building institutions for smarter public spending … · building institutions for smarter public...
TRANSCRIPT

Priority-Setting in HealthBuilding institutions for smarter public spending
A report of the Center for Global Development’s Priority-Setting Institutions for Global Health Working Group
Amanda Glassman and Kalipso Chalkidou, Co-chairs
Prio
rity-Settin
g in
Health
B
uild
ing in
stitu
tions fo
r smarte
r public sp
endin
g
Cente
r for G
lobal D
eve
lopm
ent
Cente
r for G
lobal D
eve
lopm
ent

Cente
r for G
lobal D
eve
lopm
ent
Priority-Setting in HealthBuilding institutions for smarter public spending
A report of the Center for Global Development’s Priority-Setting Institutions for Global Health Working Group
Amanda Glassman and Kalipso Chalkidou, Co-chairs

5 4 3 2
Copyright © 2012 by the Center for Global Development
ISBN 978-1-933286-73-0
CGD is grateful to its funders and board of directors for support of this work.
Editing, design, and production by Communications Development Incorporated, Washington, D.C., and Peter Grundy Art & Design, London.

“No country in the world can provide health services to meet all the
possible needs of the population, so it is advisable to establish criteria
for which services to provide.”1
“Disease burden estimations . . . cost-effectiveness studies of
interventions . . . [and] independent evaluations of program
implementation are examples of the kind of work that needs to be
undertaken. In the absence of such capacity, current policy-making is
ad hoc and driven by individual perceptions.”2
“Fostering health policy and systems research and making ethical and
effective use of innovations in medical technology and pharmaceuticals
are relevant for all countries; health technology assessment should be
used to support more informed decisionmaking.”3
“Nations must ultimately be able to fund more of their own needs,
[therefore] country ownership is about far more than funding. It is
principally about building capacity to set priorities, manage resources,
develop plans, and carry them out. We are well aware that moving to
full country ownership will take considerable time, patience, investment,
and persistence. But I think there are grounds for optimism.”4
1. Bobadilla et al. (1994), p. 653.2. National Commission on Macroeconomics and Health, Ministry of Health & Family Welfare, Government of India, August 2005.3. WHO (2008), p.. 4.4. Clinton (2012).

iv
Preface viiAcknowledgments viii
Executive summary ix
Chapter 1 Finite resources, unlimited demand 1A framework of de facto rationing mechanisms 3The timing of rationing: ex ante and ex post 3The rationing implications of allocation between areas and within levels of the health system 4In a practical sense, however, priority is often revealed by action and spending 6Rationing is constrained by historical and political processes 6Why the Priority-Setting Institutions in Health Working Group? 7Notes 7
Chapter 2 The opportunity: evidence, economies, and donor agendas converge to make explicit rationing necessary and possible 8Force 1: A growing body of evidence suggests huge health gains are possible 8Force 2: Public spending on health is growing in low- and middle-income countries 10Force 3: Donors are beginning to restrict health aid flows, putting renewed emphasis on impact, co-financing, and value for
money 13Notes 14
Chapter 3 Considering cost-effectiveness: the moral perspective 15The cost-effectiveness landscape in global health 15The moral case 18Challenges addressed 18Conclusions 18Notes 19
Chapter 4 Progress on policy instruments for explicit priority setting 20Essential medicines lists 20
Table of contents

vTab
le of conten
ts
Health benefits plans 20National Immunization Technical Advisory Committees 23Health technology assessment agencies 25Case studies 30Conclusions 31Notes 32
Chapter 5 Donors and decisions 34Development assistance partners’ support to recipient country priority- setting processes 34GAVI Alliance prioritization mechanisms 37Global Fund prioritization mechanisms 38Conclusions 40Notes 40
Chapter 6
Building institutions for explicit priority setting 42Institutionalizing health technology assessment systems in low- and middle-income countries 45Conclusions 52Notes 53
Chapter 7
Recommendations for action 54Looking ahead 56Notes 57
Appendix A Profiles of Working Group members 60
Appendix B Detailed tables and sources on potential gains from improved efficiency 66
Appendix C Current international support to priority setting in low- and middle-income countries 68
Appendix D Sources for low- and middle-income countries with health benefits plans 75
References 80

viTa
ble
of
conte
nts
Boxes4.1 Case studies of Chile, Mexico, and Uganda 245.1 GAVI Alliance adoption of the HPV vaccine 396.1 Secondary prevention of myocardial infarction using pharmacological treatment in the U.K. National Health Service 46
Figures1.1 Advocates, researchers, and policy makers have labeled almost every disease, condition, medication, or intervention
a “health priority” 21.2 A spectrum of relative priority of interventions based on actions 62.1 Health impact and per person cost of the Centre for Global Health Research package in India 102.2 Per capita public spending on health, 2009 122.3 Sales growth in Avastin in 2010 133.1 Cost-effectiveness of HIV-related health services 163.2 Cost effectiveness of 108 health interventions evaluated in DCP2 173.3 Preventable deaths from immunization-preventable illness, diarrhea, malaria, smallpox, and war 174.1 Agency for Health Technology Assessment in Poland process structure 325.1 Number of current global efforts to support domestic priority-setting 36
Tables1.1 Rationing how and when services are provided 31.2 Rationing to whom services are provided 41.3 Rationing by what services provided 41.4 Rationing mechanisms classified as ex ante or ex post 41.5 Rationing possibilities across and within sectors 52.1 Efficiency gains from switching to health-maximizing alternatives 112.2 Health gains and savings for three intervention alternatives 124.1 Low- and middle-income countries with health benefits plans 214.2 Health technology assessment entities in selected middle-income countries, responsibilities and relationship to coverage
decision making 264.3 Health technology assessment agencies in selected middle-income countries — how and why topics are selected 284.4 Health technology assessment agencies in selected middle-income countries — the role of economic evaluation
in decision making 294.5 The Health Intervention and Technology Assessment Program’s strengths in conducting health technology assessment 315.1 GAVI prioritization procedure 386.1 Funding sources and budgets of health technology assessment agencies in selected countries 496.2 Staffing, time requirements, and costs for health technology assessment agencies in selected countries 507.1 Do’s and don’ts for international agencies and global health funders 55

vii
Most health care systems end up spending some of their money badly. In Egypt, one in five children are stunted, but 20 percent of public expenditure goes to send a very few patients overseas for medi-cal treatment. India funds open-heart surgery while children die of diseases that could be prevented by vaccines that cost a few cents.
While health gains have been significant in low- and middle-income countries in recent years, relatively low coverage of highly cost-effective health interventions continues to co-exist with public spending on high-cost, less effective or even ineffective care. Evi-dence from around the world demonstrates missed opportunities to improve health through reallocation of public monies towards more cost-effective interventions. India could reduce deaths by almost 30 percent via reallocation within their existing public bud-get. Moving money from least cost-effective interventions to most cost-effective interventions can potentially produce about 15,000 times the benefit for people’s health.
Over the past decades, global health experts have focused on financing and purchasing as the central policy instruments to improve the impact of health spending. While such policies are important in determining who gets what health benefits, these instruments have generally been neutral or silent on the choices of which health interventions, services, and products will actu-ally be funded by public and donor monies. These choices may be as important for health impact as the financing and purchasing arrangements in place.
The final report of the Priority-Setting Institutions for Global Health Working Group suggests that large efficiency gains can be achieved by introducing rules, processes, and sometimes “agencies” with the sole function of speaking to priorities. They would evalu-ate the relative costs and effects of different interventions, assess their affordability, deliberate on their distributional and ethical implications, and connect these recommendations and deliberations to decisions on the use of public monies in the health sector. The
report also draws attention to the complicated political and legal wrangling that surrounds resource- allocation decisions in health, and the need to transparently and ethically manage the multiple national and international interest groups that seek a voice in the use of public monies. This is true at the national level, and at the global level.
Past CGD reports have worked to guide what decisions are made regarding global health investments. This report aims to change the decision-making framework itself, to aid in the difficult process of assessing costs, benefits, and trade-offs of new technologies and to inform decisions on public and donor spending. The working group, consisting of experts and policymakers from around the world, aims to shape how countries and the global community can be more effective through improved decision-making processes that man-age the complex politics of resource allocation in the health sector.
The result of this report is a set of thoughtful, pragmatic, and actionable recommendations that can be utilized by countries and global health organizations alike. Successful examples of priority setting mechanisms, from Thailand, the UK, and elsewhere, provide lessons for countries that do not currently have explicit systems to set priorities across interventions and technologies and to manage the political and other costs that typically result.
This report is being released in a time of opportunity. The global economic downturn, rising health-care costs, improvements in tech-nology, and increased information on costs and effectiveness make now an opportune time to build smart and ethical decision-making systems that will better utilize resources and improve health. Deci-sions on the uses of scarce health funding are decisions of life and death—and should be treated with the due process they deserve.
Nancy BirdsallPresident
Center for Global Development
Preface

viii
This report was written by Amanda Glassman and Kalipso Chalki-dou, informed by the discussions of the Priority-Setting Institutions for Global Health Working Group. Jesse Bump is a co-author of chapter 1. Toby Ord is the author of chapter 3.
The authors particularly thank Yot Teerawattananon, Ursula Giedion, Jesse Bump, Tomasz Bochenek, Mala Rao, Lydia Kapiriri, Ruth Faden, Sean Tunis, Rachel Nugent, and Sripen Tantivess for their substantive input and careful reading of the report. The tech-nical review of Ruth Lopert and Victoria Fan is gratefully acknowl-edged and served to improve the coherence of the report.
The authors thank Kate McQueston for her tireless editorial efforts and work to produce the report as well as her contributions to chapter 2, as well as Derek Cutler who has coordinated and organized the launch of the report. The research assistance of Mila Gorokovich and Denizhan Duran is also gratefully acknowledged.
Nancy Birdsall and CGD senior staff—particularly Mead Over and Owen Barder—have provided constructive feedback on the work, while the CGD communications team has greatly improved all aspects of the report and its associated materials.
All errors are the responsibility of the authors.
Acknowledgments
ix
Data, methods, and evidence on the costs, effectiveness, and equity of health interventions and technologies are increasingly available, but there is a persistent gap between this evidence and the uses of scarce public budgets for health in low- and middle-income countries. This is illustrated by low coverage of highly cost-effective health care inter-ventions, dependency on donor finance for the most basic health care interventions, and—sometimes—public subsidies for care considered ineffective in the world’s wealthiest countries. These anomalies that reduce the impact of public and donor spending on health are the result of ad hoc decision making on budgets, driven more by inertia and interest groups than science, ethics, and the public interest.
Many more lives could be saved and health equity enhanced by reallocating part of public and donor monies toward the most cost-effective and equity-enhancing health interventions and technolo-gies. Yet too many countries lack the fair processes and institutions needed to make the connection between evidence and decisions on public spending and spell out the opportunity costs of one decision versus another, while managing the myriad interest groups and ethical conundrums that revolve around new technologies and scarce budgets.
In this report, the Center for Global Development’s Priority-Setting Institutions for Health Working Group has identified core features of priority-setting processes and institutions worldwide, recommending direct substantive support for creating fair and evidence-based national and global health technology assessment systems that will be applicable in any kind of health system.
Finite resources, unlimited demand, unfair processDecisions on public and donor spending on health are controver-sial because they affect who receives what, when, and at what cost, often with life-or-death consequences. In low- and middle-income countries facing highly constrained budgets, the conflicting pres-sures are acute.
Allocating funding to treat HIV/AIDS is among the most vis-ible dilemmas facing donors and policy makers. Only 53 percent
of those needing antiretroviral therapy were receiving treatment in Africa in December 2009.i Countries and their development assistance partners decide who will receive life-saving therapy, when, and under what circumstances, yet neither have defined explicit criteria to make such decisions—leading to nontransparent processes rife with opportunities for abuse by those with influence, and partly or completely void of ethical considerations. Further, current HIV/AIDS allocation strategies do not optimize for dis-ease reduction either.
As countries spend more on health and population demands grow, public spending begins to respond even more to interest groups and wealthy populations, and cost-effective health interventions are often the opportunity cost of that response when priorities are not explicitly set. In India, for example, only 44 percent of children 1–2 years old are fully vaccinated, yet open-heart surgery is subsidized in national public hospitals. In Colombia 58 percent of children are fully vaccinated, but in 2011 the legal system ordered the use of public monies to subsidize treating breast cancer with Avastin, a brand name medicine considered ineffective and unsafe for that purpose in the United States.1
The moral casePeople who decide how to spend health budgets hold the lives and livelihoods of many other people in their hands, and they must lit-erally make life-or-death decisions. Most such decisions take little account of the cost-effectiveness of the interventions they choose to finance, or the human costs and tradeoffs implied by choosing to fund less cost-effective interventions.
The cost-effectiveness of interventions funded by global health agencies varies greatly. For example, some of the least effective interventions for HIV/AIDS produce less than 0.1 percent of the
i. Using the WHO 2006 guidelines to initiate treatment at a CD4 cell count below 200 cells/uL (Institute of Medicine of the National Acad-emies 2011).
Executive summary

xExe
cuti
ve s
um
mar
y
value of the most effective (in disability-adjusted life years). And looking across multiple disease burdens, this fraction drops to less than 0.01 percent.
As a result, ignoring cost-effectiveness can easily mean losing 99 percent or more of the potential value that a health budget could have achieved. Even choosing the median intervention, as analyzed by the Disease Control Priorities in Developing Coun-tries project, can mean losing 85 percent of the potential value.2 In practical terms this can mean hundreds, thousands, or mil-lions of additional deaths from the failure to set effective priori-ties. The moral case for considering the relative value of health interventions implies the need to divert the bulk of funds to the very best interventions.
Current progress and limitations in low- and middle-income countriesIn a growing number of countries, explicit processes to assess health interventions and technologies as inputs to budget decision making and the design of publicly subsidized health benefits are under way and merit better support.
National efforts to support explicit priority setting in health have taken three main paths: essential medicines lists, health ben-efits plans or lists, and health technology assessment agencies. The three have much in common, frequently using similar methods of economic evaluation and criteria for making decisions. The growth of these policy instruments in low- and middle-income countries over the past decade has been motivated by growing populations, increasing financial pressures, greater availability of new and gen-erally higher cost technologies, persistent inequities in health and coverage, and—perhaps— maturation in democratic processes. In middle-income countries the three are converging, with health tech-nology assessment agencies beginning to inform coverage decisions on health benefits plans and essential medicines lists. Yet all have common limitations as well—a shortage of quality data, inadequate local capacity, lack of legal frameworks, limited formal institutional structures, incapacity to revise and update benefits based on newly available data or new products, minimal stakeholder involvement, and sometimes limited connection to decision making on public and donor budgets.
The need for a systematic process of priority settingA set of seven core processes of priority setting, if implemented under an explicit legal and institutional framework, could improve health for any desired level of health spending, while channeling and managing political, commercial, advocacy, and donor interests fairly and ethically.
These seven processes are defined as a “health technology assess-ment system”:•Registration. Assures safety and efficacy of new products and
provides a gateway for considering a technology for public or donor funding.
•Scoping. Identifies and selects technologies (broadly defined as policies, interventions, drugs, diagnostics, and other products) for evaluation depending on country or donor priority-setting goals.
Case study: Uganda
Uganda, a low-income country, spends about $12.50
per capita on health care. The government uses priority-
setting processes (both formal and informal) to inform
health coverage decisions supported by public spending.
It recently offered Ugandans access to a national health
care package, but the cost is almost four times the
funds available for its provision. Moreover, policy mak-
ers have voiced complaints that the complex priorities
in the health care package are donor-driven and do not
fully consider the Ugandan context.1 The government is
committed to providing essential care to its people, but
it faces issues in setting priorities fairly and justifying its
decisions to the public. A Ugandan physician observes:
Somebody can have malaria, and there are no drugs
for malaria, and you find there are drugs for crypto-
coccal meningitis, and then you say to yourself, “If I
come with malaria, and cannot be treated, another
(patient) comes with cryptococcal meningitis and can
be treated, where is the fairness?”2
Notes
1. Kapiriri (2012).
2. Kapiriri, Norheim, and Martin (2009).

xiExecu
tive sum
mary
•Cost-effectiveness analysis. Analyzes technologies using widely accepted economic evaluation methods, tools, and systematic evi-dence reviews, building on defined priority-setting criteria, such as health impact, equity, and financial protection, as relevant.
•Budget impact analysis. Analyzes and projects the potential finan-cial and fiscal impact of adopting and diffusing a technology.
•Deliberative process. Considers the results of cost-effectiveness analysis and budget impact analysis as well as more subjective decision-making criteria dependent on national values and con-text to recommend public or donor funding.
•Decision. Assesses recommendations and makes decisions to include a technology in public or donor budgets.
•Appeals, tracking, and evaluation. Allows for the appeal of rec-ommendations and associated analysis, as well as the tracking and evaluation of the impact of decisions.
Developing health technology assessment systems globally and nationallyThe Working Group recommends direct substantive support for creating and developing both global and domestic health technol-ogy assessment systems:•A global health technology assessment facility should be created to
provide sustained technical and consultative support to global fund-ing agencies and low- and middle-income country governments. Building on the Working Group’s findings and recommenda-tions, as well as instruments already developed to assess clinical guidelines, standards could be developed that would establish the full range of analytical and decision-making components of a working system. Such a facility would have two purposes. First, it would support low- and middle-income country govern-ments that wish to establish permanent national health technol-ogy assessment systems to make evidence-based and ethically informed decisions on public spending for health. Second, it would provide guidance to global health funders that wish to improve and leverage greater value for money in their grants.
The facility would provide peer-to-peer expertise and know-how in economic evaluation, budget impact analysis, and deliberative processes as an input to priority setting (design and adjustment of health benefits plans, negative lists, target-ing of specific disease burdens, or cost control measures). It would help to build institutions and, potentially, accredit-ing methods and processes for research reports sourced by academic, nongovernmental organization, and commercial sectors in low- and middle-income countries. It could also help countries avoid repeating health technology assessment studies on the same technologies by carrying out joint and coordinated evaluations for adaptation and deliberation in each country.
•Direct support to countries creating or developing their own health technology assessment systems could take several forms. Current capacity-building efforts could be more directly targeted to gov-ernment counterparts charged with setting priorities. Hands-on technical pilots and demonstration projects—from the rel-evant starting point—could engage policy makers on real-time concerns. Coaching through procedural advice and knowledge exchange among countries, assisted by a global facility or regional network, would also be essential. Exchanging examples of legisla-tion, process guidelines (including conflict-of-interest manage-ment), handling of confidential data, stakeholder involvement, and overall governance and oversight would prevent duplicate efforts.Given the global economic outlook and anticipated drops in aid,
how low- and middle-income countries spend their money will be a main determinant of the size and pace of future health improve-ment. Supporting countries and global health funders to develop health technology assessment systems that will increase value for money is one way forward.
Notes1. Giedion (2011).2. Jamison et al. (2006).
Priority-Setting in HealthBuilding institutions for smarter public spending

1
Chapter 1
Finite resources, unlimited demand
This chapter sets out the rationing problem common to all health systems — the challenge of managing finite resources to address the potentially unlimited demand for services. Since most rationing mechanisms are only implicit, we frame the dimensions along which actual rationing is often enforced. For low- and middle-income coun-tries (LMICs), “priority setting” is often used to refer to processes that allocate resources with the goal of maximizing health impact within a given expenditure limit. We discuss definitions and theo-retical modes of priority setting as well as how it usually unfolds in practice: as an ad hoc, haphazard series of nontransparent choices that reflect the competing interests of governments, donors, and other stakeholders. Against this background, we discuss the purpose of the Center for Global Development Priority-Setting Institutions for Health Working Group, which is to examine how priorities are set currently — and to propose institutional arrangements that pro-mote country ownership and systematically manage the improve-ment of health outcomes. This introduction is intended to motivate subsequent chapters examining current priority- setting practices in LMICs, the potential for stronger national institutions and more global support, possible ways to evaluate the impact of priority- setting agencies in LMICs, and recommendations for action.
A fundamental challenge for all health systems is to allocate finite resources across the unlimited demand for health services. This is a rationing problem, regardless of whether it is explicitly addressed as such, because it requires choices on what and how services are provided, at what quantity, to whom, at what time, and at whose expense. Inevitably, some demand goes unmet, which is one source of the intense pressure to provide more services within any given resource envelope. Efforts to reduce waste, increase quality, and improve efficiency are all responses to this pressure. Expanding health care costs are another reflection of the same forces. A recent Organisation for Economic Co-operation and Development
(OECD) report found that growth in health spending had exceeded economic growth in almost all OECD countries over the past 15 years.i With worsening fiscal positions and rising demand due to aging populations and advances in technology, the pressure on OECD health systems to deliver more care with greater efficiency is unprecedented.
Policy makers and analysts studying the way health care resources are allocated in LMICs are concerned with the same issues. Many have employed technical approaches to argue for certain interven-tions over others, a process broadly known as “priority setting.” The disability-adjusted life year (DALY) is a standardized measure of disease burden designed expressly to facilitate comparisons of one health problem versus another. In general, these approaches are intended to maximize the impact (however defined) of health spending in LMICs, but donors and other partners usually produce their own analyses using differing methods, which undermine the comparability of their findings and result in a lack of consensus on what should be prioritized.
The result of myriad actors championing a kaleidoscope of “pri-orities” is confusion. Advocates, researchers, and policy makers have labeled almost every disease, condition, medication, or intervention a “health priority” (figure 1.1). From rotavirus to mental illness, from leishmaniasis to prostate cancer, from vaccines to palliative care, the gamut of health needs and possible responses are prominent on the agendas of various groups. Competing advocacy efforts are not new and are likely to remain a key feature of the policy-making landscape. For instance, the recent United Nations High-Level Meeting on Non-communicable Diseases promoted at least four new conditions as global priorities, without recognizing the difficult reality of rationing — that elevating the priority of some interven-tions inevitably means lowering the priority of others.
i. OECD Health Statistics (database), updated February 14, 2011.
This first draft of this chapter was coauthored by Amanda Glassman and Jesse Bump.

2Fin
ite
reso
urc
es,
unlim
ited
dem
and
Conflicts in rationing decisions reflect many natural features of all societies, including differences in demographics, disease burden, and cultural preferences and beliefs. Further, there are no universal answers to inevitable policy and implementation issues, such as the balance of support for preventive and therapeu-tic measures, or how to choose among several treatment options or intervention strategies. This problem is particularly acute for policy makers in many LMICs because of insufficient institutional mechanisms to assess various proffered “priorities,” evaluate politi-cal and economic constraints, and gather input from citizens and stakeholders.
In addition, many LMICs depend on external resources to finance their health systems, and many also rely on donors or other partners for technical assistance or implementation support. This adds a further international dimension to the complexity of set-ting priorities, because relying on external financing and advice leaves countries’ domestic policy processes open to influence by donors. LMICs are also vulnerable to the largesse of donors, which can dry up precipitously — and if this occurs, countries can be left scrambling and priorities must be rapidly recalibrated across dimin-ished resources. A common outcome is a negotiated set of priorities that reflect some domestic needs and some technical, political, and
Figure 1.1Advocates, researchers, and policy makers have labeled almost every disease, condition, medication, or intervention a “health priority”

3Fin
ite resources, u
nlim
ited dem
and
economic considerations, often defined largely by donor interests. Few would argue that this process is optimal.
Potential conflicts over priorities are already complicated within the domestic sphere. For instance, one important driver of costs in some middle-income countries has been rights-based legal arguments by which citizens have used the court system to compel the provision of often-expensive therapies.ii This strategy has been used widely in Central and South American countries where the right to health is enshrined in constitutional law, based on United Nations recom-mendations related to Article 12 of the International Covenant on Economic, Social and Cultural Rights.iii In these instances, citizens, often supported by commercial and professional interests, have forced the expansion of state-provided services, leading to higher health system expenditures and more cuts in other services. But since this strategy only compels the government to provide additional services irrespective of the price, it does not address the wider implications of how much should be spent or how the resources should be used, nor does it directly address tradeoffs that might affect equity and health.
In many cases health systems themselves set out to provide far more services than are possible under their current budgets, creating the difficulty of rationing the provision of promised services. A July 2010 review of national health plans found that, “list(s) of indica-tors (to evaluate health systems) are generally present . . . however, in some cases, the lists include more than 100 indicators” — suggesting the plurality of health systems targets.1 Many plans have no budgets linked to the activities described in the plan. Tashobya, Ssengooba, and Cruz (2003) illustrate this quandary in Uganda, where a pack-age of services costing $28 per capita was expected to be delivered with an $8 per capita actual expenditure.
The multiplicity of priorities and lack of institutional mecha-nisms to rationalize services and spending often results in poor overall system performance, as manifested in low coverage for highly cost-effective health technologies (or coverage of fairly inefficient ones), inefficient and underused health facilities, inequitable access to services, and ultimately poor health outcomes. Yet rarely are the
ii. While this strategy has mainly been used in middle-income countries to date, the practice is likely to expand, since 68 percent of constitutions worldwide include a provision addressing health or health care (Kinney and Clark 2004).iii. See www.unhchr.ch/tbs/doc.nsf/(symbol)/E.C.12.2000.4.En (accessed May 14, 2012).
rationing compromises of different priority- setting mechanisms made explicit to policy makers or the citizens they serve.
A framework of de facto rationing mechanismsWithout explicit rationing processes, rationing occurs haphazardly, by default, and without systematic attention to the ethical issues it raises. It often occurs on more than one level, affecting how and when services are provided, to whom they are provided, in what quantities they are provided, and what services are available. To illustrate, tables 1.1–1.3 show common rationing mechanisms and comprise a framework for considering the dimensions of rationing.
Rationing almost always occurs along most of these dimen-sions simultaneously, which is a natural, normal, and inevitable consequence of the conflict between unlimited demand and finite resources. All countries face the same general issues, but not all pay enough (if any) attention to the issues of efficiency and equity in managing the process. In addition, rationing occurs through the actions of various agents, including, but not limited to, ministries of finance, ministries of health, insurance companies in a private pay system, or employers in an employer-pay system.
The timing of rationing: ex ante and ex postRationing occurs both before and after a country makes a formal commitment to provide services. Some rationing decisions are made
Table 1.1Rationing how and when services are provided
Source: Ham and Robert (2003).
Rationing mechanism Examples
Time Waiting lists and delays in service result in reduced demand
Price Price faced by households limits demand
Distance Services provided at a distance from some or all of the population result in more limited access, thus diminishing demand because of higher transport and opportunity costs
Chance Services are provided based on a lottery, or funding the first thing that comes along

4Fin
ite
reso
urc
es,
unlim
ited
dem
and
by specifying patient subgroups and indications where services will be made available — ex ante rationing decisions. Other decisions — ex post rationing decisions — limit the quantity of services pro-vided after a decision is made to make these services available. All countries use both ex ante and ex post rationing mechanisms. Ex ante mechanisms include benefit packages or defined lists of cov-ered services, both of which specify the services that a government pledges to provide (table 1.4).
In practice further rationing may occur at the implementation stage. In extreme cases promised services may not be provided at all or may be provided on a much smaller scale than planned. And in most cases the services provided are rationed through ex post mechanisms, including rationing by time, price, and distance. For example, when supply is limited, some services will be implicitly rationed by those able to wait for the service (waiting lists for trans-plants are an example of this) or able to travel the distance to receive health care services. Rationing by population group can be done either ex ante or ex post, depending on design and implementation issues. Programs for children and the elderly would reflect ex ante decisions about who is eligible, and the geography of delivery can introduce inequitable biases against population groups living far from the point of service provision.
The rationing implications of allocation between areas and within levels of the health systemAllocation and planning decisions directly affect service delivery by regulating important aspects of the health system, including who is employed with what qualifications, where infrastructure is located and what type is built, and what pharmaceuticals and equipment are available at which facilities. The decisions affect allocation between areas of the health system and also within each area. Rationing implications for decisions exist in each dimension. A matrix of sample areas and levels is presented in table 1.5.
Within a given resource envelope, there are tradeoffs between investing in personnel and infrastructure — for instance, with the two extremes being many personnel with no facilities or many facili-ties with no personnel. With few facilities, rationing by distance is an inevitable consequence in all but the smallest city-states. Increas-ing the number of facilities will reduce the burden of distance but
Table 1.3Rationing by what services provided
Source: Ham and Robert (2003).
Restriction type Examples
Benefit package, essential package, covered services, positive list
Included services defined by government, insurer, and so on; other services not included
Negative list Certain services excluded; those not mentioned assumed to be included
Practice guidelines
Typical services defined; others decided case by case
Table 1.4Rationing mechanisms classified as ex ante or ex post
Source: Authors.
Ex ante rationing mechanisms
Ex post rationing mechanisms
Benefit package, essential package, covered services
Time, price, distance, chance
Table 1.2Rationing to whom services are provided
Source: Ham and Robert (2003).
Definition of included group Examples
Citizens All nationals of a country
Residents Nationals plus other legal residents
All comers Anyone who goes to a facility, including tourists, undocumented persons, and refugees, provided they could reach the facility
All in need and nearby
Rescues at sea; needs-based targeting
Privileged groups
Overt de facto or de jure discrimination by ethnicity, income status, race, age, gender, class, religious affiliation, insurance status, or other characteristics

5Fin
ite resources, u
nlim
ited dem
and
may reduce the services offered at each one. Within each area, how resources are allocated necessarily affects the capabilities of the system. Among personnel, hiring more community health workers allows wider delivery of interventions but limits the complexity of possible services. Hiring more physicians instead has the reverse effect.
With these tradeoffs, the rationing process must consider the range of what is required to deliver services effectively.iv This process should build in choices of care “platforms,”v levels of care (primary or secondary), inputs (beds, buildings, or machinery), staff (nurses, primary care doctors and general practitioners, or specialists), and mixes of drugs, devices, and procedures. Within each of these choice categories, there may be subanalyses to conduct.
A simple example. In considering the burden of vaccine-prevent-able disease (VPD) on newly available public funds, there is first a choice among specific VPDs. Within each VPD, there is a choice of prevention or treatment. Within prevention, there is sometimes a choice among different vaccines (as with the oral polio vaccine or the inactivated polio vaccine). These choices are related to the costs
iv. A concept termed “effective coverage” by the Institute for Health Metrics and Evaluation, defined as “the fraction of the potential health gain of an intervention that is being delivered to a population and is used to track the performance of societies in addressing health challenges.” “Effective Intervention Coverage,” available at www.healthmetricsandevaluation.org/research/team/effective-intervention-coverage (accessed April 13, 2012).v. Term coined by the Disease Control Priorities Network, available at www.healthmetricsandevaluation.org/research/team/cost-effectiveness/ (accessed April 13, 2012).
of the vaccine itself and the delivery strategy, the size of the eligible population, and the associated infrastructure, staffing, and inputs to achieve effective coverage of the eligible cohort of children. Costs will also depend on the installed capacity and coverage level. Finally, the benefit against which costs are measured must be established, whether by health metrics such as deaths averted, life years saved, DALYs, or quality-adjusted life years — or by other standards, such as differences in safety profiles, social values, equity, financial protec-tion, ethical merit, public finance criteria, or other considerations.vi
As is immediately evident, prioritization decisions in health care are controversial because they affect who receives what, how much, when, and at what cost. Patients and their families — particularly the relatively wealthy — may expect access to any treatments with the potential to improve outcomes, irrespective of the costs. Pro-fessionals wish for as many treatment options as possible to offer their patients. Donors expect to see their investments incorporated into public budgets. And industry and product development part-nerships are keen to ensure that every product developed diffuses quickly and is covered by donors, as well as public and private insurance systems.
In the lowest income countries, these conflicting pressures may be acute. Coping with tradeoffs in the prevention and treatment of HIV/AIDS is among the most visible global rationing dilemmas
vi. In the literature, these metrics of benefits are known as “decision crite-ria.” There is an extensive literature on health maximization as a decision criterion, and a smaller literature on the rest. Work from the Disease Con-trol Priorities Network, the Norwegian Research Council, is forthcoming on multicriteria decision analysis and ethics.
Table 1.5Rationing possibilities across and within sectors
Source: Authors.
Allocation across sample areas
Personnel Infrastructure Pharmaceuticals Equipment
Allo
cati
on
wit
hin
are
as Administrators Reference hospitals Antiretrovirals MRIs
Physicians Surveillance centers Blood thinners X-ray
Nurses Laboratories Vaccines Ambulances
Community health workers Health centers Basic antibiotics Thermometers

6Fin
ite
reso
urc
es,
unlim
ited
dem
and
facing policy makers and donors. Only 53 percent of those in Africa needing antiretroviral therapy (ART) received treatment as of December 2009.vii Countries must not only decide who will receive life-saving ART, but also when and under what circumstances. Yet in most cases countries have not defined explicit rationing criteria — leading to nontransparent processes rife with opportunities for abuse by those with influence, and partly or completely void of ethi-cal considerations.2 An Institute of Medicine panel on the future of HIV/AIDS in Africa (2011) acknowledged this problem, calling for a “decision-making process for resource allocation [that] incor-porates robust safeguards not only against discrimination but also against arbitrary or self-serving exercises of power.”3 As Rosen et al. (2005, p. 303) put it, “the question facing African governments and societies is not whether to ration ART, but how to do so.”
In a practical sense, however, priority is often revealed by action and spendingWhat form does a health priority actually take? One dictionary defines priority as “precedence, especially established by order of importance or urgency.” Others, referring to the use of cost-effec-tiveness analysis to set priorities, describe a health priority as a “preferentially rated health-related activity or function.”
In a practical sense, however, priority is often revealed by action and actual spending choices. Over any time span, some things are done and others are not; one reasonable distinction between these two groups would recognize the former as prioritized in some way
vii. Using the WHO 2006 guidelines to initiate treatment at a CD4 cell count below 200 cells/uL (Institute of Medicine of the National Acad-emies 2011).
over the latter. To apply this idea to developed, implementation-ready health interventions, we propose a spectrum of priority, where zero priority is defined by complete inaction and highest priority is defined by the effective delivery of the intervention. For simplic-ity, for the moment we hold constant all dimensions of rationing, meaning that we do not consider the scale of delivery or other issues that would affect access. Along the spectrum, particularly important actions represent key indicators of priority, while many ways exist to frame this normative continuum. Figure 1.2 represents a rational example of how the spectrum might be framed.
Rationing is constrained by historical and political processesAlthough rationing occurs along the dimensions and mechanisms of the frameworks we discuss, governments do not have the free-dom to set policies in a vacuum. In practice rationing and priority- setting decisions are constrained by historical and political factors. Historical factors strongly influence almost every aspect of health systems, including the extent and location of infrastructure; the mix of personnel, their skills, and their locations; the resources available to the country and the health system; and the socioeconomic status, demographics, and geographic patterns of population subgroups whose needs the system should meet. Priority setting is also influ-enced strongly by political, cultural, and ideological factors because its core issues are fundamentally political and ethical: how resources, rights, and responsibilities are distributed. Political considerations largely underpin why it is often very difficult to implement validated technical interventions. The many low-cost life-improving and life-saving interventions yet to be implemented in LMICs indicate potential for improvement in the priority- setting process, which
Figure 1.2A spectrum of relative priority of interventions based on actions
Source: Authors.
Zero priority
No action taken
Actions to evaluate suitability of intervention
Formal bureaucratic actions
(for example, decision to fund or reimburse)
Actions to deliver
intervention
Highest priority
Intervention delivered effectively

7Fin
ite resources, u
nlim
ited dem
and
can accommodate, in a procedurally fair fashion, both the technical and cultural/political aspects of setting priorities.
Why the Priority-Setting Institutions in Health Working Group?We propose that rationing through explicit systems using the tools of cost-effectiveness analysis, budget impact analysis, and delibera-tive processes is likely to improve the health outcomes now achieved through rationing by political and historical forces. A growing literature provides relevant evidence, methodologies, and tools in LMICs, but very little attention has been paid to the policies, pro-cesses, and politics of rationing itself, or to how the global com-munity might better support these efforts. The Working Group’s
report and recommendations aim to fill this gap, taking advantage of a unique window of opportunity in science and technology — the clear opportunities for massive health gain alongside the improve-ment of methods and availability of data; the global economy (char-acterized by growth in middle-income countries and recession in high-income countries); and the donor agenda (with its emphasis on impact and value for money). This unprecedented window of opportunity is discussed in chapter 2.
Notes1. WHO (2010a), p. 2.2. Rosen et al. (2005).3. Institute of Medicine of the National Academies (2011), p. 7.
8
Chapter 2
The opportunity: evidence, economies, and donor agendas converge to make explicit rationing necessary and possibleThis chapter describes why the current global health environment has created an opportune time to invest in priority- setting mecha-nisms and institutions. Three key forces are driving the need for improved systems to create policies on how explicit benefits could be better defined: growing evidence of the cost and efficacy of health care interventions; economic trends; and reductions in donor spend-ing. This chapter evaluates the state of each force — identifying current research on improving the mix of service allocations and demonstrating increased spending for health in many low- and middle-income countries (LMICs). The chapter makes the initial suggestion that donors support countries’ priority- setting capacities as a mechanism for improving impact per dollar spent in health, a topic that will be further discussed in subsequent chapters.
While examples of the inefficiencies and inequities of implicit ration-ing are still plentiful, the science and evidence of what works has grown enormously, illustrating the huge potential health gains from explicit rationing based on cost-effectiveness criteria. A scientific opportunity has come at a time when the global economy has created unprecedented bounties amid pressures on low- and middle-income economies. Most low- and middle-income economies continue to grow quickly, and spending on health is rising, creating new oppor-tunities to decide on the optimal spending of the marginal dollar in health care. In some middle-income countries, however, the recession in the United States and Europe is creating renewed budgetary pres-sures to impose cuts. Worries are also present that current spending trajectories are unsustainable in richer and poorer countries alike.
These same forces are restricting donor spending, leading to a renewed emphasis on demonstrating health impact, improving value for money, and leveraging ever-greater amounts of co-financing from recipients. This emphasis, combined with three forces — increasing evidence of what works, economic trends, and donor cuts — has cre-ated an unprecedented window of opportunity to develop LMIC and donor priority- setting systems that can use scientific knowl-edge and methods to create a greater impact and improve value for
money. This chapter looks at these three forces, setting the stage for the Working Group’s analysis of the strengths and weaknesses of current efforts to ration explicitly, and for its recommendations about expanded efforts to support LMICs.
Force 1: A growing body of evidence suggests huge health gains are possibleAs in high-income-country health systems, examples of the inefficien-cies and inequities of implicit rationing in LMIC health systems are plentiful.i In a simple country comparison of the ratio of life expec-tancy to expenditure on health, Chisholm and Evans (2010) find significant variation among countries spending similar amounts of money, suggesting that poorly performing health systems can achieve improved outcomes if funds are better invested. The World Health Report 2000 and related papers measured health system efficiency, finding variations between countries and scope for improvement when compared with top performers on health metrics.1
At the country level, it is difficult to assess directly the efficiency and effectiveness of public spending, since historical budgetary prac-tices imply that funds are connected to functional categories (sala-ries, transport) rather than specific health interventions or disease reduction outcomes. However, a marker of inefficiency is the fairly low uptake of cost-effective preventive technologies, particularly in the presence of public subsidies for interventions of unknown or limited effectiveness at the population level. In India, for example, only 44 percent of children 1–2 years old are fully vaccinated, but open-heart surgery is subsidized in national public hospitals. In Colombia 58 percent of children are fully vaccinated, but public
i. In this report, we use a definition of efficiency proposed by Evans et al. (1999, p. 3–4), reflecting “not only whether health programs and interven-tions are produced at the lowest possible cost (i.e., technical efficiency), but also whether the health system chooses to provide the most cost-effective set of programs or interventions for the given level of expenditure (alloca-tive efficiency).”

9Th
e opportu
nity: evid
ence, econ
omies, an
d don
or agen
das con
verge
monies subsidize the use of Avastin to treat breast cancer, though it is considered ineffective and unsafe for this purpose in the United States. (The U.S. Food and Drug Administration revoked its license for this use.)2 In Egypt up to 20 percent of children are stunted; however, 20 percent of public expenditure goes to send patients overseas for treatment.3
Another way of illustrating the problem is to compare public spending per capita with the costs of providing a set of highly cost-effective services. Although theoretically affordable in even the poorest countries at $5 per infant not including new vaccines,4 only half of routine immunization programs in Africa are financed by recipient governments.5 This example, and others like it, demon-strates the difference between theoretical affordability and practical affordability — which can diverge in the context of limited resources.
Within specific diseases, there is also evidence of inefficiencies that affect the impact of both public and donor monies. Work undertaken as part of the aids2031 project finds that even though overall spending targets were met, programmatic achievements in HIV/AIDS were substantially below expected levels.6 Forsythe, Stover, and Bollinger (2009) examine the allocation of HIV-related health spending across countries by the type of interventions funded. When countries are organized by HIV prevalence, from least (Madagascar) to greatest (Swaziland), there is enormous variation in the use of funds, particu-larly among countries facing similar levels of HIV prevalence. Despite similar levels of disease burden and country level budgets, Botswana (prevalence 24 percent) opted to spend a greater percentage of fund-ing on providing assistance to orphans and vulnerable children, while Swaziland (prevalence 26 percent) spent primarily on antiretroviral treatment. Neither spent more than 20 percent of their respective funding budgets on prevention efforts. The rationale for these allo-cation decisions is unclear, as is the relationship between allocation choices and the characteristics of the epidemic. In Accra, Ghana, it was estimated that more than 75 percent of new HIV infections occur between sex workers and their partners, yet the World Bank program spent less than 1 percent on resources for this population, contributing the remaining funds to the general population, where only 24 percent of new HIV infections occur.7
Despite this, gains can be made — the Center for Global Health Research estimated that providing a cost-effective health benefits package in India would cost about half of current per capita public spending on health and reduce total deaths by a further 28 percent. The Center’s results for selecting interventions are shown in figure 2.1.
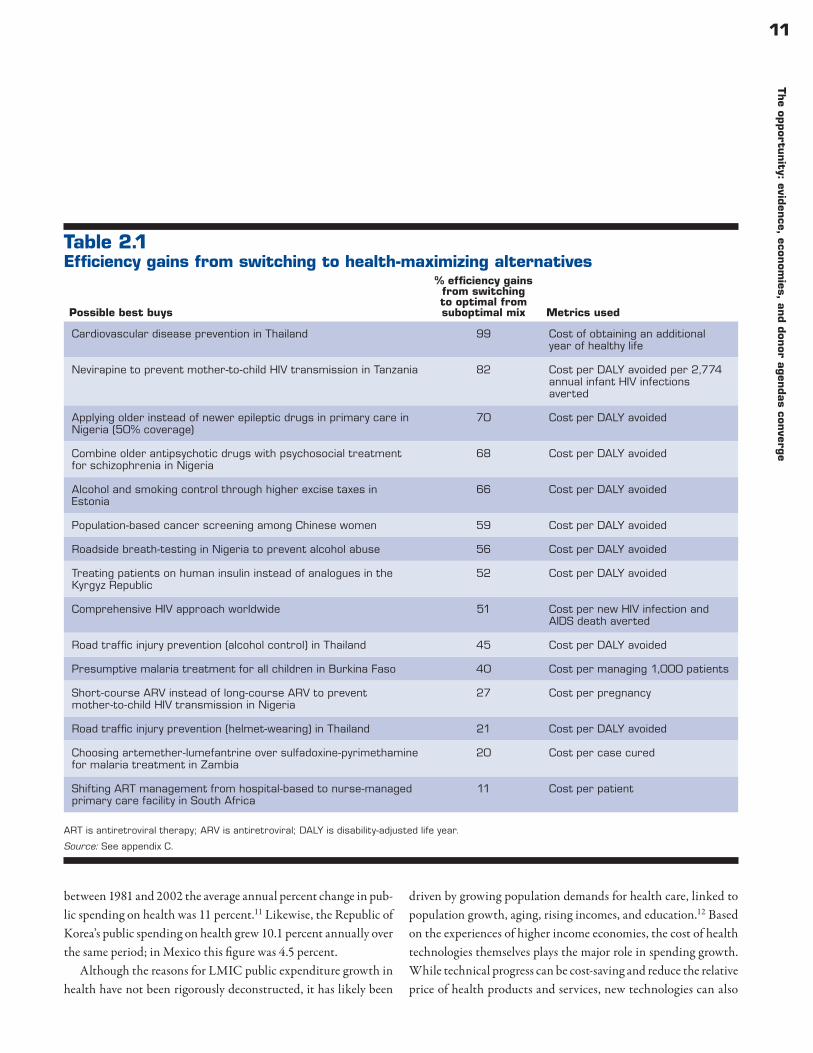
Switching from current practice to a health maximizing or least cost mix of technologies can lead to large health gains — from 11 to 99 percent improvement using various outcome metrics.ii Table 2.1 provides some illustrative examples;iii appendix B provides biblio-graphic detail. The Disease Control Priorities in Developing Coun-tries volumes (2006) also provide a comprehensive examination of the cost-effectiveness literature in LMICs.8
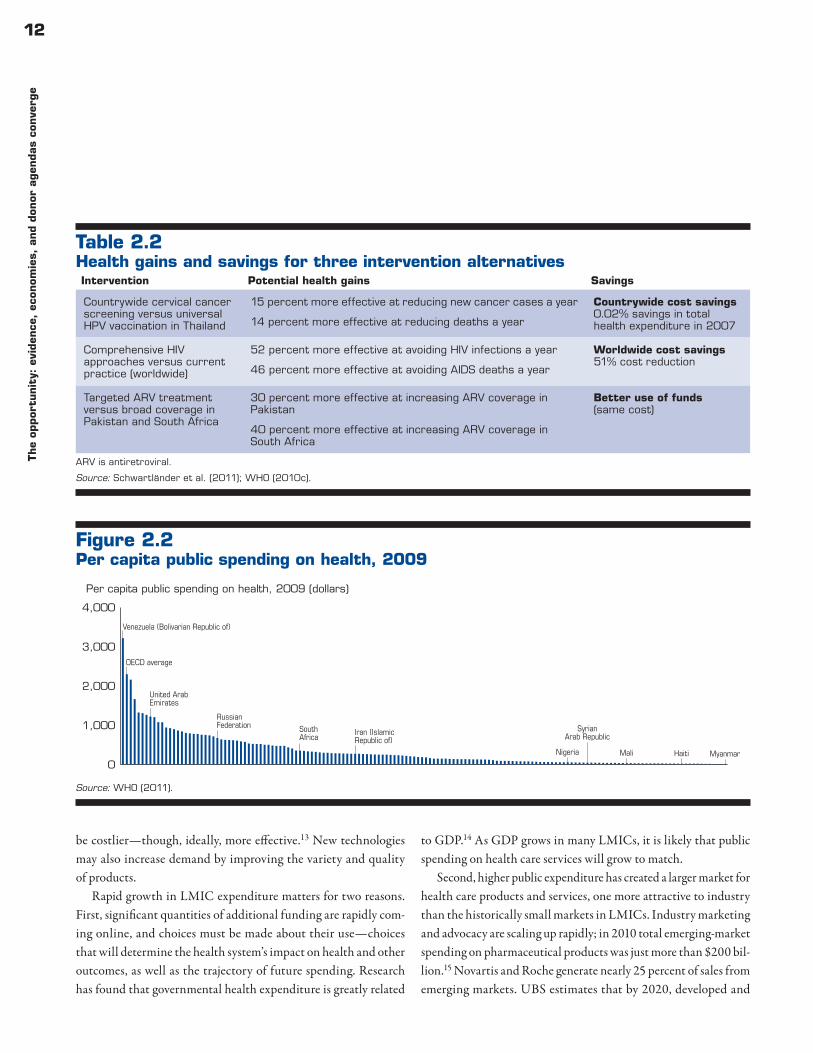
Although cost-effective health interventions are rarely cost-sav-ing, a few LMIC-based studies have demonstrated opportunities to achieve health gains alongside cost savings or with a neutral impact on cost. Table 2.2 shows health gains and savings that could be achieved for three intervention alternatives: cervical cancer screening compared with HPV vaccinations; a comprehensive set of HIV approaches including condom promotion, mother-to-child transmission preven-tion, promotion of male circumcision, activities to reach vulnerable populations, and ARV therapy programs, as compared with current practice; and targeted compared with broad antiretroviral coverage. The example of HPV vaccine for prevention versus countrywide screening and treatment of cervical cancer in Thailand is of particular interest. In many global health statements vaccines are described as almost automatically cost-effective because they are preventive tech-nologies.iv Yet, among the Thai population and assuming a $15 per
ii. One of the difficulties in comparing cost and cost-effectiveness studies is the differing health outcome metrics. For this review, metrics included cost per disability-adjusted life year avoided, cost of an additional healthy life year , cost per infection averted, cost per pregnancy, cost per case, and cost per patient.iii. Illustrative analyses, or even cross-country systematic reviews, are informative, but there is no absolute measure of efficiency, as efficiency is determined by relative input prices. An economically efficient process in one country may be inefficient in another, due to differences in rela-tive prices. Population factors, such as disease burden and demography, will also vary country to country. Sorenson et al. (2008) also describe the transferability of economic evaluations, showing that the problem is not only related to prices. The differences between global estimates of cost-effectiveness and estimates produced using regional or local data can be illustrated when comparing the results of Disease Control Priorities in Developing Countries studies with World Health Organization estimates of cost-effectiveness ratios using regionally adjusted prices.iv. For example, the GAVI Alliance website describes immunization as “one of the most cost-effective ways to save lives, improve health and

10Th
e op
por
tunit
y: e
viden
ce,
econ
omie
s, a
nd
don
or a
gen
das
conve
rge
course vaccine, cervical cancer screening and treatment scale-up was found to be more cost-effective than the vaccine, and thus the HPV vaccine was not funded by the national health system.
In sum, the evidence base on what is cost-effective in individual countries is growing, suggesting there are substantial opportunities to improve health and sometimes generate savings through shifts in the mix of interventions subsidized by public and donor expenditures.
Force 2: Public spending on health is growing in low- and middle-income countriesThe need to maximize health outcomes using explicit rationing meth-ods is greater than ever — not only because potential health gains are huge, but also because resources remain very scarce. Although
ensure long-term prosperity.” See www.gavialliance.org/about/value/cost-effective/ (accessed May 3, 2012).
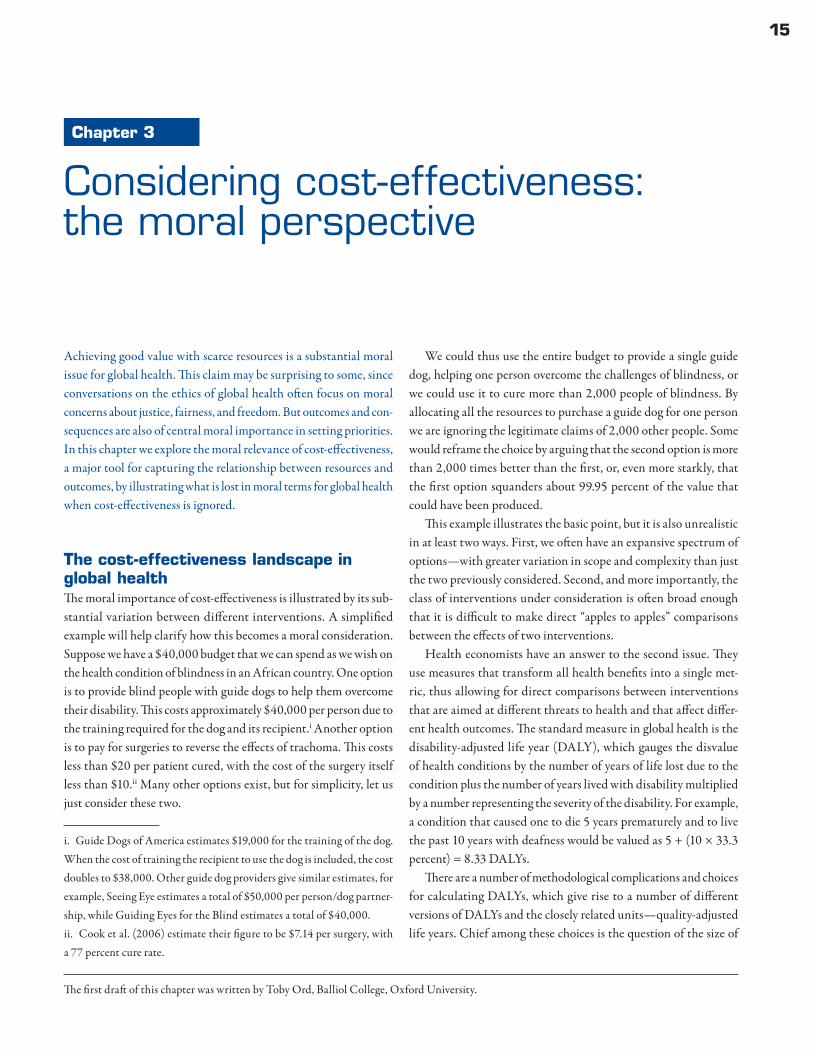
10 percent of world economic product is spent on health, all LMICs together contribute less than 3 percent of this total. Per capita annual public spending on health in LMICs ranges from a low of $2 in Myan-mar to a high of $1,072 in Botswana (figure 2.2). Scarcity matters for priority setting because it increases the significance of tradeoffs between funded interventions and intensifies the health consequences of allocation decisions. Although many health technologies may be cost-effective when assessed against a health maximization or finan-cial protection goal,9 they may be unaffordable under a given budget constraint, forcing countries to say “no” to good value and effective technologies — or resort to inequitable, implicit rationing methods.
However, from a low baseline, public spending on health is grow-ing. On average, LMIC public spending increased about 0.1 percent every 10 years between 1985 and 2010, which translates into an annual percentage change in real per capita terms of 3.4 percent for public spending on health.10 In some middle-income coun-tries growth in public spending is notable. In Turkey, for example,
Figure 2.1Health impact and per person cost of the Centre for Global Health Research package in India
a. 56%, based on 2007 U.S. dollars to Indian Rs exchange rate and total per capita expenditure on health figures.
Source: Reddy et al. (2011).
Tuberculosis: DOTS forsputum + cases and – cases
Vaccination effort for military tuberculosis,polio, DTP, and measles
Noncommunicable diseases: diabetes,cancers, respiratory: metformin treatment
for diabetes, average of three years
Cervical cancer: Once-lifetime screeningfor adult women using acetic acid and
visual inspection
Neonatal intervention: All newbornsreceive postnatal care in institutions
Reduction in deaths (%)Cost per person a year(Indian Rs)
In India, such a package would cost just over half the current total per capita government expenditure on healtha and reduce total deaths by 28%
26
25
20
17
11
15
2
2
23
18
11Th
e opportu
nity: evid
ence, econ
omies, an
d don
or agen
das con
verge
between 1981 and 2002 the average annual percent change in pub-lic spending on health was 11 percent.11 Likewise, the Republic of Korea’s public spending on health grew 10.1 percent annually over the same period; in Mexico this figure was 4.5 percent.
Although the reasons for LMIC public expenditure growth in health have not been rigorously deconstructed, it has likely been
driven by growing population demands for health care, linked to population growth, aging, rising incomes, and education.12 Based on the experiences of higher income economies, the cost of health technologies themselves plays the major role in spending growth. While technical progress can be cost-saving and reduce the relative price of health products and services, new technologies can also
Table 2.1Efficiency gains from switching to health-maximizing alternatives
ART is antiretroviral therapy; ARV is antiretroviral; DALY is disability-adjusted life year.
Source: See appendix C.
Possible best buys
% efficiency gains from switching to optimal from suboptimal mix Metrics used
Cardiovascular disease prevention in Thailand 99 Cost of obtaining an additional year of healthy life
Nevirapine to prevent mother-to-child HIV transmission in Tanzania 82 Cost per DALY avoided per 2,774 annual infant HIV infections averted
Applying older instead of newer epileptic drugs in primary care in Nigeria (50% coverage)
70 Cost per DALY avoided
Combine older antipsychotic drugs with psychosocial treatment for schizophrenia in Nigeria
68 Cost per DALY avoided
Alcohol and smoking control through higher excise taxes in Estonia
66 Cost per DALY avoided
Population-based cancer screening among Chinese women 59 Cost per DALY avoided
Roadside breath-testing in Nigeria to prevent alcohol abuse 56 Cost per DALY avoided
Treating patients on human insulin instead of analogues in the Kyrgyz Republic
52 Cost per DALY avoided
Comprehensive HIV approach worldwide 51 Cost per new HIV infection and AIDS death averted
Road traffic injury prevention (alcohol control) in Thailand 45 Cost per DALY avoided
Presumptive malaria treatment for all children in Burkina Faso 40 Cost per managing 1,000 patients
Short-course ARV instead of long-course ARV to prevent mother-to-child HIV transmission in Nigeria
27 Cost per pregnancy
Road traffic injury prevention (helmet-wearing) in Thailand 21 Cost per DALY avoided
Choosing artemether-lumefantrine over sulfadoxine-pyrimethamine for malaria treatment in Zambia
20 Cost per case cured
Shifting ART management from hospital-based to nurse-managed primary care facility in South Africa
11 Cost per patient
12Th
e op
por
tunit
y: e
viden
ce,
econ
omie
s, a
nd
don
or a
gen
das
conve
rge
be costlier — though, ideally, more effective.13 New technologies may also increase demand by improving the variety and quality of products.
Rapid growth in LMIC expenditure matters for two reasons. First, significant quantities of additional funding are rapidly com-ing online, and choices must be made about their use — choices that will determine the health system’s impact on health and other outcomes, as well as the trajectory of future spending. Research has found that governmental health expenditure is greatly related
to GDP.14 As GDP grows in many LMICs, it is likely that public spending on health care services will grow to match.
Second, higher public expenditure has created a larger market for health care products and services, one more attractive to industry than the historically small markets in LMICs. Industry marketing and advocacy are scaling up rapidly; in 2010 total emerging-market spending on pharmaceutical products was just more than $200 bil-lion.15 Novartis and Roche generate nearly 25 percent of sales from emerging markets. UBS estimates that by 2020, developed and
Table 2.2Health gains and savings for three intervention alternatives
ARV is antiretroviral.
Source: Schwartländer et al. (2011); WHO (2010c).
Intervention Potential health gains Savings
Countrywide cervical cancer screening versus universal HPV vaccination in Thailand
15 percent more effective at reducing new cancer cases a year
14 percent more effective at reducing deaths a year
Countrywide cost savings0.02% savings in total health expenditure in 2007
Comprehensive HIV approaches versus current practice (worldwide)
52 percent more effective at avoiding HIV infections a year
46 percent more effective at avoiding AIDS deaths a year
Worldwide cost savings51% cost reduction
Targeted ARV treatment versus broad coverage in Pakistan and South Africa
30 percent more effective at increasing ARV coverage in Pakistan
40 percent more effective at increasing ARV coverage in South Africa
Better use of funds(same cost)
Figure 2.2Per capita public spending on health, 2009
Source: WHO (2011).
Per capita public spending on health, 2009 (dollars)
0
1,000
2,000
3,000
4,000
Iran (IslamicRepublic of)
SouthAfrica
United ArabEmirates
RussianFederation
OECD average
Venezuela (Bolivarian Republic of)
Nigeria
SyrianArab Republic
Mali Haiti Myanmar

13Th
e opportu
nity: evid
ence, econ
omies, an
d don
or agen
das con
verge
emerging markets could be almost equal in size, driven by an expan-sion of state health care coverage. Figure 2.3 shows growth in sales in Avastin (bevacizumab); for advanced colorectal, breast, lung, and kidney cancer; and for relapsed glioblastoma (a type of brain tumor) by region. Balancing the public interest with commercial interests will become increasingly complex.
Force 3: Donors are beginning to restrict health aid flows, putting renewed emphasis on impact, co-financing, and value for moneyAccompanying the quadrupling of health aid between 1990 and 2010 was an increase in direct funding for service provision in LMICs. For example, the World Bank, the U.S. government, and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) provide 98 percent of their funds to direct service deliv-ery.16 While donor contributions rarely make up a majority share of national health budgets,v World Health Organization (WHO) estimates that 23 countries — mainly in Sub-Saharan Africa — have more than 30 percent of their total health expenditures funded by donors. In some key programs in Africa, such as childhood immu-nization, less than half of funding comes from national sources.vi In Southeast Asia, after the introduction of new vaccines, the share of total routine immunization financed by governments has actu-ally fallen.
However, the U.S. and European economic slowdown is forc-ing reductions in donor budgets. Growth in global health and foreign aid slowed in 2011, and funding for certain organiza-tions such as the Global Fund and the WHO has even been reduced, meaning that donors and countries will need to cope with smaller budgets while maximizing their impact.17 Moreover, donor governments are being challenged by taxpayers in richer countries to become more accountable and transparent in their spending practices, often through retrospective value-for-money external audits.18
In response to these new pressures, some donors have asked that recipient countries gradually assume spending obligations associated
v. Except for Mozambique, with 66 percent of the national health budget financed from external resources.vi. See “Immunization Finance Indicators,” www.who.int/immunization_financing/analyses/jrf_analysis/en/index.html (accessed May 14, 2012).
with providing key health technologies, such as vaccination, family planning, antiretroviral therapy, and antimalarials, among others. New co-financing requirements among global health payers like the Global Fund, the GAVI Alliance, and the U.S. President’s Emer-gency Plan for AIDS Relief (PEPFAR) create legal obligations to give greater priority to these expenditure items.vii
Yet thus far, health aid mechanisms have done little to support countries to make the connection between what is best value and affordable and what is included on public budgets. On the contrary, although there is controversy around methods, some studies find that aid spending displaces about 50 cents of every dollar of public spend-ing on health.viii As aid budgets contract, the search for sustainability
vii. The Global Fund uses cost sharing policies, GAVI requires co-financ-ing, and PEPFAR uses partnership frameworks to share financial burdens and support country ownership of programs.viii. Institute for Health Metrics and Evaluation (2010). Unlike public budgets in recipient countries, donor funding has had much influence on knowledge, evidence, and standard-setting products produced at the global level. In an analysis of the priority of diarrheal diseases over time, Bump et al. (2011) look at the trends in the published literature, finding that—while diarrheal disease burden remained high—publications on infant diarrhea in developing countries rose quickly in the 1980s and
Figure 2.3Sales growth in Avastin in 2010
Source: Giedion (2011), from IMS, OveralI growth pharmamarkets 2010. http://www.pharmaphorum.com/2011/04/06/pharma-emerging-markets-latin-america/; Avastin/Bevacizumab La Roche, annual report.
0
10
20
30
40
50
Latin Americaand the
Caribbean
Europe UnitedStates
Growth rate (percent)Overall pharmaceutical growthAvastin (Bevaviczumab)
25
51
42
9
0

14Th
e op
por
tunit
y: e
viden
ce,
econ
omie
s, a
nd
don
or a
gen
das
conve
rge
or an exit strategy for donors from funding routine services in LMICs requires the recognition that priority setting must be done at the national level, and with the improved support of global agencies.
The next chapter looks at the morality and ethics of rationing based on cost-effectiveness, while the following chapters exam-ine how countries and their development partners have supported explicit rationing so far.
Notes1. WHO (1999); Evans et al. (1999). 2. Giedion, Munoz, and Avila (2012).3. Ministry of Health, Egypt, and Health Systems 20/20 (2010).4. WHO (2006).5. Politi and Galayda (2010).
tapered off in the late 1990s and 2000s. Using dissertations, the authors find that the frequency of dissertations on malaria and tuberculosis has grown steadily—likely due to donor funding emphases—while disserta-tions on diarrheal diseases have remained flat.
6. Hecht (2010).7. Forsythe, Stover, and Bollinger (2009).8. Jamison et al. (2006).9. Weinstein and Stason (1977); Johannesson and Weinstein
(1993); Culyer et al. (2007). 10. Clements, Gupta, and Nazaki (2011).11. Martins and Maisonneuve (2006).12. World Bank (2006).13. Martins and Maisonneuve (2006). 14. Xu, Saksena, and Holly (2011).15. Plumridge (2010).16. Sridhar and Batniji (2008). 17. Leach-Kemon et al. (2012).18. National Audit Office (2011).
15
Chapter 3
Considering cost-effectiveness: the moral perspective
Achieving good value with scarce resources is a substantial moral issue for global health. This claim may be surprising to some, since conversations on the ethics of global health often focus on moral concerns about justice, fairness, and freedom. But outcomes and con-sequences are also of central moral importance in setting priorities. In this chapter we explore the moral relevance of cost-effectiveness, a major tool for capturing the relationship between resources and outcomes, by illustrating what is lost in moral terms for global health when cost-effectiveness is ignored.
The cost-effectiveness landscape in global healthThe moral importance of cost-effectiveness is illustrated by its sub-stantial variation between different interventions. A simplified example will help clarify how this becomes a moral consideration. Suppose we have a $40,000 budget that we can spend as we wish on the health condition of blindness in an African country. One option is to provide blind people with guide dogs to help them overcome their disability. This costs approximately $40,000 per person due to the training required for the dog and its recipient.i Another option is to pay for surgeries to reverse the effects of trachoma. This costs less than $20 per patient cured, with the cost of the surgery itself less than $10.ii Many other options exist, but for simplicity, let us just consider these two.
i. Guide Dogs of America estimates $19,000 for the training of the dog. When the cost of training the recipient to use the dog is included, the cost doubles to $38,000. Other guide dog providers give similar estimates, for example, Seeing Eye estimates a total of $50,000 per person/dog partner-ship, while Guiding Eyes for the Blind estimates a total of $40,000.ii. Cook et al. (2006) estimate their figure to be $7.14 per surgery, with a 77 percent cure rate.
We could thus use the entire budget to provide a single guide dog, helping one person overcome the challenges of blindness, or we could use it to cure more than 2,000 people of blindness. By allocating all the resources to purchase a guide dog for one person we are ignoring the legitimate claims of 2,000 other people. Some would reframe the choice by arguing that the second option is more than 2,000 times better than the first, or, even more starkly, that the first option squanders about 99.95 percent of the value that could have been produced.
This example illustrates the basic point, but it is also unrealistic in at least two ways. First, we often have an expansive spectrum of options — with greater variation in scope and complexity than just the two previously considered. Second, and more importantly, the class of interventions under consideration is often broad enough that it is difficult to make direct “apples to apples” comparisons between the effects of two interventions.
Health economists have an answer to the second issue. They use measures that transform all health benefits into a single met-ric, thus allowing for direct comparisons between interventions that are aimed at different threats to health and that affect differ-ent health outcomes. The standard measure in global health is the disability-adjusted life year (DALY), which gauges the disvalue of health conditions by the number of years of life lost due to the condition plus the number of years lived with disability multiplied by a number representing the severity of the disability. For example, a condition that caused one to die 5 years prematurely and to live the past 10 years with deafness would be valued as 5 + (10 × 33.3 percent) = 8.33 DALYs.
There are a number of methodological complications and choices for calculating DALYs, which give rise to a number of different versions of DALYs and the closely related units — quality-adjusted life years. Chief among these choices is the question of the size of
The first draft of this chapter was written by Toby Ord, Balliol College, Oxford University.

16C
onsi
der
ing
cost
-eff
ecti
venes
s: t
he
mor
al p
ersp
ecti
ve
the weightings representing how bad it is on average to suffer from a particular disability. There are also considerations on discount rates and age weightings.
These methodological choices have ethical implications. People disagree on the appropriateness of particular disability weights, or about the method for eliciting these weights, or about discounting health benefits, or weighting benefits depending on the age of the recipients, or whether other issues such as equal moral consideration need to be factored in. Members of the Working Group and the author of this chapter have many of the same concerns and agree that DALYs should be considered only as a rough measure of the disvalue of different conditions.
In most cases, however, different reasonable choices on these parameters change the number of DALYs due to a condition by a few percent or by as much as a factor of two. By contrast, the dif-ference in cost-effectiveness between interventions is often a factor of 100 or more. Thus, even a rough measure of DALYs saved can supply information of critical moral importance in informing key comparisons.
The two concerns raised in the hypothetical blindness case can be addressed by looking at a real-world example of funding the prevention or treatment of HIV/AIDS. Let us consider five inter-vention types: surgical treatment for Kaposi’s sarcoma (an AIDS defining illness), antiretroviral therapy to fight the virus in infected people, prevention of transmission of HIV from mother to child during pregnancy, condom distribution to prevent transmission more generally, and education for high-risk groups such as sex work-ers. It is initially very unclear which of these interventions would be best to fund, and one might assume that they are roughly equal in importance. However, the most comprehensive compendium on cost-effectiveness in global health, Disease Control Priorities in Developing Countries, 2nd edition (2006), hereafter DCP2, lists their estimated cost-effectiveness as follows (figure 3.1).
Note the wide discrepancies between the effectiveness obtained for the same amount of money. Treatment for Kaposi’s sarcoma can-not be seen on the chart at this scale, but that says more about the other interventions being good than about this treatment being bad: treatment for Kaposi’s sarcoma is often considered cost-effective in high-income countries. But antiretroviral therapy is estimated to be 50 times as effective as treatment for Kaposi’s sarcoma, prevention of transmission during pregnancy is 5 times as effective, condom distribution is about twice as effective, and education for high-risk
groups is again about twice as effective. In total the best of these interventions is estimated to be 1,400 times as cost-effective as the least good, or more than 1,400 times better than it would need to be in order to be funded in rich countries.
This discrepancy becomes even larger if we make comparisons between interventions targeted at different types of illness. DCP2 includes cost-effectiveness estimates for 108 health interventions, arranged from least effective to most effective (figure 3.2).
This larger sample of interventions is even more disparate in cost-effectiveness. The least effective intervention analyzed is still the treatment for Kaposi’s sarcoma, but some other interventions are up to 10 times more cost-effective than education for high-risk groups. In total the interventions are spread over more than four orders of magnitude, ranging from 0.02 to 300 DALYs per $1,000, with a median of 5 DALYs. Thus, moving money from the least effective intervention to the most effective would theoretically pro-duce about 15,000 times the benefit, and even moving it from the median intervention to the most effective would produce about 60 times the benefit.
It can also be seen that due to the skewed distribution, the most effective interventions produce a disproportionate amount of the benefits. According to the DCP2 data, if we funded all of these inter-ventions equally, 80 percent of the benefits would be produced by the top 20 percent of the interventions. It must be noted that these
Figure 3.1Cost-effectiveness of HIV-related health services
Source: Jamison et al. (2006).
0
10
20
30
Education forhigh risk groups
Condomdistribution
Prevention oftransmission
during pregnancy
Antiretroviraltherapy
Surgicaltreatment for
Kaposi’s Sarcoma
Cost-effectiveness: disability-adjusted life years per $1,000

17C
onsid
ering cost-effectiven
ess: the m
oral persp
ective
are merely estimates of cost-effectiveness and there may be less vari-ance between the real, underlying cost-effectiveness values. However, even if the most effective interventions are one-tenth as effective as these figures suggest and the least effective are 10 times better than they appear, there would still be a factor of 150 between them.
Moreover, there have been health interventions that are even more effective than any of those studied in the DCP2. For example, consider the progress that has been made on saving lives lost to immunization-preventable illness, diarrhea, malaria, and smallpox (figure 3.3).
In all cases these interventions have led to at least 2.5 million fewer deaths per year. To aid the reader in comprehending the scale of these achievements, a final bar in the graphic shows the average number of deaths per year due to war and genocide together over the 20th century (2.3 million).
Moreover, these gains have been achieved very cheaply. For instance, with smallpox, the total cost of eradication was about $400 million.1 Since more than 100 million lives have been saved so far, this has come to less than $4 per life saved — significantly superior to all interventions in the DCP2. Moreover, the eradication also saved large amounts of money. About $70 million was being spent across developing countries per year in routine vaccination and treatment for smallpox, and more than $1,000 million was lost per year in reduced productivity.2 Even just in the United States, smallpox vaccination and vigilance cost $150 million per year before eradication.3 The eradication program thus saved an enormous
number of lives per year, while saving money for both donors and recipients, paying back its entire costs every few months. It serves as an excellent proof of just how cost-effective global health can be.
The main effect of understanding the moral need of consid-eration of cost-effectiveness is spending our budgets to produce greater health benefits, saving many more lives and preventing or treating more disabling conditions. However, it also shows a very interesting fact about global health funding. If we can save 1,000 lives with one intervention and 10,000 with another at an equal price, then merely moving our funding from the first intervention to the second saves 9,000 lives. As such, moving funding from one intervention to a more cost-effective one can produce almost as much benefit as adding an equal amount of additional funding to the more cost-effective intervention. This is counterintuitive since it is not the case when one option is merely 10 percent or 30 percent better than another. However, when one option is 10 times or 100 times better, as is often the case in global health, redirecting funding is so important that it can be equivalent to new funding directed toward the superior intervention. In times of global austerity and shrinking budgets, it is good to know how much more can be done within current resources.
Figure 3.2Cost effectiveness of 108 health interventions evaluated in DCP2
Source: Jamison et al. (2006).
0
100
200
300
400
Cost-effectiveness: disability-adjusted life years per $1,000
Figure 3.3Preventable deaths from immunization-preventable illness, diarrhea, malaria, smallpox, and war
Note: Estimates for the death toll from all acts of war and genocide in the 20th century vary from about 160 million to 240 million, differing in which deaths they include (Leitenberg 2006).
Source: Jha et al. (2004).
War(20th century
average)SmallpoxMalariaDiarrheaImmunization-
preventable illness
Deaths per year (millions)
0
1
2
3
4
5
1950193019801960 1979199020012001

18C
onsi
der
ing
cost
-eff
ecti
venes
s: t
he
mor
al p
ersp
ecti
ve
The moral caseIn these examples we have seen how incredibly variable cost-effec-tiveness can be within global health. The least effective intervention in the HIV/AIDS case produces less than 0.1 percent of the value of the most effective, and if we are willing to look at different kinds of disease, this fraction drops to less than 0.01 percent. Ignoring cost-effectiveness thus does not mean losing 10 or 20 percent of the potential value that a health budget could have achieved, but it can easily mean losing 99 percent or more. Even choosing the median intervention can involve losing 85 percent of the potential value. In human and moral terms this can mean hundreds, thousands, or millions of people who will lose their lives due to the failure to take cost-effectiveness into account in allocating health resources. In non-life-saving contexts it means thousands or millions of people who will live with significant disabilities that could be prevented, mitigated, or cured.
In this chapter we make the case that considering cost-effective-ness is a necessary condition for making decisions on global health spending, but on its own, it is not enough. Other moral values similarly need to be factored into a decision-making framework; these include, but are not limited to, fairness, impact on unjust inequalities and systematic disadvantage, and other dimensions of well-being such as respect and self-determination, as well as prox-imity, financial protection, and the like.
Learning how to factor these other ethical considerations cor-rectly into our decision making is an important and challenging problem. But it is important to recognize that we are failing at one terribly important moral imperative — how to achieve good value with limited resources — at the expense of untold human suffering, and not because we are intentionally forgoing securing more good in the interests of acting virtuously or avoiding violat-ing people’s rights.
Challenges addressedSome people do not see cost-effectiveness as advancing ethical considerations, perhaps because its empirical methodology makes it appear more like a technical or scientific matter. This is mis-guided. People who decide how to spend health budgets hold the lives and well-being of many other people in their hands. They are literally making life-or-death decisions. Most decisions of this sort take dramatically insufficient account of cost-effectiveness. As a result, thousands or millions of people die who otherwise
would have lived. The few are saved at the expense of the many, without any justification or compelling rationale. It is typically done out of ignorance about the significance of the cost-effec-tiveness landscape rather than out of prejudice, but the effects are equally serious.
Another reason people might be initially suspicious of using cost-effectiveness to guide prioritization is through confusion with cost-benefit analysis. The latter is an economic method for priori-tization that involves determining the benefits for each person by how many dollars they would be willing to pay, adding these up, and then dividing by the total costs in order to produce a benefit-cost ratio in units of dollars. This method is ethically suspect as it considers benefits to wealthy people (or groups) to be worth more than comparable benefits to poorer people (or groups), since the wealthy are willing to pay more for a given benefit.
However, the cost-effectiveness discussed in this chapter is very different, a type of analysis known as cost-effectiveness analysis. This method does not convert benefits into dollars but provides a raw measure of the benefits in units such as DALYs per dollar, or lives saved per dollar. Thus this method is not biased toward interven-tions favored by the wealthy.
Concern may be an inevitable response to cost-effectiveness since it makes a connection between dollars and health (or even life itself). Making tradeoffs between sacred values such as life and nonsacred values such as money strikes many people as morally problematic. However, no such tradeoff is made in cost-effectiveness analysis. Instead there is a budget constraint of some fixed number of dollars and the cost-effectiveness ratios help to illustrate how much benefit could be produced if this money were spent on a given intervention — for example, saving 1,000 lives or saving 10,000 lives.
ConclusionsIgnoring cost-effectiveness altogether in assessing global health risks means losing much if not most of the value that we could potentially create. For this reason alone the cost-effectiveness of interventions needs to be considered on moral grounds. This does not simply mean implementing current interventions in the most cost-effective way possible, for the improvements to be gained within a single intervention are quite small in comparison. It also does not mean just doing retrospective measures of the cost-effectiveness of the interventions you fund as part of program evaluation. It does mean expanding the domain of interventions

19C
onsid
ering cost-effectiven
ess: the m
oral persp
ective
under consideration to include all those whose cost-effectiveness has been established and that are currently underfunded. And, above all, it means allocating funds to interventions that corre-spond to all relevant moral considerations, including, as a core ethical priority, the moral value of producing the good of global health efficiently. Without a commitment to making value for money central to priority setting, we will continue to fail to honor
obligations to improve the life prospects of those in need and to act justly.
Notes1. Fenner et al. (1988).2. Fenner et al. (1988).3. Fenner et al. (1988).

20
Chapter 4
Progress on policy instruments for explicit priority setting
This chapter explores the major national efforts to support alloca-tion toward cost-effective technologies in low- and middle-income countries (LMICs), describing progress and limitations, and set-ting the stage for the Working Group’s proposal for strengthened national and global priority setting in chapter 5. The topics exam-ined include essential medicines lists, health benefits plans, national immunization technical advisory groups, and health technology assessment agencies.
Policy makers in LMICs are increasingly adopting policy instru-ments that explicitly define, limit, control, or guarantee particular health technologies, interventions, and benefits to be funded and sometimes provided by the government. In this chapter we exam-ine the impact of essential medicines lists, health benefits plans, national immunization technical advisory committees, and health technology assessment entities, discussing progress and limitations.
Essential medicines listsThe essential medicines list is among the earliest efforts to inform explicit priority setting in LMICs. Essential medicines are defined as “those [medicines] that satisfy the priority health-care needs of the population.” In 1977 the World Health Organization (WHO) — with the help of an international expert committee made up mainly of clinical pharmacologists and pharmacists — launched a program to make lists of medicines “with due regard to public health relevance, evidence on efficacy and safety, and compara-tive cost-effectiveness” to inform purchasing decisions in national health agendas.1 A model list — updated every two years based on applications — is published online and frequently adopted (though not necessarily funded or provided) by governments in developing countries. As of 2011, 156 countries have adopted versions of the essential medicines list. While indicators to track access to essen-tial medicines were only established in 2009 and information on
funding is not available, a review of medicines used in primary care in developing countries found that the share of all prescribed medicines included on an essential medicines list has increased over time. However, this does not imply availability of all — or indeed most — of the medicines listed on the essential medicines list. A study published in Lancet in 2009 reported on 45 surveys undertaken in 36 countries.2 These surveys showed that the mean availability of the 15 most frequently surveyed medicines was only 38.4 percent in public sector facilities and 64.2 percent in private sector facilities.
The disconnect between the lists and availability is likely related to the absence of attention and support to the analysis of affordability in a specific country’s public spending envelope, as well as a limited connection to the budgetary process. While the WHO model list of essential medicines includes some hospital and specialist medicines, many countries are seeking international advice on how to handle new higher cost medications, which — while they may be cost-effective — may be beyond the resources of the health system to purchase.3
Health benefits plansA well-known early effort to support explicit priority setting — inspired by the Oregon Health Services Commission’s effort to prioritize within the U.S. Medicaid program — was embodied in the World Bank’s 1993 World Development Report (WDR) and related literature.4 This work introduced the global health com-munity to the idea of using cost-effectiveness to determine which health interventions would be financed publicly — and by extension, by donors. These authors argued that estimates of the current bur-den of disease could be combined with a cost-effectiveness ranking of interventions to derive per capita packages of services that, for a given budget, will purchase the largest improvement in health as measured by a reduction in disability-adjusted life years (DALYs).
Thanks to Richard Laing and Tessa Tan-Torres Edejer at the World Health Organization for their suggested edits and references in this section.

21P
rogress on
policy in
strum
ents for exp
licit priority settin
g
Murray, Kreuser, and Whang (1994) distinguished calculating these packages from a “ground zero” — in which the budget is applied to the whole of the disease burden in the absence of currently financed health interventions — versus doing a “marginal expansion” — in which a package would be constructed with an additional or mar-ginal increase in budget applied to the disease burden.
Criticisms of the 1993 WDR–type package focused on the weak data and evidence base on which estimates of burden and cost relied, the value judgments implicit in DALY age-weighting and age-discounting decisions, the treatment of equity issues,5 and the political difficulties associated with translating a “ground zero” 1993 WDR–style package into a public budget based on histori-cal inputs.6 The uncritical adoption of global-level recommenda-tions by countries was also problematic, since generalization of cost-effectiveness results will necessarily involve the generalization of a single technique of production. Hensher (2001, p. 27) notes: “even with the use of factors such as health care PPP [purchasing power parity] to ‘adjust’ the estimate to reflect local costs, the pos-sibility of different . . . techniques reflecting local relative prices and resource availability is instantly lost,” potentially saddling countries with inappropriate technologies. Further, early cost-effectiveness analysis only considered health maximization as the priority- setting
objective. Later work has highlighted the need for multidimensional priority- setting objectives, including equity and fairness,7 financial protection,8 and current health system capacity.9
Despite the critiques, at least 64 countries — both low and mid-dle income — have established an explicit positive and/or negative package, plan, or list of health interventions to be funded by pub-lic resources, insurance, or social security contributions — albeit using varying (if any) formal methodologies (table 4.1). Although health benefits plans are sometimes thought to pertain exclusively to health insurance schemes, they are being used in all kinds of health systems, even those without purchaser–provider splits, as a means to structure resource allocation and potentially improve accountability, equity, enforcement of rights, and control of spend-ing. In some countries these benefits packages have become one of the main drivers of public health expenditure and thus a key tool for strategic purchasing of health services. In a review of the 98 World Bank health projects approved between 2009 and 2011, 31 — about a third — refer to plans to develop or support a health benefits package. In addition, health benefits plans have been used directly by donors in fragile states such as Afghanistan, Haiti, and South Sudan to contract with nongovernmental organizations for direct service provision.
Table 4.1Low- and middle-income countries with health benefits plans
Source: See appendix D for country source information.
World Bank developing country group Countries
Central and Eastern Europe
Health insurance schemes: Azerbaijan, Bulgaria, Croatia, Estonia, Georgia, Hungary, Kyrgyz Republic, Lithuania, Macedonia, Moldova, Poland, Romania, Russian Federation, and SloveniaTax-funded systems: Armenia, Kazakhstan, Slovak Republic, and Tajikistan
Latin America and Caribbean
Health insurance schemes: Argentina, Chile, Colombia, Dominican Republic, Nicaragua, Peru, and UruguayTax-funded systems: Argentina, Bolivia, Brazil, Honduras, Mexico, and Nicaragua
Asia Health insurance schemes: Lao PDR, Philippines, and VietnamTax-funded systems: Cambodia, China, India, Malaysia, and Thailand
Middle East and North Africa
Health insurance schemes: Egypt, Israel, Lebanon, Malta, Syria, Tunisia, United Arab Emirates, West Bank and Gaza, and YemenTax-funded systems: Bahrain, Djibouti, Jordan, Morocco, Oman, Qatar, and Saudi Arabia
Sub-Saharan Africa Health insurance schemes: Ghana, Kenya, Namibia, Nigeria, Senegal, South Africa, Tanzania, and UgandaTax-funded systems: Uganda and Zambia

22P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
Benefits plans can be mechanisms to reform budgeting in the health sector and align funding with priority technologies and populations. In work conducted by the Inter-American Devel-opment Bank (IDB), researchers found that 70 percent of public resources for health in Colombia were allocated to the financing of the benefits package, the Plan Obligatorio de Salud and Plan Obligatorio de Salud Subsidiado (estimation 2010). In Mexico in 2007, 17 percent of total public resources were allocated to the health plans operating as part of the Seguro Popular.10 In Chile in 2010, about 37 percent of the total public expenditure in health was related to the provision of Regime of Explicit Health Guar-antees.11 In Uruguay in 2010, about 66 percent of total health expenditure was related to the provision of Plan Integral de Aten-ción en Salud.12
A plan-by-plan review is required to document systematically the characteristics of these efforts; however, current literature describes a number of challenges.•Poor data. Health benefits plans sometimes rely on poor data,
no local data, and no cost information. Ghana’s health benefits plan and its contents, for example, were legislated before being costed.13 Health benefits plans in Latin America do not take future demographic and epidemiological trends into account.14
•Lack of connection to available budgets. Health benefits plans are not always linked to available resources or are unaffordable, leading to erosion of health impact and financial protection as well as legal and political challenges. Chile’s Regime of Explicit Health Guarantees (AUGE) only recently calculated the addi-tional costs associated with providing guaranteed benefits.15 Mexico’s Catálogo Universal de Servicios de Salud grew from 91 interventions in 2004 to 266 interventions in 2008, while the capitation payment associated with the package was only adjusted for inflation.16 The example of the Ugandan package in chapter 1, in which a $28 per capita package was expected to be provided with only $8 actually available, is another case of the failure to assess the affordability and fiscal impact of a health benefits plan prior to implementation. Where health benefits plans have worked to structure expenditures, they are accom-panied by changes in budgeting, from inputs to the packages themselves, where input costs are wrapped up in the packaged interventions.
•Need for better techniques in calculation methods. Lacking data on the costs and effectiveness of existing health system activities,
health benefits plan costs are generally calculated based on the ground zero assumption, on a per capita basis rather than incre-mentally. This is the case in Chile, Honduras, and Peru.17
•Poorly defined benefits. Health benefits plans can be vague, grouped in general categories with no specificity (Kenya) or grouped by diagnosis rather than interventions, such that anything can be provided (Peru).18 A recent review by the Nuffield Trust notes that the level of detail included in benefits packages plays a role in the degree that local decision makers are given the autonomy to interpret the remit of the package in relation to specific cases, and describe Chile and Germany as two ends of a continuum.19 Chile’s AUGE includes relatively few benefits, described in great detail, and the goal is to have the system provide “at least” this level of care in a few priority areas. Germany’s social health insur-ance scheme is — by contrast — wide in scope, with little detail and much inconsistency in the description of benefits provided.
•Unclear criteria for benefit selection. In some cases no explicit cri-teria exist for defining the content of health plans, or — in some decentralized countries — plans vary by subnational entity, and their financing depends on the wealth of that particular local-ity or constituency. This is the case for various health insurance programs in China,i with consequences for care variation and equity between rural and urban plans; and in Thailand, with the difference between the plan for civil servants versus the general population covered by the Universal Coverage scheme.
•Need for continual reevaluation. Health benefits plans are some-times conceived as one-off exercises, and no arrangements are in place to update analyses based on new information or techno-logical developments. Where updates occur and disinvestment decisions are taken, there are few methodological, procedural, or implementation standards.
•Disconnect between evaluation and funding decisions. Cost-effec-tiveness research is generally carried out and funded separately from the policy-making process, and it can have limited relevance to and connection with coverage and reimbursement decisions. In China primary and secondary research in health is funded separately by different government agencies, which makes it difficult for decision makers to get well-coordinated evidence.
•Lack of institutional buy-in. Health benefits plans are frequently designed by government or consultants in isolation, often as a part
i. Personal communication, Zhao Kun (February 27, 2012).

23P
rogress on
policy in
strum
ents for exp
licit priority settin
g
of development bank programs. Colombia is an example of a health benefits plan designed by technocrats based on cost-effectiveness, later challenged in the courts by patient advocates.20 Chile’s AUGE package of guaranteed services was also delegated to technical staff at the Ministry of Health.21 The legal contestation of health benefits is spreading in South Africa22 and Latin America.23 Par-liaments are also getting involved. In Colombia, Congress recently required a public subsidy for treatment of rare orphan diseases without regard for tradeoffs or costs.ii Conflicts of interest among those participating in the evaluation of technologies and the design of health benefits plans are generally undeclared.
•Short time frames. Countries are often required to develop health benefits plans under condensed or one-off time frames that may not allow comprehensive analysis or changes in cost estimations due to various contextual factors. Malaysia and Romania are recent examples of countries that have requested the World Bank to “design the package” in a very short time frame.iii
•Lack of records. There is usually insufficient documentation of methods, processes, and actual decisions. The IDB reviewed cov-erage decisions for 20 high-cost drugs in four Organisation for Economic Co-operation and Development and four Latin Amer-ica and the Caribbean countries, encountering an almost total lack of systematic information supporting coverage decisions.
•Lack of a clear stakeholder process. Finally, the lack of a consulta-tive, transparent, multistakeholder process in health benefits plan evidence evaluation, design, and adjustment is a prominent feature of efforts in LMICs. This is a troubling pattern, given the ethical, political, and legal issues involved in the priority- setting process. In South Africa in 1999, for example, university researchers — using evidence-based criteria — designed an essential package of hospital benefits for medical schemes that was established in regulation without any alteration and with no public debate.24
A persistent issue related to health benefits plans is what to do about services not included on a positive list. Because positive lists can never be exhaustive and because professional freedom to decide
ii. Congreso de la República de Colombia (2010). Other work estimated that the cost of treating Fabry’s disease alone, which would benefit 31–37 persons, was equivalent to affiliating 664,000 additional people in the subsidized regime of insurance (Masis et al., 2008).iii. Personal communication, Kalipso Chalkidou, NICE International (February 27, 2012); IMF (2011).
on a patient’s care is a major issue in the field, governments may only put hard limits on pharmaceuticals and medical devices for reimbursement purposes. While this is a practical approach, it can be problematic in LMICs, where the entire delivery apparatus needs to be considered simultaneously. Further, this very specific approach has elicited resistance from industry in Europe.
Clearly, health benefits plans have had a mixed track record, but their frequency is an expression of a trend toward more explicit rationing, motivated by growing population demands and related legal, political, fiscal, and health concerns, particularly among mid-dle-income countries. Three brief case studies of Chile, Mexico, and Uganda are presented in box 4.1 to illustrate some of the issues.
National Immunization Technical Advisory CommitteesAmong the few donor-sponsored initiatives that have directly strengthened explicit priority setting in low-income countries is the Supporting Independent Immunization and Vaccine Advisory Com-mittees Initiative (SIVAC). SIVAC builds the capacity of National Immunization Technical Advisory Groups (NITAGs) and — in some cases — provides support to carry out cost-effectiveness studies of new vaccine introduction or new vaccine technology.25 Bryson et al. (2010) report that the NITAGs are most successful when they are independent but still closely linked to the policy-making process. However, a limitation of the project is the absence of outcome indica-tors “matched to immunization policy-making processes.” Further, no NITAG has ever looked at the budget impact of vaccine adoption recommendations, possibly limiting their policy relevance.iv Although SIVAC operates in some GAVI Alliance– eligible countries (Benin, Côte d’Ivoire, Lesotho, Mongolia, Mozambique, Nepal, and Senegal), these activities could be more closely linked to vaccine introductions financed by the GAVI Alliance, signifying opportunities to better inform country decision making in the context of GAVI vaccine financing. While GAVI does not contribute directly to SIVAC, GAVI does provide financial support to WHO with the objective of improv-ing country-level decisionmaking processes and structures, with the ouput of increasing the performance of GAVI-supported countries on NITAG basic process indicators.v
iv. Personal communication, Kamel Senouci (March 12, 2012).v. w w w.gavia l l iance.org /about/strateg y/phase-i i i-(2011-15)/strategic-goal-1-business-objectives-table/

24P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
Box 4.1Case studies of Chile, Mexico, and Uganda
(continued)
Chile. Launched in 2003, the Regime of Explicit Health
Guarantees (AUGE) guarantees a set of services for all
users.1 AUGE prioritizes diseases and health conditions
based on the burden of disease. It defines the medical
response for each disease and condition. And it empha-
sizes prevention, early examination of symptoms, and
primary care. In addition, AUGE defines the activities,
procedures, and technologies necessary for treating
each medical condition (subguarantee of “quality”). To de-
termine the medical conditions included in AUGE, health
care professionals themselves ranked all major health
problems according to their frequency, seriousness,
and cost of treatment. The principal ranking criterion
was the number of healthy life years lost. Once priorities
were set, the possibility of affecting the outcomes of
the condition through medical treatment was assessed,
together with the infrastructure required to guarantee
treatment to all citizens, regardless of their geographic
residence and socioeconomic status.
In addition, the process considered citizens’ demands
for attention to certain diseases, such as cystic fibrosis.
As a result of this process of prioritization, 56 health
conditions, accounting for about 70 percent of the bur-
den of disease, were identified. While AUGE effectively
channeled both public and private spending for health,
the package was not initially costed, and future public ex-
penditure requirements associated with the guarantees
were never estimated. Further, pressure to expand the
list of guaranteed interventions has grown over time.
Public spending on health in Chile has doubled since the
reform, driven in part by the scope of the interventions
included in the package.2
Mexico. Gonzalez-Pier et al. describe the evolution
of health benefits plans in the public sector in a well-
known article published in the Lancet in 2006. Mexico’s
health benefits plan evolved from a very modest set
of interventions associated with the poverty-targeted
Oportunidades conditional cash transfer program (34
basic public health interventions, $45 per capita) to
the Seguro Popular plan (known as Catálogo Universal
de Servicios de Salud, or CAUSES), which incorporated
cost-effectiveness, financial protection, and social val-
ues criteria to arrive at 249 interventions at $154 per
capita. These capitation payments were transferred
to the states for their use in attending beneficiaries.
Subsequent work has illustrated the continuing
growth in the numbers of interventions in the benefits
plan in the absence of adjustments of the capitation
payment, suggesting that the initial links between the
marginal cost of the intervention and the budget alloca-
tion has been lost in recent years.3 In addition, current
interventions in CAUSES have not been updated from
a medical or cost perspective, resulting in potential
mismatches between the legally mandated benefits
and the actual ability of providers to deliver services.
Without a publicly accountable institution charged with
updating the benefits plan year-to-year using standard
processes and methods, decisions on exclusion and
inclusion of interventions have been opaque. Based
on their review of CAUSES, Giedion, Panopoulou, and
Gomez-Fraga (2009) conclude that CAUSES would be
a more effective priority- setting instrument if prepared
and reviewed regularly by a dedicated entity, based on
regularly collected cost and use data, and linked closely
to available budget resources and the costs of providing
the prioritized benefits.
Uganda. Uganda is a low-income country with high in-
fant and child mortality.4 A third of the population lives
below the poverty line. Using burden of disease and
cost-effectiveness analysis, the country established
the Uganda National Minimum Health Care Package

25P
rogress on
policy in
strum
ents for exp
licit priority settin
g
Health technology assessment agenciesAnother approach to explicit priority setting has been to establish health technology assessment entities to assess new and current medical technologies. Health technology assessment is the system-atic appraisal of the properties, effects, or impacts of health technol-ogy (defined broadly) through a wide range of research methods.vi Although the type of evidence considered comprises the safety, efficacy, effectiveness, cost, social, institutional, legal, and ethical implications, value for money derived from comparative clinical and economic evaluation analysis (cost-effectiveness) is the major component of health technology assessment.
Some European countries, as well as Australia, Canada, and New Zealand, have long used health technology assessment to
vi. Definition of health technology assessment from K. Facey on behalf of the International Network of Agencies for Health Technology Assess-ment, July 5, 2006. Available at www.inahta.net/ (accessed May 14, 2012).
inform public reimbursement or coverage decisions, though the precise use and methodology differ from one country to another.26 Almost all countries have national health technology assessment agencies that prepare evidence dossiers, including cost-effective-ness analysis, as part of applications for including new medicines for public reimbursement. This is particularly so for innovative products or for situations where the manufacturer is seeking a premium price.27 Traditionally, little attention has been paid to identifying obsolete technology for disinvestment, an emphasis now growing due to budget constraints. European experience also illustrates that many health technology assessment bodies involve a wide range of stakeholders in the process, including decision makers, health professionals, academics, patient repre-sentatives, and laypersons.
Over the past five years, health technology assessment agencies or units have been established in upper middle-income or newly high-income countries including Brazil, Chile, Colombia, Croatia,
Box 4.1 (continued)Case studies of Chile, Mexico, and Uganda
(UNMHCP).5 However, as referenced in chapter 1, the
per capita cost of the package per year is estimated at
$41.00 while per capita government expenditure comes
to $12.50, and the plan was not revised or adjusted to
accommodate the budget limitation, leading to a second
round of nontransparent, implicit rationing. Government
policy makers complained that the approach was donor-
driven and complex, and did not consider values that
are relevant to the Ugandan context.6
Further, there is a parallel process of prioritization
by development assistance partners that do not partici-
pate in the sectorwide approach funding mechanism,
sometimes resulting in non-UNMHCP interventions re-
ceiving both donor and government funding.7 In addi-
tion, there is a Health Sector Strategic Plan that also
includes priorities not reflected in the Uganda National
Essential Health Package and vice versa. The relation-
ship of these multiple priority- setting instruments to the
budget is unclear, and both local politicians and donors
were concerned with the reluctance of government to
explicitly set priorities and relate them to the budget.
Notes
1. The General Regime on Explicit Guarantees was es-
tablished by Law 19.966. A list of 40 diseases and
health conditions, and guaranteed services relating
to those conditions, was established by Supreme
Decree 228, issued by the Ministry of Health and
the Treasury in 2005.
2. WHO (2011).
3. Giedion, Panopoulou, and Gomez-Fraga (2009).
4. Kapiriri (2012).
5. Kapiriri, Norheim, and Martin (2009); Kapiriri and
Martin (2006).
6. Kapiriri, Norheim, and Heggenhougen (2003).
7. Kapiriri (2012).
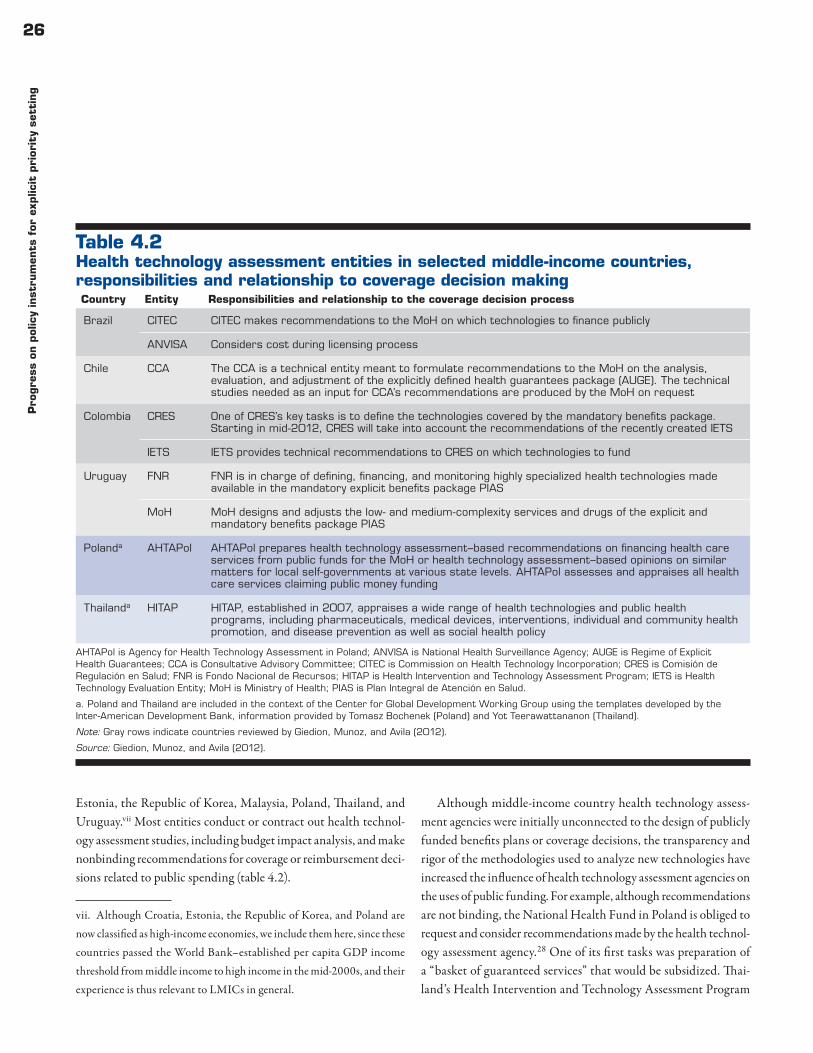
26P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
Estonia, the Republic of Korea, Malaysia, Poland, Thailand, and Uruguay.vii Most entities conduct or contract out health technol-ogy assessment studies, including budget impact analysis, and make nonbinding recommendations for coverage or reimbursement deci-sions related to public spending (table 4.2).
vii. Although Croatia, Estonia, the Republic of Korea, and Poland are now classified as high-income economies, we include them here, since these countries passed the World Bank–established per capita GDP income threshold from middle income to high income in the mid-2000s, and their experience is thus relevant to LMICs in general.
Although middle-income country health technology assess-ment agencies were initially unconnected to the design of publicly funded benefits plans or coverage decisions, the transparency and rigor of the methodologies used to analyze new technologies have increased the influence of health technology assessment agencies on the uses of public funding. For example, although recommendations are not binding, the National Health Fund in Poland is obliged to request and consider recommendations made by the health technol-ogy assessment agency.28 One of its first tasks was preparation of a “basket of guaranteed services” that would be subsidized. Thai-land’s Health Intervention and Technology Assessment Program
Table 4.2Health technology assessment entities in selected middle-income countries, responsibilities and relationship to coverage decision making
AHTAPol is Agency for Health Technology Assessment in Poland; ANVISA is National Health Surveillance Agency; AUGE is Regime of Explicit Health Guarantees; CCA is Consultative Advisory Committee; CITEC is Commission on Health Technology Incorporation; CRES is Comisión de Regulación en Salud; FNR is Fondo Nacional de Recursos; HITAP is Health Intervention and Technology Assessment Program; IETS is Health Technology Evaluation Entity; MoH is Ministry of Health; PIAS is Plan Integral de Atención en Salud.
a. Poland and Thailand are included in the context of the Center for Global Development Working Group using the templates developed by the Inter-American Development Bank, information provided by Tomasz Bochenek (Poland) and Yot Teerawattananon (Thailand).
Note: Gray rows indicate countries reviewed by Giedion, Munoz, and Avila (2012).
Source: Giedion, Munoz, and Avila (2012).
Country Entity Responsibilities and relationship to the coverage decision process
Brazil CITEC CITEC makes recommendations to the MoH on which technologies to finance publicly
ANVISA Considers cost during licensing process
Chile CCA The CCA is a technical entity meant to formulate recommendations to the MoH on the analysis, evaluation, and adjustment of the explicitly defined health guarantees package (AUGE). The technical studies needed as an input for CCA’s recommendations are produced by the MoH on request
Colombia CRES One of CRES’s key tasks is to define the technologies covered by the mandatory benefits package. Starting in mid-2012, CRES will take into account the recommendations of the recently created IETS
IETS IETS provides technical recommendations to CRES on which technologies to fund
Uruguay FNR FNR is in charge of defining, financing, and monitoring highly specialized health technologies made available in the mandatory explicit benefits package PIAS
MoH MoH designs and adjusts the low- and medium-complexity services and drugs of the explicit and mandatory benefits package PIAS
Polanda AHTAPol AHTAPol prepares health technology assessment–based recommendations on financing health care services from public funds for the MoH or health technology assessment–based opinions on similar matters for local self-governments at various state levels. AHTAPol assesses and appraises all health care services claiming public money funding
Thailanda HITAP HITAP, established in 2007, appraises a wide range of health technologies and public health programs, including pharmaceuticals, medical devices, interventions, individual and community health promotion, and disease prevention as well as social health policy

27P
rogress on
policy in
strum
ents for exp
licit priority settin
g
(HITAP) is now formally part of the team that designs the Ministry of Health’s “universal coverage” package. In 2007 Korea made the use of health technology assessment mandatory in decision mak-ing on drug and device reimbursement under the Health Insurance Review Agency.29 In Brazil new technologies are assessed by the National Health Surveillance Agency (ANVISA), and decisions are binding on pricing decisions. In Colombia, starting in 2012, a health technology assessment institute will provide recommenda-tions related to whether evaluated technologies should be included in the benefits package or whether, more generally, they should be financed with public resources. In Hungary health technology assessment forms part of the listing and reimbursement process,viii and in Taiwan, China, the Health Insurance Agency seeks input from the health technology assessment division of the regulator, the Center for Drug Evaluation, for information and analysis of value for money and budget impact.30
In general, health technology assessment agencies assess drugs as a first-order priority, a reasonable emphasis given that public spending on medications drives much of the expenditure increases in the participating countries. However, five of the six agencies assessed by Giedion, Munoz, and Avila (2012) also analyze proce-dures/interventions and medical devices. Only Thailand’s HITAP examines public health interventions, while only Chile uses health technology assessment to develop protocols and clinical practice guidelines. Brazil is the only country evaluated in this paper that uses health technology assessment to inform prices set for public sector purchasing of medications.
Table 4.3 describes how health technology assessment agen-cies in middle-income countries select topics for health technol-ogy assessment analyses, and reveals that — except for Thailand’s HITAP — most operate on a “first come, first served” or ad hoc basis to determine which technologies will be examined. This is a crucial issue since the choice of what to evaluate determines to a large extent whether the technology will be eligible for public fund-ing or reimbursement. Ad hoc processes can imply that advocates and industry will dominate topic selection, while the most health-promoting technologies may remain unfinanced.
While cost-effectiveness is rarely used as the only input to deci-sion making, most health technology assessment agencies assessed
viii. Hungary-Reimbursement Process, available at www.ispor.org/htaroadmaps/hungary.asp (accessed April 16, 2012).
by Giedion et al. (2012) and the Working Group use it as part of the preparation of an evidence dossier (table 4.4). However, the most advanced health technology assessment entities in Poland and Thailand have also established — through precedent or official guidance — a locally relevant threshold against which to assess cost-effectiveness. A general critique of using thresholds is that the health system and most current technologies have never been evalu-ated. When faced with assessing a new intervention for coverage within an existing budget, it is possible to establish the incremen-tal cost per unit of additional health benefit of a new technology, but it is unclear what decision makers are supposed to do with this information. For this reason, a counterfactual alternative is more useful to a decision on coverage. Nonetheless, such cutoffs have been recommended by organizations including the WHO and World Bank.31
For stakeholder consultation or participation during the review of health technology assessment evidence, most of the health tech-nology assessment agencies reviewed by Giedion et al. (2012) and the Working Group do not include mechanisms that would allow expert or nongovernmental participation in evidence review and recommendations — except for Poland and Thailand.
In Poland formal participation of different public entities and nongovernment experts is permitted in the Transparency Council, the key body in charge of assessing technologies previously appraised by the analytical staff of the Agency for Health Technology Assess-ment in Poland (AHTAPol). The Transparency Council is an independent consultative body with 20 members, half of whom are experts. Representatives of various patient organizations and experts, but not industry, have been invited to Council sessions. Stakeholders are also invited to comment on health technology assessments and recommendations carried out by AHTAPol.
In Thailand stakeholders formally participate during the whole process. During topic selection, representatives of several groups of stakeholders (four for each group of policy makers, health profes-sionals, academics, patient associations, civic groups, and lay citizens, and three for the health care industry group) can each propose six topics annually. A panel comprising representatives of four stake-holder groups (health professionals, academics, patients, and civic groups) selects at least 10 topics a year for assessment according to six prioritization criteria (see table 4.3). When conducting a health technology assessment, clinical specialists and methodologists may be invited to take part as researchers, while some are consulted on

28P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
particular elements. During the appraisal of results, HITAP wel-comes reviews of its research findings by interested parties. Selected interested parties might be invited to participate in discussions on the reliability and validity of the research. Finally, health technol-ogy assessment results and associated policy recommendations are publicized, using different approaches to get the messages to par-ticular target populations.
Except for Poland and Thailand, the absence of a deliberative process around health technology assessment is problematic, par-ticularly given the complex tradeoffs involved in adopting a new technology. It is unclear whether citizens want their health care system single-mindedly to maximize health status, since there is a revealed preference for immediate treatment of severe or life-threatening diseases over the removal of minor complaints or even
Table 4.3Health technology assessment agencies in selected middle-income countries — how and why topics are selected
a. Poland and Thailand are included in the context of the Center for Global Development Working Group using the templates developed by the Inter-American Development Bank, information provided by Tomasz Bochenek (Poland) and Yot Teerawattananon (Thailand).
Note: See abbreviations in table 4.2. Gray rows indicate countries reviewed by Giedion, Munoz, and Avila (2012).
Source: Giedion, Munoz, and Avila (2012).
Country/entity Prioritization process for topic selection Criteria for deciding high-priority topics
Brazil/ANVISA/CITEC
No formal process. The definition of priorities has been made through an Annual Workshop on Priorities
Epidemiological relevance and the quality of health care program for patients, opportunity for the Brazilian market, and budgetary impact
Chile/CCA No formal process. Topic selection is carried out by the CCA
Health status of the population, the effectiveness of interventions, their contribution to the extension or the quality of life and, where possible, their cost-effectiveness
Colombia/CRES
No preestablished process for topic selection. In 2011 for the first time a more systematic process was used, but this has not been institutionalized Colombian law
As established by law: epidemiological profile, appropriate technology available in the country, and the financial conditions of the system. In practice, cost of technology to the system has been a main driver for topic selection
Uruguay/FNR/MoH
There is no formal process for topic selection. Both the MoH and the FNR define the topics
Prevalence, burden of disease, uncertainty, health impact, and potential economic, organizational, ethical, social, or legal impact
Polanda/AHTAPol
The process has been performed through consensus meetings run between the AHTAPol and the MoH authorities. The MoH has the final voice, as AHTAPol is subordinated to the MoH. So far, if deadlines were not stated, a first-in, first-out approach has been applied
No precisely defined criteria to select health technology assessment topics at the AHTAPol
Thailanda/HITAP
Representatives of four groups of stakeholders — health professionals, academics, patient groups, and civil society organizations — are appointed to sit on a panel overseeing intervention prioritization. To undertake the task, the panel introduces six agreed criteria (see the right column). A scoring approach with well-defined parameters and thresholds was employed to address each criterion. However, the ranks of interventions could be adjusted through deliberation among the panelists, and those that are prioritized are recommended to the Benefit Package and Service Delivery for endorsement
Size of population affected, severity of disease, effectiveness of health intervention, variation in practice, economic impact on household expenditure, and equity/ethical and social implications

29P
rogress on
policy in
strum
ents for exp
licit priority settin
g
prevention, no matter how much more cost-effective the latter is. This is an issue that — to some extent — can be managed by a delib-erative process around evidence on cost-effectiveness as input to a final decision.
The implementation of health technology assessment in LMICs faces four obstacles, similar to those observed in relation to health benefits plans.•First, evidence from Africa, Asia, and Latin America reveals a severe
shortage of local research capacity for health technology assessment compared with high-income countries where health technology assessment has long been used in policy decision making.32
•Second, the reviews of health technology assessment studies in LMICs found that most of the studies were vulnerable to bias
due to the poor quality of evidence used and deficient report-ing features.33 This may be explained by an absence of standard methodological and process guidelines in most LMICs.34
•Third, health technology assessment research is not usually directed toward major health problems because most health technology assessment studies in LMICs are funded by inter-national organizations and pharmaceutical companies.35 Given resource constraints, it is necessary that health technology assess-ment studies themselves be prioritized and focus on interventions that would assist decisions targeting major health problems that could subsequently have a large impact on population health.
•Fourth, many studies found that health technology assessment was a new discipline among health professionals and decision
Table 4.4Health technology assessment agencies in selected middle-income countries — the role of economic evaluation in decision making
a. Poland and Thailand are included in the context of the Center for Global Development Working Group using the templates developed by the Inter-American Development Bank, information provided by Tomasz Bochenek (Poland) and Yot Teerawattananon (Thailand).
Note: See abbreviations in table 4.2. Gray rows indicate countries reviewed by Giedion, Munoz, and Avila (2012).
Country Role of economic evaluation in decision makingAre there explicit “thresholds” for cost-effectiveness?
Brazil Cost-effectiveness analysis is sometimes used in the coverage decision-making process
No thresholds
Chile The law mandates the use of cost-effectiveness analysis when deciding on inclusions in the benefits package (AUGE), but its use in practice is still limited and not formally organized
No thresholds
Colombia The law mandates that adjustments to the benefits package must be based on the available evidence. In this context there is an increasing yet not mandatory use of cost-effectiveness as a criterion
No thresholds
Uruguay Not mandatory but often used in practice No thresholds
Polanda Cost-effectiveness analysis (or some other type of economic analyses, if applicable) is an integral part of the health technology assessment report, together with clinical effectiveness analysis and analysis of impact on the health care system (including budget impact analysis)
No clear-cut cost-effectiveness threshold has been officially adopted by the Polish health authorities. But there have been thresholds applied in recommendations of the AHTAPol, starting in 2008. They have related to the cost of gaining one quality-adjusted life year against a multiple GDP per capita
Thailanda Cost-effectiveness analysis is an important but not the sole criterion in decision making; budget impact (both technical and political), feasibility, and social and ethical dimensions are also under consideration by the Benefit Package and Service Delivery
The threshold was set at 100,000 baht by the Benefit Package and Service Delivery in 2006; the current GDP per capita in the year 2005 was 120,036 baht. This figure has not yet been updated and is still being used as a cutoff point to indicate whether health interventions are cost-effective under the Thai health care system

30P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
makers in LMICs, and the lack of a clear understanding of health technology assessment among these potential users was identified as one of the major barriers facing the use of health technology assessment in policy and practice.36 Similarly, in an article on health technology assessment agencies in Central and Eastern Europe, Sorenson et al. (2008) identify the obstacles to health technology assessment institutionalization as lack of capacity, lack of data, scoping difficulties, lack of timeliness, and limited connection to decision making and implementation.
Case studiesAmong the countries with an identifiable health technology assess-ment agency, Thailand’s HITAP and Poland’s AHTAPol are the best-documented in the literature. This literature has been comple-mented by consultation with policy makers to develop the two case studies below.
Health Intervention and Technology Assessment ProgramCombined with the rapid aging of the population and widely inef-ficient use of technology, the introduction of a universal coverage policy in 2001 led to a 40 percent increase in public spending on health in Thailand between 2003 and 2006.ix In response, the Ministry of Health established HITAP in 2007 as an autono-mous public arm of the ministry.x HITAP uses technical evidence to inform health policy decision making, using local data, and incorporates social values and preferences of Thai society to assess interventions. Further, HITAP uses various methods — including cost-effectiveness and budget impact analysis — to make recom-mendations to the Benefit Package and Service Delivery regarding listing or delisting.
As in this report, HITAP defines its scope broadly beyond phar-maceuticals and includes procedures, public health interventions,
ix. Examples were misuse and maldistribution of PET/CT, biochemistry lab tests used as screening tests, and inappropriate prescribing of statins. Personal communication, HITAP (September 8, 2011).x. International Health Policy Program, Thailand, and Health Interven-tion and Technology Assessment Program, Ministry of Public Health, Thailand (2011); Pradit sitthikorn et al. (2011); HITAP case study (March 12, 2011, unpublished); personal communication, HITAP (Sep-tember 8, 2011).
and health system policies. For example, HITAP estimated the economic costs of alcohol consumption, which led to a comprehen-sive law for alcohol control (including taxation) in 2008. HITAP’s health technology assessment decisions have more than paid for its annual operating cost. With $6 million purchasing power parity in savings, one health technology assessment study and recommenda-tion on the prevention of cervical cancer in 2007 more than covered HITAP’s operating costs that same year (0.01 percent of the total budget). In 2010 HITAP’s budget came to just 0.007 percent of total health spending, and the scope of work includes 10–15 health technology assessment studies per year on average. A 2010 evalua-tion of a new drug regimen for the prevention of maternal-to-child transmission of HIV compared three antiretroviral regimens with current AZT monotherapy and a single dose of nevirapine, finding that introducing one of the new regimens would avert more than 100 pediatric HIV infections and save $2.6 million for each child saved. HITAP’s health technology assessment has also been used to inform the essential medicines list in 2007–08 (table 4.5).
Agency for Health Technology Assessment in PolandWith the end of the Semashko (Soviet model) health care system in 1999 and the introduction of the National Health Fund in 2002, there have been successive waves of health system reform in Poland. Given the country’s abrupt opening to modern health technologies — which created huge discrepancies between market offers, available funding, and growing needs — several reforms con-centrated on priority setting, decision making on financing health services, and practical applications of health technology assessment. The inclusion or exclusion of health services, pharmaceuticals, or devices into or out of a publicly financed “guaranteed basket” is performed by the Ministry of Health in close collaboration with AHTAPol. Two of AHTAPol’s main tasks are preparing health technology assessment–based recommendations on financing health care services from public funds for the MoH and issuing health technology assessment–based opinions on similar matters for local self-governing authorities at the regional level. In 2009 AHTAPol became a legal and autonomous public entity, and as of 2012 it will be directly involved in the pharmaceutical reimbursement system and in pricing and reimbursement policy.
AHTAPol assesses externally prepared health technology assess-ment reports contracted from outside organizations — including

31P
rogress on
policy in
strum
ents for exp
licit priority settin
g
academic institutions inside and outside Poland — and, to a lesser extent, produces health technology assessment reports in-house. A health technology assessment Pol collects, makes available, and disseminates information on health technology assessment results, methodologies, and recommendations generated within or outside of Poland (figure 4.1).xi
The Ministry of Health directly initiates the process of evalu-ating a given health care service as to whether it will be provided under the public health plan. AHTAPol must also be consulted for removing a particular service from the positive list of financing (guaranteed service) — or for changing its level of financing from public sources or changing the conditions of a particular service. For cases where the service is already guaranteed, the National Consultants (physicians representing various fields of medicine
xi. Agencja Oceny Technologii Medycznych, available at www.aotm.gov.pl/ (accessed April 14, 2011).
appointed by the Ministry of Health), national scientific associa-tions, the president of the National Health Fund, and nongovern-mental organization involved in patients’ rights protection, can all initiate the process, in addition to the Ministry of Health. The final stage of a decision-making process on inclusion or exclusion of publicly funded health care services is issuing an appropriate order of the ministry. AHTAPol uses a variety of criteria to arrive at its recommendations, including efficacy, safety, cost-effectiveness versus that of alternatives, impact on expenditures, health priorities, and price competitiveness.
ConclusionsThis chapter has looked at the application of different explicit ration-ing approaches in LMICs, identifying strengths and weaknesses of essential medicines lists, health benefits plans, and NITAGs and health technology assessment agencies as mechanisms to influ-ence the efficiency of public spending on health. The review has
Table 4.5The Health Intervention and Technology Assessment Program’s strengths in conducting health technology assessment
Source: Teerawattananon et al., personal communication (October 3, 2011).
Diverse stakeholder engagementRobust health technology assessment approach Timely policy response
Regular dialogue to prioritize and fine-tune health technology assessment topics, review research approaches, and inform universal care implementation
Stakeholders include:• Policy makers• Health• Professionals• Academics• Patients• Civil societies• Private sector
Push strategy• Audience-customized print and
electronic media, and face-to-face interactions
Pull strategy• Educating and recruiting research
staff through mentorship, fellowships, and publication opportunities
Process principles of transparency, accountability, timeliness, technical excellence, and effective communication
Context-specific• Priorities for health technology
assessment analysis are based on:• Size of population affected• Severity of disease• Effectiveness of health
intervention• Variation in practice• Economic impact on household
expenditure• Equity/ethical and social
implications• Value for money and budget
impact analysis
• Established societal value for a ceiling threshold in Thailand
Ability to respond to policy priorities (assessing newly promoted HPV vaccine, treatment options for postmenopausal osteoporosis)
Conducts 10–15 health technology assessment studies per year on average
Examples of policy influence
• Alcohol control: Economic costs of alcohol consumption in Thailand led to policy makers issuing a comprehensive law for alcohol control in 2008
• National List of Essential Drugs: 10/12 health technology assessment reports in 2007–08 informed essential drug list policy making

32P
rogre
ss o
n p
olic
y in
stru
men
ts f
or e
xplic
it p
rior
ity
sett
ing
illustrated the following: that the effort to select priorities explicitly, using evidence, is quite widespread and not confined to wealthier middle-income countries; many countries still do not use any of the priority- setting approaches described; there is an important role for social preferences and values in setting priorities and highlighting the importance of procedural fairness in selecting priorities, which is not a solely technocratic exercise; and there is scope to improve national efforts on a number of dimensions, which will be explored in the following chapters.
Notes1. van den Ham, Bero, and Laing (2011), p. 2.2. Cameron et al. (2009). 3. PAHO (2010).4. World Bank (1993); Bobadilla et al. (1994).5. Anand and Hanson (1997).
6. Glassman et al. (1999).7. Sassi (2001); Cookson, Drummond, and Weatherly (2009);
Hauck, Smith, and Goddard (2004). 8. Smith (2012). 9. Jamison et al. (2006).10. Giedion, Panopoulou, and Gomez-Fraga (2009).11. Bitran and Escobar (2008).12. Buglioli and Rodríguez 2011.13. Ramachandra and Hsiao (2007).14. Glassman et al. (2010).15. Bitran and Escobar (2008).16. Giedion, Panopoulou, and Gomez-Fraga (2009). 17. Giedion (2011).18. Hsiao and Shaw (2007).19. Rumbold, Alakeson, and Smith (2012). 20. Yamin and Vera (2008).
Figure 4.1Agency for Health Technology Assessment in Poland process structure
Source: Authors.
National Health FundPresident
National Consultantin a relevant field of medicine
AHTAPolPresident
Ministry of Health
AHTAPolTransparency Council
1 Request for recommendation of a particularhealth care service as guaranteed andassessment of level or type of its financing
4 Presentation of gathered opinions,assessment of a health technology
5 Issuing position on qualification of ahealth care service as guaranteed andkind or level of its financing (positive or
negative), appraisal of a health technology
6 Presentation ofrecommendation
2 Requestfor opinions
3 Issuingopinions

33P
rogress on
policy in
strum
ents for exp
licit priority settin
g
21. Landwehr and Böhm (2011). 22. MacLeod (2010).23. Budlender (1999).24. MacLeod (2010).25. Bryson et al. (2010).26. Schreyogg et al. (2005); Nielsen, Funch, and Kristensen (2011).27. Sorenson et al. (2008).28. Bochenek (2011).
29. HTAsiaLink (January–April 2011).30. Pwu (2010).31. Shillcutt et al. (2009).32. Tarn et al. (2008); Iglesias et al. (2005); Gavaza et al. (2010). 33. Mulligan, Walker, and Fox-Rushby (2006).34. Walker et al. (2010).35. Teerawattananon, Russell, and Mugford (2007).36. Chaikledkaew et al. (2009).
34
This chapter discusses the role of priority setting in the activities and decisions made by development assistance partners, donors, and inter-national agencies. It finds that efforts to support national policy mak-ing have primarily been limited to specific diseases, conditions, or types of technologies and have done little to assist in the creation of country-specific data that would best aid national-level policy decisions. Orga-nizations such as the GAVI Alliance (GAVI) and the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) are following a set process to decide priorities to inform internal decisions for funding allocation, yet these practices could be strengthened and made more transparent. Development assistance partners can do more to support national and international decision-making processes.
Aid is an important source of health financing for many low-income countries, which is why the ways in which development assistance partners set their priorities are important. Like country policy mak-ers, development assistance partners that fund health policy and service delivery in recipient countries — directly or indirectly — must choose among disease control priorities, among interventions to address disease control priorities, and among alternative procedures, devices, and products within interventions.
Development assistance partners must also choose among coun-tries. Declarations on aid effectiveness in health call for the align-ment of development assistance partner priorities with recipient country priorities, suggesting that — in an ideal world — development assistance partners could rely on country priority- setting processes to inform their own spending priorities. In practice — as described in chapter 1 — and without adequate priority- setting processes in recipient countries, development assistance partners set or intend to leverage their own priorities by using direct donations and co-financing requirements. This strategy could be appropriate if spend-ing is directed to global public goods in health — like infectious disease control or prevention — and if, within global public goods, development assistance partners support very cost-effective and affordable interventions in recipient countries.
Although much of global health funding goes to cost-effective interventions and global public goods, most development assistance partners have, so far, provided limited support to country priority- setting processes and are only now starting to consider establishing rigorous processes for identifying priorities for funding within their own agencies.
Development assistance partners’ support to recipient country priority- setting processesIn addition to providing modest support to the country activities described in the previous chapter, development assistance partners have funded the regular update of estimates of the global burden of disease, injuries, and risk factors (1993, 2002, 2006, and 2010 projections under way) via the Disease Control Priorities Project (DCPP) and a connected World Health Organization (WHO)/Institute for Health Metrics and Evaluation collaboration.i The DCPP has evolved into the Disease Control Priorities Network, which produces empirical estimates of intervention effectiveness, gathers cost data from a limited number of countries, carries out economic analysis on financial protection, equity, and other dimen-sions, and develops capacity in a limited number of low- and middle-income country (LMIC) settings.
The availability of the DCPP has played a role in the increasing number of LMIC-focused cost-effectiveness studies published in the peer-reviewed literature. Cost-effectiveness studies based in LMIC settings now number in the thousands. However, their application in practice to real life coverage decision processes is likely to be very small. Walker et al. (2000) and Mulligan, Walker, and Fox-Rushby (2006) review the literature on communicable and noncom-municable diseases in developing countries, respectively. Young-kong, Kapiriri, and Baltussen (2009) conduct a literature review
i. “Global Burden of Disease Study,” available at www.globalburden.org/ (accessed April 11, 2012).
Chapter 5
Donors and decisions

35D
onors an
d decision
s
of empirical studies on priority setting in developing countries, identifying 18 studies, all of which were published after 1999, mostly between 2006 and 2008. The growing number of cost-effectiveness studies has also begotten a number of database-oriented projects to support systematic reviews and disseminate results, such as the Evidence-Informed Policy Network and the Guidance on Priority Setting in Health (see appendix C).
A concurrent and growing area of support is related to models and tools that would allow policy makers to design their own pack-ages. Murray and coauthors’ 1994 Health Resource Allocation Model optimized for burden of disease, cost-effectiveness of available health interventions, and available health system infrastructure.1 Reporting results in 2005, WHO’s Choosing Interventions that are Cost Effective (CHOICE) project incorporates interactions between concurrent interventions, modeling the effect of scale on costs and effectiveness for every intervention and every combination at different levels of coverage,2 and subsequently applying the model to Millennium Development Goal–related priorities.
The Lives Saved Tool developed by Johns Hopkins University is another model that allows users to compare alternative coverage strategies over a period of time, but it does not build in costs. A Harvard University Project — Antares — has developed a prioriti-zation model for the private sector that incorporates household income, impact on women, and other medical and social externali-ties to identify health issues with a disproportionate impact on a poor family’s income.ii
The comprehensiveness of these models is also growing. Evidence and Value: Impact on Decision Making, for example, combines a multicriteria decision analysis value matrix made up of 15 quantifi-able components of decisions (quality of evidence, disease, interven-tion, and economics) with a qualitative tool including six ethical and health system–related components of decisions, and pilots the tool for a single disease in South Africa and Canada.3 Baltussen et al. (2010) use multi criteria decision analysis to prioritize interventions in seven LMICs, concluding that methodologies like this “can have far-reaching and constructive influences on policy formulation.” Yet in all cases, the models remain in the literature or in pilots rather than being part of a routine policy-making process.
ii. “Innovative Approach to Global Health & Poverty: Capitalism for Good,” available at www.eventbrite.com/event/1605234299 (accessed April 11, 2011).
Less visibly, the international community has also focused on improving the country-level availability and quality of the epidemio-logical, demographic, use, and cost data that feed into burden of disease and cost-effectiveness estimations, most notably via the Health Metrics Networkiii and the Demographic and Health Surveys.iv Nevertheless, basic statistics on births and cause of death remain problematic,v and no effort is being made to track country progress systematically in the availability of data critical to priority setting, maybe because in the absence of priority- setting processes, it is not clear what types of data are most important for policy decisions and ought to be collected.
While various organizations seek to increase information exchange and collaboration among different health technology assessment agencies, the support is fragmented and lacks a single organization that would serve as a global hub for LMIC needs. The International Network of Agencies for Health Technology Assess-ment (INAHTA), founded in 1993 with representatives from 29 mostly European countries, aims to provide a forum for the iden-tification and pursuit of interests common to health technology assessment agencies, as well as promote information sharing and thus prevent unnecessary duplication of activities. It currently sup-plies a series of publications and briefs, as well as checklists to assess health technology assessment programs. INAHTA has limited partnerships with various international and regional organizations.
Health Technology Assessment International (HTAi) serves mainly as a forum for information sharing among national health technology assessments through the organization of annual meetings and the publication of its journal. HTAi is aiming to increase par-ticipation from LMICs, with its last annual meeting held in Rio de Janeiro registering record numbers of participants from across Latin America as well as Europe and the United States. Various other ini-tiatives, such as the Cost-Effectiveness Analysis Registry, provide sys-tematic reviews aimed mainly at physicians in high-income countries.
iii. “What is HMN?,” available at www.who.int/healthmetrics/about/whatishmn/en/index.html (accessed April 11, 2012).iv. “What’s New at MEASURE DHS?,” available at www.measuredhs.com/ (accessed April 11, 2012).v. According to the United Nations Statistics Division, only around 20 percent of African countries provided complete information on births and deaths for at least one year over 2003–07. See “Availability of Vital Statistics,” http://unstats.un.org/unsd/demographic/CRVS/VS_avail-ability.htm (accessed May 14, 2012).

36
Other than these global research and collaboration platforms, vari-ous specific or regional efforts support health technology assessment. The Cochrane Collaboration is a global initiative pulling together evidence to inform clinical decisions around the world. The Collabora-tion recently launched evidenceaid,vi a new initiative aiming to collate and evaluate evidence of effectiveness of interventions in disasters and humanitarian emergencies. The SUPPORT initiative is another attempt to help the application of evidence in policy and practice, through a series of articles.vii EUnetHTA looks into scientific coopera-tion within Europe and develops health technology assessment tools and methods for member countries. A newly formed organization, HTAsiaLink, is a regional network that connects health technology assessment units and practitioners in a number of Asian countries, hoping to increase the level of interaction and collaboration. There are also efforts to launch health technology assessment collaboration networks across Latin American countries, such as the Pan American Health Organization’s Regional Platform of Access and Innovation for Health, as well as the Comisión Técnica Subregional de Evaluación de Tecnologías Sanitarias, which works in the Andean subregion.
In development assistance partners’ work to fund or carry out different priority- setting activities, its efforts to support national policy making have mostly been limited to specific diseases, con-ditions, or types of technologies (such as drugs or vaccines), and focused on the generation of global evidence, rather than generating country-specific data, supporting country decision making, building national institutions, or facilitating exchanges and collaboration. The global health technology assessment collaboration networks are fragmented, lack a systematized approach to evidence genera-tion and know-how sharing for their members, and have limited LMIC representation. Figure 5.1 illustrates the concentration of donor effort in the development of evidence and the predominance of academic institutions in the execution of resources.
Donor and international agency priority- setting processesIdeally, health aid would align with recipient country priorities and track higher preventable disease burdens, but few donors allocate
vi. “Evidence Aid Project,” available at www.cochrane.org/cochrane -reviews/evidence-aid-project (accessed April 16, 2012).vii. “Support: For Health Policy Makers,” available at www.support -collaboration.org/ (accessed April 16, 2012).
their funding according to preventable disease burden. When con-trolling for health spending, income, and governance, disease bur-den was significantly related to funding allocation for only seven donors. Of 30 evaluated donors, 12 gave less to countries with higher disease burdens in 2009. Those that best allocated funding in rela-tion to disease burden were multilateral donors, including GAVI and the Global Fund, as well as certain bilateral donors, including the United Kingdom, Germany, and Denmark.viii However, few donors have the remit of looking across diseases and conditions when establishing priorities for funding.
viii. Analysis based on the Organisation for Economic Co-operation and Development’s 2009 Creditor Reporting System database. For more information, see Duran and Glassman (2012).
Figure 5.1Number of current global efforts to support domestic priority-setting
MDBs is multilateral development banks; NGOs is nongovernmental organizations; UN is United Nations.
Source: Authors’ analysis.
0
10
20
30
AdviceCollaborationTrainingEvidence
By category (not mutually exclusive)
0
5
10
15
NGOsGovernmentsUniversitiesUN/MDBs
By actors
Don
ors
and
dec
isio
ns

37D
onors an
d decision
s
Otherwise, various mechanisms such as sectorwide approaches or the International Health Partnership advocate aligning country priorities with national priorities, and while initial efforts have been made in this area, there still is room for improvement. For exam-ple, donors not participating in a sectorwide approach in Uganda decide and fund specific interventions outside of the health benefits plan defined by government in what is described as “a concurrent priority- setting process.”4
Only GAVI and the Global Fund have specific policies in place to decide which interventions and technologies can be funded with their monies. In the next section we discuss these mechanisms, identifying strengths and weaknesses.
GAVI Alliance prioritization mechanismsGAVI provides financing for vaccination, a health intervention that is generally considered highly cost-effective. Currently, GAVI accepts applications for pentavalent (DTP-HepB-Hib), HPV, measles second dose, meningitis A, pneumococcal, rubella, rotavirus, and yellow fever vaccines. GAVI uses a competitive application- based process to decide what grant proposals are funded by country. GAVI’s Inde-pendent Review Committee — which is responsible for reviewing new proposals and monitoring support to recipient countries — does not assess for value for money and does not do price benchmarking exercises for common “big ticket items”ix such as vehicles.5 During the grant application process, countries must provide adequate justi-fication for the vaccine introduction, including national or regional data on disease burden if available, as well as supporting financial and budgetary information, including: “(i) A situation analysis of the immunization program including socio-economic and gender barriers; (ii) Analyses of the current and future costing and financ-ing of the program.”6 However, without limits on supply and fund-ing, GAVI does not prioritize among high burden and low burden countries.x Funding for some vaccines, for example, meningitis A and yellow fever, are limited to countries for whom WHO has issued a recommendation due to the country-specific burden.xi
ix. The evaluation of the Independent Review Committee does not specify if this occurs during the evaluation of cash based grants as part of New and Underused Vaccine or Health System Strengthening Support. The Committee participates in the selection process and monitoring of both types of grants.x. Personal communication, Alex Placios (April 13, 2012).xi. Personal communication, Alex Placios (April 13, 2012).
In 2007–08 GAVI defined a new Vaccine Investment Strat-egy that assists the organization in deciding what vaccines will be GAVI-funded, based on criteria including cost-effectiveness, health impact, and vaccine delivery.xii Previous to this strategy, GAVI had made ad hoc investment decisions regarding vaccine incorporation. To begin the new process, GAVI evaluated a long list of 18 priority diseases expecting licensed vaccines by 2012, as determined by WHO’s Immunization, Vaccines and Biologi-cals.7 This vaccine pool was evaluated by processes including initial vaccine screening, country consultation, analysis by vaccine, and review. As of 2012 the GAVI vaccines that have become available through this process include HPV, typhoid, Japanese encephalitis, rubella, and meningitis A.xiii
In 2010 GAVI’s board also approved a mechanism that would rank technically sound proposals in the event that GAVI resources were limited in a particular application round. Under the procedure, countries are able to apply for multiple vaccines; however, GAVI will only fund a single vaccine per country per application round — which is meant to ensure equitable distribu-tion of funding across countries.xiv The proposals are then evalu-ated on the basis of the four criteria — health impact, value for money, financial sustainability, and need (table 5.1).8 However, this prioritization mechanism will only apply exceptionally, if not enough funding is available to cover all applications recom-mended by the Independent Review Committee. Should there be a short-term limit on supply — for example, a shortage of a particular vaccine — the health impact for the particular coun-try and vaccine becomes one of the main criteria for allocation of resources.xv
It is not clear why this prioritization process applies only in case of severe resource limitations. Box 5.1 discusses the recent adoption of the HPV vaccine by GAVI.
xii. “Which Vaccines to Invest in and When: GAVI’s Strategic Approach,” available at http://fr.gavialliance.org/vision/strategy/vaccine_investment/index.php (accessed April 14, 2012).xiii. “Vaccine Investment Strategy,” available at www.gavialliance.org/about/strategy/vaccine-investment-strategy/ (accessed April 13, 2012).xiv. “GAVI Alliance Pilot Prioritisation Mechanism,” available at http://fr.gavialliance.org/vision/programme_policies/prioritisation/index.php (accessed April 13, 2012).xv. Personal communication, Alex Placios (April 13, 2012).
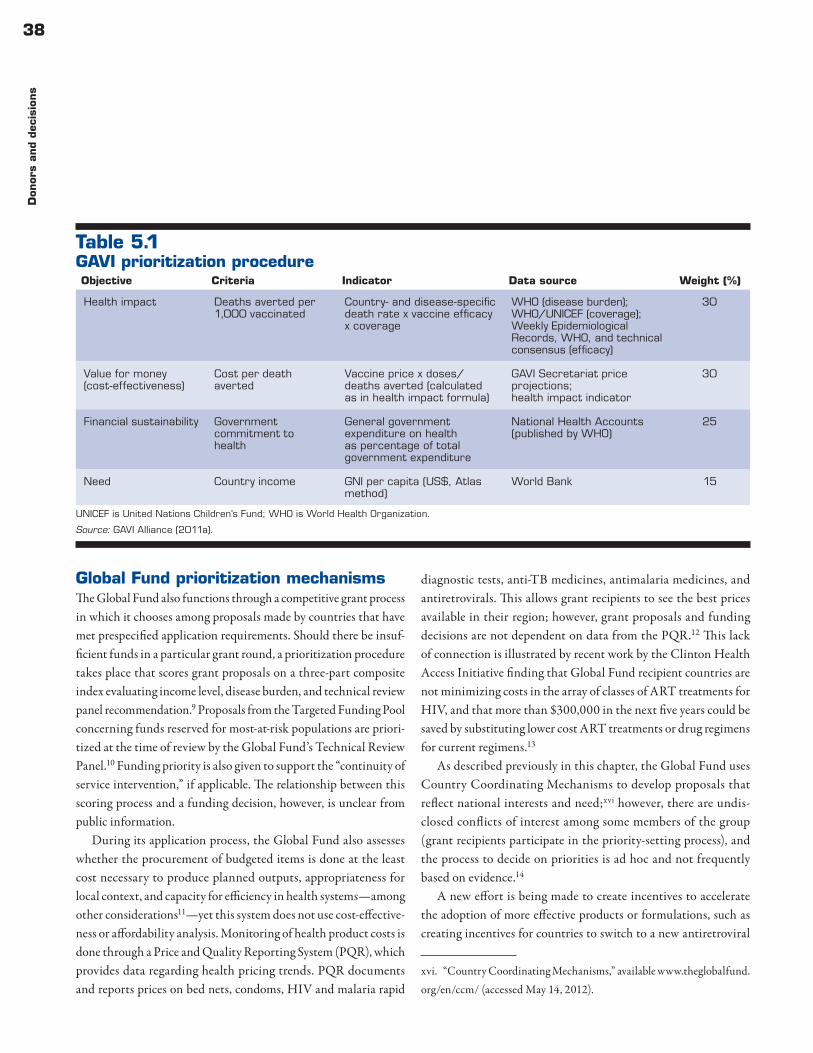
38D
onor
s an
d dec
isio
ns
Global Fund prioritization mechanismsThe Global Fund also functions through a competitive grant process in which it chooses among proposals made by countries that have met prespecified application requirements. Should there be insuf-ficient funds in a particular grant round, a prioritization procedure takes place that scores grant proposals on a three-part composite index evaluating income level, disease burden, and technical review panel recommendation.9 Proposals from the Targeted Funding Pool concerning funds reserved for most-at-risk populations are priori-tized at the time of review by the Global Fund’s Technical Review Panel.10 Funding priority is also given to support the “continuity of service intervention,” if applicable. The relationship between this scoring process and a funding decision, however, is unclear from public information.
During its application process, the Global Fund also assesses whether the procurement of budgeted items is done at the least cost necessary to produce planned outputs, appropriateness for local context, and capacity for efficiency in health systems — among other considerations11 — yet this system does not use cost-effective-ness or affordability analysis. Monitoring of health product costs is done through a Price and Quality Reporting System (PQR), which provides data regarding health pricing trends. PQR documents and reports prices on bed nets, condoms, HIV and malaria rapid
diagnostic tests, anti-TB medicines, antimalaria medicines, and antiretrovirals. This allows grant recipients to see the best prices available in their region; however, grant proposals and funding decisions are not dependent on data from the PQR.12 This lack of connection is illustrated by recent work by the Clinton Health Access Initiative finding that Global Fund recipient countries are not minimizing costs in the array of classes of ART treatments for HIV, and that more than $300,000 in the next five years could be saved by substituting lower cost ART treatments or drug regimens for current regimens.13
As described previously in this chapter, the Global Fund uses Country Coordinating Mechanisms to develop proposals that reflect national interests and need;xvi however, there are undis-closed conflicts of interest among some members of the group (grant recipients participate in the priority- setting process), and the process to decide on priorities is ad hoc and not frequently based on evidence.14
A new effort is being made to create incentives to accelerate the adoption of more effective products or formulations, such as creating incentives for countries to switch to a new antiretroviral
xvi. “Country Coordinating Mechanisms,” available www.theglobalfund.org/en/ccm/ (accessed May 14, 2012).
Table 5.1GAVI prioritization procedure
UNICEF is United Nations Children’s Fund; WHO is World Health Organization.
Source: GAVI Alliance (2011a).
Objective Criteria Indicator Data source Weight (%)
Health impact Deaths averted per 1,000 vaccinated
Country- and disease-specific death rate x vaccine efficacy x coverage
WHO (disease burden);WHO/UNICEF (coverage);Weekly Epidemiological Records, WHO, and technical consensus (efficacy)
30
Value for money (cost-effectiveness)
Cost per death averted
Vaccine price x doses/deaths averted (calculated as in health impact formula)
GAVI Secretariat price projections;health impact indicator
30
Financial sustainability Government commitment to health
General government expenditure on health as percentage of total government expenditure
National Health Accounts(published by WHO)
25
Need Country income GNI per capita (US$, Atlas method)
World Bank 15

39D
onors an
d decision
s
Box 5.1GAVI Alliance adoption of the HPV vaccine
(continued)
In late 2011 the GAVI Alliance Board announced its
intention to make the HPV vaccine available to GAVI-eligi-
ble countries, in large part based on cost-effectiveness
impact models constructed for Brazil, India, and Viet-
nam.1 These actions are supported by the World Health
Organization (WHO), among others, which recommends
comprehensive cervical cancer prevention plans that
include both vaccination of young girls and screening and
treatment of women. The global evidence underpinning
the GAVI adoption decision is strong. Yet the decision
to introduce does not plan for analyses of the cost-
effectiveness, affordability, and ethics of new technology
introduction in recipient countries themselves.
On cost-effectiveness. Is the HPV vaccine cost-
effective in a low-income country vis-à-vis alternative
uses of funding for health (or alternative approaches
to reducing cervical cancer)? At an earlier price point,
Thai researchers at the Ministry of Health found the
HPV vaccine to be cost-ineffective as an alternative to
scaled-up screening and treatment.2 In a model con-
structed by Kim et al. (2010) for the 72 GAVI-eligible
countries, the current GAVI price of $15 per girl was
thought to be unaffordable for most countries. Further,
global and regional models rely on very poor epidemio-
logical and cost data.3
Many current priorities also remain inadequately
funded — facility births, integrated management of
childhood illness, family planning, and so on. Is cervi-
cal cancer prevention, screening, and treatment the
next best use of funding? Countries should have their
own responses, but donors could help with analytical
support and collection of local epidemiology and cost
data to support an informed decision. To put this idea
in perspective, in the United States, a country that
spends 18 percent of GDP on health, eight studies of
U.S. data on the cost-effectiveness of the HPV vaccine
were reviewed before a decision about which to rec-
ommend was taken.4 Yet in settings where resources
are much more constrained and the opportunity costs
of the marginal dollar are significant, the global health
community asks that policy makers take a decision with
no studies of local efficacy or cost-effectiveness.
On affordability. Are HPV-related interventions afford-
able to low-income country governments in the medium
term, given price assumptions, co-financing require-
ments, and realistic donor flow projections? GAVI-eligibles
are spending $36 per capita annually on average. The
Expanded Program on Immunization (EPI), net of HPV and
rotavirus vaccine, is said to cost $62 per child.5 How
much money is left to pick up the new vaccines like HPV?
Affordability will imply that a country budget will be
able to finance the full costs and operations of the pro-
gram after GAVI and U.S. President’s Emergency Plan
for AIDS Relief support ends. Yet a paper on HPV vac-
cine costs and financing by Saxenian and Hecht (2006)
illustrated that — given fully loaded costs of $8–$25 per
vaccinated girl (a reasonable assumption given a $15
course of HPV vaccine) — it would cost an additional
1–3 percent of all public spending on health, a huge
outlay that would assume heroic levels of reallocation
or resource mobilization. In addition, reaching a new
cohort — young girls — would likely imply a significant new
investment for the average EPI program.
Further, in these cases, using the WHO GDP per
capita threshold for cost-effectiveness may do systems
more harm than good. A threshold ought to reflect the
“opportunity costs of resources for the programs that
would be curtailed or not financed if a new program is
undertaken.”6 Although a reduction in price makes the
vaccine look even more cost-effective according to the
WHO rule of thumb, it may still be unaffordable in a
low-income country, and therefore neither good value

40D
onor
s an
d dec
isio
ns
that will yield substantially greater value for money. In addition, the Market Dynamics Committee has suggested that health tech-nology assessment can be used more broadly to look at best value and affordability in the products purchased by the Global Fund.
ConclusionsAlthough substantial proportions of global health funding goes to cost-effective interventions and global public goods, in general, development assistance partners have provided only limited sup-port to country priority- setting processes and have not developed rigorous processes within their own agencies. Development assis-tance partner efforts to support national policy making can do more to generate country-specific data, support country decision making, build national institutions, or facilitate exchanges and collaboration.
Interestingly, although many efforts are global in scope, very few actions directly help development partners to decide which
technologies to support or finance, despite a growing number of newly available technologies and the context of declining global health resources. The push toward value for money is felt across all funding institutions; more systematic priority setting — both globally and nationally — can help and is proposed in chapter 6.
Notes1. Murray (1994).2. Evans et al. (2005).3. Goetghebeur et al. (2010). 4. Kapiriri (2012); Kapiriri and Martin (2010); Kapiriri,
Norheim, and Heggenhougen (2003).5. GAVI Alliance (2011b); Donoghue et al. (2010).6. GAVI Alliance (2011a), p. 4.7. GAVI Alliance (2009).8. GAVI Alliance (2007).9. The Global Fund (2011c).
Box 5.1 (continued)GAVI Alliance adoption of the HPV vaccine
for money nor cost-effective. Each country will need
its own empirical estimates of the cost-effectiveness
threshold to inform decision making.7
On the ethics of tradeoffs. What is the right mix of
vaccination, screening, and treatment that is cost-ef-
fective, affordable, and ethically acceptable, consistent
with local values and preferences? Would it be better to
cover young girls completely with vaccination first, and
only use “leftover” money for screening and treatment?
Or would a country prefer to screen and treat cases
that are already showing up in their health facilities?
An optimal HPV strategy still has to include a substan-
tial budget line for screening, as the vaccine does not
protect against all strains of the virus or account for
women already infected. Further, the time until health
gains are realized from a vaccine are 25 years or more
into the future — and international discount rates might
be different from national rates.
Ideally, the global health community could do it all.
According to its projections, GAVI has projected com-
mitments to cover a phased program of vaccine in-
troduction, including HPV, until 2023, for a total of
$1.32 billion.8 This is a significant but still limited pot
of resources and, in many countries, terrible choices
may have to be made.
Notes
1. “Impact Model References,” available at www.rho.org/
ap/ics-references.htm (accessed May 14, 2012).
2. Praditsitthikorn et al. (2011).
3. Jit et al. (2011).
4. Markowitz et al. (2007).
5. Saxenian and Hecht (2006).
6. Johannesson and Weinstein (1993).
7. Shillcutt et al. (2009).
8. Schwalbe (2011).

41D
onors an
d decision
s
10. The Global Fund (2011b).11. The Global Fund (2011d).12. The Global Fund (2011a).13. Amole et al. (2011).14. The Global Fund (2008).

42
Chapter 6
Building institutions for explicit priority setting
The Priority-Setting Institutions for Health Working Group sees opportunities to support the creation, expansion, and strengthen-ing of systems in low- and middle-income countries (LMICs) that inject an objective assessment of risks, benefits, costs, and value into decision making on publicly funded health services and technolo-gies. This decision making is often dominated by donor preferences, industry pressures, and other forces that reduce the health-optimiz-ing allocation of resources. This chapter sets out a framework for structuring explicit priority- setting processes, describes the insti-tutional requirements necessary to make these systems a reality, assesses obstacles to be overcome, and draws some conclusions.
After examining trends and characteristics in priority- setting pro-cesses and institutions worldwide and building on Giedion and col-leagues’ recommendation to analyze priority setting as a multistep process from a systemic perspective,i the Working Group adopted a “7+7 framework” that describes seven principles and seven core processes of priority setting. If this framework were implemented — ideally under an explicit legal and institutional frameworkii — it would have the potential to improve health for any desired level of health spending, while channeling and managing political, com-mercial, advocacy, and donor interests via a fair process.
Building on the collective experience of entities currently using health technology assessment (health technology assessment) to inform decisions, the Working Group recommends that health technology assessment system governance follow seven principles:
i. Giedion et al. (forthcoming). Note that the original source described 15 principles, which have been distilled to 7 for the purposes of this paper (Neumann et al., 2010).ii. Without a legal framework for setting up and using health technology assessment, it is difficult to ensure enforceability or budget. Equally, if the courts wish to enforce right to health legislation, but have no access to infor-mation and process related to evidence appropriateness and affordability, decisions will not have intended effects.
it should be scientifically rigorous, transparent, consistent, inde-pendent from vested interests, contestable, timely, and enforceable.1
A set of seven processes that can help implement the seven prin-ciples is described below, and is considered an “health technology assessment system” whose level of data and methodological com-plexity could be scaled according to country or funding agency circumstances. In this usage, “health technology assessment system” does not refer exclusively to the technical and analytic function of assessing an individual technology or intervention, but instead to the entire decision-making process and context, including the legislative, regulatory, policy, payment, and reimbursement frame-work within which evidence is developed and used. Additionally, the term “health technology assessment system” is chosen to reflect that priority setting involves multiple actors and processes, and is based on inputs provided by health systems, the legal framework, and social values prevailing in each society. The process can lead to different types of outputs such as coverage decisions, guidelines, protocols, or other evidence-based recommendations. The specific “health technology assessment system” emerges from a country’s priority- setting starting point — whether it is designing or adjusting a health benefits plan, establishing a positive or negative list, trying to accelerate access of cost-effective medical innovations for patients, or deciding whether or not to finance a specific new technology or service. The seven processes include the following:•Registration. Registration or marketing authorization is a first
step in the priority- setting process, especially in the case of technologies. Obtaining regulatory approval in the country is typically a first step toward becoming available, and pos-sibly a priority for public or donor spending. Some countries have used the registration process to proactively speed access to good value technologies, while others have been more pas-sive, letting the process be initiated by industry or donors. Increasingly, pharmacoeconomic evidence is required along with clinical data for drug applications. Once a technology is registered in a country, products diffuse quickly to those with

43B
uild
ing in
stitution
s for explicit p
riority setting
ability to pay, creating immediate pressure for a public sector coverage decision. Off-license use is also an issue.iii Further, the potential for synergies between regulators and payers at the registration stage is large, given that security and efficacy of analyzed products are important evaluation dimensions. It is important to note, however, that many health care interven-tions, including services, health promotion, human resources decisions, or service configuration interventions often fall out-side the remit of licensing systems.
•Topic selection and scoping. Depending on a country’s current assessment practices, it will be necessary to identify and select technologies — broadly defined — for evaluation. A poor country may start with a major, underaddressed burden of disease, such as cardiovascular disease, and examine prevention and treat-ment alternatives. In other cases a country may start from a costly device — for which the incremental value for money is suspected to be low — that, if funded, would potentially divert public monies from higher value uses. Or it might start with new technologies with great potential to generate health improve-ments or cost savings. Given more limited resources, the scoping exercise is especially challenging in LMICs where the number of technologies outside lists or packages will be large.
•Cost-effectiveness. A cost-effectiveness analysis or value for money of a technology should be undertaken using widely accepted methods, tools, and systematic evidence reviews. This is the area in which most global efforts to support LMICs to date have centered, but have not gone far enough to generate and use local data or establish local cost-effectiveness threshold ranges (as well as other decision criteria) for use by decision makers. Cost-effectiveness analysis should establish a comparative clinical or community health benefit and an incremental cost-effectiveness ratio, ideally combining local data on costs and use with inter-national data on efficacy, thus adapting and translating inter-national evidence to local circumstances. The identification of the appropriate counterfactual (ideally through an appropriately calibrated threshold), which may reflect previous adoption deci-sions,2 should be given particular attention to avoid the zero-based scenario and appropriately reflect the installed capacity
iii. Off-license use can be necessary (as in pediatric medicines) or inap-propriate (as in Colombia and the recent decision to use a certain brand of antiretroviral as prophylaxis).
of the health system. In addition, multiple quantitative criteria can be built into the cost-effectiveness analyses to reflect both health and nonhealth priorities in a country. For example, cost-effectiveness analysis can reflect equity considerations through differential weighting of health benefits, such as for different health states at different ages, a concern for poverty reduction through the incorporation of financial protection criteria,3 and different discount rates given the time preferences of a given soci-ety, among others. A preliminary recommendation to adopt or not adopt is then developed based on cost-effectiveness analysis, using a country-specific threshold.
•Budget impact. The budget impact of a preliminary recommenda-tion emerging from cost-effectiveness analysis should be assessed. Budget impact analysis is a tool to predict the potential finan-cial impact of the adoption and diffusion of a technology into a health care system. Whereas cost-effectiveness analysis can help assess the cost (or saving) for the additional health benefit gained from investment in a technology — such as the cost per additional disability-adjusted life year gained — budget impact analysis addresses the affordability of the technology, for exam-ple, the net annual financial cost of adopting the technology for a finite number of years. This is essential for LMICs that have highly constrained fiscal resources in the health sector, yet is almost never conducted as part of the introduction of new tech-nologies. A recent example is the adoption of the HPV vaccine by Rwanda.4 Tools like the Marginal Budgeting for Bottlenecks can be adapted for this use.iv
•Deliberative process. A deliberative process should be run to examine the results of the cost-effectiveness analysis or budget impact analysis; hear from stakeholders, including regarding the evidence that can inform cost-effectiveness analysis and budget impact analysis; and consider more subjective decision criteria such as the severity of conditions, the magnitude of individual health gain, the relative rarity of the disease condition, and tradeoffs with ethical implications.5 In processes worldwide, an appointed, multidisciplinary committee that publicly discloses conflicts of interest is tasked with making final technology fund-ing recommendations or decisions. Payers, providers, experts,
iv. Marginal Budgeting for Bottlenecks: UNICEF/The World Bank [online costing tool], available at www.who.int/pmnch/topics/economics/cost-ing_tools/en/index12.html (accessed May 14, 2012).

44B
uild
ing
inst
ituti
ons
for
explic
it p
rior
ity
sett
ing
and — sometimes — patient or public representatives are included in the deliberation, though voting members may be limited to a subset of the group. In some countries, industry/manufacturer representatives may attend as observers. Culyer (2008) describes the circumstances, common in LMICs, that make the use of deliberative processes in a health care priority setting necessary and relevant: “decisions have been delegated by a body with a democratic mandate to one without it; evidence from more than one expert discipline is involved; evidence from more than one profession is involved; stakeholders have conflicting interests; there are technical disputes to resolve and the evidence may be scientifically controversial; evidence gathered in one context is to be applied in another; there are issues of outcome, benefits, and costs that go beyond the conventional boundaries of medi-cine; there is substantial uncertainty about key values and risks that needs to be assessed and weighed; there are other social and personal values not taken into account in the scientific evi-dence; there are issues of equity and fairness; there are issues of . . . operational feasibility involving knowledge beyond that of the decision makers; and wide public and professional ‘own-ership’ is desired.” Setting up a fair, deliberative process around a technical recommendation for coverage allows for debate on the ethical and equity implications of decisions — such as who will receive antiretroviral drugs, given limited resources — while providing a space for different interest groups to air concerns or bring new evidence to the table for consideration.
•Decision. Decisions should be guided by the results of the evi-dence and recommendations produced by the processes of budget selection and scoping, cost-effectiveness, and budget impact. Recommendations should be considered by the appropriate authority, and a coverage decision taken and then linked con-tinuously to public budgets. While seemingly self-evident, the health benefits plan as well as the national health plan experience suggests that many policies and plans remain aspirational and unconnected to budget, or have only a one-time connection to budgets that can lead to erosion of effectiveness over time. While some advocate specific technology or program budget line items as the solution to this issue,v that approach is ultimately prob-lematic, as it is unconnected with individuals entitled to receive a
v. “Accreditation Process,” available at www.evidence.nhs.uk/accredita-tion/accreditation-process (accessed February 23, 2012).
given intervention or technology. Depending on the setting, the decision to fund or cover a service may be devolved by the payer (insurance fund or government) to the multistakeholder com-mittee carrying out the interpretation of the evidence through the deliberative process described in the budget impact process, or it may remain, at least at the earlier stages of the process, the responsibility of the payer at either the central or local levels. In the latter case, the reasons for rejecting or deferring a positive or negative recommendation ought to be made public and be contestable (see the next process).
•Appeals, tracking, and evaluation. Finally, a coverage decision and/or the underlying recommendation and associated analy-ses should be contestable via an appeals process. This can range from the “lighter” option of a public or peer review that may be triggered by a select group of stakeholders, to a full-scale appeal, which may include formal resubmission of evidence and a public hearing. It is important that the right balance be struck between offering the opportunity to challenge a decision publicly — potentially leading to its reversal — and ensuring that the overall process remains timely and insulated from, for exam-ple, vested commercial or professional interests. Such interests may, as they have access to relevant resources, be more likely to challenge and at least delay unfavorable decisions. Finally, a more elaborate appeal process may be more relevant in settings where legal challenges and perceptions of procedural weakness have been common, since it may reduce the chances of judicial reviews and enhance stakeholders’ faith in the decision-making process.
Just as decisions should be tracked and evaluated in the public domain, the implementation (degree of uptake) and longer term impact (in terms of health outcomes and/or budgetary impact) of decisions need to be monitored and reported. Uptake evaluation can drive data collection systems, which will in turn feed into further, better targeted and better informed updates of policies. It can also form the basis for performance assessment of purchas-ers and providers at the local level, through the identification of the most appropriate and least burdensome uptake metrics to be assessed. Finally, impact assessment can strengthen the case for using evidence and an independent process to inform coverage decisions, including on occasions where additional investment is needed. Making the financial case for further investment will likely become increasingly important both for global donors and LMIC ministries of finance.

45B
uild
ing in
stitution
s for explicit p
riority setting
A regular assessment of whether the process needs repeating is also necessary. For example, in the event of new safety data, the process would restart at the first step, or if new clinical or cost data become available, the process could restart at the third step. Regular review and update are critical in ensuring that decisions are based on credible processes and up-to-date information.A number of critical elements of a robust, sustainable health
technology assessment system do not fit directly within the seven processes described above. Priority-setting decisions must be made in the context of legal, statutory, and regulatory policies that may support or undermine the ability to implement these decisions. For that reason, there is often a need to design health technology assessment systems that are mindful of these contextual factors, and in some cases the successful implementation of health technology assessment-driven priority- setting policies will require reconsid-eration of statutes and regulations. Furthermore, because of the limited availability of information about comparative effectiveness of many health technologies and services, it will also be critical for the evaluation process to be linked to systems for evidence building to address critical uncertainties and high priority domains. Local or regional mechanisms for funding and implementing research will need to be organized to address questions that arise so that the objective of policy making driven by effectiveness and value can be more consistently achieved.
Together, the health technology assessment system — whether global or national — will increase the rigor and relevance of evidence considered, provide a fair and transparent mechanism to manage the politics of resource allocation, connect evidence-based decisions to budget, and create permanent institutional channels to consider resource allocation choices over time.
In box 6.1, we apply the 7+7 framework using a real case study from the British National Institute for Health and Clinical Excel-lence (NICE) and the British National Health Service (NHS), which examined whether to prioritize secondary prevention of myocardial infarction using pharmacological treatment as part of its pay for performance program (itself a type of positive list of interventions). It is worth noting that this was not a decision on the pharmaceutical agents themselves, but on whether the health service should adopt this type of pharmacological secondary prevention, and the analyses included the service configuration and feasibility aspects of implementing such an approach into the NHS. Britain has one of the best-developed systems of translating evidence into
policy; others include Canada, Sweden, New Zealand, and Aus-tralia. This need not mean that the NICE institutional standard is (or ought to be) the model for other countries. Every country has to develop its own mechanism for identifying priorities and acting on them based on context-specific evidence and values. Equally, our choice of example need not imply that implementing the 7+7 frame-work is unattainable in an LMIC setting. Indeed, countries such as Brazil, China, and Thailand are building similar mechanisms. We chose this example because of the accessibility of NICE data on its methods, processes, and individual decisions, and the fact that the study is in English. It is one of the better-documented cases of applying the 7+7 framework to real policy decisions.
Institutionalizing health technology assessment systems in low- and middle-income countriesSetting up a tailored version of the health technology assessment system described will depend on each country’s starting point for priority setting, but must recognize the need to assign key func-tions, budgets, and capacities to individuals and agencies in govern-ment charged with carrying out the tasks under consideration. As discussed in chapter 3, it is too often the case that priority setting occurs in an ad hoc, one-off manner in LMICs, without attention to the long-term institutional requirements needed to make the effort relevant for policy makers and budgets.
To inform country and donor support about these institutional design decisions, the Working Group examined health technology assessment institutions in high- and middle-income countries — their portfolio of functions; the legal character of the entities and their recommendations; each entity’s funding sources and budget requirements; and the human resources, time, and unitary costs of producing health technology assessment. The tables draw on work supported by the Inter-American Development Bank and pub-lished by Giedion et al. (2012), which describes health technology assessment entities in Europe (Germany, Netherlands, the United Kingdom), Latin America (Brazil, Chile, Colombia, Uruguay), and Australia, and adds the cases of Poland and Thailand from Work-ing Group members.
Table 6.1 describes how health technology assessment agencies are funded and gives their budgets as a proportion of total public spending on health. health technology assessment agencies’ costs range from 0.01–1 percent of total public spending on health, and

46B
uild
ing
inst
ituti
ons
for
explic
it p
rior
ity
sett
ing
Box 6.1Secondary prevention of myocardial infarction using pharmacological treatment in the U.K. National Health Service
(continued)
Registration. The four drug classes recommended for
secondary prevention of myocardial infarction are: ACE
inhibitor (or ARB, if intolerant), aspirin (or an alternative
antiplatelet), beta-blocker, and statin (unless a contra-
indication or side effects are reported). All four drug
classes have been registered in Europe with the Euro-
pean Medicines Agency (and in the United Kingdom by
Medicines and Healthcare products Regulatory Agency),
and all four are available in generic form at a price
lower than the branded generics, with ARBs being the
last class to lose patent (losartan was the first drug
in its class to become generic in March 2010, valsar-
tan followed in 2011, and candesartan and irbesartan
in 2012).
Topic selection and scoping.
• According to the Royal College of General Practi-
tioners and the National Collaborating Centre for
Primary Care, “the annual incidence of myocardial
infarction for men aged between 30–69 is about
600 per 100,000 and for women about 200 per
100,000. The British Heart Foundation (2004)
has estimated that there are about 147,000 MIs
[myocardial infarctions] per year in men of all ages
in the UK and 121,000 in women, giving a total
of 268 000 cases. In the UK, about 838,000
men and 394,000 women have had a myocardial
infarction at some point in their lives.”1
• Reducing mortality from cardiovascular disease
and secondary prevention of myocardial infarction
are listed as key national priorities in the British
National Health Service (NHS) Operating Frame-
work of 2007/20082 and the National Service
Framework for Coronary Heart Disease: Winning
the War on Heart Disease.3 These nationally set
priorities are important inputs in British National
Institute for Health and Clinical Excellence’s (NICE)
work program.
• Cost-effectiveness analysis. Based on published
research, the incremental cost of offering car-
diovascular disease medicines as secondary myo-
cardial infarction prevention, including the cost
of the drugs and the visit to the primary care
center, was estimated at £514.4 The incremental
benefit was estimated at 0.049 quality-adjusted
life years (QALYs). Therefore, the cost per QALY
was £10,816. Based on sensitivity analysis, phar-
macological secondary prevention is deemed to
be cost-effective even if the overall cost of the
intervention is twice as high as the estimated
one. Further, given the current levels (baseline) of
offering secondary prevention at a primary care
setting across the United Kingdom of 11.3 per-
cent of the patient group, and with a primary care
center level prevalence of myocardial infarction
of 0.75 percent, offering monetary incentives to
encourage secondary prevention also becomes
cost-effective.
Budget impact analysis. Using prescription and
prevalence data5 from IMS and the national Myocar-
dial Infarction Audit Project, Tariffs/Diagnosis-Related
Group costs; unit costs from the British National For-
mulary; and assumptions on the likely proportion of
people on two-, three-, and four-drug combinations as
practice changes over one year, the additional annual
net budget impact of rolling out secondary prevention
across the country for weighted drug combinations
ranged from £0.3 million to £2.1 million (starting from
a baseline current cost estimate of £9.2 million). The
cost of all four combinations is £195.6 a year per pa-
tient. Although the potential savings from implanting

47B
uild
ing in
stitution
s for explicit p
riority setting
Box 6.1 (continued)Secondary prevention of myocardial infarction using pharmacological treatment in the U.K. National Health Service
(continued)
secondary prevention were not quantified, the analysis
found that uncomplicated acute myocardial infarction
costs the NHS approximately £3,500, and 24 hours
in the cardiac intensive care unit costs approximately
£1,000 per day.
Deliberative process. A multidisciplinary committee6
of experts and laypeople, all of whom abide by a strict
conflict of interest policy, was convened by NICE as per
the published NICE process of operation.7 The commit-
tee discussed the evidence and made a recommenda-
tion as to whether the NHS ought to incentivize the
pharmacological secondary prevention of myocardial
infarction, which drugs should be included, and what the
size of the monetary incentive ought to be. In addition
to the clinical and economic data, the committee was
presented with results of field testing and stakeholder
consultation. The minutes of the discussion and all the
evidence were placed on NICE’s website. The commit-
tee recommended that a new indicator be included in
the NHS’s pay for performance in primary care: “The
percentage of patients with a history of myocardial
infarction (from 1 April 2011) currently treated with
an ACE inhibitor (or ARB if ACE intolerant), aspirin or
an alternative antiplatelet therapy, beta-blocker and
statin (unless a contraindication or side effects are
recorded).”8
Decisions. The NHS Employers’ organization and the
professional association of British general practitioners
will make the final decision as to whether pharmacologi-
cal secondary prevention of myocardial infarction will
become part of the NHS’s pay for performance (P4P)
scheme for primary care doctors across the country.
During their annual negotiations, the two parties can
choose from a menu of indicators/activities, evaluated
and recommended by NICE’s committees. For 2011/12
the two parties agreed to include the secondary preven-
tion indicator in the P4P scheme.9
Appeal, tracking, and evaluation. Compliance with
the P4P guidance (introduced in 2011) on secondary
prevention of myocardial infarction will be evaluated
through annual assessment of data collected through
the online General Practitioners Results Database, and
primary care centers will be rewarded accordingly. In
the meantime, there is evidence of uptake of NICE’s
advice on secondary prevention, with 95.5 percent of
post–myocardial infarction patients receiving at least
one of the recommended medications.10 In addition, data
on cardiovascular disease mortality are regularly col-
lected through the national audit (Myocardial Ischaemia
National Audit Project) and overall NHS performance is
assessed against the 2011/12 Outcomes Framework.
Finally, the costs of prescribing and the percentage of
generic prescribing (also incentivized by NICE and the
NHS) for select drug classes such as ACE inhibitors and
statins, are monitored by region, and benchmarking
data are made publicly available through NHS Prescrip-
tion Services.11
The recommendation and final decision are regularly
reviewed as new clinical evidence emerges, including
effectiveness and safety information, and also as unit
costs and use volumes may differ from year to year
or new pharmaceutical products may be introduced
to the U.K. market. The clinical guideline underpinning
the recommendation on secondary prevention is being
reviewed. The grounds for the review include the fact
that patents on the antiplatelet agent clopidogrel have
expired in the United Kingdom; and new trial data show
that the clinical effectiveness of ARBs is similar to that
of ACE inhibitors, while combination of the two is not
clinically better than monotherapy.12
48B
uild
ing
inst
ituti
ons
for
explic
it p
rior
ity
sett
ing
in Europe and Latin America these entities have been primarily financed from general revenues and budgets. Thailand’s HITAP is funded in part by donor contracts for specific studies (World Bank, World Health Organization, Rockefeller), while Australia’s Pharmaceutical Benefits Advisory Committee and the Agency for Health Technology Assessment in Poland are funded by fees col-lected from pharmaceutical industry firms.vi
Table 6.2 describes the human resources employed in support of priority setting, the time required to produce a recommendation, and the cost per assessment. Human resource requirements vary greatly depending on the extent to which analyses are carried out “in-house” or contracted out. In Poland health technology assessment studies are frequently outsourced to national and foreign universities since the agency is small and depends on outside expertise, while in Thailand, most studies are conducted in-house so as to increase the confidence of stakeholders in the unit’s relevance and recommen-dations. However, conducting studies in-house generally requires a smaller annual production, given limited human resources.
A key issue highlighted by table 6.2 is the time required to produce a single health technology assessment study on a given
vi. On Australia’s fee-based PBAC, see www.pbs.gov.au/info/industry/listing/elements/fees-and-charges (accessed May 14, 2012).
technology, which ranges from 3 to 18 months. This time require-ment demonstrates the infeasibility of “quick” benefits plan designs and adjustments as currently practiced by some countries and inter-national agencies; yet it also demonstrates the potential gains from greater regional and global collaboration in the conduct of health technology assessment. While it is necessary to use local data to inform analyses and local processes to examine and deliberate on the evidence, it is not necessary to repeat studies in every country, particularly given the expense involved in carrying out a health technology assessment study (last column).
Obstacles and mitigating strategies in institutionalizing health technology assessment systems in low- and middle-income countriesThe Working Group has identified six major obstacles to the further development of health technology assessment systems in LMICs, and developed a series of risk-mitigating strategies.
Unmanageable scope, urgent demands. As noted earlier, many benefits plans are designed under unreasonable time frames asso-ciated with a window of opportunity for broader health reform. Such efforts will result in a list and some notional costs but, to mitigate the risks associated with this usual practice, efforts must
Box 6.1 (continued)Secondary prevention of myocardial infarction using pharmacological treatment in the U.K. National Health Service
Notes
1. Cooper et al. (2007).
2. U.K. Department of Health (2006).
3. U.K. Department of Health (2004).
4. NICE (2010a).
5. NICE (2010b).
6. NICE (2010d).
7. NICE (2009).
8. NICE (2010d), p. 1.
9. British Medical Association (2011).
10. “Quality and Outcomes Framework: Online GP
practice results database,” available at www.qof.
ic.nhs.uk/index.asp (accessed May 14, 2012);
“Summary of Results: Cardiovascular,” available
at www.nice.org.uk/usingguidance/evaluation
andreviewofniceimplementationevidenceernie/
searchernie/resultsummary.jsp?o=11008
( accessed May 14, 2012).
11. “Low Cost Lipid Modifying Drugs,” Available at
www.nhsbsa.nhs.uk/PrescriptionServices/3425.
aspx (accessed May 14, 2012).
12. NICE (2010c).
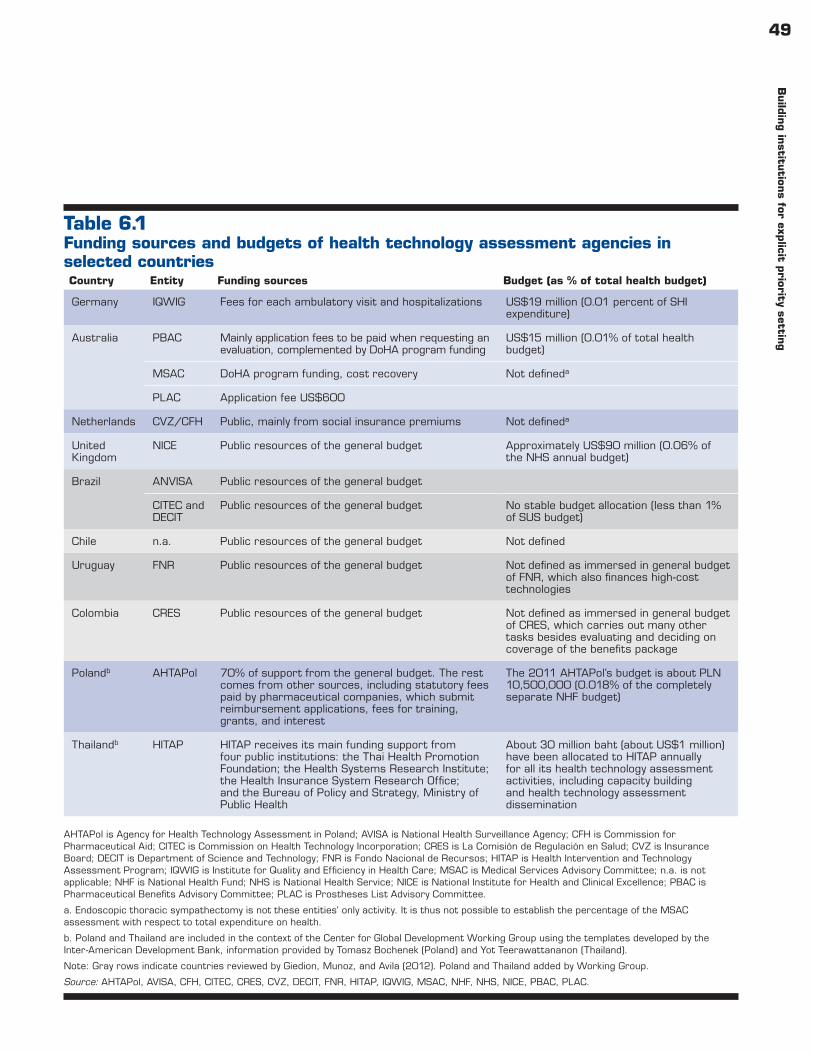
49B
uild
ing in
stitution
s for explicit p
riority setting
Table 6.1Funding sources and budgets of health technology assessment agencies in selected countries
AHTAPol is Agency for Health Technology Assessment in Poland; AVISA is National Health Surveillance Agency; CFH is Commission for Pharmaceutical Aid; CITEC is Commission on Health Technology Incorporation; CRES is La Comisión de Regulación en Salud; CVZ is Insurance Board; DECIT is Department of Science and Technology; FNR is Fondo Nacional de Recursos; HITAP is Health Intervention and Technology Assessment Program; IQWIG is Institute for Quality and Efficiency in Health Care; MSAC is Medical Services Advisory Committee; n.a. is not applicable; NHF is National Health Fund; NHS is National Health Service; NICE is National Institute for Health and Clinical Excellence; PBAC is Pharmaceutical Benefits Advisory Committee; PLAC is Prostheses List Advisory Committee.
a. Endoscopic thoracic sympathectomy is not these entities’ only activity. It is thus not possible to establish the percentage of the MSAC assessment with respect to total expenditure on health.
b. Poland and Thailand are included in the context of the Center for Global Development Working Group using the templates developed by the Inter-American Development Bank, information provided by Tomasz Bochenek (Poland) and Yot Teerawattananon (Thailand).
Note: Gray rows indicate countries reviewed by Giedion, Munoz, and Avila (2012). Poland and Thailand added by Working Group.
Source: AHTAPol, AVISA, CFH, CITEC, CRES, CVZ, DECIT, FNR, HITAP, IQWIG, MSAC, NHF, NHS, NICE, PBAC, PLAC.
Country Entity Funding sources Budget (as % of total health budget)
Germany IQWIG Fees for each ambulatory visit and hospitalizations US$19 million (0.01 percent of SHI expenditure)
Australia PBAC Mainly application fees to be paid when requesting an evaluation, complemented by DoHA program funding
US$15 million (0.01% of total health budget)
MSAC DoHA program funding, cost recovery Not defineda
PLAC Application fee US$600
Netherlands CVZ/CFH Public, mainly from social insurance premiums Not defineda
United Kingdom
NICE Public resources of the general budget Approximately US$90 million (0.06% of the NHS annual budget)
Brazil ANVISA Public resources of the general budget
CITEC and DECIT
Public resources of the general budget No stable budget allocation (less than 1% of SUS budget)
Chile n.a. Public resources of the general budget Not defined
Uruguay FNR Public resources of the general budget Not defined as immersed in general budget of FNR, which also finances high-cost technologies
Colombia CRES Public resources of the general budget Not defined as immersed in general budget of CRES, which carries out many other tasks besides evaluating and deciding on coverage of the benefits package
Polandb AHTAPol 70% of support from the general budget. The rest comes from other sources, including statutory fees paid by pharmaceutical companies, which submit reimbursement applications, fees for training, grants, and interest
The 2011 AHTAPol’s budget is about PLN 10,500,000 (0.018% of the completely separate NHF budget)
Thailandb HITAP HITAP receives its main funding support from four public institutions: the Thai Health Promotion Foundation; the Health Systems Research Institute; the Health Insurance System Research Office; and the Bureau of Policy and Strategy, Ministry of Public Health
About 30 million baht (about US$1 million) have been allocated to HITAP annually for all its health technology assessment activities, including capacity building and health technology assessment dissemination

50B
uild
ing
inst
ituti
ons
for
explic
it p
rior
ity
sett
ing
be made — perhaps as part of the reform legislation — to assure that a long-term process or institution is built and charged with updating and revising plans, coverage decisions, or negative lists. The multi-lateral development banks — as agencies that frequently provide technical assistance and funding for the development of benefits plans — can assure that institutions and processes are part of the agenda for policy dialogue.
Our case studies have shown that scaling up is the most practical mitigating strategy. The Thai, Polish, and Colombian experiences suggest that — initially — a small-scale effort is not only most fea-sible, but also builds confidence on the approach and methodology;
educates policy makers to create demand; and trains professionals and stakeholders involved in deliberations to prepare, oversee, and understand the evidence, through the pilot evaluation of one or two key health burdens or technologies. The Supporting Independent Immunization and Vaccine Advisory Committees Initiative and Malaria Vaccine Initiative programs are the seeds of such efforts that have yet to be connected with a permanent institutional entity, bud-get affordability assessments, and budget decision making. Where the courts or Congress have been active in legislating health pri-orities, it will be vital to involve both entities in the design of the process and the small-scale pilot.
Table 6.2Staffing, time requirements, and costs for health technology assessment agencies in selected countries
(continued)
Country Entity Staff
Time needed to produce a health technology assessment
Cost per health technology assessment
Germany IQWIG Total 122 employees (as of 2011) Full reports, approximately 18 months; rapid reports, approximately 4–6 months; dossier-assessment, 3 months
US$65,000–650,000
Australia PBAC 18 members in committee; more than 40 support staff (within MoH); 5 contracted external evaluation groups
17 weeks; dossier assessment 8–9 weeks
Approximately US$60,000
MSAC 4 executives and approximately 20 additional staff with expertise in clinical medicine, health economics, and consumer matters
13 months (12–13 evaluations are conducted every year)
Approximately US$250,000
PLAC 16 total staff; independent board with members having expertise in clinical practice, health insurance, consumer health, health economics, health policy, private hospitals, and the medical device industry
n.a.; list updated semi-annually
n.a.
Netherlands CVZ /CFH CFH has a secretariat of 15 staff and 22 external experts
n.a. n.a.
United Kingdom
NICE Approximately 500 total staff 7–14 months US$320,000–400,000/CPG; from US$90,000 for a review of manufacturers’ submission to US$230,000 for a de novo systematic review and decision model

51B
uild
ing in
stitution
s for explicit p
riority setting
Capacity shortfalls. The availability of enough capacity to carry out clinical and economic evaluations is a major feasibility concern. However, while capacity to undertake these evaluations is often limited in-country, the entity could call for national-international partnerships to prepare core evidence packages, or simply contract out to a foreign university with expertise (as in Poland in some cases). In parallel, as has been done in Thailand, scholarships and sabbaticals can be arranged to build more capacity in the medium term. Finally, capacity building driven by demand and within the context of a budding health technology assessment system may be the most efficient way of developing fit-for-purpose human resources. This is what the Thai model has shown, and it is an experience shared by relatively resource-rich countries such as England, where health economic capacity burgeoned in response to NICE’s requests for evaluations.
Unclear roles and responsibilities in fragmented settings. Many countries struggle with existing priority- setting arrangements that are fragmented among multiple agencies and individuals. What is needed is a baseline mapping of who does what, in order to build a coordinated priority- setting policy and understand whether a new institution or process is required and where it should be positioned, or whether the institutional functions and processes should be assumed by an existing entity. Such an analysis has been carried out in Colombia during the preparatory phase of the design of a new health technology evaluation institute.6
Weak governance and corruption. Given the emphasis of cur-rent institutions on the role of expert and stakeholder committees to consider the evidence and reach a recommendation, there is a worry that such processes may be illegitimate if subject to political manipulation or if the top leadership does not support the concept.
Table 6.2 (continued)Staffing, time requirements, and costs for health technology assessment agencies in selected countries
a. Poland and Thailand are included in the context of the Center for Global Development Working Group using the templates developed by the Inter-American Development Bank, information provided by Tomasz Bochenek (Poland) and Yot Teerawattananon (Thailand).
Note: See abbreviations in table 6.1. Gray rows indicate countries reviewed by Giedion, Munoz, and Avila (2012).
Country Entity Staff
Time needed to produce a health technology assessment
Cost per health technology assessment
Brazil CITEC/DECIT
Approximately 30 total staff Quick review, 3 months; primary studies, 1–2 years
US$15,000–150,000
Chile CCA/MoH Production of technical studies conducted by MoH
Not clear Not clear
Colombia CRESCCA Total staff 63, of which expert commissioners and 20 technical with expertise in clinical medicine, economists, public policy, statisticians, actuarial sciences
3–4 months Approximately US$6,000–10,000US$ 250,000/GPC
Uruguay FNR Most studies contracted out; 6 institutes and about 60 experts are producing most assessments upon request of FNR
Approximately 3 months US$ 3,000–15,000
Polanda AHTAPol Approximately 55 total staff The time duration of preparing full health technology assessment reports varies; generally a couple of months
Approximately US$ 28,000–34,000
Thailanda HITAP 50 staff (39 researchers and 11 administrative)
9–12 months 500,000 baht (US$17,000; not including dissemination)

52B
uild
ing
inst
ituti
ons
for
explic
it p
rior
ity
sett
ing
There are ways to manage these threats: through clearly set-out pro-cedural rules for engagement, conflict of interest disclosures, and audits; elections within professional bodies; limits on voting rights of government and committee chairs; and engagement of civil soci-ety and experts, among others. The role of physicians’ organizations has been mixed, but professional engagement and buy-in are key for a functioning process of priority setting. And while clinical engage-ment and leadership, as well as service user involvement throughout priority- setting processes, are essential, there is a need to ensure that professional and commercial interests do not capture the process of evidence assessment and decision making. In many LMICs, for example, there is a need to distinguish between physician-led sci-entific associations, and unions focused on wage negotiations or patient organizations funded by the industry.
However, it is worth noting that priority- setting entities and processes supported by external donors already are in place in many low-income countries. At least one priority- setting com-mittee exists in every Global Fund beneficiary country, including the most impoverished fragile states — the Country Coordinating Mechanism (CCM). Yet, despite adequate funding and a mandate, the CCM seldom uses locally adapted cost-effectiveness and budget impact studies to decide on the optimal mix of technologies, does not assess whether its budgets reflect true costs or whether efficien-cies can be attained, does not always assess the availability of new technologies that might be cost-saving or more effective, sometimes fails to address the rationing problem directly, and so forth. The CCM also lacks a defined process to carry out its functions. At least in this context, it seems feasible to build CCM capacity to set priorities more rigorously and in consultation, possibly building on economies of scale at a regional level.
In the end, for any health technology assessment/priority- setting activity to gain traction within a country, there ought to be a clearly articulated political demand and longer-term political backing (within and outside the country in cases where foreign donors have a significant say in what gets funded). Without such backing, any attempt to rationalize priority setting, build capacity, and generate data will be unlikely to succeed.
Intransigent data problems. In low-income settings particularly, there will be very limited data with which to carry out clinical and economic evaluations. Beyond the inevitable suggestion that more support be given to the production of these data (and asking for what is needed is a start), in the interim, countries may need
to rely on data from “similar” countries, efficacy and effectiveness estimates from studies conducted elsewhere, assumptions about cost and use based on small samples, and outdated demographic projections. While this will be frustrating, problematic studies may galvanize greater demand for measurement, and perhaps motivate donors to support routine consolidated data collection and disease surveillance at scale. Alternatively, entities themselves can com-mission original data collection. A donor-funded project in India, for example, is collecting representative data on costs in primary health care clinics as an input into a more accurate cost-effectiveness estimate and affordability analysis.7 Nevertheless, it is important to acknowledge that there will be limited evidence and consequent uncertainty about value for different technologies and in different contexts. However, as things stand, similarly important decisions are taken with even less relevant data and without an open acknowl-edgement of the uncertainty and potential perverse impact of such decisions. The ability of a health technology assessment system to update and revise analyses and reconsider recommendations is thus an important feature.
Weak links to decision making. A final problem encountered in many health technology assessment systems in high-income coun-tries is the limited connection between the assessment programs and decision making. More progress has been made recently, though for many years the technical production of health technology assess-ment reports received only limited attention in coverage, benefit, or budgetary decisions. It is possible that a similar phenomenon could occur in LMICs; in Malaysia, for example, while health technology assessment conducted within the Ministry of Health on drugs has an impact on listing in the ministry’s formulary, health technology assessment on devices and practices has no impact on reimbursement decisions.8 In a study in Latin America policy makers identified the lack of a transparent and clearly defined link between health technology assessment and the decision-making processes as a major barrier to the effective application of health technology assessment to resource allocation decisions.9 This risk is mitigated by the more pronounced fiscal pressures under which LMICs operate, lessons learned from the high-income countries, and potentially proactive global support to an integral health technology assessment system.
ConclusionsWith the goal of improving health impact given scarce resources, international experience suggests that it is possible to establish a

53B
uild
ing in
stitution
s for explicit p
riority setting
standardized ex ante priority- setting system for the inclusion and exclusion of technologies in a health benefits plan or a health care provision system. Although no single best method exists, there are examples of standard processes from all over the world. Such pro-cesses could also be used to inform policies among development assistance partners that fund service delivery in LMICs.
Cost-effectiveness is not the only mechanism for including or excluding technologies or funding services, but it is one of the most important if priority setting is intended to achieve greater value for money. For both countries and development assistance partners, affordability of new technologies and services is an important issue to consider, particularly given newly introduced co-financing and sustainability policies as well as the broader drive for universal health care coverage. The definition of explicit priority- setting mechanisms such as cost-effectiveness analyses can contribute to the development of a transparent and legitimate process of priority setting.
Deliberation based on the evidence is another element missing from many existing priority- setting processes, in spite of the signifi-cant political, economic, and patient interests at play in decision
making. In other cases, as in the Global Fund Country Coordi-nating Mechanisms, deliberation frequently takes place without evidence or disclosure of conflicts of interest.
Potential obstacles to the development of health technology assessment systems in LMICs can be overcome, but it will take time. In chapter 7 we suggest directions for future global support and regional networking.
Notes1. Yothasamut, Tantivess, and Teerawattananon (2009).2. Johannesson and Weinstien (1993); Culyer and Sculpher
(2008).3. Smith (2012).4. Binagwaho, Wagner, and Nutt (2011). 5. Miljeteig et al. (2009).6. IDB (2012).7. Doherty and Govender (2004).8. Shafie (2011).9. Pichon-Riviere et al. (2010).

54
Recommendations for actionChapter 7
The Working Group recommends direct, substantive support for the creation and development of both domestic and global health technology assessment systems. Within domestic priority- setting activities, the Working Group has made a distinction between strategies relevant to middle-income countries and those relevant to low-income countries. To accomplish this recommendation, a global health technology assessment facility should be created to provide sustained technical and consultative support to both low- and middle-income country (LMIC) governments and global health funders.
Given conflicting views and competing interests, the process of setting priorities or rationing health care is inevitably a process of debate. It is a debate that must be centrally informed by cost-effectiveness and other kinds of evidence and analysis but can-not be resolved by science or decision-making rules alone. Getting the institutional setting of this perennial debate right is critical; Rudolf Klein has argued: “I give primacy to institutions . . . unless we strengthen our institutional capacity to analyze evidence, to clarify policy choices and to promote informed debate, generating more information is more likely to compound confusion than to lead to better decision-making.”1
This report has looked at global and national efforts to sup-port better rationing of public funding in LMICs, and found a great neglect of the institutional settings and capacities necessary to make the rationing process work for better health. In this con-cluding section, the Working Group recommends direct support to the creation of both domestic and global health technology assessment systems.
Direct support to LMICs creating or developing their own health technology assessment systems could take several forms. Existing capacity-building efforts via evidence creation, tools, and methods could be more directly targeted to government counter-parts charged with carrying out priority- setting work. Further, hands-on technical pilots and demonstration projects — from the
relevant starting point — would be a way to engage with policy makers on real-time concerns. For example, advice and financial support to generate data on effectiveness, efficacy, medical prac-tice, and patient use patterns in-country has been highlighted as a priority in Asia.2
Coaching through procedural advice and knowledge exchange among countries, facilitated by a global facility or a regional net-work, will also be essential. Exchanging examples of legislation, process guidelines (including conflict of interest management), handling of confidential data, stakeholder involvement, and over-all governance and oversight can prevent “reinventing the wheel.” Providing support to communications and public awareness-raising can also be useful to build stakeholder support and demonstrate the commonality of problems and solutions.
The Working Group drew an important distinction between low-income countries and middle-income countries, by the need to develop health technology assessment system options for low-income settings that would build on bodies like National Immunization Technical Advisory Groups and Country Coordinating Mecha-nisms that are — in some cases — already setting priorities for public and donor budgets. Even in countries that only use health benefits plans in the context of results-based financing or performance-based contracting and where donors take a more direct role in priority setting, a version of a health technology assessment system could be put in place, which would relieve donors of the difficult techni-cal and ethical decisions that are taking place implicitly, without adequate technical justification, and without local participation.
Global funders themselves have an ongoing need for rigorous eco-nomic evaluation of technologies to be funded, from antiretroviral medication to bed nets to determining the best strategy for funding cardiovascular disease prevention and multidrug-resistant tuber-culosis control. For example, a comparison of least-cost equivalent antiretroviral therapy with the standard first-line regimens in 43 World Health Organization (WHO) focus countries finds that 59 percent of countries — with limited or no explicit rationale — use

55R
ecomm
endation
s for action
drug combination regimens that are more expensive but equally effective compared to available alternatives, demonstrating the possibility for funders to achieve similar results at a reduced cost by systematically evaluating alternative technologies using health technology assessment.
A global health technology assessment facility might under-take the accreditation of national health technology assessment systems and evaluations. Building off the Working Group’s find-ings and recommendations as well as instruments already devel-oped to assess clinical guidelines,3 it would be possible to develop standards for a system that would establish the full range of ana-lytic and decision-making components of a working system. Func-tional and quality standards might include basic analytic skills sets, a defined relationship to decision-making authorities, trans-parency, public engagement, appeals, health technology assess-ment/regulatory alignment, appeals mechanisms, basic analytical methods standards, and a link to research priorities, among others. Donors such as the Global Fund to Fight AIDS, Tuberculosis and Malaria could require that accredited health technology assess-ment systems be in place and in use as a condition of grants and loans. The facility could also track the health and budget impact of coverage decisions in a selection of countries over time, to inform future reforms.
A global health technology assessment entity could also derive economies of scale in the generation and adaptation of evidence dossiers, following toolkits and glossaries already developed.4 As new technologies come online, there is little need for each coun-try to repeat core analyses, but a great need to appropriately adapt health technology assessment conducted in other countries to the domestic epidemiological, cost, and use profiles. Recent work on a geographic “transferability checklist” for health technology assess-ment will also be useful.5 There are also great synergies in the shar-ing and benchmarking of coverage decisions among countries at similar levels of GDP per capita. A simple strategy could provide local decision makers with the ammunition needed to adopt a new cost-effective technology, to tailor high-cost interventions to high-need subgroups, or to say no to inappropriate and expensive interventions. This approach has been used by the Inter-American Development Bank in the context of a regional project and has been used to inform coverage decision making during a 2010 update of Colombia’s benefits plan.6
Building off the report’s findings, table 7.1 summarizes “do’s” and “don’ts” for international agencies and donors seeking to sup-port systematized priority- setting efforts in LMICs. Among the recommendations, the working group particularly called on inter-national funders, especially organizations such as the WHO and
Table 7.1Do’s and don’ts for international agencies and global health funders
HTA is health technology assessment.
Source: Authors.
International agencies and donors should start:
• Supporting a global HTA facility and national HTA accreditation processes as conditions for funding
• Viewing HTA and priority setting integrally, minimizing duplication of effort
• Respecting country decisions on public spending priorities and monitoring whether co-financing requirements are consistent with priorities
International agencies and donors should stop:
• One-off consultancies to “define the package”
• Introducing new technologies with no regard to opportunity costs and affordability
• Generalizing global or regional costs, effectiveness and social preferences data to specific country settings
• Using implicit rationing to decide who gets what
• Treating medicines, devices, interventions, and diseases as separate HTA categories

56R
ecom
men
dati
ons
for
act
ion
the World Bank, and multinational pharmaceutical companies to limit the use of health technology assessment conducted in one setting for a different setting, especially when the studies involve economic parameters and social preferences. A recent proposal by the Pan American Health Organization (PAHO) to its 150th Executive Committee illustrates one way forward — a draft resolu-tion calling on member countries to build, institutionalize, and use health technology assessment systems to define which technolo-gies to include or exclude from public funding for health and on PAHO to provide integral support to countries in the development of health technology assessment policies and institutions, to facili-tate knowledge and know-how exchange, and to develop a regional strategy and network.7
The support of a global health technology assessment facility would be guided by a deep, current knowledge of the history and best practices of health technology assessment systems developed in other countries, applying lessons learned in those situations to ensure that best practices are replicated and common mistakes are avoided. Above all, a tailored approach to technical assistance, with practitioners in each country relating directly to one another, will be useful and will help protect and enhance the independence and status of those charged with carrying out this very difficult task.
In short, the proposed functions of a global health technology assessment facility are:•Accredit health technology assessment systems and institutions
in LMICs (possibly through a self-assessment of competencies), and work to include phased accreditation requirements as condi-tions for external funding.
•Undertake research to increase the allocative efficiency of both global health donors and national health systems.
•Serve as a hub of know-how, technical assistance, and knowledge brokerage on institutionalizing health technology assessment systems and on the design/adjustment of health benefits plans, defining best practices and evaluating results, at the service of LMIC governments and global health funding agencies through a practitioner-to-practitioner approach of knowledge sharing.
•Generate economies of scale in the generation and adaptation of evidence dossiers for specific LMICs, applying toolkits and glossaries already developed, in order to avoid duplication of effort and save money.
•Benchmark and compare coverage decisions (through GDP per capita normalization, for example) on high-cost drugs and
devices worldwide, as an input to decision making where local health technology assessment analysis is not possible.
•Build and support regional networks of policy makers and prac-titioners, such as HTAsiaLink.
•Work to maximize the consistency of the methods and evidence included in health technology assessment, in cooperation with existing networks working on harmonization. This will reduce the burden to industry and to product development partnerships.
•Facilitate dialogue between health systems and industry to ensure that the benefits of new technology and system needs are mutually understood and reflected in price and availability.
•Be of use both to countries with health technology assessment agencies and those without them.In order to carry out these functions, the facility will require a
set of capacities:•An ability to work with and mobilize expertise from health tech-
nology assessment agencies and academic institutions around the world, in order to allow for a practitioner-to- practitioner model of technical assistance and just-in-time support to decisions.
•An ability to attract and retain world-class health technology assessment experts to assist LMICs directly in accreditation or health technology assessment system development.
•An ability to ensure independence and transparency.•A financial model that is self-sustaining, although seeded by
initial donations or support, ideally from health technology assessment pioneers in LMICs like Brazil, Poland, and Thailand or from countries that are investing heavily in their health care systems and are committed to evidence of return on investment, such as China and Turkey.
•A governance model that assures independence and rigor, while permitting engagement with governments and stakeholders involved in health technology assessment around the world.
•Close coordination with the WHO and the PAHO.
Looking aheadLMICs are facing a twofold challenge in health financing. Health aid is set to flat-line and drop, particularly for middle-income coun-tries. But domestic pressures from increased demand, aging, new technologies, and the transition from infectious to chronic diseases bring an upward pressure to health care costs. These trends are too serious to be ignored, and are set to define budgets in LMICs for decades to come.

57R
ecomm
endation
s for action
In this report we make the moral and economic case for respond-ing to these trends by improving the health impact of resource allocation and systematizing priority- setting processes. Given the global economic outlook and anticipated drops in aid, how LMICs spend their own money will be a major determinant of the size and pace of health improvement. Helping countries develop health technology assessment systems that will increase value for money is one way forward.
Notes1. Coulter and Ham (2000), p. 24.2. Yang and Lee (2009).3. Goeree et al. (2011).4. Teerawattananon, Russell, and Mugford (2007).5. Chase et al. (2009).6. Doherty and Govender (2004). 7. PAHO (2012).


Appendixes

60
Appendix A
Profiles of Working Group members
Sara Bennett is an Associate Professor in International Health and Health Systems at Johns Hopkins School of Public Health. Her background is in the politics and economics of health systems. She has previously studied issues in health financing, the role of the private sector, health worker motivation, changing roles of govern-ment, and the impact of global health initiatives on health systems. Her current interest is in understanding and addressing some of the institutional and capacity challenges in promoting stronger governance for health in developing countries.
Tomasz Bochenek is an academic lecturer (MD, MPH, PhD) at the Department of Drug Management, Institute of Public Health, Jagiellonian University School of Medicine, Krakow, Poland. The scope of his professional interests embraces pharmaceutical policy, pharmaceutical pricing and reimbursement, management of phar-maceuticals and medical devices, pharmacoeconomics and health technologies assessment. The author and co-author of original research papers, author of academic textbooks and a contributor of special focus chapters into a number of publications within the same domain. Involved in the pursuit and management of a number of public health projects and in monitoring clinical tri-als. Co-organiser and co-ordinator of diverse training schemes for medical professionals, senior editor of a specialist journal for health care professionals. Senior consultant in nationwide projects aimed at restructuring Polish public health care system. In the period spanning 1998-2006 appointed the first Managing Director at the Department of Pharmaceuticals and Medical Devices, the Malopolska Regional Sickness Fund and the Malopolska Provincial Branch of the National Health Fund. He completed his medical graduate studies in Poland (Jagiellonian University, Krakow) and pursued further education at Hartford University and Harvard University, USA; University of Liege, Belgium; University of Shef-field, UK; Maastricht University, The Netherlands; Nordic School of Public Health, Sweden; universities of the Baltic states - THE BRIMHEALTH Network; Management Sciences for Health,
USA, striving throughout to broaden the scope of his professional experience and expertise in the field.
Michael Borowitz is a public health physician (MD, MPH) and health economist (PhD). He currently works as a senior health economist at the Organisation for Economic Co-operation and Development (OECD). He started his career working on U.S. health reform but later moved to the United Kingdom, where he worked for the U.K. Department of International Development on HIV/AIDS, TB, malaria, and health reform, and then moved to the World Bank, where he worked on China and Indonesia. A couple of years ago, he moved to the U.K. Department of Health to work on reform of the NHS and health systems in developed countries. He has a long-standing interest in inequalities in health and public policies in addressing social determinants of health.
Jesse Bump is an assistant professor in the Department of Inter-national Health at Georgetown University. His research interests include the application of historical and social science tools to cur-rent public health problems in developing countries, community-directed programs, health system design, and priority- and agenda-setting processes in global health. His current projects focus on the political economy of universal health coverage, the effects of competition in development assistance for health, and research methodologies for studying health systems.
Kalipso Chalkidou is the founding director of NICE’s interna-tional program, advising governments overseas on building technical and institutional capacity for using evidence and values to inform health policy. She is interested in how local information, local exper-tise and local institutions can drive scientific and legitimate health care resource allocation decisions. She is involved in the Chinese rural health reforms and also in national health reform projects in Georgia, Turkey, the Middle East, and Latin America. She holds a doctorate on the molecular biology of prostate cancer from the

61P
rofiles of W
orking G
roup m
embers
University of Newcastle (United Kingdom) and an MD (Hons) from the University of Athens, and is an honorary lecturer at the London School of Hygiene and Tropical Medicine, a senior advi-sor on international policy at the Center for Medical Technology Policy (United States), and a visiting faculty member at the Berman Institute for Bioethics at Johns Hopkins University (United States).
Leonardo Cubillos is a consultant for the World Bank Institute. Prior to joining the Institute, Dr. Cubillos was Director General of Demand Management (Insurance) and Acting Viceminister at the Ministry of Social Protection in Colombia. He led a team respon-sible for the Direction and Regulation of the Subsidized Regime that insures 23 million Colombians, and was also responsible for designing, implementing, and monitoring policies that reached 43 million citizens in regard to the benefits plan, and contracting and payment mechanisms for both insurers and providers. Mr. Cubillos and his team designed and implemented a rigorous and systematic plan to update and cost the benefits plan. At the end of his work in the MPS, the Subsidized Regime achieved Universal Health Insurance Coverage.
Tessa Edejer is the Coordinator of the Unit of Costs, Effectiveness, Expenditure, and Priority Setting (CEP) under the Department of Health systems financing in the Cluster of Health Systems and Ser-vices in WHO. For the past 10 years, she has been primarily respon-sible for leading the work on defining the cost-effectiveness of health interventions (WHO-CHOICE) and the costs of scaling up. Her recent work has revolved around developing a guidance document for policy makers on equity/efficiency tradeoffs and the opportunity costs of making more equitable choices. She is also engaged in the ongoing development of a UN interagency health system costing tool. Another major area of work in the Unit is on national health accounts (NHA), which includes annually updating the health expenditure estimates of WHO’s 194 member states and assisting countries to generate and use their own estimates. She just completed work on the revision of the system of health accounts, which was done in collaboration with OECD and Eurostat.
Ruth R. Faden is the Philip Franklin Wagley Professor of Bio-medical Ethics and Executive Director of Johns Hopkins Berman Institute of Bioethics. She is also a Senior Research Scholar at the Kennedy Institute of Ethics, Georgetown University. Dr. Faden
is the author and editor of numerous books and articles on bio-medical ethics and health policy. She is a member of the Institute of Medicine and a Fellow of the Hastings Center and the Ameri-can Psychological Association. She has served on several national advisory committees and commissions, including the President’s Advisory Committee on Human Radiation Experiments, which she chaired. Her current research interests include bioethics and public policy; ethics and cellular engineering; ethics and neurosci-ence; ethics and bioterrorism; ethics, genetics, and public policy; research ethics; and justice.
Jeremy Farrar is Director of the Oxford University Clinical Research Unit (OUCRU) in Ho Chi Minh City, Vietnam. Jeremy works on clinical, pathophysical, and molecular aspects of infectious diseases. The work of his unit supports the global initiative to locate and analyze diversity in immunity-related genes.
James Fitzgerald is a Senior Advisor on Essential Medicines and Biologicals for the Pan American Health Organization (PAHO).
Ursula Giedion has been working as a health economist for the last 20 years on issues related to health care reform and financing in Latin America, Africa, and Asia. Her work experience includes a combination of academic and policy advisory positions facilitating the understanding of technical as well as political and institutional issues at stake in the design, implementation, and evaluation of health sector reforms. Her main areas of interest include impact evaluation studies in the health sector, financial protection, health insurance and the poor, equity and efficiency of different health financing mechanisms, priority setting in health, and design and implementation of benefits packages.
Amanda Glassman is the Director of Global Health Policy and a Research Fellow at the Center for Global Development. She has 20 years of experience working on health and social protection policy and programs in Latin America and elsewhere in the developing world. Prior to her current position, Glassman was principal techni-cal lead for health at the Inter-American Development Bank, where she led health economics, the financing of knowledge products, and policy dialogue with member countries. From 2005 to 2007, she was deputy director of the Global Health Financing Initiative at Brookings and carried out policy research on aid effectiveness and

62P
rofile
s of
Wor
king
Gro
up
mem
ber
s
domestic financing issues in the health sector of low-income coun-tries. Before joining the Brookings Institution, Glassman designed, supervised, and evaluated health and social protection loans at the Inter-American Development Bank and worked as a Popula-tion Reference Bureau Fellow at the U.S. Agency for International Development. Glassman holds an MSc from the Harvard School of Public Health and a BA from Brown University. She has published on a wide range of health and social protection finance and policy topics and is editor and coauthor of the books From Few to Many: A Decade of Health Insurance Expansion in Colombia (IDB and Brookings 2010) and The Health of Women in Latin America and the Caribbean (World Bank 2001).
Charles Hongoro is a Research Director in the Policy Analysis Unit of the Human Sciences Research Council of South Africa (HSRC). He is a former Lecturer in Health Economics and Systems at the London School of Hygiene and Tropical Medicine. Before joining the HSRC in September 2006, he was a program director of health economics and systems at the Aurum Institute for Health Research in Johannesburg. He has also worked as a senior medical research officer (Health Econo-mist) in the Health Systems Research Unit at the National Institute of Health Research (formerly Blair Research Institute). His areas of research interest include the economics of HIV/AIDS and other infec-tious diseases, health systems and policy-oriented research in general, social health insurance, and the impact of legislation.
Dai Hozumi is a Senior Technical Advisor for health systems and policy with the Immunization Solutions Program at PATH. He received his MD from the Juntendo School of Medicine, Tokyo; his MS in Management from the Sloan School of Management, Mas-sachusetts Institute of Technology; and his MPH in Epidemiology from the University of California at Berkeley. Dr. Hozumi has been a Senior Monitoring and Evaluation advisor at John Snow, Inc., Boston; a manager at the Department of International Health, St. Mary’s Hospital, Kurume, Japan; and an Instructor at the Harvard School of Public Health. His research interests include health service planning, health care resource distribution, health management information systems, the improvement of health systems, and chil-dren’s health in developing countries.
Lydia Kapiriri is an Assistant Professor and undergraduate chair of Health, Aging, & Society at McMaster University. She is mainly
interested in health systems and global health research. Her previ-ous and current research has focused on understanding the fac-tors that influence the health-seeking behavior of underprivileged populations; community-based participatory intervention research to promote the adoption of HIV preventive behavior — specifically, the use of condoms in urban poor populations in Uganda, and examining the criteria and processes used in patient selection for access to HAART in Uganda; improving the health of urban poor populations through urban primary health care; and priority set-ting in health care at the different levels of decision making (macro, meso, and micro levels), mainly in developing countries but also comparing the approaches to priority setting in both low- and high-income countries, specifically Canada and Norway. Kapiriri is also interested and involved in research related to public health and global health ethical issues, including but not limited to interna-tional research ethics, access to HAART, pandemic flu prepared-ness, and XDR-TB.
Felicia Knaul is the Director of the Harvard Global Equity Initia-tive and Associate Professor at the Harvard Medical School. As a result of her personal experience, she founded Cáncer de Mama: Tómatelo a Pecho (Breast Cancer: Take it to Heart) in 2007, a pro-gram that undertakes and promotes research, advocacy, awareness, and early detection initiatives on breast cancer in Latin America. Her book on her life with breast cancer, Tómatelo a Pecho, was released in October 2011.
Zhao Kun is a Researcher in the Division of Health Technology Assessment and Policy Evaluation in the China National Health Development Research Center of the Ministry of Health in Beijing. She received her medical degree from China Medical University and has Master’s degrees from the Capital University of Medical Sciences in Beijing and the Faculty of Medicine of the University of British Columbia. She is currently a PhD candidate in Health Economics Evaluation in the Faculty of Applied Health Science at the University of Waterloo, Canada. Her research projects include the policy and technology evaluation of “Healthy China 2020”; evaluation of clinical pathways in rural China; a cost-benefit analysis of H1N1 influenza prevention measures in China; a comparison of community health care service among 37 facilities with differ-ent ownerships in China; and a cost-effectiveness analysis of stroke treatment models of treatment in China.

63P
rofiles of W
orking G
roup m
embers
Rachel Nugent is a Senior Research Scientist and Associate Pro-fessor at the University of Washington’s Department of Global Health and a Project Director for the Disease Control Priorities Network. Previously she was the Deputy Director of global health at the Center for Global Development. She led CGD’s Demographics and Development in the 21st Century Initiative, managed the Drug Resistance & Global Health Initiative, and conducted research on noncommunicable diseases in developing countries.
Mead Over is a Senior Fellow at the Center for Global Develop-ment, researching the economics of efficient, effective, and cost-effective health interventions in developing countries. Much of his work since 1987, first at the World Bank and now at the CGD, has been on the economics of the AIDS epidemic. After work on this subject as well as on cost-effective interventions, he coauthored the Bank’s first comprehensive treatment of the economics of AIDS in the book Confronting AIDS: Public Priorities for a Global Epidemic (1997, 1999). His most recent book is Achieving an AIDS Transition: Preventing Infections to Sustain Treatment (2011), in which he offers options for donors, recipients, activists, and other participants in the fight against HIV, to reverse the trend in the epidemic through bet-ter prevention. Recruited to the World Bank as a Health Economist in 1986, Over advanced to the position of Lead Health Economist in the Development Research Group before leaving the Bank to join the Center for Global Development in 2006.
Andrés Pichon-Riviere is the Executive Director of the Institute for Clinical Effectiveness and Health Policy and Director of the Health Technology Assessment and Economic Evaluation. He is also a Professor of Public Health at the University of Buenos Aires and member of the Board of the Clinical Effectiveness Program, a Master’s program of the University of Buenos Aires, where he coordinates the courses of Biostatistics, Statistical Computing, and Survival Analysis. Dr. Pichon-Riviere is Executive Board Member of LatinCLEN (the Latin American division of the International Clinical Epidemiology Network (INCLEN)), and member of the Foundation Board of IC-Health (Initiative for Cardiovascular Health Research in the Developing Countries).
Diana Pinto is a Health Lead Specialist in the IDB’s office in Washington DC. Prior to joining the IDB, she worked as Associate Professor at Pontificia Universidad Javeriana’s School of Medicine
and as Research Associate at Fedesarrollo, conducting research in applied health economics. She also worked as Health Policy Advi-sor to the Minister of Social Protection in Colombia, in charge of the design and evaluation of health sector policy, and of the design, development, and coordination of technical studies to support decision making with respect to benefits packages and their financial sustainability. Diana has also carried out numerous consultancies for the World Bank, CAF, and IDB, among other institutions. She has published and served as editor of book chapters on health financing and insurance.
Mala Rao joined the Indian Institute of Public Health (Hyderabad) at the invitation of the Public Health Foundation of India as its Director in July 2008. Prior to this, she was Head of Public Health Workforce and Capacity at the Department of Health, London for five years, having led the public health capacity-building strategy for England. She was previously a Director of Public Health in the U.K. NHS for many years, during which she established the first cancer network in the country. Dr. Mala published the landmark U.K. Public Health Skills and Career Framework in 2008 and was one of the main architects of the newly created specialty of sexual and reproductive health care in the United Kingdom. Throughout her career, she has been committed to developing multidisciplinary public health, and bringing public health teaching, research, policy, and practice closer together.
Michael Rawlins has been Chairman of the National Institute of Health & Clinical Excellence (NICE) since its formation in 1999. Sir Rawlins is also Honorary Professor at the London School of Hygiene and Tropical Medicine, University of London, and Emeri-tus Professor at the University of Newcastle upon Tyne, where he was the Ruth and Lionel Jacobson Professor of Clinical Pharma-cology from 1973 to 2006. At the same time he held the position of consultant physician and consultant clinical pharmacologist to the Newcastle Hospitals NHS Trust. He was Vice Chairman (1987–92) and Chairman (1993–98) of the Committee on Safety of Medicines, and Chairman of the Advisory Council on the Misuse of Drugs (1998–2008).
Alarico Rodriguez de Leon is the Vice Director of the Uru-guayan National Agency for Highly Specialized Medical Proce-dures (FNR). His research focuses on health technology assessment,

64P
rofile
s of
Wor
king
Gro
up
mem
ber
s
health systems, health policies, funding health coverage, policies on drugs, organ transplantation, hospital infections, quality assur-ance in health services, utilization review of health services, health human resources, and bioethics. He has a medical degree from the Universidad de la República Uruguay School of Medicine and a postgraduate and Master’s degree in public health from its Medical School. He has taught at a number of national and foreign universi-ties, tutored in the Pan American Health Organization’s Virtual Campus, and is a member of its board of examiners. He has lectured on several scientific activities of international organizations in Latin America, Europe, Africa, and Asia. He is also a member of the Uruguayan Cochrane Collaboration Center, a Researcher at the Evaluation Quality Program of Fondo Nacional de Recursos, and a Latin American representative in the World Medical Association Council, and he manages relation officers with the Pan American Health Organization of Confederación Médica Latinoamericana y del Caribe. He is a Founding Partner of Sociedad Uruguaya de Salud Colectiva and Founding Partner and Vice Chairman of Asociación de Economía de la Salud del Uruguay.
Lloyd Sansom is a Professor Emeritus at the University of South Australia and the former Chair of the Australian Pharmaceutical Benefits Advisory Committee (PBAC). Professor Sansom gradu-ated in Pharmacy in 1962 and completed his PhD in Biophysical Chemistry at the University of Adelaide in 1972. In 2006 he was awarded honorary doctorate degrees by Newcastle, Griffith, and Queensland universities. Professor Sansom’s research interests are in the areas of pharmacokinetics, biopharmaceutics, and the quality use of medicines, and he has received more than 20 major grants and contributed to over 100 scientific publications.
Jeremy Shiffman is Associate Professor of Public Administration and Policy at American University. A political scientist by training, he researches the politics of health policy and administration in poor countries. He has a particular interest in health agenda–setting: why some issues receive priority while others are neglected. Among other topics, he has investigated maternal survival, newborn survival, fam-ily planning, donor funding for health, and health systems reform.
Yot Teerawattananon is a medical doctor and economist and currently serves as Program Leader and Senior Researcher for the Health Intervention and Technology Assessment Program
in India. He previously served as a Director of Pong District Hospital Phayao Province in northern Thailand, where he devel-oped an intense interest in health economics and policy. Since 2000 he has worked as a Health System Researcher at the Senior Research Scholar Program in Health Financing and Policy (which later became the International Health Policy Program — IHPP), where he gained experience in project evaluations at the grassroots and national levels. From 2001 to 2002 he worked as principal investigator in a project that evaluated the national program for prevention of mother-to-child HIV transmission in Thailand, which subsequently led to the revision of the national protocol. In 2003 he received the World Health Organization Fellowship Award to study at the University of East Anglia, England, where he completed his PhD in Health Economics. He has a number of publications related to health economics evaluation in leading international journals such as Value in Health and Pharmacoeco-nomics. His current research focuses on health technology assess-ment, decision making in health care, and reproductive health, including HIV/AIDS.
Ignez Tristao is an economist in the Social Protection and Health Division of the Inter-American Development Bank. Her work at the IDB has focused on issues involving health finance and priori-tization. Previously, she served as an Economic Specialist in Health Policy and Social Security in the U.S. Congress’s Congressional Budget Office, where she was involved in analysis, projections, and several studies on U.S. public health insurance programs (Medic-aid and Medicare) and the impact of rising obesity rates on health expenditures. Her research has been published in peer-reviewed journals such as Health Economics and National Tax Journal. Tristao is a Brazilian national. She holds a PhD in Economics from the University of Maryland, United States, where she specialized in health and labor market economics.
Sean Tunis is the Founder and Director of the Center for Medi-cal Technology Policy, an independent nonprofit entity focused on improving the value of clinical research for decision making by engaging a range of experts and stakeholders in study design and implementation. He advises numerous domestic and international health care agencies and organizations on issues of comparative effectiveness, evidence-based medicine, clinical research, and tech-nology policy.

65P
rofiles of W
orking G
roup m
embers
Adriana Velazquez Berumen is the Coordinator of Diagnostic Imaging and Medical Devices, under the Department of Essential Health Technologies at the World Health Organization.
Damian Walker is a Senior Program Officer in Global Health Delivery at the Bill & Melinda Gates Foundation. Dr. Walker is a health economist with more than 13 years of experience in inter-national health economics, with a specific focus on the economic evaluation of public health programs in low- and middle-income countries. Prior to working at the Gates Foundation, Dr. Walker was an Associate Professor in the Department of International Health, Bloomberg School of Public Health, Johns Hopkins University. In
addition to conducting research, Dr. Walker also taught courses on health economics, economic evaluation, and health systems. He supervised numerous doctoral and Master’s students. Before that, Dr. Walker was a Lecturer in the Department of Public Health and Policy at the London School of Hygiene and Tropical Medicine, where he also received his PhD in health economics. Dr Walker received his BSc and MSc in health economics from the University of York. He has published over 80 peer-reviewed journal articles and numerous book chapters. Recently he was lead author on the World Health Organization’s Guide for Standardization of Economic Evaluations of Immunization Programmes. He is Deputy Editor of Cost-Effectiveness and Resource Allocation.

66
Detailed tables and sources on potential gains from improved efficiency
Appendix B
Potential efficiency gains from critically assessing interventions
Source Best buy CountryPotential
cost savings DescriptionHealth gains Description
Sweat et al. (2004)
Nevirapine to prevent mother-to-child HIV transmission
Tanzania 81% Cost per DALY saved or from 77 to 13
2,774 Annual infant HIV infections averted
Schwartländer et al. (2011)
Comprehensive HIV approach
Worldwide (139 countries)
51% Current cost vs. optimal cost of worldwide care, treatment, and prevention
52%46%
Reduction in new infectionsReductions in AIDS deaths
WHO (2010b) Cardiovascular disease prevention in Thailand
Thailand — 99% Current mix to optimal mix to obtain an additional healthy year of life
Slide 9 in Gates Best Buy slide deck
Treating patients on human insulin vs. analogues
Kyrgyz Republic 52% Cost per patient on humans and analogues vs. cost per patient on all analogues
19 or 90% increase (from 2 on humans to 19 on insulin)
Potential increase in the number of patients on insulin for the same budget ($100)
Bisoffi et al. (2011)
Presumptive malaria treatment for all children
Burkina Faso 40% Cost per management of 1000 patients for children in the rainy season at “real life” adherence rate
Shah et al. (2011)
Short-course ARV instead of long-course ARV for PMCT
Nigeria 27% Cost per pregnancy

67D
etailed tab
les and sou
rces on p
otential g
ain
s from im
proved effi
ciency
Source Best buy Country Efficiency gains Description
Gureje et al. (2007) Combine older antipsychotic drugs with psychosocial treatment for schizophrenia
Nigeria 68% Cost per DALY avoided: current state vs. optimal intervention
Road-side breath-testing to prevent alcohol abuse
Nigeria 56% Cost per DALY avoided: current state vs. optimal intervention
Applying older over newer epileptic drugs in primary care (50% coverage)
Nigeria 70% Cost per DALY avoided: current state vs. optimal intervention
Lai et al. (2007) Alcohol and smoking control through increased excise taxes
Estonia 66% Cost per DALY avoided: current state vs. optimal intervention
Woo et al. (2007) Population-based cancer screening in Chinese women
China 59% Cost per DALY avoided: current state vs. optimal intervention
Chanda et al. (2007) Choosing artemether-lumefantrine (AL) over sulfadoxine-pyrimethamine (SP) for malaria treatment
Zambia 20% Cost per case cured
Long et al. (2011) Shifting ART management from hospital-based to nurse-managed primary care facility
South Africa 11% Cost per patient
WHO (2010b) Road traffic injury prevention (helmet wearing)
Thailand 21% Cost per DALY avoided: current state vs. optimal intervention
Road traffic injury prevention (alcohol control)
Thailand 45% Cost per DALY avoided: current state vs. optimal intervention

68
Current international support to priority setting in low- and middle-income countries
Appendix C
Initiative Objective Activities Web site Reported impactHost institution
African Vaccine Regulatory Forum (AVAREF)
To provide a resource of expert advice to regula-tors to support their regu-latory system for evalua-tion of vaccines. This fo-rum may be considered an ad hoc scientific advisory body that will help regula-tors make an informed regulatory decision with regard to authorizations of clinical trials, evaluation of registration dossiers, or any other challenging is-sues regarding evaluation of vaccines
Information session and regulatory discussions. According to the stage of development of the vaccine, dif-ferent kinds of presentations will be included, i.e. vaccine developers, clinical trial sponsors, and vaccine manufacturers. Experts in relevant areas of expertise will be invited by WHO to make presentations and assist regulators. There will be information sessions and sessions only for regulators, WHO staff and experts brought by WHO to provide a nonthreatening environment for regulators to feel free to discuss their concerns, doubts, and weak-nesses and openly ask questions of experts and colleague regulators
www.who.int/immunization_ standards/vaccine _regulation/africa _network/en/index.html
Not reported WHO
Alliance for Health Policy and Systems Research
Promote generation and use of health policy and systems research as a means to improve health and health systems
Generate and synthesize policy-relevant health systems knowledge; promote dissemination and use of HPSR; strengthen capacity for generation, dissemination, and use of HPSR among researchers, policy makers, and other stakeholders. From 2010, includes a new pro-gram on access to medicines
www.who.int/alliance-hpsr/en/
WHO
Cochrane Collaboration
Help health care providers, policy makers, patients, and their advocates, make well-informed decisions about human health care
Preparing, updating and promoting the accessibility of systematic re-views of primary research in human health care and health policy. Run international register of ongoing systematic reviews. Assess accu-racy of diagnostic tests for a given condition in a specific patient group and setting. Includes EvidenceAid project to provide reliable, up-to-date evidence on interventions to consider in context of disasters and emergencies. Runs WHO reproduc-tive health library and WHO library of evidence for nutrition actions. Ten CC Centers in low- and middle-income countries, mainly universi-ties and private firms
www.cochrane.org/cochrane-reviews/evidence-aid-project
“The main output of The Cochrane Collabo-ration, the Cochrane Reviews, has had a real and significant impact on practice, policy decisions and research around the world.” For examples, see www.who.int/bulletin/volumes/82/10/volmink1004abstract/en/ and http://care.diabetesjournals.org/content/23/9/1217.full.pdf
The Co-chrane Col-laboration (an NGO in official rela-tions with the WHO)

69C
urren
t intern
ation
al support to p
riority setting in
low- an
d mid
dle-in
come cou
ntries
Initiative Objective Activities Web site Reported impactHost institution
Cost- Effectiveness Analysis Registry
Analyze the benefits, risks, and costs of strategies to improve health and health care, and communicate the findings to clinicians and policy makers, mainly in the United States
The CEAV Registry is a comprehen-sive database of 2,576 cost-utility analyses on a wide variety of dis-eases and treatments. Activities include advancing methods develop-ment for the field; training the next generation of practitioners; and working with policy makers world-wide to develop reasoned policy solutions. CEVR’s researchers bring experience in economics and decision analysis to a host of clini-cal and public health policy issues. The work encompasses formal cost-effectiveness analysis and related techniques, as well as policy research and analysis pertaining to resource allocation. To facilitate this work, CEVR has developed and maintains databases that support evidence-based and value-based evaluation of interventions and that document decision making by the Centers for Medicare and Medicaid Services (CMS). These resources provide information and insights to inform health care stakeholders
https://research.tufts-nemc.org/cear4/default.aspx
45 peer-reviewed publications; decisions by CMS
Tufts University
Disease Control Priorities Network (DCPN)
The DCPN aims to improve how health resources are allocated across a wide range of options, includ-ing interventions, health service delivery platforms (such as hospitals and clinics), and the research and development of new health technologies. One of the key questions is how we can best dedicate resources to get the maxi-mum impact in improving population health
Activities include: assessing health benefits of technologies; producing empirical estimates of interven-tion effectiveness; assessing costs of delivering interventions, expanding platforms, or changing quality of platforms; computing comparable cost- effectiveness ratios and acceptability curves for all inter ventions in the DCPN, and identifying adoptable policies that are efficient; creating a network of institutions for training and capacity- building; and extending the cost-effectiveness analysis frame-work to take into account nonhealth consequences, among others. Includes collaboration with U.S. Institute of Medicine for workshop on country-level decision making for control of chronic diseases. Will conduct country policy assess-ments in India and South Africa and two additional countries
www.health metricsand evaluation.org/research/project/disease-control -priorities-network -draft
The DCP publications have “stimulated na-tional and international debate on health sec-tor investments and have become reference works used extensively by policy makers, inter-national development agencies, and academic institutions.” Expected impact of DCPN: “(i) provide a consistent and comparable set of cost inputs to be used across CEA as-sessments, calibrated regionally; (ii) provide in-sights about health ser-vice delivery constraints and their measurable impact on outcomes; (iii) allow policy makers to consistently consider complex dimensions of resource allocation and impact, including equity tradeoffs and platform contexts; (iv) result in a wide range of compa-rable estimates of C/E adjusted regionally”
Institute for Health Metrics and Evaluation, University of Washington

70C
urr
ent
inte
rnati
onal
suppor
t to
pri
orit
y se
ttin
g in
low
- an
d m
iddle
-inco
me
countr
ies
Initiative Objective Activities Web site Reported impactHost institution
EUnetHTA Focusing on scientific cooperation in health tech-nology assessment in Eu-rope, 34 government-ap-pointed organizations from the EU member states, Accession Countries, and EEA work together to help develop reliable, timely, transparent, and transferable information to contribute to health technology assessment in European countries
Development of health technology assessment tools and methods; application and field testing of developed tools and methods; quar-terly communication protocol for information flow on ongoing/planned national assessments of same technologies, among others
www.eunethta.net/ Secretariat, National Board of Health, Denmark
EVIDEM To promote public health by developing efficient MCDA-based solutions for health care decision mak-ing and priority setting
Provides free access to decision-making framework, open access web registry of evidence of health care interventions, support for application of tools, and a forum for discussion
www.evidem.org/ Independent nonprofit organization
Evidence- Informed Policy Network (EVIPNet)
Strengthen skills and capabilities in evidence-informed policy making
Handbooks and training on knowl-edge brokering and policy influence; EVIPNet portal to disseminate best practices; SURE for policy in African health systems — policy research
www.who.int/rpc/evipnet/policybrief/en/index.html
www.who.int/rpc/evipnet/EVIPNet%20America%20Lan-cet%20article%20Sept08.pdf
WHO
Global initiative on health technologies (GIHT)
Establish a framework for the development of national health technology programs that will impact the burden of disease and ensure effective use of resources (focused mainly on medical devices)
Among others: development of a methodology and relevant tools to help member states conduct an assessment of health technologies; identification of national, regional, and global standards for countries to identify current gaps and future needs in order to prioritize health technologies; development of tools to assist countries to integrate their prioritized needs into national policies, action plans, and programs
www.who.int/medical_devices/appropriate_use/en/
WHO De-partment of Essential Health Technologies
Guidance on priority setting in health (GPS Health)
Provide guidance to those producing cost- effectiveness studies and interpreting their conclusions
Define criteria and questions rel-evant to health priority setting and not adequately considered by cost-effectiveness analysis, focused on LMICs
WHO CEP unit with Ole Frithjof Norheim
Health Evidence Network (HEN)
HEN is a network of orga-nizations or institutions promoting the use of evidence in health policy or health technology assess-ment, also involving United Nations agencies with a mandate related to health
In reply to specific questions from policy makers in EURO, provide evidence reports; joint policy briefs and policy summaries; HEN summa-ries of network members’ reports
www.euro.who.int/en/what-we-do/ data-and-evidence/health-evidence -network-hen
Swedish Council on Technol-ogy As-sessment in Healthcare (SBU), Sweden
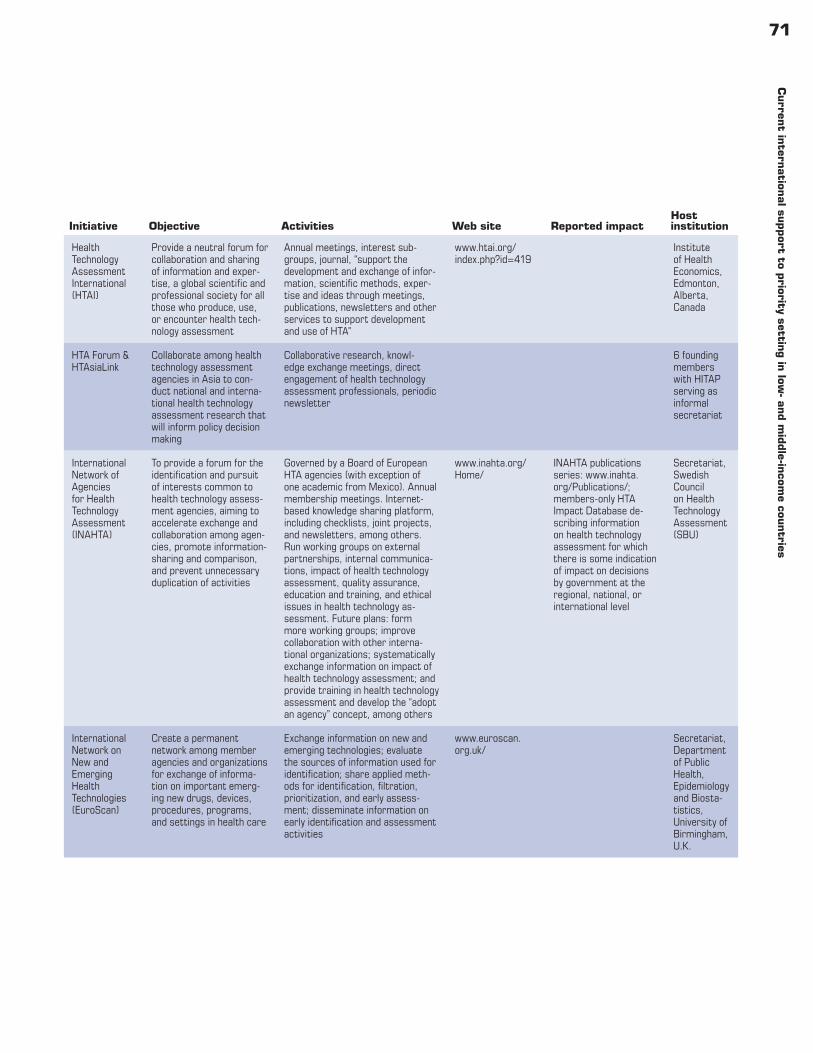
71C
urren
t intern
ation
al support to p
riority setting in
low- an
d mid
dle-in
come cou
ntries
Initiative Objective Activities Web site Reported impactHost institution
Health Technology Assessment International (HTAI)
Provide a neutral forum for collaboration and sharing of information and exper-tise, a global scientific and professional society for all those who produce, use, or encounter health tech-nology assessment
Annual meetings, interest sub-groups, journal, “support the development and exchange of infor-mation, scientific methods, exper-tise and ideas through meetings, publications, newsletters and other services to support development and use of HTA”
www.htai.org/index.php?id=419
Institute of Health Economics, Edmonton, Alberta, Canada
HTA Forum & HTAsiaLink
Collaborate among health technology assessment agencies in Asia to con-duct national and interna-tional health technology assessment research that will inform policy decision making
Collaborative research, knowl-edge exchange meetings, direct engagement of health technology assessment professionals, periodic newsletter
6 founding members with HITAP serving as informal secretariat
International Network of Agencies for Health Technology Assessment (INAHTA)
To provide a forum for the identification and pursuit of interests common to health technology assess-ment agencies, aiming to accelerate exchange and collaboration among agen-cies, promote information-sharing and comparison, and prevent unnecessary duplication of activities
Governed by a Board of European HTA agencies (with exception of one academic from Mexico). Annual membership meetings. Internet-based knowledge sharing platform, including checklists, joint projects, and newsletters, among others. Run working groups on external partnerships, internal communica-tions, impact of health technology assessment, quality assurance, education and training, and ethical issues in health technology as-sessment. Future plans: form more working groups; improve collaboration with other interna-tional organizations; systematically exchange information on impact of health technology assessment; and provide training in health technology assessment and develop the “adopt an agency” concept, among others
www.inahta.org/Home/
INAHTA publications series: www.inahta.org/Publications/; members-only HTA Impact Database de-scribing information on health technology assessment for which there is some indication of impact on decisions by government at the regional, national, or international level
Secretariat, Swedish Council on Health Technology Assessment (SBU)
International Network on New and Emerging Health Technologies (EuroScan)
Create a permanent network among member agencies and organizations for exchange of informa-tion on important emerg-ing new drugs, devices, procedures, programs, and settings in health care
Exchange information on new and emerging technologies; evaluate the sources of information used for identification; share applied meth-ods for identification, filtration, prioritization, and early assess-ment; disseminate information on early identification and assessment activities
www.euroscan.org.uk/
Secretariat, Department of Public Health, Epidemiology and Biosta-tistics, University of Birmingham, U.K.

72C
urr
ent
inte
rnati
onal
suppor
t to
pri
orit
y se
ttin
g in
low
- an
d m
iddle
-inco
me
countr
ies
Initiative Objective Activities Web site Reported impactHost institution
International Society for Pharmaco-economics and Outcomes Research (ISPOR)
Foster excellence in the science of pharmaco-economics and health outcomes research and its use in health care decisions
Provide resources for researchers, including journals, ethics guidelines, databases; resources for health care decision makers including jour-nal, pharmacoeconomic guidelines around the world, councils; and educational resources, including short courses, meetings, distance learning, toolkit, speakers bureau, and so on. Also, to conduct regional meetings in Latin America and Asia-Pacific, and have directory of health technology assessment agencies and organizations
www.ispor.org/Default.asp
Journal special is-sues on Asia and Latin America, use of health technology assessment
ISPOR
Kazakhstan Health Technology Transfer and Institutional Reform Project
Strengthen capacity to develop and disseminate international-standard clinical practice guidelines; carry out health technol-ogy assessment for better clinical and policy decision making
To establish a system for con-tinuous development, revision, and dissemination of evidence-based clinical practice guidelines (CPGs); to develop methods of health care standardization processes based on international best practices and provide practical assistance in ensuring their sustainability; to develop and disseminate at least 20 international-standard Clinical Practice Guidelines in each of the five key clinical specialties; to build the capacity of Kazakhstani special-ists to carry out Health Technology Assessment; to introduce the prin-ciples of evidence-based medicine into medical education
www.csih.org/en/projects/hta.asp
Establishment of a functioning system for the continuous develop-ment, review, and dis-semination of evidence-based clinical practice guidelines; development and widespread dissem-ination of at least 20 international standard CPGs in each of the five key clinical specialties; capacity-building for Kazakhstani special-ists to carry out health technology assessment and conduct at least four health technol-ogy assessments by the end of the project; intro duction of EBM into medical education
Canadian Society for International Health
Malaria Vaccine Decision- Making Framework
The framework aims to “facilitate more effective cooperation between governments and partners at national, regional and global levels, so that a decision can be made on a malaria vaccine within 1–3 years of licensure”
Briefing papers analyzing potential demand, return on investment, public health impact, possible introduction guidelines, pathways for decision making with respect to malaria control policies, historical practice in moving from develop-ment to policy to implementation of new products in malaria-endemic countries as pertains to introduc-tion of malaria vaccine. Second, regional decision-making framework document, a tool that describes the required data and processes for malaria vaccine introduction in the African region, made available January 2009
www.malvacdecision.net/index.html
Over 90% responded that the associated presentation, briefing, and reporting materials were clear and easy to understand. A solid majority indicated that participation in the DMF process had con-tributed either greatly or moderately to their country’s prepared-ness to collect data and establish the processes needed to support a malaria vaccine decision
PATH with 13 African health of-ficials and a Steering Committee composed of WHO, BMGF, USAID, and others
NICE International
Provide advice on use of evidence and social values in making clinical and policy decisions
Advice; knowledge products; tools; facilitation of knowledge transfer among decision makers
www.nice.org.uk/aboutnice/niceinternational/niceinternational.jsp
NICE

73C
urren
t intern
ation
al support to p
riority setting in
low- an
d mid
dle-in
come cou
ntries
Initiative Objective Activities Web site Reported impactHost institution
Priority Setting and Health Benefit Plans
IDB aims to provide the region with assistance to perform careful and detailed consideration of the most current techni-cal evidence available to guide the decision-making process — improving sustainability of the health systems and resulting in better, more informed decisions in terms of eq-uity, quality, efficiency, and financial protection for the population
Forges regional and nonregional alliances with academic institutions and other organizations involved in health priority setting to build knowledge on the design, implemen-tation, and adjustment of the health benefits plans throughout the re-gion, and to support governments in the implementation of such plans
www.iadb.org/en/topics/health/priority- setting-in -health,2077.html
IDB
Project Antares
To develop self-sustaining approaches to health care for low-income populations using market systems
Antares works to identify and part-ner with field organizations that deliver such interventions, deploy-ing joint teams of public health and business students to analyze and help improve existing models or develop new ones to meet Antares objectives
www.hbs.edu/healthcare/pdf/antaresintro.pdf
(Official website coming soon.)
Since 2007 Antares has engaged 77 stu-dents in 14 projects spanning 11 countries in Latin America, Af-rica, and Asia
Harvard Business School and the Harvard School of Public Health
ProVac To strengthen the national capacity to make informed, evidence-based decisions regarding vaccine intro-duction in Latin America and the Caribbean
Activities include: assessing current decision-making processes and cur-rent advisory bodies; strengthening national committees on immuniza-tion; supporting the formation of multidisciplinary teams for data col-lection and cost- effectiveness analy-sis; establishing a regional network of centers for excellence in health costing (six universities); establish-ing the ProVac e-support center to assist with economic analysis and provide training to users; carrying out cost-effectiveness analyses for pneumo coccal disease; generating and disseminating a “decision case” for advocacy based on evidence
http://new.paho.org/provac/index.php?option=com_frontpage&Itemid=1
http://content. healthaffairs.org/ content/30/6/1104.full
PAHO
Regional Initiative on Priority- Setting, Equity and Constitutional Mandates in Health (two- year initiative)
Support regional dialogue on current impact of health litigation in seven Latin American countries
Structured multistakeholder discussions, seminars, videocon-ferences, country visits, joint ap-plied research, study tours, and workshops
http://wbi.worldbank.org/wbi/stories/setting -priorities-health -latin-america%E2 %80%99s-story
World Bank Institute
Regional Platform for Access and Innovation for Health, PAHO
To create a platform com-posed of Internet-based tools that will support and promote innovation, access, rational use, and good governance in the area of essential medicines and other health technologies
Among others: health technology assessment evidence and good practices; “evidence-based rapid response for decision-making”
http://new.paho.org/hq/index.php ?option=com_ content&task=view&id=2168&Itemid= 1178
PAHO HSS/MT
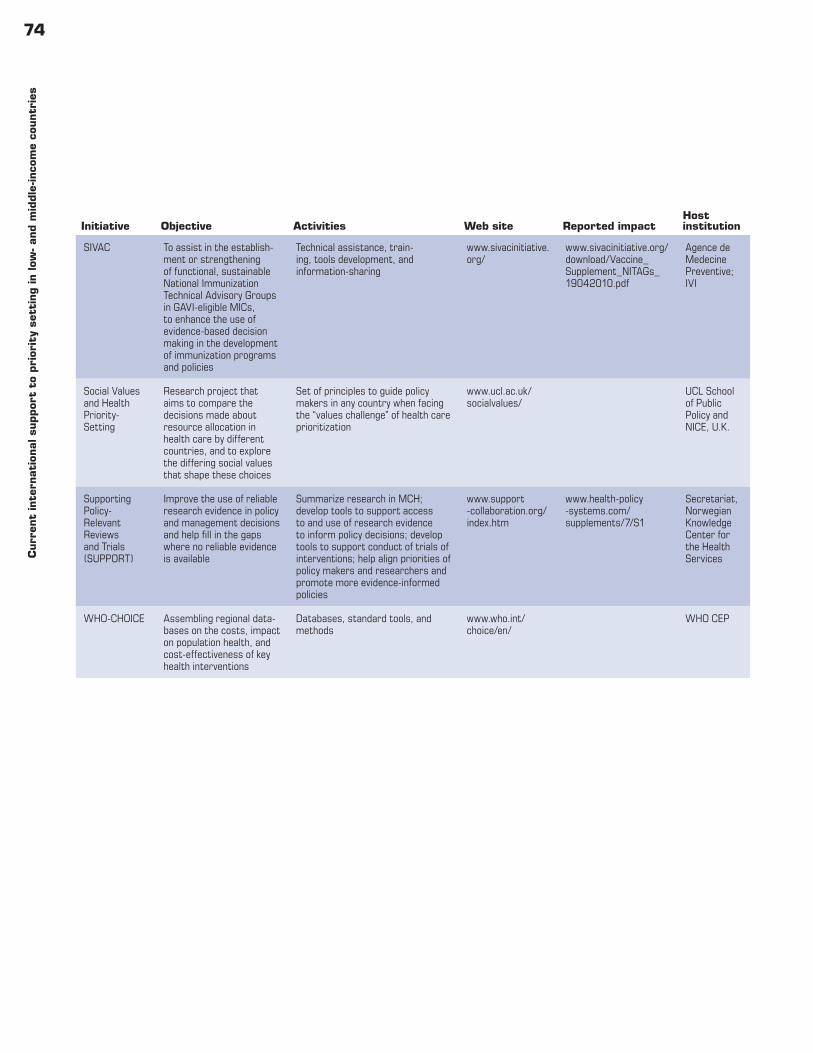
74C
urr
ent
inte
rnati
onal
suppor
t to
pri
orit
y se
ttin
g in
low
- an
d m
iddle
-inco
me
countr
ies
Initiative Objective Activities Web site Reported impactHost institution
SIVAC To assist in the establish-ment or strengthening of functional, sustainable National Immunization Technical Advisory Groups in GAVI-eligible MICs, to enhance the use of evidence-based decision making in the development of immunization programs and policies
Technical assistance, train-ing, tools development, and information-sharing
www.sivacinitiative.org/
www.sivacinitiative.org/download/Vaccine_ Supplement_NITAGs_ 19042010.pdf
Agence de Medecine Preventive; IVI
Social Values and Health Priority- Setting
Research project that aims to compare the decisions made about resource allocation in health care by different countries, and to explore the differing social values that shape these choices
Set of principles to guide policy makers in any country when facing the “values challenge” of health care prioritization
www.ucl.ac.uk/socialvalues/
UCL School of Public Policy and NICE, U.K.
Supporting Policy- Relevant Reviews and Trials (SUPPORT)
Improve the use of reliable research evidence in policy and management decisions and help fill in the gaps where no reliable evidence is available
Summarize research in MCH; develop tools to support access to and use of research evidence to inform policy decisions; develop tools to support conduct of trials of interventions; help align priorities of policy makers and researchers and promote more evidence-informed policies
www.support -collaboration.org/index.htm
www.health-policy -systems.com/supplements/7/S1
Secretariat, Norwegian Knowledge Center for the Health Services
WHO- CHOICE Assembling regional data-bases on the costs, impact on population health, and cost-effectiveness of key health interventions
Databases, standard tools, and methods
www.who.int/choice/en/
WHO CEP

75
Sources for low- and middle-income countries with health benefits plans
Appendix D
Central and Eastern Europe
Health insurance schemesCountry Source
Azerbaijan (SAMHI decree 2008)
USAID, PHCS, and Abt Associates, Azerbaijan Primary Healthcare Strengthening Project: Year 2 Annual Report (September 1, 2008–August 31, 2009), available at http://pdf.usaid.gov/pdf_docs/PDACQ985.pdf (accessed January 19, 2012).
Bulgaria (NHIF 1998) H3OK, National Health Insurance Fund — Bulgaria, available at www.en.nhif.bg/ (accessed January 19, 2012).
Croatia (HZZO) HZZO, What You Should Know about the Usage of Healthcare Services During Temporary Stay in the Republic of Croatia, available at www.hzzo-net.hr/03_03_05_eng.php (accessed January 19, 2012).
Estonia (EHIF 2001) Estonian Health Insurance Fund, available at www.haigekassa.ee/eng/ehif (last visited January 19, 2012).
Georgia (SMIC 1996) European Observatory on Health Systems and Policies, “Georgia — Health System Review.” 2 Health Syst Transition (2009), available at www.euro.who.int/__data/assets/pdf_file/0003/85530/E93714.pdf (last visited January 19, 2012).
Hungary (OEP 1992) Orsza´gos Ege´szse´gbiztosı ta´si Pe´nzta r.[Health Care in Hungary]. Available at www.oep.hu/portal/page?_ pageid=34,1&_dad=portal&_schema=PORTAL (last visited January 19, 2012).
Kyrgyz Republic (MHIF 1996)
European Observatory on Health Systems and Policies, “Kyrgyzstan — Health System Review.” 13 Health Syst Transition (2011), available at www.euro.who.int/__data/assets/pdf_file/0017/142613/e95045.pdf (last visited January 19, 2012).
Lithuania (NHIF) VLK, National Health Insurance Fund under the Ministry of Health, available at www.vlk.lt/vlk/en/?l=info&id=175 (last visited January 19, 2012).
Macedonia (HIFM) Health Insurance Fund of Macedonia, Health Insurance Fund of Macedonia, available at www.fzo.org.mk/default-en.asp (last visited January 19, 2012).
Moldova (MHI 2002) E. Richardson, B. Roberts, V. Sava, R. Menon, and M. McKee, Health Insurance Coverage and Health Care Access in Moldova. Health Policy Plan (March 26, 2011) [e-pub ahead of print], available at http://heapol.oxfordjournals.org/content/early/2011/03/26/heapol.czr024.abstract (last visited January 19, 2012.
Poland (NFZ 1999) Narodowy Fundusz Zdrowia [Ministry of Health — Poland], available at www.nfz.gov.pl/new/ (last visited January 19, 2012).
Romania (NHIF 2002)
European Observatory on Health Systems and Policies, “Romania — Health System Review.” 10 Health Syst Transition (2008), available at www.euro.who.int/__data/assets/pdf_file/0008/95165/E91689.pdf (last visited January 19, 2012).
Russia (MHIF1993) Federal Fund — Russia, available at www.ffoms.ru/portal/page/portal/top/index (last visited January 19, 2012).
Slovenia (HIIS 1992) Zavod za zdravstveno zavarovanje Slovenije, Health Insurance Institute of Slovenia, available at www.zzzs.si/indexeng.html (last visited January 19, 2012).

76S
ourc
es f
or low
- an
d m
iddle
-inco
me
countr
ies
wit
h h
ealt
h b
enefi
ts p
lans
Tax-funded systems
Armenia (SHA 1998) Armenian Health Insurance Fund, available at www.pag.am/ (last visited January 19, 2012).
Kazakhstan (MOH 2005)
Ministry of Health of Republic of Kazakhstan. Welcome!, available at www.mz.gov.kz/index.php?wakka=/Eng (last visited January 19, 2012).
Slovak Republic (MOH)
Ministerstvo zdravotnı ctva SR. Slovakia Ministry of Health, available at www.health.gov.sk/ (last visited January 19, 2012).
Tajikistan (MOH 2007)
[Ministry of Health — Tajikistan], available at www.health.tj/en/ (last visited January 19, 2012).
Latin America and Caribbean
Health insurance schemes
Argentina (PMO 1997)
Pan American Health Organization, Profile of the Health Services System Argentina (February 25, 2002), available at http://new.paho.org/hq/dmdocuments/2010/Health_System_Profile-Argentina_ 2002.pdf (last visited January 19, 2012).
Chile (AUGE) Auge en Línea — Fonasa, available at http://augeenlinea.fonasa.cl/portal/ (accessed January 19, 2012).
Colombia (POS1993)a Ministry of Social Protection, Republic of Colombia, Última jornada de socialización del texto final de la GPC sobre el manejo del Asma infantil, available at www.pos.gov.co/Paginas/default.aspx (last visited January 19, 2012).
Dominican Republic (SENASA 2002)
SeNaSa, Seguro nacional de salud, available at www.arssenasa.gov.do/index/gsau.asp (last visited January 19, 2012).
Nicaragua (Listado de Prestaciones Médicas Quirurgicas de Salud)
Ursula Giedion, Personal Communication (February 27, 2012); Gobierno de Reconciliación y Unidad Nacional [Ministry of Health — Nicaragua], available at www.minsa.gob.ni/ (last visited January 19, 2012).
Peru (PEAS 2009) MINSA inició difusión del Plan Esencial de Aseguramiento de Salud (PEAS), available at www.infomediarios.com/2009/06/22/minsa-inicio-difusion-del-planesencial-de-aseguramiento-desalud -peas/ (last visited January 19, 2012).
Uruguay (PIAS 2007) D. Aran, Sistema de salud de Uruguay, available at www.scielosp.org/pdf/spm/v53s2/21.pdf (Last visited March 2, 2012).
Tax-funded systems
Argentina (Plan Nacer 2005)
Plan Nacer. Noticias, available at www.plannacer.msal.gov.ar/ (last visited January 19, 2012).
Bolivia (SUMI 2003) World Bank, Health Sector Reform in Bolivia: A Decentralization Case Study. Washington, DC: World Bank (2004), available at http://books.google.com/books?id=uzWxjAg9ziYC&pg=PA4&lpg=PA4&dq= Bolivia+SUMI&source=bl&ots=l0K2rDKYnN&sig=CPvafEssR7uxMSsWIni48rak_tg&hl=en&ei= P1N6TujOEOb40gGYztncAg&sa=X&oi=book_result&ct=result&resnum=9&ved=0CGkQ6AEwCA#v= onepage&q=Bolivia%20SUMI&f=false; http://publications.paho.org/english/Bolivia_OP_213.pdf (last visited January 19, 2012).
Brazilb Lista de Medicamentos de Referencia, available at www.scribd.-com/doc/73742931/Lista-de -Medicamentos-SUS-I (last visited March 2, 2012).

77S
ources for low
- and m
iddle-in
come cou
ntries w
ith h
ealth b
enefi
ts plan
s
Honduras (IHSS 1995)
IHSS (Instituto Hondureño de Seguridad Social), available at www.ihss.hn/Paginas/IHSS.aspx (last visited January 19, 2012).
Mexico (CAUSES 2001)
Comisión Nacional de Protección Social en Salud/Seguro Popular, Catálogo Universal de Servicios de Salud (CAUSES) (2010), available at www.seguro-popular.gob.mx/images/contenidos/Causes/catalogo_2010.pdf (last visited January 19, 2012).
Nicaragua (MINSA) United Nations Economic and Social Commission for Asia and the Pacific, Promoting Sustainable Strategies to Improve Access to Health Care in the Asian and Pacific Region (2009), available at www.unescap.org/esid/hds/pubs/2529/pub2529.pdf (last visited March 2, 2012).
Asia
Health insurance schemes
Lao People’s Democratic Republic (HEF 2008)
United Nations Economic and Social Commission for Asia and the Pacific (2009).
Philippines (PhilHealth 2006)
PhilHealth, Phillippine Health Insurance Corporation. Home page, available at www.philhealth.gov.ph/ (last visited January 19, 2012).
Vietnam (HCFP 2003)
World Bank Group, Vietnam: Partnershipin Health, available at http://translate.google.com/translate?hl=en&sl=vi&u=http://web.worldbank.org/WBSITE/EXTERNAL/COUNTRIES/EASTASIAPACIFICEXT/VIETNAMINVIETNAMESEEXTN/0,,contentMDK:20600263~pagePK:141137 ~piPK:141127~theSitePK:486752,00.html&ei=C2dyTtbgI (last visited January 19, 2012).
Tax-funded systems
Cambodia (HEF 2000)
P. Ir, M. Bigdeli, and W. Van Damme, “Translating Knowledge into Policy and Action to Promote Health Equity: The Health Equity Fund Policy Process in Cambodia 2000–2008.” 96 Health Policy 200–209 (2010).
China (NRCMS 2003) World Bank, Reforming China’s Rural Health System, available at http://issuu.com/world.bank.publications/docs/9780821379820 (last visited January 19, 2012).
India (NRHM 2005) Ministry of Health and Family Welfare, Government of India, National Rural Health Mission, available at http://mohfw.nic.in/NRHM.htm (last visited January 19, 2012).
Malaysia (MOH) Ministry of Health Malaysia, Official Portal. Available at www.moh.gov.my/ (last visited January 19, 2012).
Thailand (UCS 2001) D. Hughes and S. Leethongdee, “Universal Coverage in the Land of Smiles Lessons from Thailand’s 30 Baht Health Reforms.” 26 Health Affairs 999–1008 (2007), available at http://content.healthaffairs.org/content/26/4/999.full (last visited January 19, 2012).
Middle East and North Africa
Health insurance schemes
Egypt (HIO 1964) Health Insurance Organization. Home page, available at http://hioegypt.org/english.aspx (last visited January 19, 2012).
Israel (NIII 1995) National Insurance Institute of Israel. Home page, available at www.btl.gov.il/English%20homepage/Pages/default.aspx (last visited January 19, 2012).

78S
ourc
es f
or low
- an
d m
iddle
-inco
me
countr
ies
wit
h h
ealt
h b
enefi
ts p
lans
Lebanon (CNSS) CNSS–Lebanon, available at http://cnss.gov.lb/ (last visited January 19, 2012).
Malta (NHS 1956) European Observatory on Health Care Systems, Health Care Systems in Transition — Malta, available at www.euro.who.int/__data/assets/pdf_file/0008/95129/E67140.pdf (accessed January 19, 2012).
Syria (NHIS 2010) Joint Learning Network, Syria: Healthcare Reforms, available at http://jointlearningnetwork.org/blog/2011/jun/29/syria-healthcarereforms (last visited January 19, 2012).
Tunisia (CNAM 2007) Republic of Tunisia, Ministry of Social Affairs. Home page, available at www.cnam.nat.tn/ (last visited January 19, 2012).
United Arab Emirates (Daman 2006)
Daman Health. Home page, available at www.damanhealth.ae/eDamanApp/en/home/index.html?version=R110.8.9 (last visited January 19, 2012).
West Bank and Gaza (GHI)
World Bank, West Bank and Gaza Health Policy Report: Reforming Prudently Under Pressure — -Health Financing Reform and the Rationalization of Public Sector Health Expenditures, available at http://siteresources. worldbank.org/INTWESTBANKGAZA/Resources/WBGHealthPolicyReport.pdf (last visited January 19, 2012).
Yemenc WHO, Country Cooperation Strategy for WHO and the Republic of Yemen: 2008–2013, available at www.who.int/countryfocus/cooperation_strategy/ccs_yem_en.pdf (last visited January 19, 2012).
Tax-funded systems
Bahrain (MOH 1979) Ministry of Health, Bahrain. Home page, available at www.moh.gov.bh/ar (last visited January 19, 2012).
Djibouti (MOH) Ministry of Health,Djibouti, Home Page, available at www.ministere-sante.dj/djibalger.php (last visited October 28, 2011).
Jordan (MOH 1965) WHO, Country Cooperation Strategy for WHO and Jordan: 2003–2007, available at www.who.int/countries/en/cooperation_strategy_jor_en.pdf (last visited January 19, 2012).
Morocco (AMO 2005)
Agence Nationale de l’Assurance Maladie, Missions, available at www.assurancemaladie.ma/anam.php?id_espace=1&id_srub=2 (last visited January 19, 2012).
Oman (MOH) Ministry of Health–Sultanate of Oman, Home Page, available at www.moh.gov.om/ (last visited January 19, 2012).
Qatar (SCH) State of Qatar Supreme Council of Health. Home page, available at www.sch.gov.qa/sch/En/ (last visited January 19, 2012).
Saudi Arabia (NHS) Kingdom of Saudi Arabia, Ministry of Health. Home page, available at www.moh.gov.sa/en/Pages/Default.aspx (last visited January 19, 2012).
Sub-Saharan Africa
Health insurance schemes
Ghana (NHIS 2004) National Health Insurance Scheme, NHIS Benefits Package, available at www.nhis.gov.gh/ ?CategoryID=158&ArticleID=120 (last visited January 19, 2012).
Kenya (NHIF 1998) NHIF. Home page, available at www.nhif.or.ke/healthinsurance/ (last visited January 19, 2012).
Namibia (NMBFd) N. Smit, “SSC Mulls National Medical Aid.” The Namibian (September 15, 2011), available at www.namibian.com.na/news-articles/national/full-story/archive/2011/september/article/ssc-mulls-nationalmedical-aid/ (last visited January 19, 2012).

79S
ources for low
- and m
iddle-in
come cou
ntries w
ith h
ealth b
enefi
ts plan
s
Nigeria (NHIS 1999) National Health Insurance Scheme. Welcome page. www.nhis.gov.ng/ (last visited January19, 2012).
Senegal (CBHI) J. Jütting, Health Insurance for the Rural Poor?, available at www.oecd.org/dataoecd/31/38/ 2510517.pdf (last visited January 19, 2012).
South Africa (NHIe) G. Khumalo, “SA gears for National Health Insurance” (August 12, 2011), available at www.southafrica.info/about/health/nhi-120811.htm (last visited January 19, 2012).
Tanzania (NHIF 1999) National Health Insurance Fund. Home page, available at www. nhif.or.tz/ (last visited January 19, 2012).
Uganda (NHIf) “Uganda Health Insurance to Improve Lives,” available at http://allafrica.com/stories/ 200906010116.html (last visited March 2, 2012).
Tax-funded systems
Uganda (UNMHCP 1999)
F. Ssengoooba, Uganda’s Minimum Health Care Package: Rationing within the Minimum?, available at https://tspace.library.utoronto.ca/bitstream/1807/6031/1/hp04005.pdf (last visited March 11, 2011).
Zambia (MOH 1993) USAID, HSSP, Strengthening Human Resources for Health. Occasional Paper Series 1 (April 2006), available at www.abtassociates.com/reports/HSSP_HRSynthesis1.pdf (last visited January 19, 2012).
NotesAMO = Compulsory Health Insurance; AUGE = Regime of Explicit Health Guarantees; CAUSES = Catálogo Universal de Servicios de Salud; CBHI = Community-based Health Insurance; CNAM = La Caisse Nationale d’Assurance Maladie de Tunisie; CNSS = National Social Security Fund; EHIF = Estonian Health Insurance Fund; GHI = Government Health Insurance ; HCFP = Health Care Pool Fund; HEF = Health Equity Funds; HIFM = Health Insurance Fund of Macedonia; HIIS = Health Insurance Institute of Slove-nia; HIO = Health Insurance Organization; HZZO = Croatian Institute of Health Insurance; IHSS = Instituto Hondureño de Seguridad Social; MHI = Mandatory Health Insurance ; MHIF = Mandatory Health Insurance Fund (Kyrgyz Republic, Romania); MHIF = Mandatory Health Insurance Funds (Russia); MINSA = Ministerio de Salud; MOH = Ministry of Health; NFZ = Narodowy Fundusz Zdrowia; NHI = National Health Insurance; NHIF = National Health Insurance Fund; NHIS = National Health Insurance Scheme; NHS = National Health Service; NIII = National Insurance Institute of Israel; NMBF = National Medical Benefit Fund; NRCMS = New Rural Cooperative Medical System; NRHM = National Rural Health Mission; OEP = National Health Care Fund/Országos Egészségbiztosítási Pénztár; PEAS = Plan Esencial de Aseguramiento de Salud; PIAS = Plan Integral de Atención en Salud; PMO = Compulsory Medical Plan; POS = Plan Obligatorio de Salud; SCH = Supreme Council of Health; SENASA = Proceso de tras-paso al Seguro Nacional de Salud; SHA = State Health Agency; SAMHI = State Agency on Mandatory Health Insurance; SMIC = State Medical Insurance Company; SUMI = Seguro Universal Materno Infantil; UCS = Universal Coverage Scheme; UNMHCP= Uganda National Minimum Health Care Package.a. Benefits package was designed with a TA from the World Bank and AIF (Personal communication with U. Giedion and M. Dinarte,
January 2012).b. The lists are conditional on Department of Science and Technology (DECIT) evaluation.c. In planning as of 2009.d. In progress.e. Being established in 2012.f. Proposed.

80
References
Amole, C., C. Brisebois, S. Essajee, E. Koehler, A. Levin, M. Moore, D. Brown, J. Sickler, and I. Singh. 2011. “Optimiz-ing Antiretroviral Product Selection: A Sample Approach to Improving Patient Outcomes, Saving Money and Scaling Up Health Services in Developing Countries.” Journal of Acquired Immune Deficiency Syndromes 57 (August): 100–03.
Anand, S., and K. Hanson. 1997. “Disability Adjusted Life Years: A Critical Review.” Journal of Health Economics 16 (6): 685–702. Available at http://economics.ouls.ox.ac.uk/12726/1/20506.pdf. Accessed March 2, 2012.
Baltussen, F., S. Youngkong, F. Paolucci, and L. Niessen. 2010. “Multi-criteria Decision Analysis to Prioritize Health Interventions: Capitalizing on First Experiences.” Health Policy 96 (3): 262–64.
Binagwaho, A., C. Wagner, and C. Nutt. 2011. “HPV Vaccine in Rwanda: Different Disease, Same Double Standard.” The Lan-cet 378 (9807): 1916. Available at www.lancet.com/journals/lancet/article/PIIS0140-6736(11)61837-0/fulltext. Accessed January 19, 2012.
Bisoffi, Z., S.B. Sirima, F. Meheus, C. Lodesani, F. Gobbi, A. Ang-heben, H. Tinto, B. Neya, K. Van den Ende, A. Romeo, and J. Van den Ende. 2011. “Strict Adherence to Malaria Rapid Test Results Might Lead to a Neglect of Other Dangerous Diseases: A Cost Benefit Analysis from Burkina Faso.” Malaria Jour-nal 10 (August): 226. Available at www.malariajournal.com/ content/pdf/1475-2875-10-226.pdf. Accessed May 31, 2012.
Bitran, R., and L. Escobar. 2008. The Politics of the AUGE Health Reform in Chile: A Case Study. Washington, DC: Results for Development Institute.
Bobadilla, J.L., P. Cowley, P. Musgrove, and H. Saxenian. 1994. “Design, Content and Financing of an Essential National Pack-age of Health Services.” Bulletin of the World Health Organiza-tion 72 (4): 653–62.
Bochenek, T. 2011. “Note on Comparative Analysis of Reference Countries Conducted as Part of the Working Group.” Center for Global Development, Washington, DC.
British Medical Association. 2011. “Summary of 2011/12 QOF Indicator Changes, Points and Thresholds.” Available at www.bma.org.uk/images/summaryqofguidance2011_v3_tcm41 -204734.pdf. Accessed May 14, 2012.
Bryson, M., P. Duclos, A. Jolly, and J. Bryson. 2010. “A Systematic Review of National Immunization Policymaking Processes.” Vaccine 28 (Suppl 1): A6–A12.
Budlender, D. 1999. The South African Women’s Budget Initia-tive. Paper presented at Meeting on Women and Political Participation: 21st Century Challenges, March 24–26, New Delhi. Available at www.equalinrights.org/fileadmin/filelist/documenten/14659_s-afr-wmn-budg-web.pdf. Accessed Janu-ary 19, 2012.
Buglioli, M., and A. Rodríguez. 2011. “Plan Integral de Atención a la Salud (PIAS).” PowerPoint presentation. Montevideo.
Bump, J.B., and M.R. Reich. 2011. “Analyzing the History of Diarrheal Disease Control on the Global Health Agenda.” Under review.
Cameron, A., M. Ewen, D. Ross-Degnan, D. Ball, and R. Laing. 2009. “Medicine Prices, Availability, and Affordability in 36 Developing and Middle-income Countries: A Secondary Analy sis.” The Lancet 373 (9659): 240–49.
Chaikledkaew, U., C. Lertpitakpong, Y. Teerawattananon, M. Thavorncharoensap, and V. Tangcharoensathien. 2009. “The Current Capacity and Future Development of Economic Eval-uation for Policy Decision-making: A Survey among Research-ers and Decision Makers in Thailand.” Value in Health 12 (Suppl 3): S31–S35.
Chanda, P., F. Masiye, B.M. Chitah, N. Sipilanyambe, M. Hawela, P. Banda, and T. Okorosobo. 2007. “A Cost-effectiveness Anal-ysis of Artemether Lumefantrine for Treatment of Uncompli-cated Malaria in Zambia.” Malaria Journal 6 (February): 21. Available at www.malariajournal.com/content/pdf/1475-2875-6-21.pdf. Accessed May 31, 2012.

81R
eferences
Chase, D., C. Rosten, S. Turner, N. Hicks, and R. Milne. 2009. “Development of a Toolkit and Glossary to Aid in the Adapta-tion of Health Technology Assessment (HTA) Reports for Use in Different Contexts.” Health Technology Assessment 13 (59). Available at www.hta.ac.uk/fullmono/mon1359.pdf. Accessed January 19, 2012.
Chisholm, D., and D. Evans. 2010. “Improving Health System Efficiency as a Means of Moving towards Universal Cover-age.” Background Paper 28 for the World Health Report 2010. Available at www.who.int/healthsystems/topics/financing/healthreport/28UCefficiency.pdf. Accessed May 31, 2012.
Clements, B., S. Gupta, and M. Nazaki. 2011. “What Happens to Social Spending in IMF-Supported Programs?” IMF Staff Discussion Note SDN/11/15, International Monetary Fund, Washington, DC. Available at www.imf.org/external/pubs/ft/sdn/2011/sdn1115.pdf. Accessed May 14, 2012.
Clinton, H.R., remarks by the U.S. Secretary of State at “A World in Transition: Charting a New Path in Global Health,” June 1, 2012, Oslo.
Cook, J., K.D. Frick, R. Baltussen, S. Resnikoff, A. Smith, J. Mecaskey, and P. Kilima. 2006. “Loss of Vision and Hearing.” In Disease Control Priorities in Developing Countries, 2nd ed., ed. Jamison, D., J.G. Breman, A.R. Measham, G. Alleyne, M. Claeson, D.B. Evans, P. Jha, A. Mills, and P. Musgrove, 953–62. Oxford, UK, and Washington, DC: Oxford University Press and World Bank.
Cookson, R., M. Drummond, and H. Weatherly. 2009. “Explicit Incorporation of Equity Considerations into Economic Evalu-ation of Public Health Interventions.” Health Economics, Policy and Law (April); 4 (Pt 2): 231–45.
Cooper, A., J. Skinner, L. Nherera, G. Feder, G. Ritchie, M. Katho-ria, N. Turnbull, G. Shaw, K. MacDermott, R. Minhas, C. Packham, H. Squires, D. Thomson, A. Timmis, J. Walsh, H. Williams, and A. White. 2007. Clinical Guidelines and Evidence Review for Post Myocardial Infarction: Secondary Prevention in Primary and Secondary Care for Patients Fol-lowing a Myocardial Infarction. London: National Collabo-rating Centre for Primary Care and Royal College of General Practitioners. Available at www.nice.org.uk/nicemedia/pdf/CG48FullGuideline.pdf.
Coulter, A., and C. Ham, eds. 2000. The Global Challenge of Health Care Rationing. Buckingham, UK: Open Univer-sity Press. Available at www.amazon.com/Global-Challenge -Health-Rationing-State/dp/0335204635. Accessed May 31, 2012.
Culyer, A.J., and M. Sculpher. 2008. “Lessons from Health Tech-nology Assessment.” In Economic Evaluation of Interventions for Occupational Health and safety: Developing Good Practice, ed. E. Tompa, A.J. Culyer, and R. Dolinschi, 51–69. Oxford, UK: Oxford University Press.
Culyer, A.J., C. McCabe, A. Briggs, K. Claxton, M. Buxton, R. Akehurst, M. Sculpher, and J. Brazier. 2007. “Searching for a Threshold, Not Setting One: The Role of the National Institute for Health and Clinical Excellence.” Journal of Health Services Research and Policy 12 (1): 56–58.
Doherty, J., and R. Govender. 2004. “The Cost-Effectiveness of Primary Care Services in Developing Countries: A Review of International Literature.” Disease Control Priorities Project Working Paper 37, World Bank, Washington, DC. Available at www.dcp2.org/file/49/wp37.pdf. Accessed January 19, 2012.
Donoghue, M., N. Druce, N. Avril, M. Ndour, and D. Lewis. 2010. “Review of GAVI Independent Review Committees (IRCs).” HLSP, London.
Duran, D., and A. Glassman. 2012. “An Index of the Quality of Official Development Assistance in Health.” CGD Work-ing Paper 287, Center for Global Development, Washing-ton, DC. Available at www.cgdev.org/content/publications/detail/1425926. Accessed May 14, 2012.
Evans, D.B., T. Adam, T.T. Edejer, S.S. Lim, A. Cassels, and T.G. Evans. 2005. “Time to Reassess Strategies for Improving Health in Developing Countries.” BMJ 331 (7525): 1133–1136.
Evans, D.B., A. Tandon, C. Murray, and J. Lauer. 1999. “The Com-parative Efficiency of National Health Systems in Producing Health: An Analysis of 191 Countries.” GPE Discussion Paper 29, World Health Organization, Geneva. Available at www.who.int/healthinfo/paper29.pdf. Accessed May 14, 2012.
Fenner, F., D.A. Henderson, I. Arita, Z. Ježek, and I.D. Ladnyi. 1988. Smallpox and Its Eradication. Geneva: World Health Organization.
Forsythe, S., J. Stover, and L. Bollinger. 2009. “The Past, Present and Future of HIV, AIDS and Resource Allocation.” BMC Public Health S4 9 (Suppl 1): S4.

82R
efer
ence
s
Gavaza, P., M. Shepherd, N. Shcherbakova, and S. Khoza. 2010. “The State of Health Economics and Pharmaceoconomics Research in Russia: A Systematic Review.” Journal of Pharma-ceutical Health Services Research 1 (3): 113–21.
GAVI Alliance. 2007. “GAVI Alliance Vaccine Investment Strat-egy: Recommended Process and Timeline.” Doc # AF1 Vaccine Investment Strategy, GAVI Alliance, Washington, DC.
———. 2009. “Vaccine Investment Strategy — GAVI’s Strate-gic Approach.” GAVI Alliance, Washington, DC. Accessed May 14, 2012.
———. 2011a. “Guidelines on Country Proposals for Support for New and Underused Vaccines, Applicable for Proposal Round June 2011.” Washington, DC. Available at www.gavialliance.org/library/documents/gavi-documents/guidelines-and -forms/guidelines-on-country-proposals-for-nvs-support-2011. Accessed May 14, 2012.
———. 2011b. “Terms of Reference of the Review of 2012 Coun-try Applications by the New Proposals Independent Review Committee (IRC).” Washington, DC. Accessed May 14, 2012.
Giedion, U. 2011. IDB Regional Study on the Design and Adjust-ment of Health Benefits Packages. Washington, DC: Prieto and Cid.
Giedion, U., A.L. Munoz, and A. Avila. 2012. Series de notas técni-cas sobre procesos de priorización de salud: Introducción a la serie de priorización explícita en salud. Nota técnica #IDB-TN-397. Washington, DC: Inter-American Development Bank. Available at http://idbdocs.iadb.org/wsdocs/getdocument. aspx?docnum=36829104. Accessed May 3, 2012.
———. Forthcoming. The need for a systemic process in priority set-ting. IDB strengthening priority-setting processes technical brief series. Nota técnica #IDB-TN-407. Washington, DC: Inter-American Development Bank.
Giedion, U., G. Panopoulou, and S. Gomez-Fraga. 2009. Diseño y ajuste de los planes explícitos de beneficios: el caso de Colombia y México. Santiago: Economic Commission for Latin Amer-ica. Available at www.eclac.org/publicaciones/xml/8/37988/lcl3131pe.pdf. Accessed May 14, 2012.
Glassman, A., T.A. Gaziano, C.P. Bouillon Buendia, and F.C. Guanais de Aguiar. 2010. “Confronting the Chronic Disease Burden in Latin America and the Caribbean.” Health Affairs 29 (12): 2142–48.
Glassman, A., M.R. Reich, K. Laserson, and F. Rojas. 1999. “Politi-cal Analysis of Health Reform in the Dominican Republic.” Health Policy and Planning 14 (2): 115–26.
The Global Fund (The Global Fund to Fight AIDS, Tuberculosis and Malaria). 2008. Five-year evaluation of the Global Fund. Evaluation Brief 5. Available at www.theglobalfund.org/en/terg/evaluations/5year/. Accessed June 1, 2012.
———. 2011a. “A Quick Guide to the Global Fund’s Price and Quality Reporting System (PQR).” The Global Fund, Geneva.
———. 2011b. “Eligibility, Counterpart Financing & Prioritiza-tion (ECFP) Policy: Frequently Asked Questions.” The Global Fund, Geneva.
———. 2011c. “Policy on Eligibility Criteria, Counterpart Financ-ing Requirements, and Prioritization of Proposals for Funding from the Global Fund.” Presented at the Twenty-Third Board Meeting, May 11–12, Geneva.
———. 2011d. “Value for Money Review Framework across Key Decision Points in the Grant Life Cycle.” The Global Fund, Geneva.
Goeree, R., J. He, D. O’Reilly, J.-E. Tarride, F. Xie, M. Lim, and N. Burke. 2011. “Transferability of Health Technology Assess-ments and Economic Evaluations: A Systematic Review of Approaches for Assessment and Application.” ClinicoEconom-ics and Outcomes Research 3 (June): 89–104.
Goetghebeur, M.M., M. Wagner, H. Khoury, D. Rindress, J.-P. Grégoire, and C. Deal. 2010. “Combining Multicriteria Deci-sion Analysis, Ethics and Health Technology Assessment: Applying the EVIDEM Decision-making Framework to Growth Hormone for Turner Syndrome Patients.” Cost Effec-tiveness and Resource Allocation 8 (April): 4.
González-Pier, E., C. Gutiérrez-Delgado, S. Gretchens, M. Bar-raza-Llorenz, R. Porras-Condey, N. Carvalho, et al. 2006. “Pri-ority setting for health interventions in Mexico’s System for Social Protection in Health.” The Lancet 368: 1608–18.
Gureje, O., D. Chisholm, L. Kola, V. Lasebikan, and S. Saxena. 2007. “Cost-effectiveness of an Essential Mental Health Inter-vention Package in Nigeria.” World Psychiatry 6 (February): 42–48. Available at www.ncbi.nlm.nih.gov/pmc/articles/PMC1805717/. Accessed May 31, 2012.
Ham, C., and G. Robert. 2003. Reasonable Rationing: Interna-tional Experience of Priority Setting in Health Care. Philadel-phia: Open University Press.

83R
eferences
Hauck, K., P.C. Smith, and M. Goddard. 2004. The Economics of Priority Setting for Health Care: A Literature Review. Washing-ton, DC: World Bank.
Hecht, R., ed. 2010. Costs and Choices: Financing the Long-Term Fight Against AIDS. Washington, DC: Results for Develop-ment Institute. Available at www.resultsfordevelopment.org/sites/resultsfordevelopment.org/files/resources/aids2031%20Cost%20&%20Choices.pdf. Accessed May 14, 2012.
Hensher, M. 2001. “Financing Health Systems through Efficiency Gains.” CMH Working Paper Series WG3:2, World Health Organization, Commission on Macroeconomics and Health, Geneva. Available at www.whoindia.org/LinkFiles/Commision _on_Macroeconomic_and_Health_03_02.pdf. Accessed May 31, 2012.
Hsiao, W.C., and P. Shaw. 2007. Social Health Insurance for Devel-oping Nations. Washington, DC: World Bank.
IDB (Inter-American Development Bank). Forthcoming. Proyecto de apoyo al fortalecimiento del proceso de priorización en salud en Colombia. Unpublished technical brief, Inter-American Devel-opment Bank, Washington, DC.
Iglesias, C.P., M.F. Drummond, J. Rovira, and NEVALAT Project Group. 2005. “Health-care Decision-making Processes in Latin America: Problems and Prospects for the Use of Economic Evaluation.” International Journal of Technology Assessment in Health Care 21 (Winter): 1–14.
IMF (International Monetary Fund). 2011. Romania: Fourth Review Under the Stand-By Arrangement and Request for Modification of Performance Criteria — Staff Report; Staff Sup-plement; Press Release on the Executive Board Discussion; and Statement by the Executive Director for Romania. IMF Coun-try Report 12/27. Available at www.imf.org/external/pubs/ft/scr/2012/cr1273.pdf. Accessed May 14, 2012.
Institute for Health Metrics and Evaluation. 2010. Financ-ing Global Health 2010: Development Assistance and Coun-try Spending in Economic Uncertainty. Seattle, WA: Insti-tute for Health Metrics and Evaluation. Available at www.healthmetricsandevaluation.org/publications/policy-report/financing-global-health-2010-development-assistance-and -country-spending-economic-uncertaint. Accessed April 13, 2012.
Institute of Medicine of the National Academies. 2011. Pre-paring for the Future of HIV/AIDS in Africa: A Shared
Responsibility. Washington, DC: Institute of Medicine of the National Academies.
International Health Policy Program, Thailand, and Health Intervention and Technology Assessment Program, Ministry of Public Health, Thailand. 2011. Research for Development of an Optimal Policy Strategy for Prevention and Control of Cervical Cancer in Thailand. Available at www.hitap.net/en/research/10481. Accessed February 22, 2012.
Jamison, D., J.G. Breman, A.R. Measham, G. Alleyne, M. Claeson, D.B. Evans, P. Jha, A. Mills, and P. Musgrove, eds. 2006. Dis-ease Control Priorities in Developing countries, 2nd ed. Oxford, UK, and Washington, DC: Oxford University Press and World Bank.
Jha, P., G. Aslanyan, M.G. Bergeron, D. Brown, R. Brunham, D. D’Alessandro, J. Hunkin, K. Kain, J. Kopelow, D.E. Low, A. McGeer, N. Nagelkerke, and F.A. Plummer. 2004. “Health and Economic Benefits of an Accelerated Program of Research to Combat Global Infectious Diseases.” Canadian Medical Asso-ciation Journal 171 (10): 1203–08.
Jit, M., N. Demarteau, E. Elbasha, G. Ginsberg, J. Kim, N. Prad-itsitthikorn, E. Sinanovic, and R. Hutubessy. 2011. “Human Papillomavirus Vaccine Introduction in Low-income and Mid-dle-income Countries: Guidance on the Use of Cost-effective-ness Models.” BMC Medicine 9 (May): 54.
Johannesson, M., and M.C. Weinstein. 1993. “On the Decision Rules of Cost-effectiveness Analysis.” Journal of Health Eco-nomics 12 (4): 459–67. Available at www.sciencedirect.com/science/article/pii/016762969390005Y. Accessed May 14, 2012.
Kapiriri, L. 2012. “Priority Setting in Low Income Countries: The Roles and Legitimacy of Development Assistance Partners.” Public Health Ethics 5 (1): 67–80.
Kapiriri, L., and D.K. Martin. 2006. “Priority Setting in Develop-ing Countries Health Care Institutions: The Case of a Ugan-dan Hospital.” BMC Health Services Research 6: 127.
———. 2010. “Successful Priority Setting in Low and Middle Income Countries: A Framework for Evaluation.” Health Care Analysis 18 (2): 129–47.
Kapiriri, L., O.F. Norheim, and K. Heggenhougen. 2003. “Using the Burden of Disease Information for Health Planning in Developing Countries: Experiences from Uganda.” Social Sci-ence and Medicine 56 (12): 2433–41.

84R
efer
ence
s
Kapiriri, L., O.F. Norheim, and D.K. Martin. 2009. “Fairness and Accountability for Reasonableness: Do the Views of Priority Set-ting Decision Makers Differ Across Health Systems and Levels of Decision Making?” Social Science & Medicine 68 (4): 766–73.
Kim, S.Y., S. Sweet, D. Slichter, and S.J. Goldie. 2010. “Health and Economic Impact of Rotavirus Vaccination in GAVI-eligible Countries.” BMC Public Health 10 (May): 253.
Kinney, E.D., and B.A. Clark. 2004. “Provisions for Health and Health Care in the Constitutions of the Countries of the World.” Cornell International Law Journal 37: 285–355. Available at http://indylaw.indiana.edu/instructors/Kinney/Articles/kinney_Constitutions.pdf.
Landwehr, C., and K. Böhm. 2011. “Delegation and Institutional Design in Health-care Rationing.” Governance 24 (Octo-ber): 665–88. Available at http://onlinelibrary.wiley.com/doi/10.1111/j.1468-0491.2011.01542.x/full. Accessed May 14, 2012.
Lai, T., J. Habicht, M. Reinap, D. Chisholme, and R. Baltussen. 2007. “Costs, Health Effects and Cost-effectiveness of Alco-hol and Tobacco Control Strategies in Estonia.” Health Policy 84 (1): 75–88. Available at www.alcsmart.ipin.edu.pl/files/cb03b_cea_alcohol_tob_estonia.pdf.
Leach-Kemon, K., D.P. Chou, M.T. Schneider, A. Tardif, J.L. Dieleman, B.P.C. Brooks, M. Hanlon, and C.J.L. Murray. 2012. “The Global Financial Crisis Has Led to a Slowdown in Growth of Funding to Improve Health in Many Developing Countries.” Health Affairs 31 (1): 228–35.
Leitenberg, M. 2006. Deaths in Wars and Conflicts in the 20th Century, 3rd ed. Occasional Paper 29, Cornell University Peace Studies Program. Ithaca, NY: Cornell University.
Long, L., A. Brennan, M.P. Fox, B. Ndibongo, I. Jaffray, I. Sanne, and S. Rosen. 2011. “Treatment Outcomes and Cost-Effec-tiveness of Shifting Management of Stable ART Patients to Nurses in South Africa: An Observational Cohort.” PLoS Medicine 8 (7): e1001055. Available at www.ncbi.nlm.nih.gov/pubmed/21811402. Accessed May 31, 2012.
MacLeod, H. 2010. “Defining the Package for a National Sys-tem.” National Health Insurance Policy Brief 10, Innovative Medicines South Africa, Houghton, South Africa. Available at www.imsa.org.za. Accessed May 14, 2012.
Markowitz, L., E. Dunne, M. Saraiya, H. Lawson, H. Chesson, and E. Unger. 2007. “Quadrivalent Human Papillomavirus
Vaccine Recommendations of the Advisory Committee on Immunization Practices.” MMWR Recommendations and Reports 56 (RR-2): 1–24. Available at www.cdc.gov/mmwr/preview/mmwrhtml/rr5602a1.htm. Accessed May 14, 2012.
Martins, J., and C. Maisonneuve. 2006. “The Drivers of Public Expenditure on Health and Long-term Care: An Integrated Approach.” OECD Economic Studies 43, Organisation for Economic Co-operation and Development, Paris. Available at www.oecd.org/dataoecd/62/19/40507566.pdf. Accessed May 14, 2012
Masis, D.P., O.P. Ortega, and R.D. Verano. 2008. “La carga eco-nomica de la enfermedad de Gaucher y Fabry en Colombia.” Fedesarrollo (August). Available at www.fedesarrollo.org.co/wp-content/uploads/2011/08/Carga-Econ-Gaucher-y-Fabry -D-Pinto.pdf Accessed February 23, 2012.
Miljeteig, I., S.A. Sayeed, A. Jesani, K.A. Johansson, and O.F. Norheim. 2009. “Impact of Ethics and Economics on End-of-life Decisions in an Indian Neonatal Unit.” Pediatrics 124 (2): e322–28.
Ministry of Health, Egypt, and Health Systems 20/20. 2010. National Health Accounts 2007/2008 Egypt Report. Bethesda, MD: Health Systems 20/20. Available at www.healthsystems2020.org/content/resource/detail/2730/. Accessed May 3, 2012.
Mulligan, J.A., D. Walker, and J. Fox-Rushby. 2006. “Economic Evaluations of Non-communicable Disease Interventions in Developing Countries: A Critical Review of the Evidence Base.” Cost Effectiveness and Resource Allocation 4 (April): 7.
Murray, C.J. 1994. “Quantifying the Burden of Disease: The Tech-nical Basis for Disability-adjusted Life Years.” Bulletin of the World Health Organization 72 (3): 429–45.
Murray, C.J., J. Kreuser, and W. Whang. 1994. “Cost-effectiveness Analysis and Policy Choices: Investing in Health Systems.” Bulletin of the World Health Organization 72 (4): 663–74.
National Audit Office. 2011. The Care Quality Commission: Regu-lating the Quality and Safety of Health and Adult Social Care. London: The Stationery Office.
Neumann, P.J., M.F. Drummond, B. Jonsson, B.R. Luce, J.S. Schwartz, U. Siebert, and S.D. Sullivan. 2010. “Are Key Prin-ciples for Improved Health Technology Assessment Supported and Used by Health Technology Assessment Organizations?” International Journal of Technological Assessment in Health

85R
eferences
Care 26 (1): 71–78. Available at http://journals.cambridge.org/action/displayFulltext?type=1&fid=7029668&jid= THC&volumeId=26&issueId=01&aid=7029660. Accessed May 29, 2012.
NICE (National Institute for Health and Clinical Excellence). 2009. “Developing Clinical and Health Improvement Indica-tors for the Quality and Outcomes Framework (QOF) Interim Process Guide.” Available at www.nice.org.uk/media/742/32/QOFProcessGuide.pdf. Accessed May 14, 2012.
———. 2010a. Health Economic Report: Net Health Ben-efits for NM07. Available at www.nice.org.uk/nicemedia/live/13071/50048/50048.pdf. Accessed May 14, 2012.
———. 2010b. “Quality and Outcomes Framework Programme NICE Cost Statement.” Available at www.nice.org.uk/nice-media/live/13071/50101/50101.pdf. Accessed May 14, 2012.
———. 2010c. “Review of Clinical Guideline (CG48) — Secondary Prevention in Primary and Secondary Care for Patients Follow-ing a Myocardial Infarction.” Available at www.nice.org.uk/nicemedia/live/11008/53347/53347.pdf. Accessed May 14, 2012.
———. 2010d. “Primary Care Quality and Outcomes Framework Indicator Advisory Committee Recommendations.” Available at www.nice.org.uk/nicemedia/live/13071/50050/50050.pdf. Accessed May 14, 2012.
Nielsen, C.P., T.M. Funch, and F.B. Kristensen. 2011. “Health Technology Assessment: Research Trends and Future Priori-ties in Europe.” Journal of Health Services Research & Policy 16 (Suppl 2): 6–15. Available at http://jhsrp.rsmjournals.com/content/16/suppl_2/6. Accessed February 23, 2012.
OECD (Organisation for Economic Co-operation and Develop-ment). n.d. Health Statistics database. Paris. Available at www.oecd.org/health/healthdata. Accessed January 19, 2012.
PAHO (Pan American Health Organization). 2010. Access to High-Cost Medicines in the Americas: Situation, Challenges and Perspectives. Technical Series No. 1 — Essential Medi-cine, Access, and Innovation. Washington, DC: Pan Ameri-can Health Organization. Available at http://new.paho.org/hq/dmdocuments/2011/Tech_Series_No.1_Dec_13_10_PM.pdf. Accessed May 14, 2012.
———. 2012. “Evaluacion e incorporacion de tecnologias sanitar-ias en los sistemas de salud.” CE150/16 Punto 4.6 del orden del dia provisional. 150a Sesion del Comite Ejecutivo, June 18–22, Washington, DC.
Pichon-Riviere, A., F. Augustovski, A. Rubinstein, S.G. Marty, S.D. Sullivan, and M.F. Drummond. 2010. “Health Technol-ogy Assessment for Resource Allocation Decisions: Are Key Principles Relevant for Latin America?” International Journal of Technology Assessment in Health Care 26 (4): 421–27.
Plumridge, H. 2010. “Rising Nations Are No Remedy for Big Pharma.” Wall Street Journal, May 25. Available at http://online.wsj.com/article/SB10001424052748704113504575264453499634626.html. Accessed May 14, 2012.
Politi, C., and V. Galayda. 2010. Analysis of Vaccine Financing Indi-cators from the WHO-UNICEF Joint Reporting Form (JRF) for the period 2000–2008. Geneva: World Health Organization.
Praditsitthikorn, N., Y. Teerawattananon, S. Tantivess, S. Limwat-tananon, A. Riewpaiboon, S. Chichareon, N. Ieumwananon-thachai, and V. Tangcharoensathien. 2011. “Economic Evalua-tion of Policy Options for Prevention and Control of Cervical Cancer in Thailand.” PharmacoEconomics 29 (9): 781–806.
Pwu, J. 2010. “Health Technology Assessment in Taiwan.” Pre-sented at ISPOR 4th Asia-Pacific Conference, September 5–7, Phuket, Thailand. Available at www.ispor.org/consortiums/asia/documents/ISPOR%20AsiaNetHTA%20Inauguration %20Presentations_For%20Website_Final.pdf. Accessed May 14, 2012.
Ramachandra, S., and W. Hsiao. 2007. Ghana: Initiating Social Health Insurance. Social Health Insurance for Developing Nations. Washington, DC: World Bank.
Rosen, S., I. Sanne, A. Collier, and J.L. Simon. 2005. “Rationing Antiretroviral Therapy for HIV/AIDS in Africa: Choices and Consequences.” PLoS Medicine 2 (11): 1098–1104. Available at www.equinetafrica.org/bibl/docs/ROSaids.pdf. Accessed May 14, 2012.
Rumbold, B., V. Alakeson, and P.C. Smith. 2012. Rationing Health Care. London: Nuffield Trust. Available at www.nuff-ieldtrust.org.uk/sites/files/nuffield/publication/rationing _health_care_240212_0.pdf. Accessed May 31, 2012.
Sassi, F., J. Le Grand, and L. Archard. 2001. “Equity Versus Effi-ciency: a Dilemma for the NHS. If the NHS Is Serious About Equity It Must Offer Guidance When Principles Conflict.” British Medical Journal 323: 762–63.
Saxenian, H., and R. Hecht. 2006. “HPV Vaccines: Costs and Financing.” Prepared for “Stop Cervical Cancer: Accelerating Global Access to HPV Vaccines” meeting, December 12–13,

86R
efer
ence
s
London. Available at www.rho.org/files/StopCxCa_financing _2006.pdf. Accessed May 14, 2012.
Schreyogg, J., T. Stargardt, M. Velasco-Garrido, and R. Busse. 2005. “Defining the ‘Health Benefit Basket’ in Nine European Countries.” European Journal of Health Economics 6 (Suppl 1): 2–10. Available at www.ncbi.nlm.nih.gov/pmc/articles/PMC1388078/. Accessed February 23, 2012.
Schwalbe, N. 2011. “Next Steps on New Vaccine Windows: HPV, JE, Rubella and Typhoid.” Report to the GAVI Alli-ance Board, November 16–17, Agenda Item 6. Available at www.gavialliance.org/about/governance/gavi-board/minutes/2011/16-nov/minutes/next-steps-on-new-windows/. Accessed May 31, 2012.
Schwartländer, B., J. Stover, T. Hallett, R. Atun, C. Avila, E. Gouws, M. Bartos, P.D. Ghys, M. Opuni, D. Barr, R. Alsal-laq, L. Bollinger, M. de Freitas, G. Garnett, C. Holmes, K. Legins, Y. Pillay, A.E. Stanciole, C. McClure, G. Hirnschall, M. Laga, and N. Padian. 2011. “Towards an Improved Invest-ment Approach for an Effective Response to HIV/AIDS.” The Lancet 377 (9782): 2031–41. Available at www.thelancet.com/journals/lancet/article/PIIS0140-6736(11)60702-2/abstract. Accessed May 29, 2012.
Shafie, A.A. 2011. Setting National Healthcare Priorities in Asia: Experiences from Malaysia. Paper presented at BMJ-NICE Conference, September 30, London.
Shah, M., B. Johns, A. Abimiku, and D.G. Walker. 2011. “Cost-effectiveness of New WHO Recommendations for Prevention of Mother-to-child Transmission of HIV in a Resource-limited Setting.” AIDS 25 (8): 1093–1102. Available at www.ncbi.nlm.nih.gov/pubmed/21505317. Accessed May 31, 2012.
Shillcutt, S.D., D.G. Walker, C.A. Goodman, and A.J. Mills. 2009. “Cost Effectiveness in Low- and Middle-Income Coun-tries: A Review of the Debates Surrounding Decision Rules.” PharmacoEconomics 27 (11): 903–17.
Smith, P.C. 2012. “Incorporating Financial Protection into Deci-sion Rules for Publicly Financed Healthcare Treatments.” Health Economics, January 13, doi: 10.1002/hec.2774. Avail-able at http://onlinelibrary.wiley.com/doi/10.1002/hec.2774/abstract. Accessed May 31, 2012.
Sorenson, C., M. Drummond, F.B. Kristensen, and R. Busse. 2008. How Can the Impact of Health Technology Assessment be Enhanced? Policy Brief. Copenhagen: WHO Regional Office
for Europe. Available at www.euro.who.int_data/assets/pdf_file/0019/73225/E93420.pdf. Accessed March 2, 2012.
Sridhar, D., and R. Batniji. 2008. “Misfinancing Global Health: A Case for Transparency in Disbursements and Deci-sion Making.” The Lancet 372 (9644): 1185–91. Available at http://download.thelancet.com/pdfs/journals/lancet/ PIIS0140673608614853.pdf. Accessed May 14, 2012.
Sweat, M.D., K.R. O’Reilly, G.P. Schmid, J. Denison, and I. de Zoysa. 2004. “Cost-effectiveness of Nevirapine to Pre-vent Mother-to-child HIV Transmission in Eight African Countries.” AIDS 18 (12): 1661–71. Available at www.crd.york.ac.uk/crdweb/ShowRecord.asp?AccessionNumber= 22004001172&UserID=0. Accessed May 31, 2012.
Tarn, Y.H., S. Hu, I. Kamae, B.M. Yang, S.C. Li, V. Tangcharoen-sathien, Y. Teerawattananon, S. Limwattananon, A. Hameed, S.M. Aljunid, and J.S. Bapna. 2008. “Health-care Systems and Pharmacoeconomic Research in Asia-Pacific region.” Value in Health 11 (Suppl 1): S137–55.
Tashobya, C.K., F. Ssengooba, and V. Cruz, eds. 2003. Health Systems Reforms in Uganda: Processes and Outputs. London: London School of Hygiene & Tropical Medicine.
Teerawattananon, Y., S. Russell, and M. Mugford. 2007. “A Sys-tematic Review of Economic Evaluation Literature in Thailand: Are the Data Good Enough to be Used by Policy-makers?” PharmacoEconomics 25 (6): 467–79.
U.K. Department of Health. 2004. National Service Framework for Coronary Heart Disease: Winning the War on Heart Dis-ease. London: Department of Health Publications. Available at www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4094275. Accessed February 22, 2012.
———. 2006. The NHS in England: Operating Frame-work for 2007–08. London: Department of Health Pub-lications. Available at www.dh.gov.uk/en/Publications andstatistics/Publications/PublicationsPolicyAndGuidance/DH_063267. Accessed February 22, 2012.
van den Ham, R., L. Bero, and R. Laing. 2011. “Selection of Essen-tial Medicines.” In World Medicines Situation 2011. Geneva: World Health Organization, Department of Essential Medi-cines and Pharmaceutical Policies. Available at http://apps.who.int/medicinedocs/documents/s18770en/s18770en.pdf. Accessed May 14, 2012.

87R
eferences
Walker, K. 2000. “Cost-comparison of DDT and Alternative Insecticides for Malaria Control.” Medicinal and Veterinary Entomology 14 (4): 345–54.
Walker, D., and J.A. Fox-Rushby. 2000. “Economic Evaluation of Communicable Disease Interventions in Developing Coun-tries: A Critical Review of the Published Literature.” Health Economics 9 (8): 681–98.
Walker, D., Y. Teerawattananon, R. Anderson, and G. Richard-son. 2010. “Generalisability, Transferability, Complexity and Relevance.” In Evidence-based Decisions and Economics: Health Care, Social Welfare, Education and Criminal Justice, ed. I. Shemlit, M. Mugford, L. Vale, K. Marsh, and C. Donaldson, 56–66. West Sussex, UK: John Wiley & Sons.
Weinstein, M.C., and W.B. Stason. 1977. “Foundations of Cost-Effectiveness Analysis for Health and Medical Practices.” New England Journal of Medicine 296 (13): 716–21.
WHO (World Health Organization). 1999. World Health Report 2000: Improving Performance. Geneva. Available at www.who.int/whr/2000/en/report.htm. Accessed October 19, 2012.
———. 2006. Immunization Financing Analysis — A Look across 50 Countries. Geneva: WHO. Available at www.who.int/immunization_financing/analysis/50_countries/en/index.html. Accessed May 14, 2012.
———. 2008. “The Tallinn Charter: Health Systems for Health and Wealth.” Available at www.euro.who.int/document/e91438.pdf. Accessed May 31, 2012.
———. 2010a. “Strengthening Monitoring and Evaluation of National Health Plans and Strategies: Operationalizing the CHeSS Framework.” Report of Technical Meeting, July 14–15, Glion, Switzerland. Available at www.inter-nationalhealthpartnership.net//CMS_files/documents/ chess_technical_meeting_-_glion,_14-15july2010_-_final_report_EN.pdf. Accessed May 14, 2012.
———. 2010b. World Health Report 2010. Geneva: WHO. Avail-able at www.who.int/whr/2010/10_chap04_en.pdf. Accessed May 31, 2012.
———. 2010c. “Human Papillomavirus and Related Cancers.” Summary Report Update, September 15, 2010. Geneva.
———. 2011. World Health Statistics 2011. Geneva. Available at www.who.int/whosis/whostat/2011/en/index.html. Accessed May 31, 2012.
Woo, P.P., J.J. Kim, and G.M. Leung. 2007. “What Is the Most Cost-effective Population-based Cancer Screening Program for Chinese Women?” Journal of Clinical Oncology 25 (6): 617–24. Available at www.ncbi.nlm.nih.gov/pubmed/17308266. Accessed May 31, 2012.
World Bank. 1993. World Development Report 1993: Investing in Health. Washington, DC: World Bank.
———. 2006. “Health Transitions, Disease Burdens, and Health Expenditure Patterns.” In Health Financing Revisited: A Prac-titioner’s Guide. Washington, DC: World Bank. Available at http://siteresources.worldbank.org/INTHSD/Resources/topics/Health-Financing/HFRChap1.pdf. Accessed May 14, 2012.
Xu, K., P. Saksena, and A. Holly. 2011. The Determinants of Health Expenditure. Working Paper December 2011. Geneva: Results for Development Institute and World Health Organization.
Yamin, A.E., and O.P. Vera. 2008. “The Role of Courts in Defin-ing Health Policy: The Case of the Colombian Constitutional Court.” Harvard Law School Working Paper, Harvard Uni-versity, Cambridge, MA. Available at www.law.harvard.edu/programs/hrp/documents/Yamin_Parra_working_paper.pdf. Accessed January 19, 2012.
Yang, B.M. and K.C. Lee. 2009. “Growing Application of Phar-macoeconomics and Outcomes Research in Health-care Deci-sion-making in the Asia-Pacific Region.” Value in Health 12 (Suppl 3): S1–2.
Yothasamut, J., S. Tantivess, and Y. Teerawattananon. 2009. “Using Economic Evaluation in Policy Decision-making in Asian Countries: Mission Impossible or Mission Probable?” Value in Health 12 (Suppl 3): S26–S30.
Youngkong, S., L. Kapiriri, and R. Baltussen. 2009. “Setting Pri-orities for Health Interventions in Developing Countries: A Review of Empirical Studies.” Tropical Medicine and Interna-tional Health 14 (8): 930–39.

ISBN 978-1-933286-73-0
Prio
rity-Settin
g in
Health
B
uild
ing in
stitu
tions fo
r smarte
r public sp
endin
g
Cente
r for G
lobal D
eve
lopm
ent