building a minnesota congenital heart network. the current status of chd leading cause of infant...
TRANSCRIPT

Building a Minnesota Congenital Building a Minnesota Congenital Heart NetworkHeart Network
The Current Status of CHDThe Current Status of CHD
Leading cause of infant Leading cause of infant deaths in the US deaths in the US
#1 cause of birth defect #1 cause of birth defect related deathsrelated deaths
1,000,000 CHD births 1,000,000 CHD births worldwideworldwide
Cost for surgical repair: Cost for surgical repair: >$2.2 billion/yr in US>$2.2 billion/yr in US
Children’s Heart Foundation Fact Sheets
CHD MorbidityCHD Morbidity
Feeding difficultiesFeeding difficulties
Learning difficultiesLearning difficulties– Lower IQ scores Lower IQ scores – 25% require special education 25% require special education
servicesservices– 20-50% display gross or fine-20-50% display gross or fine-
motor dysfunctionmotor dysfunction– Language delaysLanguage delays
Decreased functional Decreased functional independence independence
Social/emotional maladjustment Social/emotional maladjustment
Increased parental risk for Increased parental risk for anxiety, depression, and anxiety, depression, and reduced quality of lifereduced quality of life
•Majnemer et al Sem Ped Neur 1999; 6: 12-19•Helfricht et al PCCM 2008;9:217-223

The Good News!The Good News!
Current surgical mortality Current surgical mortality rate: 2 to 4%rate: 2 to 4%
CHD death rates have CHD death rates have declined by 30% in the declined by 30% in the last decadelast decade
Estimated 2,000,000 Estimated 2,000,000 CHD survivors in United CHD survivors in United StatesStates
More than 50% of CHD More than 50% of CHD survivors are adultssurvivors are adults
http://www.chforegon.org/kids.html
Changing ParadigmChanging Paradigm
Quantity of Life Quality of LifeQuantity of Life Quality of Life

Risk Factors for MorbidityRisk Factors for Morbidity
Cardiopulmonary bypass Cardiopulmonary bypass
Deep Hypothermic Circulatory ArrestDeep Hypothermic Circulatory Arrest
Peri-operative hemodynamic labilityPeri-operative hemodynamic lability
Undesirable pharmacotherapy effectsUndesirable pharmacotherapy effects
Prolonged mechanical ventilationProlonged mechanical ventilation
How do we define strategiesHow do we define strategies
that decrease risk for morbidity?that decrease risk for morbidity?

In a perfect world we would…..In a perfect world we would…..
Compare current Compare current perioperative perioperative management through management through clinical trial investigationclinical trial investigation
Identify superior Identify superior strategies that translate strategies that translate into improved long term into improved long term outcomesoutcomes
Major Obstacles Lie AheadMajor Obstacles Lie Ahead
http://starlightwalker.com/blog/?p=45http://starlightwalker.com/blog/?p=45
Clinical ObstaclesClinical Obstacles
Every institution is Every institution is uniqueunique
Congenital heart Congenital heart disease is relatively disease is relatively rarerare
Establishing clinical Establishing clinical equipoiseequipoise
Investigational ObstaclesInvestigational Obstacles
Gauging improvementGauging improvement
Measuring morbidityMeasuring morbidity
Choosing outcome Choosing outcome measuresmeasures– Morbidity is Morbidity is
multi-factorialmulti-factorial– Surrogate markers????Surrogate markers????
Delayed outcomesDelayed outcomes– Child must ageChild must age– Losses to follow upLosses to follow up

Overcoming the ObstaclesOvercoming the Obstacles
+

Minnesota Congenital Minnesota Congenital Heart Network Heart Network
Objectives Objectives
Establish a collaborative multicenter multidisciplinary network to develop and implement clinical research proposals evaluating congenital heart disease management.
Define the current perioperative environment.
Develop strategies for long term follow up linked to acute perioperative interventions and outcomes.

MCHN Objective #1 MCHN Objective #1
Establish a collaborative multicenter multidisciplinary
network to develop and implement clinical research proposals evaluating congenital heart
disease management.
MCHN InfrastructureMCHN Infrastructure
Clinical Investigators Core: Network members represent all the clinical areas involved in CHD perioperative care: Cardiology, Anesthesiology, Perfusion, Critical Care Nursing, and Pharmacy. This type of multidisciplinary representation is ensuring that clinical research questions are asked with a multidisciplinary voice and have a greater impact on a broader spectrum of patient care.
Biostatistical Core: Designing and analyzing CHD clinical trials presents many challenges due to the heterogeneous patient populations and the potential confounding of diverse management strategies. Appropriate utilization of and design for collecting data requires experienced biostatistical support to maximize the potential clinical implications of research findings. The MCHN is addressing these concerns by involving experienced and advanced biostatistical support at all levels of the clinical research design and analysis process.
Biomedical Informatics Core:Biomedical Informatics Core: The MCHN’s objective to collect and analyze clinical data generated during and after The MCHN’s objective to collect and analyze clinical data generated during and after congenital heart surgery requires techniques for efficient and accurate data collection, congenital heart surgery requires techniques for efficient and accurate data collection, sharing, and analysis. The bioinformatics core is essential for leveraging current sharing, and analysis. The bioinformatics core is essential for leveraging current informatic tools to facilitate MCHN CHD research initiatives.informatic tools to facilitate MCHN CHD research initiatives.

MCHN Objective #2MCHN Objective #2
Define the current perioperative environment.

RationaleRationale
Provides backdrop for interpreting future clinical Provides backdrop for interpreting future clinical investigationsinvestigations
Highlights differences in peri-operative strategies Highlights differences in peri-operative strategies for future clinical trial comparisonfor future clinical trial comparison
Informs medical community regarding current Informs medical community regarding current clinical practice variationclinical practice variation
Establishes clinical equipoiseEstablishes clinical equipoise

Defining the Perioperative Defining the Perioperative EnvironmentEnvironment
Comprehensive collection of acute Comprehensive collection of acute perioperative vital statisticsperioperative vital statistics

Information GainedInformation Gained
Representative graph of cohortRepresentative graph of cohort
Clinicians are informed of how the perioperative Clinicians are informed of how the perioperative period looksperiod looks
Identify “vulnerable” peri-operative periods Identify “vulnerable” peri-operative periods
Compare changes in this background as new Compare changes in this background as new management strategies are introduced.management strategies are introduced.
Identifies an institution specific “fingerprint”Identifies an institution specific “fingerprint”
Overcoming Data Overcoming Data Collection ObstaclesCollection Obstacles

DATABASEDATABASE
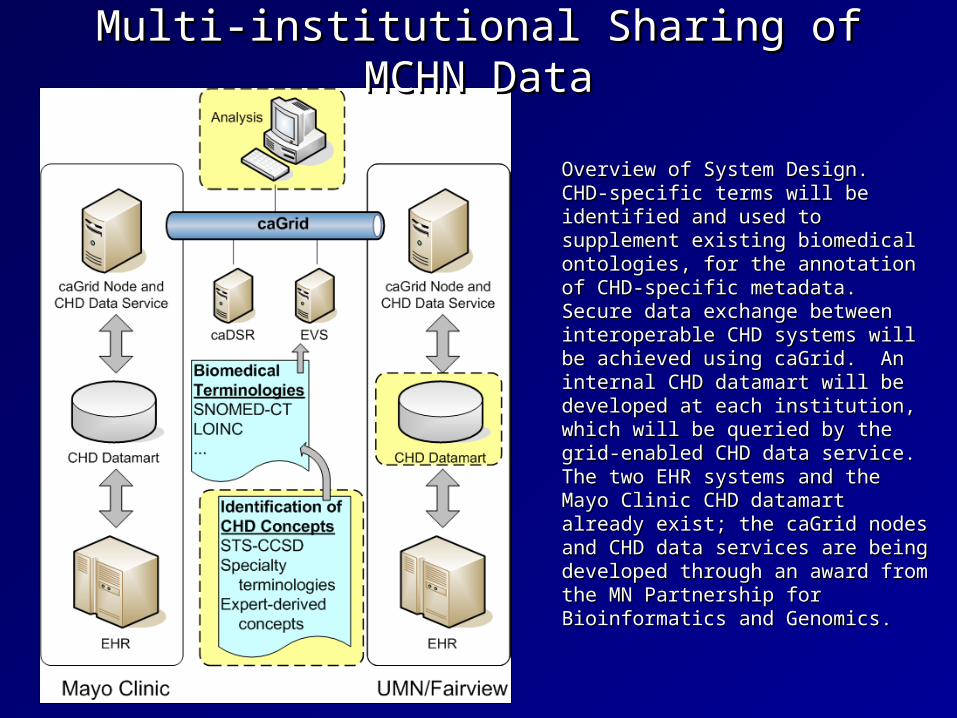
Multi-institutional Sharing of MCHN DataMulti-institutional Sharing of MCHN Data
Overview of System Design. CHD-Overview of System Design. CHD-specific terms will be identified and specific terms will be identified and used to supplement existing used to supplement existing biomedical ontologies, for the biomedical ontologies, for the annotation of CHD-specific metadata. annotation of CHD-specific metadata. Secure data exchange between Secure data exchange between interoperable CHD systems will be interoperable CHD systems will be achieved using caGrid. An internal achieved using caGrid. An internal CHD datamart will be developed at CHD datamart will be developed at each institution, which will be queried each institution, which will be queried by the grid-enabled CHD data service. by the grid-enabled CHD data service. The two EHR systems and the Mayo The two EHR systems and the Mayo Clinic CHD datamart already exist; the Clinic CHD datamart already exist; the caGrid nodes and CHD data services caGrid nodes and CHD data services are being developed through an award are being developed through an award from the MN Partnership for from the MN Partnership for Bioinformatics and Genomics.Bioinformatics and Genomics.

Accessing MCHN DataAccessing MCHN Data
Inotrope Score Query Patient characteristics Clinical data points (i.e.
HR, BP, inotrope dose) Time interval
caGrid
CHD Datamart CHD Datamart
caGrid Node and CHD
Data Service
caGrid Node and CHD
Data Service
Mayo Clinic UMN Fairview
Output with
Statistical Results
caGrid Applications (Statistical Toolbox)
Investigator Querying the MCHN Data Querying the MCHN Data Infrastructure. The hashed arrows Infrastructure. The hashed arrows show the query being distributed show the query being distributed via the caGrid to each institutional via the caGrid to each institutional CHD datamart. The open arrows CHD datamart. The open arrows show data being returned to the show data being returned to the investigator. Existing caGrid investigator. Existing caGrid applications may be used where applications may be used where appropriate (i.e. Statistical appropriate (i.e. Statistical Toolbox).Toolbox).

Inaugural MCHN Clinical TrialInaugural MCHN Clinical Trial
Defining the perioperative Defining the perioperative inflammatory/stress responseinflammatory/stress response
Trial Objective:Trial Objective:
To describe baseline adrenal function and To describe baseline adrenal function and the impact of congenital cardiac surgery on the impact of congenital cardiac surgery on
the hypothalamic-pituitary-adrenal axis. the hypothalamic-pituitary-adrenal axis.
