breast cancer low
TRANSCRIPT

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 1/30

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 2/30
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 3/30
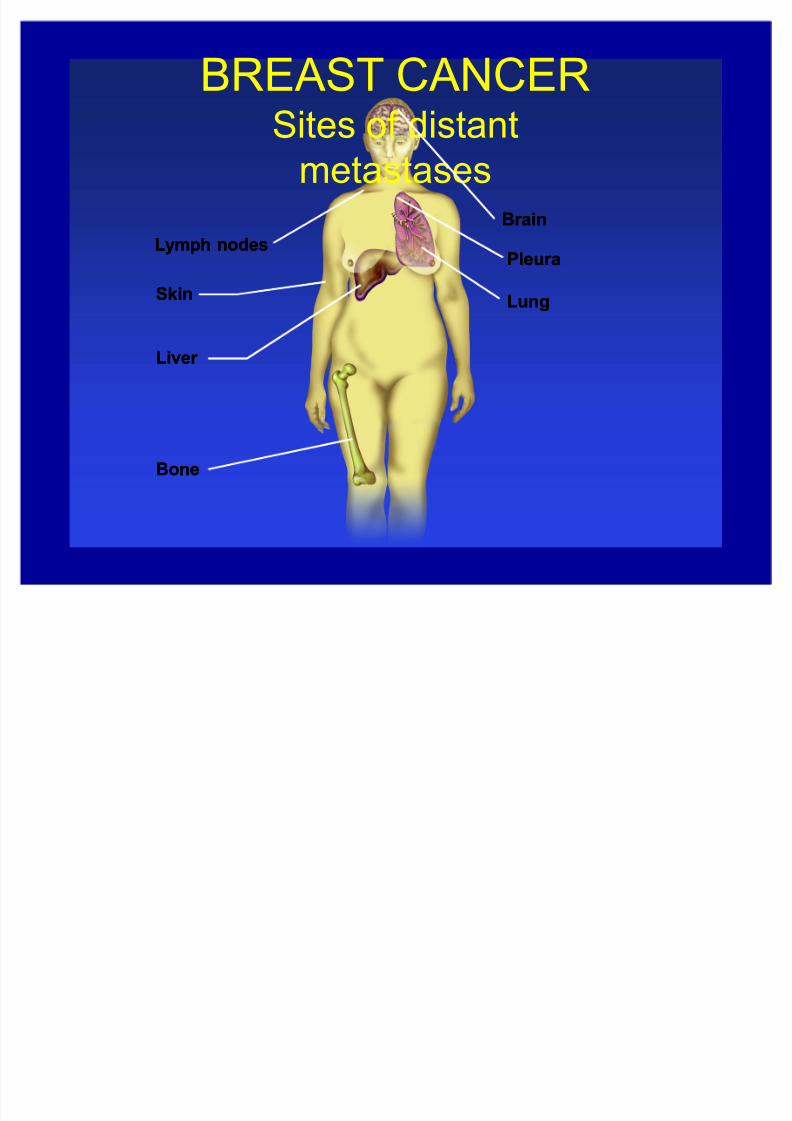
BREAST CANCER
Sites of distantmetastases
SkinSkin
Liver Liver
BoneBone
Pleur aPleur a
LungLung
Lymph nodesLymph nodes
Br ainBr ain

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 4/30
BREAST CANCER
Liver metastasis

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 5/30
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 6/30
Modalities of treatment Surgery may be considered for isolated local
and regional recurrences, possibly for some
isolated metastases Radiation for ³impending catastrophe´ (spinal
cord compression, superior vena cavasyndrome, impending fracture, palliation,
brain metastases) or inoperable local/regionaldisease
Systemic therapy for disseminated disease,disease not falling into above categories
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 7/30
Targeted Therapy in Breast
Cancer Hormone receptor status
± Any Estrogen Receptor (ER) or Progesterone
Receptor (PR) expression indicates possibleresponse to hormonal therapy
± 1% or more cells positive or ER or PR byimmunohistochemistry
Her2/neu (ErbB-2) overexpression ± High overexpression of Her2/neu indicates
possible responder to trastuzumab therapy
ER/PR/Her2 negative patients: chemotherapy
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 8/30
Metastatic Breast Cancer Generally considered incurable
For most patients, primary goal should
be palliation
First recurrences are always biopsied to
confirm diagnosis
± Confirm ER/PR status and Her2/neu status
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 9/30
Metastatic disease:
Systemic therapy principles Hormonal therapy for indolent disease
Single agent chemotherapy for
aggressive/symptomatic disease or
disease not responsive to hormonal
therapy
Polyagent chemotherapy for visceralcrisis or disease requiring rapid response

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 10/30

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 11/30
Rationale f or Hor monal Treatment
of Breast Cancer Endocrine manipulation can:
± Decrease levels of estrogen thatstimulate tumor growth
± Block estrogen inter action withestrogen receptors
Less toxicity
Response r ates in metastatic disease: ± 30% of unselected patients
± u50% of ER-positive patients

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 12/30
Hormonal Therapies
(FDA indications) 1st line therapy:
± Tamoxifen, anastrozole (Arimidex),
letrozole (Femara) 2nd line therapy:
± Fulvestrant (Faslodex), toremifene(Fareston), exemestane (Aromasin)
³Palliative´
± Goserelin (LHRH analog, Zoladex)
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 13/30
Hormonal Therapies for Post-
menopausal Metastatic Tamoxifen 20 mg po daily
Aromatase inhibitors:
anastrozole 1 mg po daily, letrozole 2.5 mg po daily
exemestane 25 mg po daily
Fulvestrant 250 mg IM q month
Megace 40 mg po QID
Aminoglutethimide 250 mg po QID with
hydrocortisone

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 14/30

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 15/30
Treatment Sequence f or
Postmenopausal Women With
Metastatic Breast Cancer
First lineFirst line
Second lineSecond line
Third lineThird line
Fourth lineFourth line
Chemother apyChemother apy
Antiestrogen or Nonsteroidal Antiestrogen or Nonsteroidal Aromatase Inhibitor (AI)Aromatase Inhibitor (AI)
Nonsteroidal AI or AntiestrogenNonsteroidal AI or Antiestrogen
Steroidal AISteroidal AI
ProgestinProgestin
Fif th lineFif th line AndrogenAndrogen
if responseif response
if responseif response
if responseif response
NoNoResponseResponse

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 16/30
Treatment of Metastatic Breast Cancer :
Cytotoxic Agents
Anthr acyclines (doxorubicin, liposomal doxorubicin)
Cyclophosphamide
Taxanes (paclitaxel, docetaxel)
Antimetabolites (5-FU, capecitabine)
Gemcitabine Vinorelbine
Carboplatin/cisplatin

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 17/30
Her2/neu status
Membrane-associated tyrosine kinase
receptor (aka erbB2) related to EGF
± Expressed in breast cancers, DCIS, and
some other tissues such as heart
± Overexpressed in 25-30% of breast
cancers
± Associated with more aggressive diseaseand worse prognosis

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 18/30
Measurement of Her2/neu Measured by immunohistochemistry (IHC)
± Graded 0, 1+, 2+, or 3+
± Based on characteristics of staining ± 0-1 = negative
± 2 = indeterminant, should be followed with FISH(fluorescent in situ hybridization) to determinestatus (amplified/not amplified)
± 3 = positive
Fluorescence In Situ Hybridization (FISH)correlates with response to Herceptin, butmore expensive than IHC

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 19/30
Trastuzumab (Herceptin) Humanized monoclonal antibody against her2/neu
FDA approved for metastatic breast cancer in 1998
Responses in patients with her2/neu positive breast
cancer ± IHC 3+
± FISH positive
Single agent therapy has 26% response rate as 1st line
therapy May be given as an IV infusion weekly or every 3
weeks

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 20/30
Herceptin + Chemotherapy Response rate approx 25% as single agent,
as high as 75% in combination therapy
± Taxol ± Taxotere
± Vinorelbine
± Gemcitabine
± Capecitabine
± Taxane/platinum
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 21/30
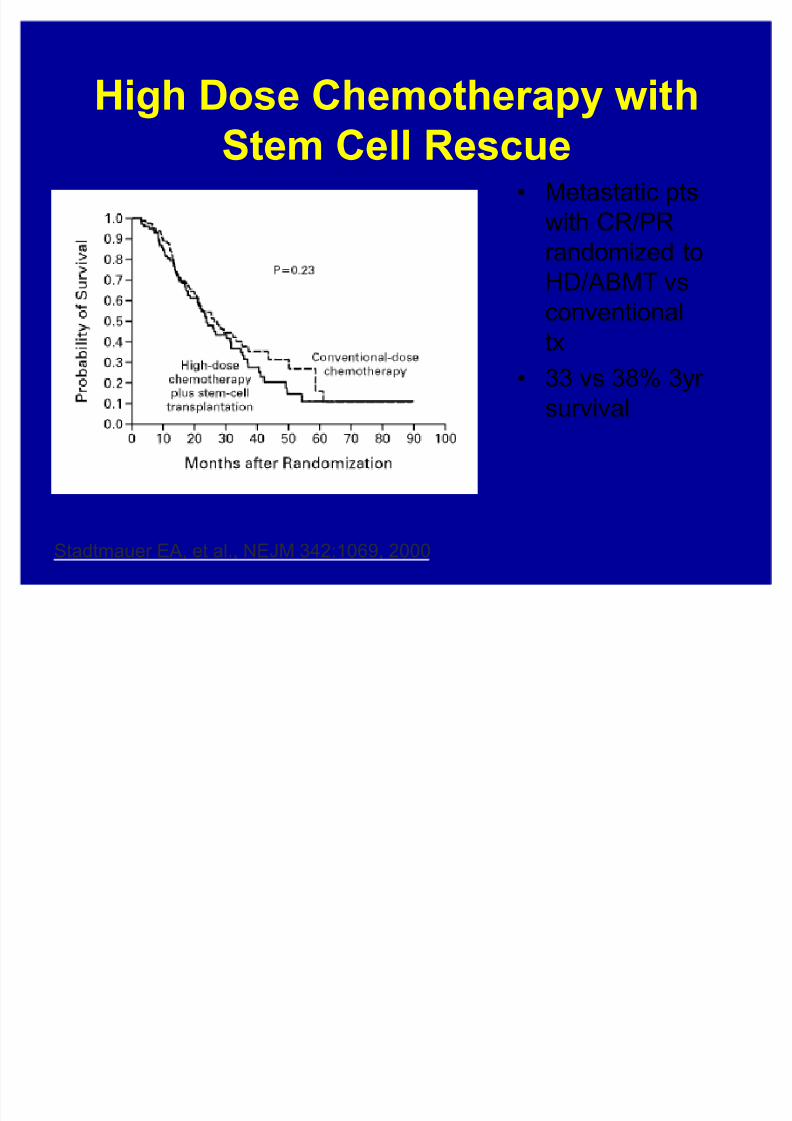
High Dose Chemother apy with
Stem Cell Rescue Metastatic pts
with CR/PR
randomized to
HD/ABMT vsconventional
tx
33 vs 38% 3yr
survival
Stadtmauer EA, et al., NEJM 342:1069, 2000

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 22/30
Pamidronate in Metastatic Cancer Biphosphonates inhibit osteoclast-
induced bone resor ption
380 r andomized patients ± stage IV disease with at least 1 lytic bone
lesion
± 195 patients: chemother apy + placebo
± 185 patients: chemother apy plus
pamidronate (90 mg IV q month x 12)
Hortobagyi GN et al, NEJM 335: 1785-1791, 1996

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 23/30
Pamidronate decreases skeletal
complications in breast cancer
Hortobagyi GN et al, NEJM 335: 1785-1791, 1996
43% vs 56%
had anyskeletal
complication
after 12
months of
therapy

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 24/30
Zoledronic Acid (Zometa)
Bisphosphonic acid ± inhibitor of osteoclastic bone resorption
Indicated for solid tumor patients with
bone metastases 4 mg IV over 15-30 minutes
Check serum creatinine before each
administration Comparable in efficacy to pamidronate
± Rosen LS, Cancer J 7:377, 2001

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 25/30
Metastatic disease: More
thoughts on palliation Because metastatic breast cancer is not
considered curable, there are very few
imperatives of treatment regimens Clinical trials at any point of metastatic
diagnosis is appropriate
Treatment should be individualized tomaximize the patient¶s needs and lifegoals
8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 26/30
NCI Phase II Clinical Trials for
Breast Cancer BMS-247550
± Epothilone B analog
± Microtubule
stabilizer ± Active in taxane
resistant tumors
Phase II trial
± Measurable disease
± Metastatic or locally
advanced patients
for whom you would
consider taxane
therapy
Tamoxifen/Zarnestra ± Oral farnesyl
transferaseinhibitor, (inhibitsras oncogenepathway)
± May reversetamoxifen
resistance Phase II trial
± Measurabledisease
± Hormone receptor positive
T cell depleted
allogeneic stem
cell transplant
± Immunotherapyto induce a graftvs tumor effect
Phase II trial ± Measurable
disease ± HLA matched
sibling donor
± Prior chemotherapy

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 27/30
Metastatic Breast Cancer
Case Presentation
Patient CC
Jennifer Low, MD, PhD

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 28/30
Case Presentation
At age 30, found to have stage IIIA rightbreast cancer ± ER/PR positive, her2/neu negative
± Treated with neoadjuvant chemotherapy, then
mastectomy with lymph node dissection andradiation and tamoxifen
1st recurrence at right chest wall duringradiation therapy
± Treated with radiation 2nd recurrence to spine a few months later
± Treated with radiation, removal of ovaries

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 29/30

8/8/2019 Breast Cancer Low
http://slidepdf.com/reader/full/breast-cancer-low 30/30
Case Presentation, cont. After Herceptin + Taxol:
± NCI Clinical trial with docetaxel and
flavopiridol (with progressive disease)
± NCI Clinical trial with BMS-247550
(epothilone analog) for 8 months with
partial response
± Herceptin + Vinorelbine since July with
stable disease