brown-sequard-plus syndrome with features of autonomic ... · down going toes, rectal exam with...
TRANSCRIPT
Physical Exam
Discussion
Patient History
Imaging
Figure 3 ECG.
.
Figure 4: MRI C Spine.
Brown-Sequard-Plus syndrome with features of Autonomic Dysreflexia and Horner’s syndrome caused by blunt trauma
Epidemiology:Etiology:
Diagnosis :Autonomic dysreflexia:
Treatment:
Prognosis:
Conclusion:
References:
Abstract
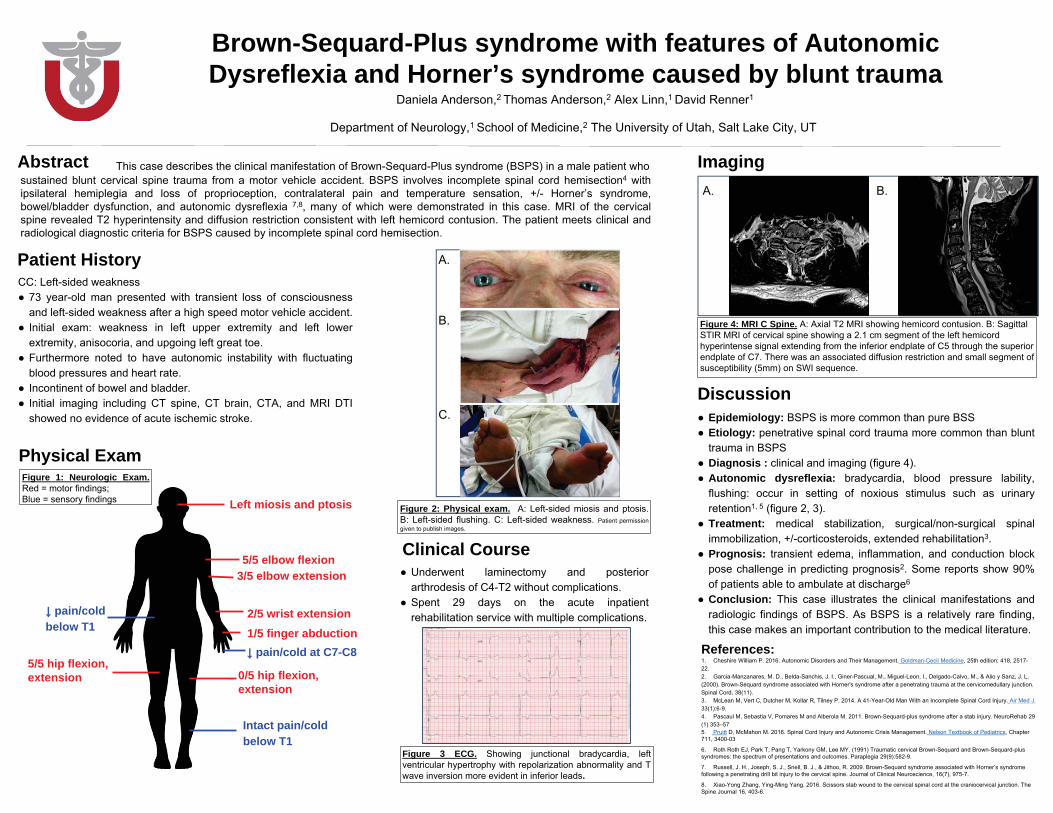
Left miosis and ptosis
5/5 elbow flexion3/5 elbow extension
2/5 wrist extension1/5 finger abduction
0/5 hip flexion, extension
pain/cold below T1
pain/cold at C7-C8
Figure 1: Neurologic Exam.
Figure 2: Physical exam.
5/5 hip flexion, extension
Clinical Course
Intact pain/cold below T1
Acute Arterial thrombosis in a cancer patientDevon Baker, MD, Kenneth Grossman, MD, Benjamin Solomen, MD
University of Utah Hospital/Huntsman Cancer Insitute
Case Description
Introduction
Objectives
Results (Research Only)
Discussion
References1.Histological variants of urothelial carcinoma: diagnostic, therapeutic and prognostic implications, Journal
of Modern Pathology 2009 2.Plasmacytoid variant urothelial bladder cancer: is it time to update the treatment paradigm?, Urologic
Oncology3.Outcome of acute limb ischemia in cancer patients, Vascular Medicine
This case describes a young patient diagnosed previously with a rare metastatic plasmacytoid urothelial cancer who presented with acute paralysis over the preceding 24 hours. The pt was found to have bilateral femoral thrombosis and taken to emergent vascular surgery for thrombectomy. The pt also was found to have compartment syndrome requiring fasciotomy. She did not have any trauma or other symptoms that would have caused compartment syndrome. A CTA done in the ER also showed splenic and renal infarcts and a CT head revealed infarcts in the brain as well. Testing for anticardiolipin antibody was positive. The pt did have a complication of SBO after her surgery requiring bowel resection as well and a long hospitalization. This case highlights a rare complication of hypercoagulability as a result of underlying malignancy. There is very little data available about this patients particular cancer and according to some reviews there are only 75 case reports available.1 It may be that these types of cancer are particularly thrombogenic but it is likely that the pts underlying malignancy led to acute arterial occlusion. She did recover some ability to remove her lower extremities although was still experiencing some paresthesia at discharge and will be on life long anticoagulation going forward.
Initially neurology was consulted for concern over acute paralysis and vascular surgery was consulted concurrently. Neurology workup was deferred after vascular surgery did doppler exam showing no obvious pulses. The pt was taken for emergent vascular surgery and thrombectomy bilaterally and was also found to have compartment syndrome requiring bilateral fasciotomies. The pt regained pulses and was starting to regain some strength in her lower extremities. She continued to have some numbness and tingling in her legs but this did improve over the next several days. The pt developed abdominal bloating and pain which required NG tube for a SBO. The pt had increasing leukocytosis up to 30 but this was thought to be due to the administration of neulasta in the week prior to presentation. The pts sxs did not improve and repeat CT abdomen was done showing bowel perforation. She was taken to the OR a second time and required bowel resection. The pt improved and was eventually discharged after a long hospital stay. She will be on indefinite anticoagulation. There is some thought the pt had catastrophic antiphospholipid syndrome, however follow up labs are needed to diagnose as it is difficult to determine this during acute illness.
Acknowledgements: Dr. Ben Solomen Fellow in Hematology-Oncology for his contributions on this case
This case is a 56 year old female with a PMH significant for plamacytoid carcinoma who presented to the Huntsman Cancer center with 24 hours of progressive bilateral lower extremity weakness. This had been evaluated the day prior in the ER at South Jordan were a MRI of the L spine was done and did not show any spinal cord compression or other etiologies of her sxs. The pt had some improvement at that time and was sent home. The next day she noted worsening of her sxs to the point that she could no loner get up and walk. She was taken to the ACC by her husband for further evaluation. The pt also noted paresthesia that progressed and started in her toes and was now at her knees. By the time she had arrived at the Hunstman she had total numbness in both of her legs up to her knees. She also noted some constipation, but did not have any problems voiding urine.
Physical Exam: significant for numbness bilaterally from the knees down to the toes, decreased hip flexor strength bilaterally 2-3/5, unable to dorsiflex or plantarflex the ankles, absent lower extremity reflexes, Babinski with down going toes, Rectal exam with decreased tone, Ext were cool to the touch and it was difficult to palpate distal pulses
Laboratory studies were positive for thrombocytopenia with platelets in the 80s. Alkaline phosphatase was elevated in the 500s. The pt was also hyponatremia with sodium of 132. LFTs were otherwise normal. Other laboratory evaluation was unrevealing. Further laboratory eval showed elevated cardiolipin IgM antibodies elevated at over 150.
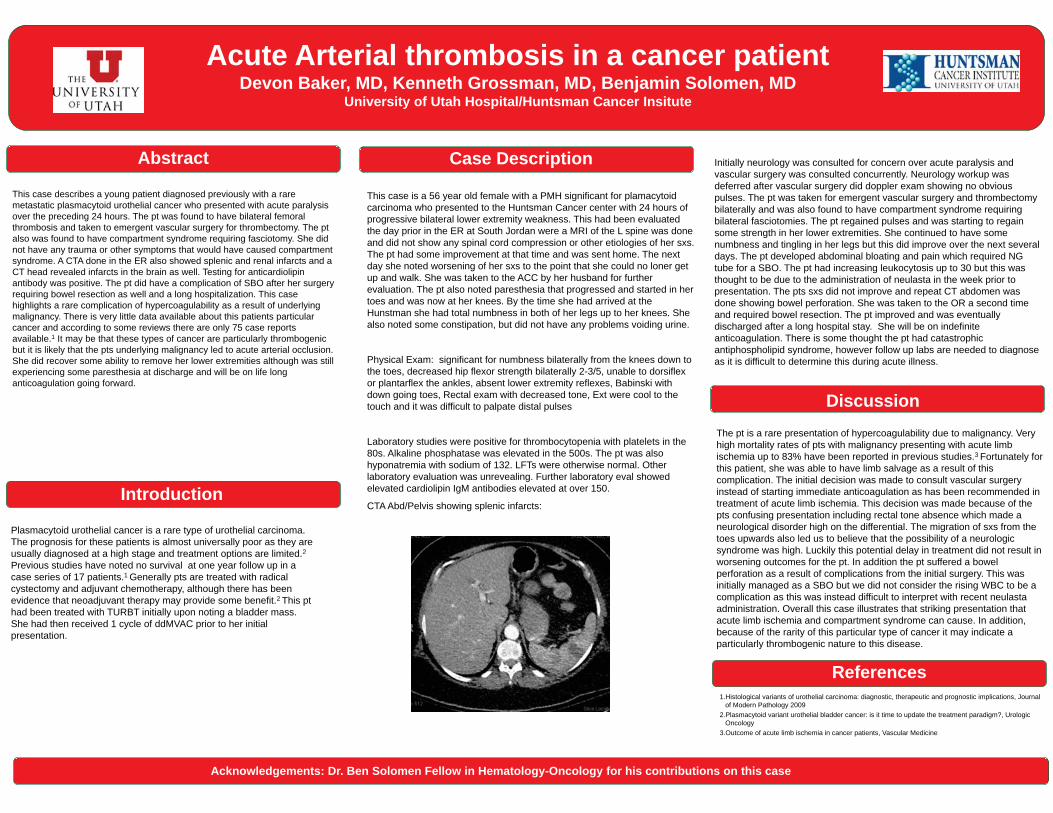
CTA Abd/Pelvis showing splenic infarcts:
The pt is a rare presentation of hypercoagulability due to malignancy. Very high mortality rates of pts with malignancy presenting with acute limb ischemia up to 83% have been reported in previous studies.3 Fortunately for this patient, she was able to have limb salvage as a result of this complication. The initial decision was made to consult vascular surgery instead of starting immediate anticoagulation as has been recommended in treatment of acute limb ischemia. This decision was made because of the pts confusing presentation including rectal tone absence which made a neurological disorder high on the differential. The migration of sxs from the toes upwards also led us to believe that the possibility of a neurologic syndrome was high. Luckily this potential delay in treatment did not result in worsening outcomes for the pt. In addition the pt suffered a bowel perforation as a result of complications from the initial surgery. This was initially managed as a SBO but we did not consider the rising WBC to be a complication as this was instead difficult to interpret with recent neulasta administration. Overall this case illustrates that striking presentation that acute limb ischemia and compartment syndrome can cause. In addition, because of the rarity of this particular type of cancer it may indicate a particularly thrombogenic nature to this disease.
Abstract
Plasmacytoid urothelial cancer is a rare type of urothelial carcinoma. The prognosis for these patients is almost universally poor as they are usually diagnosed at a high stage and treatment options are limited.2Previous studies have noted no survival at one year follow up in a case series of 17 patients.1 Generally pts are treated with radical cystectomy and adjuvant chemotherapy, although there has been evidence that neoadjuvant therapy may provide some benefit.2 This pt had been treated with TURBT initially upon noting a bladder mass. She had then received 1 cycle of ddMVAC prior to her initial presentation.
Pathogenesis of sarcoidosis:• Accumulation of granulomas (Figure 6)• Inciting event is unknown – generally granulomas form to
sequester infection, inflammation, and collateral damage• Granulomas are compact, centrally organized collections of
macrophages and epithelioid cells encircled by lymphocytes• Presence of CD4+ T cells that interact with antigen-presenting
cells to initiate the formation and maintenance of granulomasClinical features:• Diagnosis of sarcoidosis is considered based on abnormalities detected on chest x-ray• Constitutional symptoms are common,
often mimics lymphoma• Organ system involvement greatly varies
(Figure 7)Diagnosis:• Remains a diagnosis of exclusion• Compatible clinical and radiographic findings,
along with histologic finding of non-caseatinggranulomas
• Exclusion of other etiologies of non-caseating granulomas, which includes neoplasms, infections, particles from occupational exposure, etc.
• If diagnosis remains elusive, FDG-PET can be usedto identify organs involved
• Angiotensin-converting enzyme elevated in 60% of patients, use is controversial
• Certain phenotypes of sarcoidosis may not require biopsy for diagnosis (i.e., Lofgren’s syndrome, whichis characterized by erythema nodosum, periarticular inflammation (especially at ankles), and hilar lymphadenopathy)
Treatment• Most organ involvement responds to steroids• Decision to treat pulmonary sarcoidosis is based on pulmonary symptoms, deteriorating lung
function, and progressive radiographic changes• Decision to treat extra-pulmonary sarcoidosis is based on involvement of eyes, CNS, heart,
kidneys, and associated hypercalcemia• Primary treatment: glucocorticoids• Other treatment regimens
• Anti-metabolites, which include methotrexate, azathioprine, mycophenolate, leflunomide • Anti-TNF biologic agents have been used in refractory disease
My Patient• In retrospect, did have a few months of fatigue and cough• Responded well to steroids, but hypercalcemia returned with tapering• Started on mycophenolate• Continues to do well
Granulomas GaloreAnees Daud, MD PGY3
University of Utah Internal Medicine
Case Description
Introduction
Discussion
References1. Al-Kofahi, Khalid, Peter Korsten, Christian Ascoli, Shanti Virupannavar, Mehdi Mirsaeidi, Ian Chang, Naim Qaqish, Lesley
Saketkoo, Robert P. Baughman, and Nadera Sweiss. 2016. “Management of Extrapulmonary Sarcoidosis: Challenges and Solutions.” Therapeutics and Clinical Risk Management Volume 12 (November): 1623–34. doi:10.2147/TCRM.S74476.
2. Horwitz MJ. Hypercalcemia of malignancy: Mechanisms. In: UpToDate, Rosen C.J., et al. (Ed), UpToDate, Waltham, MA. 3. Iannuzzi, Michael C., Benjamin A. Rybicki, and Alvin S. Teirstein. “Sarcoidosis.” The New England Journal of Medicine 357, no. 21
(November 22, 2007): 2153–65. doi:10.1056/NEJMra071714.4. Shane E, Berensen, JR. Treatment of hypercalcemia. In: UpToDate, Rosen C.J., et al. (Ed), UpToDate, Waltham, MA. 5. Shane E. Clinical manifestations of hypercalcemia. In: UpToDate, Rosen CJ, et al. (Ed), UpToDate, Waltham, MA. 6. Shane E. Diagnostic approach to hypercalcemia. In: UpToDate, Rosen CJ, et al. (Ed), UpToDate, Waltham, MA. 7. Tebben, Peter J., Ravinder J. Singh, and Rajiv Kumar. “Vitamin D-Mediated Hypercalcemia: Mechanisms, Diagnosis, and
Treatment.” Endocrine Reviews 37, no. 5 (October 2016): 521–47. doi:10.1210/er.2016-1070.8. Yee, Arthur M. F. “Sarcoidosis: Rheumatology Perspective.” Best Practice & Research. Clinical Rheumatology 30, no. 2 (April
2016): 334–56. doi:10.1016/j.berh.2016.07.001.
Hypercalcemia is a common finding, but can be associated with many uncommon diseases, such as sarcoidosis. Sarcoidosis can be an elusive diagnosis because of the seemingly disconnected organs that are often involved. While “bilateral hilar lymphadenopathy” is the classic chest radiographic finding described in exam questions, the presentation of sarcoidosis can be variable. Up to 30% of patients present with extra-thoracic manifestations of sarcoidosis, and since no single diagnostic modality is sufficient, the diagnosis is often missed or delayed.
Discussed here is the case of a 57-year-old woman who presented with encephalopathy, and was found to have hypercalcemia, along with widespread lymphadenopathy and other internal organ involvement. While the initial imaging modalities were concerning for lymphoma, it was not until additional laboratory and pathologic evaluation was done that the diagnosis of sarcoidosis was solidified. Although the initial treatment of hypercalcemia in this patient was relatively straightforward, confirming the diagnosis of sarcoidosis was important in directing future care.
Management of sarcoidosis can be varied, and treatment is dependent on the level of symptoms and organ involvement. Since this patient’s primary presenting finding was symptomatic hypercalcemia, treatment was indicated. She responded well to steroids, eventually was transitioned to mycophenolate, and continues to do well.
Radiographic Images Courtesy of University of Utah Health Care
This is a case of a 57-year-old woman who was brought by her husband to an outside hospital because of acute onset of encephalopathy. Based on history provided by her husband, she was working in the garden in high heat, and felt unusually tired. The following day, she slept for most of the morning, and was confused upon awaking. She was wandering through the house without purpose, throwing food on the floor, and was not able to prepare for bed or dress herself. When this behavior continued the following morning, her husband became concerned and brought her to their local hospital.
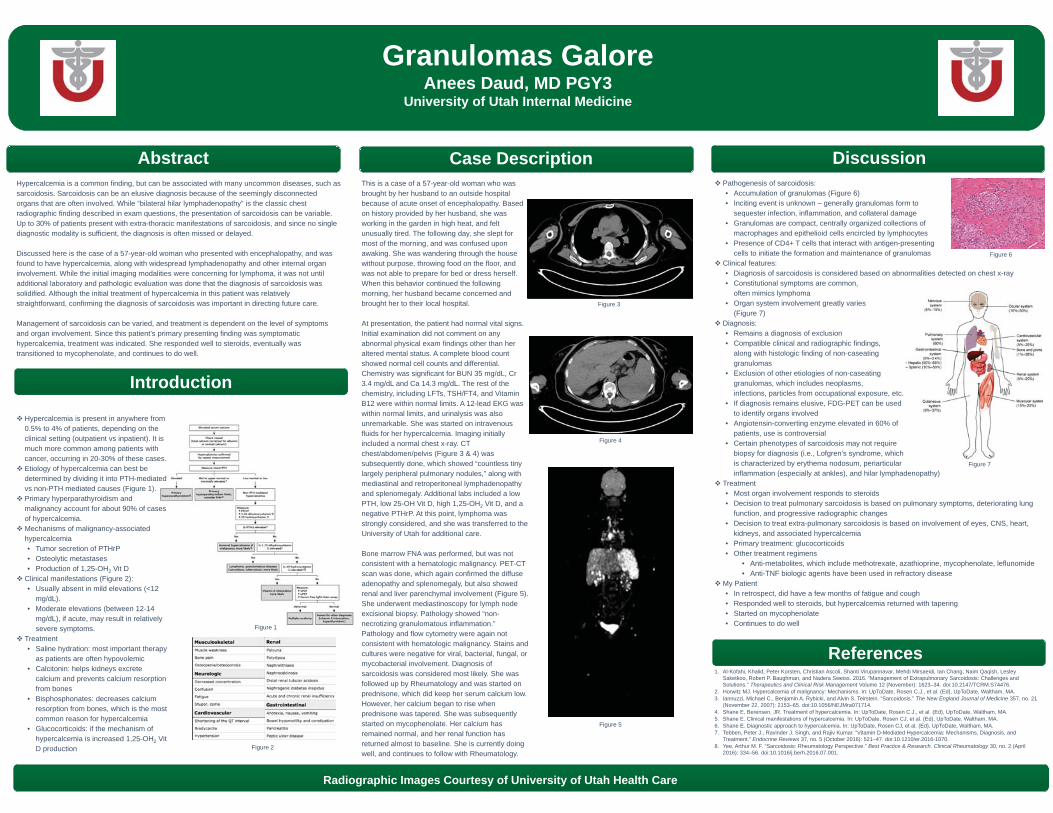
At presentation, the patient had normal vital signs. Initial examination did not comment on any abnormal physical exam findings other than her altered mental status. A complete blood count showed normal cell counts and differential. Chemistry was significant for BUN 35 mg/dL, Cr 3.4 mg/dL and Ca 14.3 mg/dL. The rest of the chemistry, including LFTs, TSH/FT4, and Vitamin B12 were within normal limits. A 12-lead EKG was within normal limits, and urinalysis was also unremarkable. She was started on intravenous fluids for her hypercalcemia. Imaging initially included a normal chest x-ray. CT chest/abdomen/pelvis (Figure 3 & 4) was subsequently done, which showed “countless tiny largely peripheral pulmonary nodules,” along with mediastinal and retroperitoneal lymphadenopathy and splenomegaly. Additional labs included a low PTH, low 25-OH Vit D, high 1,25-OH2 Vit D, and a negative PTHrP. At this point, lymphoma was strongly considered, and she was transferred to the University of Utah for additional care.
Bone marrow FNA was performed, but was not consistent with a hematologic malignancy. PET-CT scan was done, which again confirmed the diffuse adenopathy and splenomegaly, but also showed renal and liver parenchymal involvement (Figure 5). She underwent mediastinoscopy for lymph node excisional biopsy. Pathology showed “non-necrotizing granulomatous inflammation.” Pathology and flow cytometry were again not consistent with hematologic malignancy. Stains and cultures were negative for viral, bacterial, fungal, or mycobacterial involvement. Diagnosis of sarcoidosis was considered most likely. She was followed up by Rheumatology and was started on prednisone, which did keep her serum calcium low. However, her calcium began to rise when prednisone was tapered. She was subsequently started on mycophenolate. Her calcium has remained normal, and her renal function has returned almost to baseline. She is currently doing well, and continues to follow with Rheumatology.
Abstract
Figure 2
Figure 4
Figure 3
Figure 5
Hypercalcemia is present in anywhere from 0.5% to 4% of patients, depending on the clinical setting (outpatient vs inpatient). It is much more common among patients with cancer, occurring in 20-30% of these cases.Etiology of hypercalcemia can best be determined by dividing it into PTH-mediated vs non-PTH mediated causes (Figure 1).Primary hyperparathyroidism and malignancy account for about 90% of cases of hypercalcemia.Mechanisms of malignancy-associated hypercalcemia• Tumor secretion of PTHrP• Osteolytic metastases• Production of 1,25-OH2 Vit D
Clinical manifestations (Figure 2):• Usually absent in mild elevations (<12
mg/dL). • Moderate elevations (between 12-14
mg/dL), if acute, may result in relatively severe symptoms.
Treatment• Saline hydration: most important therapy
as patients are often hypovolemic• Calcitonin: helps kidneys excrete
calcium and prevents calcium resorption from bones
• Bisphosphonates: decreases calcium resorption from bones, which is the most common reason for hypercalcemia
• Glucocorticoids: if the mechanism of hypercalcemia is increased 1,25-OH2 Vit D production
Figure 1
Figure 6
Figure 7
Seeing Double:A Rare Presentation of Non-Hodgkin Lymphoma
Lindsey Fitzgerald, MDUniversity of Utah
Discussion
References1. Yu Y, Ren M, Qi X. Pathologically proven peripheral neurolymphomatosis. Neurol India 2016;64:805-72. Grisariu S, Avni B, Batchelor TT, van den Bent MJ, Bokstein F, Schiff D, et al. Neurolymphomatosis: An International
Primary CNS Lymphoma Collaborative Group report. Blood 2010;115:5005-113. Baehring JM, Damek D, Martin EC, Betensky RA, Hochberg FH: Neurolymphomatosis. Neuro-oncol 5: 104–115, 20034. Norden A, Hochberg E, Hochberg F. Clinical presentation and diagnosis of secondary central nervous system
lymphoma. UpToDate. Last updated: April 04, 2016 5. Shree R, Goyal MK, Modi M, et al. The diagnostic dilemma of neurolymphomatosis. J Clin Neurol. 2016 Jul; 12(3):
274-816. Mead GM, Kennedy P, Smith JL, et al. Involvement of the central nervous system by non-Hodgkin's lymphoma in
adults. A review of 36 cases. Q J Med. 1986;60(231):699
Acknowledgements: Dr. Corwin Edwards, for providing pathology photomicrographs
Abstract• This case demonstrates the timely identification of malignant nervous system involvement. • Why this patient most likely had NL:
• The significance of prompt recognition lies in the potential for rapid treatment to prevent further neurologic morbidity and preserve quality of life. Despite absence of definitive NHL classification,which would determine overall treatment, R-CHOP was initiated as the oncologist recognized that delaying treatment may worsen neurologic morbidity.
Neurolymphomatosis (NL) is a rare clinical entity that can be a manifestation of non-Hodgkin lymphoma and leukemia. This poster illustrates the case of a 65 year-old female presenting with symptoms suggestive of stroke. However, upon further evaluation, she is diagnosed with non-Hodgkin lymphoma (NHL) and neurologic morbidities become attributable to NL.
Learning Objectives:• Consider neurolymphomatosis in the differential diagnosis of patients with or without NHL
presenting with neurologic complaints. • Prompt recognition can prevent neurologic deterioration and prolong survival.
Case DescriptionHPI• A 65 year-old female presents with weakness,
double vision, and slurred speech. • Symptoms occurred acutely and have
progressively worsened• In the ED, the patient also endorsed
headache, abdominal pain, nausea, and dry heaves.
• She was noted to have multiple cranial nerve palsies on exam; thus, the stroke team was activated.
Past Medical History1. Cirrhosis of the Liver, secondary to chronic Hepatitis C infection. Complicated by ascites, esophageal varices, chronic thrombocytopenia.2. Hepatitis C, cured s/p Harvoni treatment 20153. Depression with Anxiety, Insomnia4. Hypothyroidism
Family HistoryNoncontributory
Social History• Lives locally with family and works part-time as
a Costco sales associate• Former smoker with >40 pack-year history• Quit drinking alcohol 10 years ago.
Medications on AdmissionPropranolol, Sertraline, Levothyroxine, Ambien
PHYSICAL EXAMVital Signs: 157/90 | HR 58 | RR 17 | Temp 36°C| O2 Saturation: 96% on room air
Physical examination was notable for:• inward gaze of the right eye (CN IV palsy)• right-sided facial droop (CN VII palsy)• mild slurring of speech (CN IX/X)• Strength was full and sensation was intact. • NIH Stroke Scale of 5
Hospital Course
Introduction• Secondary involvement of the nervous system by NHL
can manifest in multiple ways, including: • leptomeningeal metastasis • parenchymal brain metastasis• intramedullary spinal metastasis• neurolymphomatosis• paraneoplastic disease.
• Neurolymphomatosis (NL) is a rare manifestation of NHL and is defined as the invasion of peripheral nerve roots by malignant lymphoma cells, typically involving the cranial or spinal nerve roots.
• The most common presentations include: peripheral neuropathy or radiculopathy, cranial neuropathy, or painless polyneuropathy.2
• In a large retrospective study on NL, the majority of cases were due to B-cell NHL. NL was the initial presenting feature in 26% of those cases.2
• The prompt recognition of NL is imperative to providing rapid treatment to prevent further neurologic deterioration and possibly prolong survival.
High Clinical Suspicion
Histopathology•Nerve biopsy•Post-mortem
Multi-Modal Imaging Studies
• high-resolution MRI
• FDG-PET
Figure 1 – Diagnosis of NL is difficult and requires a combination of clinical
suspicion, multimodal imaging, and a nerve biopsy. Typically, conventional MRI and CT
imaging are normal in NL.
Diagnosis of NL
KEY POINTS• Keep secondary involvement of the CNS by NHL on the differential diagnosis in patients
presenting with neurologic complaints• Rapid control of the disease can prevent neurologic morbidity and potentially prolong survival
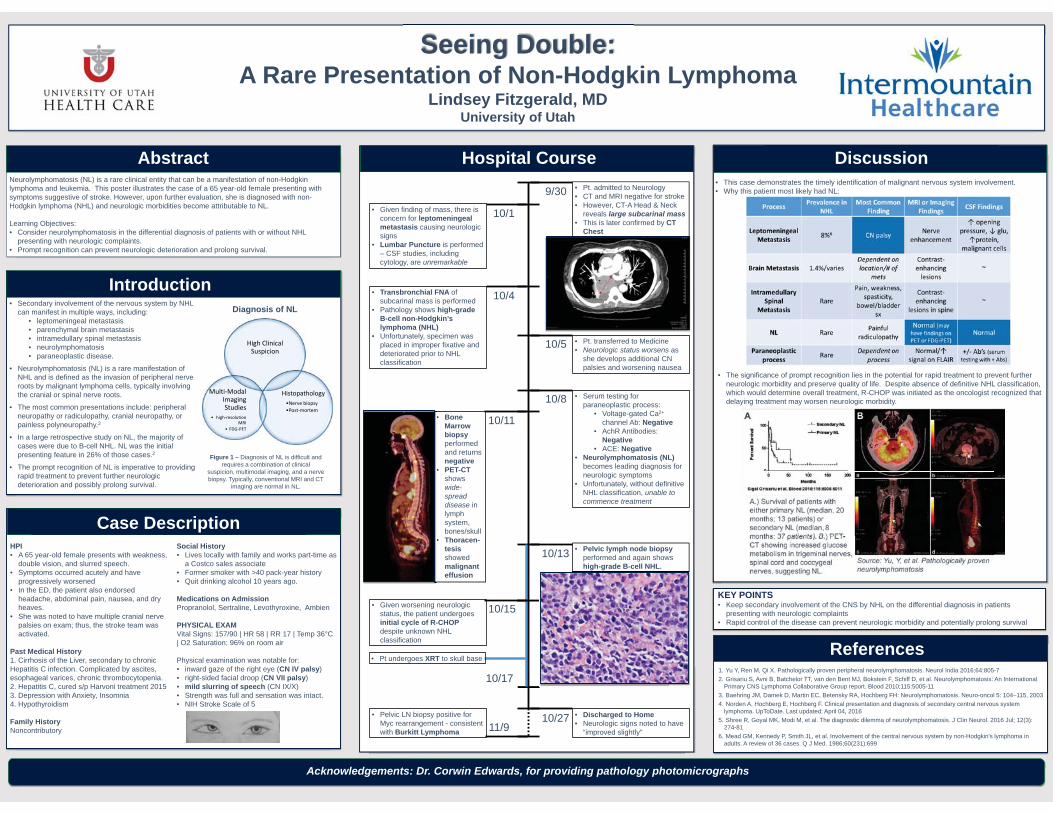
9/30
10/1
• Pt. admitted to Neurology• CT and MRI negative for stroke• However, CT-A Head & Neck
reveals large subcarinal mass• This is later confirmed by CT
Chest
• Given finding of mass, there is concern for leptomeningealmetastasis causing neurologic signs
• Lumbar Puncture is performed – CSF studies, including cytology, are unremarkable
10/4• Transbronchial FNA of subcarinal mass is performed
• Pathology shows high-grade B-cell non-Hodgkin’s lymphoma (NHL)
• Unfortunately, specimen was placed in improper fixative and deteriorated prior to NHL classification
10/5 • Pt. transferred to Medicine• Neurologic status worsens as
she develops additional CN palsies and worsening nausea
• Serum testing for paraneoplastic process:
• Voltage-gated Ca2+
channel Ab: Negative• AchR Antibodies:
Negative• ACE: Negative
• Neurolymphomatosis (NL) becomes leading diagnosis for neurologic symptoms
• Unfortunately, without definitive NHL classification, unable to commence treatment
10/8
10/13 • Pelvic lymph node biopsyperformed and again shows high-grade B-cell NHL.
10/17
• Pt undergoes XRT to skull base
10/27 • Discharged to Home• Neurologic signs noted to have
“improved slightly”11/9• Pelvic LN biopsy positive for
Myc rearrangement - consistent with Burkitt Lymphoma
10/11• Bone Marrow biopsy performed and returns negative
• PET-CTshows wide-spread disease in lymph system, bones/skull
• Thoracen-tesisshowed malignant effusion
10/15• Given worsening neurologic status, the patient undergoes initial cycle of R-CHOP despite unknown NHL classification


NAILING THE DIAGNOSIS:A CASE OF PLANTAR PAIN, PLANTAR KERATODERMA, & TOENAIL DYSTROPHY
Than
k yo
u to
Pac
hyon
ychi
a Co
ngen
ita P
roje
ct fo
r pro
vidi
ng th
e pa
tient
imag
es.
II. Case Description
The physician suspects genetic etiology and ordersgenetic testing for inherited skin diseases. The resultsshow a mutation in the KRT16 gene, and the patient iscorrectly diagnosed with the PC-K16 subtype of PC.
The patient is referred to the Pachyonychia CongenitaProject, a non-profit that provides genetic testing andsupports medical research for PC. It also serves as a hubfor the PC community worldwide. Follow-up care beganto address appropriate pain management. Currently, nocure exists for PC.
III. Diagnosis & Management
Laura J. Gardner, University of Utah School of Medicine | C. David Hansen MD, Department of Dermatology, University of Utah
Eliason, M. J., MD, Leachman, S. A., MD, PhD, Feng, B., PhD, Schwartz, M. E., AA, & Hansen, C. D., MD. (2012). A review of the clinical phenotype of 254 patients with genetically confirmed pachyonychia congenita. Journal of the American Academy of Dermatology.
Fu, T., Leachman, S. A., Wilson, N. J., Smith, F. J., Schwartz, M. E., & Tang, J. Y. (2011). Genotype–Phenotype Correlations among Pachyonychia Congenita Patients with K16 Mutations. Journal of Investigative Dermatology, 131(5), 1025-1028.
Pachyonychia Congenita Project. (n.d.). Retrieved January 13, 2017, fromhttp://www.pachyonychia.org/
IV. References
www.pachyonychia.org
Laura J. GardnerUniversity of Utah School of Medicine
JL is a 31yo woman presenting to internal medicineclinic for evaluation of “foot pain” and to establishprimary care. Around the age of 4 JL first developedthe formation of thick plantar calluses, along withplantar pain, which she recalls prevented her fromplaying tag and jump-rope at recess as a child. Atthe age of 6 JL first noticed thickening of hertoenails, which was refractive to anti-fungaltherapy prescribed by her pediatrician. As theplantar pain persisted into her teenage years, shewas referred to a podiatrist who told her the footpain was due to “growing”, and fitted her fororthotic inserts for her shoes.
The plantar pain is so intense that JL often crawlsaround her home to avoid standing on her feet. Shedescribes this pain as aching. However, she alsooccasionally feels a burning sensation in her feetwhile she is seated with her feet flat on the ground.JL works at a call center and was promoted to teamleader 3 weeks ago, which requires her to be onher feet more often than she is used to. Since thenthe pain has been almost unbearable and she isconsidering asking to be moved back to herprevious job, where she could sit in a cubicle duringthe day and did not have to walk around as much.She has been taking 800mg ibuprofen almost everyday for the past 2 weeks, which only provides mildpain relief. She denies thick fingernails, oralleukokeratosis, hoarseness, hyperhidrosis, follicularhyperkeratosis, cysts, and the presence of natalteeth.
HISTORY OF PRESENT ILLNESS
DIFFERENTIAL DIAGNOSIS
In patients presenting with thetriad of plantar pain, plantarkeratoderma, and toenail dystrophy, genetic testing forPC is recommended as these arethe three most common symptomsin PC across all mutation types.
Fingernail dystrophy is notalways present in PC, but mostmedical texts erroneously list twenty-nail dystrophy asa diagnostic feature of PC.
Plantar pain is a complex symptom of PC that canseverely impact quality of life. The pain reported by PCpatients tends to be out of proportion to theappearance and extent of the plantar keratoderma andmust be managed appropriately. Many patients requirechronic pain medication and/or the use of durablemedical equipment such as a wheelchair.
IV. DiscussionPachyonychia congenita (PC) is a rare inherited skindisease caused by a mutation in one of five keratingenes. The phenotypic presentation variesdepending on the specific keratin gene affected,thus, the nomenclature of the disease has recentlybeen re-classified based on the gene involved.
Patients with PC are often misdiagnosed or fail toreceive a diagnosis for many years, with mostpatients being diagnosed in adulthood. Because theplantar pain associated with this disease canseverely impair functionality in daily activities,making the correct diagnosis is important.
Misdiagnosis of PC can lead to unnecessarytreatments, lack of access to durable medicalequipment, and inappropriate pain management.
I. Introduction
Historical ClassificationType I “Jadassohn–Lewandowsky syndrome”Type II "Jackson–Lawler syndrome "
New ClassificationPC-K6aPC-K6bPC-K6cPC-K16PC-K17
Table 1. A new classification scheme was accepted in 2012 based on analysis of genomic data in 254 patients with PC
Figure 2. a) Plantar keratoderma in a pressure distribution bilaterally. b) Toenail dystrophy.
Plantar Pain
Figure 3. The presence of these 3 symptoms indicates a high likelihood that PC is present.
82.9% of allPC patients
.
...
..
..
PAST MEDICAL HISTORY
PAST SURGICAL HISTORY
MEDICATIONS & ALLERGIES
SOCIAL HISTORY
FAMILY HISTORY
REVIEW OF SYSTEMS
PHYSICAL EXAM
DIFFERENTIAL DIAGNOSIS
- Broken wrist at age 6 after jumping off of a swing, no complications
- Persistent plantar pain and calluses since age 4- No other medical history
- 800mg Ibuprofen daily for the past 2 weeks for foot pain- 200mg Acetaminophen for foot pain PRN, says ibuprofen
works better- 180mg Fexofenadine for hay fever as needed in the spring
- Has never had surgery
- Works at a call center, enjoys her work when she doesn’t have to be on her feet, considers coworkers to be friends
- Never tried illicit drugs, drinks 1-2 glasses of wine per week- Denies depression, feels socially isolated due to foot pain
- Mother 62yo, alive. Hay fever in spring, otherwise healthy- Father 63yo, alive. Diagnosed with Type 2 DM at age 61yo- Brother 34yo, alive, healthy - Family members lack plantar callus/pain, toenail dystrophy
- Negative for dyspnea, palpitations
Skin:- Yellow plantar calluses in a pressure distribution. Toenails of digits 1-5 show increased curvature with subungual thickening & dystrophy of nail plate. No plantar or web space scale.- No palmar keratoderma or callus. Fingernails normal.Musculoskeletal:- Both feet are tender to palpation across the plantar surfaces- Range of motion, strength, reflexes, & sensation normal
Pachyonychia congenita, palmoplantar keratoderma, Clouston syndrome, Olmsted syndrome, Carvajal syndrome, 20-nail dystrophy, psoriasis, lichen planus, onychomycosis
Figure 1. a) Symptoms of PC. b) Symptoms previously believed to be associated with PC.
..
.
SYMPTOMS NOT PART OF PC:
Alopecia
Deafness
Diabetes
Mental retardation
Bone deformities
Cataracts
Menstrual irregularities
Tooth loss
Oral leukokeratosisHoarsenessNatal teeth
Follicular HyperkeratosisCysts
Palmar keratodermaFingernail dystrophy
Plantar painPlantar keratodermaToenail dystrophy
COMMON SYMPTOMSOF PC:
a) b)
. .
.
a) b)
David Gaston, M.D. Ph.D.1, Jessica Donigan, M.D.2, and Robert Odrobina M.D.3Departments of 1Internal Medicine, 2Dermatology, and 3Infectious Diseases; The University of Utah, Salt Lake City, UT
Presentation
References
Discussion
Patient HistoryMedical, Family, and Social History: - 60+ year old woman; acute myeloid leukemia (AML) and hypothyroidism- Mother with lymphoma; married with children, no occupational exposures
2006: 23% MB
2007: 7+3, 22% MB D14HiDAC x4 cycles
2011: 35% MB
2011: Vidaza x14 cycles
2012: 9/10 MUD allo HSCT
2016: 3% MB; Tetraploid, 8q22
(RUNX1T1)
2013: GvHD, GI 2016:DAH x3
Abbreviations: 7+3- cytarabine and idarubicin; D14- day 14;DAH- diffuse alveolar hemorrhage; GvHD- graft versus hostdisease; GI- gastointestinal; HiDAC- high dose cytarabine;LFTs- liver function tests; MB- myeloblast; MUD allo HSCT-mixed unrelated donor allo-hematopoietic stem cell transplant
2016: DAH admission one month prior to presented admission with:- Etanercept x4 doses- Prednisone 100mg BID at discharge; tapered to 60mg BID on readmission- Voriconazole transitioned to Posaconazole due to elevated LFTs
AML History and Complications
- Moon facies; No murmur; Diffuse bilateral crackles- RUE and RLE weakness, positive R pronator drift, decreased sensation to light touch and vibration on R- Oriented x2, somnolent, perseverating about “space ships”
Initial Evaluation- One day of confusion (on “space ship”) and right arm/leg weakness - Vital signs: T 38.7, HR 91, BP 128/66, RR 18, SpO2 88% (room air)- ROS obscured by encephalopathy- Posaconazole level: 0.9 ug/mL (2.9 ug/mL two weeks prior)- WBC 2.17 k/uL (ANC 700), Hgb 8.6 mg/dL, Platelet 18 k/uL
- ALT 103, all other labs grossly within normal limits- Exam:
Notable admission medications: Acyclovir 800mg BIDBactrim DS M/W/F Penicillin V 500 QD
Posaconazole 300mg QD Prednisone 60 BID
A B C
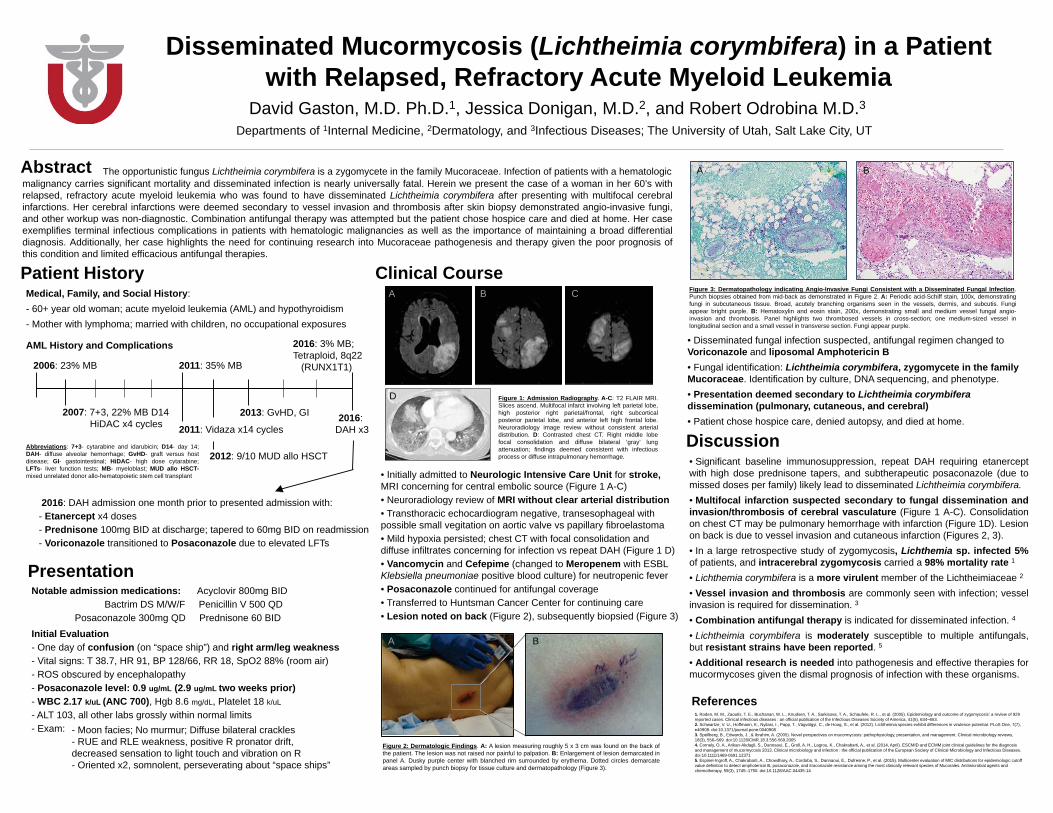
D Figure 1: Admission Radiography. A-C: T2 FLAIR MRI.Slices ascend. Multifocal infarct involving left parietal lobe,high posterior right parietal/frontal, right subcorticalposterior parietal lobe, and anterior left high frontal lobe.Neuroradiology image review without consistent arterialdistribution. D: Contrasted chest CT. Right middle lobefocal consolidation and diffuse bilateral ‘gray’ lungattenuation; findings deemed consistent with infectiousprocess or diffuse intrapulmonary hemorrhage.
Clinical Course
A B
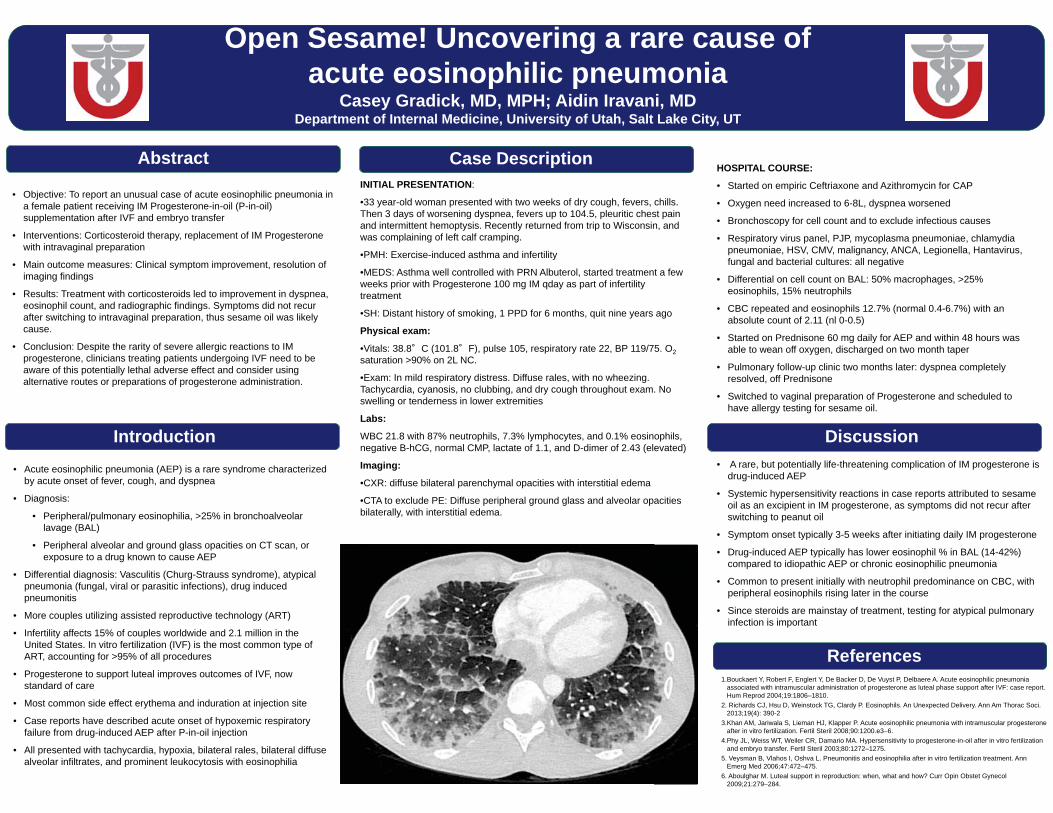
Figure 2: Dermatologic Findings. A: A lesion measuring roughly 5 x 3 cm was found on the back ofthe patient. The lesion was not raised nor painful to palpation. B: Enlargement of lesion demarcated inpanel A. Dusky purple center with blanched rim surrounded by erythema. Dotted circles demarcateareas sampled by punch biopsy for tissue culture and dermatopathology (Figure 3).
A B
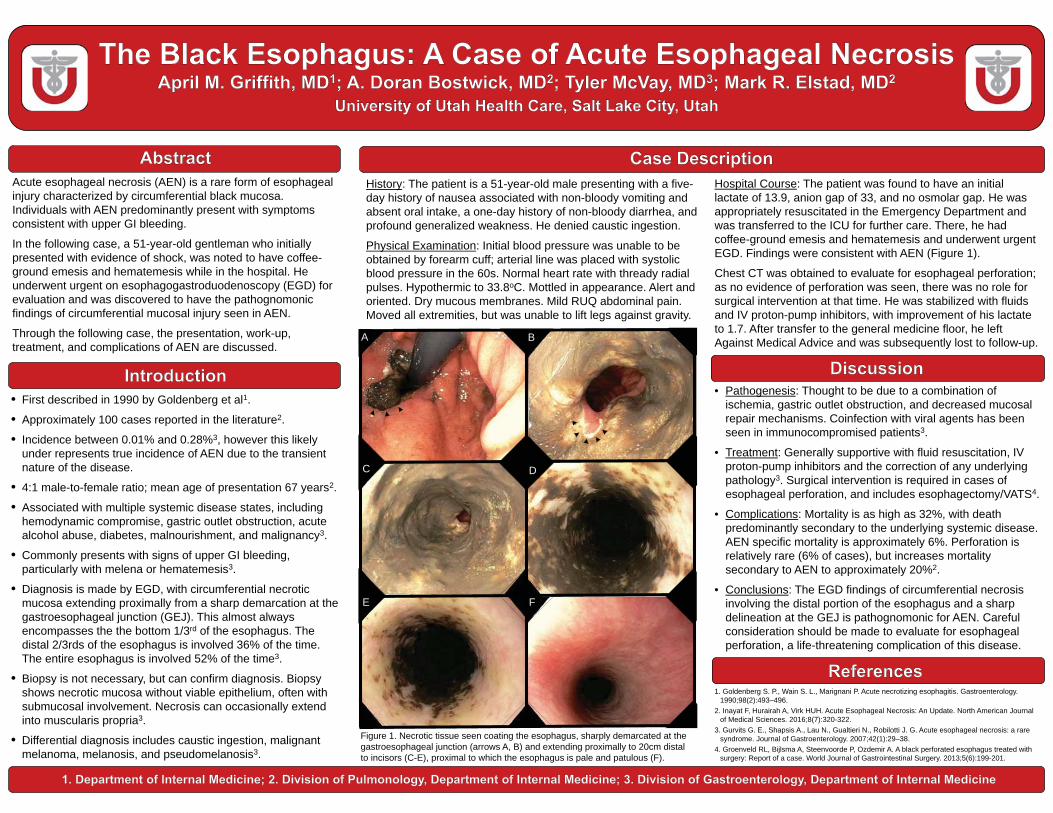
Figure 3: Dermatopathology indicating Angio-Invasive Fungi Consistent with a Disseminated Fungal Infection.Punch biopsies obtained from mid-back as demonstrated in Figure 2. A: Periodic acid-Schiff stain, 100x, demonstratingfungi in subcutaneous tissue. Broad, acutely branching organisms seen in the vessels, dermis, and subcutis. Fungiappear bright purple. B: Hematoxylin and eosin stain, 200x, demonstrating small and medium vessel fungal angio-invasion and thrombosis. Panel highlights two thrombosed vessels in cross-section; one medium-sized vessel inlongitudinal section and a small vessel in transverse section. Fungi appear purple.
• Disseminated fungal infection suspected, antifungal regimen changed to Voriconazole and liposomal Amphotericin B• Fungal identification: Lichtheimia corymbifera, zygomycete in the family Mucoraceae. Identification by culture, DNA sequencing, and phenotype.• Presentation deemed secondary to Lichtheimia corymbiferadissemination (pulmonary, cutaneous, and cerebral)• Patient chose hospice care, denied autopsy, and died at home.
Disseminated Mucormycosis (Lichtheimia corymbifera) in a Patient with Relapsed, Refractory Acute Myeloid Leukemia
• Initially admitted to Neurologic Intensive Care Unit for stroke, MRI concerning for central embolic source (Figure 1 A-C)• Neuroradiology review of MRI without clear arterial distribution• Transthoracic echocardiogram negative, transesophageal with possible small vegitation on aortic valve vs papillary fibroelastoma• Mild hypoxia persisted; chest CT with focal consolidation and diffuse infiltrates concerning for infection vs repeat DAH (Figure 1 D)• Vancomycin and Cefepime (changed to Meropenem with ESBLKlebsiella pneumoniae positive blood culture) for neutropenic fever• Posaconazole continued for antifungal coverage• Transferred to Huntsman Cancer Center for continuing care• Lesion noted on back (Figure 2), subsequently biopsied (Figure 3)
• Significant baseline immunosuppression, repeat DAH requiring etanerceptwith high dose prednisone tapers, and subtherapeutic posaconazole (due tomissed doses per family) likely lead to disseminated Lichtheimia corymbifera.• Multifocal infarction suspected secondary to fungal dissemination andinvasion/thrombosis of cerebral vasculature (Figure 1 A-C). Consolidationon chest CT may be pulmonary hemorrhage with infarction (Figure 1D). Lesionon back is due to vessel invasion and cutaneous infarction (Figures 2, 3).• In a large retrospective study of zygomycosis, Lichthemia sp. infected 5%of patients, and intracerebral zygomycosis carried a 98% mortality rate 1
• Lichthemia corymbifera is a more virulent member of the Lichtheimiaceae 2
• Vessel invasion and thrombosis are commonly seen with infection; vesselinvasion is required for dissemination. 3
• Combination antifungal therapy is indicated for disseminated infection. 4
• Lichtheimia corymbifera is moderately susceptible to multiple antifungals,but resistant strains have been reported. 5
• Additional research is needed into pathogenesis and effective therapies formucormycoses given the dismal prognosis of infection with these organisms.
1. Roden, M. M., Zaoutis, T. E., Buchanan, W. L., Knudsen, T. A., Sarkisova, T. A., Schaufele, R. L., et al. (2005). Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 41(5), 634–653.2. Schwartze, V. U., Hoffmann, K., Nyilasi, I., Papp, T., Vágvölgyi, C., de Hoog, S., et al. (2012). Lichtheimia species exhibit differences in virulence potential. PLoS One, 7(7), e40908. doi:10.1371/journal.pone.00409083. Spellberg, B., Edwards, J., & Ibrahim, A. (2005). Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clinical microbiology reviews, 18(3), 556–569. doi:10.1128/CMR.18.3.556-569.20054. Cornely, O. A., Arikan-Akdagli, S., Dannaoui, E., Groll, A. H., Lagrou, K., Chakrabarti, A., et al. (2014, April). ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. doi:10.1111/1469-0691.123715. Espinel-Ingroff, A., Chakrabarti, A., Chowdhary, A., Cordoba, S., Dannaoui, E., Dufresne, P., et al. (2015). Multicenter evaluation of MIC distributions for epidemiologic cutoff value definition to detect amphotericin B, posaconazole, and itraconazole resistance among the most clinically relevant species of Mucorales. Antimicrobial agents and chemotherapy, 59(3), 1745–1750. doi:10.1128/AAC.04435-14
Abstractmalignancy carries significant mortality and disseminated infection is nearly universally fatal. Herein we present the case of a woman in her 60’s withrelapsed, refractory acute myeloid leukemia who was found to have disseminated Lichtheimia corymbifera after presenting with multifocal cerebralinfarctions. Her cerebral infarctions were deemed secondary to vessel invasion and thrombosis after skin biopsy demonstrated angio-invasive fungi,and other workup was non-diagnostic. Combination antifungal therapy was attempted but the patient chose hospice care and died at home. Her caseexemplifies terminal infectious complications in patients with hematologic malignancies as well as the importance of maintaining a broad differentialdiagnosis. Additionally, her case highlights the need for continuing research into Mucoraceae pathogenesis and therapy given the poor prognosis ofthis condition and limited efficacious antifungal therapies.
The opportunistic fungus Lichtheimia corymbifera is a zygomycete in the family Mucoraceae. Infection of patients with a hematologic
Open Sesame! Uncovering a rare cause ofacute eosinophilic pneumonia
Casey Gradick, MD, MPH; Aidin Iravani, MDDepartment of Internal Medicine, University of Utah, Salt Lake City, UT
Case Description
Introduction
Objectives
Discussion
References1.Bouckaert Y, Robert F, Englert Y, De Backer D, De Vuyst P, Delbaere A. Acute eosinophilic pneumonia
associated with intramuscular administration of progesterone as luteal phase support after IVF: case report. Hum Reprod 2004;19:1806–1810.
2. Richards CJ, Hsu D, Weinstock TG, Clardy P. Eosinophils. An Unexpected Delivery. Ann Am Thorac Soci. 2013;19(4): 390-2
3.Khan AM, Jariwala S, Lieman HJ, Klapper P. Acute eosinophilic pneumonia with intramuscular progesterone after in vitro fertilization. Fertil Steril 2008;90:1200.e3–6.
4.Phy JL, Weiss WT, Weiler CR, Damario MA. Hypersensitivity to progesterone-in-oil after in vitro fertilization and embryo transfer. Fertil Steril 2003;80:1272–1275.
5. Veysman B, Vlahos I, Oshva L. Pneumonitis and eosinophilia after in vitro fertilization treatment. Ann Emerg Med 2006;47:472–475.
6. Aboulghar M. Luteal support in reproduction: when, what and how? Curr Opin Obstet Gynecol 2009;21:279–284.
• Objective: To report an unusual case of acute eosinophilic pneumonia in a female patient receiving IM Progesterone-in-oil (P-in-oil) supplementation after IVF and embryo transfer
• Interventions: Corticosteroid therapy, replacement of IM Progesterone with intravaginal preparation
• Main outcome measures: Clinical symptom improvement, resolution of imaging findings
• Results: Treatment with corticosteroids led to improvement in dyspnea, eosinophil count, and radiographic findings. Symptoms did not recur after switching to intravaginal preparation, thus sesame oil was likely cause.
• Conclusion: Despite the rarity of severe allergic reactions to IM progesterone, clinicians treating patients undergoing IVF need to be aware of this potentially lethal adverse effect and consider using alternative routes or preparations of progesterone administration.
HOSPITAL COURSE:
• Started on empiric Ceftriaxone and Azithromycin for CAP
• Oxygen need increased to 6-8L, dyspnea worsened
• Bronchoscopy for cell count and to exclude infectious causes
• Respiratory virus panel, PJP, mycoplasma pneumoniae, chlamydia pneumoniae, HSV, CMV, malignancy, ANCA, Legionella, Hantavirus, fungal and bacterial cultures: all negative
• Differential on cell count on BAL: 50% macrophages, >25%eosinophils, 15% neutrophils
• CBC repeated and eosinophils 12.7% (normal 0.4-6.7%) with an absolute count of 2.11 (nl 0-0.5)
• Started on Prednisone 60 mg daily for AEP and within 48 hours was able to wean off oxygen, discharged on two month taper
• Pulmonary follow-up clinic two months later: dyspnea completely resolved, off Prednisone
• Switched to vaginal preparation of Progesterone and scheduled to have allergy testing for sesame oil.
• A rare, but potentially life-threatening complication of IM progesterone isdrug-induced AEP
• Systemic hypersensitivity reactions in case reports attributed to sesame oil as an excipient in IM progesterone, as symptoms did not recur after switching to peanut oil
• Symptom onset typically 3-5 weeks after initiating daily IM progesterone
• Drug-induced AEP typically has lower eosinophil % in BAL (14-42%) compared to idiopathic AEP or chronic eosinophilic pneumonia
• Common to present initially with neutrophil predominance on CBC, with peripheral eosinophils rising later in the course
• Since steroids are mainstay of treatment, testing for atypical pulmonary infection is important
INITIAL PRESENTATION:
•33 year-old woman presented with two weeks of dry cough, fevers, chills. Then 3 days of worsening dyspnea, fevers up to 104.5, pleuritic chest pain and intermittent hemoptysis. Recently returned from trip to Wisconsin, and was complaining of left calf cramping.
•PMH: Exercise-induced asthma and infertility
•MEDS: Asthma well controlled with PRN Albuterol, started treatment a few weeks prior with Progesterone 100 mg IM qday as part of infertility treatment
•SH: Distant history of smoking, 1 PPD for 6 months, quit nine years ago
Physical exam:
•Vitals: 38.8 C (101.8 F), pulse 105, respiratory rate 22, BP 119/75. O2saturation >90% on 2L NC.
•Exam: In mild respiratory distress. Diffuse rales, with no wheezing. Tachycardia, cyanosis, no clubbing, and dry cough throughout exam. No swelling or tenderness in lower extremities
Labs:
WBC 21.8 with 87% neutrophils, 7.3% lymphocytes, and 0.1% eosinophils, negative B-hCG, normal CMP, lactate of 1.1, and D-dimer of 2.43 (elevated)
Imaging:
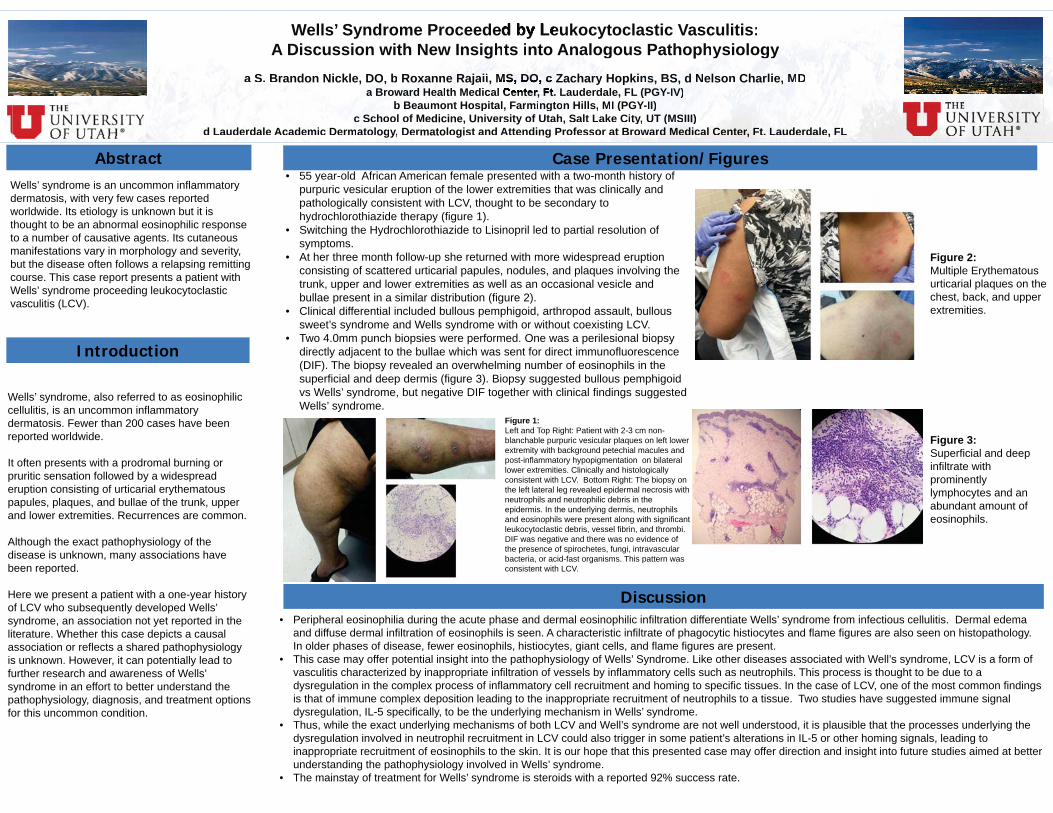
•CXR: diffuse bilateral parenchymal opacities with interstitial edema
•CTA to exclude PE: Diffuse peripheral ground glass and alveolar opacities bilaterally, with interstitial edema.
Abstract
• Acute eosinophilic pneumonia (AEP) is a rare syndrome characterized by acute onset of fever, cough, and dyspnea
• Diagnosis:
• Peripheral/pulmonary eosinophilia, >25% in bronchoalveolar lavage (BAL)
• Peripheral alveolar and ground glass opacities on CT scan, or exposure to a drug known to cause AEP
• Differential diagnosis: Vasculitis (Churg-Strauss syndrome), atypical pneumonia (fungal, viral or parasitic infections), drug induced pneumonitis
• More couples utilizing assisted reproductive technology (ART)
• Infertility affects 15% of couples worldwide and 2.1 million in the United States. In vitro fertilization (IVF) is the most common type of ART, accounting for >95% of all procedures
• Progesterone to support luteal improves outcomes of IVF, now standard of care
• Most common side effect erythema and induration at injection site
• Case reports have described acute onset of hypoxemic respiratory failure from drug-induced AEP after P-in-oil injection
• All presented with tachycardia, hypoxia, bilateral rales, bilateral diffuse alveolar infiltrates, and prominent leukocytosis with eosinophilia
D
A B
C D
E F
Objectives
1. Goldenberg S. P., Wain S. L., Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990;98(2):493–496.
2. Inayat F, Hurairah A, Virk HUH. Acute Esophageal Necrosis: An Update. North American Journal of Medical Sciences. 2016;8(7):320-322.
3. Gurvits G. E., Shapsis A., Lau N., Gualtieri N., Robilotti J. G. Acute esophageal necrosis: a rare syndrome. Journal of Gastroenterology. 2007;42(1):29–38.
4. Groenveld RL, Bijlsma A, Steenvoorde P, Ozdemir A. A black perforated esophagus treated with surgery: Report of a case. World Journal of Gastrointestinal Surgery. 2013;5(6):199-201.
Acute esophageal necrosis (AEN) is a rare form of esophageal injury characterized by circumferential black mucosa. Individuals with AEN predominantly present with symptoms consistent with upper GI bleeding.
In the following case, a 51-year-old gentleman who initially presented with evidence of shock, was noted to have coffee-ground emesis and hematemesis while in the hospital. He underwent urgent on esophagogastroduodenoscopy (EGD) for evaluation and was discovered to have the pathognomonic findings of circumferential mucosal injury seen in AEN.
Through the following case, the presentation, work-up,treatment, and complications of AEN are discussed.
• Pathogenesis: Thought to be due to a combination of ischemia, gastric outlet obstruction, and decreased mucosal repair mechanisms. Coinfection with viral agents has been seen in immunocompromised patients3.
• Treatment: Generally supportive with fluid resuscitation, IV proton-pump inhibitors and the correction of any underlying pathology3. Surgical intervention is required in cases of esophageal perforation, and includes esophagectomy/VATS4.
• Complications: Mortality is as high as 32%, with death predominantly secondary to the underlying systemic disease.AEN specific mortality is approximately 6%. Perforation is relatively rare (6% of cases), but increases mortality secondary to AEN to approximately 20%2.
• Conclusions: The EGD findings of circumferential necrosis involving the distal portion of the esophagus and a sharp delineation at the GEJ is pathognomonic for AEN. Careful consideration should be made to evaluate for esophageal perforation, a life-threatening complication of this disease.
• First described in 1990 by Goldenberg et al1.
• Approximately 100 cases reported in the literature2.
• Incidence between 0.01% and 0.28%3, however this likely under represents true incidence of AEN due to the transient nature of the disease.
• 4:1 male-to-female ratio; mean age of presentation 67 years2.
• Associated with multiple systemic disease states, including hemodynamic compromise, gastric outlet obstruction, acute alcohol abuse, diabetes, malnourishment, and malignancy3.
• Commonly presents with signs of upper GI bleeding, particularly with melena or hematemesis3.
• Diagnosis is made by EGD, with circumferential necrotic mucosa extending proximally from a sharp demarcation at the gastroesophageal junction (GEJ). This almost always encompasses the the bottom 1/3rd of the esophagus. The distal 2/3rds of the esophagus is involved 36% of the time. The entire esophagus is involved 52% of the time3.
• Biopsy is not necessary, but can confirm diagnosis. Biopsy shows necrotic mucosa without viable epithelium, often with submucosal involvement. Necrosis can occasionally extend into muscularis propria3.
• Differential diagnosis includes caustic ingestion, malignant melanoma, melanosis, and pseudomelanosis3.
History: The patient is a 51-year-old male presenting with a five-day history of nausea associated with non-bloody vomiting and absent oral intake, a one-day history of non-bloody diarrhea, and profound generalized weakness. He denied caustic ingestion.
Physical Examination: Initial blood pressure was unable to be obtained by forearm cuff; arterial line was placed with systolic blood pressure in the 60s. Normal heart rate with thready radial pulses. Hypothermic to 33.8oC. Mottled in appearance. Alert and oriented. Dry mucous membranes. Mild RUQ abdominal pain. Moved all extremities, but was unable to lift legs against gravity.
Hospital Course: The patient was found to have an initial lactate of 13.9, anion gap of 33, and no osmolar gap. He was appropriately resuscitated in the Emergency Department and was transferred to the ICU for further care. There, he had coffee-ground emesis and hematemesis and underwent urgent EGD. Findings were consistent with AEN (Figure 1).
Chest CT was obtained to evaluate for esophageal perforation; as no evidence of perforation was seen, there was no role for surgical intervention at that time. He was stabilized with fluids and IV proton-pump inhibitors, with improvement of his lactate to 1.7. After transfer to the general medicine floor, he left Against Medical Advice and was subsequently lost to follow-up.
Figure 1. Necrotic tissue seen coating the esophagus, sharply demarcated at the gastroesophageal junction (arrows A, B) and extending proximally to 20cm distal to incisors (C-E), proximal to which the esophagus is pale and patulous (F).
City, Utah
Introduction
Wells’ syndrome is an uncommon inflammatory dermatosis, with very few cases reported worldwide. Its etiology is unknown but it is thought to be an abnormal eosinophilic response to a number of causative agents. Its cutaneous manifestations vary in morphology and severity, but the disease often follows a relapsing remitting course. This case report presents a patient with Wells’ syndrome proceeding leukocytoclasticvasculitis (LCV).
Wells’ syndrome, also referred to as eosinophilic cellulitis, is an uncommon inflammatory dermatosis. Fewer than 200 cases have been reported worldwide.
It often presents with a prodromal burning or pruritic sensation followed by a widespread eruption consisting of urticarial erythematous papules, plaques, and bullae of the trunk, upper and lower extremities. Recurrences are common.
Although the exact pathophysiology of the disease is unknown, many associations have been reported.
Here we present a patient with a one-year history of LCV who subsequently developed Wells’ syndrome, an association not yet reported in the literature. Whether this case depicts a causal association or reflects a shared pathophysiology is unknown. However, it can potentially lead to further research and awareness of Wells’ syndrome in an effort to better understand the pathophysiology, diagnosis, and treatment options for this uncommon condition.
• Peripheral eosinophilia during the acute phase and dermal eosinophilic infiltration differentiate Wells’ syndrome from infectious cellulitis. Dermal edema and diffuse dermal infiltration of eosinophils is seen. A characteristic infiltrate of phagocytic histiocytes and flame figures are also seen on histopathology. In older phases of disease, fewer eosinophils, histiocytes, giant cells, and flame figures are present.
• This case may offer potential insight into the pathophysiology of Wells’ Syndrome. Like other diseases associated with Well’s syndrome, LCV is a form of vasculitis characterized by inappropriate infiltration of vessels by inflammatory cells such as neutrophils. This process is thought to be due to a dysregulation in the complex process of inflammatory cell recruitment and homing to specific tissues. In the case of LCV, one of the most common findings is that of immune complex deposition leading to the inappropriate recruitment of neutrophils to a tissue. Two studies have suggested immune signal dysregulation, IL-5 specifically, to be the underlying mechanism in Wells’ syndrome.
• Thus, while the exact underlying mechanisms of both LCV and Well’s syndrome are not well understood, it is plausible that the processes underlying the dysregulation involved in neutrophil recruitment in LCV could also trigger in some patient’s alterations in IL-5 or other homing signals, leading to inappropriate recruitment of eosinophils to the skin. It is our hope that this presented case may offer direction and insight into future studies aimed at better understanding the pathophysiology involved in Wells’ syndrome.
• The mainstay of treatment for Wells’ syndrome is steroids with a reported 92% success rate.
Abstract Case Presentation/Figures
Discussion
Figure 1: Left and Top Right: Patient with 2-3 cm non-blanchable purpuric vesicular plaques on left lower extremity with background petechial macules and post-inflammatory hypopigmentation on bilateral lower extremities. Clinically and histologically consistent with LCV. Bottom Right: The biopsy on the left lateral leg revealed epidermal necrosis with neutrophils and neutrophilic debris in the epidermis. In the underlying dermis, neutrophils and eosinophils were present along with significant leukocytoclastic debris, vessel fibrin, and thrombi. DIF was negative and there was no evidence of the presence of spirochetes, fungi, intravascular bacteria, or acid-fast organisms. This pattern was consistent with LCV.
Figure 2: Multiple Erythematous urticarial plaques on the chest, back, and upper extremities.
City, UtahWells’ Syndrome Proceeded by Leukocytoclastic Vasculitis:A Discussion with New Insights into Analogous Pathophysiology
a S. Brandon Nickle, DO, b Roxanne Rajaii, MS, DO, c Zachary Hopkins, BS, d Nelson Charlie, MDa Broward Health Medical Center, Ft. Lauderdale, FL (PGY-IV)
b Beaumont Hospital, Farmington Hills, MI (PGY-II)c School of Medicine, University of Utah, Salt Lake City, UT (MSIII)
d Lauderdale Academic Dermatology, Dermatologist and Attending Professor at Broward Medical Center, Ft. Lauderdale, FL
Ciityt , UtUtahah
Cit Ut hWells’ Syndrome Proceeded byyyyy Leukocytoclastic Vasculitis:City, UtahCi y, UtU ah
A Discussion with New IInnsssiiiggggggghhhttttsssss iiiiiiinnnntttooo AAAAAAAAnnnnnnnaaaaalogous Pathophhhhyyyyyssssssssiiiiooollloooooggggggyyyyyyyyyy a aaaa S.S.S.SSS BBBBrararr ndndnddonoo Nickle, DODOOD , , , bbbbbb RoRooxaxaxaxaxannnnnneeeeee RaRaRaRaRaRaRajajajajajjaajaiiiiiiiiiii , , , , MSMSMSSMSSMSSM DODODODODODODO cccccccc ZaZZZaZaZaZZZachchchhccc arararrrryy yy HoooHoooH pkpkpppkkkkkkp inninininnni s,s,s,sss,, BBBBBBBS,SS,S,S,S,S,, ddddddd NNNNNNNNelelele ssososososooonnnnnn ChChCChhhChaarararararlilililillie,e,e,ee,, MMMMMMMDDDCiityty UtUtahaCCiCityttyy UUtUUttUtahahahhhaa aa BrBBBBrBrowowowowwwwwaaararaaaa d d dddd HeHeHeealalalalththhhhth MMMMedede icicicicci alalalall CCCCCCenennene tetetetetttter,r,r,r,r,r, FFFFFFFtt.t.t.t.tt LLLLauauauauaua dedededderdrdrrrdrdalaala e,e,e,ee, FFFFFL L L L (P(PP(P(P(PPP( GGGYGYGYGYGCity, UtUtahhCCiCi yyyyyy,,, ahahahahh --YYYYY IVIVIVIVVV)))))
b b bb BeBeBBeBeBeeB auauaumommontntt HHHHospitataaal,l,l, FFFFararararmimimiimmmimiimmm ngngngngngnggggtototoonnn HiHiHiHHHH lllllls,ss,s, MMMMI III (PPP(PPPGYGYGYGY--YYYY IIIIIIIIII))))))c c cc c c SScScSScchohohohoooolol ooof f MMedicine, Univvvvverererere sissitytyy ooof ff UtUtUtUtUttahahahahh,,,, SaSaSSaSaS ltlttt LLLakakakkkee e CiCityyty,,, UTUUTTTT ((((((MSMSMSMSMSSMSIIIIIIIIIIII)I)I)))
d d d d LaLaLaLaL uduudududererererererdadadadad lelelele AAAAcacaacadededeemimimimiiccccc DeDeDeDermmmatatatatttoolololologogogy,y,y, DDDeere matoloogi tst aaandndnddd AAtttttttteneene didingngngngn PPPPProrororoorofefefefesssssssororor aaaatt t t BrBrBrBrB owowowowararararrdddd d MMeMediiidicaaacacacacaall CeCentnterer, FtFtttt. . LaLaLaLaaL udududududerereererdadadadaalelelel , , FLFFLFLL
• 55 year-old African American female presented with a two-month history of purpuric vesicular eruption of the lower extremities that was clinically and pathologically consistent with LCV, thought to be secondary to hydrochlorothiazide therapy (figure 1).
• Switching the Hydrochlorothiazide to Lisinopril led to partial resolution of symptoms.
• At her three month follow-up she returned with more widespread eruption consisting of scattered urticarial papules, nodules, and plaques involving the trunk, upper and lower extremities as well as an occasional vesicle and bullae present in a similar distribution (figure 2).
• Clinical differential included bullous pemphigoid, arthropod assault, bullous sweet’s syndrome and Wells syndrome with or without coexisting LCV.
• Two 4.0mm punch biopsies were performed. One was a perilesional biopsy directly adjacent to the bullae which was sent for direct immunofluorescence (DIF). The biopsy revealed an overwhelming number of eosinophils in the superficial and deep dermis (figure 3). Biopsy suggested bullous pemphigoid vs Wells’ syndrome, but negative DIF together with clinical findings suggested Wells’ syndrome.
Figure 3: Superficial and deep infiltrate with prominently lymphocytes and an abundant amount of eosinophils.
The Differential Diagnosis of a Neck Mass: Infectious, Inflammatory, or Both?John H. Murray, MD
Dept. of Internal Medicine, University of Utah, Salt Lake City, UT
History of Present Illness
Results
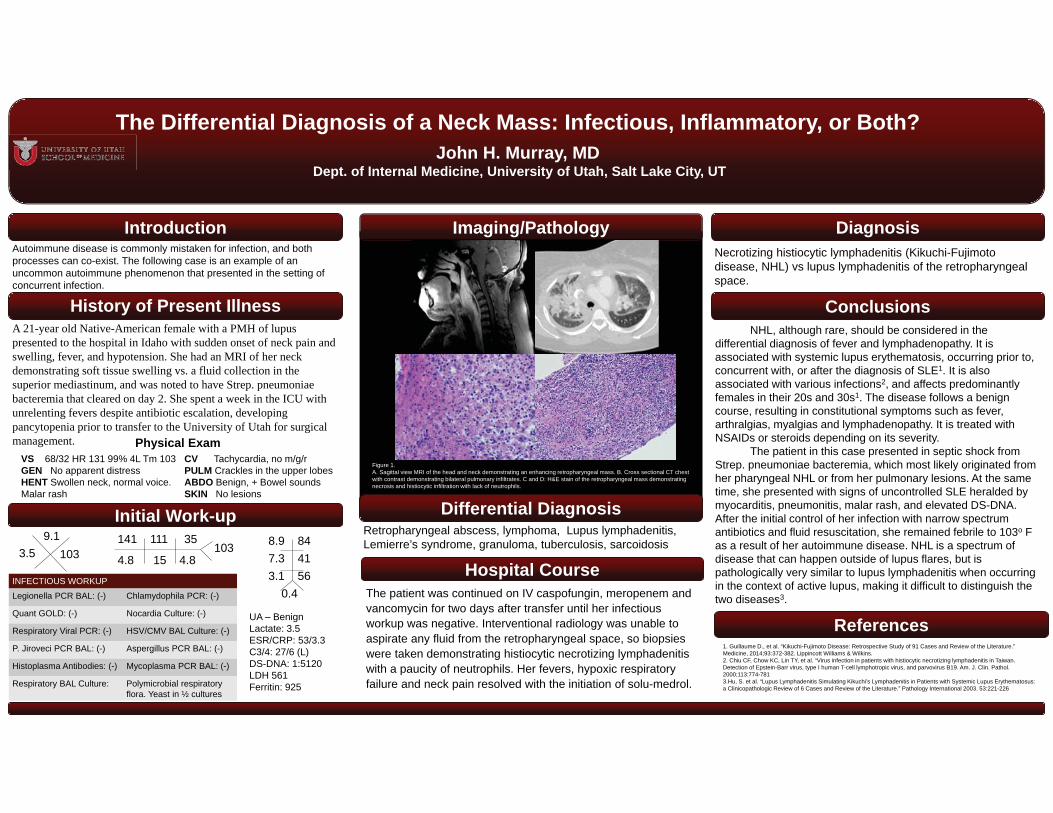
A 21-year old Native-American female with a PMH of lupus presented to the hospital in Idaho with sudden onset of neck pain and swelling, fever, and hypotension. She had an MRI of her neck demonstrating soft tissue swelling vs. a fluid collection in the superior mediastinum, and was noted to have Strep. pneumoniaebacteremia that cleared on day 2. She spent a week in the ICU with unrelenting fevers despite antibiotic escalation, developing pancytopenia prior to transfer to the University of Utah for surgical management.
Necrotizing histiocytic lymphadenitis (Kikuchi-Fujimoto disease, NHL) vs lupus lymphadenitis of the retropharyngeal space.
Diagnosis
Conclusions
References
Imaging/Pathology
Retropharyngeal abscess, lymphoma, Lupus lymphadenitis, Lemierre’s syndrome, granuloma, tuberculosis, sarcoidosis
Initial Work-up
1033.59.1 141 111 35
4.8 15 4.8103
UA – BenignLactate: 3.5ESR/CRP: 53/3.3C3/4: 27/6 (L)DS-DNA: 1:5120LDH 561Ferritin: 925
Hospital Course
VS 68/32 HR 131 99% 4L Tm 103GEN No apparent distressHENT Swollen neck, normal voice. Malar rash
CV Tachycardia, no m/g/rPULM Crackles in the upper lobesABDO Benign, + Bowel soundsSKIN No lesions
Physical Exam
INFECTIOUS WORKUP
Legionella PCR BAL: (-) Chlamydophila PCR: (-)
Quant GOLD: (-) Nocardia Culture: (-)
Respiratory Viral PCR: (-) HSV/CMV BAL Culture: (-)
P. Jiroveci PCR BAL: (-) Aspergillus PCR BAL: (-)
Histoplasma Antibodies: (-) Mycoplasma PCR BAL: (-)
Respiratory BAL Culture: Polymicrobial respiratory flora. Yeast in ½ cultures
8.9 847.3 413.1 56
0.4
Differential Diagnosis
The patient was continued on IV caspofungin, meropenem and vancomycin for two days after transfer until her infectious workup was negative. Interventional radiology was unable to aspirate any fluid from the retropharyngeal space, so biopsies were taken demonstrating histiocytic necrotizing lymphadenitis with a paucity of neutrophils. Her fevers, hypoxic respiratory failure and neck pain resolved with the initiation of solu-medrol.
IntroductionAutoimmune disease is commonly mistaken for infection, and both processes can co-exist. The following case is an example of an uncommon autoimmune phenomenon that presented in the setting of concurrent infection.
NHL, although rare, should be considered in the differential diagnosis of fever and lymphadenopathy. It is associated with systemic lupus erythematosis, occurring prior to, concurrent with, or after the diagnosis of SLE1. It is also associated with various infections2, and affects predominantly females in their 20s and 30s1. The disease follows a benign course, resulting in constitutional symptoms such as fever, arthralgias, myalgias and lymphadenopathy. It is treated with NSAIDs or steroids depending on its severity.
The patient in this case presented in septic shock from Strep. pneumoniae bacteremia, which most likely originated from her pharyngeal NHL or from her pulmonary lesions. At the same time, she presented with signs of uncontrolled SLE heralded by myocarditis, pneumonitis, malar rash, and elevated DS-DNA. After the initial control of her infection with narrow spectrum antibiotics and fluid resuscitation, she remained febrile to 103o F as a result of her autoimmune disease. NHL is a spectrum of disease that can happen outside of lupus flares, but is pathologically very similar to lupus lymphadenitis when occurring in the context of active lupus, making it difficult to distinguish the two diseases3.
1. Guillaume D., et al. “Kikuchi-Fujimoto Disease: Retrospective Study of 91 Cases and Review of the Literature.” Medicine, 2014;93:372-382. Lippincott Williams & Wilkins. 2. Chiu CF, Chow KC, Lin TY, et al. “Virus infection in patients with histiocytic necrotizing lymphadenitis in Taiwan. Detection of Epstein-Barr virus, type I human T-cell lymphotropic virus, and parvovirus B19. Am. J. Clin. Pathol.2000;113:774-7813.Hu, S. et al. “Lupus Lymphadenitis Simulating Kikuchi’s Lymphadenitis in Patients with Systemic Lupus Erythematosus:a Clinicopathologic Review of 6 Cases and Review of the Literature.” Pathology International 2003. 53:221-226
Figure 1.A. Sagittal view MRI of the head and neck demonstrating an enhancing retropharyngeal mass. B. Cross sectional CT chestwith contrast demonstrating bilateral pulmonary infiltrates. C and D: H&E stain of the retropharyngeal mass demonstrating necrosis and histiocytic infiltration with lack of neutrophils.
A Game of Cat and Mouse; Respiratory Distress in the Setting of Multiple Zoonotic Exposures
Stacy Johnson MD, Devin Horton MD, Matthew G Petersen BSUniversity of Utah Department of Internal Medicine
Case Description
Introduction
Objectives
Discussion
References
1.Yadav H, Thompson BT, Gajic O. Fifty Years of Research in ARDS. Is Acute Respiratory Distress Syndrome a Preventable Disease? Am J Rspir Crit Care Med. 2016 Dec 31. [Epub ahead of print]
2.Anand S, Jayakumar D, Aronow WS, Chandy D. Role of Extracorporeal Membrane Oxygenation in Adult Respiratory Failure: An Overvoew. Hosp Pract (1995). 2016;44(2):76-85.
3.Warner GS. Hantavirus illness in humans: review and update. South Med J. 1996 Mar;89(3):264-71.
4.Marx G, Stinson K Deatrich M, Albanese B. Notes from the Field: Hantavirus Pulmonary Syndrome in a Migrant Farm Worker – Colorado, 2016. MMWR Morb Mortal Wkly Rep. 2017 Jan 20;66(2):62-6.
Respiratory compromise may progress very rapidly in the hospitalized patient, causing significant morbidity and mortality. Acutely ill patients are at particularly high risk for acute respiratory distress syndrome (ARDS), a process presenting initially with dyspnea and tachypnea. Diagnostic criteria for ARDS include profound hypoxemia and bilateral pulmonary infiltrates in the absence of cardiac causes. The overall mortality rate for ARDS is 41%. The differential diagnosis is broad, including many infectious agents, environmental exposures, and inflammatory processes.
A thorough workup is important in identifying the etiology of ARDS and thus informing management. However, the workup is most effective when it is informed by a comprehensive history with close attention payed to social history including sick contacts, living conditions, travel and environmental exposures. Here we present a patient with ARDS in which zoonotic exposures elicited in the history led to a diagnosis of Hantavirus.
The key to diagnosis and successful management in this case was our clinical suspicion for Hantavirus which was based on the patient’s self-reported exposure to rodent droppings. Although Hantavirus is rare, the patient history directly informed our workup and management. While there is no definitive treatment for Hantavirus, early supportive intervention with intubation and ECMO contributed to the patient being discharged after one week without the need for supplemental oxygen. To date, the patient has had no complications from her hospitalization.
Chasing the etiology of a diagnosis like ARDS can feel a little like a game of cat and mouse, but when workup is guided by a carefully elicited history it can drastically change patient management as we have seen in this case.
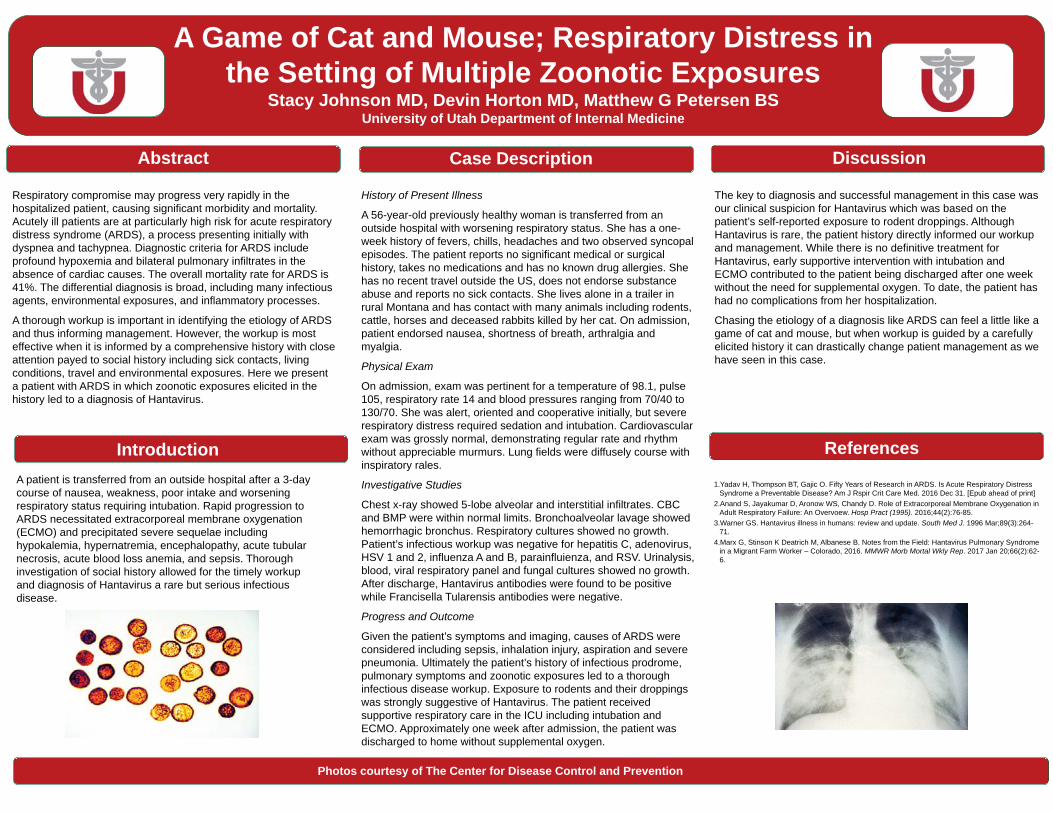
Photos courtesy of The Center for Disease Control and Prevention
History of Present Illness
A 56-year-old previously healthy woman is transferred from an outside hospital with worsening respiratory status. She has a one-week history of fevers, chills, headaches and two observed syncopal episodes. The patient reports no significant medical or surgical history, takes no medications and has no known drug allergies. She has no recent travel outside the US, does not endorse substance abuse and reports no sick contacts. She lives alone in a trailer in rural Montana and has contact with many animals including rodents, cattle, horses and deceased rabbits killed by her cat. On admission, patient endorsed nausea, shortness of breath, arthralgia and myalgia.
Physical Exam
On admission, exam was pertinent for a temperature of 98.1, pulse 105, respiratory rate 14 and blood pressures ranging from 70/40 to 130/70. She was alert, oriented and cooperative initially, but severe respiratory distress required sedation and intubation. Cardiovascular exam was grossly normal, demonstrating regular rate and rhythm without appreciable murmurs. Lung fields were diffusely course with inspiratory rales.
Investigative Studies
Chest x-ray showed 5-lobe alveolar and interstitial infiltrates. CBC and BMP were within normal limits. Bronchoalveolar lavage showed hemorrhagic bronchus. Respiratory cultures showed no growth. Patient’s infectious workup was negative for hepatitis C, adenovirus, HSV 1 and 2, influenza A and B, parainfluienza, and RSV. Urinalysis, blood, viral respiratory panel and fungal cultures showed no growth. After discharge, Hantavirus antibodies were found to be positive while Francisella Tularensis antibodies were negative.
Progress and Outcome
Given the patient’s symptoms and imaging, causes of ARDS were considered including sepsis, inhalation injury, aspiration and severe pneumonia. Ultimately the patient’s history of infectious prodrome,pulmonary symptoms and zoonotic exposures led to a thorough infectious disease workup. Exposure to rodents and their droppings was strongly suggestive of Hantavirus. The patient received supportive respiratory care in the ICU including intubation and ECMO. Approximately one week after admission, the patient was discharged to home without supplemental oxygen.
Abstract
A patient is transferred from an outside hospital after a 3-day course of nausea, weakness, poor intake and worsening respiratory status requiring intubation. Rapid progression to ARDS necessitated extracorporeal membrane oxygenation (ECMO) and precipitated severe sequelae including hypokalemia, hypernatremia, encephalopathy, acute tubular necrosis, acute blood loss anemia, and sepsis. Thorough investigation of social history allowed for the timely workup and diagnosis of Hantavirus a rare but serious infectious disease.
Discussion
References1. Khong, J. J., Casson, R. J., Huilgol, S. C., & Selva, D. (2006). Madarosis. Surv Ophthalmol, 51(6), 550-560. doi:10.1016/j.survophthal.2006.08.0042. Lee, K. W., Kim, S. H., Kim, K. J., Kim, S. H., Kim, H. Y., Kim, B. J., . . . Choi, D. S. (2015). A Rare Manifestation of Hypothyroid Myopathy: Hoffmann's Syndrome. Endocrinol Metab (Seoul), 30(4), 626-630. doi:10.3803/EnM.2015.30.4.6263. Mangaraj, S., & Sethy, G. (2014). Hoffman's syndrome - A rare facet of hypothyroid myopathy. JNeurosci Rural Pract, 5(4), 447-448. doi:10.4103/0976-3147.1400254. Sindoni, A., Rodolico, C., Pappalardo, M. A., Portaro, S., & Benvenga, S. (2016). Hypothyroid myopathy: A peculiar clinical presentation of thyroid failure. Review of the literature. Rev Endocr Metab Disord. doi:10.1007/s11154-016-9357-0
This case represents a rare form of hypothyroid myopathy also known as Hoffman’s syndrome in the medical literature.
On further review of the patient’s medical history he had presented to the emergency department multiple times over the preceding two years, often with concern for confusion, generalized weakness, and bilateral lower extremity pain. His history of alcohol abuse often clouded the picture and took precedence over documented physical exam findings and laboratory abnormalities.
He was noted to have elevated CK levels dating back at least two years prior to this encounter and was found to have mild hypothyroidism though this was apparently never addressed.
The clinic course of hypothyroidism is often insidious but due to early screening and treatment it rarely progresses to the level of neurological and muscle involvement which were seen in this patient.
This case demonstrates the importance of physicians earnestly taking a complete history, performing a thorough physical exam, and following up all abnormal laboratory values no matter how common and insignificant they may seem.
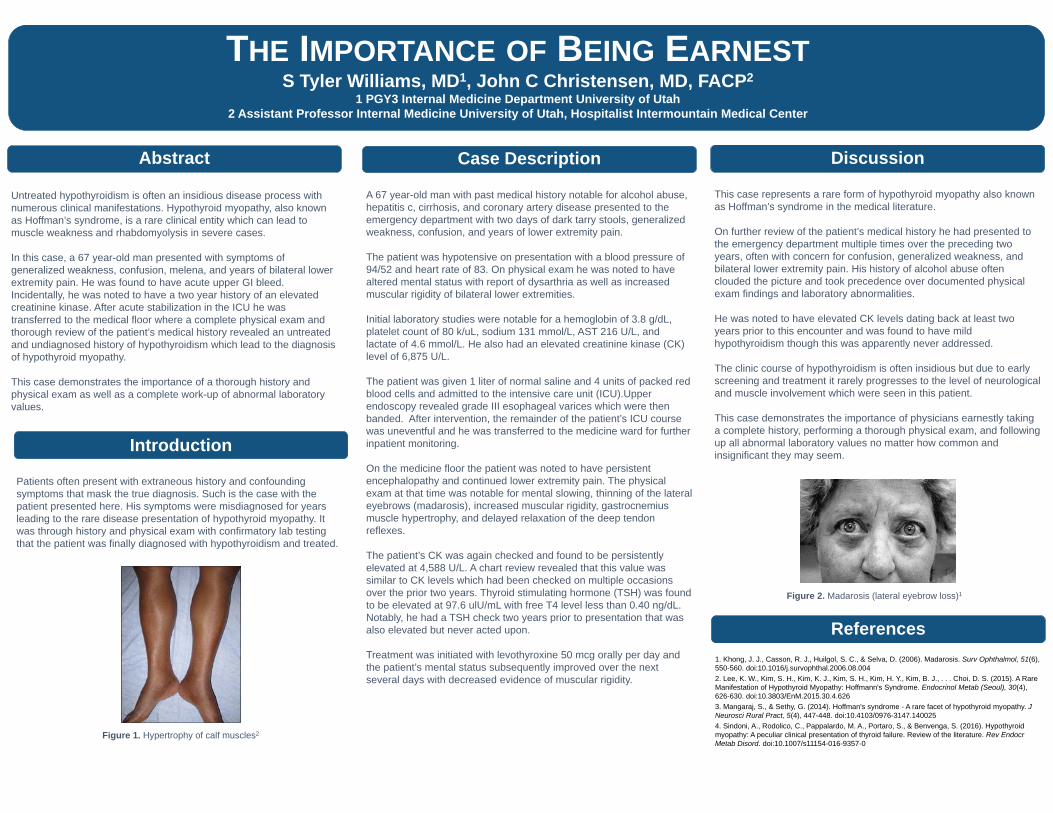
Figure 2. Madarosis (lateral eyebrow loss)1
Introduction
Untreated hypothyroidism is often an insidious disease process with numerous clinical manifestations. Hypothyroid myopathy, also known as Hoffman’s syndrome, is a rare clinical entity which can lead to muscle weakness and rhabdomyolysis in severe cases.
In this case, a 67 year-old man presented with symptoms of generalized weakness, confusion, melena, and years of bilateral lower extremity pain. He was found to have acute upper GI bleed. Incidentally, he was noted to have a two year history of an elevated creatinine kinase. After acute stabilization in the ICU he was transferred to the medical floor where a complete physical exam and thorough review of the patient’s medical history revealed an untreated and undiagnosed history of hypothyroidism which lead to the diagnosis of hypothyroid myopathy.
This case demonstrates the importance of a thorough history and physical exam as well as a complete work-up of abnormal laboratory values.
Abstract
Patients often present with extraneous history and confounding symptoms that mask the true diagnosis. Such is the case with the patient presented here. His symptoms were misdiagnosed for years leading to the rare disease presentation of hypothyroid myopathy. It was through history and physical exam with confirmatory lab testing that the patient was finally diagnosed with hypothyroidism and treated.
Figure 1. Hypertrophy of calf muscles2
THE IMPORTANCE OF BEING EARNESTS Tyler Williams, MD1, John C Christensen, MD, FACP2
1 PGY3 Internal Medicine Department University of Utah2 Assistant Professor Internal Medicine University of Utah, Hospitalist Intermountain Medical Center
Case Description
A 67 year-old man with past medical history notable for alcohol abuse, hepatitis c, cirrhosis, and coronary artery disease presented to the emergency department with two days of dark tarry stools, generalized weakness, confusion, and years of lower extremity pain.
The patient was hypotensive on presentation with a blood pressure of 94/52 and heart rate of 83. On physical exam he was noted to have altered mental status with report of dysarthria as well as increased muscular rigidity of bilateral lower extremities.
Initial laboratory studies were notable for a hemoglobin of 3.8 g/dL, platelet count of 80 k/uL, sodium 131 mmol/L, AST 216 U/L, and lactate of 4.6 mmol/L. He also had an elevated creatinine kinase (CK) level of 6,875 U/L.
The patient was given 1 liter of normal saline and 4 units of packed red blood cells and admitted to the intensive care unit (ICU).Upper endoscopy revealed grade III esophageal varices which were then banded. After intervention, the remainder of the patient’s ICU course was uneventful and he was transferred to the medicine ward for further inpatient monitoring.
On the medicine floor the patient was noted to have persistent encephalopathy and continued lower extremity pain. The physical exam at that time was notable for mental slowing, thinning of the lateral eyebrows (madarosis), increased muscular rigidity, gastrocnemius muscle hypertrophy, and delayed relaxation of the deep tendon reflexes.
The patient’s CK was again checked and found to be persistently elevated at 4,588 U/L. A chart review revealed that this value was similar to CK levels which had been checked on multiple occasions over the prior two years. Thyroid stimulating hormone (TSH) was found to be elevated at 97.6 ulU/mL with free T4 level less than 0.40 ng/dL. Notably, he had a TSH check two years prior to presentation that was also elevated but never acted upon.
Treatment was initiated with levothyroxine 50 mcg orally per day and the patient’s mental status subsequently improved over the next several days with decreased evidence of muscular rigidity.
An Unexpected Etiology of EncephalopathyAlex J. Wright, MS3
University of Utah School of Medicine
Case Description
Introduction
Discussion
References1.Differential Diagnosis for Bilateral Abnormalities of the Basal Ganglia and Thalamus, RadioGraphics 2011. 2.Nonalocoholic Thiamine-Related Encephalopathy (Wenicke-Korsakoff Syndrome) Among Inpatient with
Cancer: A Series of 18 Cases, Psychosomatics 2016.3.Wernicke Encephalopathy: A Future Problem Even After Sleeve Gastrectomy? A Systematic Literature
Review, Obes Surg. 2016.4.The Wernicke-Korsakoff syndrome and related disorders due to alcoholism and malnutrition. FA Davis,
Philadelphia 1989.
This clinical vignette presents a patient with a history of decompensated cirrhosis secondary to Primary Sclerosing Cholangitis and Crohn’s disease who transferred from an outside hospital with sepsis and concerns for spontaneous bacterial peritonitis.
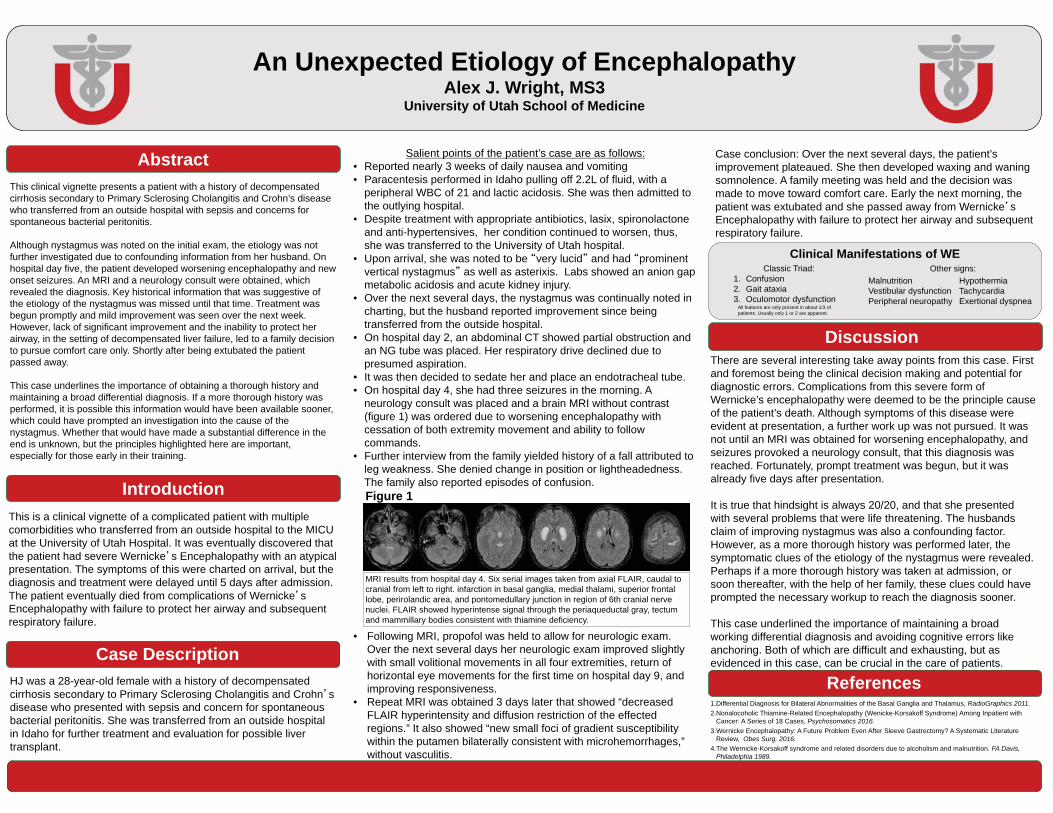
Although nystagmus was noted on the initial exam, the etiology was not further investigated due to confounding information from her husband. On hospital day five, the patient developed worsening encephalopathy and new onset seizures. An MRI and a neurology consult were obtained, which revealed the diagnosis. Key historical information that was suggestive of the etiology of the nystagmus was missed until that time. Treatment was begun promptly and mild improvement was seen over the next week. However, lack of significant improvement and the inability to protect her airway, in the setting of decompensated liver failure, led to a family decision to pursue comfort care only. Shortly after being extubated the patient passed away.
This case underlines the importance of obtaining a thorough history and maintaining a broad differential diagnosis. If a more thorough history was performed, it is possible this information would have been available sooner, which could have prompted an investigation into the cause of the nystagmus. Whether that would have made a substantial difference in the end is unknown, but the principles highlighted here are important, especially for those early in their training.
There are several interesting take away points from this case. First and foremost being the clinical decision making and potential for diagnostic errors. Complications from this severe form of Wernicke’s encephalopathy were deemed to be the principle cause of the patient’s death. Although symptoms of this disease were evident at presentation, a further work up was not pursued. It was not until an MRI was obtained for worsening encephalopathy, and seizures provoked a neurology consult, that this diagnosis was reached. Fortunately, prompt treatment was begun, but it was already five days after presentation.
It is true that hindsight is always 20/20, and that she presented with several problems that were life threatening. The husbands claim of improving nystagmus was also a confounding factor. However, as a more thorough history was performed later, the symptomatic clues of the etiology of the nystagmus were revealed. Perhaps if a more thorough history was taken at admission, or soon thereafter, with the help of her family, these clues could have prompted the necessary workup to reach the diagnosis sooner.
This case underlined the importance of maintaining a broad working differential diagnosis and avoiding cognitive errors like anchoring. Both of which are difficult and exhausting, but as evidenced in this case, can be crucial in the care of patients.
HJ was a 28-year-old female with a history of decompensated cirrhosis secondary to Primary Sclerosing Cholangitis and Crohn sdisease who presented with sepsis and concern for spontaneous bacterial peritonitis. She was transferred from an outside hospital in Idaho for further treatment and evaluation for possible liver transplant.
Abstract
This is a clinical vignette of a complicated patient with multiple comorbidities who transferred from an outside hospital to the MICU at the University of Utah Hospital. It was eventually discovered that the patient had severe Wernicke s Encephalopathy with an atypical presentation. The symptoms of this were charted on arrival, but the diagnosis and treatment were delayed until 5 days after admission. The patient eventually died from complications of Wernicke sEncephalopathy with failure to protect her airway and subsequent respiratory failure.
Salient points of the patient’s case are as follows: • Reported nearly 3 weeks of daily nausea and vomiting• Paracentesis performed in Idaho pulling off 2.2L of fluid, with a
peripheral WBC of 21 and lactic acidosis. She was then admitted to the outlying hospital.
• Despite treatment with appropriate antibiotics, lasix, spironolactone and anti-hypertensives, her condition continued to worsen, thus, she was transferred to the University of Utah hospital.
• Upon arrival, she was noted to be very lucid and had prominent vertical nystagmus as well as asterixis. Labs showed an anion gap metabolic acidosis and acute kidney injury.
• Over the next several days, the nystagmus was continually noted in charting, but the husband reported improvement since being transferred from the outside hospital.
• On hospital day 2, an abdominal CT showed partial obstruction and an NG tube was placed. Her respiratory drive declined due to presumed aspiration.
• It was then decided to sedate her and place an endotracheal tube.• On hospital day 4, she had three seizures in the morning. A
neurology consult was placed and a brain MRI without contrast (figure 1) was ordered due to worsening encephalopathy with cessation of both extremity movement and ability to follow commands.
• Further interview from the family yielded history of a fall attributed to leg weakness. She denied change in position or lightheadedness. The family also reported episodes of confusion.
Case conclusion: Over the next several days, the patient’s improvement plateaued. She then developed waxing and waning somnolence. A family meeting was held and the decision was made to move toward comfort care. Early the next morning, the patient was extubated and she passed away from Wernicke sEncephalopathy with failure to protect her airway and subsequent respiratory failure.
Figure 1
MRI results from hospital day 4. Six serial images taken from axial FLAIR, caudal to cranial from left to right. infarction in basal ganglia, medial thalami, superior frontal lobe, perirolandic area, and pontomedullary junction in region of 6th cranial nerve nuclei. FLAIR showed hyperintense signal through the periaqueductal gray, tectum and mammillary bodies consistent with thiamine deficiency.
• Following MRI, propofol was held to allow for neurologic exam. Over the next several days her neurologic exam improved slightly with small volitional movements in all four extremities, return of horizontal eye movements for the first time on hospital day 9, and improving responsiveness.
• Repeat MRI was obtained 3 days later that showed “decreased FLAIR hyperintensity and diffusion restriction of the effected regions.” It also showed “new small foci of gradient susceptibility within the putamen bilaterally consistent with microhemorrhages,” without vasculitis.
Clinical Manifestations of WEClassic Triad:
1. Confusion2. Gait ataxia3. Oculomotor dysfunction
MalnutritionVestibular dysfunctionPeripheral neuropathy
HypothermiaTachycardiaExertional dyspnea
Other signs:
All features are only present in about 1/3 of patients. Usually only 1 or 2 are apparent.
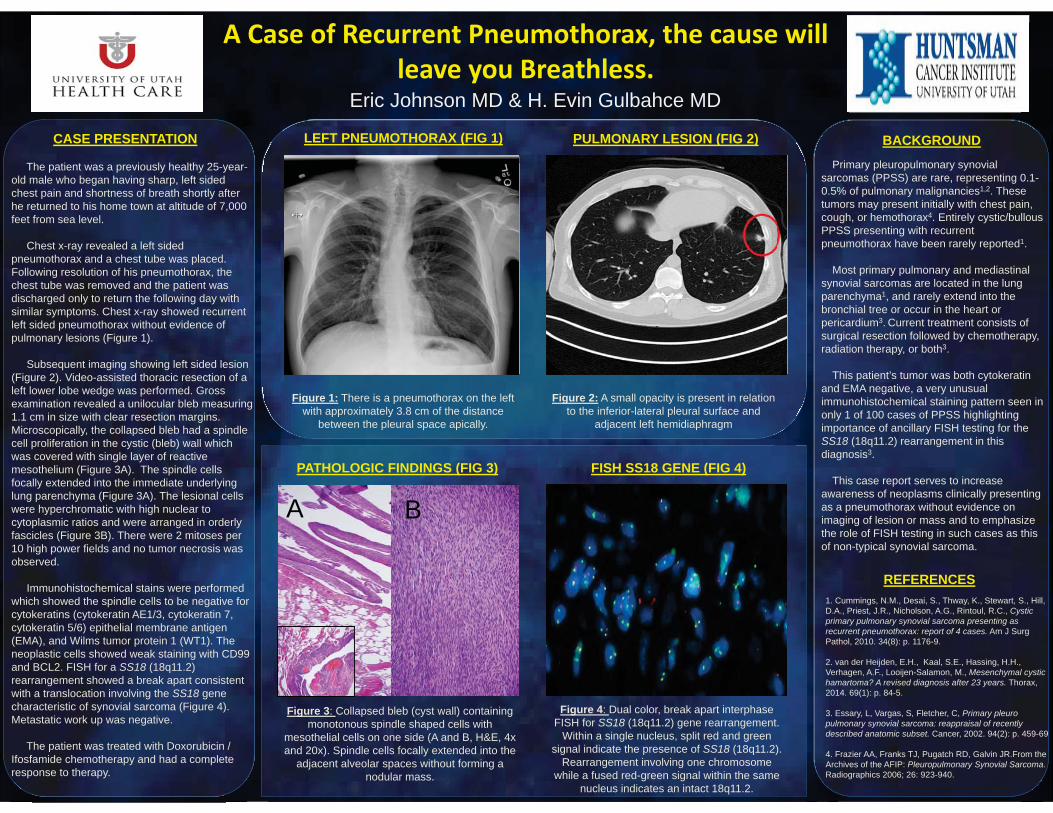
A Case of Recurrent Pneumothorax, the cause will leave you Breathless.
1. Cummings, N.M., Desai, S., Thway, K., Stewart, S., Hill, D.A., Priest, J.R., Nicholson, A.G., Rintoul, R.C., Cystic primary pulmonary synovial sarcoma presenting as recurrent pneumothorax: report of 4 cases. Am J Surg Pathol, 2010. 34(8): p. 1176-9.
2. van der Heijden, E.H., Kaal, S.E., Hassing, H.H., Verhagen, A.F., Looijen-Salamon, M., Mesenchymal cystic hamartoma? A revised diagnosis after 23 years. Thorax, 2014. 69(1): p. 84-5.
3. Essary, L, Vargas, S, Fletcher, C, Primary pleuro pulmonary synovial sarcoma: reappraisal of recently described anatomic subset. Cancer, 2002. 94(2): p. 459-69
4. Frazier AA, Franks TJ, Pugatch RD, Galvin JR.From the Archives of the AFIP: Pleuropulmonary Synovial Sarcoma.Radiographics 2006; 26: 923-940.
CASE PRESENTATION BACKGROUND
REFERENCES
Eric Johnson MD & H. Evin Gulbahce MD
Figure 1: There is a pneumothorax on the left with approximately 3.8 cm of the distance
between the pleural space apically.
LEFT PNEUMOTHORAX (FIG 1) PULMONARY LESION (FIG 2)
Figure 2: A small opacity is present in relation to the inferior-lateral pleural surface and
adjacent left hemidiaphragm
The patient was a previously healthy 25-year-old male who began having sharp, left sided chest pain and shortness of breath shortly after he returned to his home town at altitude of 7,000 feet from sea level.
Chest x-ray revealed a left sided pneumothorax and a chest tube was placed. Following resolution of his pneumothorax, the chest tube was removed and the patient was discharged only to return the following day with similar symptoms. Chest x-ray showed recurrent left sided pneumothorax without evidence of pulmonary lesions (Figure 1).
Subsequent imaging showing left sided lesion (Figure 2). Video-assisted thoracic resection of a left lower lobe wedge was performed. Gross examination revealed a unilocular bleb measuring 1.1 cm in size with clear resection margins. Microscopically, the collapsed bleb had a spindle cell proliferation in the cystic (bleb) wall which was covered with single layer of reactive mesothelium (Figure 3A). The spindle cells focally extended into the immediate underlying lung parenchyma (Figure 3A). The lesional cells were hyperchromatic with high nuclear to cytoplasmic ratios and were arranged in orderly fascicles (Figure 3B). There were 2 mitoses per 10 high power fields and no tumor necrosis was observed.
Immunohistochemical stains were performed which showed the spindle cells to be negative for cytokeratins (cytokeratin AE1/3, cytokeratin 7, cytokeratin 5/6) epithelial membrane antigen (EMA), and Wilms tumor protein 1 (WT1). The neoplastic cells showed weak staining with CD99 and BCL2. FISH for a SS18 (18q11.2) rearrangement showed a break apart consistent with a translocation involving the SS18 genecharacteristic of synovial sarcoma (Figure 4). Metastatic work up was negative.
The patient was treated with Doxorubicin / Ifosfamide chemotherapy and had a complete response to therapy.
PATHOLOGIC FINDINGS (FIG 3) FISH SS18 GENE (FIG 4)
Figure 4: Dual color, break apart interphase FISH for SS18 (18q11.2) gene rearrangement.
Within a single nucleus, split red and green signal indicate the presence of SS18 (18q11.2).
Rearrangement involving one chromosome while a fused red-green signal within the same
nucleus indicates an intact 18q11.2.
Figure 3: Collapsed bleb (cyst wall) containing monotonous spindle shaped cells with
mesothelial cells on one side (A and B, H&E, 4x and 20x). Spindle cells focally extended into the
adjacent alveolar spaces without forming a nodular mass.
A B
Primary pleuropulmonary synovial sarcomas (PPSS) are rare, representing 0.1-0.5% of pulmonary malignancies1,2. These tumors may present initially with chest pain, cough, or hemothorax4. Entirely cystic/bullous PPSS presenting with recurrent pneumothorax have been rarely reported1.
Most primary pulmonary and mediastinal synovial sarcomas are located in the lung parenchyma1, and rarely extend into the bronchial tree or occur in the heart or pericardium3. Current treatment consists of surgical resection followed by chemotherapy, radiation therapy, or both3.
This patient’s tumor was both cytokeratin and EMA negative, a very unusual immunohistochemical staining pattern seen in only 1 of 100 cases of PPSS highlighting importance of ancillary FISH testing for the SS18 (18q11.2) rearrangement in this diagnosis3.
This case report serves to increase awareness of neoplasms clinically presenting as a pneumothorax without evidence on imaging of lesion or mass and to emphasize the role of FISH testing in such cases as this of non-typical synovial sarcoma.
Rheumatological Disease from Cardiac Point of View:A Systematic Review
Mossab A. Aljuaid, MD, Gurusher Panjrath, MD
Heart and Vascular Institute, George Washington University School of Medicine, Washington, DC, USA.
Methods
Introduction
Objectives
Results
Discussion
References
Rheumatologic disorders have been associated with
premature atherosclerosis leading to ischemic heart
disease at a young age. The increased risk for coronary
events may be a result of chronic systemic inflammation
from the rheumatic disease. A close collaboration is
needed between cardiologists and rheumatologists in
managing this group of patients for overlapping
conditions. Further research is needed to understand the
impact of cardiovascular diseases on morbidity and
mortality in rheumatic diseases.
Online databases (PubMed and Medline) were searched
from inception to January 2016. Search terms included:
“systemic lupus erythematosus”, “rheumatoid arthritis”,
“cardiovascular diseases”, “cardiovascular mortality”,
“sudden cardiac death”, and “atherosclerosis”. Studies
meeting the following criteria were included: (a) Articles
are written in English language, (b) Reference to the
cardiac involvement in rheumatic diseases, and (c)
Articles where full text available.
Cardiovascular diseases are commonly encountered in
rheumatic disease. The current systematic review was
useful in describing the prevalence of cardiovascular
involvement in each of the rheumatic diseases.
Online databases (PubMed and Medline) were searched
from inception to January 2016. Search terms included:
“systemic lupus erythematosus”, “rheumatoid arthritis”,
“cardiovascular diseases”, “cardiovascular mortality”,
“sudden cardiac death”, and “atherosclerosis”. Studies
meeting the following criteria were included: (a) Articles
are written in English language, (b) Reference to the
cardiac involvement in rheumatic diseases, and (c)
Articles where full text available.
.
Abstract
Cardiac involvement in rheumatic diseases is associated
with increased risk of mortality compared to general
population and require prompt diagnosis and treatment. It
can be the first presentation in patients with no previous
diagnosis or manifest in patients with a known
rheumatologic disorder. The aim of our study was to
conduct a systematic review of the literature regarding the
cardiovascular involvement in various rheumatic
diseases. Commonly used treatments for rheumatic
disease and their cardiovascular side effects were studied
as well.
1. Cardiac manifestations of rheumatological conditions: a narrative review. ISRN Rheumatol.
2. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N Engl J Med.
3. Connective-tissue disease, antibodies to ribonucleoprotein, and congenital heart block. N Engl J Med.
4. Epidemiology of the rheumatic diseases. Oxford
Figure 1. Cardiovascular involvement in different rheumatological diseases.
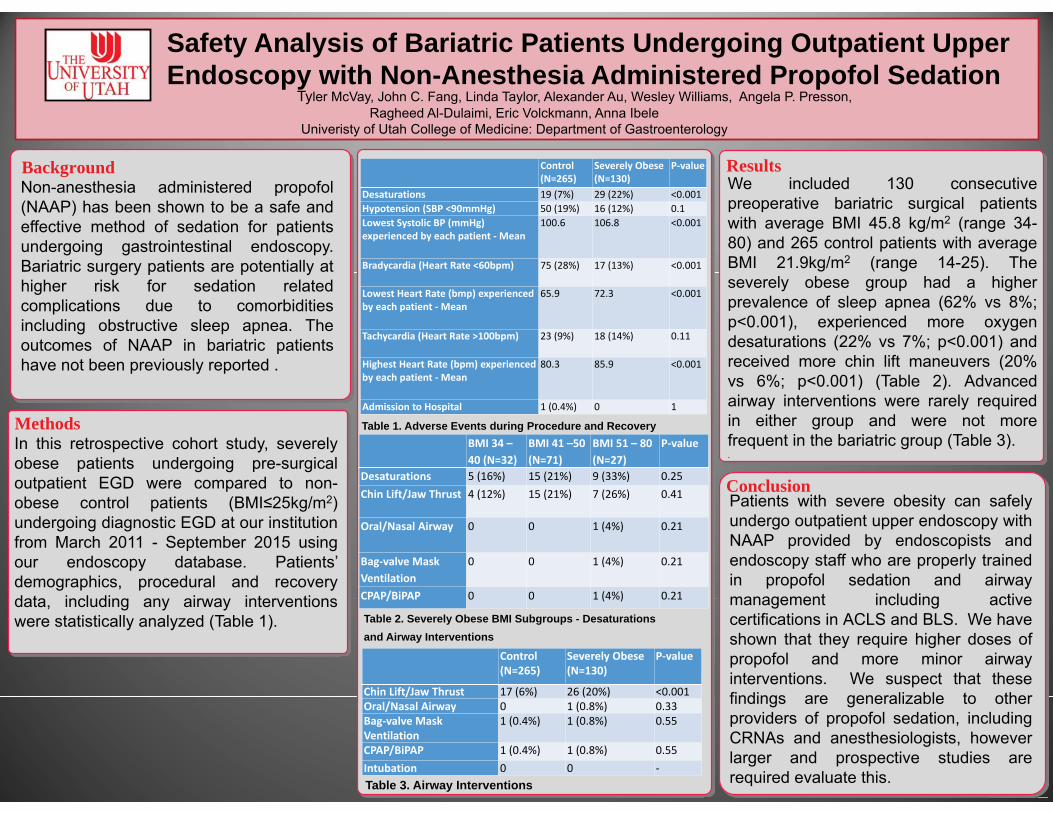
Background Results
Conclusion
Methods
Safety Analysis of Bariatric Patients Undergoing Outpatient Upper Endoscopy with Non-Anesthesia Administered Propofol Sedation
Control (N=265)
Severely Obese(N=130)
P-value
Desaturations 19 (7%) 29 (22%) <0.001Hypotension (SBP <90mmHg) 50 (19%) 16 (12%) 0.1Lowest Systolic BP (mmHg) experienced by each patient - Mean
100.6 106.8 <0.001
Bradycardia (Heart Rate <60bpm) 75 (28%) 17 (13%) <0.001
Lowest Heart Rate (bmp) experienced by each patient - Mean
65.9 72.3 <0.001
Tachycardia (Heart Rate >100bpm) 23 (9%) 18 (14%) 0.11
Highest Heart Rate (bpm) experienced by each patient - Mean
80.3 85.9 <0.001
Admission to Hospital 1 (0.4%) 0 1
Control (N=265)
Severely Obese (N=130)
P-value
Chin Lift/Jaw Thrust 17 (6%) 26 (20%) <0.001Oral/Nasal Airway 0 1 (0.8%) 0.33Bag-valve Mask Ventilation
1 (0.4%) 1 (0.8%) 0.55
CPAP/BiPAP 1 (0.4%) 1 (0.8%) 0.55Intubation 0 0 -
BMI 34 –40 (N=32)
BMI 41 –50 (N=71)
BMI 51 – 80 (N=27)
P-value
Desaturations 5 (16%) 15 (21%) 9 (33%) 0.25Chin Lift/Jaw Thrust 4 (12%) 15 (21%) 7 (26%) 0.41
Oral/Nasal Airway 0 0 1 (4%) 0.21
Bag-valve Mask Ventilation
0 0 1 (4%) 0.21
CPAP/BiPAP 0 0 1 (4%) 0.21
Table 2. Severely Obese BMI Subgroups - Desaturations and Airway Interventions
Table 1. Adverse Events during Procedure and Recovery
Table 3. Airway Interventions

The Descriptive Epidemiology of Multimorbidity and Health Service Utilization in Primary Care in England
Anna Cassell, Duncan Edwards, and Amelia HarshfieldUniversity of Cambridge Department of Public Health and Primary Care
Methods
Introduction
Objectives
Results
Discussion
References1.van den Akker, M., Buntinx, F., Metsemakers, J. F. M., Roos, S. & Knottnerus, J. A. Multimorbidity in General
Practice: Prevalence, Incidence, and Determinants of Co-Occurring Chronic and Recurrent Diseases. J. Clin. Epidemiol. 51, 367–375 (1998).
2.Salisbury, C., Johnson, L., Purdy, S., Valderas, J. M. & Montgomery, A. A. Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br. J. Gen. Pract. 61, e12–21 (2011).
3.van Oostrom, S. H. et al. Multimorbidity of chronic diseases and health care utilization in general practice. BMC Fam. Pract. 15, 61 (2014).
4.Barnett, K. et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 380, 37–43 (2012).
5.Clinical Practice Research Datalink - CPRD. at <https://www.cprd.com/intro.asp>6.Herrett, E. et al. Data Resource Profile: Clinical Practice Research Datalink (CPRD). Int. J. Epidemiol.
dyv098– (2015). doi:10.1093/ije/dyv09
Background: Studies suggest that increasing numbers of people have multimorbidity, which is the simultaneous presence of two or more long-term illnesses, such as diabetes or depression. Multimorbidity places a substantial burden on patients as well as on primary care medicine providers, especially General Practitioners (GPs), who must treat and manage patients with multiple illnesses and diseases. This study used routinely collected primary care medical record data to describe the prevalence of multimorbidity in adults in England and to investigate the association of multimorbidity with usage of health services.
Methods: Medical records from the UK’s Clinical Practice Research Datalink (CPRD) were used to conduct a cross-sectional study of the prevalence of multimorbidity and a cohort study of health service utilisation. In the cross-sectional component of this study, data was extracted from patient records for a random sample of 403,985 adult patients in England who were registered with a general practice as of January 1, 2012. Multimorbidity was defined as the presence of two or more of 36 comorbidities and comorbidities were identified based on diagnostic and prescription codes in the patients’ medical records. Health service utilization was determined by following the cohort of patients from the initial sample for four years to investigate the association between multimorbidity and the yearly incident rates of GP consultations, prescription medications, and hospital admissions, as well as the all-cause mortality rate.
Results: 27.4% of patients had multimorbidity and increased multimorbidity was strongly associated with higher levels of socioeconomic deprivation. Multimorbidity was strongly associated with health service utilisation. While 27% of the population were multimorbid, those patients accounted for 53% of GP consultations, 64% of issued prescriptions, and 56% percent of hospital admissions.
Conclusion: Multimorbidity is common condition and is highly associated with increased health service utilisation. This study highlights the need for practice and national-level policies to improve the quality and efficiency of general practice care provided to multimorbid patients.
Acknowledgements: Special thanks to Dr. Lucy Gerza and James Brimicombe
Abstract
Multimorbidity is generally defined as the coexistence of two or more chronic medical conditions or diseases. Patients with numerous chronic conditions often have more complicated medical needs, which include understanding and self-managing multiple illnesses and managing complex medication regimens. Multimorbidity can be challenging to manage from a healthcare perspective because these patients often require more intensive treatment and monitoring by physicians, nurses, and other healthcare team members.2 As the population of elderly individuals in England continues to grow, multimorbidity will become an increasingly common and burdensome medical problem in primary care.
Patients with multiple chronic conditions place great strains on individual GPs, which is compounded by the fact that in England consultation rates and overall GP clinical workload have been increasing substantially, and it has been suggested that this rate of increase in the primary care workload is unsustainable.15 Thus, describing the relationship and quantifying the associations between multimorbidity and health service utilisation is essential to optimising the planning, organisation, and delivery of health services to multimorbid patients in order to provide sustainable, high quality medical care. Investigating these associations can provide information about the aspects of primary care that are overburdened, identifying areas for increased resource allocation or systems-level restructuring to target.
This study sought to replicate and expand upon previous work that had been conducted by Karen Barnett studying the prevalence of multimorbidity in Scotland.4 Our study achieved this by consulting with GP physicians to improve the list of diseases and conditions that were considered multimorbidity and the diagnostic and prescription codes that we used to identify patients with these conditions. Additionally, we sought to take our study a step further by not only describing the epidemiology of multimorbidity, but also evaluating the way that multimorbid patients utilize health services.
Data for this study was obtained from the Clinical Practice Research Datalink (CPRD)• Anonymized patient information from electronic medical recrods in UK• Information from 6.9% of UK population, and representative of the whole UK
population • 403,985 random adult patients participated in the study
Data linkages:• CPRD only provides information from general practice electronic medical record• Linked data to Index of Multiple Deprivation (IMD) for socioeconomic status• Linked to Integrated Hospital Episode Statistics for information on
hospitalizaitons• Data linkage was only available for English practices (not Scotland, Wales, or N.
Ireland)
Definition of multimorbidity: • Multimorbidity was defined by creating a list of comorbidities that consisted of
chronic diseases and long-term illnesses that had face value validity as conditions contributing to multimorbidity in primary care.
• The list of comorbidities was created by a group of researchers and GP physicians in the University of Cambridge’s Primary Care Unit, and drew largely on the previous work of Barnett et al. (published in 2012) that had examined the epidemiology of multimorbidity in primary care in Scotland.
• The morbidities that were selected for our study followed the same criterion as Barnett et al., which was to identify “those morbidities which were likely to be chronic (defined as having significant impact over at least the most recent year) and with significant impact on patients in terms of need for chronic treatment, reduced function, reduced quality of life, and risk of future morbidity and mortality.”42
36 conditions that defined multimorbidity: hypertension; depression and anxiety; painful condition; asthma; coronary heart disease; diabetes; thyroid disorders; rheumatoid arthritis and inflammatory polyarthropathies; hearing loss; COPD; IBS; recent cancer diagnosis; alcohol problems; psychoactive substance misuses; treated constipation; stroke; chronic kidney disease; diverticulitis; atrial fibrillation; peripheral vascular disease; heart failure; prostate disorders; treated epilepsy; dementia; schizophrenia and non-organic psychosis; psoriasis or eczema; inflammatory bowel disease; migraine; blindness; chronic sinusitis; learning disability; anorexia or bulimia; bronchiectasis; Parkinson’s disease; multiple sclerosis; chronic liver disease and viral hepatitis.
Extracting data from medical records: • Information identifying morbidities was extracted from CPRD by applying
algorithms to the medical and prescription codes in the patient’s record.• Medical codes (med codes) provided medical diagnoses and prescription codes
provided information on prescriptions that could be used to diagnose a morbidity. For example, for a patient to have asthma, they had to have a medical code for asthma in their record and 4 prescriptions for asthma medication in the last year.
Study Design:1. A cross-sectional study design to describe the prevalence of multimorbidity in
English general practice, and to describe the prevalence of multimorbidity in relation to sex, age, and socioeconomic status.
2. A cohort study design to describe health service utilization based on GP consultations, number of prescriptions, and number of hospitalizations between 2012 and 2015.
Descriptive Epidemiology of Multimorbidity:• 27.4% of patients were multimorbid• Females had significantly higher prevalence than males, 30.1% versus 24.6%. • Prevalence was higher with greater levels of socioeconomic deprivation; 25.8% in the
least deprived quintile compared to 30.0% in the most deprived quintile.• The most prevalent morbidities were: Hypertension (18.2%), Depression and Anxiety
(10.3%), Painful Condition (10%), and Hearing Loss (9.5%)
Health Service Utilization:• A majority of GP consultations, prescriptions, and hospital admissions were devoted to
multimorbid patients. • 53.35% of GP consultations during the study’s 4-year follow-up period were in
multimorbid patients, despite only 27.4% of patients having multimorbidity.• The incident rate for GP consultations in multimorbid patients was 2.45 • The median number of GP consultations for a non-multimorbid patient was 2 per year
compared to 9 consultations per year for multimorbid patients. • 77.46% of all prescriptions were given to patients with multimorbidity. • 63.9% of “unique prescriptions” (only counting each type of prescription medication
once) were for multimorbid patients. • The incident rate of unique prescriptions in multimorbid patients being 3.49 times the
rate in the non-multimorbid group. • 55.82% of hospitalizations were multimorbid patients. • The incident rate of hospital admissions in multimorbid patients was 2.47 times the rate
in non-multimorbid patients.
• The population prevalence of multimorbidity was slightly higher in this study compared with previous studies on similar populations in Scotland and England (23.2% and 16% respectively).
• Higher frequency of multimorbidity in socioeconomically deprived individuals is likely partially attributable to disproportionately higher levels of mental-health morbidities in those patients
• Higher rates of GP consultations in multimorbid patients might be reduced by increasing the length of consultations for patients with multimorbidity so that all of their health problems can be addressed in one visit. Expanding routine, outpatient care that is conducted by non-physician medical professionals might also reduce the number of GP consultations, while not compromising quality of care.
• High rates of hospitalizations in multimorbid patients could be reduced by providing multimorbid patients with secondary care that intermediates between their primary care physician and the hospital. This could help reduce the number of hospitalizations, which would benefit patients while also reducing healthcare costs.
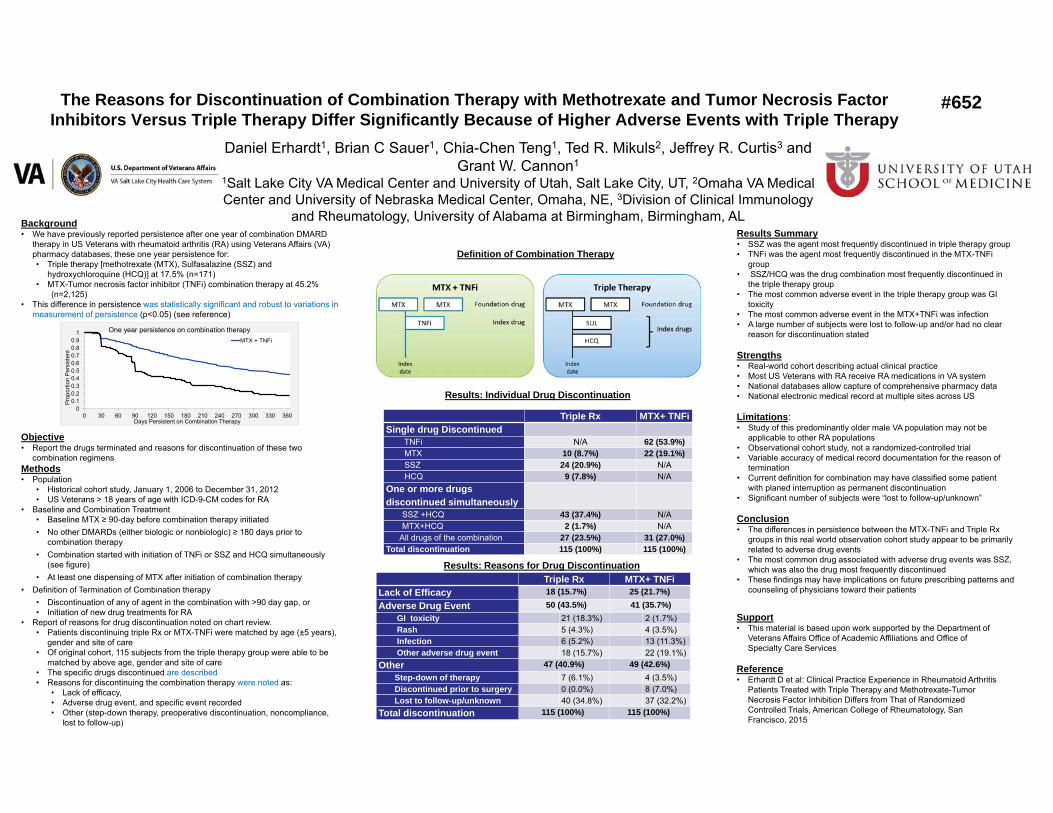
The Reasons for Discontinuation of Combination Therapy with Methotrexate and Tumor Necrosis Factor Inhibitors Versus Triple Therapy Differ Significantly Because of Higher Adverse Events with Triple Therapy
Background
Objective
Methods
Results Summary
Strengths
Limitations
Conclusion
Support
Reference
#652
Definition of Combination Therapy
Triple Rx MTX+ TNFi Single drug Discontinued
62 (53.9%)10 (8.7%) 22 (19.1%)
24 (20.9%)9 (7.8%)
One or more drugs discontinued simultaneously
43 (37.4%)2 (1.7%)
27 (23.5%) 31 (27.0%)Total discontinuation 115 (100%) 115 (100%)
Triple Rx MTX+ TNFiLack of Efficacy 18 (15.7%) 25 (21.7%)Adverse Drug Event 50 (43.5%) 41 (35.7%)
GI toxicityRashInfection Other adverse drug event
Other 47 (40.9%) 49 (42.6%)Step-down of therapyDiscontinued prior to surgeryLost to follow-up/unknown
Total discontinuation 115 (100%) 115 (100%)
Results: Individual Drug Discontinuation
Results: Reasons for Drug Discontinuation
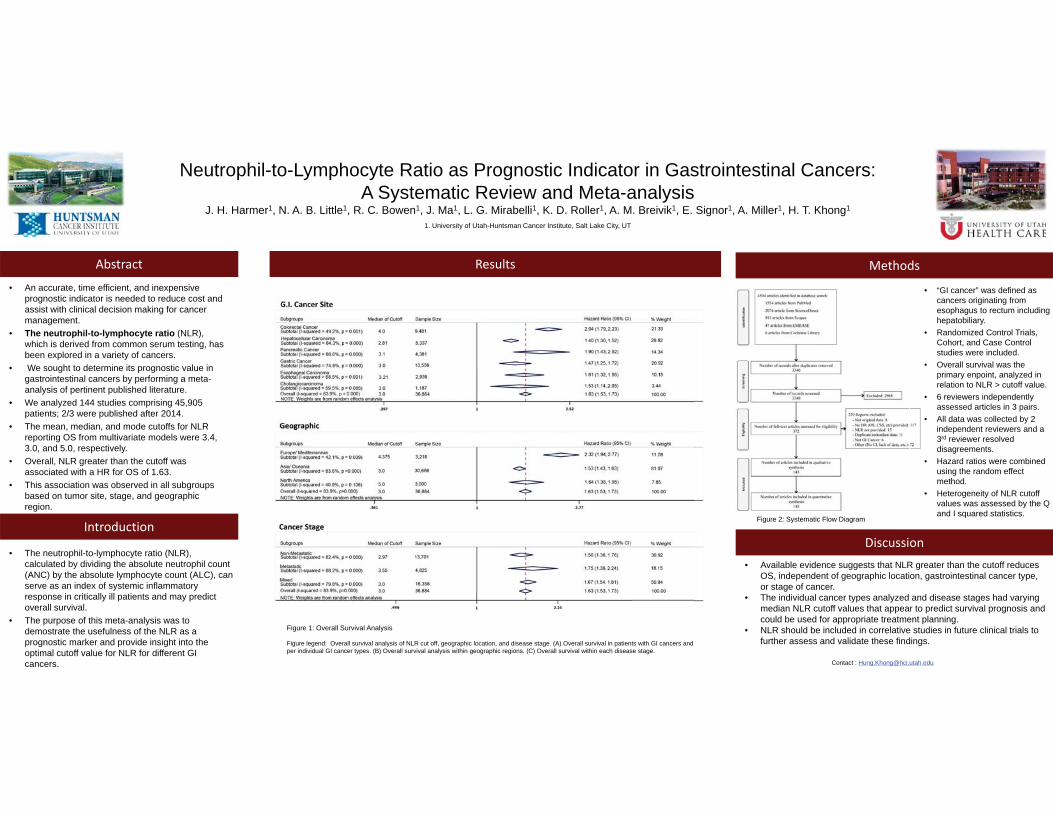
Neutrophil-to-Lymphocyte Ratio as Prognostic Indicator in Gastrointestinal Cancers: A Systematic Review and Meta-analysis
J. H. Harmer1, N. A. B. Little1, R. C. Bowen1, J. Ma1, L. G. Mirabelli1, K. D. Roller1, A. M. Breivik1, E. Signor1, A. Miller1, H. T. Khong1
1. University of Utah-Huntsman Cancer Institute, Salt Lake City, UT
Abstract Results
• An accurate, time efficient, and inexpensive prognostic indicator is needed to reduce cost and assist with clinical decision making for cancer management.
• The neutrophil-to-lymphocyte ratio (NLR), which is derived from common serum testing, has been explored in a variety of cancers.
• We sought to determine its prognostic value in gastrointestinal cancers by performing a meta-analysis of pertinent published literature.
• We analyzed 144 studies comprising 45,905 patients; 2/3 were published after 2014.
• The mean, median, and mode cutoffs for NLR reporting OS from multivariate models were 3.4, 3.0, and 5.0, respectively.
• Overall, NLR greater than the cutoff was associated with a HR for OS of 1.63.
• This association was observed in all subgroups based on tumor site, stage, and geographic region.
Introduction
• The neutrophil-to-lymphocyte ratio (NLR), calculated by dividing the absolute neutrophil count (ANC) by the absolute lymphocyte count (ALC), can serve as an index of systemic inflammatory response in critically ill patients and may predict overall survival.
• The purpose of this meta-analysis was to demostrate the usefulness of the NLR as a prognostic marker and provide insight into the optimal cutoff value for NLR for different GI cancers.
Discussion• Available evidence suggests that NLR greater than the cutoff reduces
OS, independent of geographic location, gastrointestinal cancer type, or stage of cancer.
• The individual cancer types analyzed and disease stages had varying median NLR cutoff values that appear to predict survival prognosis and could be used for appropriate treatment planning.
• NLR should be included in correlative studies in future clinical trials to further assess and validate these findings.
Contact : [email protected]
Methods
Figure 2: Systematic Flow Diagram
• “GI cancer” was defined as cancers originating from esophagus to rectum including hepatobiliary.
• Randomized Control Trials, Cohort, and Case Control studies were included.
• Overall survival was the primary enpoint, analyzed in relation to NLR > cutoff value.
• 6 reviewers independently assessed articles in 3 pairs.
• All data was collected by 2 independent reviewers and a 3rd reviewer resolved disagreements.
• Hazard ratios were combined using the random effect method.
• Heterogeneity of NLR cutoff values was assessed by the Q and I squared statistics.
Figure 1: Overall Survival Analysis
Figure legend: Overall survival analysis of NLR cut off, geographic location, and disease stage. (A) Overall survival in patients with GI cancers and per individual GI cancer types. (B) Overall survival analysis within geographic regions. (C) Overall survival within each disease stage.
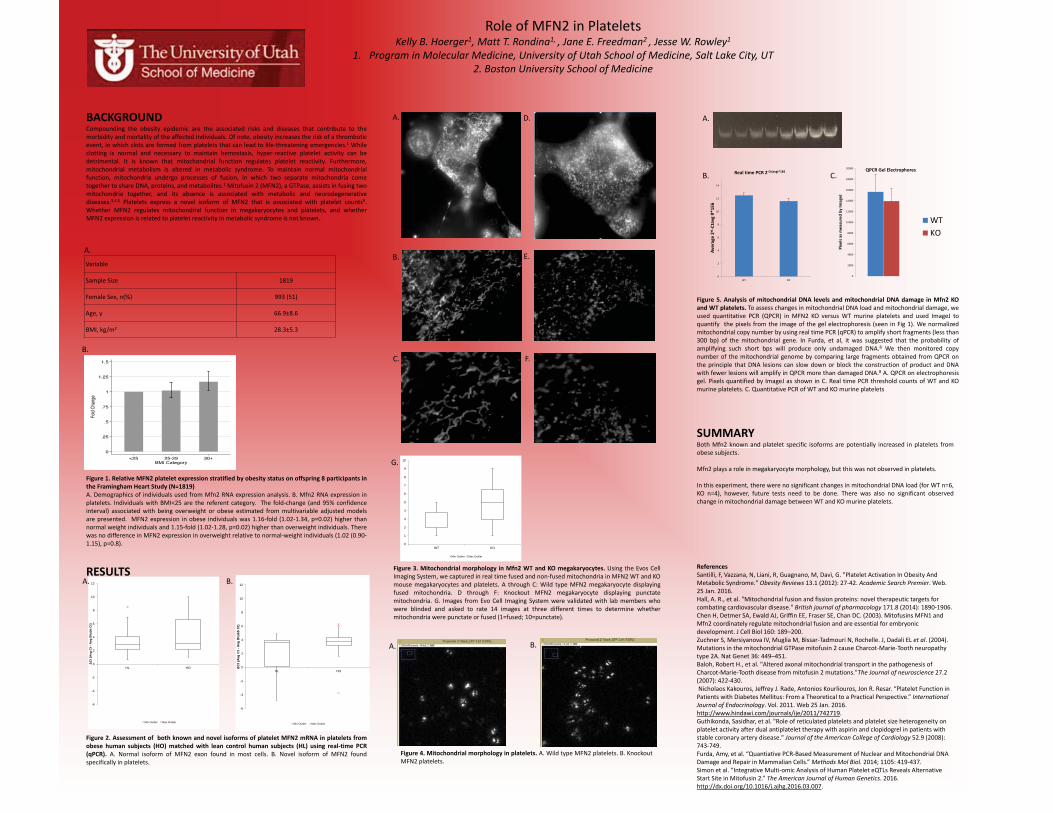
Role of MFN2 in Platelets Kelly B. Hoerger1, Matt T. Rondina1, , Jane E. Freedman2 , Jesse W. Rowley1
1. Program in Molecular Medicine, University of Utah School of Medicine, Salt Lake City, UT 2. Boston University School of Medicine
BACKGROUND Compounding the obesity epidemic are the associated risks and diseases that contribute to the morbidity and mortality of the affected individuals. Of note, obesity increases the risk of a thrombotic event, in which clots are formed from platelets that can lead to life-threatening emergencies.1 While clotting is normal and necessary to maintain hemostasis, hyper-reactive platelet activity can be detrimental. It is known that mitochondrial function regulates platelet reactivity. Furthermore, mitochondrial metabolism is altered in metabolic syndrome. To maintain normal mitochondrial function, mitochondria undergo processes of fusion, in which two separate mitochondria come together to share DNA, proteins, and metabolites.2 Mitofusin 2 (MFN2), a GTPase, assists in fusing two mitochondria together, and its absence is associated with metabolic and neurodegenerative diseases.3,4,5 Platelets express a novel isoform of MFN2 that is associated with platelet counts9. Whether MFN2 regulates mitochondrial function in megakaryocytes and platelets, and whether MFN2 expression is related to platelet reactivity in metabolic syndrome is not known.
Figure 1. Relative MFN2 platelet expression stratified by obesity status on offspring 8 participants in the Framingham Heart Study (N=1819) A. Demographics of individuals used from Mfn2 RNA expression analysis. B. Mfn2 RNA expression in platelets. Individuals with BMI<25 are the referent category. The fold-change (and 95% confidence interval) associated with being overweight or obese estimated from multivariable adjusted models are presented. MFN2 expression in obese individuals was 1.16-fold (1.02-1.34, p=0.02) higher than normal weight individuals and 1.15-fold (1.02-1.28, p=0.02) higher than overweight individuals. There was no difference in MFN2 expression in overweight relative to normal-weight individuals (1.02 (0.90-1.15), p=0.8).
RESULTS
Figure 2. Assessment of both known and novel isoforms of platelet MFN2 mRNA in platelets from obese human subjects (HO) matched with lean control human subjects (HL) using real-time PCR (qPCR). A. Normal isoform of MFN2 exon found in most cells. B. Novel isoform of MFN2 found specifically in platelets.
SUMMARY Both Mfn2 known and platelet specific isoforms are potentially increased in platelets from obese subjects. Mfn2 plays a role in megakaryocyte morphology, but this was not observed in platelets. In this experiment, there were no significant changes in mitochondrial DNA load (for WT n=6, KO n=4), however, future tests need to be done. There was also no significant observed change in mitochondrial damage between WT and KO murine platelets. References Santilli, F, Vazzana, N, Liani, R, Guagnano, M, Davì, G. "Platelet Activation In Obesity And Metabolic Syndrome." Obesity Reviews 13.1 (2012): 27-42. Academic Search Premier. Web. 25 Jan. 2016. Hall, A. R., et al. "Mitochondrial fusion and fission proteins: novel therapeutic targets for combating cardiovascular disease." British journal of pharmacology 171.8 (2014): 1890-1906. Chen H, Detmer SA, Ewald AJ, Griffin EE, Fraser SE, Chan DC. (2003). Mitofusins MFN1 and Mfn2 coordinately regulate mitochondrial fusion and are essential for embryonic development. J Cell Biol 160: 189–200. Zuchner S, Mersiyanova IV, Muglia M, Bissar-Tadmouri N, Rochelle. J, Dadali EL et al. (2004). Mutations in the mitochondrial GTPase mitofusin 2 cause Charcot-Marie-Tooth neuropathy type 2A. Nat Genet 36: 449–451. Baloh, Robert H., et al. "Altered axonal mitochondrial transport in the pathogenesis of Charcot-Marie-Tooth disease from mitofusin 2 mutations."The Journal of neuroscience 27.2 (2007): 422-430. Nicholaos Kakouros, Jeffrey J. Rade, Antonios Kourliouros, Jon R. Resar. “Platelet Function in Patients with Diabetes Mellitus: From a Theoretical to a Practical Perspective.” International Journal of Endocrinology. Vol. 2011. Web 25 Jan. 2016. http://www.hindawi.com/journals/ije/2011/742719. Guthikonda, Sasidhar, et al. "Role of reticulated platelets and platelet size heterogeneity on platelet activity after dual antiplatelet therapy with aspirin and clopidogrel in patients with stable coronary artery disease." Journal of the American College of Cardiology 52.9 (2008): 743-749. Furda, Amy, et al. “Quantiative PCR-Based Measurement of Nuclear and Mitochondrial DNA Damage and Repair in Mammalian Cells.” Methods Mol Biol. 2014; 1105: 419-437. Simon et al. “Integrative Multi-omic Analysis of Human Platelet eQTLs Reveals Alternative Start Site in Mitofusin 2.” The American Journal of Human Genetics. 2016. http://dx.doi.org/10.1016/j.ajhg.2016.03.007.
Variable Sample Size 1819 Female Sex, n(%) 993 (51) Age, y 66.9±8.6 BMI, kg/m2 28.3±5.3
-6
-4
-2
0
2
4
6
8
10
12
HL HO
Ct (
Avg
Ct -
Avg
Btu
bbC
t)
Min Outlier Max Outlier
Figure 3. Mitochondrial morphology in Mfn2 WT and KO megakaryocytes. Using the Evos Cell Imaging System, we captured in real time fused and non-fused mitochondria in MFN2 WT and KO mouse megakaryocytes and platelets. A through C: Wild type MFN2 megakaryocyte displaying fused mitochondria. D through F: Knockout MFN2 megakaryocyte displaying punctate mitochondria. G. Images from Evo Cell Imaging System were validated with lab members who were blinded and asked to rate 14 images at three different times to determine whether mitochondria were punctate or fused (1=fused; 10=punctate).
A. B.
-6
-4
-2
0
2
4
6
8
10
12
HL HO
Ct (
Avg
Ct -
Avg
Btu
bb C
t)
Min Outlier Max Outlier
A.
B.
C.
D.
E.
F.
Figure 4. Mitochondrial morphology in platelets. A. Wild type MFN2 platelets. B. Knockout MFN2 platelets.
B. A.
Figure 5. Analysis of mitochondrial DNA levels and mitochondrial DNA damage in Mfn2 KO and WT platelets. To assess changes in mitochondrial DNA load and mitochondrial damage, we used quantitative PCR (QPCR) in MFN2 KO versus WT murine platelets and used ImageJ to quantify the pixels from the image of the gel electrophoresis (seen in Fig 1). We normalized mitochondrial copy number by using real time PCR (qPCR) to amplify short fragments (less than 300 bp) of the mitochondrial gene. In Furda, et al, it was suggested that the probability of amplifying such short bps will produce only undamaged DNA.8 We then monitored copy number of the mitochondrial genome by comparing large fragments obtained from QPCR on the principle that DNA lesions can slow down or block the construction of product and DNA with fewer lesions will amplify in QPCR more than damaged DNA.8 A. QPCR on electrophoresis gel. Pixels quantified by ImageJ as shown in C. Real time PCR threshold counts of WT and KO murine platelets. C. Quantitative PCR of WT and KO murine platelets
0
1
2
3
4
5
6
7
8
9
10
WT KO
Min Outlier Max Outlier
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
Pixe
ls as
mea
sure
d by
Imag
eJ
QPCR Gel Electrophores
WTKO
0
2
4
6
8
10
12
14
WT KO
Aver
age
2^-C
tavg
#*1
E6
Real time PCR 2-Ct(avg)*1E6
G.
C.
A.
B.
A.
B.
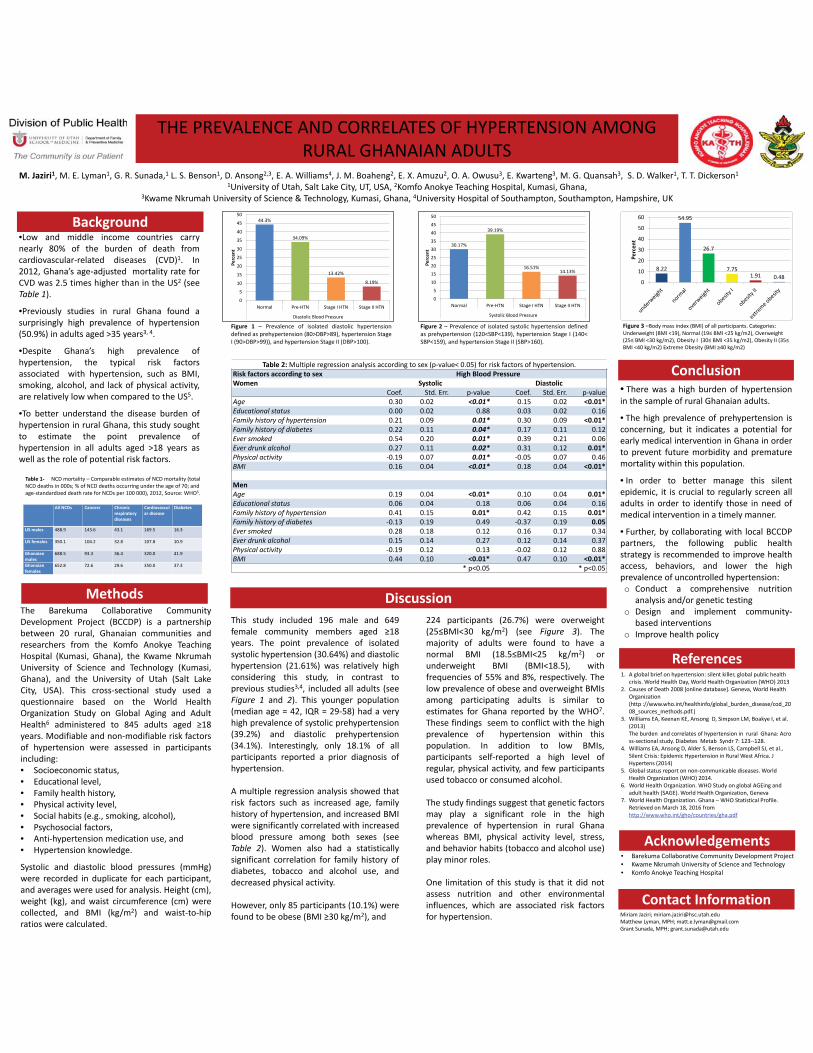
M. Jaziri1, M. E. Lyman1, G. R. Sunada,1 L. S. Benson1, D. Ansong2,3, E. A. Williams4, J. M. Boaheng2, E. X. Amuzu2, O. A. Owusu3, E. Kwarteng3, M. G. Quansah3, S. D. Walker1, T. T. Dickerson1
1University of Utah, Salt Lake City, UT, USA, 2Komfo Anokye Teaching Hospital, Kumasi, Ghana, 3Kwame Nkrumah University of Science & Technology, Kumasi, Ghana, 4University Hospital of Southampton, Southampton, Hampshire, UK
•Low and middle income countries carrynearly 80% of the burden of death fromcardiovascular-related diseases (CVD)1. In2012, Ghana’s age-adjusted mortality rate forCVD was 2.5 times higher than in the US2 (seeTable 1).
•Previously studies in rural Ghana found asurprisingly high prevalence of hypertension(50.9%) in adults aged >35 years3, 4.
•Despite Ghana’s high prevalence ofhypertension, the typical risk factorsassociated with hypertension, such as BMI,smoking, alcohol, and lack of physical activity,are relatively low when compared to the US5.
•To better understand the disease burden ofhypertension in rural Ghana, this study soughtto estimate the point prevalence ofhypertension in all adults aged >18 years aswell as the role of potential risk factors.
Background
MethodsThe Barekuma Collaborative CommunityDevelopment Project (BCCDP) is a partnershipbetween 20 rural, Ghanaian communities andresearchers from the Komfo Anokye TeachingHospital (Kumasi, Ghana), the Kwame NkrumahUniversity of Science and Technology (Kumasi,Ghana), and the University of Utah (Salt LakeCity, USA). This cross-sectional study used aquestionnaire based on the World HealthOrganization Study on Global Aging and AdultHealth6 administered to 845 adults aged 18years. Modifiable and non-modifiable risk factorsof hypertension were assessed in participantsincluding:• Socioeconomic status,• Educational level,• Family health history,• Physical activity level,• Social habits (e.g., smoking, alcohol),• Psychosocial factors,• Anti-hypertension medication use, and• Hypertension knowledge.
Systolic and diastolic blood pressures (mmHg)were recorded in duplicate for each participant,and averages were used for analysis. Height (cm),weight (kg), and waist circumference (cm) werecollected, and BMI (kg/m2) and waist-to-hipratios were calculated.
• There was a high burden of hypertensionin the sample of rural Ghanaian adults.
• The high prevalence of prehypertension isconcerning, but it indicates a potential forearly medical intervention in Ghana in orderto prevent future morbidity and prematuremortality within this population.
• In order to better manage this silentepidemic, it is crucial to regularly screen alladults in order to identify those in need ofmedical intervention in a timely manner.
• Further, by collaborating with local BCCDPpartners, the following public healthstrategy is recommended to improve healthaccess, behaviors, and lower the highprevalence of uncontrolled hypertension:o Conduct a comprehensive nutrition
analysis and/or genetic testingo Design and implement community-
based interventionso Improve health policy
Conclusion
1. A global brief on hypertension: silent killer, global public health crisis. World Health Day, World Health Organization (WHO) 2013
2. Causes of Death 2008 [online database]. Geneva, World Health Organization
3. Williams EA, Keenan KE, Ansong D, Simpson LM, Boakye I, et al. (2013) The burden and correlates of hypertension in rural Ghana: Across-sectional study. Diabetes Metab Syndr 7: 123--128.
4. Williams EA, Ansong D, Alder S, Benson LS, Campbell SJ, et al., Silent Crisis: Epidemic Hypertension in Rural West Africa. J Hypertens (2014)
5. Global status report on non-communicable diseases. World Health Organization (WHO) 2014.
6. World Health Organization. WHO Study on global AGEing and adult health (SAGE). World Health Organization, Geneva
7. World Health Organization. Ghana – WHO Statistical Profile. Retrieved on March 18, 2016 from http://www.who.int/gho/countries/gha.pdf
References
• Barekuma Collaborative Community Development Project• Kwame Nkrumah University of Science and Technology• Komfo Anokye Teaching Hospital
Acknowledgements
Miriam Jaziri; [email protected] Lyman, MPH; [email protected] Sunada, MPH; [email protected]
Contact Information
THE PREVALENCE AND CORRELATES OF HYPERTENSION AMONG RURAL GHANAIAN ADULTS
Figure 3 –Body mass index (BMI) of all participants. Categories: Underweight (BMI <19), Normal (19 kg/m2), Overweight ( (30BMI <40 kg/m2) Extreme Obesity ( 0 kg/m2)
Figure 2 – Prevalence of isolated systolic hypertension definedas prehypertension (120<SBP<139), hypertension Stage I (140<SBP<159), and hypertension Stage II (SBP>160).
44.3%
34.09%
13.42%
8.19%
0
5
10
15
20
25
30
35
40
45
50
Normal Pre-HTN Stage I HTN Stage II HTN
Diastolic Blood Pressure
Perc
ent
30.17%
39.19%
16.51%14.13%
Normal Pre-HTN Stage I HTN Stage II HTN
Systolic Blood Pressure
0
5
10
15
20
25
30
35
40
45
50
Perc
ent
8.22
54.95
26.7
7.751.91 0.48
0
10
20
30
40
50
60
Perc
ent
Figure 1 – Prevalence of isolated diastolic hypertensiondefined as prehypertension (80>DBP>89), hypertension StageI (90>DBP>99)), and hypertension Stage II (DBP>100).
All NCDs Cancers Chronic respiratory diseases
Cardiovascular disease
Diabetes
US males 488.9 143.6 43.1 169.5 16.3
US females 350.1 104.2 32.8 107.8 10.9
Ghanaian males
688.5 93.3 36.4 320.0 41.9
Ghanaian females
652.8 72.6 29.6 350.0 37.3
Table 1- NCD mortality – Comparable estimates of NCD mortality (total NCD deaths in 000s; % of NCD deaths occurring under the age of 70; and age-standardized death rate for NCDs per 100 000), 2012, Source: WHO5.
Table 2: Multiple regression analysis according to sex (p-value< 0.05) for risk factors of hypertension.Risk factors according to sex High Blood PressureWomen Systolic Diastolic
Coef. Std. Err. p-value Coef. Std. Err. p-valueAge 0.30 0.02 <0.01* 0.15 0.02 <0.01*Educational status 0.00 0.02 0.88 0.03 0.02 0.16Family history of hypertension 0.21 0.09 0.01* 0.30 0.09 <0.01*Family history of diabetes 0.22 0.11 0.04* 0.17 0.11 0.12Ever smoked 0.54 0.20 0.01* 0.39 0.21 0.06Ever drunk alcohol 0.27 0.11 0.02* 0.31 0.12 0.01*Physical activity -0.19 0.07 0.01* -0.05 0.07 0.46BMI 0.16 0.04 <0.01* 0.18 0.04 <0.01*
MenAge 0.19 0.04 <0.01* 0.10 0.04 0.01*Educational status 0.06 0.04 0.18 0.06 0.04 0.16Family history of hypertension 0.41 0.15 0.01* 0.42 0.15 0.01*Family history of diabetes -0.13 0.19 0.49 -0.37 0.19 0.05Ever smoked 0.28 0.18 0.12 0.16 0.17 0.34Ever drunk alcohol 0.15 0.14 0.27 0.12 0.14 0.37Physical activity -0.19 0.12 0.13 -0.02 0.12 0.88BMI 0.44 0.10 <0.01* 0.47 0.10 <0.01*
* p<0.05 * p<0.05
This study included 196 male and 649female community members aged 18years. The point prevalence of isolatedsystolic hypertension (30.64%) and diastolichypertension (21.61%) was relatively highconsidering this study, in contrast toprevious studies3,4, included all adults (seeFigure 1 and 2). This younger population(median age = 42, IQR = 29-58) had a veryhigh prevalence of systolic prehypertension(39.2%) and diastolic prehypertension(34.1%). Interestingly, only 18.1% of allparticipants reported a prior diagnosis ofhypertension.
A multiple regression analysis showed thatrisk factors such as increased age, familyhistory of hypertension, and increased BMIwere significantly correlated with increasedblood pressure among both sexes (seeTable 2). Women also had a statisticallysignificant correlation for family history ofdiabetes, tobacco and alcohol use, anddecreased physical activity.
However, only 85 participants (10.1%) werefound to be obese (BMI 30 kg/m2), and
Discussion224 participants (26.7%) were overweight(25 30 kg/m2) (see Figure 3). Themajority of adults were found to have anormal BMI (18.5 25 kg/m2) orunderweight BMI (BMI<18.5), withfrequencies of 55% and 8%, respectively. Thelow prevalence of obese and overweight BMIsamong participating adults is similar toestimates for Ghana reported by the WHO7.These findings seem to conflict with the highprevalence of hypertension within thispopulation. In addition to low BMIs,participants self-reported a high level ofregular, physical activity, and few participantsused tobacco or consumed alcohol.
The study findings suggest that genetic factorsmay play a significant role in the highprevalence of hypertension in rural Ghanawhereas BMI, physical activity level, stress,and behavior habits (tobacco and alcohol use)play minor roles.
One limitation of this study is that it did notassess nutrition and other environmentalinfluences, which are associated risk factorsfor hypertension.
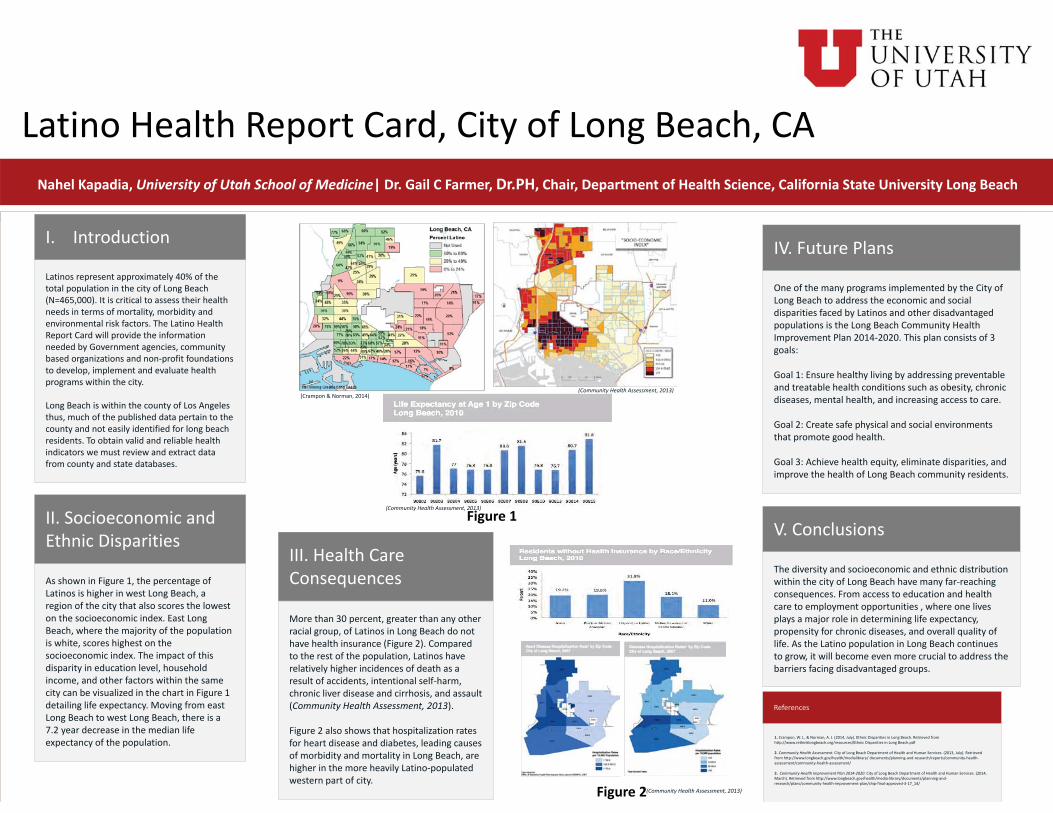
Latinos represent approximately 40% of the total population in the city of Long Beach (N=465,000). It is critical to assess their health needs in terms of mortality, morbidity and environmental risk factors. The Latino Health Report Card will provide the information needed by Government agencies, community based organizations and non-profit foundations to develop, implement and evaluate health programs within the city.
Long Beach is within the county of Los Angeles thus, much of the published data pertain to the county and not easily identified for long beach residents. To obtain valid and reliable health indicators we must review and extract data from county and state databases.
Latino Health Report Card, City of Long Beach, CANahel Kapadia, University of Utah School of Medicine| Dr. Gail C Farmer, Dr.PH, Chair, Department of Health Science, California State University Long Beach
As shown in Figure 1, the percentage of Latinos is higher in west Long Beach, a region of the city that also scores the lowest on the socioeconomic index. East Long Beach, where the majority of the population is white, scores highest on the socioeconomic index. The impact of this disparity in education level, household income, and other factors within the same city can be visualized in the chart in Figure 1 detailing life expectancy. Moving from east Long Beach to west Long Beach, there is a 7.2 year decrease in the median life expectancy of the population.
More than 30 percent, greater than any other racial group, of Latinos in Long Beach do not have health insurance (Figure 2). Compared to the rest of the population, Latinos have relatively higher incidences of death as a result of accidents, intentional self-harm, chronic liver disease and cirrhosis, and assault (Community Health Assessment, 2013).
Figure 2 also shows that hospitalization rates for heart disease and diabetes, leading causes of morbidity and mortality in Long Beach, are higher in the more heavily Latino-populated western part of city.
One of the many programs implemented by the City of Long Beach to address the economic and social disparities faced by Latinos and other disadvantaged populations is the Long Beach Community Health Improvement Plan 2014-2020. This plan consists of 3 goals:
Goal 1: Ensure healthy living by addressing preventable and treatable health conditions such as obesity, chronic diseases, mental health, and increasing access to care.
Goal 2: Create safe physical and social environments that promote good health.
Goal 3: Achieve health equity, eliminate disparities, and improve the health of Long Beach community residents.
Figure 1
Figure 2
I. Introduction
II. Socioeconomic and Ethnic Disparities
III. Health Care Consequences
IV. Future Plans
V. Conclusions
The diversity and socioeconomic and ethnic distribution within the city of Long Beach have many far-reaching consequences. From access to education and health care to employment opportunities , where one lives plays a major role in determining life expectancy, propensity for chronic diseases, and overall quality of life. As the Latino population in Long Beach continues to grow, it will become even more crucial to address the barriers facing disadvantaged groups.
References
1. Crampon, W. J., & Norman, A. J. (2014, July). Ethnic Disparities in Long Beach. Retrieved from http://www.rethinklongbeach.org/resources/Ethnic Disparities in Long Beach.pdf
2. Community Health Assessment. City of Long Beach Department of Health and Human Services. (2013, July). Retrieved from http://www.longbeach.gov/health/medialibrary/ documents/planning-and-research/reports/community-health-assessment/community-health-assessment/
3. Community Health Improvement Plan 2014-2020. City of Long Beach Department of Health and Human Services. (2014, March). Retrieved from http://www.longbeach.gov/health/media-library/documents/planning-and-research/plans/community-health-improvement-plan/chip-final-approved-3-17_14/
(Crampon & Norman, 2014)
(Community Health Assessment, 2013)
(Community Health Assessment, 2013)
(Community Health Assessment, 2013)
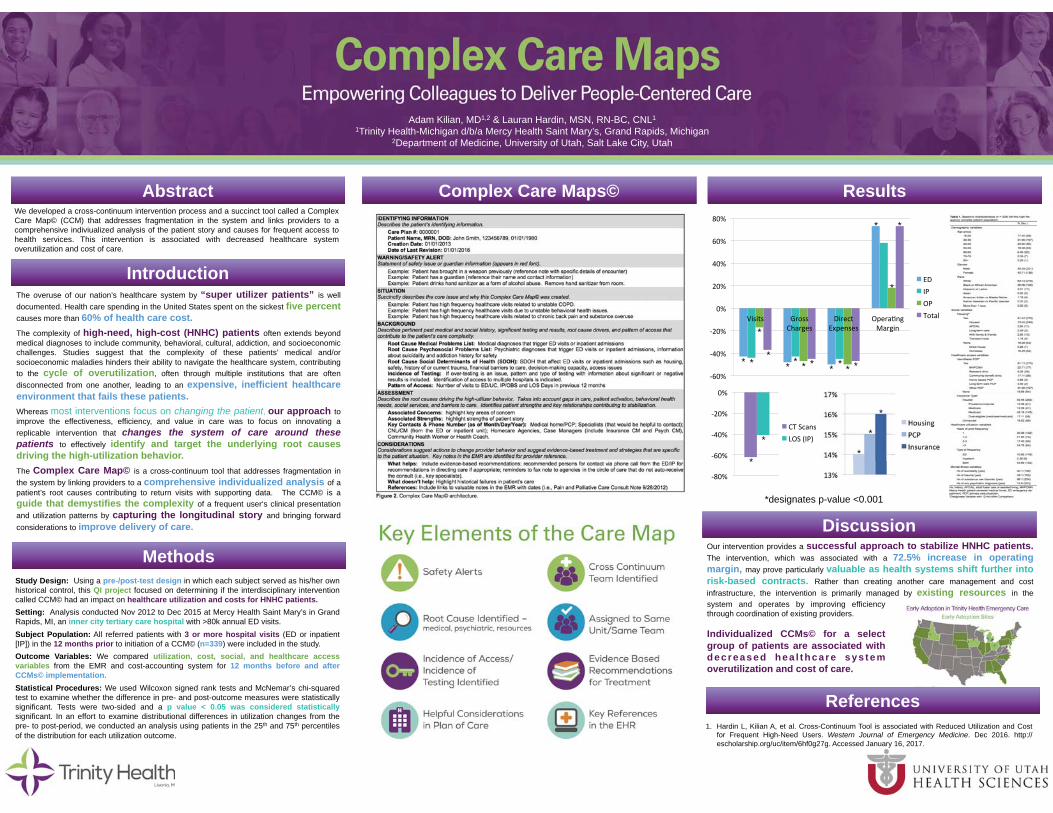
1. Hardin L, Kilian A, et al. Cross-Continuum Tool is associated with Reduced Utilization and Cost for Frequent High-Need Users. Western Journal of Emergency Medicine. Dec 2016. http://escholarship.org/uc/item/6hf0g27g. Accessed January 16, 2017.
The overuse of our nation’s healthcare system by “super utilizer patients” is well documented. Health care spending in the United States spent on the sickest five percent causes more than 60% of health care cost. The complexity of high-need, high-cost (HNHC) patients often extends beyond medical diagnoses to include community, behavioral, cultural, addiction, and socioeconomic challenges. Studies suggest that the complexity of these patients’ medical and/or socioeconomic maladies hinders their ability to navigate the healthcare system, contributing to the cycle of overutilization, often through multiple institutions that are often disconnected from one another, leading to an expensive, inefficient healthcare environment that fails these patients. Whereas most interventions focus on changing the patient, our approach to improve the effectiveness, efficiency, and value in care was to focus on innovating a replicable intervention that changes the system of care around these patients to effectively identify and target the underlying root causes driving the high-utilization behavior. The Complex Care Map© is a cross-continuum tool that addresses fragmentation in the system by linking providers to a comprehensive individualized analysis of a patient’s root causes contributing to return visits with supporting data. The CCM© is a guide that demystifies the complexity of a frequent user‘s clinical presentation and utilization patterns by capturing the longitudinal story and bringing forward considerations to improve delivery of care.
Our intervention provides a successful approach to stabilize HNHC patients. The intervention, which was associated with a 72.5% increase in operating margin, may prove particularly valuable as health systems shift further into risk-based contracts. Rather than creating another care management and cost infrastructure, the intervention is primarily managed by existing resources in the healthcare system and operates coordination
We developed a cross-continuum intervention process and a succinct tool called a Complex Care Map© (CCM) that addresses fragmentation in the system and links providers to a comprehensive indiviualized analysis of the patient story and causes for frequent access to health services. This intervention is associated with decreased healthcare system overutilization and cost of care.
Study Design: Using a pre-/post-test design in which each subject served as his/her own historical control, this QI project focused on determining if the interdisciplinary intervention called CCM© had an impact on healthcare utilization and costs for HNHC patients. Setting: Analysis conducted Nov 2012 to Dec 2015 at Mercy Health Saint Mary’s in Grand Rapids, MI, an inner city tertiary care hospital with >80k annual ED visits. Subject Population: All referred patients with 3 or more hospital visits (ED or inpatient [IP]) in the 12 months prior to initiation of a CCM© (n=339) were included in the study. Outcome Variables: We compared utilization, cost, social, and healthcare access variables from the EMR and cost-accounting system for 12 months before and after CCMs© implementation. Statistical Procedures: We used Wilcoxon signed rank tests and McNemar’s chi-squared test to examine whether the difference in pre- and post-outcome measures were statistically significant. Tests were two-sided and a p value < 0.05 was considered statistically significant. In an effort to examine distributional differences in utilization changes from the pre- to post-period, we conducted an analysis using patients in the 25th and 75th percentiles of the distribution for each utilization outcome.
Abstract
Introduction
Methods
Results
Discussion
References
Complex Care Maps©
Adam Kilian, MD1,2 & Lauran Hardin, MSN, RN-BC, CNL1 1Trinity Health-Michigan d/b/a Mercy Health Saint Mary’s, Grand Rapids, Michigan
2Department of Medicine, University of Utah, Salt Lake City, Utah
* * * * * * * *
*
*
* * *
*designates p-value <0.001
*
*
*
*
* *
*
system and operates by improving efficiency through coordination of existing providers. Individualized CCMs© for a select group of patients are associated with decreased hea l thcare sys tem overutilization and cost of care.
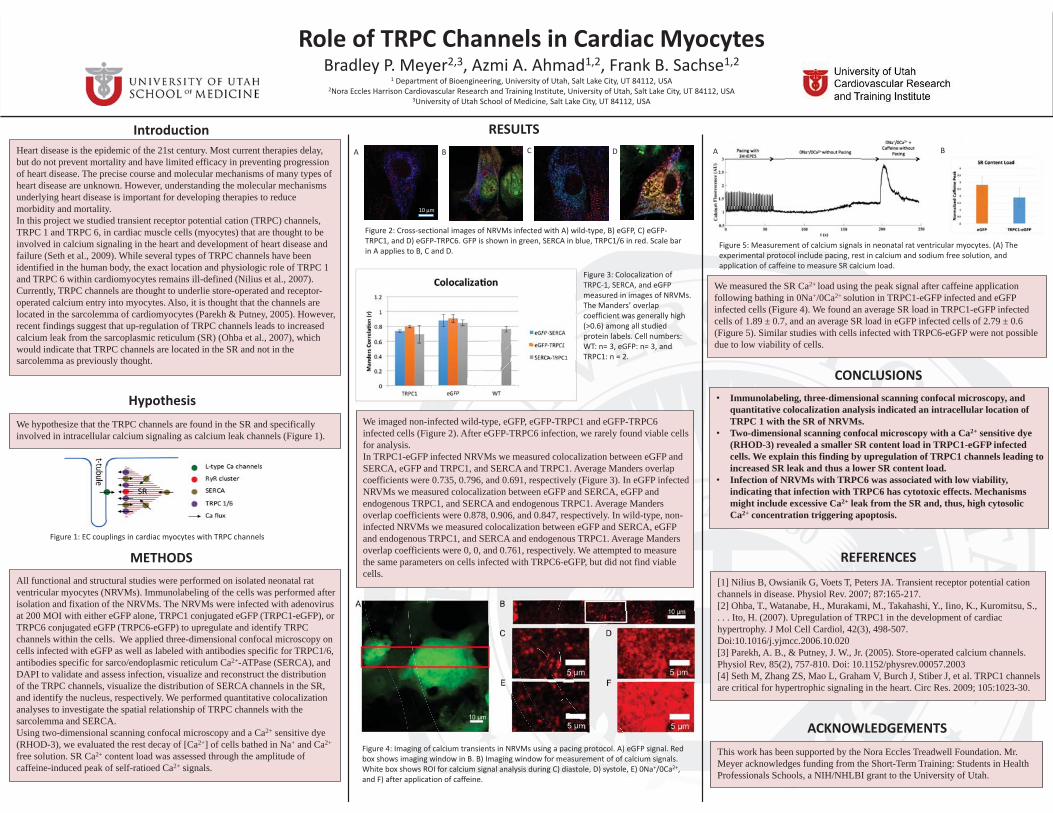
Role of TRPC Channels in Cardiac MyocytesBradley P. Meyer2,3, Azmi A. Ahmad1,2, Frank B. Sachse1,2
1 Department of Bioengineering, University of Utah, Salt Lake City, UT 84112, USA2Nora Eccles Harrison Cardiovascular Research and Training Institute, University of Utah, Salt Lake City, UT 84112, USA
3University of Utah School of Medicine, Salt Lake City, UT 84112, USA
Introduction RESULTSHeart disease is the epidemic of the 21st century. Most current therapies delay, but do not prevent mortality and have limited efficacy in preventing progression of heart disease. The precise course and molecular mechanisms of many types of heart disease are unknown. However, understanding the molecular mechanisms underlying heart disease is important for developing therapies to reduce morbidity and mortality. In this project we studied transient receptor potential cation (TRPC) channels, TRPC 1 and TRPC 6, in cardiac muscle cells (myocytes) that are thought to be involved in calcium signaling in the heart and development of heart disease and failure (Seth et al., 2009). While several types of TRPC channels have been identified in the human body, the exact location and physiologic role of TRPC 1 and TRPC 6 within cardiomyocytes remains ill-defined (Nilius et al., 2007). Currently, TRPC channels are thought to underlie store-operated and receptor-operated calcium entry into myocytes. Also, it is thought that the channels are located in the sarcolemma of cardiomyocytes (Parekh & Putney, 2005). However, recent findings suggest that up-regulation of TRPC channels leads to increased calcium leak from the sarcoplasmic reticulum (SR) (Ohba et al., 2007), which would indicate that TRPC channels are located in the SR and not in the sarcolemma as previously thought.
HypothesisWe hypothesize that the TRPC channels are found in the SR and specifically involved in intracellular calcium signaling as calcium leak channels (Figure 1).
METHODSAll functional and structural studies were performed on isolated neonatal rat ventricular myocytes (NRVMs). Immunolabeling of the cells was performed after isolation and fixation of the NRVMs. The NRVMs were infected with adenovirus at 200 MOI with either eGFP alone, TRPC1 conjugated eGFP (TRPC1-eGFP), or TRPC6 conjugated eGFP (TRPC6-eGFP) to upregulate and identify TRPC channels within the cells. We applied three-dimensional confocal microscopy on cells infected with eGFP as well as labeled with antibodies specific for TRPC1/6, antibodies specific for sarco/endoplasmic reticulum Ca2+-ATPase (SERCA), and DAPI to validate and assess infection, visualize and reconstruct the distribution of the TRPC channels, visualize the distribution of SERCA channels in the SR, and identify the nucleus, respectively. We performed quantitative colocalization analyses to investigate the spatial relationship of TRPC channels with the sarcolemma and SERCA. Using two-dimensional scanning confocal microscopy and a Ca2+ sensitive dye (RHOD-3), we evaluated the rest decay of [Ca2+] of cells bathed in Na+ and Ca2+
free solution. SR Ca2+ content load was assessed through the amplitude of caffeine-induced peak of self-ratioed Ca2+ signals.
We imaged non-infected wild-type, eGFP, eGFP-TRPC1 and eGFP-TRPC6infected cells (Figure 2). After eGFP-TRPC6 infection, we rarely found viable cells for analysis.In TRPC1-eGFP infected NRVMs we measured colocalization between eGFP andSERCA, eGFP and TRPC1, and SERCA and TRPC1. Average Manders overlap coefficients were 0.735, 0.796, and 0.691, respectively (Figure 3). In eGFP infected NRVMs we measured colocalization between eGFP and SERCA, eGFP andendogenous TRPC1, and SERCA and endogenous TRPC1. Average Mandersoverlap coefficients were 0.878, 0.906, and 0.847, respectively. In wild-type, non-infected NRVMs we measured colocalization between eGFP and SERCA, eGFPand endogenous TRPC1, and SERCA and endogenous TRPC1. Average Mandersoverlap coefficients were 0, 0, and 0.761, respectively. We attempted to measure the same parameters on cells infected with TRPC6-eGFP, but did not find viable cells.
CONCLUSIONSImmunolabeling, three-dimensional scanning confocal microscopy, and quantitative colocalization analysis indicated an intracellular location of TRPC 1 with the SR of NRVMs. Two-dimensional scanning confocal microscopy with a Ca2+ sensitive dye (RHOD-3) revealed a smaller SR content load in TRPC1-eGFP infected cells. We explain this finding by upregulation of TRPC1 channels leading to increased SR leak and thus a lower SR content load. Infection of NRVMs with TRPC6 was associated with low viability, indicating that infection with TRPC6 has cytotoxic effects. Mechanisms might include excessive Ca2+ leak from the SR and, thus, high cytosolic Ca2+ concentration triggering apoptosis.
REFERENCES[1] Nilius B, Owsianik G, Voets T, Peters JA. Transient receptor potential cation channels in disease. Physiol Rev. 2007; 87:165-217.[2] Ohba, T., Watanabe, H., Murakami, M., Takahashi, Y., Iino, K., Kuromitsu, S., . . . Ito, H. (2007). Upregulation of TRPC1 in the development of cardiac hypertrophy. J Mol Cell Cardiol, 42(3), 498-507.Doi:10.1016/j.yjmcc.2006.10.020[3] Parekh, A. B., & Putney, J. W., Jr. (2005). Store-operated calcium channels. Physiol Rev, 85(2), 757-810. Doi: 10.1152/physrev.00057.2003[4] Seth M, Zhang ZS, Mao L, Graham V, Burch J, Stiber J, et al. TRPC1 channels are critical for hypertrophic signaling in the heart. Circ Res. 2009; 105:1023-30.
This work has been supported by the Nora Eccles Treadwell Foundation. Mr. Meyer acknowledges funding from the Short-Term Training: Students in Health Professionals Schools, a NIH/NHLBI grant to the University of Utah.
ACKNOWLEDGEMENTS
We measured the SR Ca2+ load using the peak signal after caffeine application following bathing in 0Na+/0Ca2+ solution in TRPC1-eGFP infected and eGFP infected cells (Figure 4). We found an average SR load in TRPC1-eGFP infected cells of 1.89 ± 0.7, and an average SR load in eGFP infected cells of 2.79 ± 0.6 (Figure 5). Similar studies with cells infected with TRPC6-eGFP were not possible due to low viability of cells.
Figure 1: EC couplings in cardiac myocytes with TRPC channels
Figure 3: Colocalization of TRPC-1, SERCA, and eGFPmeasured in images of NRVMs. The Manders’ overlap coefficient was generally high (>0.6) among all studied protein labels. Cell numbers: WT: n= 3, eGFP: n= 3, and TRPC1: n = 2.
Figure 5: Measurement of calcium signals in neonatal rat ventricular myocytes. (A) The experimental protocol include pacing, rest in calcium and sodium free solution, and application of caffeine to measure SR calcium load.
Figure 4: Imaging of calcium transients in NRVMs using a pacing protocol. A) eGFP signal. Red box shows imaging window in B. B) Imaging window for measurement of of calcium signals. White box shows ROI for calcium signal analysis during C) diastole, D) systole, E) 0Na+/0Ca2+, and F) after application of caffeine.
10 μm
A B C D A B
Figure 2: Cross-sectional images of NRVMs infected with A) wild-type, B) eGFP, C) eGFP-TRPC1, and D) eGFP-TRPC6. GFP is shown in green, SERCA in blue, TRPC1/6 in red. Scale bar in A applies to B, C and D.
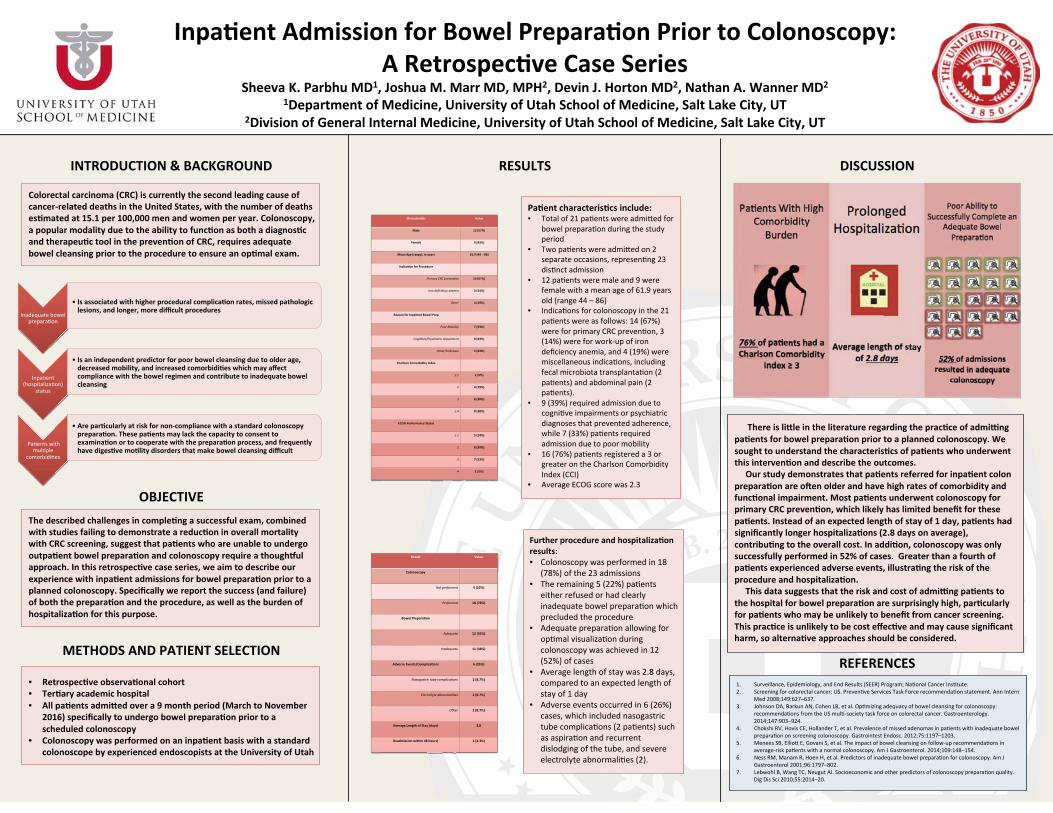
• • •
•
•
•
•
•
•
•
•
•
•
•
•
•
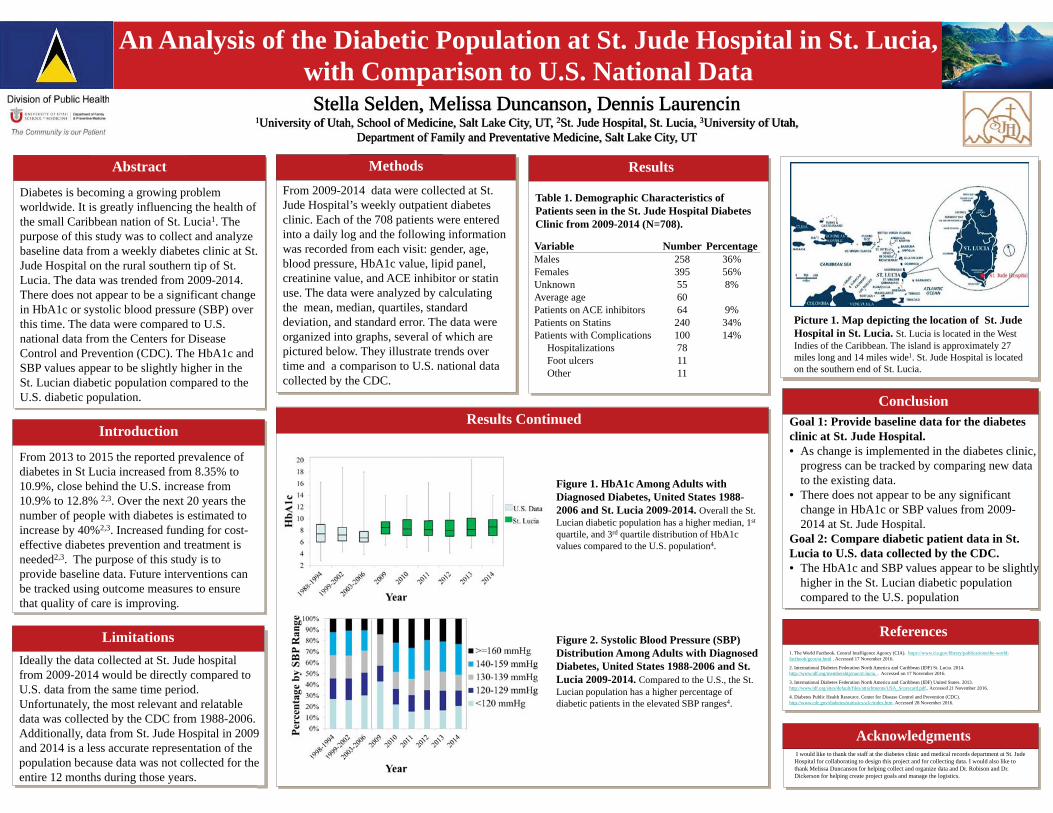
An Analysis of the Diabetic Population at St. Jude Hospital in St. Lucia, with Comparison to U.S. National DatapStella Selden, Melissa Duncanson, Dennis Laurencin
1University of Utah, School of Medicine, Salt Lake City, UT, 2St. Jude Hospital, St. Lucia, 3University of Utah, Department of Family and Preventative Medicine, Salt Lake City, UT
LIMITATIONS
METHODSFrom 2009-2014 data were collected at St. Jude Hospital’s weekly outpatient diabetes clinic. Each of the 708 patients were entered into a daily log and the following information was recorded from each visit: gender, age, blood pressure, HbA1c value, lipid panel, creatinine value, and ACE inhibitor or statin use. The data were analyzed by calculating the mean, median, quartiles, standard deviation, and standard error. The data were organized into graphs, several of which are pictured below. They illustrate trends over time and a comparison to U.S. national data collected by the CDC.
ACKNOKLEDGMENTSI would like to thank the staff at the diabetes clinic and medical records department at St. Jude
Hospital for collaborating to design this project and for collecting data. I would also like to thank Melissa Duncanson for helping collect and organize data and Dr. Robison and Dr. Dickerson for helping create project goals and manage the logistics.
ABSTRACTDiabetes is becoming a growing problem worldwide. It is greatly influencing the health of the small Caribbean nation of St. Lucia1. The purpose of this study was to collect and analyze baseline data from a weekly diabetes clinic at St. Jude Hospital on the rural southern tip of St. Lucia. The data was trended from 2009-2014. There does not appear to be a significant change in HbA1c or systolic blood pressure (SBP) over this time. The data were compared to U.S. national data from the Centers for Disease Control and Prevention (CDC). The HbA1c and SBP values appear to be slightly higher in the St. Lucian diabetic population compared to the U.S. diabetic population.
Picture 1. Map depicting the location of St. Jude Hospital in St. Lucia. St. Lucia is located in the WestIndies of the Caribbean. The island is approximately 27 miles long and 14 miles wide1. St. Jude Hospital is located on the southern end of St. Lucia.
Figure 1. HbA1c Among Adults with Diagnosed Diabetes, United States 1988-2006 and St. Lucia 2009-2014. Overall the St. Lucian diabetic population has a higher median, 1st
quartile, and 3rd quartile distribution of HbA1c values compared to the U.S. population4.
Figure 2. Systolic Blood Pressure (SBP) Distribution Among Adults with Diagnosed Diabetes, United States 1988-2006 and St. Lucia 2009-2014. Compared to the U.S., the St. Lucian population has a higher percentage of diabetic patients in the elevated SBP ranges4.
Goal 1: Provide baseline data for the diabetes clinic at St. Jude Hospital. • As change is implemented in the diabetes clinic,
progress can be tracked by comparing new data to the existing data.
• There does not appear to be any significant change in HbA1c or SBP values from 2009-2014 at St. Jude Hospital.
Goal 2: Compare diabetic patient data in St. Lucia to U.S. data collected by the CDC. • The HbA1c and SBP values appear to be slightly
higher in the St. Lucian diabetic population compared to the U.S. population
INTRODUCTIONFrom 2013 to 2015 the reported prevalence of diabetes in St Lucia increased from 8.35% to 10.9%, close behind the U.S. increase from 10.9% to 12.8% 2,3. Over the next 20 years the number of people with diabetes is estimated to increase by 40%2,3. Increased funding for cost-effective diabetes prevention and treatment is needed2,3. The purpose of this study is to provide baseline data. Future interventions can be tracked using outcome measures to ensure that quality of care is improving.
1. The World Factbook. Central Intelligence Agency (CIA). https://www.cia.gov/library/publications/the-world-factbook/geos/st.html . Accessed 17 November 2016.
2. International Diabetes Federation North America and Caribbean (IDF) St. Lucia. 2014. http://www.idf.org/membership/nac/st-lucia. . Accessed on 17 November 2016.
3. International Diabetes Federation North America and Caribbean (IDF) United States. 2013. http://www.idf.org/sites/default/files/attachments/USA_Scorecard.pdf.. Accessed 21 November 2016.
4. Diabetes Public Health Resource. Center for Disease Control and Prevention (CDC). http://www.cdc.gov/diabetes/statistics/a1c/index.htm. Accessed 28 November 2016.
RESULTS
Table 1. Demographic Characteristics of Patients seen in the St. Jude Hospital Diabetes Clinic from 2009-2014 (N=708).
Variable Number PercentageMales 258 36%Females 395 56%Unknown 55 8%Average age 60Patients on ACE inhibitors 64 9%Patients on Statins 240 34%Patients with Complications 100 14%
Hospitalizations 78Foot ulcers 11Other 11
Ideally the data collected at St. Jude hospital from 2009-2014 would be directly compared to U.S. data from the same time period. Unfortunately, the most relevant and relatable data was collected by the CDC from 1988-2006. Additionally, data from St. Jude Hospital in 2009 and 2014 is a less accurate representation of the population because data was not collected for the entire 12 months during those years.
Abstract Methods Results
Conclusion
Introduction
Limitations
Results Continued
References
Acknowledgments

Colon Pathology Characteristics in Li-Fraumeni Syndrome: Age and Size Don’t Matter
Hailey M. Shepherd1, William Rengifo-Cam MD2, Wendy Kohlmann MS, CGC3, Joshua D. Schiffman MD3, Kory Jasperson MS, CGC3,Jewel Samadder MD4, Wade Samowitz MD5, S. Tripp5 MD, Randall
Burt MD3,4
University of Utah Medical School1, Jupiter Medical Center2, University of Utah Huntsman Cancer Institute3, University of Utah Division of Gastroenterology4, University of Utah Department of Pathology5
INTRODUCTIONEarly onset colon cancer has been describedas a component of LFS, and currentguidelines recommend colonoscopyscreening begin at age 25 and repeat every 2to 5 years in patients with LFS. Earlydetection is key for preventative treatment inthese patients, yet guidelines for colorectalscreening have not yet been evaluated in thispopulation. To our knowledge, no prior studyhas yet to extensively detail thecharacteristics of the lesions found duringscreening colonoscopy in LFS patientsregarding number, size, location, histology,and genotype/phenotype associations.
METHODSParticipants were identified from theIRB approved Cancer Genetics Studyprotocol at Huntsman Cancer Institute.All participants had a confirmedpathogenic TP53 variant.Medical records were reviewed todetermine the number of polyps, ageat colonoscopy, histologic features ofpolyps [tubular adenoma (TA), sessileserrated polyps (SSP), hyperplasticpolyps (HP), normal or benign colonicmucosa (BCM), and colorectalcancer/high grade dysplasia(CRC/HGD)].
Among 66 confirmed TP53 mutation carriers, 31(47%) individuals underwent a total of 73procedures, 36 (49%) included abnormal findings(Fig 2).
A total of 58 lesions were detected and biopsiedincluding 23 (40%) TA, 5 (9%) SSP, 8 (13%) HP, 12(21%) BCM, and 8 (13%) CRC/HGD.Small TA (2-6 mm) in the descending colon was themost frequent lesion found, while the sigmoid colonwas the most common site for all lesion types.
DISCUSSIONAlthough one patient presented with a significantlylarger CRC lesion (7 cm), all other CRC/HGD lesions(average 6.7 mm) were considerably smaller thanthe 4.5 cm average colon tumor size reported in thegeneral population.
Current guidelines are likely to be insufficient toidentify colon cancers at an early stage because themajority may occur before age 25.
Colonoscopy is an important part of screening for allpatients with LFS, but earlier and more frequentscreening may be necessary for families with ahistory of colon cancer.
ACKNOWLEDGMENTSA special thanks to Wendy Kohlmann and JoshuaSchiffman for input and collaboration with thisproject, as well as the study participants and theGenetic Counseling core facilities supported by P30CA042014 awarded to Huntsman Cancer Institute.
Figure 5: SSA with HGD from LFS participant
High grade dysplasia (200X)
RESULTS
Figure 3: Colonoscopy lesion size in LFS patients
Figure 2: LFS patients receiving colonoscopy
Table 1: Features of CRC/HGD in LFS patients
The most aggressive colon pathologyphenotypes were observed in Del Exon 1,R258W, I125L, and P177R TP53 mutations(Fig. 4).
Figure 4: Distribution of TP53 GermlineMutations in Colorectal lesions
8 CRC/HGD lesions found in 5 patients with amedium size of 13.4 mm (2-70 mm) predominatelyarising from TA (63%)
ABSTRACTThe purpose of this study was to examine thefrequency and characteristics of colon polyps andcolorectal cancer (CRC) in individuals with Li-Fraumeni Syndrome (LFS). LFS is an inheritedcancer predisposition syndrome caused by TP53mutations. LFS is associated with a dramaticallyincreased risk for a spectrum of cancers. Bone andsoft tissue sarcomas, breast cancer, brain tumors,adrenal cortical carcinoma and leukemia have beenclassically associated with this syndrome.Approximately 50% of the individuals carryingmutations in TP53 will develop cancer by the age of30 years, with a lifetime risk of up to 70% in men andalmost 100% in women.

β
ZI ≥5mm) βFrequency CZ CAZ* CTX FOX GM MEM SXT ATM CIP CLPercent of total
Resistant (R) 40 26 38 17 28 0 29 22 22 0
Intermediate (I) 0 3 1 4 5 4 11 2 12 3
Sensitive (S) 0 11 1 19 7 36 0 16 6 37

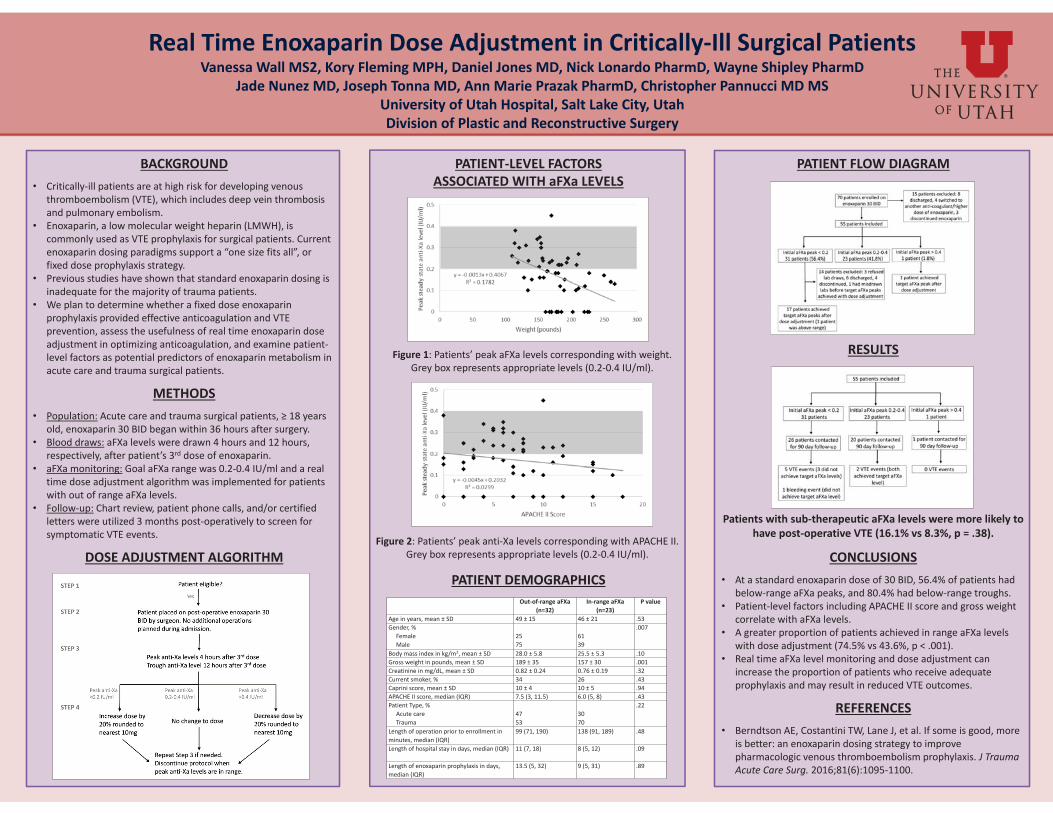
PATIENT-LEVEL FACTORS ASSOCIATED WITH aFXa LEVELS
PATIENT DEMOGRAPHICS
Real Time Enoxaparin Dose Adjustment in Critically-Ill Surgical PatientsVanessa Wall MS2, Kory Fleming MPH, Daniel Jones MD, Nick Lonardo PharmD, Wayne Shipley PharmD
Jade Nunez MD, Joseph Tonna MD, Ann Marie Prazak PharmD, Christopher Pannucci MD MSUniversity of Utah Hospital, Salt Lake City, UtahDivision of Plastic and Reconstructive Surgery
BACKGROUNDCritically-ill patients are at high risk for developing venous thromboembolism (VTE), which includes deep vein thrombosis and pulmonary embolism. Enoxaparin, a low molecular weight heparin (LMWH), is commonly used as VTE prophylaxis for surgical patients. Current enoxaparin dosing paradigms support a “one size fits all”, or fixed dose prophylaxis strategy.Previous studies have shown that standard enoxaparin dosing is inadequate for the majority of trauma patients. We plan to determine whether a fixed dose enoxaparin prophylaxis provided effective anticoagulation and VTE prevention, assess the usefulness of real time enoxaparin dose adjustment in optimizing anticoagulation, and examine patient-level factors as potential predictors of enoxaparin metabolism in acute care and trauma surgical patients.
METHODSPopulation: Acute care and trauma surgical patients, ≥ 18 years old, enoxaparin 30 BID began within 36 hours after surgery. Blood draws: aFXa levels were drawn 4 hours and 12 hours, respectively, after patient’s 3rd dose of enoxaparin.aFXa monitoring: Goal aFXa range was 0.2-0.4 IU/ml and a real time dose adjustment algorithm was implemented for patients with out of range aFXa levels. Follow-up: Chart review, patient phone calls, and/or certified letters were utilized 3 months post-operatively to screen for symptomatic VTE events.
DOSE ADJUSTMENT ALGORITHM
PATIENT FLOW DIAGRAM
RESULTS
Patients with sub-therapeutic aFXa levels were more likely to have post-operative VTE (16.1% vs 8.3%, p = .38).
CONCLUSIONSAt a standard enoxaparin dose of 30 BID, 56.4% of patients had below-range aFXa peaks, and 80.4% had below-range troughs. Patient-level factors including APACHE II score and gross weight correlate with aFXa levels.A greater proportion of patients achieved in range aFXa levels with dose adjustment (74.5% vs 43.6%, p < .001).Real time aFXa level monitoring and dose adjustment can increase the proportion of patients who receive adequate prophylaxis and may result in reduced VTE outcomes.
REFERENCESBerndtson AE, Costantini TW, Lane J, et al. If some is good, more is better: an enoxaparin dosing strategy to improve pharmacologic venous thromboembolism prophylaxis. J Trauma Acute Care Surg. 2016;81(6):1095-1100.
Figure 1: Patients’ peak aFXa levels corresponding with weight. Grey box represents appropriate levels (0.2-0.4 IU/ml).
Figure 2: Patients’ peak anti-Xa levels corresponding with APACHE II. Grey box represents appropriate levels (0.2-0.4 IU/ml).
Out-of-range aFXa(n=32)
In-range aFXa(n=23)
P value
Age in years, mean ± SD 49 ± 15 46 ± 21 .53Gender, %
FemaleMale
2575
6139
.007
Body mass index in kg/m2, mean ± SD 28.0 ± 5.8 25.5 ± 5.3 .10Gross weight in pounds, mean ± SD 189 ± 35 157 ± 30 .001Creatinine in mg/dL, mean ± SD 0.82 ± 0.24 0.76 ± 0.19 .32Current smoker, % 34 26 .43Caprini score, mean ± SD 10 ± 4 10 ± 5 .94APACHE II score, median (IQR) 7.5 (3, 11.5) 6.0 (5, 8) .43Patient Type, %
Acute careTrauma
4753
3070
.22
Length of operation prior to enrollment in minutes, median (IQR)
99 (71, 190) 138 (91, 189) .48
Length of hospital stay in days, median (IQR) 11 (7, 18) 8 (5, 12) .09
Length of enoxaparin prophylaxis in days, median (IQR)
13.5 (5, 32) 9 (5, 31) .89
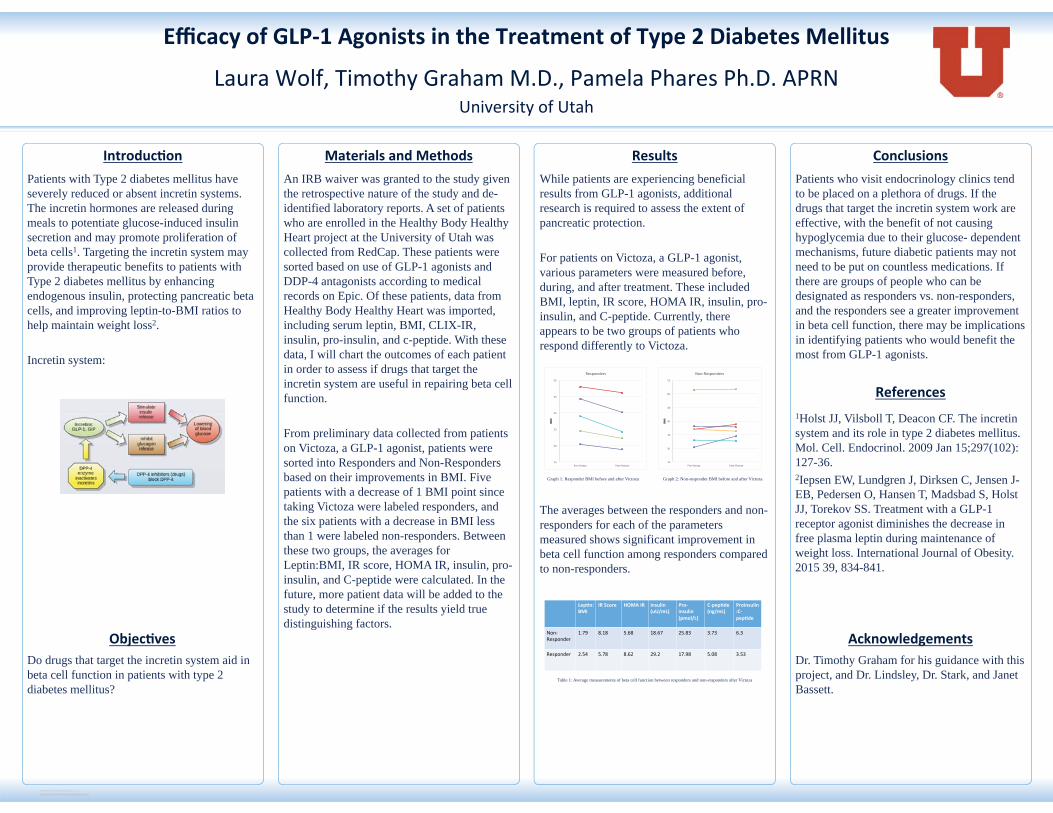
RESEARCH POSTER PRESENTATION DESIGN © 2015
www.PosterPresentations.com
Patients with Type 2 diabetes mellitus have severely reduced or absent incretin systems. The incretin hormones are released during meals to potentiate glucose-induced insulin secretion and may promote proliferation of beta cells1. Targeting the incretin system may provide therapeutic benefits to patients with Type 2 diabetes mellitus by enhancing endogenous insulin, protecting pancreatic beta cells, and improving leptin-to-BMI ratios to help maintain weight loss2. Incretin system:
An IRB waiver was granted to the study given the retrospective nature of the study and de-identified laboratory reports. A set of patients who are enrolled in the Healthy Body Healthy Heart project at the University of Utah was collected from RedCap. These patients were sorted based on use of GLP-1 agonists and DDP-4 antagonists according to medical records on Epic. Of these patients, data from Healthy Body Healthy Heart was imported, including serum leptin, BMI, CLIX-IR, insulin, pro-insulin, and c-peptide. With these data, I will chart the outcomes of each patient in order to assess if drugs that target the incretin system are useful in repairing beta cell function. From preliminary data collected from patients on Victoza, a GLP-1 agonist, patients were sorted into Responders and Non-Responders based on their improvements in BMI. Five patients with a decrease of 1 BMI point since taking Victoza were labeled responders, and the six patients with a decrease in BMI less than 1 were labeled non-responders. Between these two groups, the averages for Leptin:BMI, IR score, HOMA IR, insulin, pro-insulin, and C-peptide were calculated. In the future, more patient data will be added to the study to determine if the results yield true distinguishing factors.
While patients are experiencing beneficial results from GLP-1 agonists, additional research is required to assess the extent of pancreatic protection. For patients on Victoza, a GLP-1 agonist, various parameters were measured before, during, and after treatment. These included BMI, leptin, IR score, HOMA IR, insulin, pro-insulin, and C-peptide. Currently, there appears to be two groups of patients who respond differently to Victoza.
Graph 1: Responder BMI before and after Victoza Graph 2: Non-responder BMI before and after Victoza
The averages between the responders and non-responders for each of the parameters measured shows significant improvement in beta cell function among responders compared to non-responders.
Table 1: Average measurements of beta cell function between responders and non-responders after Victoza
Patients who visit endocrinology clinics tend to be placed on a plethora of drugs. If the drugs that target the incretin system work are effective, with the benefit of not causing hypoglycemia due to their glucose- dependent mechanisms, future diabetic patients may not need to be put on countless medications. If there are groups of people who can be designated as responders vs. non-responders, and the responders see a greater improvement in beta cell function, there may be implications in identifying patients who would benefit the most from GLP-1 agonists.
1Holst JJ, Vilsboll T, Deacon CF. The incretin system and its role in type 2 diabetes mellitus. Mol. Cell. Endocrinol. 2009 Jan 15;297(102):127-36. 2Iepsen EW, Lundgren J, Dirksen C, Jensen J-EB, Pedersen O, Hansen T, Madsbad S, Holst JJ, Torekov SS. Treatment with a GLP-1 receptor agonist diminishes the decrease in free plasma leptin during maintenance of weight loss. International Journal of Obesity. 2015 39, 834-841.
Dr. Timothy Graham for his guidance with this project, and Dr. Lindsley, Dr. Stark, and Janet Bassett.
Do drugs that target the incretin system aid in beta cell function in patients with type 2 diabetes mellitus?
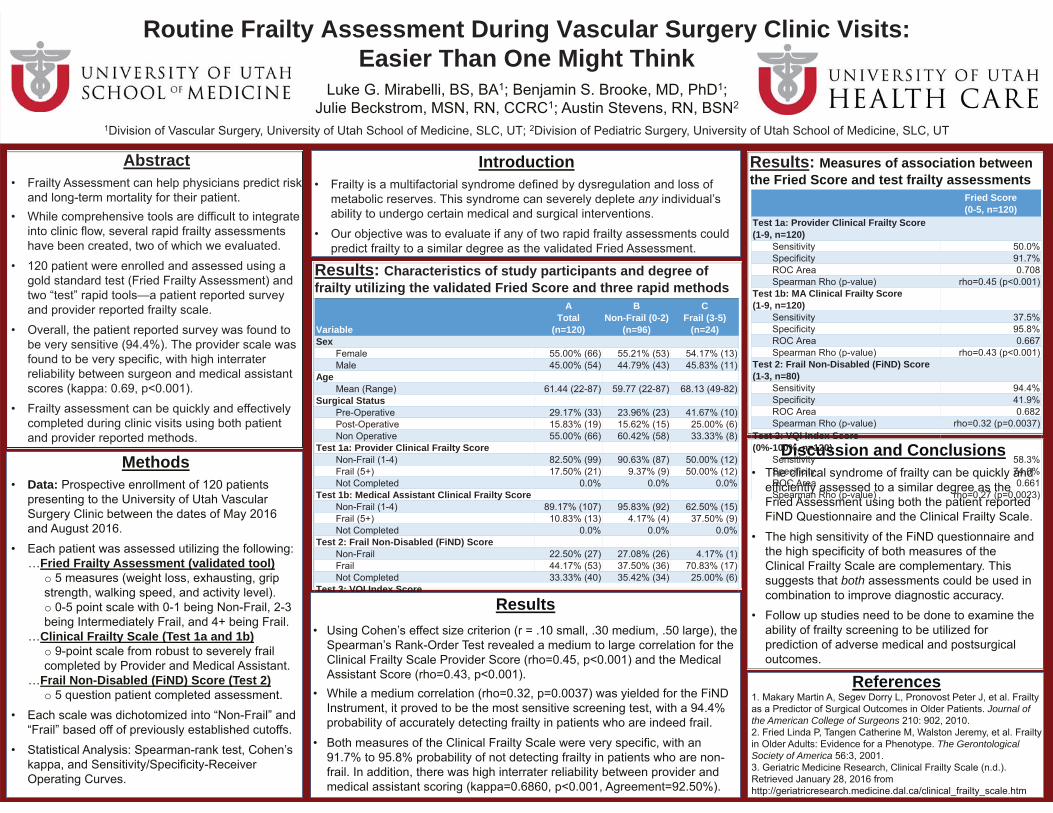
Routine Frailty Assessment During Vascular Surgery Clinic Visits: Easier Than One Might Think
Abstract
Discussion and Conclusions
both
Results: Measures of association between the Fried Score and test frailty assessments
Results: Characteristics of study participants and degree of frailty utilizing the validated Fried Score and three rapid methods
Variable
A Total
(n=120)
B Non-Frail (0-2)
(n=96)
C Frail (3-5)
(n=24)Sex
Age
Surgical Status
Test 1a: Provider Clinical Frailty Score
Test 1b: Medical Assistant Clinical Frailty Score
Test 2: Frail Non-Disabled (FiND) Score
Test 3: VQI Index Score
Fried Score (0-5, n=120)
Test 1a: Provider Clinical Frailty Score (1-9, n=120)
Test 1b: MA Clinical Frailty Score (1-9, n=120)
Test 2: Frail Non-Disabled (FiND) Score (1-3, n=80)
Test 3: VQI Index Score (0%-100%, n=120)
Introduction
any
MethodsData:
Fried Frailty Assessment (validated tool)o
o
Clinical Frailty Scale (Test 1a and 1b)o
Frail Non-Disabled (FiND) Score (Test 2)o
Results
ReferencesJournal of
the American College of Surgeons
The Gerontological Society of America