brain protection ahmad n. hamdy, md. objectives (iols) cerebral physiology 1 explain cerebral...
TRANSCRIPT
Brain Protection
Ahmad N. Hamdy, MD
Objectives (IOLs)
Cerebral physiology1
Explain cerebral ischemia2
3
Algorithm for brain protection4
Strategies to protect the brain from cerebral ischemia
Cerebral Physiology
BRAIN 1350 gm- 2% of total adult body wtReceives 12 to 15 % of cardiac output Global cerebral blood flow 45-55ml/100
gm / min
Cortical Subcortical 75-80ml /100gm/min 20ml /100gm/min
CMRO2 3 to 3.5 ml/100gm/min
Whole brain O2 consumption 50ml/min
(20% of total body O2 consumption)
Cerebral glucose utilization 5.5 gm/100gm of brain tissue (1ry energy source)
ICP ( supine) 5 to 15 mm Hg
CPP= MAP- ICP or (CVP), whichever is greater (90-100 mm Hg)
Cerebral Physiology
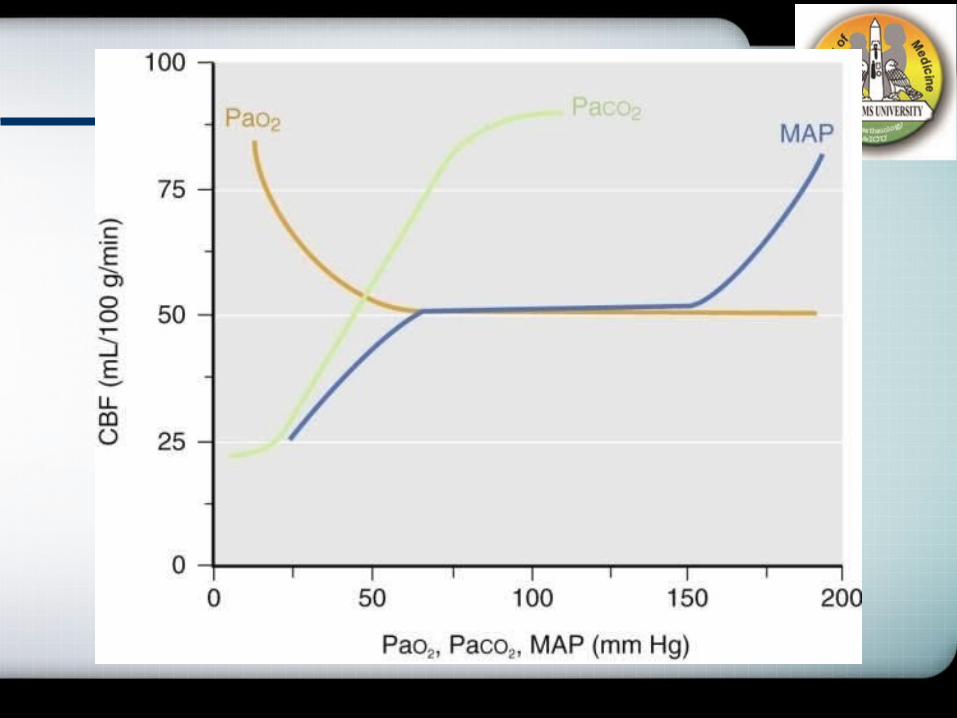
Factors Influencing CBF
Chemical/Metabolic /Humoral Cerebral metabolic rate Anaesthetics Temperature PaCO2 (20-80 mmHg) PaO2 Vasoactive drugs - Anaesthetics,Vasodilators,
Vasopressors Myogenic / Autoregulation Blood viscosityNeurogenic
Company Logo
Cerebral Ischemia
It is the potentially reversible altered state of brain physiology and biochemistry that occurs when substrate delivery is cut off or substantially reduced by vascular stenosis or occlusion
Metabolic demands > substrate delivery
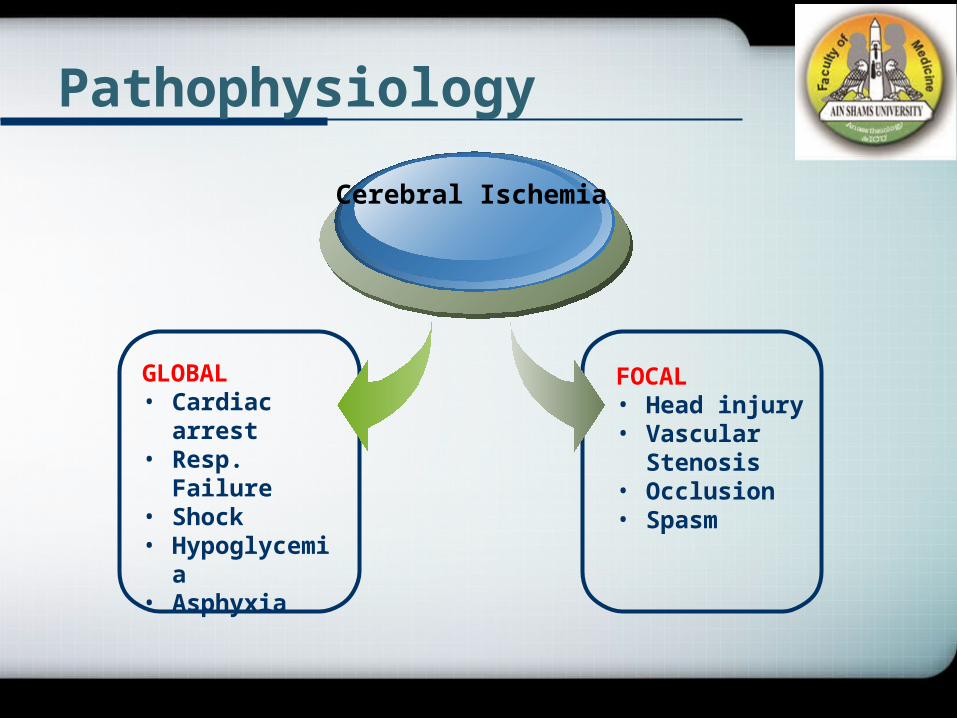
Pathophysiology
GLOBAL• Cardiac arrest• Resp. Failure• Shock• Hypoglycemia• Asphyxia
Cerebral Ischemia
FOCAL• Head injury• Vascular
Stenosis• Occlusion• Spasm
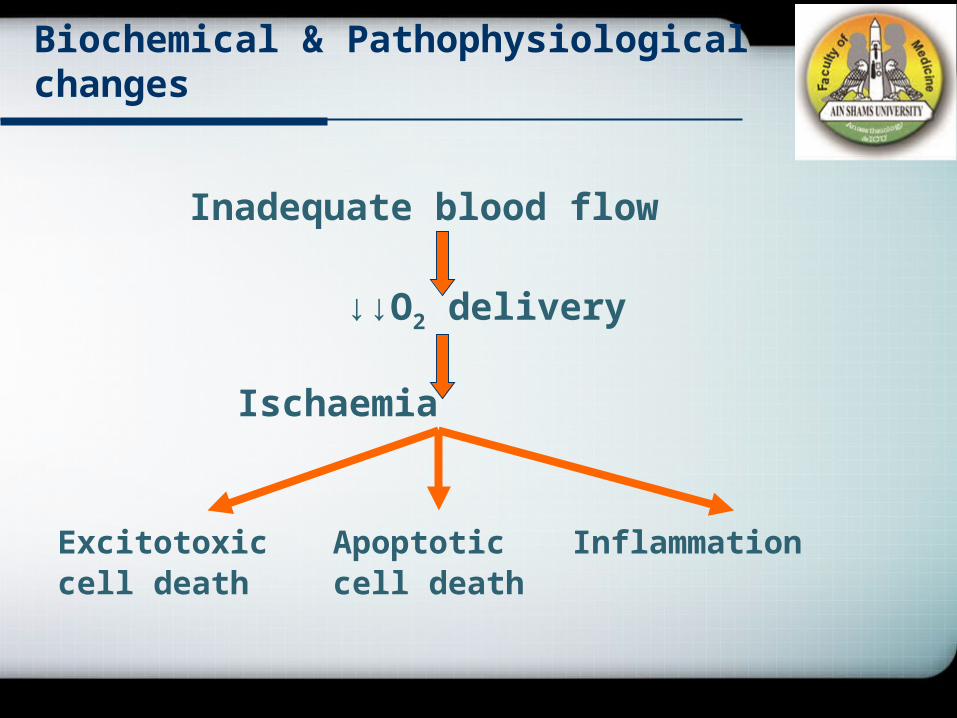
Biochemical & Pathophysiological changes
Inadequate blood flow
↓↓O2 delivery
Ischaemia
Excitotoxic Apoptotic Inflammationcell death cell death
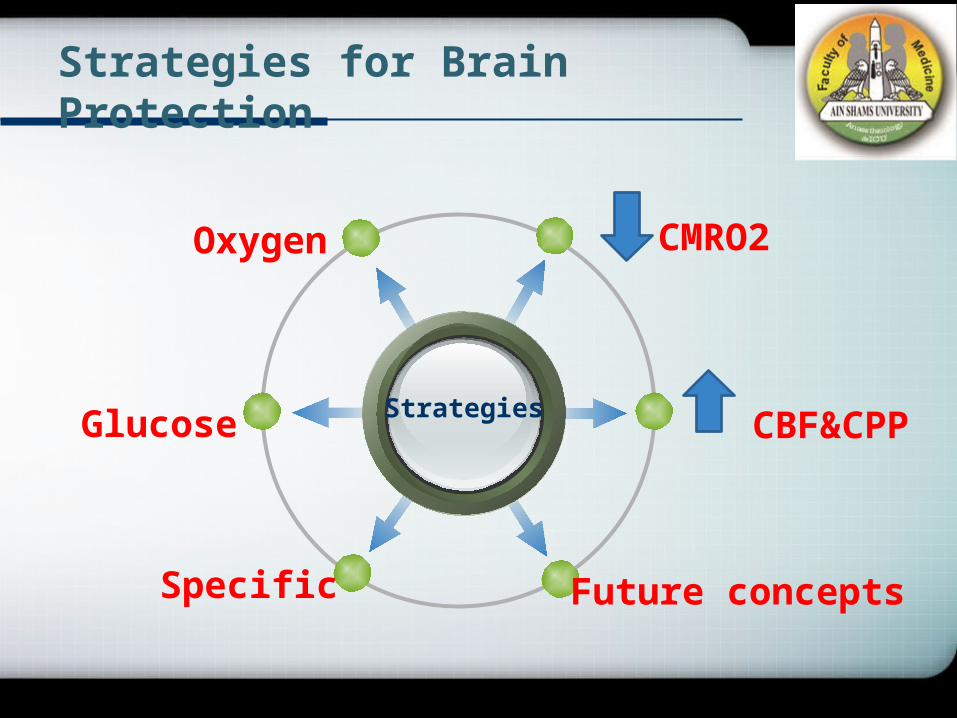
Strategies for Brain Protection
Strategies
CMRO2Oxygen
CBF&CPP
Future concepts
Glucose
Specific
Oxygen & Glucose
In the absence of oxygen, glucose undergoes anaerobic glycolysis resulting in intracellular acidosis Patients with higher blood glucose concentrations have
worse outcomes from stroke, TBI, etc. More rapid expansion of ischemic lesion in
hyperglycemic, compared with normoglycemic patients
For all of this reasons, it is rational to maintain normoglycemia in all patients at risk for ,or recovering from acute brain injury

CMRO2
Hypothermia
Anesthetics

Body Temperature
Hyper HypoIschaemic Injury
Temperature
Hypothermia Reduce CMR in a temperature-dependent fashion Mild hypothermia(32-35 ) ; negliable effect on CMR℃
• But, in several studies mild hypothermia produce major protection ; provides scientific basis of using off-bypass hypothermia to provide meaningful neuroprotection
Deep hypothermia(18-22 ) ; highly neuroprotective℃• In normothermic brain ; only a few minutes of complete
global ischemia cause neuronal death• In deep hypothermia before circulatory arrest ; brain can
tolerate over 40 min and completely or near-completely recover
Temperature
Hyperthermia In animal studies, spontaneous post-
ischemic hyperthermia is common and intra-ischemic or even delayed post-ischemic hyperthermia dramatically worsen outcome
Advocate frequent temperature monitoring in patients with cerebral injuy
Aggressive treatment of hyperthermia should be considered
Anesthetics
Volatile anesthetics Protect against both focal and global ischemia
• Transient improvement in global ischemia• Persistent improvement in focal ischemia
Suppression of energy requirements• Inhibition of excitatory neurotransmission• Potentiation of inhibitory receptors• Regulation of intracellular calcium response during ischemia
Isoflurane, sevoflurane ; Desflurane ; insufficiently studied
Company Logo
Anesthetics
Barbiturates have major actions on CNS: • hypnosis• depression of CMR • anticonvulsant activity.
These properties make barbiturates, particularly thiopental, the most commonly used induction agents in neuroanesthesia.

Anesthetics Propofol
Suppression of CMR Free radical scavenging Anti-inflammatory properties Appears efficacy similar to barbiturates
Etomidate Paradoxically exacerbate ischemic injury Cannot use for neuroprotection
Lidocaine Suppress CMR Inhibition of apoptosis No long-term outcome studies
Ketamine Inhibition of glutamate at NMDA receptor Little or no protection against global insult Substantial protection against focal insult However, no human data
CPP
More than 65-70mmHg
Elevation of MAP
Decrease ICP
Decrease blood viscosity
Specific
CCBs as nimodipine (SAH)
Na CBs as lamotrigine (SDH)
NMDA antagonist
Steroids (Brain tumors)
Preconditioning
Ischaemic Preconditioning
Homeothermic mammal
Elicits “an evolutionary conserved endogenous response to decreased blood flow and oxygen limitation such as seen during hibernation”
Clinical methods of preconditioning
Pre - op hyperbaric oxygen
Normobaric 100 % oxygen
Electroconvulsive shock
K+ channel opener→ Diazoxide
Erythropoietin (EPO)
Erythropoietin
Cytokine growth hormone-↓ apoptosis-↑ erythrocyte production
↑↑ haematocrit
Deleterious effect on ischaemia
Intravenous recombinant erythropoietin
Once daily for 3 days
60 -100 fold ↓glial markers ↓ infarct
↑ of EPO in CNS of cerebral size & injury
improved (S 100)recovery
Astrocytes in ischaemic penumbra produces EPO in mammalian brain
Stimulates protein Stimulates of repair
neurogenesis & angiogenesis
↓neural apoptosis
↓↓neural ↓inflammatoin excitotoxicity
Magnesium
Membrane stabilizerSuggested protective mechanism:
• Reduction of presynaptic release of glutamate• Blockade of NMDA receptors• Smooth muscle relaxation• Improved mitochondrial Ca2+ buffering• Blockage of Ca2+ entry
Protection depends on:• Time of treatment initiation• Type of cerebral ischemia
Benefit in neocortical stroke
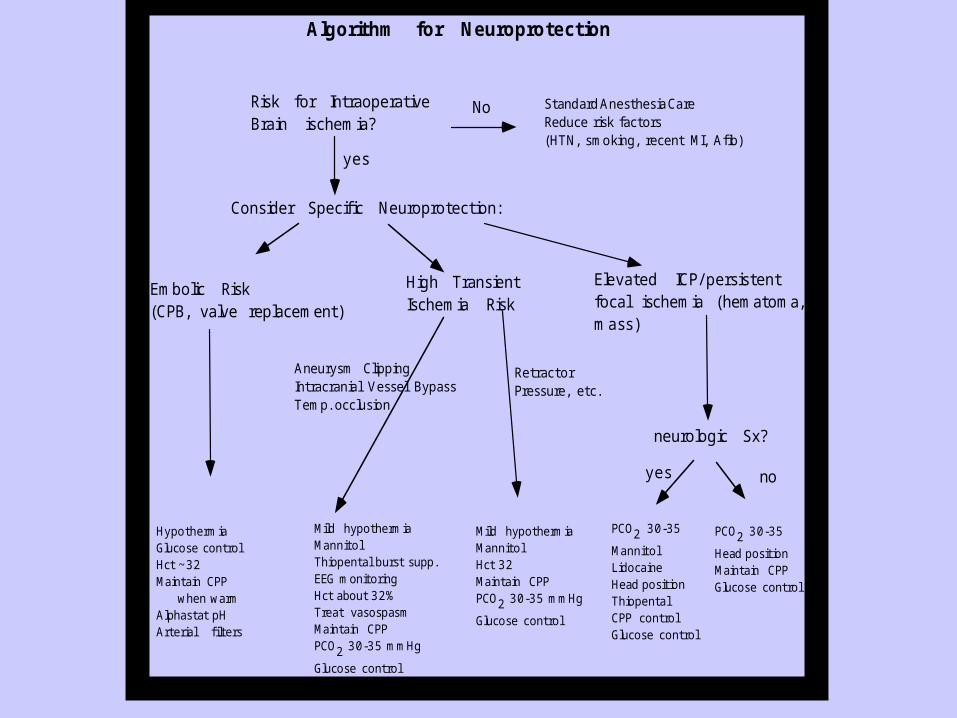
Algorithm for Neuroprotection
Risk for IntraoperativeBrain ischemia?
No Standard Anesthesia CareReduce risk factors(HTN, smoking, recent MI, Afib)
yes
Embolic Risk(CPB, valve replacement)
HypothermiaGlucose controlHct ~32Maintain CPP when warmAlphastat pHArterial filters
neurologic Sx?
noyes
PCO2 30-35
Head positionMaintain CPPGlucose control
PCO2 30-35
MannitolLidocaineHead positionThiopentalCPP controlGlucose control
Aneurysm ClippingIntracranial Vessel BypassTemp. occlusion
RetractorPressure, etc.
Mild hypothermiaMannitolThiopental burst supp.EEG monitoringHct about 32%Treat vasospasmMaintain CPPPCO2 30-35 mmHg
Glucose control
Mild hypothermiaMannitolHct 32Maintain CPPPCO2 30-35 mmHg
Glucose control
Consider Specific Neuroprotection:
High TransientIschemia Risk
Elevated ICP/ persistentfocal ischemia (hematoma,mass)
Strategies for Brain Protection
O2
• HCT: 30-34 %
• PaO2 Levels
GL.
• 100- 150 mg/dl
CMRO2
• Hypothermia• Anesthetics
Strategies of Brain Protection (Cont.)
CBF
• CPP: ≥ 70 mmhg• MBP: Elevated• Viscosity:
Decresed• ICP: Decrease
Future
• NO• Cerebral
preconditioning• Apoptosis
Specific
• CCBs• Na CBs• NMDA
antagonist
Add your company slogan