breast hormone receptors: putting today in focus and...
TRANSCRIPT

Breast Hormone Receptors: Putting today in
focus and tomorrow in prospective
Merdol Ibrahim UK NEQAS ICC & ISH, London

OUTLINE OF TALK
Breast hormonal Receptors (ER & PR)
• Is there really a testing problem?
• What’s being used in IHC
• Choices and trends
• IHC vs mRNA
HER2
• Recommendations
• Audit data

UK NEQAS ICC & ISH
• Service now running for over 25 years
• Assess the Quality of IHC & ISH & Provide Objective Help &
Advice
• Commercially independent & ‘not for profit’
• 4 Assessments per year- Allows for continued improvement
• Accredited EQA scheme and undergoing ISO 17043
accreditation
Accredited EQA Scheme
No: 044

Breast Hormone Receptors
Is there an Issue?

Breast hormone Receptor Issues
Dextran-Coated Charcoal (DCC) Assay
1. McGuire WL (1973) Estrogen receptors in human breast cancer J Clin Invest. 52 (1):73-77.
1984

Breast hormone Receptor Issues
Canada
Healthcare Management Forum – Fall 2010
39.1% false –ve results
2010

Breast hormone Receptor Issues
UK 2012

Cellular Pathology: The chain of events
Preanalytic
Fixation
Analytic 2
interpretation
Analytic 1
Technical
IHC/ISH
Staining
Uncertainty: What’s Yours? (workshop n =53)
• Fixation
• Transport • Methods/assays
• Controls
• Reporting
• TATS
• Audits
• IT

- Appropriate container for sample
- minimum 15–20:1 ratio fixative to tissue
Fixation
Image from: www.southend.nhs.uk Plastic bags not recommended

Breast ER IHC
Pre-treatment Biggest Factor Between Good & Poor IHC

1990’s IHC: High False-negative staining
IDC: 50-75%
Intensity: Medium
Allred = 6
Breast
Hormonal
Receptors

Oestrogen Receptors - EQA Material 1990’s: High frequency of False +ve’s
IDC: 0%
Intensity: Negative
Allred = 0

Oestrogen Receptors - EQA Material UK NEQAS: Era-ve lines (HT-29) = False +ve Staining
IDC: 0%
Intensity: Negative
Allred = 0
Cell lines kindly provided by Dako

Same Antibody = Two Results: Whose right?
Colon adenocarcinoma
Xenograft
A’ False +ve?
B’ As expected
Distributed ER -ve Breast
tumour
On Bond III
+
High pH retrieval
+
Bond Refine
Detection
False +ve? A
Ventana Benchmark
+
High pH retrieval
+
Ultraview Detection
B As expected
6F11

ER – Multiple Methodologies
UK Data : Assessment 96 (2012)
6F11 (Concentrate) Clone on The Leica Bond Max
Retrieval Methods: 32% Low pH (recommended protocol) & 68% High pH
7 Retrieval
Times (mins)
10
15
20
25
30
35
40
11
Antibody
dilutions
1:20
1:50
1:60
1:75
1:80
1:100
1:150
1:200
1:250
1:300
1:400
4 Incubation
Times (mins)
15
20
20
30
60
Too Many Protocols!
Labs have their
preferences!
22/29 (76%) * =
Protocol Variations *Labs who submitted
complete Methods
+ +

6F11: Correct Result Can be Achieved

Breast PR IHC

mouse monoclonals
636, 16, 1A6
Rabbit monoclonals
1E2 , SP2
Progesterone Receptors (Nov 2006)
2006 Some cause for concern
>80% 10-30% negative

Published SP2 Recommendation & What the lab likes to use
‘NO ANTIGEN RETRIEVAL’
Huang et al. (2006) Appl Immunohistochem Mol Morphol. 14(2):229-33.
EQA
Assessments
SP2 clone
users
75 (2006) 30 (6 UK labs)
79 (2007) 15 (0 UK labs)
93 (2011) 3 (0 UK labs)

What’s Happening to PR Now?
Leica PR clone 16
(isoform A)
Dako PgR 636
(isoform A & B)
Roche 1E2
(isoform A & B + C?)
Colon Adenocarcinoma

Run 102: 1E2 Small Change in Protocol = Big Difference
Routine Protocol
• Antibody: 1E2 (predilute)
• Retrieveal: CC1 - 52 mins
• Incubation: 44 mins; RT
Adapted Protocol
• Antibody: 1E2 (predilute)
• Retrieveal: CC1 - 64 mins
• Incubation: 44 mins; 37°C
• Dako protein block: 28 mins
More Sensitive Antibody?
OR More Sensitive Methods = Non-specific Staining

Run 102 PR: Inclusion of Tonsil as a Negative Control
1E2 Routine Protocol 1E2 with Dako block Dako PgR 636
Inclusion of Tonsil in Breast Control
• Out of 30 participants with PR False -ve
• 90% (27/30) showed +ve staining in tonsil

PR (1E2 clone) antibody Pre-diluted but numerous
retrieval and incubation times
3
Retrieval
Times (mins) CC1 mild
(32mins)
CC1 Standard
(60mins)
CC1 Extended
(90mins)
1 Antibody
dilutions
Pre-dilute
14
Incubation
Times (mins) 8
12
13
16
20
24
28
30
32
36
40
44
48
52
60
+ +
Average Score 17/20
Very good
14/25 (56%) * =
Protocol Variations *Labs who submitted
complete Methods
EQA – Score Guide
13-20/20 = Acceptable
10-12/20 = Improvements Required
<9-20 = Unacceptable e.g. False +/-

PR: Clinical Case Submitted by Participant:
1E2 on Sequential Core Biopsies
Ventana Ultra, CC1 standard,
44 mins. incubation
Ventana recommended
protocol; CC1 standard,
16 mins incubation
Ventana Ultra, CC1 standard,
44 mins. Incubation + Dako protein
block (at the UltraBlock step)

UK: Change in ER Antibody Usage
17%
3%
68%
29%
28%
15%
40%
0%
10%
20%
30%
40%
50%
60%
70%
80%
1D5 6F11 EP1 SP1
Year 2007 2015
1D5
EP1
6F11
SP1
2011

UK: Change in PR Antibody Usage

UK Breast ER
EQA Pass Rates 2004-2015
5% 7%
88%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
67
69
71
73
76
79
81
83
85
87
89
91
93
95
97
10
1
10
4
10
6
10
8
unacceptable Borderline acceptable
2004 2015

UK NEQAS ER Audit Data
2009-2012
PR
• Overall = 67.4%
• Primary = 68.4%
• Metastatic = 44.6%
ER
• Overall = 82.6%
• Primary = 83.7%
• Metastatic = 69.7%
Screened vs symptomatic rates
being analysed

ER (09-12): UK Individual Participant Audit Data &
95% Conf. intervals
88%
77%
83%
+5.25%
94%
73%
70
75
80
85
90
95
n=
404
54
n=
400
0
n=
400
n=
200
2 (
n=
1,7
83)
6 (
n=
1,6
33)
8 (
n=
1,5
01)
10
(n
=1
18)
16
(n
=1
94)
24
(n
=2
03)
28
(n
=1
,666
)
29
(n
=2
52)
31
(n
=4
60)
32
(n=
1,7
20
)
35
(n
=2
,271
)
42
(n
=2
56)
43
(n
=1
,318
)
44
(n
=7
08)
45
(n
=3
,705
)
47
(n
=1
,248
)
48
(n
=2
,243
)
49
(n
=6
,774
)
52
(n
=1
,457
)
56
(n
=4
63)
64
(n
=3
,533
)
65
(n
=3
,320
)
71
(n
=3
27)
73
(n
=1
,395
)
75
(n
=2
30)
80
(n
=1
,471
)
81
(n=
20
5)
Anonymised Participant codes (n=) * * * * *

More Sensitive
Antibodies?
Problem
With EQA
Samples?
Protocol Driven
Discordance?
Antibody
validation
based on
concordance =
always a
discordance
Numerous ‘lab-
derived
protocols’
being used
Could be….
But the
majority do get
the ‘expected’
result
So…

Further insights into ‘false +ve’ ER/PR EQA Samples?
Accept the Discordance…End of Story?
• Advanced Cell Diagnostics (Acdbio): October 2013
• RNAScope: mRNA ISH on FFPE slide sections
• Probes available for ER & PR (and a lot more!)

RNAscope on NEQAS Tissue
Year Run Assessment
Result
2012 99 ER
2012 100 PR
2013 102 PR
2013 103 ER
2014 104 ER
2014 105 ER
2014 106 ER
RNAscope QC
Cyclophilin B (PPIB):
RNA integrity
Bacterial DapB:
Tissue fixation
• Initially test integrity of NEQAS breast tumour samples
• Retrospective and prospective quality control
+ve +ve +ve +ve +ve +ve +ve
-ve -ve -ve -ve -ve -ve -ve

Reference: Advanced Cell Diagnostics
• ESR1: transcript variant 4, mRNA
• Number of double Z probe pairs: 40
• Gene region probes designed against: 677-
3065 nucleotides
A’
ER 6F11 IHC Good Comparative
Correlation
Between ER IHC and
mRNA
ESR1 RNAscope mRNA
A High ER+ mRNA high
B B’ Mid ER+ mRNA mid
C C’ Low ER+ mRNA low
High
Low

Run 104 ER Negative: IHC vs RNAScope
A A’
B’ B
ER 6F11 IHC ESR1 RNAscope mRNA

ER Run 104 H-Score:
IHC H-Score vs Devised RNAScope H-Score
SpotStudio (each dot = single mRNA
copy sensitivity)
4 scoring
‘bins’
x %
of
cells
Overall
H - Score
No staining or <1 dot/
10 cells
0 % 0 x % +
1 x % +
2 x % +
3 x % =
score range
0-300
1-3 dots /cell 1 %
4-10 dots/cell 2 %
>10 dots per cell 3 %
intensity x % of cells Overall
H - Score
0 % 0 x % +
1 x % +
2 x % +
3 x % =
score range
0-300
1 %
2 %
3 %
Manual IHC H-Score
Automated mRNA (RNAscope) counts & H-Score

Correlation of ER (6F11) IHC & ESR1 mRNA n= 28
R² = 0.9179
0
50
100
150
200
250
300
0 50 100 150 200 250 300
ES
R1
mR
NA
H-s
core
ER IHC (6F11) H-score)
P<0.00001
Spearman Rank Correlation: r2 = 0.8991
Breast tumour
BT474 MCF7 CAMA-1
CAMA-1 + HT29
Tonsil
Stomach
Tonsil
Compromised
DapB: Poor Fixation
PPIB: mRNA compromised

ER IHC & ESR1 mRNA H-Scores in
External Quality Control Distributed Tumour Samples
0
50
100
150
200
250
300
99 103 104 105a 105b 106
IHC H Score mRNA H score
Retrospective mRNA Prospective mRNA
High
ER +ve
Low-
mid
ER +ve
ER -ve
2012 2014

R² = 0.8934
0
50
100
150
200
250
300
0 50 100 150 200 250 300
PgR
mR
NA
ER IHC (PgR 636)
P<0.00001
Spearman Rank Correlation: r2 = 0.8063
Correlation of PR IHC and PgR mRNA n=20
Breast tumour
BT474 MCF7
Tonsil
CAMA-1
HT29

PR IHC & PgR mRNA H scores in
External Quality Control Distributed Tumour Samples
0
50
100
150
200
250
300
100 102 105 106
IHC MRNA
Retrospective mRNA Prospective mRNA
High
PR +ve
Low
PR +ve
PR -ve
2012 2014
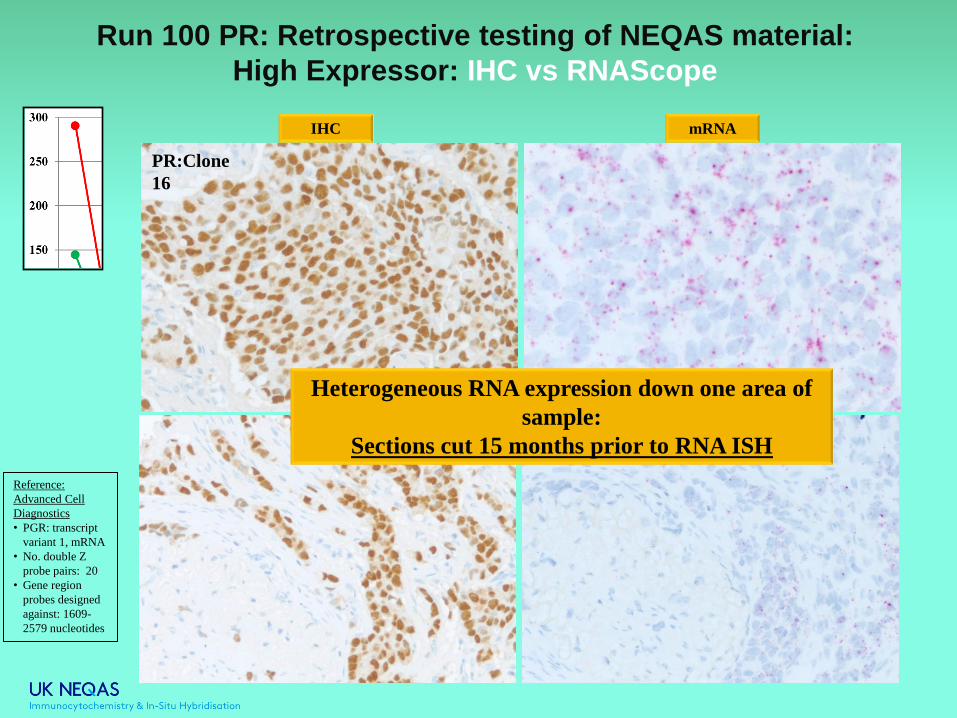
PR:Clone
16
Run 100 PR: Retrospective testing of NEQAS material:
High Expressor: IHC vs RNAScope
Heterogeneous RNA expression down one area of
sample:
Sections cut 15 months prior to RNA ISH
Reference:
Advanced Cell
Diagnostics
• PGR: transcript
variant 1, mRNA
• No. double Z
probe pairs: 20
• Gene region
probes designed
against: 1609-
2579 nucleotides
IHC mRNA

Run 106 PR – Heterogeneity between sections
A
B
Reference:
Advanced Cell
Diagnostics
• PGR: transcript
variant 1, mRNA
• No. double Z
probe pairs: 20
• Gene region
probes designed
against: 1609-
2579 nucleotides
A’
B’
Heterogeneity between section could account for score differences
IHC
mRNA

0
50
100
150
200
250
300
100 100 (repeat)
H-S
core
Assessment Number
IHC
MRNA
PR IHC & PgR mRNA H scores
Repeat Analysis of Samples
0
50
100
150
200
250
300
106 106 (repeat)
H-S
core
Assessment Number
IHC
MRNA
Fresh tissue Sequential Sections
Importance of sample
quality
…EQA Required!

Summary
Breast Hormonal Receptors
• Staining is still variable
• 100% of lab using ‘lab-derived’ Methods
• Discordant ER (6F11) and PR (1E2) Appear to be Protocol
Driven and not necessarily antibody specific
• Adhere to Commercial Companies Protocols
• Use Controls Showing Range of ER/PR Expression
• Continually Audit Clinical Cases
Is mRNA the future?
- IHC & mRNA ISH = Good correlation for ER and PR
- Provides further evidence that some methods = ‘false +ve’ IHC
results
- Further analysis for Ki67 and HER2
mRNA
- Acceptance by pathology community?
- Clinical cut-offs required for every probe!
- Has to be quality controlled

Breast HER2 IHC

HER2 ASCO/CAP recommendations
Correction to: IHC 2+‘incomplete/weak circumferential staining’
ISH: Copy no .>6 = positive

UK HER2 Rates
J Clin Pathol.
2015 68(2):93-99

Importance of Clinical Audit
Web based breast HER2 audit

UK Audit: Different HER2 Methods Produce
‘Similar’ Positivity Rates
Ibrahim et al., (in prep)

New Website … Available in French!

Searchable
‘Best Methods’
Database
June 2015
Select your
language…
Including
French!
Thank You Acknowledgments
• Advanced Cell Diagnostics:
RNAScope
Carried out all mRNA staining
Ruby Hsu
Barry Lynch
Xiao-Jun Ma
Yuling Luo
• Dako: Providing ER/PR Cell
lines
• Roche products, Leica & Dako:
Staining of NEQAS samples
using recommended protocols