brain stimulation & neuromodulation september 2016 - bh summit
TRANSCRIPT

Brain Stimulation & Neuromodulation
Jay A. Yeomans, MD, DFAPA
Medical Director of Psychiatry Consult Liaison and Brain Stimulation Service
Carolinas HealthCare System
September 27th, 2016
First Annual CHS BH Summit
• No disclosures• Acknowledgements
Dr. Mark George, et al. at MUSC
• Objectives:
• The participant will:• Be aware of the underlying premise of neuromodulation.• Be aware of the Neuropsychiatric indications for Brain Stimulation.• Be aware of the FDA approved classifications and non-FDA approved
brain stimulation devices.
The Burden of Depression• Approximately 18.8 million adults aged 18 and older
are stricken with depression in an given year (NIMH)
• Suicides eclipse homicides in the US annually by one third (DHHS). The elderly are particularly at risk
• Medications and psychotherapy may fail to alleviate severe depressions, particularly those complicated by psychosis or catatonia
• Antidepressants may increase suicidality in some patients and may not be safely used during pregnancy.
Why Brain Stimulation for Depression?• limits of current treatment strategies
NIMH STAR*D study:Sequenced treatment alternatives to relieve depression (screened > 4K pts)Focus on treatment of depressed patients when the 1st prescribed antidepressant proved inadequate & included remission as an outcome measure
4 levels (SSRI / antidepressant & CBT / Li or T3 & antidepressant / MAOI or combo antidepressant)
• Level one: 1/3 remitted, then 1/3 with 2nd, 13% with 3rd and 13% with 4th
Data suggest that a patient with persistent depression can get well after trying several treatment strategies, but his or her odds of beating depression diminish as additional treatment strategies are needed
12 months later: 25% sustained remission w/level 1; 13% (L2), 4 % (L3) and 3% (L4)

Why Brain Stimulation for Depression?• Medication under treatment, e.g.
‘pseudoresistance’ – have not received sufficient guideline-concordant treatment
• Side Effects from medication (non discriminate): e.g. weight gain, fatigue, etc.
• Psychotherapy (patient resistance / limited INS coverage)
Important Points• Underlying premise of neuromodulation is that the
brain is an electrochemical organ that can be modulated by pharmacotherapy or devise-based (ECT / TMS) approaches or their combination
• There is an explosion of new techniques for electrically stimulating the brain, primarily focally
• These new tools are changing neuroscience research and neuropsychiatric therapies
• They validate and inform us about functional neuroanatomy
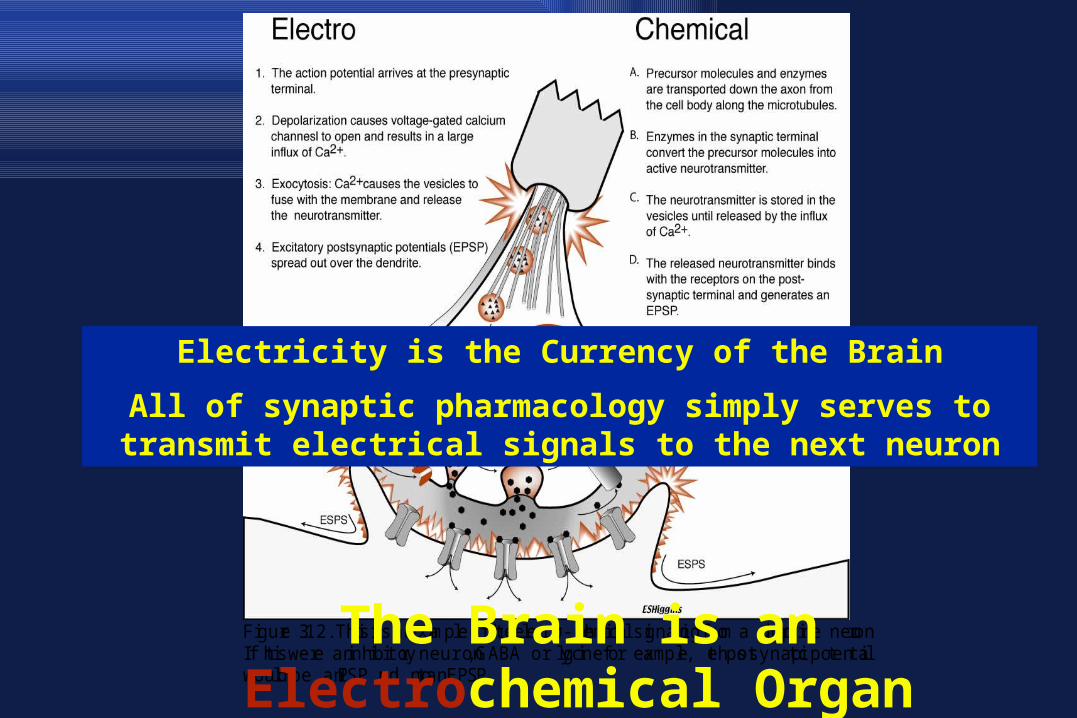
Figure 3.12. This is an example of the electro-chemical signaling from a dopamine neuron.If this were an inhibitory neuron, GABA or glycine for example, the postsynaptic potentialwould be an IPSP and not an EPSP.The Brain is an Electrochemical Organ
Electricity is the Currency of the Brain
All of synaptic pharmacology simply serves to transmit electrical signals to the next neuron
Brain Stimulation Techniques (partial listing)
• ECT - Electroconvulsive Therapy - Alternating current, directionless • Ultra brief pulse • (FEAST (Focal Electrically Administered Seizure Therapy) - Cycle it, turning it on and off rapidly and make sure all pulses are rectified, causing a direct current-like direction - Extremely fast tDCS.
• TMS - Transcranial Magnetic Stimulation
• VNS - Vagus Nerve Stimulation• DBS - Deep Brain Stimulation
FDA Approved
Brain Stimulation Techniques (partial listing)
• tACS – transcranial Alternating Current Stimulation Cranial Electrotherapy Stimulators (CES)
• tDCS - transcranial Direct Current Stimulation • MST - Magnetic Seizure Therapy - Super TMS
– limited to cortex for site of seizure• LFMS- Low field magnetic stimulation• TENS - transcutaneous Electrical Nerve Stimulation• Transcranial pulsed ultrasound• eTNS (external trigeminal nerve stimulation)
FDA Classi-fication
When it First Started, Things Were Rough

History of ECT• 16th century, camphor by mouth to induce convulsions to ‘cure lunacy’• 1934: Meduna, Hungarian Neuropsychiatrist, believed Schizophrenia and Epilepsy were antagonistic disorders
- epileptics have many glial cells, Schizophrenia have too few- ergot, causing seizures might stop or cure schizophrenia (sic)
• Injected patients w/Schizophrenia with camphor oil to cause a seizure, Patient had a 60 sec grand mal seizure, ‘woke up’.. Full recovery, left hospital …
• Later replaced camphor with metrazol … spread throughout Europe.
• 1937: AmJPsych: ‘therapeutic seizure’ (worldwide)
(Drawing by Renato Sabattini, PhD)

What about ‘Electrical’ CT?• 1938 -Italian psychiatrists, working in Rome, Cerletti and Bini, worked on electrical parameters that could induce seizures. Dog model• treated Italian man, ? Psychotic depression - recovered after 11 treatments
Nominated for the Nobel Prize
ECT was born… • Kalinowsky started ECT at NY State Psychiatric Hospital/Columbia Presbyterian Hospital in NY
1940’s – Widespread use throughout the world … RUL
1950’s – Modifications in ECT technique initially curare then (‘52 – Holmberg) used succinylcholine as a muscle relaxant with ECT
Standard treatment for hospitalized depression
History of ECT
• 1960’s – 1980s … Decline in use of ECT• Psychoanalyst marginalized ECT • Pharmaceutical industry marginalized ECT• 1960s counterculture hostility toward ECT• 1961: Erving Goffman’s Asylums • 1962: Ken Kesey’s anti-psychiatry novel / play
(‘70) / movie (‘75):
One Flew Over the Cuckoo’s Nest

1980’s: Resurgence in the use of ECT1985: JAMA “not a single controlled study has shown another form of
treatment to be superior to ECT in the short-term management of severe depression”
How does ECT (therapeutic seizures) modify mood?• A) Brain Structure … o hippocampal neurogenesis
• B) Neurotransmitter Enhancement … o after Seizure - flood of Catecholamines: 5HT, NE DA, GABA & BDNF
• C) Normalization of Neuro-Endocrine Abnormalities …o Surge of Hypothalamic & Pituitary peptide (prolactin & TRH) o Hypercortisolemia frequently found in Melancholia - Cortisol function normalizes; TSH & GH responses are abnormal during illness and normalize with remission

How does ECT (therapeutic seizures) modify mood?
D) Electrophysiology … Anticonvulsant effects (kindling)Analogous to Cardioversion: heart in a dysrhythmic state is restored to normal rhythm by an electrical stimulus
Cerebroversion: hyperactive hypothalamic-pituitary system (leads to a breakdown of the feedback mechanism in the stress response) is normalized after a therapeutic seizure.
•
How does ECT (therapeutic seizures) modify mood?
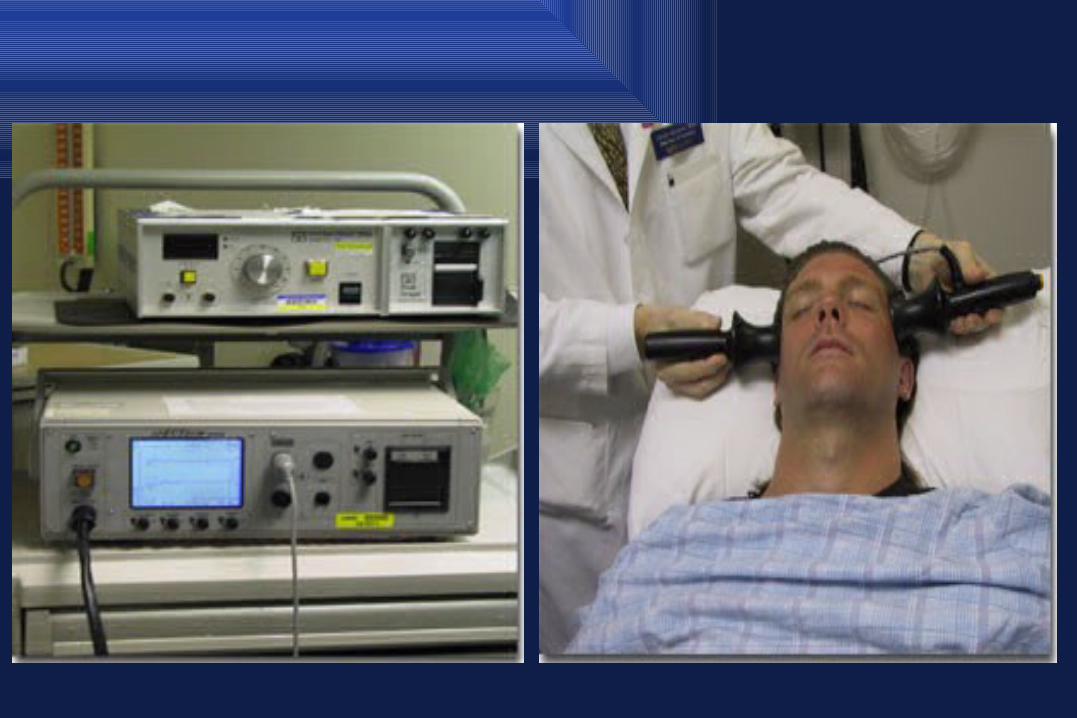
Ctrl-Alt-Delete-----------------------------
DownsidesHeadacheNausea Myalgia
Retrograde / anterograde amnesiaMini Mental State Exam / Montgomery Depression Rating Scale
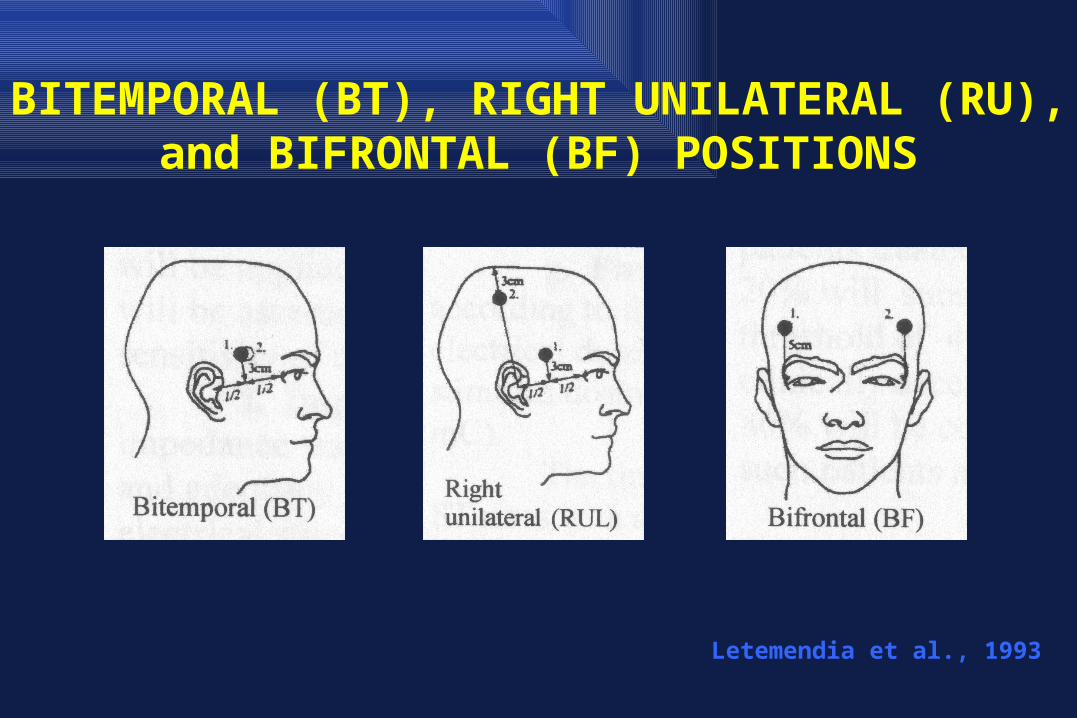
BITEMPORAL (BT), RIGHT UNILATERAL (RU), and BIFRONTAL (BF) POSITIONS
Letemendia et al., 1993
Electroconvulsive TherapyECT
• Guideline recommendations – Acute Treatment of Depression, especially psychotic or suicidal– Acute Mania– Catatonia– Helpful in treatment refractory conditions (e.g. treatment for intractable seizures)– Need for rapid definitive intervention– Medically ill, risk of inanition– Elderly– Pregnancy (teratogenicity a function of exposure duration / succinylcholine: low ratio of
placental transfer)
• New findings / where the field is going?– Right unilateral, ultra brief pulse– Perhaps FEAST, MST

Acute & Maintenance ECT
CHS
CHS
ECT Summary• ECT is a safe & very effective treatment for
depressive disorders either first-line treatment or after medications fail.*
• Between 80% and 90% of patients will respond to ECT. It is the most efficient and fast-acting treatment for urgent-care, severely depressed patients for which medications take 4-6 weeks to work.*
• Treatment of choice for Catatonia, Failure-to thrive, Psychotic & Suicidal depression.
*APA Taskforce book, The Practice of Electroconvulsive Therapy, 2001
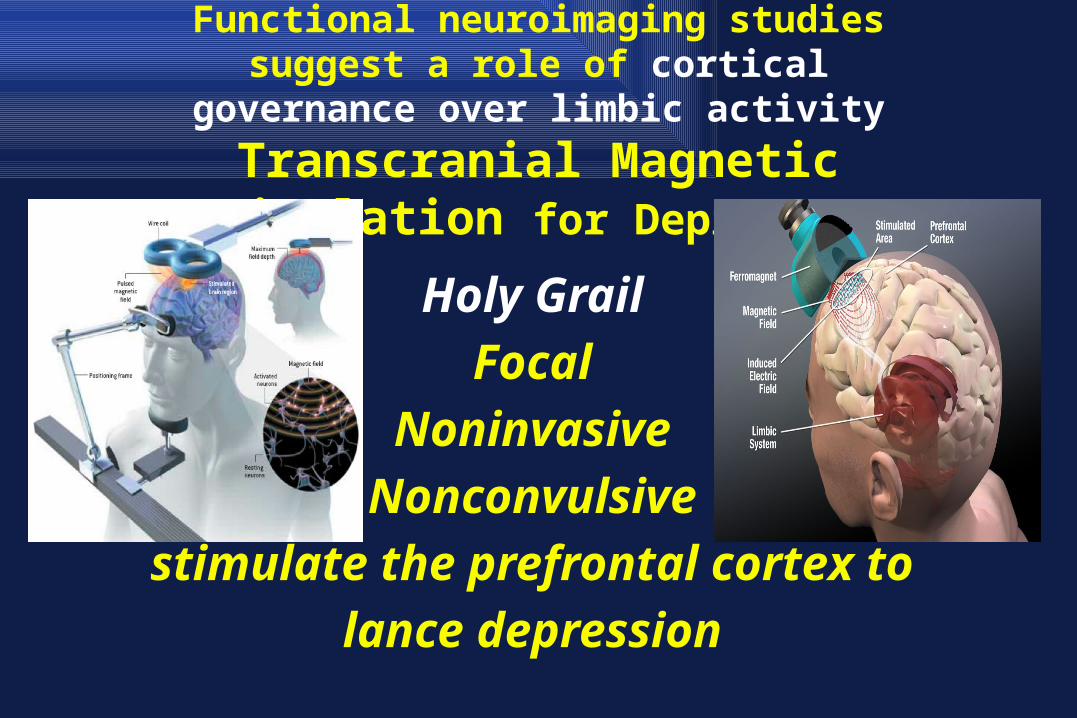
Functional neuroimaging studies suggest a role of cortical governance over limbic activity
Transcranial Magnetic Stimulation for Depression
Holy Grail Focal
Noninvasive Nonconvulsive
stimulate the prefrontal cortex to lance depression
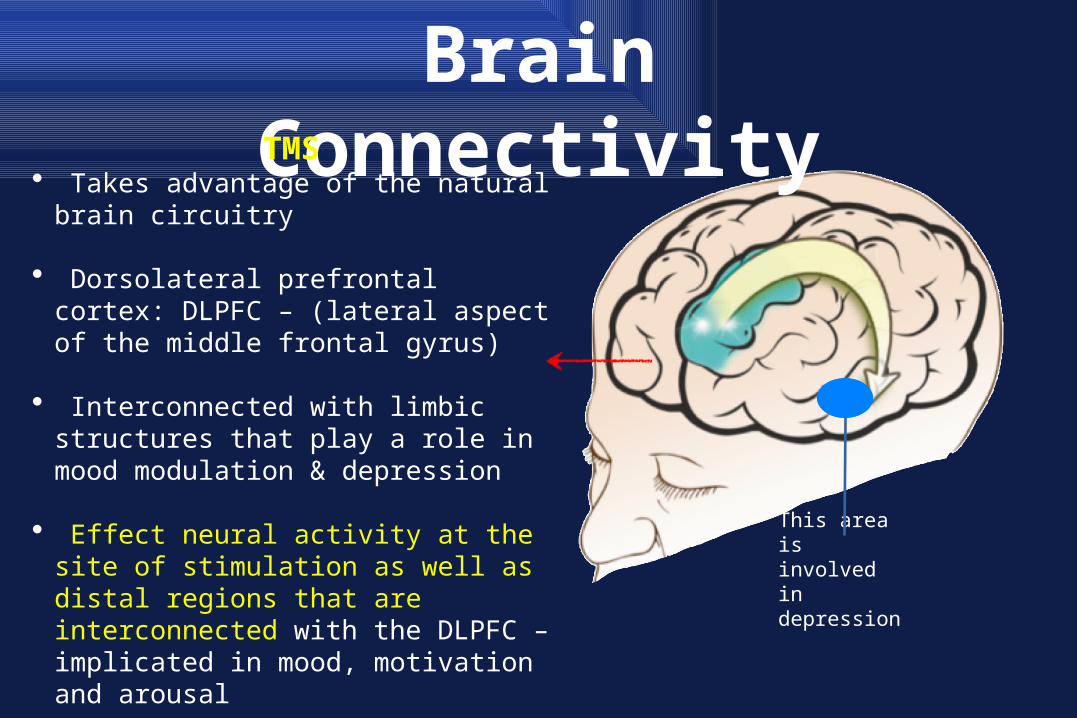
Brain Connectivity
This area is involved in depression
TMS• Takes advantage of the natural brain circuitry
• Dorsolateral prefrontal cortex: DLPFC – (lateral aspect of the middle frontal gyrus)
• Interconnected with limbic structures that play a role in mood modulation & depression
• Effect neural activity at the site of stimulation as well as distal regions that are interconnected with the DLPFC – implicated in mood, motivation and arousal
TMS HISTORY• 1831 - *Michael Faraday - principle of electromagnetic
induction • 1896 - D’Arsonval - first TMS
• 1903 - patent: Pollacsek and Beer• 1910 - Sylvanius P. Thompson: 3 papers on TMS and
phosphenes
• 1959 - Kolin demonstrated magnetic fields stimulate frog muscle
• 1985 - Barker, modern TMS• 1993 - First therapeutic cases reported in depression
Early TMS
Sylvanius P.Thompson
with one of the first
transcranial magnetic
stimulators (1910)Thompson SP. A physiological effect of an alternating magnetic field. Proc R Soc Lond B Biol Sci. 1910;82:396-398.

Applications of TMS• Investigative Tool
– (sTMS) Mapping the cortex of the brain– Probing neural networks by stimulation or inhibition at different places
and times– Measuring cortical excitability in health and disease, and response to
drugs– Modulating brain function to study the pathophysiology of a variety of
neuropsychiatric conditions• Treatment Tool
– Neuropsychiatric conditions; depression, pain, substance craving, anxiety (OCD), Tourette’s Disorder, etc.
– Alter physiologic states like reversing sleep deprivation
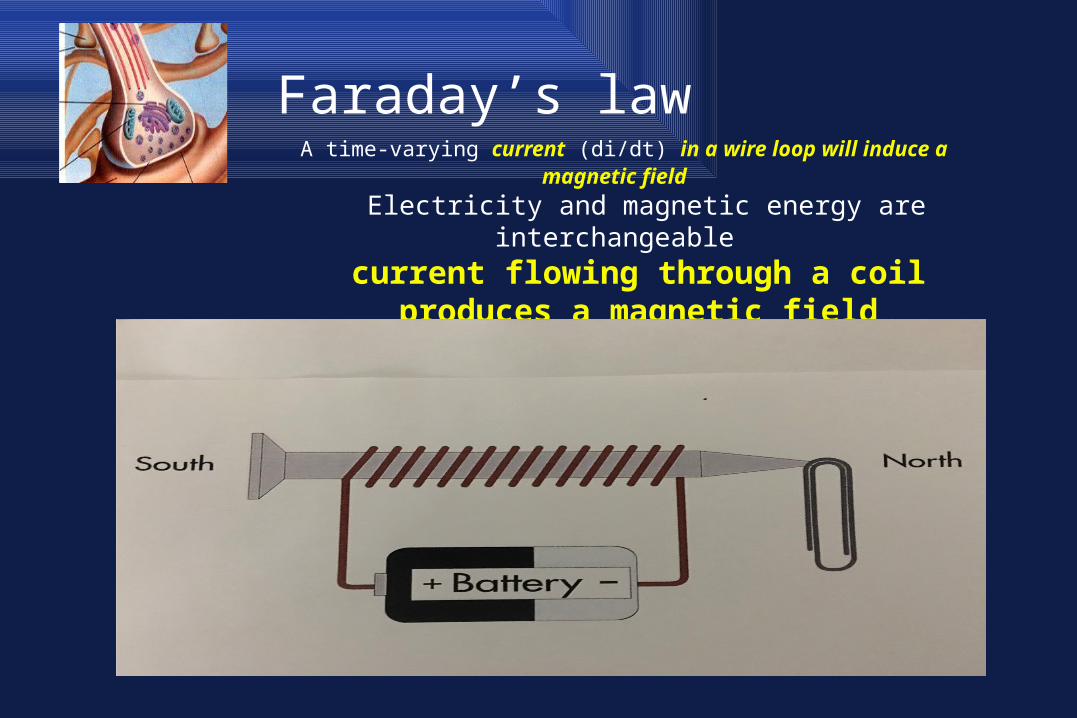
Faraday’s law A time-varying current (di/dt) in a wire loop will induce a magnetic field
Electricity and magnetic energy are interchangeablecurrent flowing through a coil produces a
magnetic field proportional to the current (& perpendicular to the current)

35
How TMS works• Electrical current flowing through a coil induces a
magnetic field• Pass a current through a hand held coil, whose shape
determines the properties and the size of the field• The coil is driven by a machine - switches the large
current necessary in a very precise / controlled way• The coil is held on the scalp and the magnetic field (2
Tesla) passes through the skull (unimpeded) and into the brain
• Alternating (pulsating) magnetic fields induce electrical current in underlying brain tissue
• Small induced currents influence the brain areas below
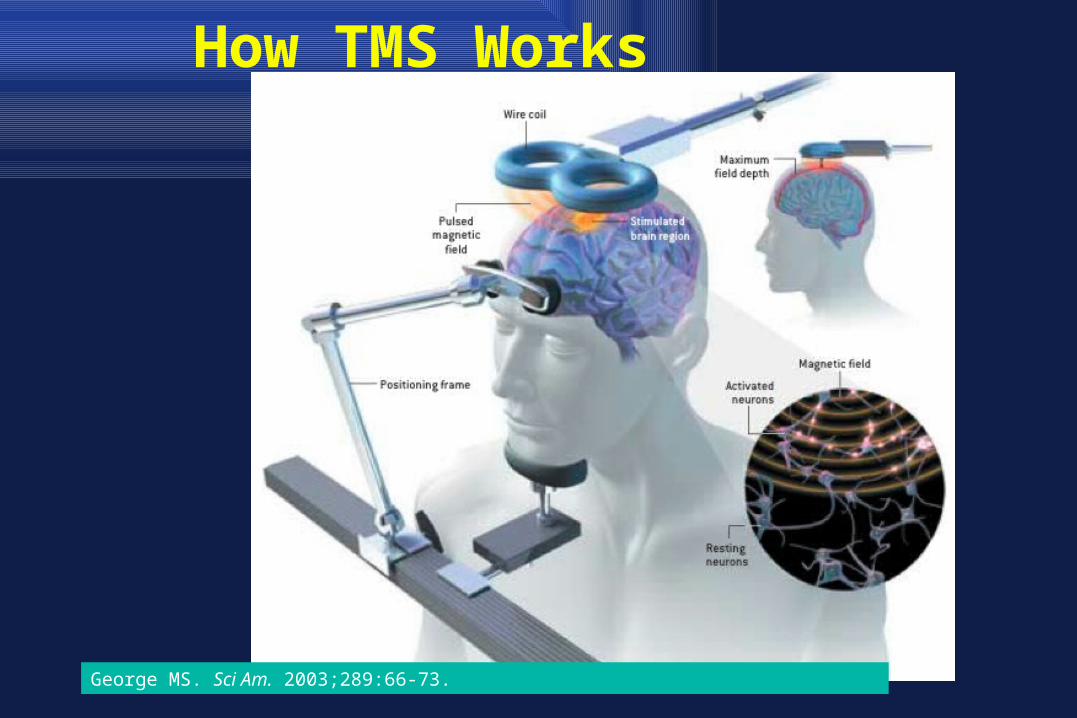
How TMS Works
George MS. Sci Am. 2003;289:66-73.
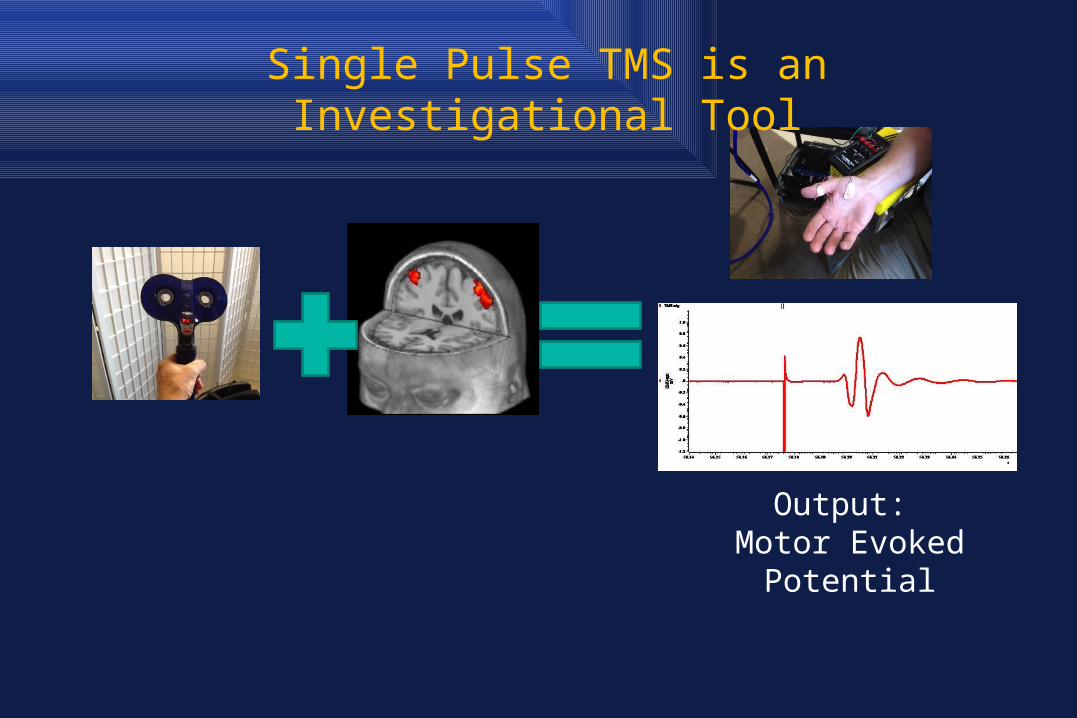
Output: Motor Evoked Potential
Single Pulse TMS is an Investigational Tool
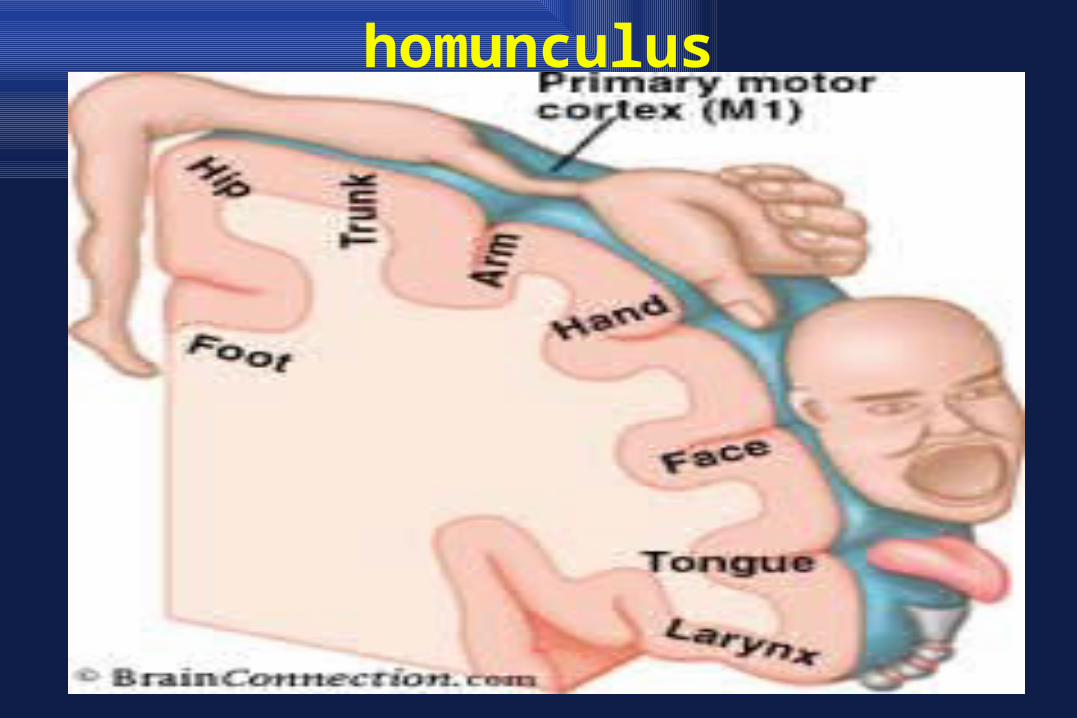
homunculus
TMS IntensityMotor Threshold (MT)
• Stimulate the motor cortex (gyrus) which is oriented 45 degrees backwards – axon lies on the gyrus
• Evoked muscle twitch threshold in response to motor cortex stimulation.
• Defined as lowest intensity capable of inducing at least 5 out of 10 MEPs (of ≥ 50 v in thumb muscle).
• Or, approximately, lowest intensity capable of making thumb muscle visibly twitch 5 0f 10 times
• Best available index of how sensitive an individual's cortex is to having a seizure with rTMS.

Prefrontal PositioningF3 and other rules for positioning
Borckardt, in blue
Anderson, in red
MUSC
Locate F3?EEGBeam F3Brain net
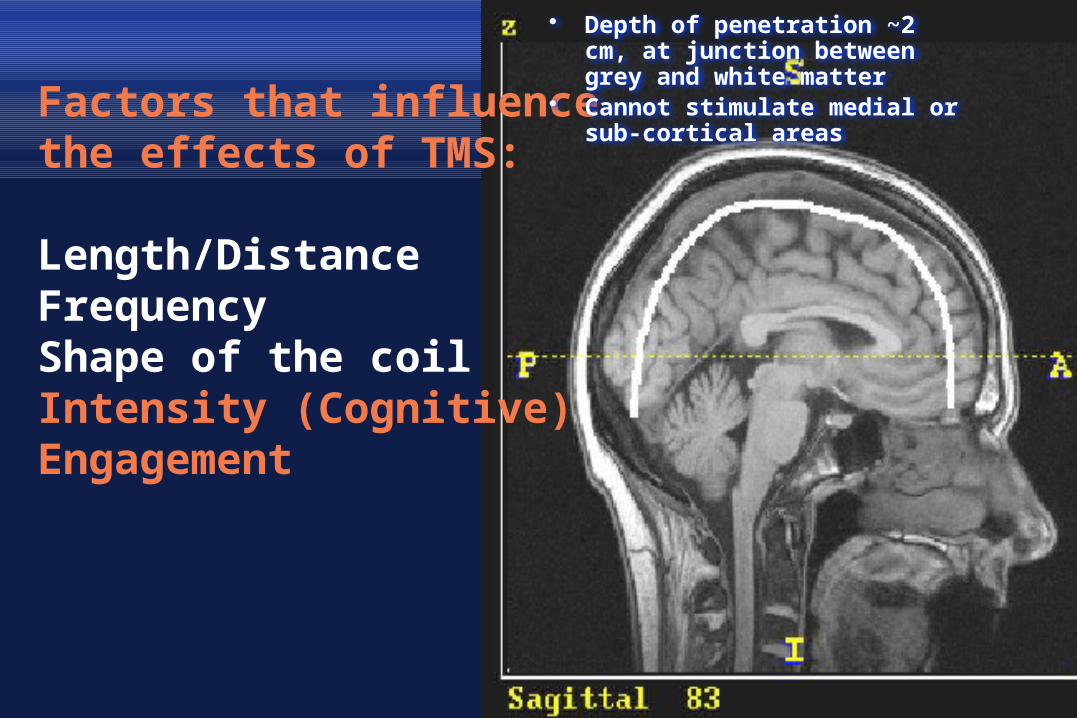
Factors that influence the effects of TMS:
Length/Distance FrequencyShape of the coilIntensity (Cognitive)Engagement
• Depth of penetration ~2 cm, at junction between grey and white matter
• Cannot stimulate medial or sub-cortical areas
THE BIGGEST FACTOR THAT
EFFECTS MOTOR
THRESHOLD IS DISTANCE FROM
THE SCALP TO THE CORTEX
Low
mot
or th
resh
old
Hig
h m
otor
thre
shol
d
FrequencyHigh vs. Low Frequency rTMS
• Low frequency rTMS = stimulation rates 1 Hz
• High frequency rTMS = stimulation rates 1 Hz
• In the motor cortex high frequency rTMS (5-20 Hz) may temporarily increase
excitability while low frequency rTMS may temporarily decrease excitability.
*(TBS) Theta burst suppression3 burst of pulses given at 50Hz & repeated every 200ms
Depression Treatment in 6 minutes
Differences in Two Magnetic Coils
Stimulate 1.5 cm Stimulate 3 cmNon focal
Transcranial Magnetic Stimulation
Neuronetics (2008): 10 Hz for 37.5 min
Brainsway (2013): 18 Hz for 20 min (deep / helmet / H coil)
MagVenture (2015): 35-37 min (theta burst: 5 Hz for 6 min)
Magstim (2015)
4 devices FDA Approved
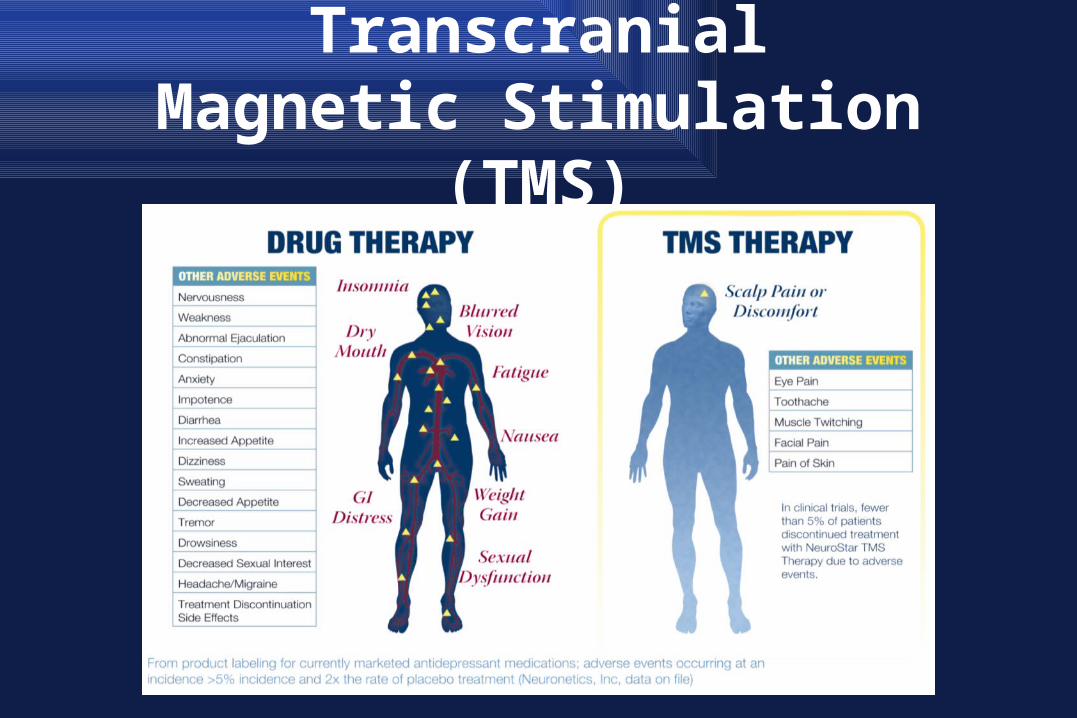
Transcranial Magnetic Stimulation (TMS)

Overview of TMS1) Electrical energy in insulated coil on the scalp induces2) Pulsed magnetic field of about 1.5 Tesla in strength3) Passes unimpeded through thecranium for 2-3 cm4) In turn induces a focal electrical current in the brain5) Get desired local and distal effects on the target neural circuitry6) Delivered as single pulses or repeated trains (rTMS)
Migraine w/aura sTMS – occipital Other TMS Applications?
(April 2016)Pain
acute/chronic: standard LPFC daily several weeks or motor cortex
Fibromyalgiavery positive results (Short, et al 2014)
Stroke recoveryusually subacute (after 2-3 mo): either high frequency ipsilateral or low
frequency contralateral, combined w/rehab
Addictionsability to decrease cue-induced craving in the lab / open label potential
clinical reduction in 1-2/52(Brainsway)
OCDRDLPFC / R orbitofrontal low frequency *acute ?sustained
(Brainsway)
Posttraumatic Stress Disorder
Other TMS Applications(April 2016)
Schizophreniainhibitory stimulus over auditory cortex : decreased auditory hallucinations /
negative sxs
Development Disorders / Autism
Epilepsypatient w/cortical focus / inhibitory TMS can reduce szs
TinnitusTMS over auditory cortex or prefrontal cortex
(VNS)
Depression (LDLPFC)pregnancy / BPD with mood component
DementiaAging/Cognitive Enhancement
Epilepsy (Treatment Assessment
Vulnerability?)
Multiple Sclerosis
(Treatment assessment?,
Staging?)
tACSTranscranial Alternating Current Stimulation
Cranial Electrotherapy Stimulation (CES)‘Electroceuticals’
• April 2016- FDA reclassified tACS (CES) into a split classification
• Tx of insomnia / anxiety: Class II• Tx of depression: Class III• Fisher Wallace Stimulator: alternate
current of 2mA of neurostimulation for 20’ per day
• AlphaStim Device
tDCSTranscranial Direct Current Stimulation
• ¼ potency of TMS• 1-2 milliampere current (ECT: 200 milliamperes)
• floats ‘up & down excitability’ vs TMS which causes depolarization (change resting membrane potential - activated circuit is a better target)
• Build up a tolerance (vs. TMS)?• tDCS will lower the seizure threshold• Shows promise during rehab for aphasia / Hopkins U.
study on cognition in patients with Schizophrenia.• DOD & Video gamers

tDCSTranscranial Direct Current Stimulation• Consumer tDCS devices Thync – neurosignaling product – ‘vibing’ energy vibe or calm vibefoc.us - 5-35 min (intensity/duration) : edream (lucid dreams at 40Hz stim)• Anode (-) (front of head) –cathode (+) (back of
head)like neutroceuticals; St. John’s Wort, Prevagen
Caveat emptor
PsychotherapyPsychotropicmedicationsBrainStimulationPsychotherapyPsychotropicmedicationsBrainStimulationPsychotherapyPsychotropicmedicationsBrainStimulationPsychotherapyPsychotropicmedicationsBrainStimulationPsychotherapyPsychotropicmedicationsBrainStimulationStimulationPsychotherapyPsychotropicmedicationsBrainStim
questions ???Stay tuned