broken hearts - putting the pieces togethermudgroup.com/files/kaufman.pdf · image. this will leave...
TRANSCRIPT

To change photo:
1. Delete the current
image. This will leave
a blank placeholder
with a picture icon.
2. Click the icon to add
a new image. The
photo will be
automatically be
cropped to fit the
placeholder.
NOTE: If you use the
“Change Picture”
function,
the image will be
imported in its original
proportions and won’t fill
the placeholder
completely and will
need to be cropped.
Broken Hearts - Putting the Pieces Together
Underwriting CAD
Valerie R. Kaufman, MD
MUD Meeting, 1/30/17
Reinsurance Group of America

2
See Appendix for
instructions on how
to change sidebar
photo
Agenda
Anatomy/Physiology/Pathophysiology review
Epidemiology overview
Preponderance of the evidence
Reconciling discordant test results
Practice guidelines and appropriate use criteria (AUC)

To change photo:
1. Delete the current
image. This will leave
a blank placeholder
with a picture icon.
2. Click the icon to add
a new image. The
photo will be
automatically be
cropped to fit the
placeholder.
NOTE: If you use the
“Change Picture”
function,
the image will be
imported in its original
proportions and won’t fill
the placeholder
completely and will
need to be cropped.
3
Review of Anatomy, Physiology and Pathophysiology

4
See Appendix for
instructions on how
to change sidebar
photo
4
By Coronary.pdf: Patrick J. Lynch, medical illustratorderivative work: Fred the Oyster (talk)adaption and further
labeling: Mikael Häggström - Coronary.pdf, CC BY-SA 3.0,
https://commons.wikimedia.org/w/index.php?curid=9967381
Heart: Exterior

5
See Appendix for
instructions on how
to change sidebar
photo
5

6
See Appendix for
instructions on how
to change sidebar
photo
The Hard Working Heart
The myocardium is constantly working
• Pumps about 5 liters of blood/minute
• About 100,000 heartbeats/day
• Pumps about 2,600 gallons of blood/day
The coronary arteries must provide adequate oxygen and nourishment
Cardiac reserve
• Cardiac output may be increased to as much as 35 liters/minute
• Normal coronary arteries can increase myocardial blood supply 5-6 fold if needed
• Early stages of disease of the heart often associated with reduced cardiac reserve
• Cardiac reserve diminishes with aging
• Atrial fibrillation reduces cardiac output by 10-15%
7
See Appendix for
instructions on how
to change sidebar
photo
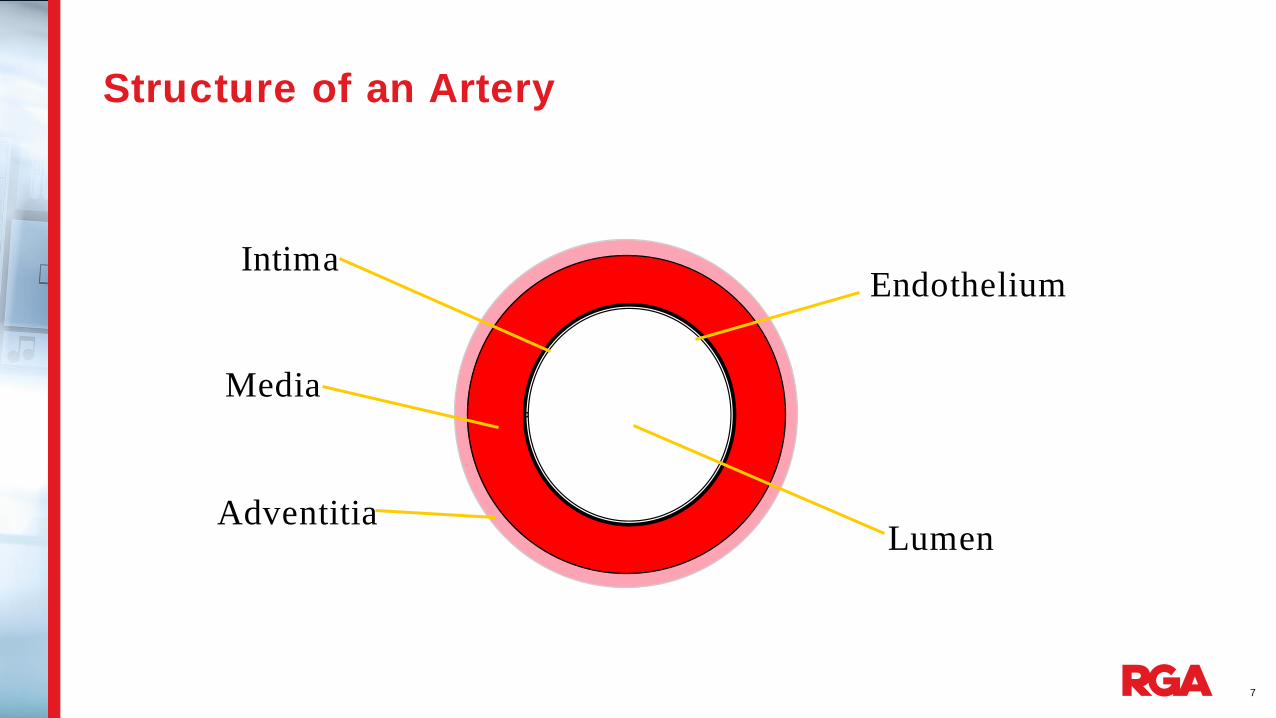
Structure of an Artery
Intima
Media
Adventitia
Endothelium
Lumen

8
See Appendix for
instructions on how
to change sidebar
photo
Stable Obstructive Plaque
Thick Cap
Small Lipid
Core
Calcium

9
See Appendix for
instructions on how
to change sidebar
photo
Nonobstructive Vulnerable Plaque
Large
Lipid Pool
Thin Cap
Inflammation

To change photo:
1. Delete the current
image. This will leave
a blank placeholder
with a picture icon.
2. Click the icon to add
a new image. The
photo will be
automatically be
cropped to fit the
placeholder.
NOTE: If you use the
“Change Picture”
function,
the image will be
imported in its original
proportions and won’t fill
the placeholder
completely and will
need to be cropped.
10
Epidemiology

11
See Appendix for
instructions on how
to change sidebar
photo
Epidemiology
CAD death rate has fallen since 1968
About 15.5 million Americans ≥ 20 years of age have CAD
In 2013
• CAD caused 370,000 deaths
• CAD was an underlying cause of death in about 1 of every 7 deaths
Nearly 1 million coronary events each year
Estimated an additional 160,000 silent MIs each year
About 34% of coronary events are fatal
Mozaffarian D, Benjamin EJ et al on behalf of the American Heart Association Statistics Committee and Stroke Subcommittee. Heart disease and stroke statistics – 2016 update: a report from the American Heart Association. Circulation 2016;133.
US Data

To change photo:
1. Delete the current
image. This will leave
a blank placeholder
with a picture icon.
2. Click the icon to add
a new image. The
photo will be
automatically be
cropped to fit the
placeholder.
NOTE: If you use the
“Change Picture”
function,
the image will be
imported in its original
proportions and won’t fill
the placeholder
completely and will
need to be cropped.
12
Underwriting CAD

13
See Appendix for
instructions on how
to change sidebar
photo
The Heart: a complex organ
• Myocardium
• Conduction system
• Heart valves
• Aorta and arterial
tree
• Coronary arteries

14
See Appendix for
instructions on how
to change sidebar
photo
Underwriting Cardiac Disease – The Evidence

15
See Appendix for
instructions on how
to change sidebar
photo
Putting the Pieces Together . . .

16
See Appendix for
instructions on how
to change sidebar
photo
Case Study #1: 1000 Piece Puzzle
2011 Cardiology note
• FH of early CAD
• H/O HTN, high chol, pre-diabetes
• On statin, BP meds, ASA and metformin
• TC 123, HDL 32
• HgbA1c 5.9%
• 2010 stress echo negative for ischemia, aortic sclerosis and mild aortic insufficiency
• No chest pain or other cardiac symptoms
• BP 140/86
61 year old man, nonsmoker

17
See Appendix for
instructions on how
to change sidebar
photo
Case Study #1 (cont)
2014: progressive dyspnea on exertion for last 3 months
• CAC 2857
• Nuclear stress o Resting EKG with nonspecific ST changes
o Upsloping ST depression and PVCs with hypertensive response.
o Perfusion scan showed partially reversible inferoapical defect and reversible anteroapical defect.
• Cath o LVEDP 26, LVEF 60%
o Left main coronary – moderate calcification with 10-20% distal disease
o Ramus is small caliber with mild disease
o LAD is very tortuous with severe calcification and diffuse 20-30% disease at the midsection
o Circumflex is co-dominant with mild disease proximally and in the 2 small OM branches
o RCA has 30% disease at the midsection
• BP meds adjusted
61 year old man, nonsmoker
18
See Appendix for
instructions on how
to change sidebar
photo
Case Study #1 (cont)
Follow up 3/15, 9/15 – no new symptoms, no testing
Current insurance labs
• HgbA1c 7.5%
• TC 147, HDL 33
• NTproBNP 60

19
See Appendix for
instructions on how
to change sidebar
photo
Case Study #1: Considerations
Enormous CAD burden with CAC nearly 3000
Despite near-maximal risk factor modification program since prior to 2011, had progression of disease with symptoms in 2014
MPI showed multiple perfusion defects
Cath showed extensive disease, but apparently not obstructive
BP not well controlled until last year; EKG abnormal - ? LVH
Now frankly diabetic with HgbA1c of 7.5%
Still relatively young at age 61
61 year old man, nonsmoker
Risk Level: Very High

20
See Appendix for
instructions on how
to change sidebar
photo
Case Study #2: Missing Pieces?
Had cardiac cath in 2012 due to chest pain with elevated troponin
• 80% stenosis mid LAD
• Nonobstructive disease in LCx and RCA
• LVEF 45% with anterolateral hypokinesis
• S/P stent in mid LAD
• Placed on statin, ASA and BP medication
Post-stent stress test in 2012 was negative, and echo showed normal LV function with LVEF 60%
Has had clinical follow up, but no follow up testing. Should we postpone?
56 year old man, nonsmoker

21
See Appendix for
instructions on how
to change sidebar
photo
Case Study #2 (cont)
Is he still on his medications?
What are his risk factors like? (Are the medications effective in reducing risk factors)
Is he diabetic?
Do we have a current EKG?
Do we have NTproBNP?
What do we know about symptoms and functional state?
Does he have any other medical issues?

22
See Appendix for
instructions on how
to change sidebar
photo
Case Study #2 (cont)
Is he still on his medications? YES
What are his risk factors like? (Are the medications effective in reducing risk factors) Chol 150, HDL 55, BP 126/78
Is he diabetic? NO HgbA1c on insurance labs is 5.4%
Do we have a current EKG? YES, it is normal
Do we have NTproBNP? NO
What do we know about symptoms and functional state? Has had regular, alternating PCP and Cardiology visits. No new cardiac symptoms and remains very active.
Does he have any other medical issues? Nothing ratable.
So, should we postpone, or can we assess?

23
See Appendix for
instructions on how
to change sidebar
photo
Follow Up for Stable Ischemic Heart Disease (IHD)
“After being treated, asymptomatic patients are typically at low risk for adverse events”
Key component in follow up: monitor symptoms
Frequency of visits – data sparse. Recommendations based on expert opinion
• May vary by local practice patterns, role of PCP, etc
• Every 4-6 months x 1st year
• Every 6-12 months thereafter if stable
Fihn SD, Gardin JM et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force, American Associati on of Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thorac ic Surgeons. J Am Coll Cardiol 2012;60:e44-164.
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline

24
See Appendix for
instructions on how
to change sidebar
photo Follow Up of Stable IHD – Clinical History and Physical
History
• Response to therapy, adverse effects, adherence to recommendations
• Development of new conditions or changes in existing conditions
• Changes in symptom pattern
• Decreasing functional capacity
Physical exam
Blood Testing
EKG
Fihn SD, Gardin JM et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force, American Associati on of Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons . J Am Coll Cardiol 2012;60:e44-164.
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline

25
See Appendix for
instructions on how
to change sidebar
photo
Follow Up Stress Testing in Stable IHD
“The data supporting follow up testing are sparse and insufficient to support routine, repeat testing in asymptomatic individuals” .
Could be considered
• Evaluation of incomplete revascularization
• Assessment of the adequacy of medical therapy
• Need to evaluate coronary status in anticipation of major noncardiovascular surgery
Fihn SD, Gardin JM et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force, American Association of Thor acic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2012;60:e44-164.
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline

26
See Appendix for
instructions on how
to change sidebar
photo
Follow Up Stress Testing in Stable IHD
Exercise EKG testing
• If at least moderate physical functioning and no disabling comorbidity
• And an interpretable EKG
Stress echo or MPI
• If EKG not interpretable
• If previously required imaging with stress
• Known or at high risk for multivessel disease
Pharmacologic stress test if unable to exercise
Fihn SD, Gardin JM et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force, American Associati on of Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thorac ic Surgeons. J Am Coll Cardiol 2012;60:e44-164.
When new or worsening symptoms (not consistent with acute coronary syndrome)

27
See Appendix for
instructions on how
to change sidebar
photo
Appropriate Use Criteria (AUC)
Developed “to support utilization of high-quality patterns of procedure use (i.e., appropriate use) while informing efforts to reduce use when benefits to patients are unlikely.”
An appropriate imaging study is one in which the expected incremental information, combined with clinical judgment, exceeds the expected negative consequences
Practice guidelines consistent with AUC
Appropriate, May be Appropriate, Rarely Appropriate
Wolk MJ, Bailey SR, et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease. J Am Coll Cardiol 2014;63:380-406.

28
See Appendix for
instructions on how
to change sidebar
photo
Appropriate Use Criteria
Ex EKG Stress
MPI
Stress
Echo
Stress
CMR
CAC CCTA Cath
< 2 years after PCI R R R R R R R
≥ 2 years after PCI M M M M R R R
< 5 years after CABG R R R R R R R
≥ 5 years after CABG M M M M R R R
Asymptomatic, After Revascularization
Symptomatic, After Revascularization
Ex EKG Stress
MPI
Stress
Echo
Stress
CMR
CAC CCTA Cath
Eval of symptoms M A A A R M A

29
See Appendix for
instructions on how
to change sidebar
photo
Case Study #2: Postpone or Offer?
Any indication of clinical change?
• No new symptoms
• Still taking medications, which appear to be effective
• No apparent change in functional status
• No new risk factors
• EKG unchanged and normal
Consider offering with currently
available evidence

30
See Appendix for
instructions on how
to change sidebar
photo
Case Study #3: Preponderance of the Evidence
History of
• DVT following hip surgery (no details) as teenager
• PE after rotator cuff surgery in 2010; on low dose ASA
• Negative cardiac cath (don’t know why done) about 2008
• Negative stress test 2011
• GERD, not on any treatment
3/16: Went to ER due to off and on atypical chest pain x 3 weeks. Concerned about possible recurrent PE
• EKG normal; troponins negative
• CTA negative for PE
57 year old man, nonsmoker

31
See Appendix for
instructions on how
to change sidebar
photo
Case Study #3 (cont)
3/16 evaluation
• Stress MPI:
o 10.3 METs, peak heart rate 144, peak BP 188/76
o Resting EKG normal, no chest pain
o No ST changes or arrhythmias
o Nuclear scan showed a small fixed defect in the mid anterior wall most consistent with old infarct. No evidence of reversibility. Normal wall motion, with EF of 61%
• Resting echo
o LV normal size, normal wall thickness, normal wall motion, EF 60%
o Valves normal
• Discharge summary noted “CAD, new diagnosis”. Begun on atorvastatin and metoprolol, continue ASA

32
See Appendix for
instructions on how
to change sidebar
photo
Case study #3: Preponderance of the Evidence
In Favor of MI
Weighing against MI

33
See Appendix for
instructions on how
to change sidebar
photo
Case study #3: Putting it all together
Mildly increased risk, but likely not due to CAD
MI is possible, but unlikely
History of 2 thromboembolic episodes, both provoked by surgery

34
See Appendix for
instructions on how
to change sidebar
photo
Case Study #4: Muddy Waters?
12/11 Chest pain
• EKG abnormal with nonspecific ST-T changes
• Stress echo o Equivocal ST changes on EKG portion
o Mild LVH (walls 1.2 and 1.2) and mild diastolic dysfunction
o Normal LVEF and wall motion before and after stress
2/15 Screening coronary artery calcium (CAC) score: 1451 (90 th = 1294)
5/15 Occasional nonexertional chest pain
• EKG unchanged
• Resting echo said to be unchanged, but LV walls 1.4 and 1.3, LA 4.6
• Stress test again with equivocal ST changes
• MPI with mostly fixed inferior perfusion defect, possibly due to diaphragmatic attenuation
67 year old man, nonsmoker, BMI 36, treated HTN

35
See Appendix for
instructions on how
to change sidebar
photo
Case Study #4: Questions/Considerations?
Does he have CAD?
Is the CAD causing his chest pain?
Are the stress tests suggestive of ischemia?
What about the LVH?
Any concerns about the combination of LVH and CAD?
67 year old man, nonsmoker

36
See Appendix for
instructions on how
to change sidebar
photo
Case Study #4: Muddy Waters
LVH
• Appears to have worsened between 2011 and 2015
• Check BP control
• Could explain EKG changes
CAD
• CAC > 90th percentile
• Resting EKG abnormal
• Equivocal stress EKG changes
• Stress echo normal 12/11
• MPI equivocal 5/15
LVH + CAD = synergistically unfavorable
Moderately increased risk due to combination of impairments

37
See Appendix for
instructions on how
to change sidebar
photo
Take Aways
Consider all the evidence and try to “put the puzzle together” to get a clear perspective on the risk at hand: “preponderance of the evidence”
1
Give more weight to the more predictive or specific pieces of evidence. 2
Evidence-based clinical guidelines are becoming more important in determining how and when clinical testing should be done 3
Abnormalities of more than one component of cardiac function are often additive and can be synergistic 4

©2015 RGA. All rights reserved.
No part of this publication may be reproduced in any form without the prior permission of RGA.
The information in this publication is for the exclusive, internal use of the recipient and may not be relied upon by any other party other than the recipient and its
affiliates, or published, quoted or disseminated to any party other than the recipient without the prior written consent of RGA.