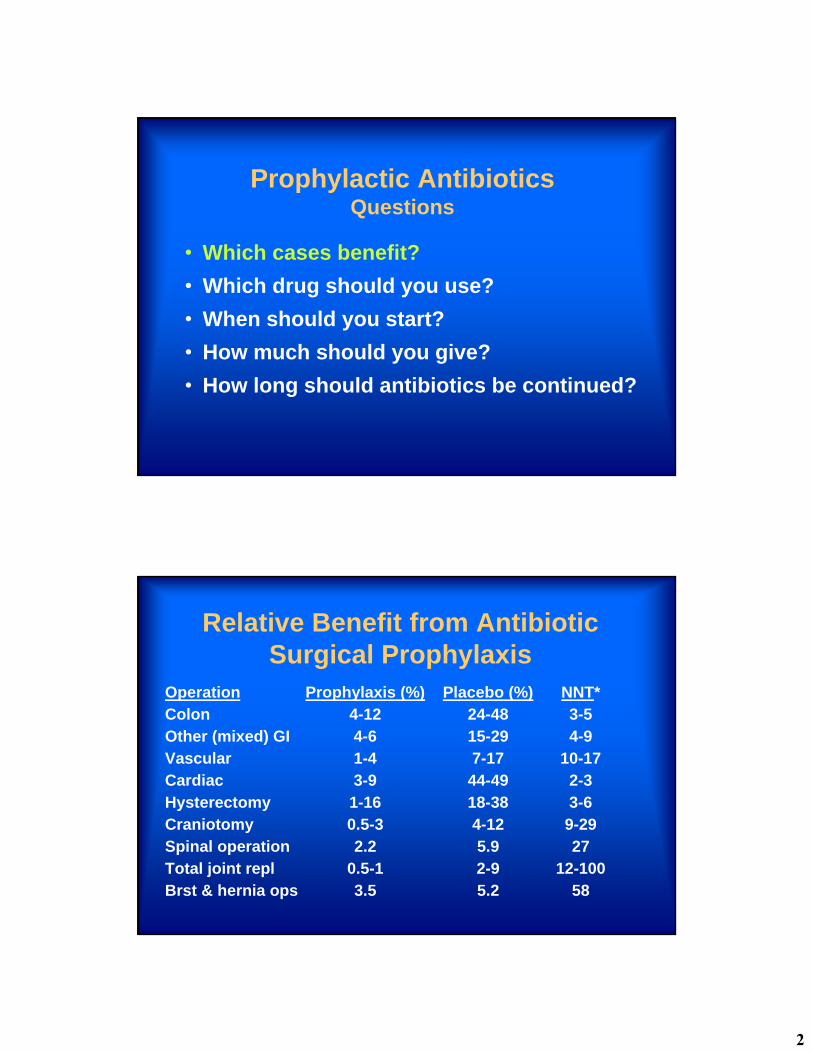
Relative Benefit from Antibiotic Surgical Prophylaxis
Operation Prophylaxis (%) Placebo (%) NNT*Colon 4-12 24-48 3-5Other (mixed) GI 4-6 15-29 4-9Vascular 1-4 7-17 10-17Cardiac 3-9 44-49 2-3Hysterectomy 1-16 18-38 3-6Craniotomy 0.5-3 4-12 9-29Spinal operation 2.2 5.9 27Total joint repl 0.5-1 2-9 12-100Brst & hernia ops 3.5 5.2 58
3
Antibiotic ProphylaxisDemonstrated Benefit
• G.I. Procedures (including appendicitis)
• Oropharyngeal procedures
• Vascular (abd & leg) procedures
• Open heart procedures
• Obstetrical and Gynecological procedures
• Orthopedic hardware placement
• Craniotomy
Antibiotic ProphylaxisDemonstrated Benefit: “Clean” Procedures
• Orthopedic joint replacements
• Open reduction of closed fractures
• Vascular prostheses
• Vascular procedures on the leg
• Median sternotomy
• Craniotomy
• Breast and hernia procedures
4
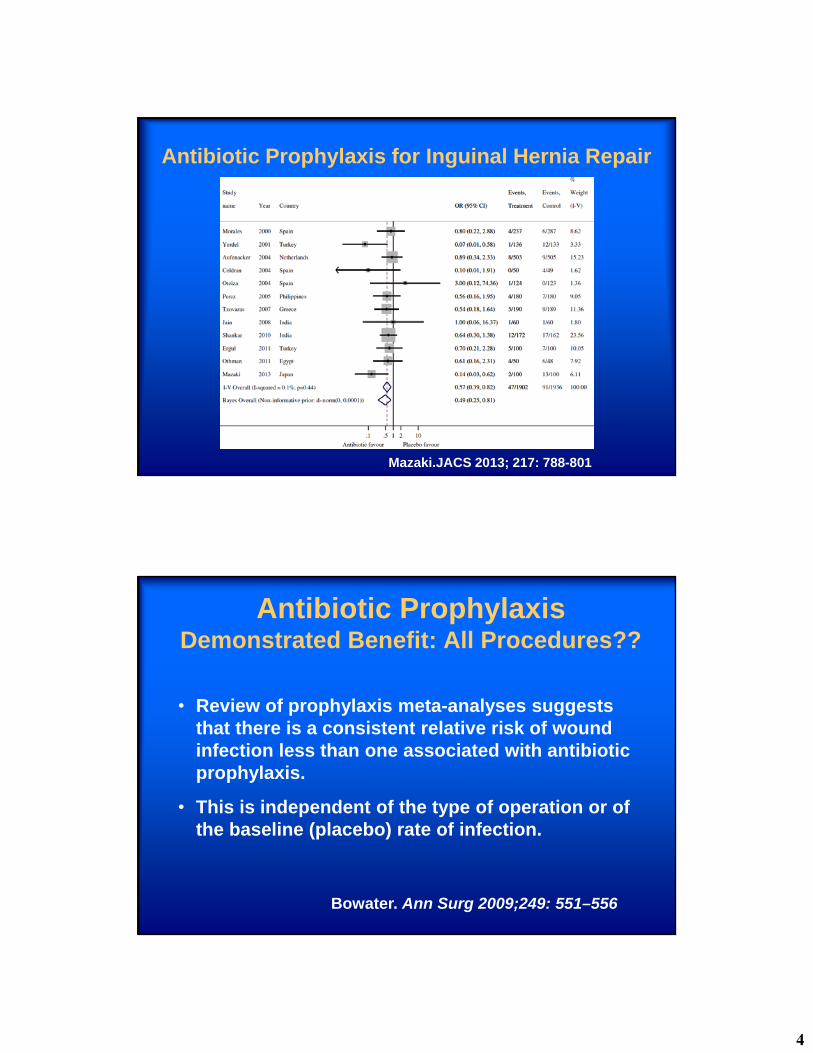
Antibiotic Prophylaxis for Inguinal Hernia Repair
Mazaki.JACS 2013; 217: 788-801
Antibiotic ProphylaxisDemonstrated Benefit: All Procedures??
• Review of prophylaxis meta-analyses suggests that there is a consistent relative risk of wound infection less than one associated with antibiotic prophylaxis.
• This is independent of the type of operation or of the baseline (placebo) rate of infection.
Bowater. Ann Surg 2009;249: 551–556
5
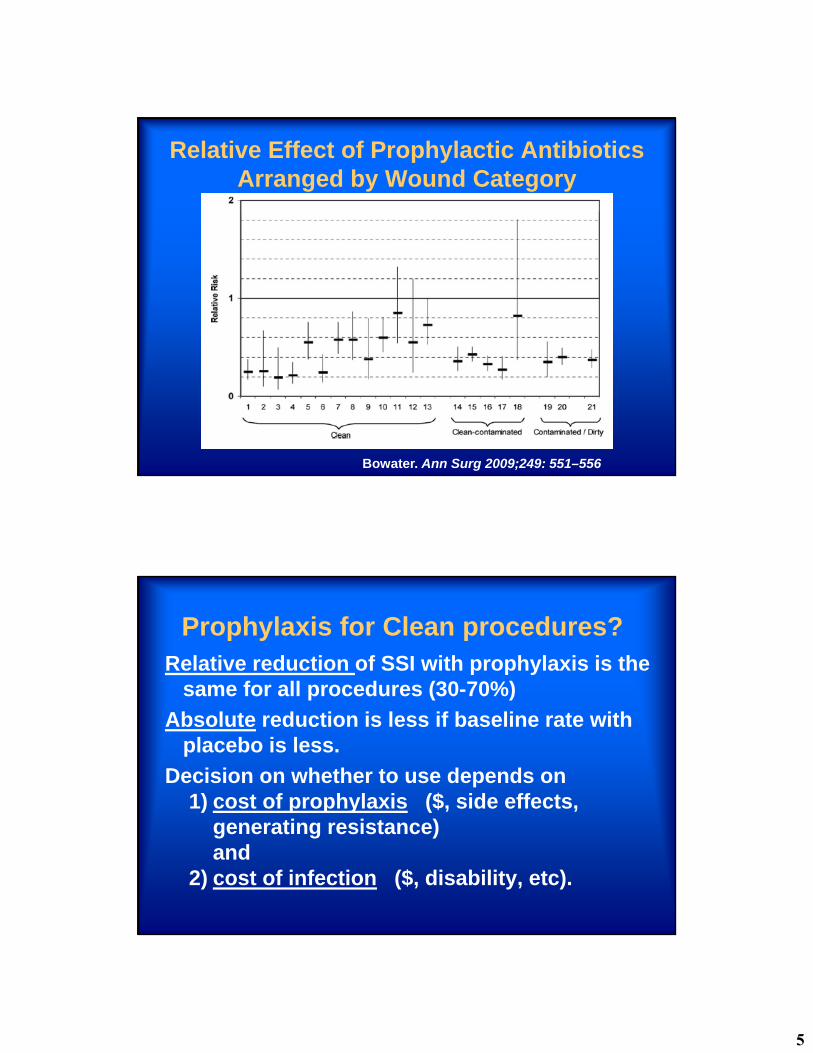
Relative Effect of Prophylactic Antibiotics Arranged by Wound Category
Bowater. Ann Surg 2009;249: 551–556
Prophylaxis for Clean procedures?Relative reduction of SSI with prophylaxis is the
same for all procedures (30-70%)
Absolute reduction is less if baseline rate with placebo is less.
Decision on whether to use depends on 1) cost of prophylaxis ($, side effects,
generating resistance) and
2) cost of infection ($, disability, etc).
6
Prophylactic AntibioticsQuestions
• Which cases benefit?
• Which drug should you use?
• When should you start?
• How much should you give?
• How long should antibiotics be continued?
7
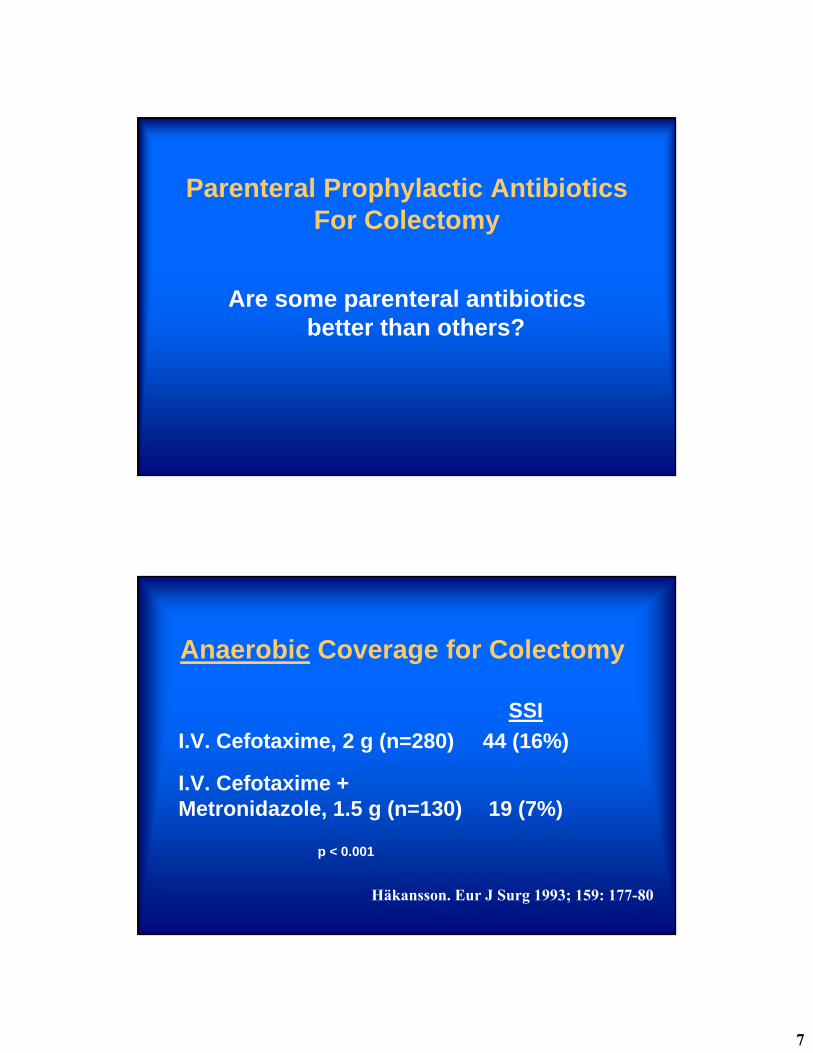
Parenteral Prophylactic AntibioticsFor Colectomy
Are some parenteral antibiotics better than others?
Anaerobic Coverage for Colectomy
SSI
I.V. Cefotaxime, 2 g (n=280) 44 (16%)
I.V. Cefotaxime +Metronidazole, 1.5 g (n=130) 19 (7%)
p < 0.001
Hӓkansson. Eur J Surg 1993; 159: 177-80
8
Aerobic Coverage for Colectomy
SSI
I.V. Ticarcillin (n=131) 10 (8%)3 g preop and 2 h later
P.O. Tinidazole (n=130) 26 (20%)2 g 10 hr preop
p < 0.007
Aust N Z J Surg. 1986; 56: 209-13
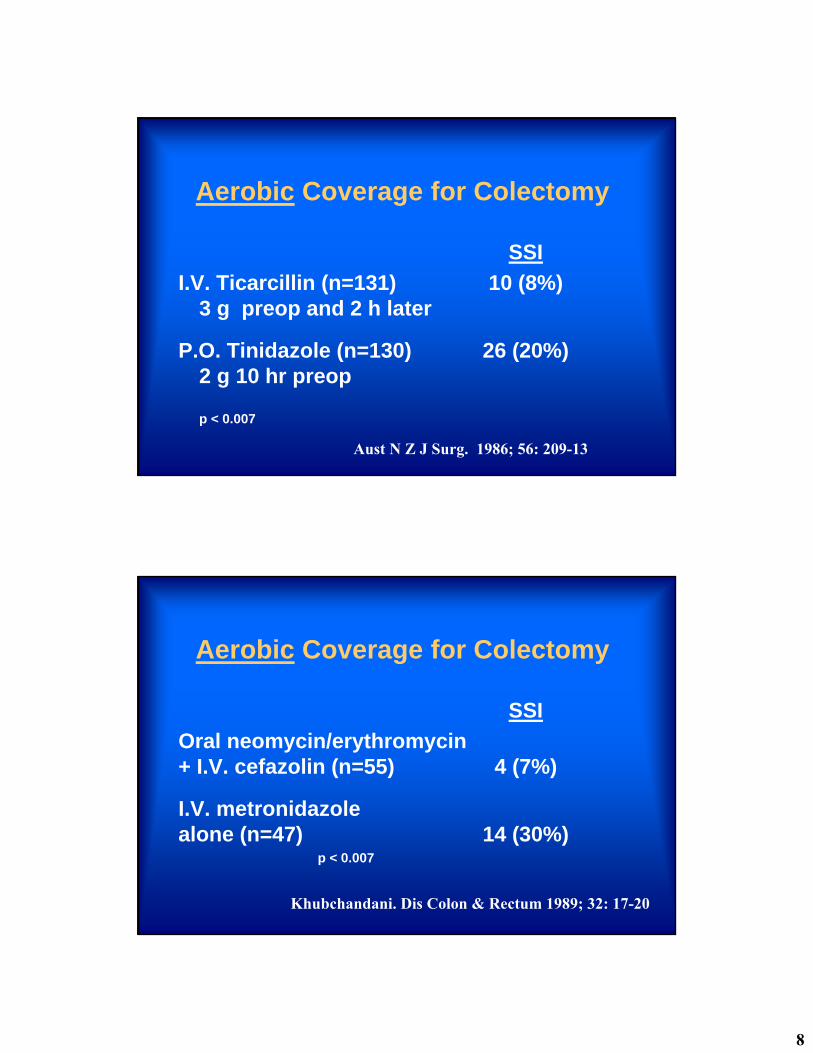
Aerobic Coverage for Colectomy
SSI
Oral neomycin/erythromycin+ I.V. cefazolin (n=55) 4 (7%)
I.V. metronidazole alone (n=47) 14 (30%)
p < 0.007
Khubchandani. Dis Colon & Rectum 1989; 32: 17-20
9
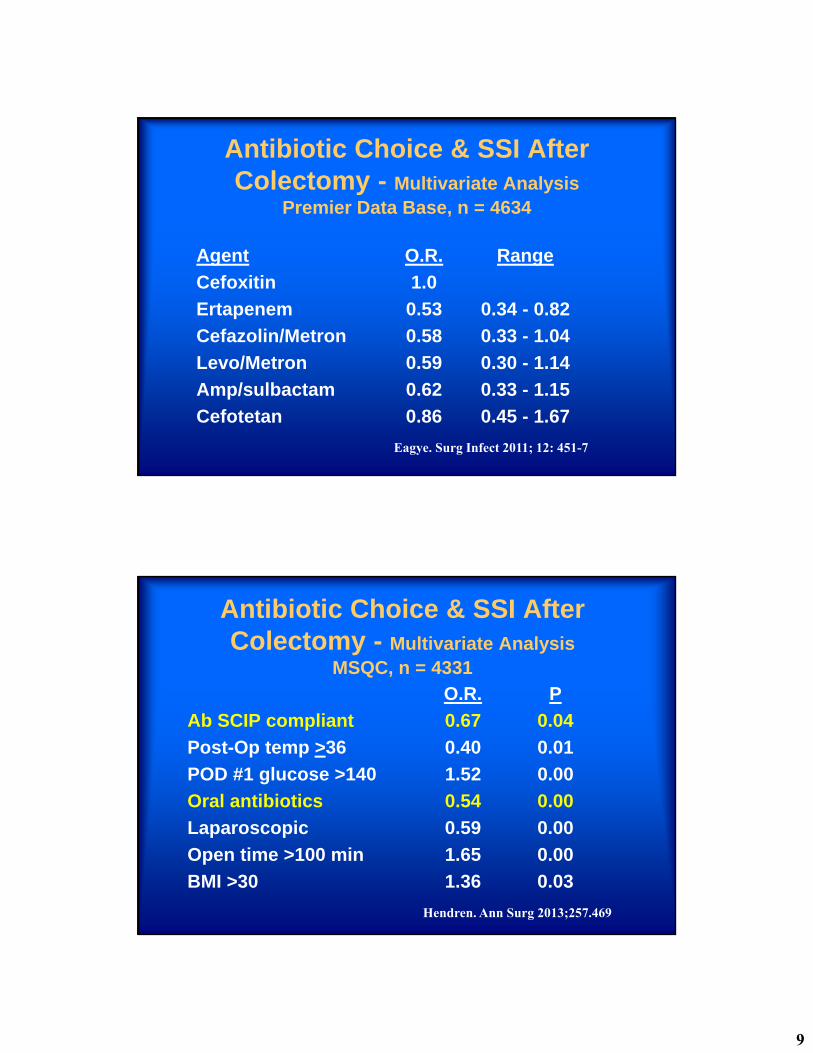
Antibiotic Choice & SSI After Colectomy - Multivariate Analysis
Premier Data Base, n = 4634
Agent O.R. Range
Cefoxitin 1.0
Ertapenem 0.53 0.34 - 0.82
Cefazolin/Metron 0.58 0.33 - 1.04
Levo/Metron 0.59 0.30 - 1.14
Amp/sulbactam 0.62 0.33 - 1.15
Cefotetan 0.86 0.45 - 1.67
Eagye. Surg Infect 2011; 12: 451-7
Antibiotic Choice & SSI After Colectomy - Multivariate Analysis
MSQC, n = 4331
O.R. P
Ab SCIP compliant 0.67 0.04
Post-Op temp >36 0.40 0.01
POD #1 glucose >140 1.52 0.00
Oral antibiotics 0.54 0.00
Laparoscopic 0.59 0.00
Open time >100 min 1.65 0.00
BMI >30 1.36 0.03
Hendren. Ann Surg 2013;257.469
10
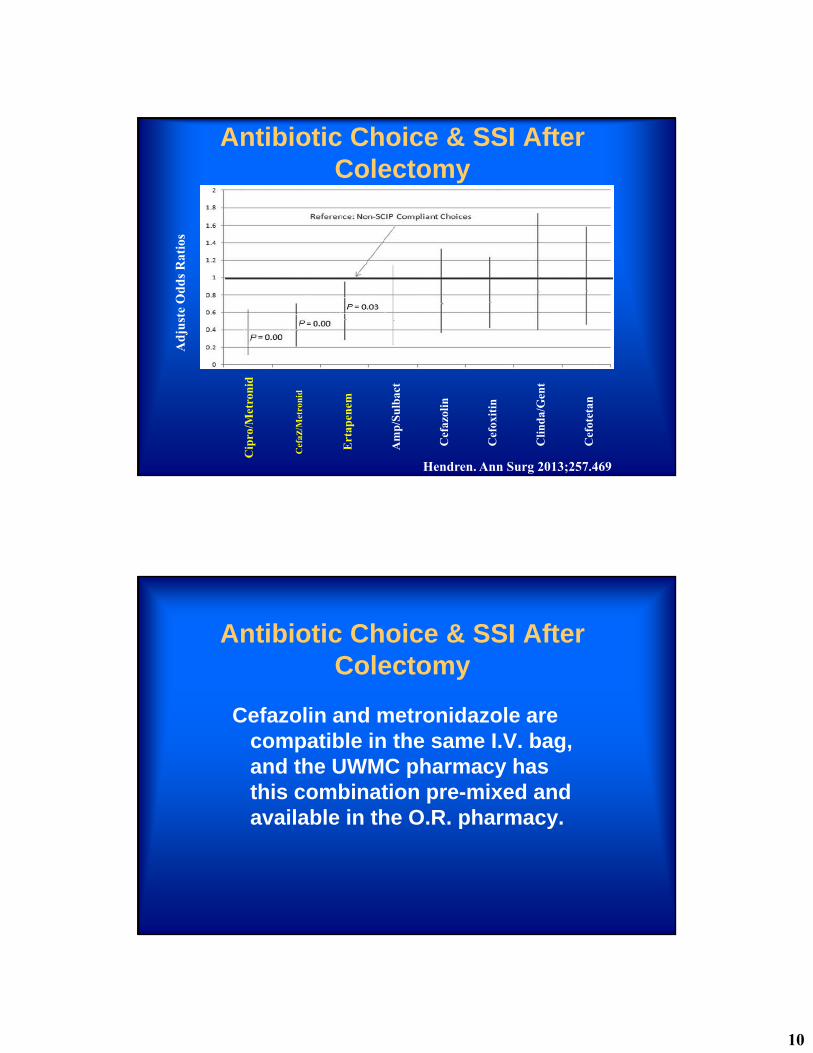
Antibiotic Choice & SSI After Colectomy
Cip
ro/M
etro
nid
Cef
az/M
etro
nid
Ert
apen
em
Am
p/S
ulb
act
Cef
azol
in
Cef
oxit
in
Cli
nd
a/G
ent
Cef
otet
an
Ad
just
eO
dd
s R
atio
s
Hendren. Ann Surg 2013;257.469
Antibiotic Choice & SSI After Colectomy
Cefazolin and metronidazole are compatible in the same I.V. bag, and the UWMC pharmacy has this combination pre-mixed and available in the O.R. pharmacy.
11
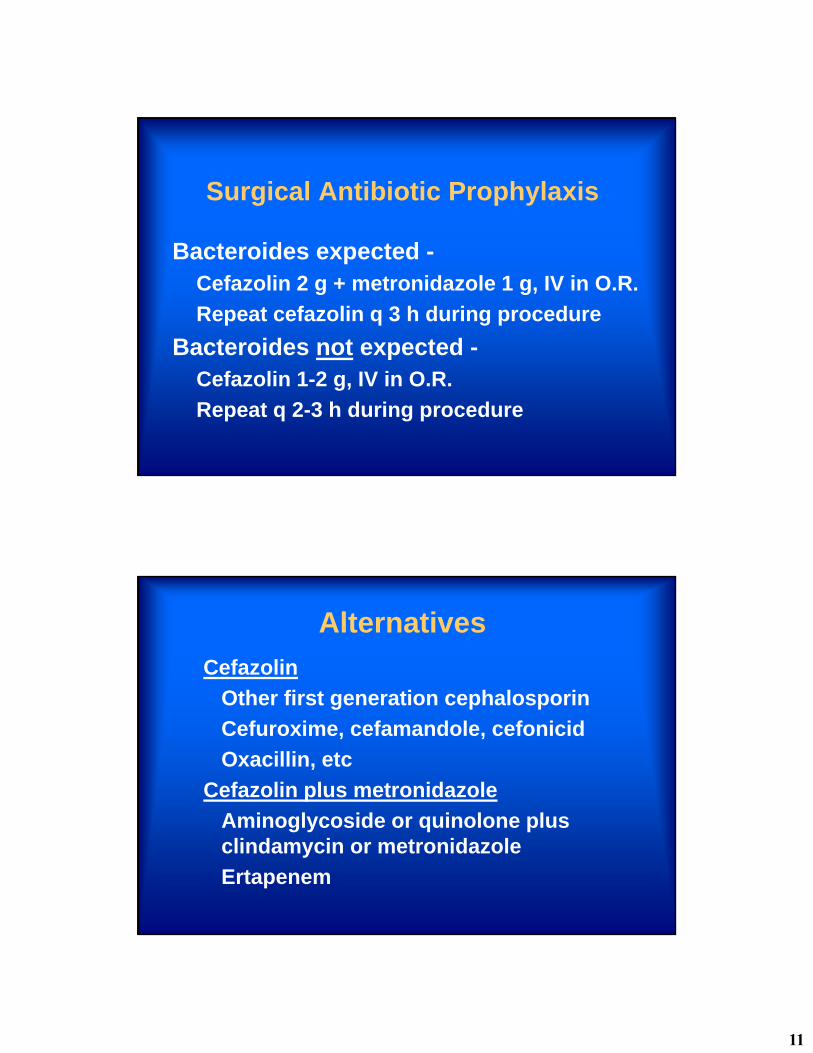
Surgical Antibiotic Prophylaxis
Bacteroides expected -Cefazolin 2 g + metronidazole 1 g, IV in O.R.
Repeat cefazolin q 3 h during procedure
Bacteroides not expected -Cefazolin 1-2 g, IV in O.R.
Repeat q 2-3 h during procedure
Alternatives
Cefazolin
Other first generation cephalosporin
Cefuroxime, cefamandole, cefonicid
Oxacillin, etc
Cefazolin plus metronidazole
Aminoglycoside or quinolone plus clindamycin or metronidazole
Ertapenem
12
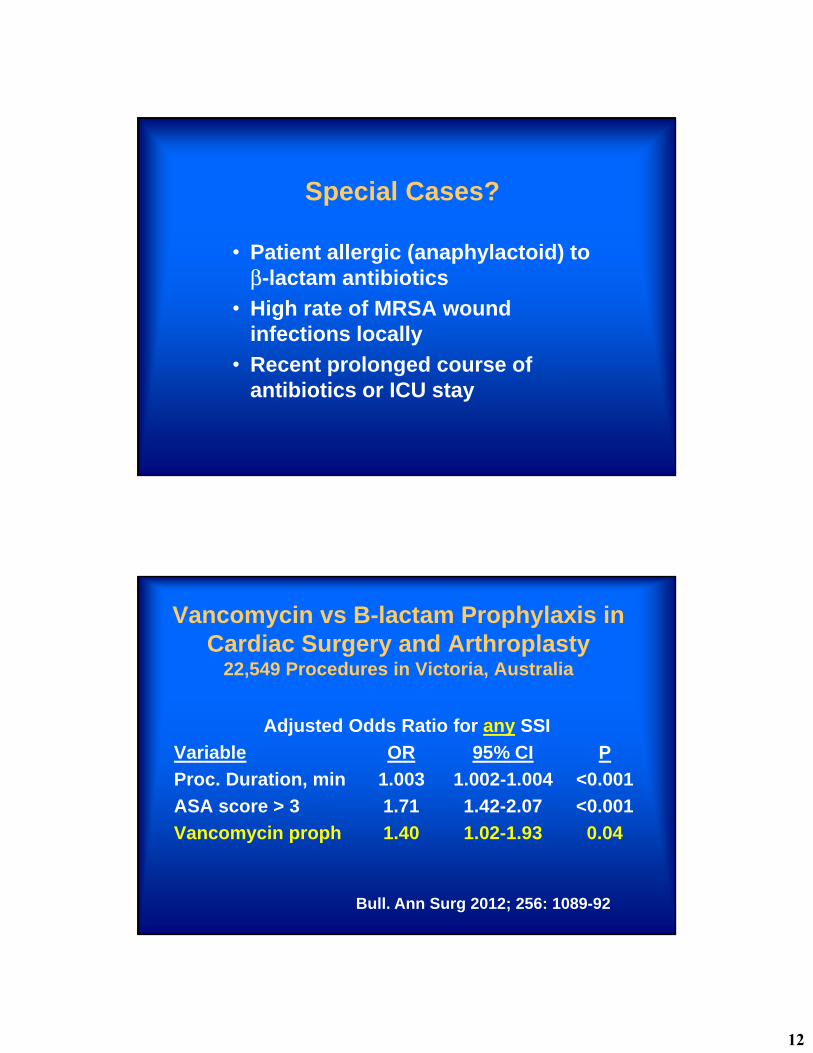
Special Cases?
• Patient allergic (anaphylactoid) to β-lactam antibiotics
• High rate of MRSA wound infections locally
• Recent prolonged course of antibiotics or ICU stay
Vancomycin vs B-lactam Prophylaxis in Cardiac Surgery and Arthroplasty
22,549 Procedures in Victoria, Australia
Adjusted Odds Ratio for any SSI
Variable OR 95% CI P
Proc. Duration, min 1.003 1.002-1.004 <0.001
ASA score > 3 1.71 1.42-2.07 <0.001
Vancomycin proph 1.40 1.02-1.93 0.04
Bull. Ann Surg 2012; 256: 1089-92
13
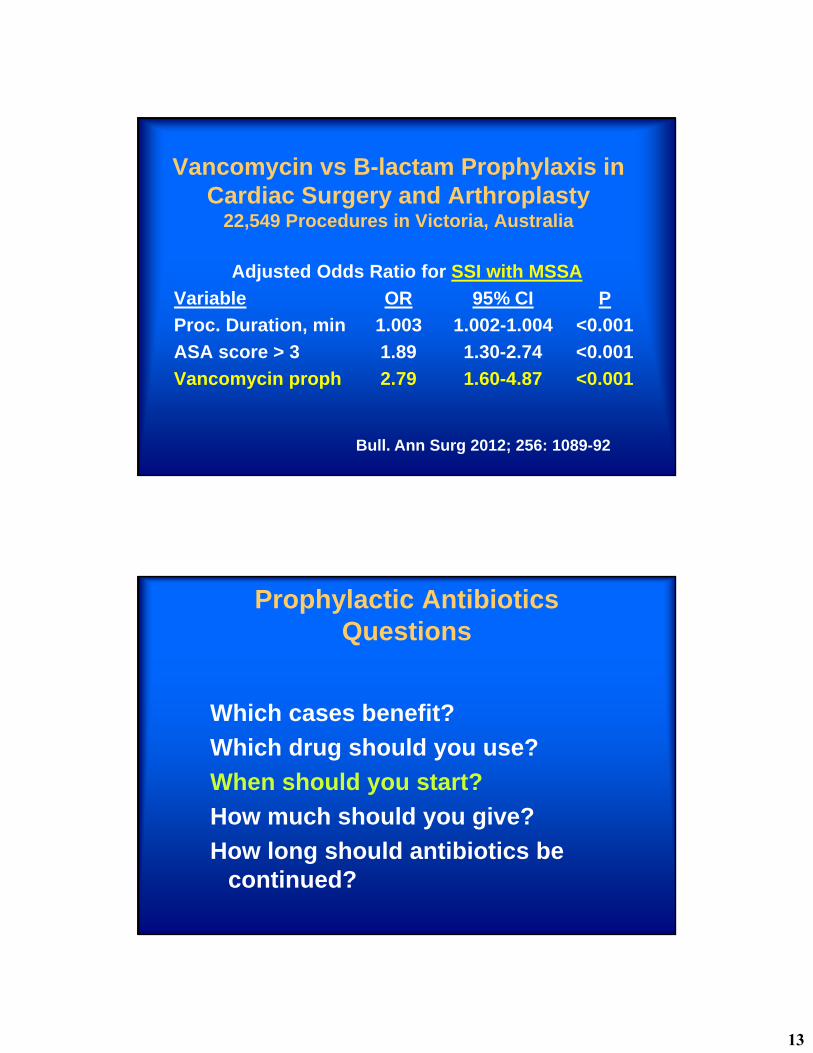
Vancomycin vs B-lactam Prophylaxis in Cardiac Surgery and Arthroplasty
22,549 Procedures in Victoria, Australia
Adjusted Odds Ratio for SSI with MSSA
Variable OR 95% CI P
Proc. Duration, min 1.003 1.002-1.004 <0.001
ASA score > 3 1.89 1.30-2.74 <0.001
Vancomycin proph 2.79 1.60-4.87 <0.001
Bull. Ann Surg 2012; 256: 1089-92
Prophylactic AntibioticsQuestions
Which cases benefit?
Which drug should you use?
When should you start?
How much should you give?
How long should antibiotics be continued?
14
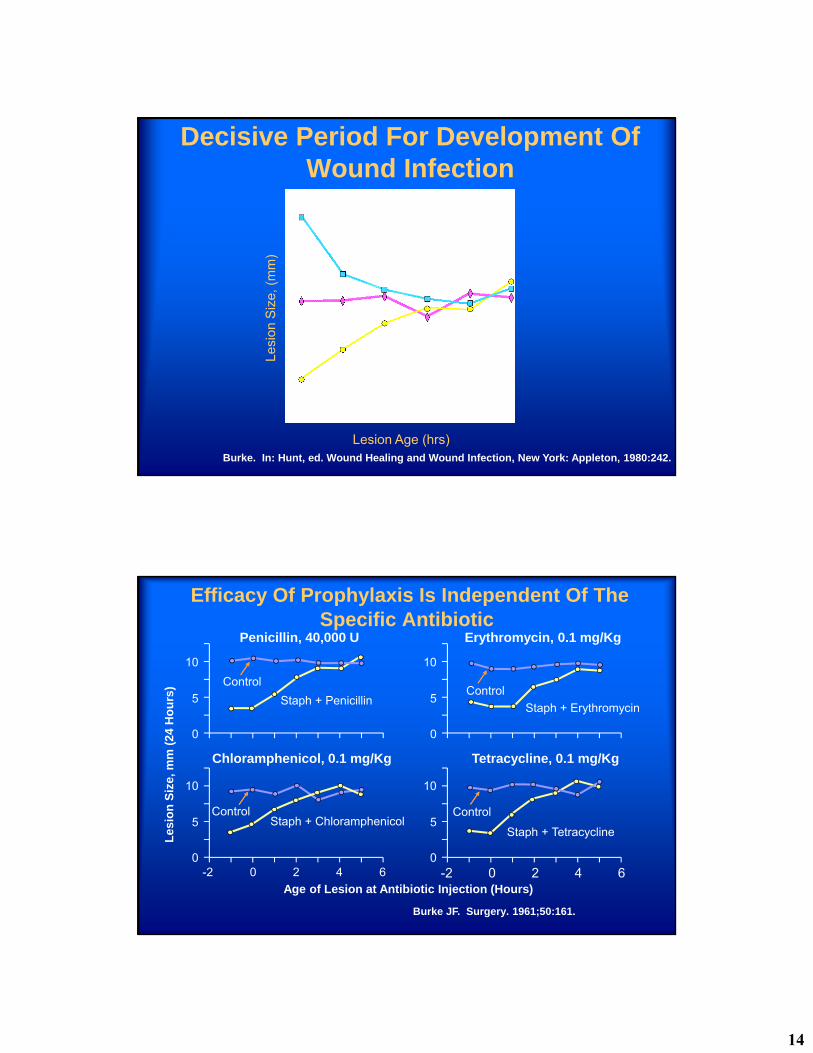
Burke. In: Hunt, ed. Wound Healing and Wound Infection, New York: Appleton, 1980:242.
Decisive Period For Development Of Wound Infection
Lesion Age (hrs)
Lesi
on S
ize,
(m
m)
Efficacy Of Prophylaxis Is Independent Of The Specific Antibiotic
Age of Lesion at Antibiotic Injection (Hours)
Les
ion
Siz
e, m
m (
24 H
ou
rs)
0
5
10
Penicillin, 40,000 U
Staph + Penicillin
Control
Chloramphenicol, 0.1 mg/Kg
Erythromycin, 0.1 mg/Kg
Tetracycline, 0.1 mg/Kg
0 2 4 6-2 0 2 4 6-2
0
5
10
0
5
10
0
5
10
Control Control
Control
Staph + Erythromycin
Staph + TetracyclineStaph + Chloramphenicol
Burke JF. Surgery. 1961;50:161.
15
0
1
2
3
4
≤-3 -2 -1 0 1 2 3 4 ≥5
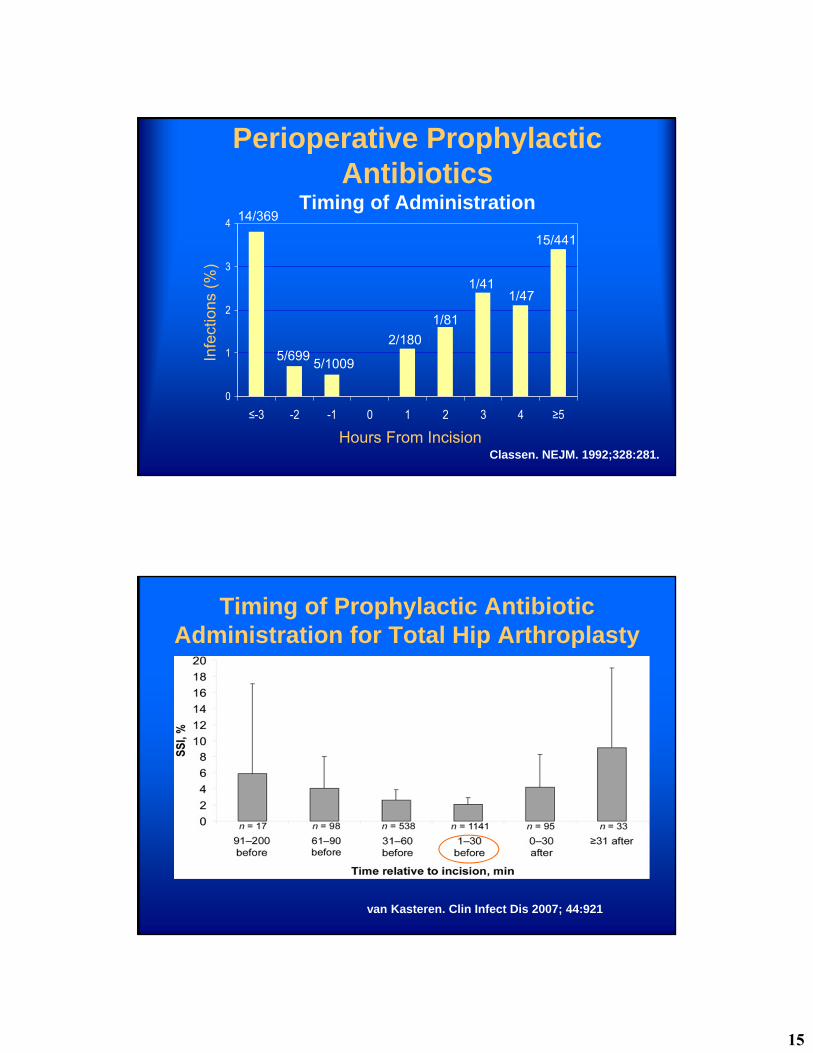
Classen. NEJM. 1992;328:281.
Perioperative Prophylactic Antibiotics
Timing of AdministrationIn
fect
ions
(%
)
Hours From Incision
14/369
5/6995/1009
2/180
1/81
1/411/47
15/441
Timing of Prophylactic Antibiotic Administration for Total Hip Arthroplasty
van Kasteren. Clin Infect Dis 2007; 44:921
16
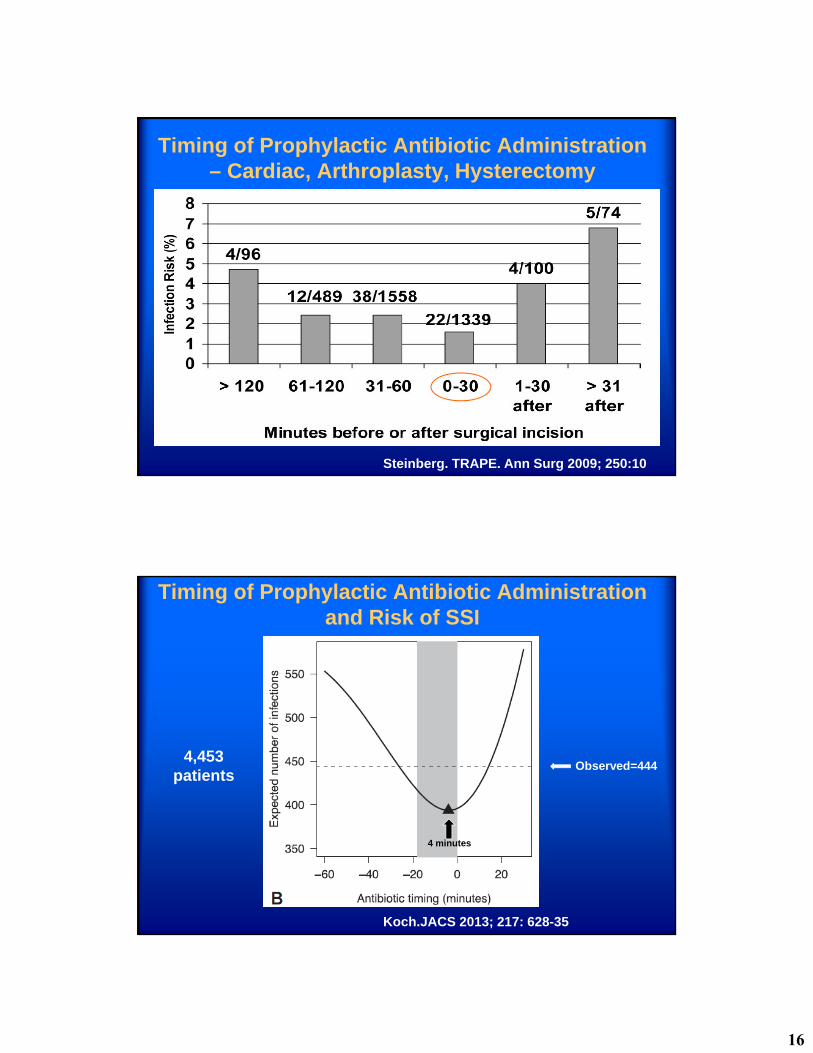
Timing of Prophylactic Antibiotic Administration – Cardiac, Arthroplasty, Hysterectomy
Steinberg. TRAPE. Ann Surg 2009; 250:10
Timing of Prophylactic Antibiotic Administrationand Risk of SSI
Koch.JACS 2013; 217: 628-35
4,453patients
4 minutes
Observed=444

17
Timing, Dose, Redose, Weight
All the evidence suggests that having effective drug levels in tissue and blood (more is better) during the entire operation reduces SSI risk.
Dosing close to incision, redosing, and using weight based dosing are logical ways to accomplish this.
Prophylactic AntibioticsTiming - Cefazolin
Serum Levels (mg/L)
On Call Anesth
Incision 87 148
1 hour 37 57
2 hours 25 39
DiPiro. Arch Surg 1985;120:829
18
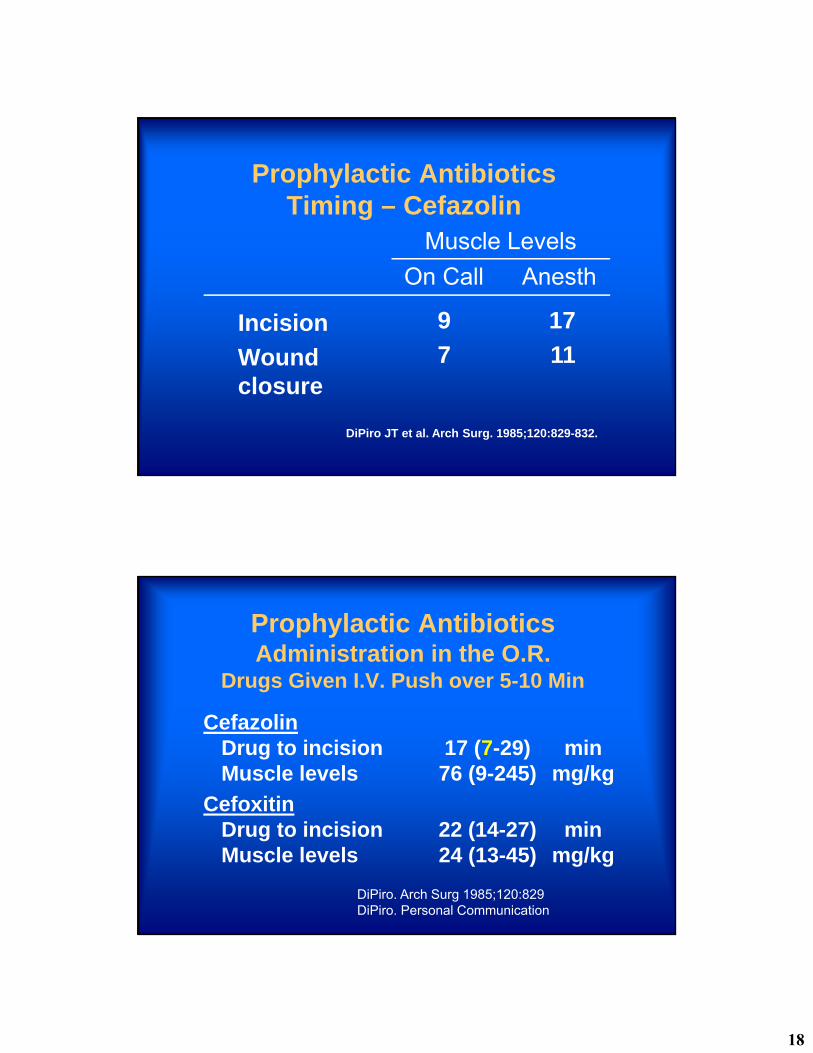
Prophylactic AntibioticsTiming – Cefazolin
Incision
Wound closure
9
7
17
11
On Call Anesth
Muscle Levels
DiPiro JT et al. Arch Surg. 1985;120:829-832.
Prophylactic AntibioticsAdministration in the O.R.
Drugs Given I.V. Push over 5-10 Min
CefazolinDrug to incision 17 (7-29) minMuscle levels 76 (9-245) mg/kg
CefoxitinDrug to incision 22 (14-27) minMuscle levels 24 (13-45) mg/kg
DiPiro. Arch Surg 1985;120:829DiPiro. Personal Communication
19
Prophylactic AntibioticsTissue Levels at Wound Closure
Time No DrugCefoxitin of Closure Detectable
On Call 2.5 hr 38%
With Anesth 2.3 hr 14%
DiPiro. Arch Surg 1985;120:829
Prophylactic AntibioticsQuestions
• Which cases benefit?
• Which drug should you use?
• When should you start?
• How much should you give?
• How long should antibiotics be continued?
20
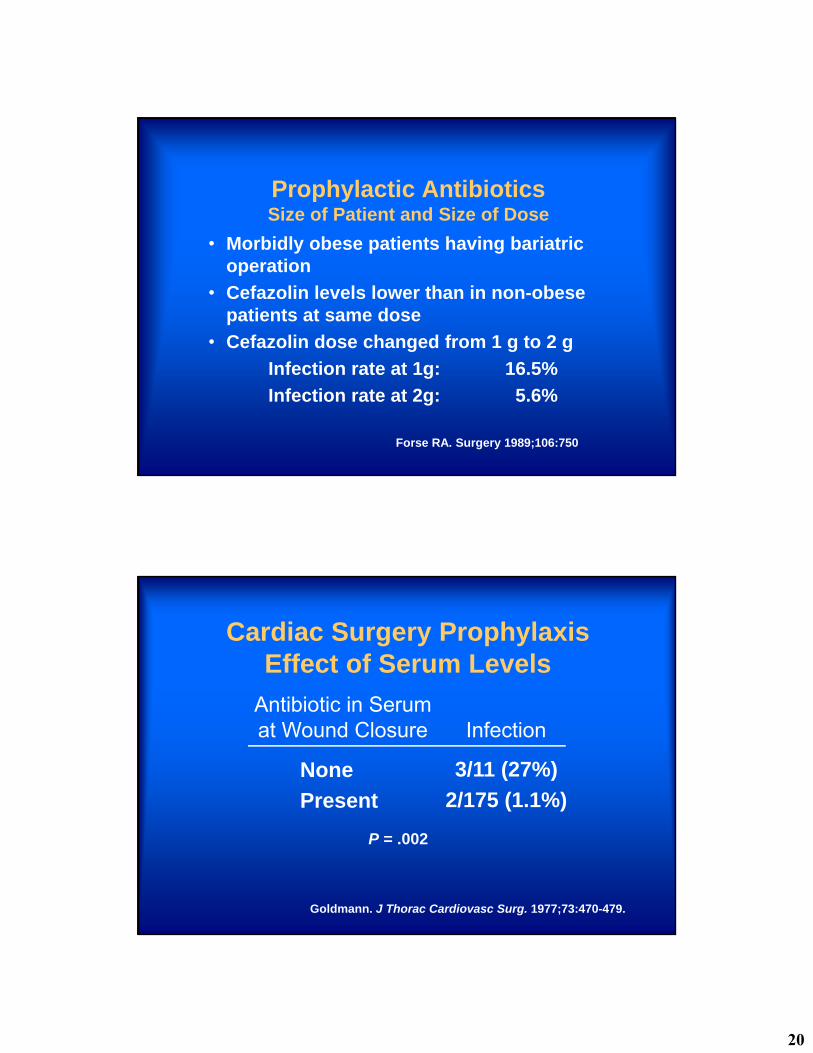
Prophylactic AntibioticsSize of Patient and Size of Dose
• Morbidly obese patients having bariatric operation
• Cefazolin levels lower than in non-obese patients at same dose
• Cefazolin dose changed from 1 g to 2 g
Infection rate at 1g: 16.5%
Infection rate at 2g: 5.6%
Forse RA. Surgery 1989;106:750
Cardiac Surgery ProphylaxisEffect of Serum Levels
None
Present
3/11 (27%)
2/175 (1.1%)
Antibiotic in Serumat Wound Closure Infection
Goldmann. J Thorac Cardiovasc Surg. 1977;73:470-479.
P = .002
21
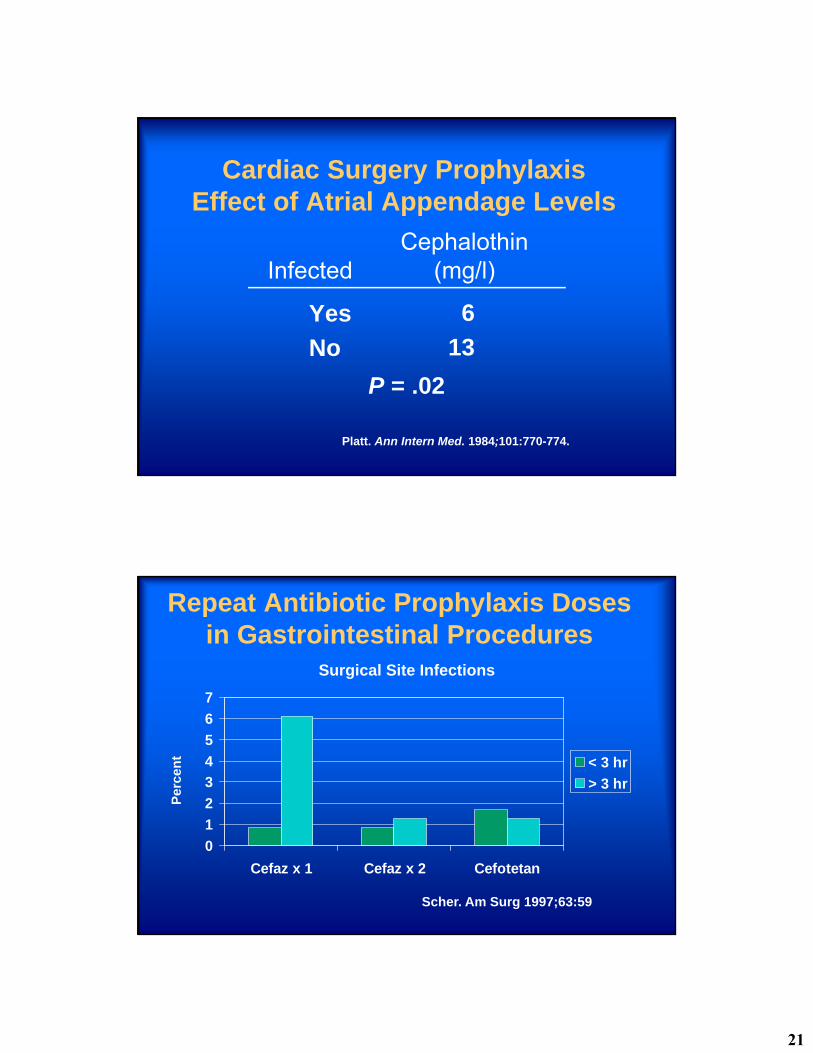
Cardiac Surgery ProphylaxisEffect of Atrial Appendage Levels
Yes
No
6
13
InfectedCephalothin
(mg/l)
Platt. Ann Intern Med. 1984;101:770-774.
P = .02
Repeat Antibiotic Prophylaxis Doses in Gastrointestinal Procedures
0
1
2
3
4
5
6
7
Cefaz x 1 Cefaz x 2 Cefotetan
< 3 hr
> 3 hr
Surgical Site Infections
Per
cen
t
Scher. Am Surg 1997;63:59
22
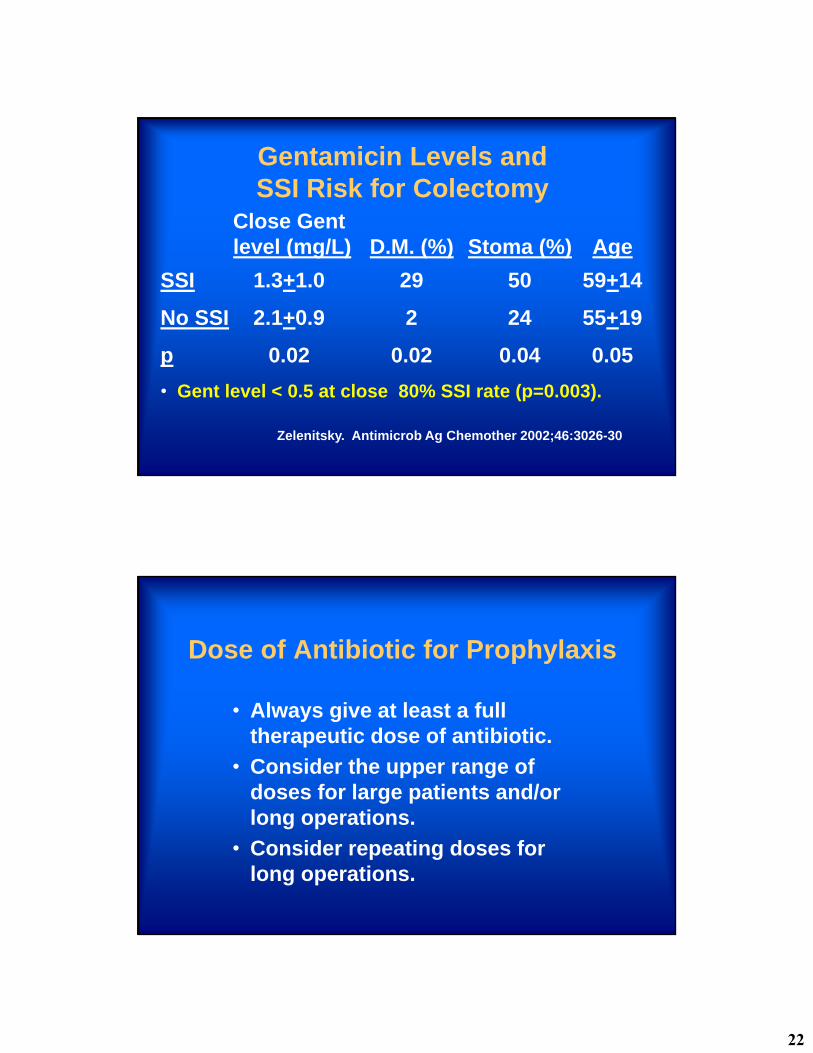
Gentamicin Levels andSSI Risk for Colectomy
Close Gentlevel (mg/L) D.M. (%) Stoma (%) Age
SSI 1.3+1.0 29 50 59+14
No SSI 2.1+0.9 2 24 55+19
p 0.02 0.02 0.04 0.05
• Gent level < 0.5 at close 80% SSI rate (p=0.003).
Zelenitsky. Antimicrob Ag Chemother 2002;46:3026-30
Dose of Antibiotic for Prophylaxis
• Always give at least a full therapeutic dose of antibiotic.
• Consider the upper range of doses for large patients and/or long operations.
• Consider repeating doses for long operations.
23
Prophylactic AntibioticsQuestions
• Which cases benefit?
• Which drug should you use?
• When should you start?
• How much should you give?
• How long should antibiotics be continued?
Antibiotic ProphylaxisDuration
Most studies have confirmed efficacy of ≤12 hrs.
Many studies have shown efficacy of a single dose.
Whenever compared, the shorter course has been as effective as the longer course.
24
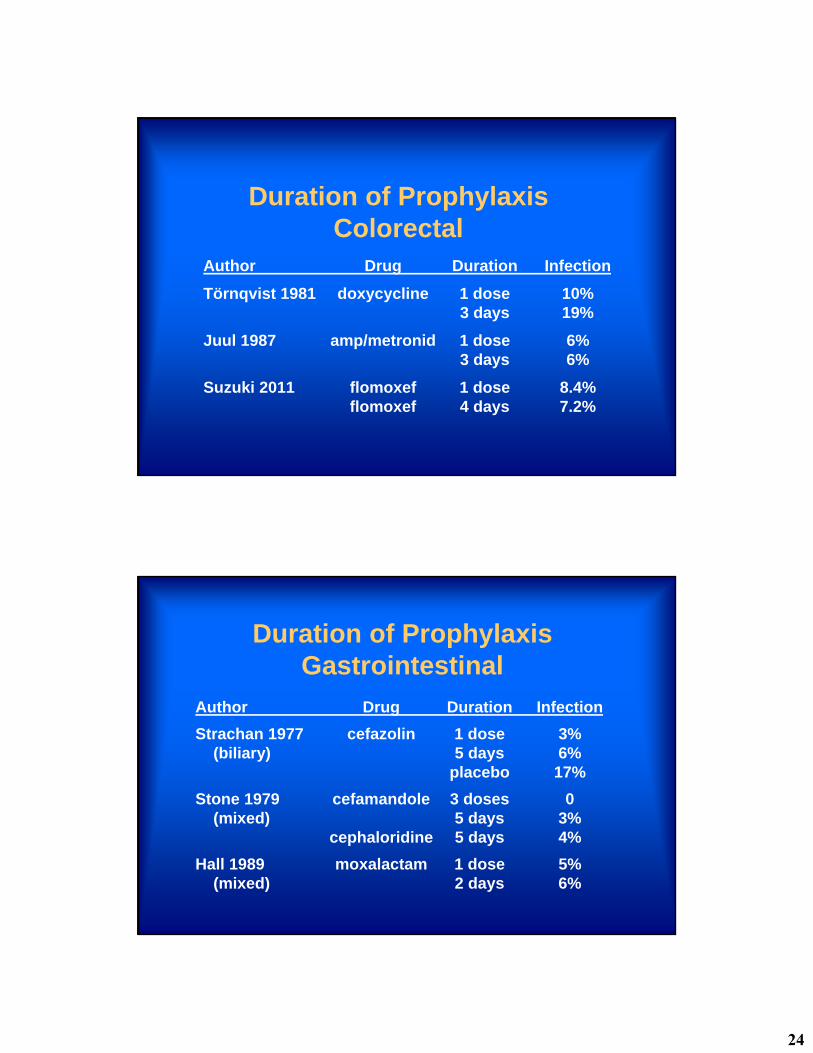
Duration of ProphylaxisColorectal
Author Drug Duration Infection
Törnqvist 1981 doxycycline 1 dose 10%3 days 19%
Juul 1987 amp/metronid 1 dose 6%3 days 6%
Suzuki 2011 flomoxef 1 dose 8.4%flomoxef 4 days 7.2%
Duration of ProphylaxisGastrointestinal
Author Drug Duration Infection
Strachan 1977 cefazolin 1 dose 3%(biliary) 5 days 6%
placebo 17%
Stone 1979 cefamandole 3 doses 0(mixed) 5 days 3%
cephaloridine 5 days 4%
Hall 1989 moxalactam 1 dose 5%(mixed) 2 days 6%
25
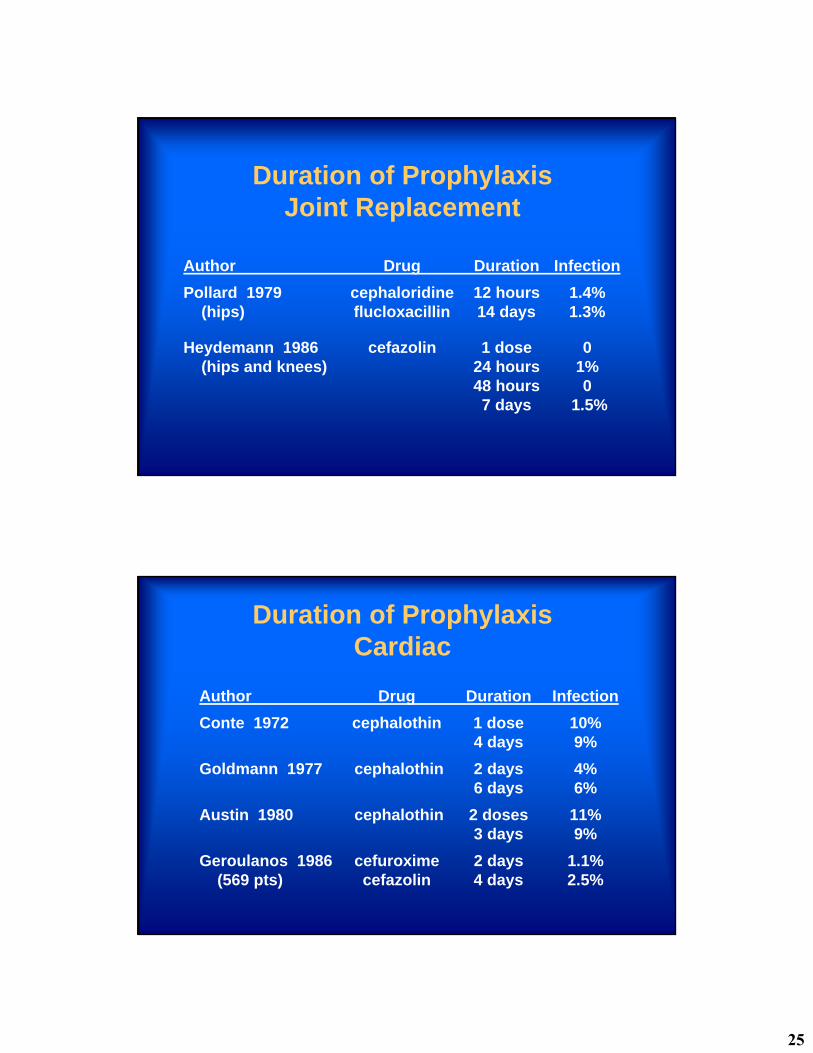
Duration of ProphylaxisJoint Replacement
Author Drug Duration Infection
Pollard 1979 cephaloridine 12 hours 1.4%(hips) flucloxacillin 14 days 1.3%
Heydemann 1986 cefazolin 1 dose 0(hips and knees) 24 hours 1%
48 hours 07 days 1.5%
Duration of ProphylaxisCardiac
Author Drug Duration Infection
Conte 1972 cephalothin 1 dose 10%4 days 9%
Goldmann 1977 cephalothin 2 days 4%6 days 6%
Austin 1980 cephalothin 2 doses 11%3 days 9%
Geroulanos 1986 cefuroxime 2 days 1.1%(569 pts) cefazolin 4 days 2.5%
26
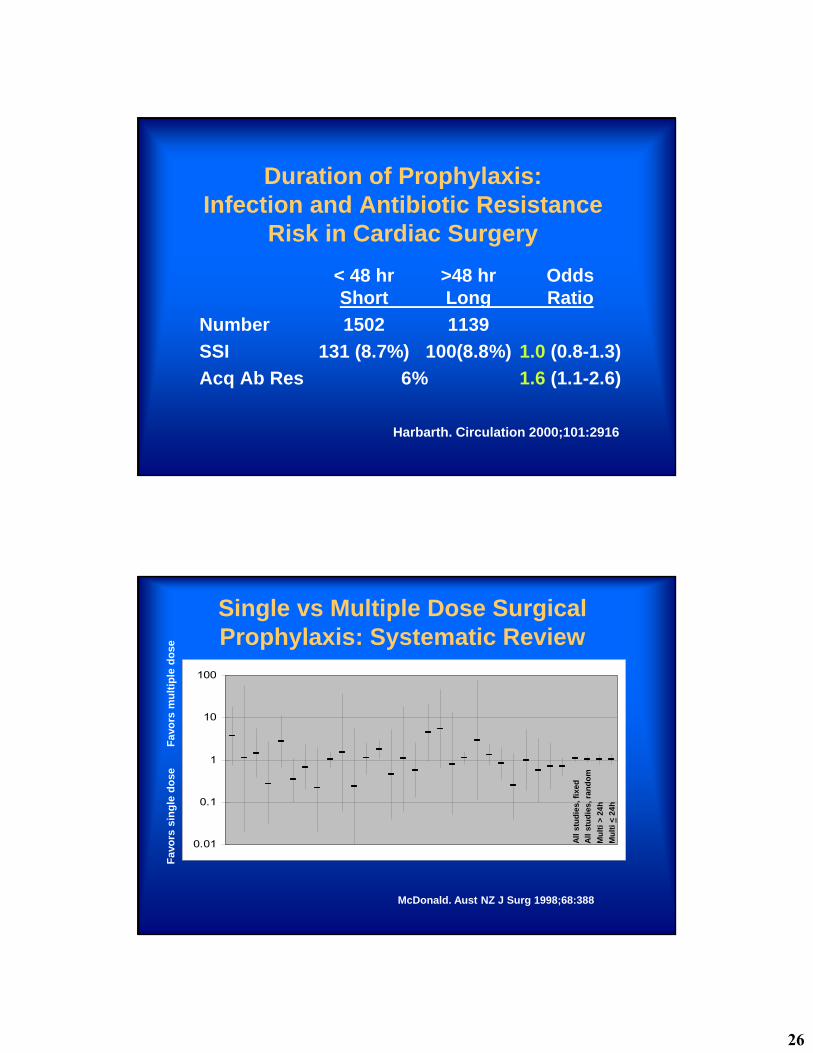
Duration of Prophylaxis:Infection and Antibiotic Resistance
Risk in Cardiac Surgery
< 48 hr >48 hr OddsShort Long Ratio
Number 1502 1139
SSI 131 (8.7%) 100(8.8%) 1.0 (0.8-1.3)
Acq Ab Res 6% 1.6 (1.1-2.6)
Harbarth. Circulation 2000;101:2916
Single vs Multiple Dose Surgical Prophylaxis: Systematic Review
0.01
0.1
1
10
100
McDonald. Aust NZ J Surg 1998;68:388
All
stu
die
s, f
ixe
d
All
stu
die
s, r
and
om
Mu
lti
> 2
4h
Mu
lti
<2
4h
Fav
ors
sin
gle
do
seF
avo
rs m
ult
iple
do
se
27
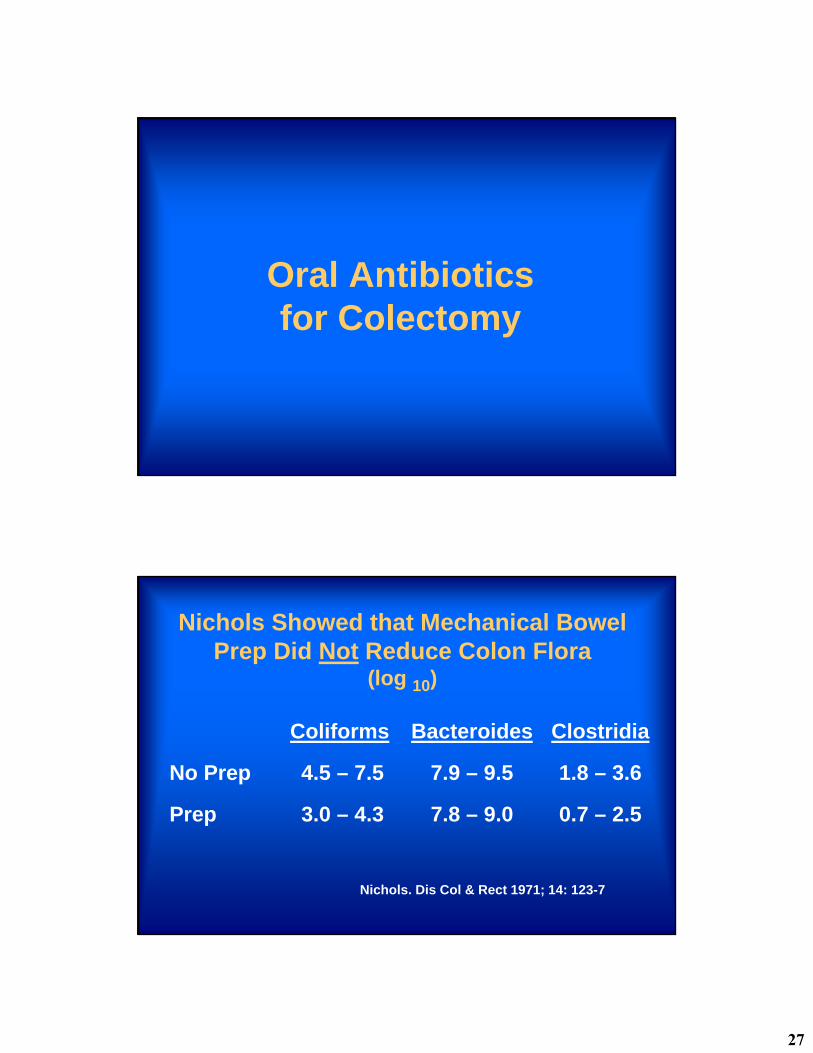
Oral Antibioticsfor Colectomy
Nichols Showed that Mechanical Bowel Prep Did Not Reduce Colon Flora
(log 10)
Coliforms Bacteroides Clostridia
No Prep 4.5 – 7.5 7.9 – 9.5 1.8 – 3.6
Prep 3.0 – 4.3 7.8 – 9.0 0.7 – 2.5
Nichols. Dis Col & Rect 1971; 14: 123-7
28
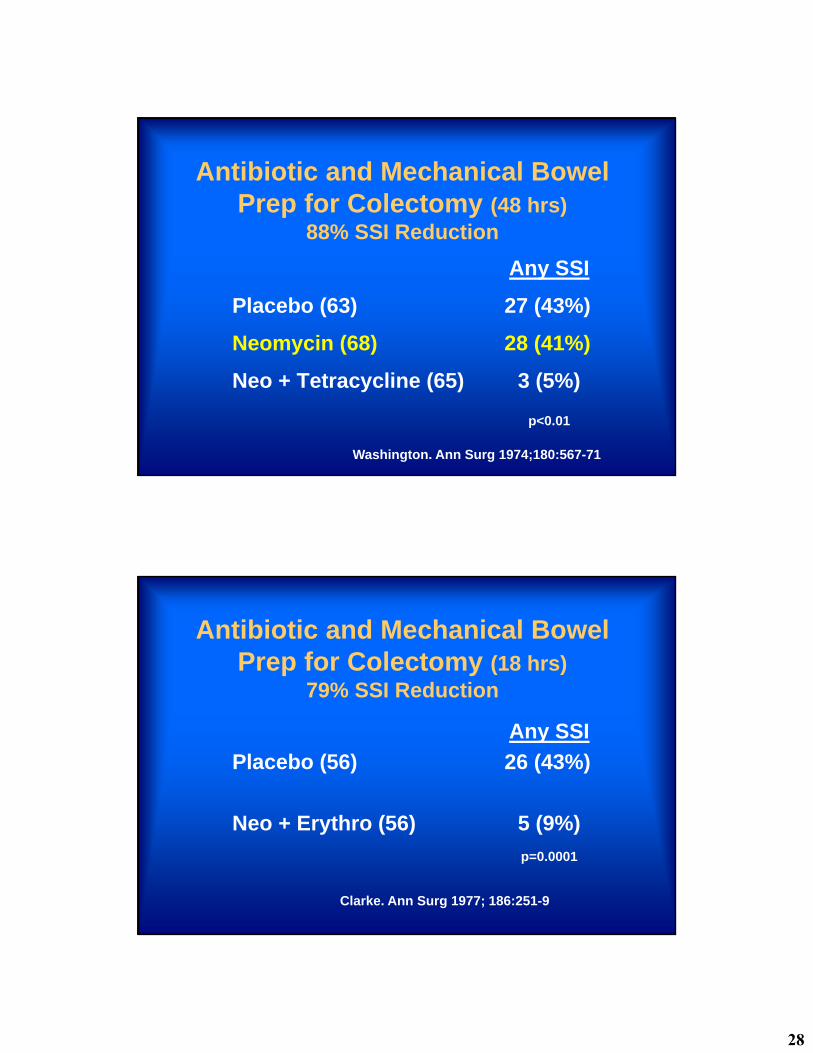
Antibiotic and Mechanical Bowel Prep for Colectomy (48 hrs)
88% SSI Reduction
Any SSI
Placebo (63) 27 (43%)
Neomycin (68) 28 (41%)
Neo + Tetracycline (65) 3 (5%)
p<0.01
Washington. Ann Surg 1974;180:567-71
Antibiotic and Mechanical Bowel Prep for Colectomy (18 hrs)
79% SSI Reduction
Any SSI
Placebo (56) 26 (43%)
Neo + Erythro (56) 5 (9%)
p=0.0001
Clarke. Ann Surg 1977; 186:251-9
29
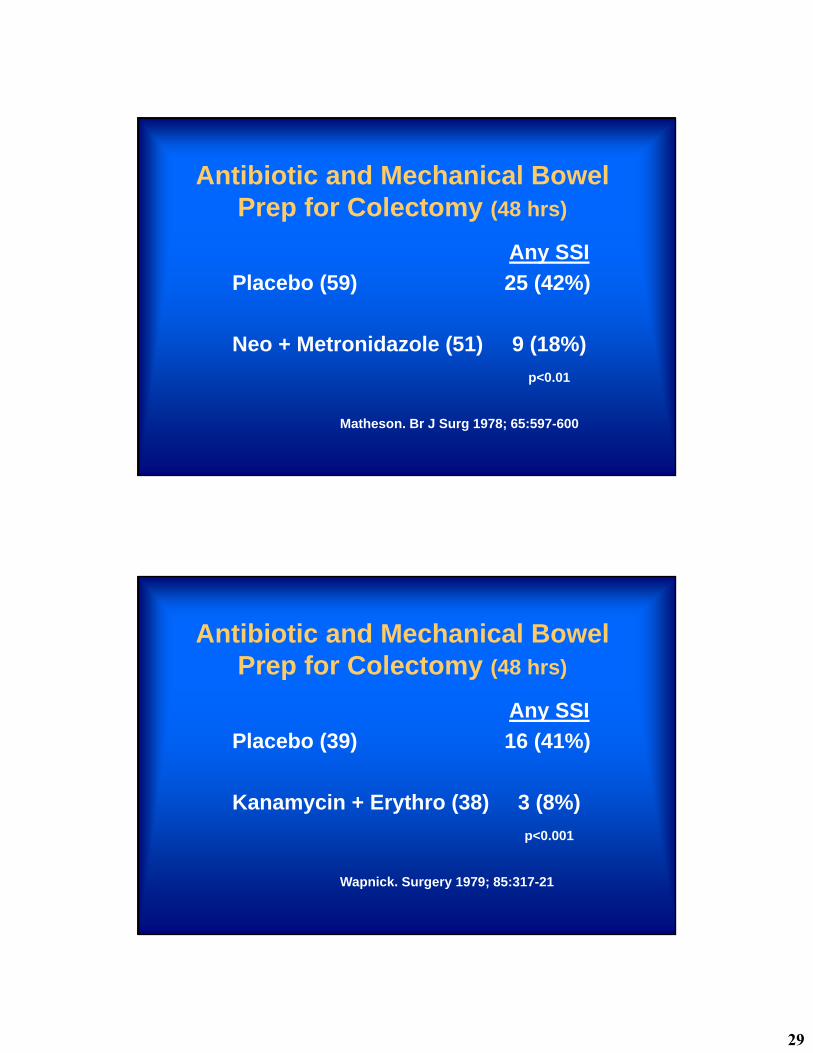
Antibiotic and Mechanical Bowel Prep for Colectomy (48 hrs)
Any SSI
Placebo (59) 25 (42%)
Neo + Metronidazole (51) 9 (18%)
p<0.01
Matheson. Br J Surg 1978; 65:597-600
Antibiotic and Mechanical Bowel Prep for Colectomy (48 hrs)
Any SSI
Placebo (39) 16 (41%)
Kanamycin + Erythro (38) 3 (8%)
p<0.001
Wapnick. Surgery 1979; 85:317-21
30
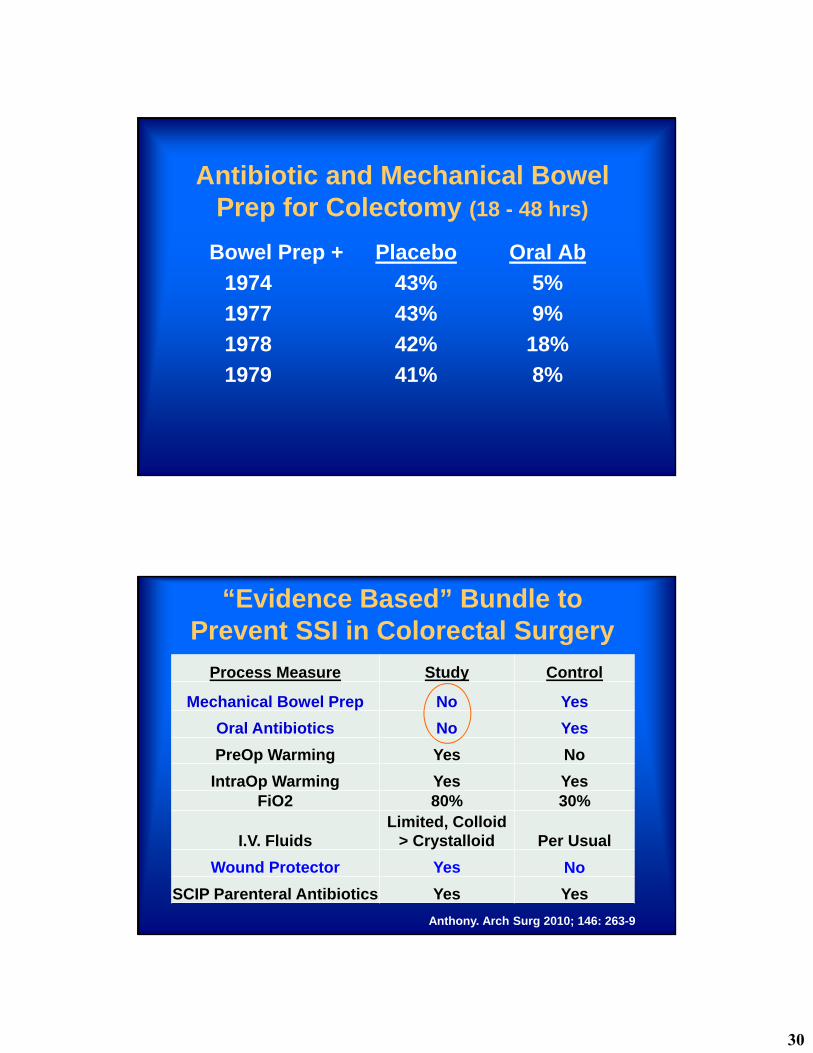
Antibiotic and Mechanical Bowel Prep for Colectomy (18 - 48 hrs)
Bowel Prep + Placebo Oral Ab
1974 43% 5%
1977 43% 9%
1978 42% 18%
1979 41% 8%
“Evidence Based” Bundle to Prevent SSI in Colorectal Surgery
Process Measure Study Control
Mechanical Bowel Prep No Yes
Oral Antibiotics No Yes
PreOp Warming Yes No
IntraOp Warming Yes YesFiO2 80% 30%
I.V. FluidsLimited, Colloid
> Crystalloid Per Usual
Wound Protector Yes No
SCIP Parenteral Antibiotics Yes Yes
Anthony. Arch Surg 2010; 146: 263-9
31
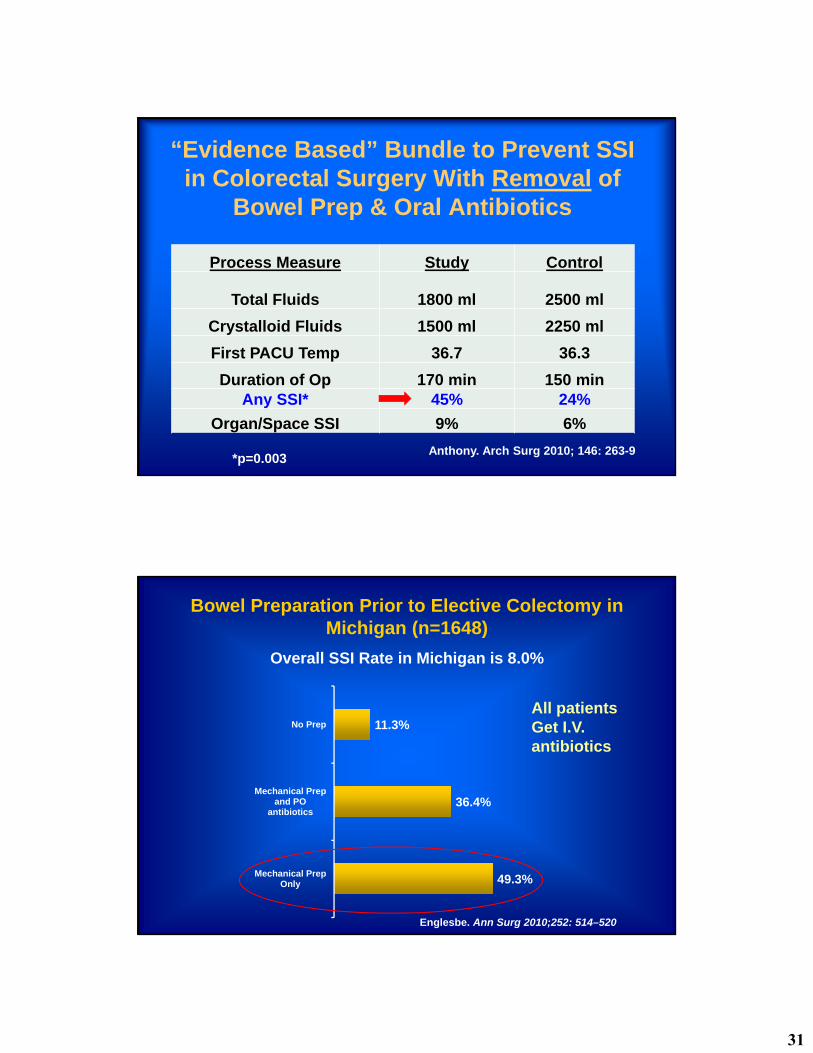
“Evidence Based” Bundle to Prevent SSI in Colorectal Surgery With Removal of
Bowel Prep & Oral Antibiotics
Process Measure Study Control
Total Fluids 1800 ml 2500 ml
Crystalloid Fluids 1500 ml 2250 ml
First PACU Temp 36.7 36.3
Duration of Op 170 min 150 minAny SSI* 45% 24%
Organ/Space SSI 9% 6%
Anthony. Arch Surg 2010; 146: 263-9*p=0.003
49.3%
36.4%
11.3%
Mechanical PrepOnly
Mechanical Prepand PO
antibiotics
No Prep
Bowel Preparation Prior to Elective Colectomy in Michigan (n=1648)
Overall SSI Rate in Michigan is 8.0%
Englesbe. Ann Surg 2010;252: 514–520
All patientsGet I.V. antibiotics
32
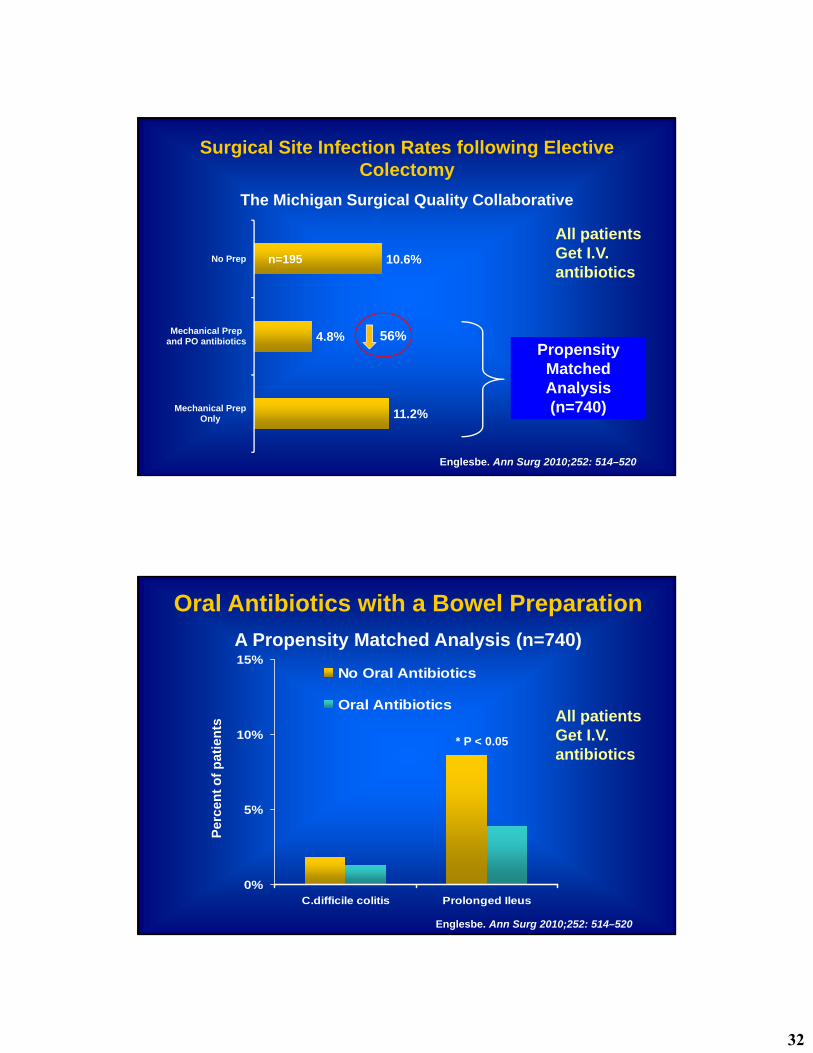
11.2%
4.8%
10.6%
Mechanical PrepOnly
Mechanical Prepand PO antibiotics
No Prep
Surgical Site Infection Rates following Elective Colectomy
The Michigan Surgical Quality Collaborative
Propensity Matched Analysis(n=740)
Englesbe. Ann Surg 2010;252: 514–520
n=195
All patientsGet I.V. antibiotics
56%
0%
5%
10%
15%
C.difficile colitis Prolonged Ileus
No Oral Antibiotics
Oral Antibiotics
Per
cen
t o
f p
atie
nts
* P < 0.05
Oral Antibiotics with a Bowel Preparation
A Propensity Matched Analysis (n=740)
Englesbe. Ann Surg 2010;252: 514–520
All patientsGet I.V. antibiotics
33
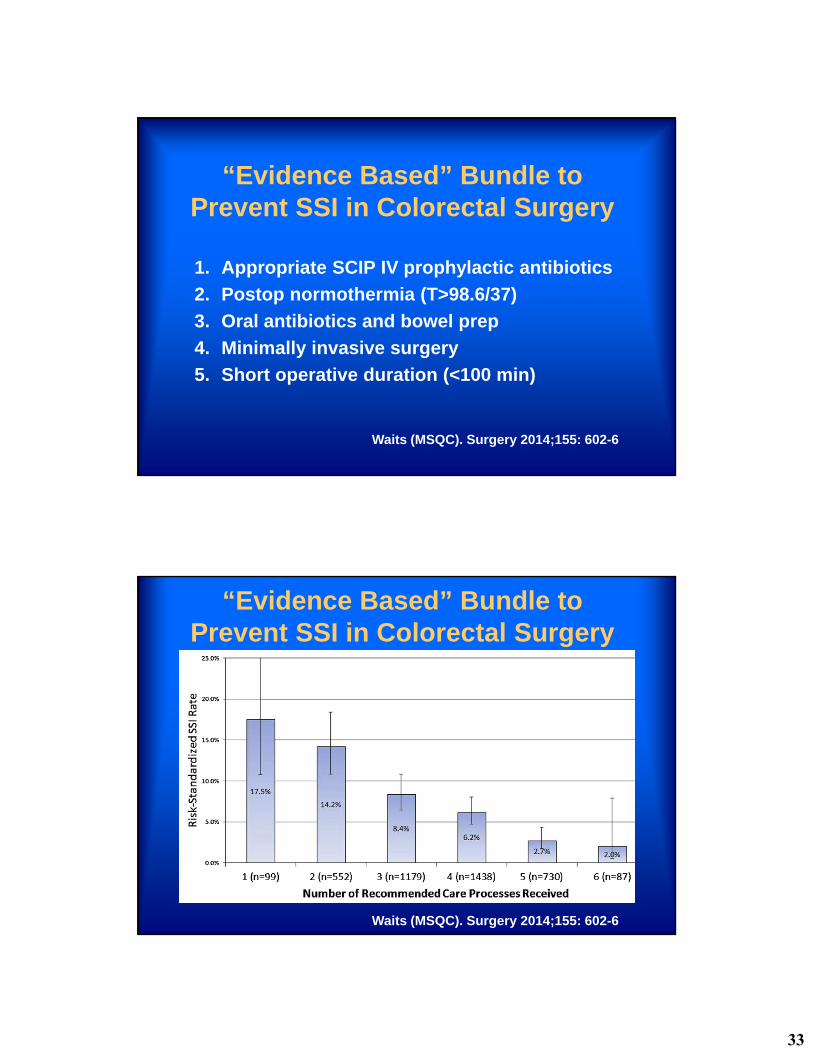
“Evidence Based” Bundle to Prevent SSI in Colorectal Surgery
1. Appropriate SCIP IV prophylactic antibiotics
2. Postop normothermia (T>98.6/37)
3. Oral antibiotics and bowel prep
4. Minimally invasive surgery
5. Short operative duration (<100 min)
Waits (MSQC). Surgery 2014;155: 602-6
“Evidence Based” Bundle to Prevent SSI in Colorectal Surgery
Waits (MSQC). Surgery 2014;155: 602-6
34
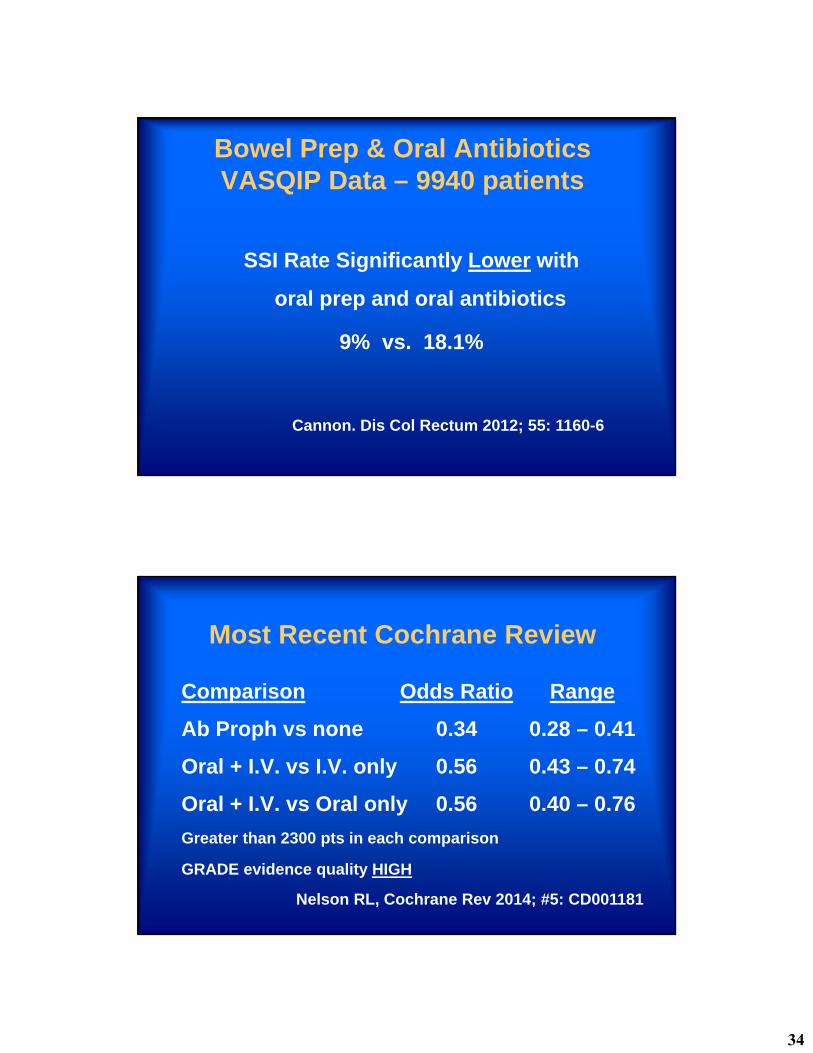
Bowel Prep & Oral AntibioticsVASQIP Data – 9940 patients
Cannon. Dis Col Rectum 2012; 55: 1160-6
SSI Rate Significantly Lower with
oral prep and oral antibiotics
9% vs. 18.1%
Most Recent Cochrane Review
Comparison Odds Ratio Range
Ab Proph vs none 0.34 0.28 – 0.41
Oral + I.V. vs I.V. only 0.56 0.43 – 0.74
Oral + I.V. vs Oral only 0.56 0.40 – 0.76
Greater than 2300 pts in each comparison
GRADE evidence quality HIGH
Nelson RL, Cochrane Rev 2014; #5: CD001181
35
Oral Antibiotic Bowel Prep Significantly Reduces SSI Rates and Readmission Rates in Elective Colorectal Surgery
NSQIP data on 8,415 colectomy pts
Open and Laparoscopic
No Prep 2150 25%
Mech Prep Only 3779 45%
Oral Ab + Mech Prep 2486 30%
Morris. Ann Surg 2015; 261:1034-40
Oral Antibiotic Bowel Prep Significantly Reduces SSI Rates and Readmission Rates in Elective Colorectal Surgery
NSQIP data on 8,415 colectomy pts
Open and Laparoscopic
SSI
Oral Ab 6.5%
No Oral Ab 13%
Morris. Ann Surg 2015; 261:1034-40
36
Oral Antibiotic Bowel Prep Significantly Reduces Complication Rates in
Elective Colorectal Surgery
Reduced P
Anastomotic leak < 0.001
Ileus < 0.001
Return to O.R. 0.02
Readmission < 0.001
Mortality 0.001
Morris. Ann Surg 2015; 261:1034-40
Oral Antibiotic Bowel Prep Significantly Reduces SSI Rates and Readmission Rates in Elective Colorectal Surgery
Targeted Colorectal NSQIP data on 4,999 pts, Open and Laparoscopic with detailed data on mechanical prep, use of oral antibiotics, operative approach and multiple other risk factors.
Scarborough. Ann Surg 2015; 262(2):331-7
37
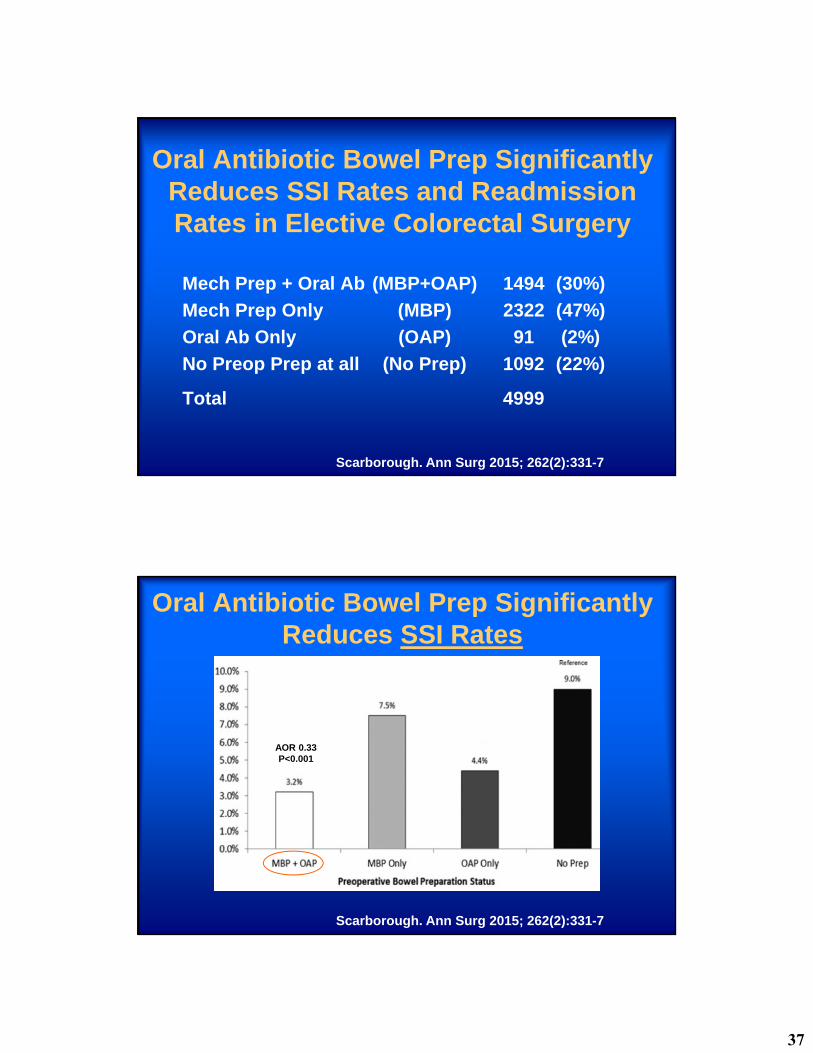
Oral Antibiotic Bowel Prep Significantly Reduces SSI Rates and Readmission Rates in Elective Colorectal Surgery
Mech Prep + Oral Ab (MBP+OAP) 1494 (30%)
Mech Prep Only (MBP) 2322 (47%)
Oral Ab Only (OAP) 91 (2%)
No Preop Prep at all (No Prep) 1092 (22%)
Total 4999
Scarborough. Ann Surg 2015; 262(2):331-7
Oral Antibiotic Bowel Prep Significantly Reduces SSI Rates
AOR 0.33P<0.001
Scarborough. Ann Surg 2015; 262(2):331-7
38
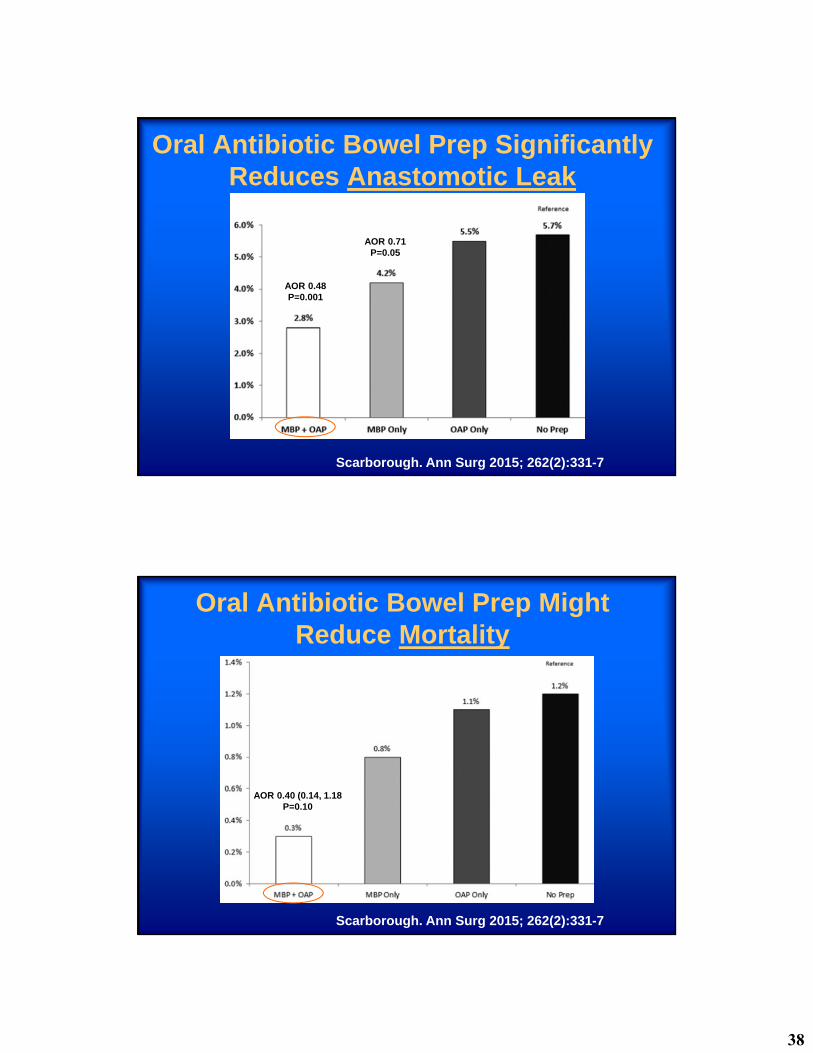
Oral Antibiotic Bowel Prep Significantly Reduces Anastomotic Leak
AOR 0.48P=0.001
AOR 0.71P=0.05
Scarborough. Ann Surg 2015; 262(2):331-7
Oral Antibiotic Bowel Prep Might Reduce Mortality
Scarborough. Ann Surg 2015; 262(2):331-7
AOR 0.40 (0.14, 1.18P=0.10
39
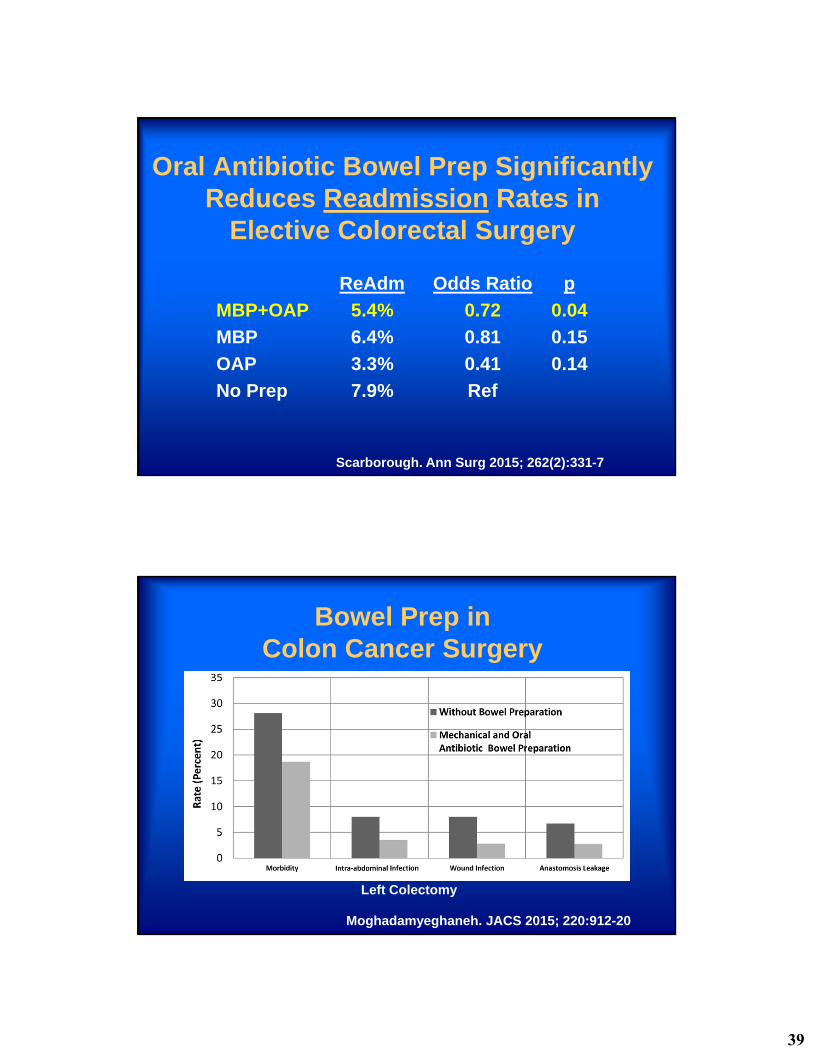
Oral Antibiotic Bowel Prep Significantly Reduces Readmission Rates in
Elective Colorectal Surgery
ReAdm Odds Ratio p
MBP+OAP 5.4% 0.72 0.04
MBP 6.4% 0.81 0.15
OAP 3.3% 0.41 0.14
No Prep 7.9% Ref
Scarborough. Ann Surg 2015; 262(2):331-7
Bowel Prep inColon Cancer Surgery
Moghadamyeghaneh. JACS 2015; 220:912-20
Left Colectomy
40
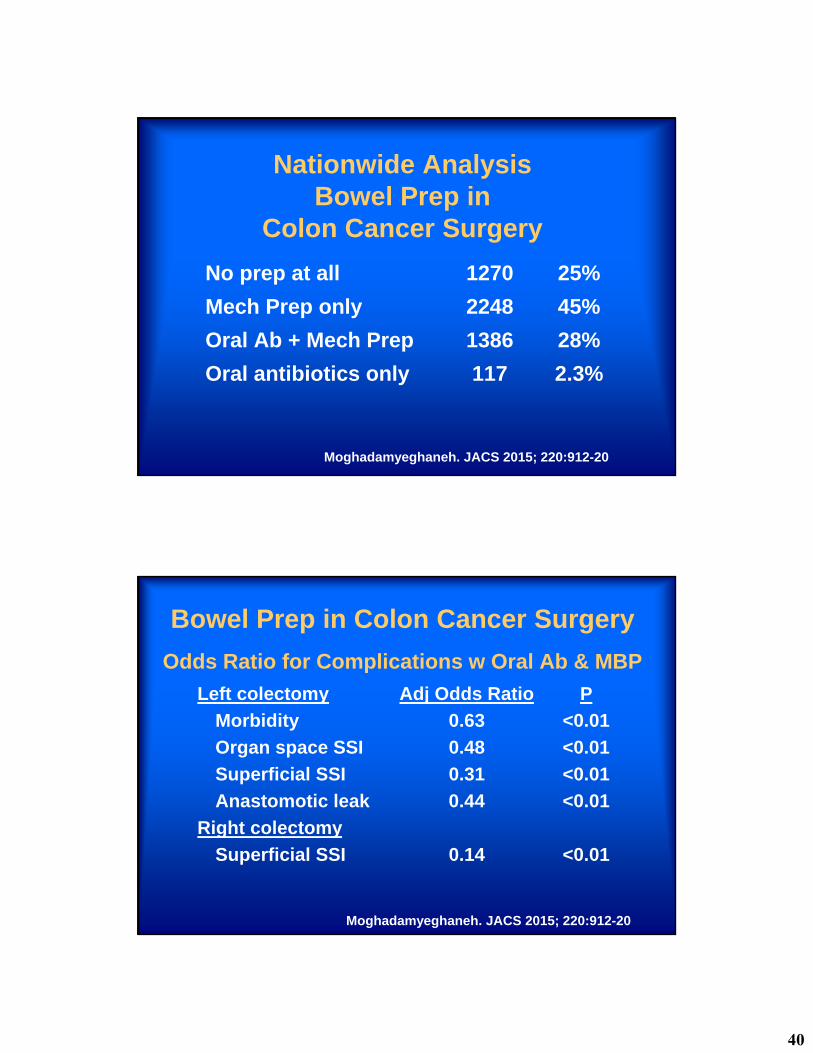
Nationwide AnalysisBowel Prep in
Colon Cancer Surgery
No prep at all 1270 25%
Mech Prep only 2248 45%
Oral Ab + Mech Prep 1386 28%
Oral antibiotics only 117 2.3%
Moghadamyeghaneh. JACS 2015; 220:912-20
Left colectomy Adj Odds Ratio P
Morbidity 0.63 <0.01
Organ space SSI 0.48 <0.01
Superficial SSI 0.31 <0.01
Anastomotic leak 0.44 <0.01
Right colectomy
Superficial SSI 0.14 <0.01
Bowel Prep in Colon Cancer Surgery
Odds Ratio for Complications w Oral Ab & MBP
Moghadamyeghaneh. JACS 2015; 220:912-20
41
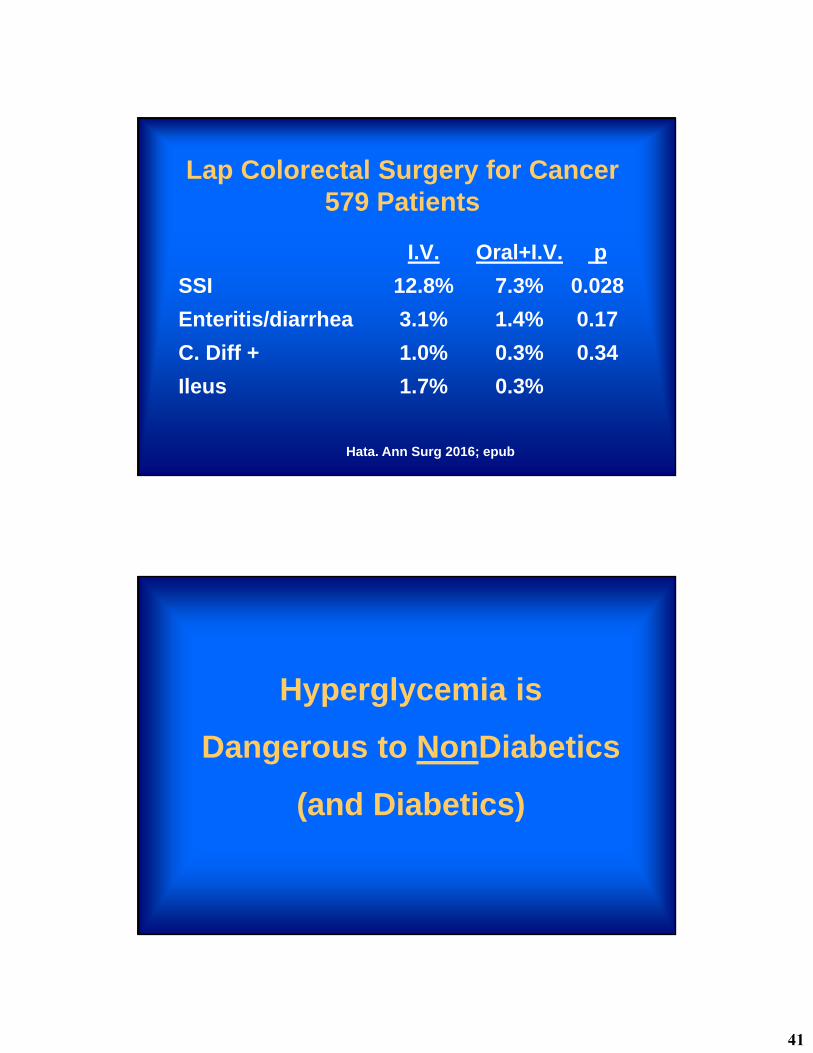
Lap Colorectal Surgery for Cancer579 Patients
I.V. Oral+I.V. p
SSI 12.8% 7.3% 0.028
Enteritis/diarrhea 3.1% 1.4% 0.17
C. Diff + 1.0% 0.3% 0.34
Ileus 1.7% 0.3%
Hata. Ann Surg 2016; epub
Hyperglycemia is
Dangerous to NonDiabetics
(and Diabetics)
42
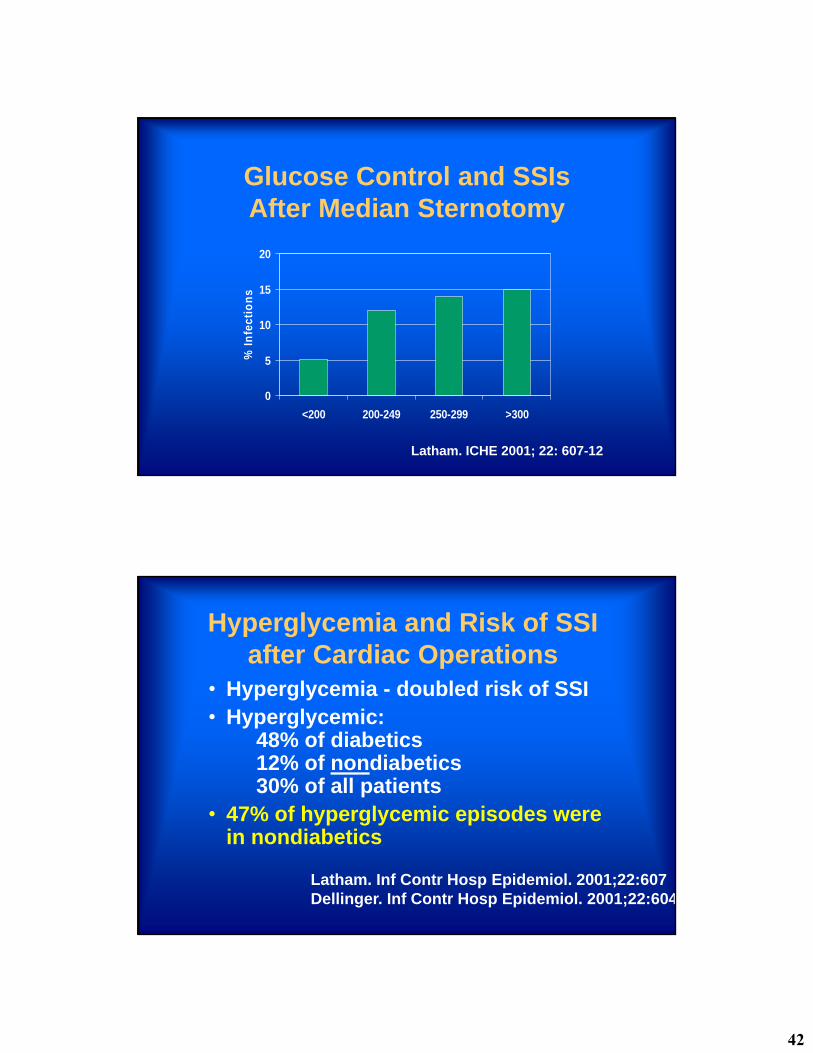
Glucose Control and SSIsAfter Median Sternotomy
0
5
10
15
20
<200 200-249 250-299 >300
% I
nfe
ctio
ns
Latham. ICHE 2001; 22: 607-12
Hyperglycemia and Risk of SSI after Cardiac Operations
• Hyperglycemia - doubled risk of SSI• Hyperglycemic:
48% of diabetics12% of nondiabetics30% of all patients
• 47% of hyperglycemic episodes were in nondiabetics
Latham. Inf Contr Hosp Epidemiol. 2001;22:607Dellinger. Inf Contr Hosp Epidemiol. 2001;22:604
43
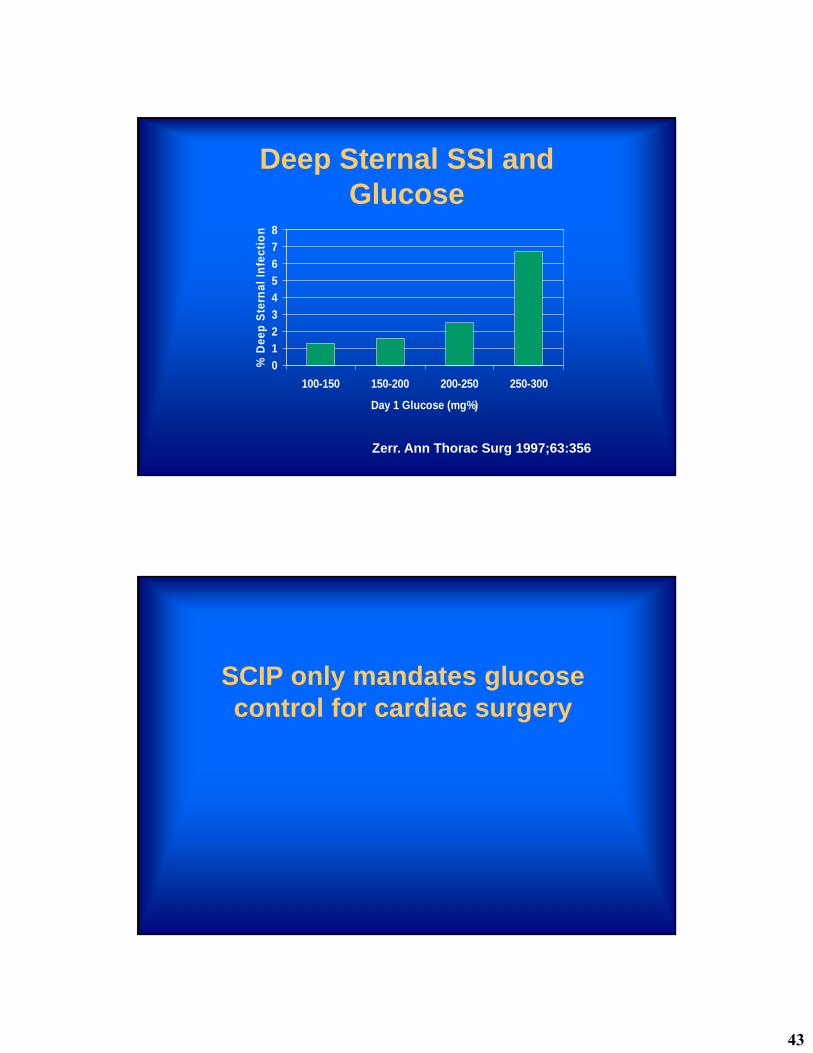
Deep Sternal SSI and Glucose
0
1
2
3
4
5
6
7
8
100-150 150-200 200-250 250-300
Day 1 Glucose (mg%)
% D
eep
Ste
rnal
In
fect
ion
Zerr. Ann Thorac Surg 1997;63:356
SCIP only mandates glucose control for cardiac surgery
44
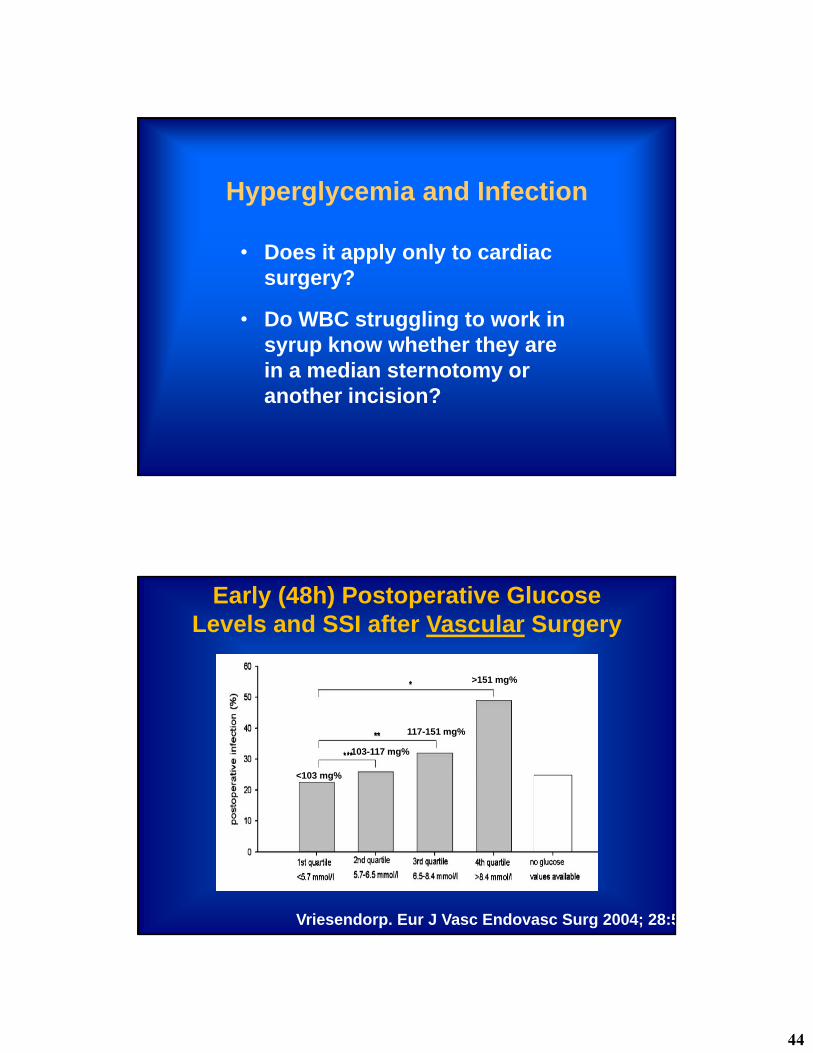
Hyperglycemia and Infection
• Does it apply only to cardiac surgery?
• Do WBC struggling to work in syrup know whether they are in a median sternotomy or another incision?
Early (48h) Postoperative Glucose Levels and SSI after Vascular Surgery
Vriesendorp. Eur J Vasc Endovasc Surg 2004; 28:5
<103 mg%
103-117 mg%
117-151 mg%
>151 mg%
45
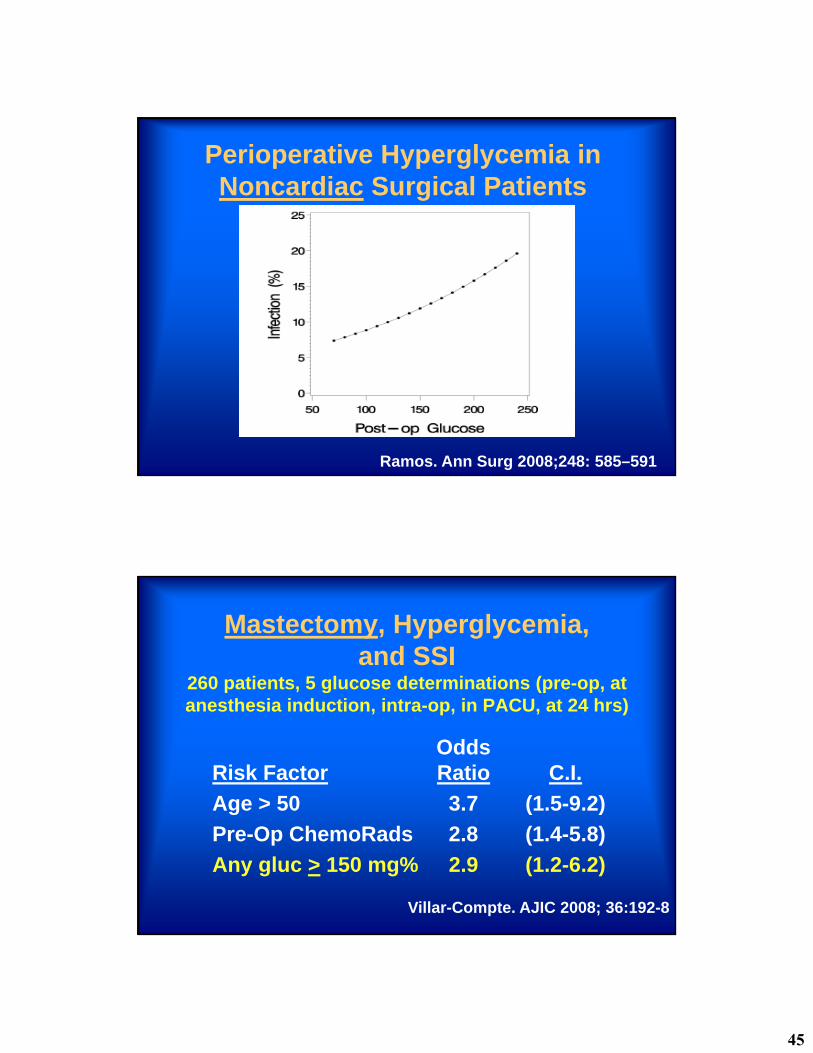
Perioperative Hyperglycemia in Noncardiac Surgical Patients
Ramos. Ann Surg 2008;248: 585–591
Mastectomy, Hyperglycemia,and SSI
260 patients, 5 glucose determinations (pre-op, at anesthesia induction, intra-op, in PACU, at 24 hrs)
OddsRisk Factor Ratio C.I.
Age > 50 3.7 (1.5-9.2)
Pre-Op ChemoRads 2.8 (1.4-5.8)
Any gluc > 150 mg% 2.9 (1.2-6.2)
Villar-Compte. AJIC 2008; 36:192-8

46
Postop Glucose (within 48h) and SSI – General Surgery
Ata. Arch Surg 2010: 145: 858-864
Glucose
Postoperative Glucose and Mortality in Noncardiac Surgery
Hyperglycemia in nondiabetic
patients was more dangerous
than hyperglycemia in diabetics!
Frisch. Diabetes Care. 2010; 33: 1883-8
47
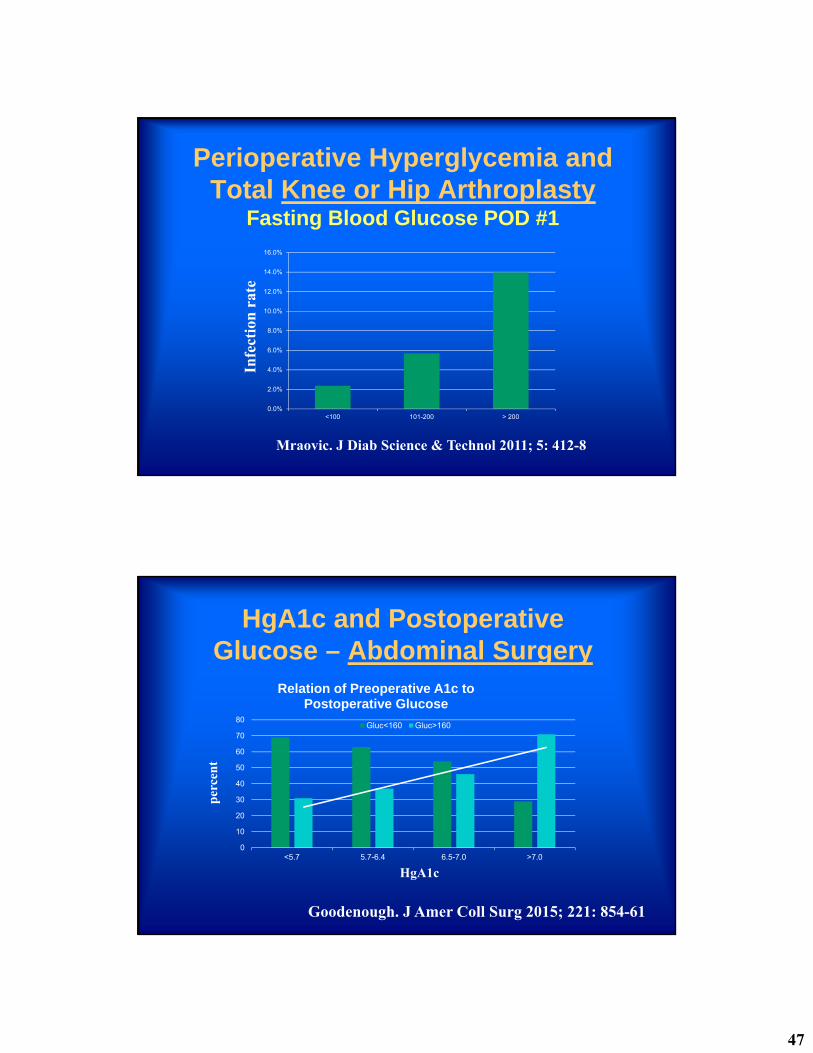
Perioperative Hyperglycemia and Total Knee or Hip Arthroplasty
Fasting Blood Glucose POD #1
Mraovic. J Diab Science & Technol 2011; 5: 412-8
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
<100 101-200 > 200
Infe
ctio
n r
ate
HgA1c and Postoperative Glucose – Abdominal Surgery
0
10
20
30
40
50
60
70
80
<5.7 5.7-6.4 6.5-7.0 >7.0
Relation of Preoperative A1c to Postoperative Glucose
Gluc<160 Gluc>160
Goodenough. J Amer Coll Surg 2015; 221: 854-61
HgA1c
per
cen
t
48
Glucose & Infection RiskNon-Cardiac Surgery & Diabetes
VASQIP – 55,408 patients
Multivariate analysis:• All the usual risk factors significant.
• HgbA1c NOT significant.
• PreOp glucose NOT significant.
• PostOp glucose > 150 very significant.
King. Ann Surg 2011; 253:158-65
Hgb A1c vs. Glucose as Risk Factor for SSI – Gastric Bypass
Multivariate Analysis
Odds ratio = 1.27 for every20 mg% increase in mean glucose level during hospitalization (p=0.008).
Mean glucose more significant than any single level above 200 Mg% or not.
Hgb A1c not significant.
Perna. Surg Obes Rel Dis 2012; 8: 685-90
49
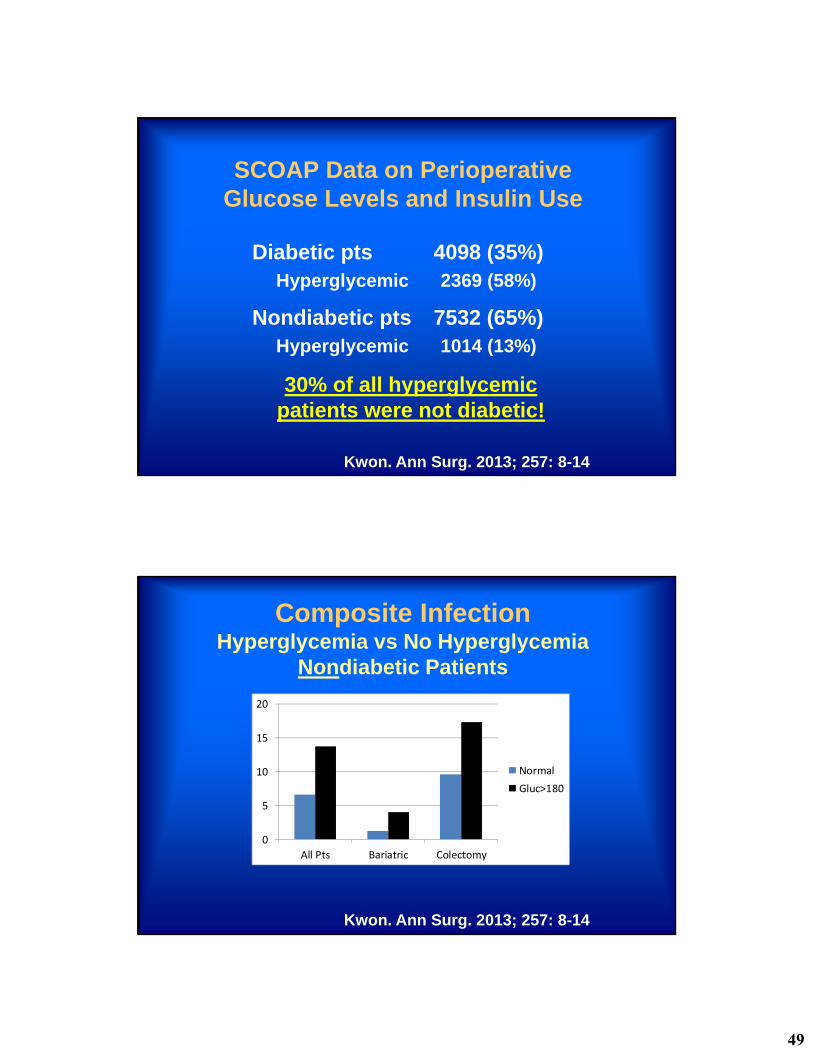
SCOAP Data on Perioperative Glucose Levels and Insulin Use
Diabetic pts 4098 (35%)Hyperglycemic 2369 (58%)
Nondiabetic pts 7532 (65%)Hyperglycemic 1014 (13%)
30% of all hyperglycemic patients were not diabetic!
Kwon. Ann Surg. 2013; 257: 8-14
Composite InfectionHyperglycemia vs No Hyperglycemia
Nondiabetic Patients
0
5
10
15
20
All Pts Bariatric Colectomy
NormalGluc>180
All p<0.01
Kwon. Ann Surg. 2013; 257: 8-14
50
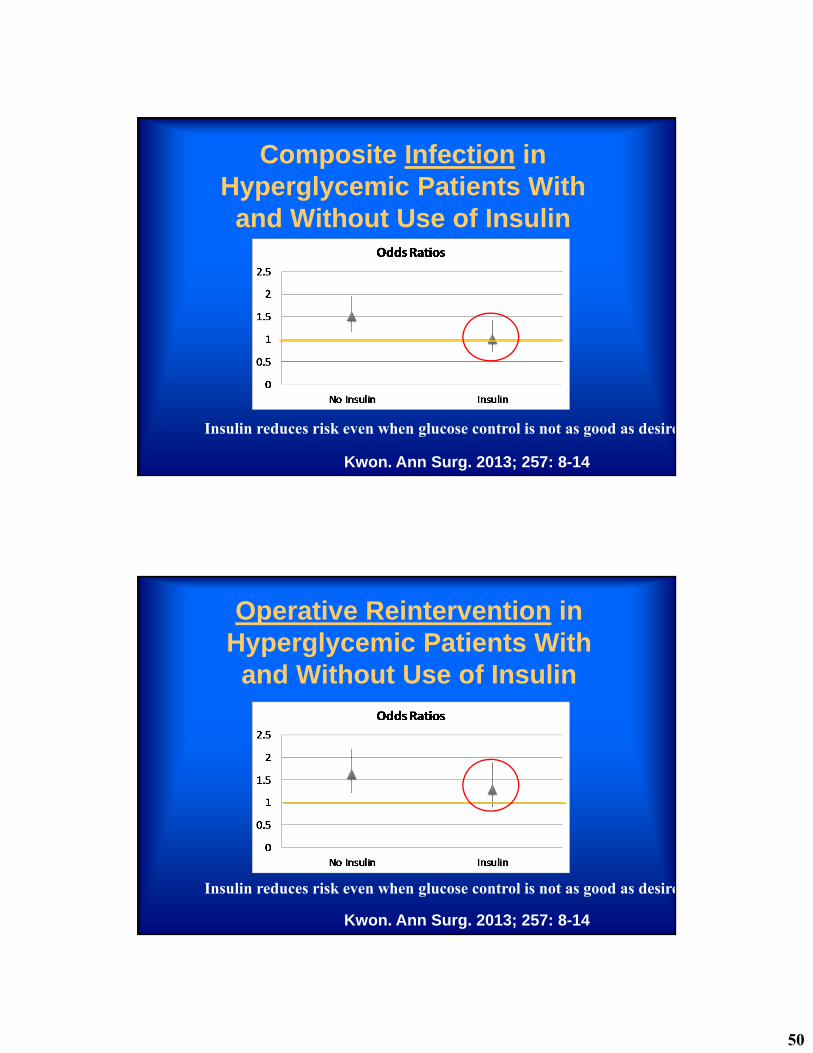
Composite Infection in Hyperglycemic Patients With
and Without Use of Insulin
Kwon. Ann Surg. 2013; 257: 8-14
Insulin reduces risk even when glucose control is not as good as desire
Operative Reintervention in Hyperglycemic Patients With
and Without Use of Insulin
Kwon. Ann Surg. 2013; 257: 8-14
Insulin reduces risk even when glucose control is not as good as desire
51
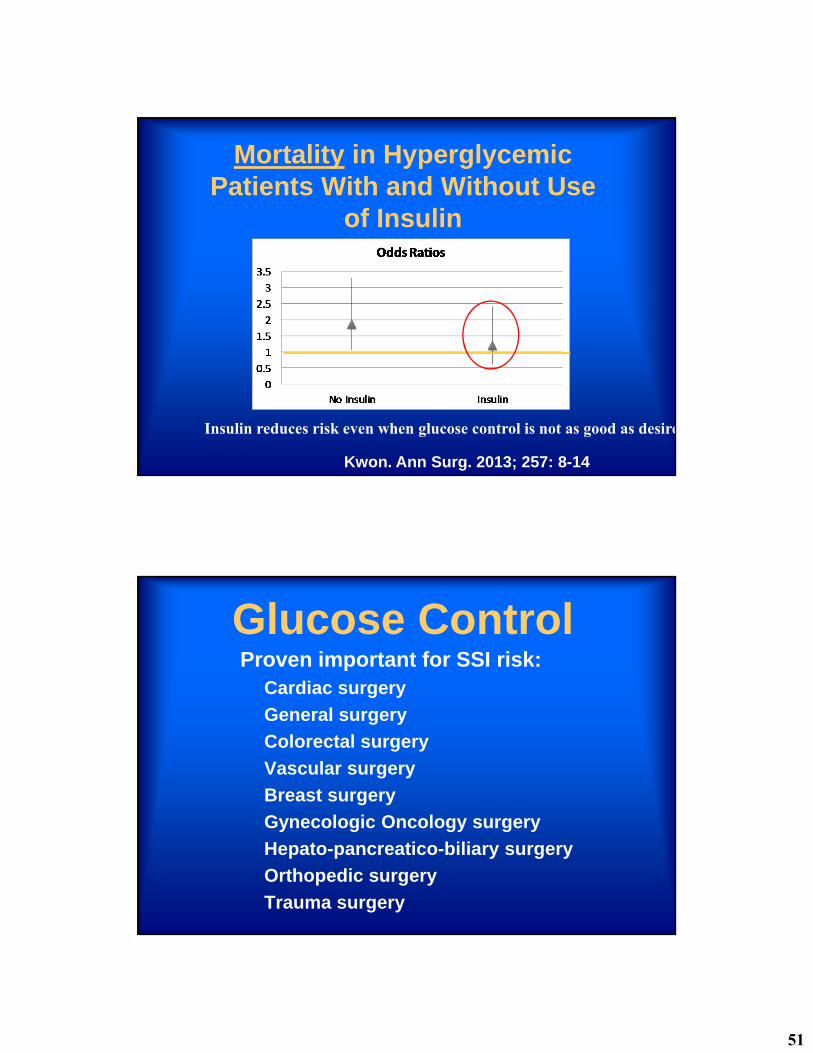
Mortality in Hyperglycemic Patients With and Without Use
of Insulin
Kwon. Ann Surg. 2013; 257: 8-14
Insulin reduces risk even when glucose control is not as good as desire
Glucose ControlProven important for SSI risk:
Cardiac surgery
General surgery
Colorectal surgery
Vascular surgery
Breast surgery
Gynecologic Oncology surgery
Hepato-pancreatico-biliary surgery
Orthopedic surgery
Trauma surgery
52
•Regardless of the Diagnosis of Diabetes(or not)
Hyperglycemia Increases
• Morbidity
• Mortality
• Length of Stay
Which Patients Are at Risk
for Hyperglycemia?
53
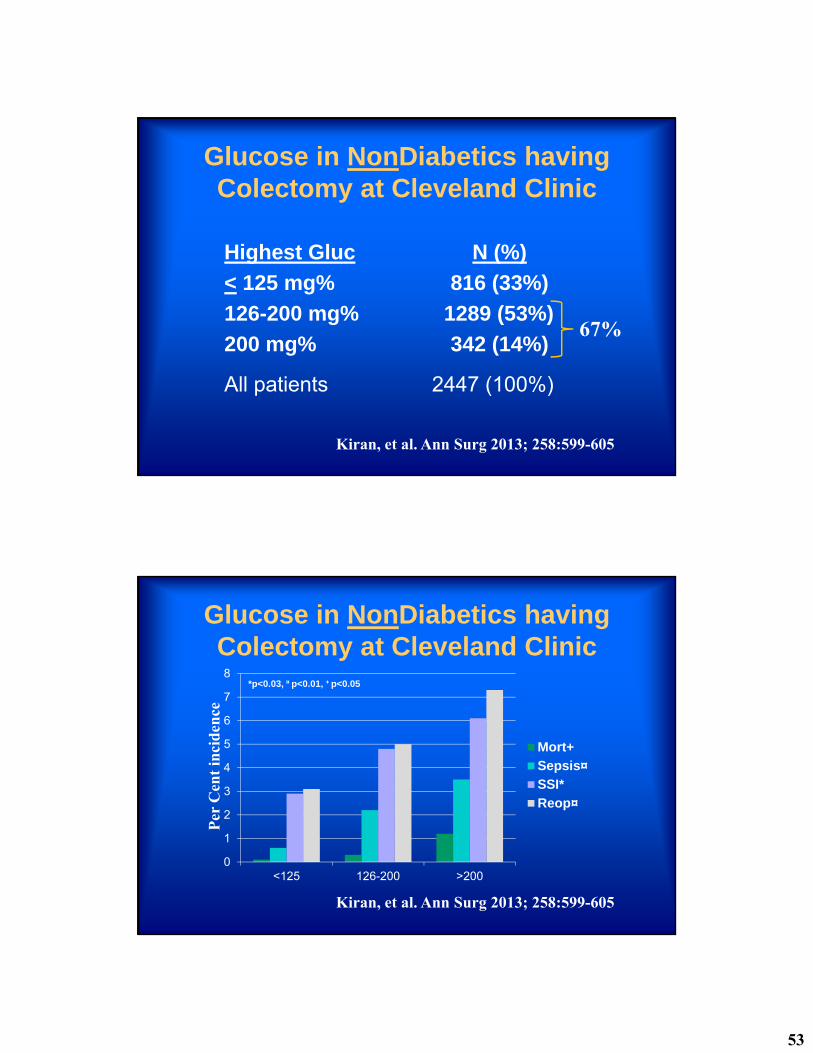
Glucose in NonDiabetics having Colectomy at Cleveland Clinic
Highest Gluc N (%)
< 125 mg% 816 (33%)
126-200 mg% 1289 (53%)
200 mg% 342 (14%)
All patients 2447 (100%)
Kiran, et al. Ann Surg 2013; 258:599-605
67%
Glucose in NonDiabetics having Colectomy at Cleveland Clinic
Kiran, et al. Ann Surg 2013; 258:599-605
Per
Cen
t in
cid
ence
0
1
2
3
4
5
6
7
8
<125 126-200 >200
Mort+
Sepsis¤
SSI*
Reop¤
*p<0.03, ¤ p<0.01, + p<0.05
54
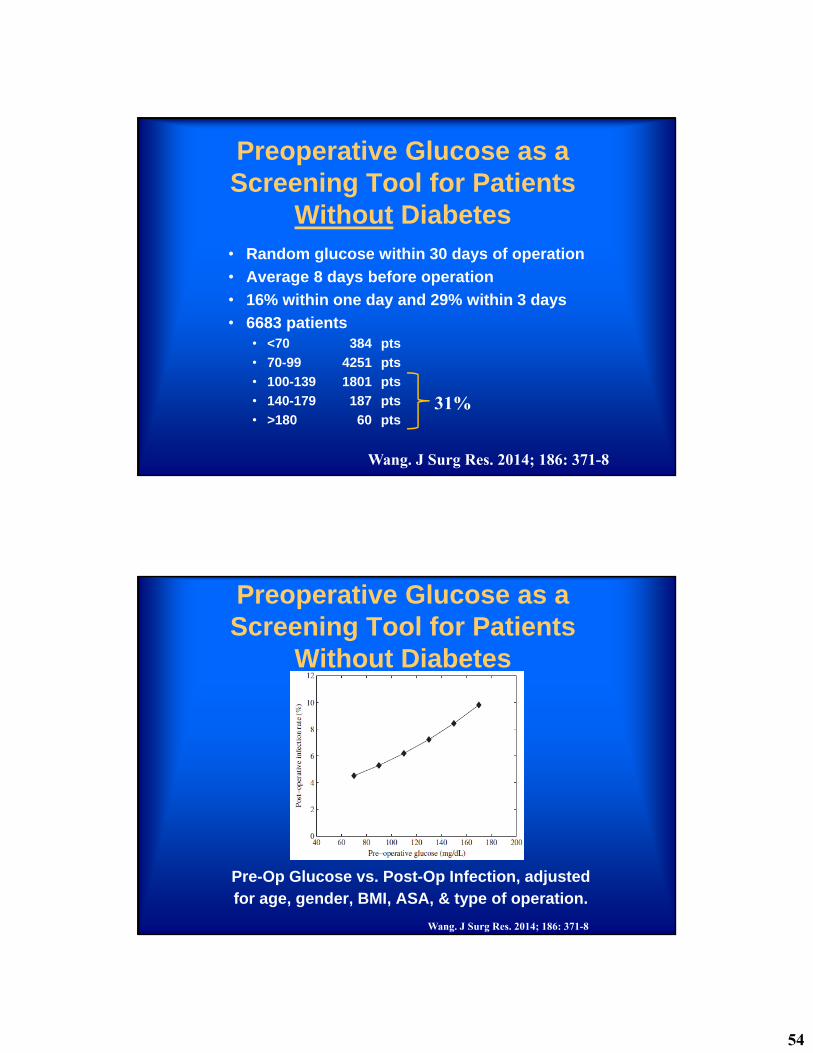
Preoperative Glucose as a Screening Tool for Patients
Without Diabetes• Random glucose within 30 days of operation
• Average 8 days before operation
• 16% within one day and 29% within 3 days
• 6683 patients• <70 384 pts
• 70-99 4251 pts
• 100-139 1801 pts
• 140-179 187 pts
• >180 60 pts
Wang. J Surg Res. 2014; 186: 371-8
31%
Preoperative Glucose as a Screening Tool for Patients
Without Diabetes
Wang. J Surg Res. 2014; 186: 371-8
Pre-Op Glucose vs. Post-Op Infection, adjusted for age, gender, BMI, ASA, & type of operation.
55
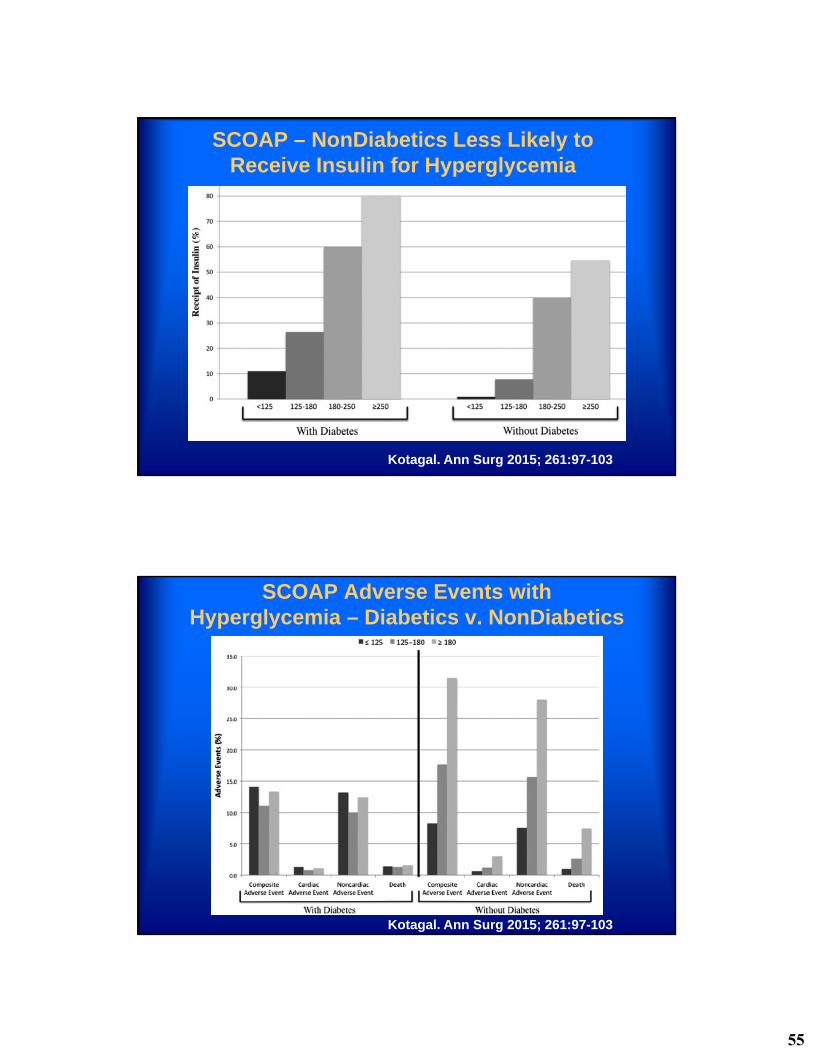
SCOAP – NonDiabetics Less Likely to Receive Insulin for Hyperglycemia
Kotagal. Ann Surg 2015; 261:97-103
SCOAP Adverse Events with Hyperglycemia – Diabetics v. NonDiabetics
Kotagal. Ann Surg 2015; 261:97-103
56
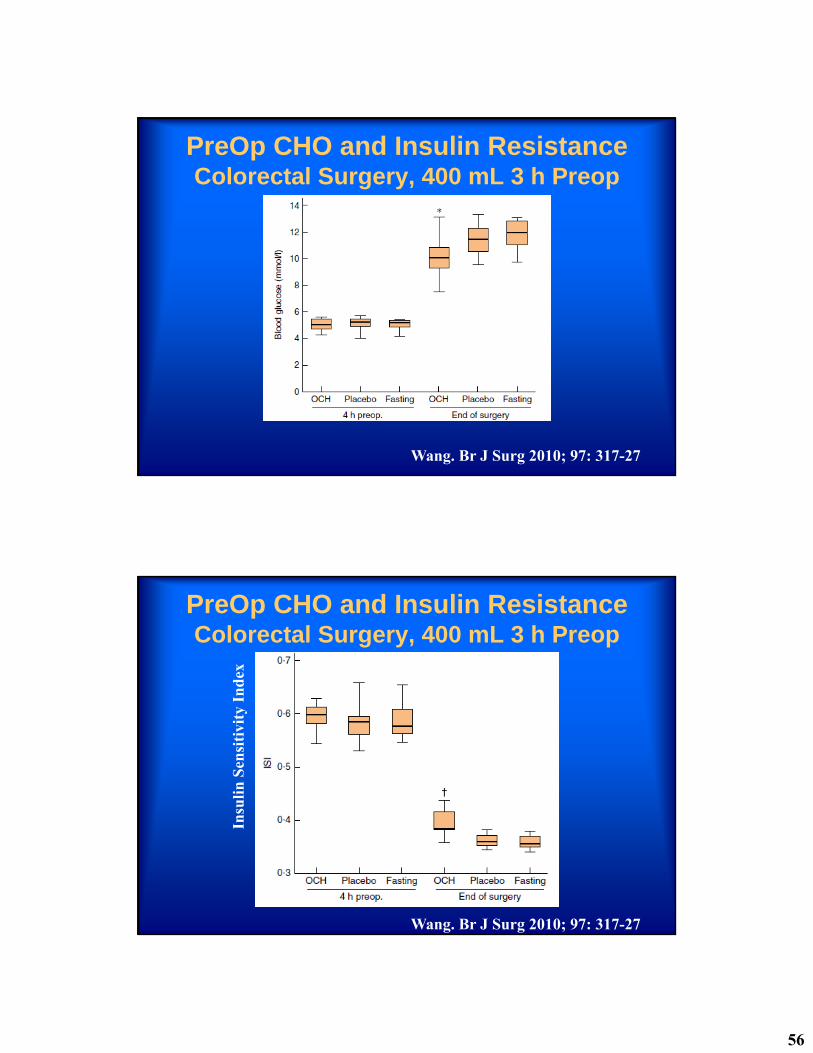
PreOp CHO and Insulin ResistanceColorectal Surgery, 400 mL 3 h Preop
Wang. Br J Surg 2010; 97: 317-27
PreOp CHO and Insulin ResistanceColorectal Surgery, 400 mL 3 h Preop
Wang. Br J Surg 2010; 97: 317-27
Insu
lin
Sen
siti
vity
In
dex

57
PreOp CHO and Muscle Mass – Major Abdominal Surgery
800 mL evening, 400 mL 2 h Preop
Svanfeldt. Br J Surg 2007; 94: 1342-50
Triceps Skin Fold Arm Muscle Circum
Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of
pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Committee
on Standards and Practice Parameters. Anesthesiology 2011;114:495-511
It is appropriate to fast from intake of clear liquids at least 2 h before elective procedures requiring general anesthesia, regional anesthesia, or sedation/analgesia. Examples of clear liquids include, but are not limited to, water, fruit juices without pulp, carbonated beverages, clear tea, and black coffee. . . . The volume of liquid ingested is less important than the type of liquid ingested.
58
Glucose Levels & SSI• The exact “best” level of glucose control in
the perioperative period is not known.
• High glucose levels unequivocally increase the risk of SSI and other perioperative infections.
• Tight glucose control in the perioperative period is tricky.
• Hypoglycemia increases the risk of morbidity and mortality.
• When algorithms are followed at UWMC hypoglycemia is very rare.
Temperature and Infection
59
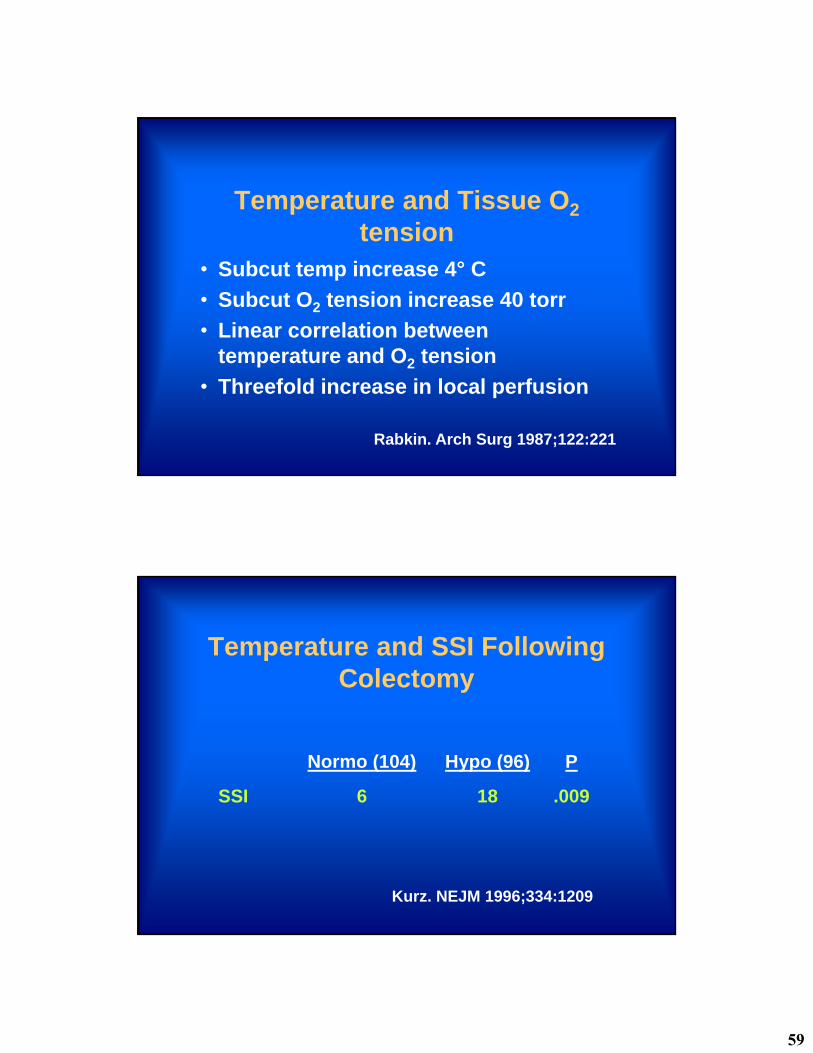
Temperature and Tissue O2
tension• Subcut temp increase 4° C
• Subcut O2 tension increase 40 torr
• Linear correlation between temperature and O2 tension
• Threefold increase in local perfusion
Rabkin. Arch Surg 1987;122:221
Temperature and SSI Following Colectomy
Normo (104) Hypo (96) P
SSI 6 18 .009
Kurz. NEJM 1996;334:1209
60
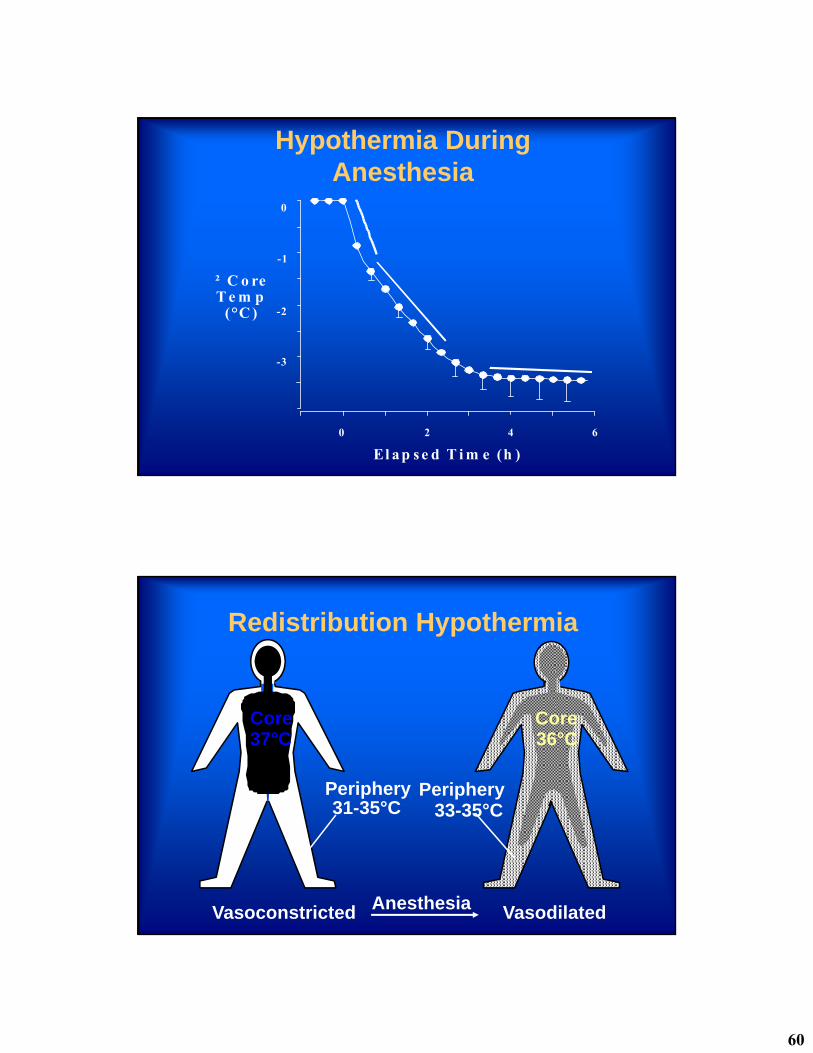
Hypothermia During Anesthesia
0 2 4 6
² C o reT e m p
(°C )
El a p s e d T i m e (h )
-1
-3
-2
0
Redistribution Hypothermia
Core37°C
Vasoconstricted
Periphery31-35°C
Anesthesia
Periphery33-35°C
Core36°C
Vasodilated
61
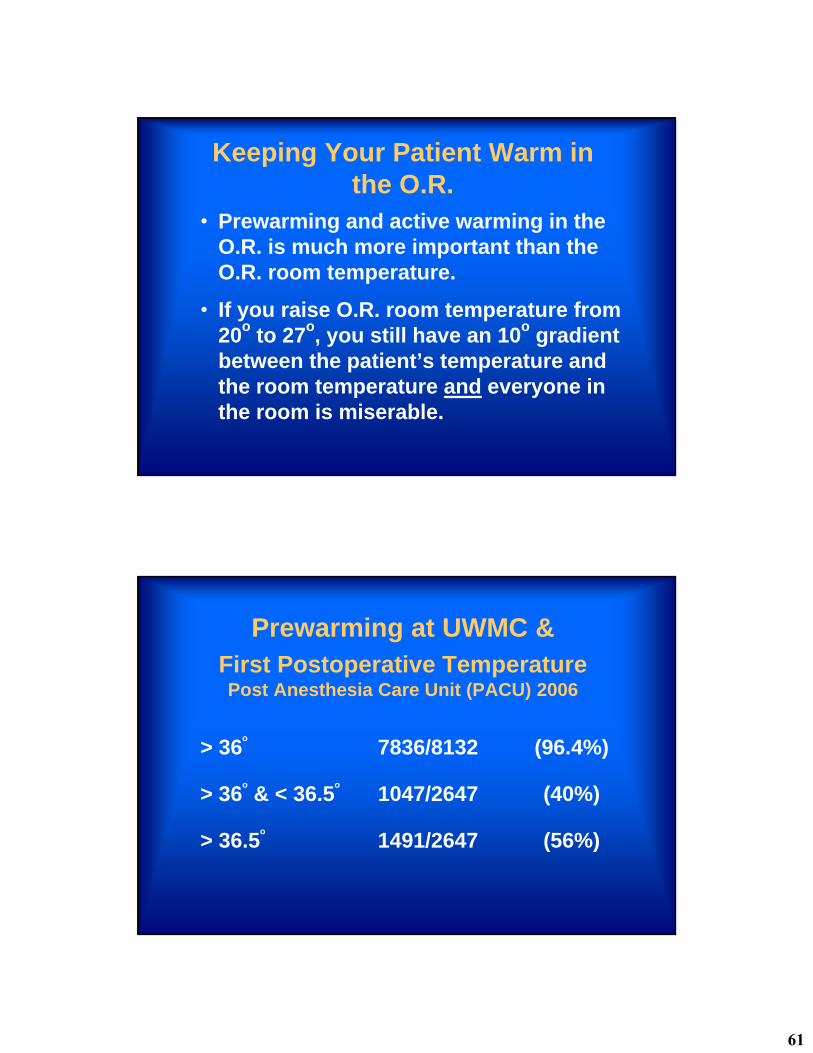
Keeping Your Patient Warm in the O.R.
• Prewarming and active warming in the O.R. is much more important than the O.R. room temperature.
• If you raise O.R. room temperature from 20o to 27o, you still have an 10o gradient between the patient’s temperature and the room temperature and everyone in the room is miserable.
Prewarming at UWMC &First Postoperative TemperaturePost Anesthesia Care Unit (PACU) 2006
> 36o
7836/8132 (96.4%)
> 36o
& < 36.5o
1047/2647 (40%)
> 36.5o
1491/2647 (56%)
62
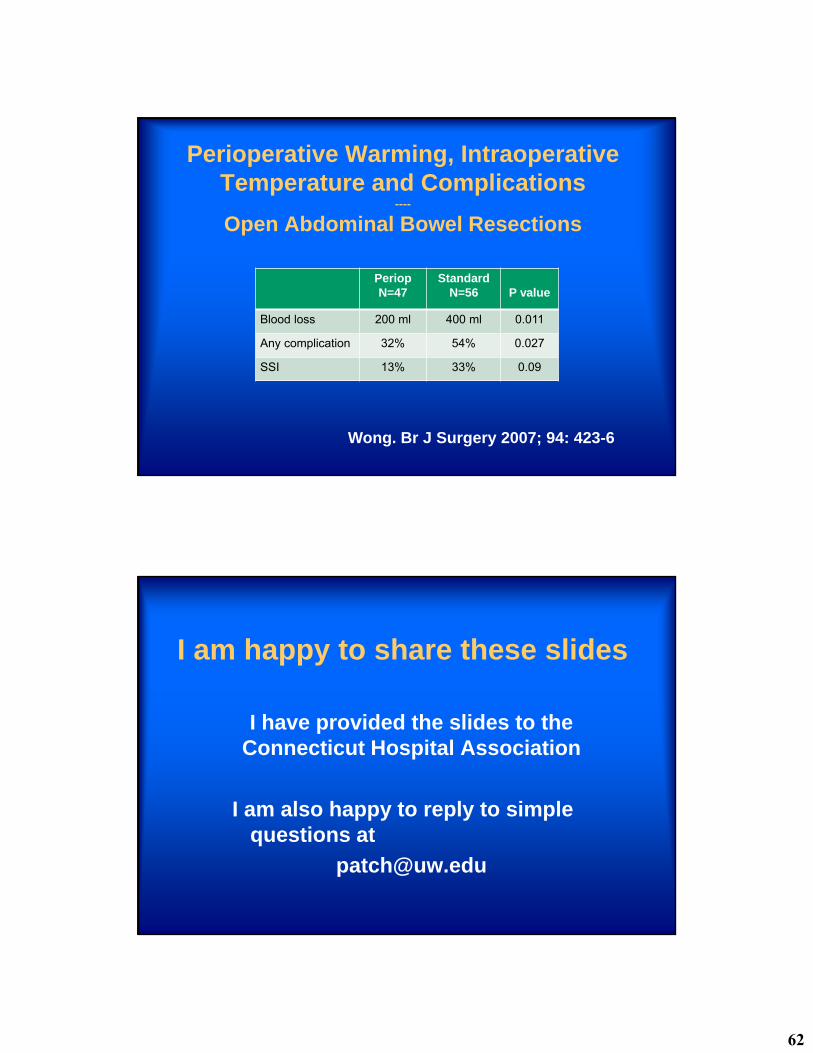
Perioperative Warming, Intraoperative Temperature and Complications
----
Open Abdominal Bowel Resections
Wong. Br J Surgery 2007; 94: 423-6
PeriopN=47
StandardN=56 P value
Blood loss 200 ml 400 ml 0.011
Any complication 32% 54% 0.027
SSI 13% 33% 0.09
I am happy to share these slides
I have provided the slides to the Connecticut Hospital Association
I am also happy to reply to simple questions at