business plan nov2012 ebook
TRANSCRIPT

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 1/119
Pharmaceutical manufacturing Plan for africa
Business Plan

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 2/119
This document has been produced without ormal United Nations editing. The designations employed and the
presentation o the material in this document do not imply the expression o any opinion whatsoever on the part
o the Secretariat o the United Nations Industrial Development Organization (UNIDO) concerning the legal status
o any country, territory, city or area or o its authorities, or concerning the delimitation o its rontiers or
boundaries, or its economic system or degree o development. Designations such as “developed”, “industrialized”
and “developing” are intended or statistical convenience and do not necessarily express a judgment about the
stage reached by a particular country or area in the development process. Mention o rm names or commercial
products does not constitute an endorsement by UNIDO. The opinions, statistical data and estimates contained
in signed articles are the responsibility o the author(s) and should not necessarily be considered as refecting the
views or bearing the endorsement o UNIDO. Although great care has been taken to maintain the accuracy o
inormation herein, neither UNIDO nor its Member States assume any responsibility or consequences which may
arise rom the use o the material.
Cover photographs
Left image Shutterstock, Inc.Middle image Shutterstock, Inc.Right image Shutterstock, Inc.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 3/119
Pharmaceutical manufacturing Plan
for africa
Business Plan
Addis Ababa, 2012

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 4/119
ACKNOWLEDGEMENT
This Business Plan was developed by a partnership o the Arican Union Commission
(AUC) and the United Nations Industrial Development Organization (UNIDO) to accel-
erate the implementation o the Pharmaceutical Manuacturing Plan or Arica (PMPA),
with unding rom the German government. The Commission thereore extends special
appreciation to UNIDO or the resourceul collaboration through which this Business Plan
has been developed.
The Commission greatly appreciates all member states constituting the Technical Com-
mittee o the Pharmaceutical Manuacturing Plan or Arica rom North Arica (Egypt andLibya), West Arica (Ghana, Nigeria and Senegal), Central Arica (Burundi, Cameroon and
Gabon), East Arica (Kenya and Ethiopia) and Southern Arica (South Arica and Angola)
or their support to the process.
The Commission urther wishes to recognize the eort o other members o the Technical
Committee such as NEPAD Planning and Coordinating Agency, WHO, UNAIDS, Region-
al Economic Communities, Southern Arican Generic Manuacturers Association, Fed-
eration o Arican Pharmaceutical Manuacturers Associations, COHRED, EDCTP, and
ANDI, who since joining the Technical Committee, have supported the implementation o
its broadened mandate.
The Commission thanks all the organizations including members o the consortium o theAMRH Programme that are supporting Arica’s development agenda through implement-
ing programmes geared towards promoting access to quality aordable medicines.
The Commission acknowledges the eorts o the authors o the Business Plan, a team com-
posed o Dr. Skhumbuzo Ngozwana & Mr. Alastair West rom UNIDO and Dr. Ademola
Olajide & Dr. Janet Byaruhanga rom the Health, Nutrition and Population Division o the
AUC Department o Social Aairs.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 5/119
iii
FOREWORD
During the last decade promoting sustainable access to quality and aordable medicines
and integrating local production as part o the overall health systems strengthening package
has been o signicant concern to Arican leaders.
A viable pharmaceutical industry in Arica shall not only impact on the Arican health sys-
tem and its capacity to respond to the health needs o the people but also will contribute to
the overall socioeconomic development o the continent.
For this reason, Arican governments have committed to enhancing the attainment o one o the set targets o the 8th Millennium Development Goal, to increase the proportion o the
population with access to aordable essential drugs on a sustainable basis.
The Arican Union Commission has been at the oreront in galvanizing the necessary po-
litical will and providing the leadership to the broad range o processes required or promot-
ing a sustainable local pharmaceutical industry.
The Commission has made signicant eorts towards ensuring delivery on set objectives o
Arica’s highest decision making body (The Assembly o Heads o State and Government)
as they relate to the implementation o a Pharmaceutical Manuacturing Plan or Arica
(PMPA). These range rom conducting studies to establish Arica’s local pharma production
capacity, building strategic partnerships required or the development o a concrete actionplan, to engaging governments in the development o the Business Plan or the operation-
alization o the PMPA.
This Business Plan is a product o multi-stakeholder eorts all geared towards providing a
package o solutions to address the various challenges conronting the Arican pharma sec-
tor in general. It is not an end in itsel but rather a means through which governments either
through their national systems or regional economic communities will engage with relevant
partners to implement specic activities according to their unique needs/priorities.
The road ahead remains long and challenging but the desired objectives remain compelling
and non-negotiable. Consequently I invite all stakeholders rom member state governments
to Regional Economic Communities; rom the Private or Prot Sector to Donors and De-
velopment partners to strategically engage and collaborate, creating the unity o purpose
and necessary synergies to realize the noble objectives o this Business Plan.
Bience P. Gawanas
Commissioner or Social Aairs

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 6/119
iv
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 7/119
v
contentS
acKnoWleDgement ...........................................................................................................
oreWorD ..........................................................................................................................
ls abbvs .......................................................................................................... v
ls s ....................................................................................................................... x
ls tbs ....................................................................................................................... x
eXecutiVe SummarY ..........................................................................................................1
SWot analYSiS ................................................................................................................... 6
1. id d Bkd ..........................................................................................11
1.1 THE STRATEGIC CONTEXT OF AFRICA’S HEALTHCARE CHALLENGES ................................ 12
1.2 THE PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA ........................................... 18
1.3 BUSINESS PLAN ................................................................................................................ 20
1.4 SUMMARY OF CHAPTER 1 ................................................................................................. 22
2. ovvw P m a .................................................... 25
2.1 INTRODUCTION: THE PHARMACEUTICAL MANUFACTURING SYSTEM ................................ 25
2.2 THE CURRENT STATUS OF THE PHARMACEUTICAL INDUSTRY AND
OTHER STAKEHOLDERS ...................................................................................................29
2.3 CHALLENGES AND OPPORTUNITIES FOR LOCAL PRODUCTION ........................................472.4 SUMMARY OF CHAPTER 2 ................................................................................................ 54
3. Ss .........................................................................................................................57
3.1 THE GENERIC SOLUTIONS PACKAGE .................................................................................58
3.2 OTHER ACTIVITIES ...........................................................................................................77
3.3 SUMMARY OF CHAPTER 3 ................................................................................................ 82
4. ip P ..................................................................................................... 85
4.1 PHASED APPROACH TO IMPLEMENTATION ...................................................................... 86
4.2 STAKEHOLDER ENGAGEMENT .......................................................................................... 91
4.3 PROPOSED STRUCTURE FOR DELIVERING THE PMPA ....................................................93
4.4 RESOURCE REQUIREMENTS ............................................................................................95
4.5 MONITORING AND EVALUATION .......................................................................................99
4.6 RISK MANAGEMENT.........................................................................................................101
4.7 SUMMARY OF CHAPTER 4 .............................................................................................. 102

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 8/119
vi

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 9/119
vii
LisT OF AbbREviATiONs
AA artesunate/amodiaquineACT Artemisinin-based Combination Therapy
ADB Arican Development Bank
AL artemether/lumeantrine
ALMA Arican Leaders Malaria Alliance
AMFm Aordable Medicines Facility or malaria
AMRH Arican Medicines Regulatory Harmonization
ANDA Abbreviated New Drug Application
ANDI Arican Network or Drugs and Diagnostics Innovation
API Active Pharmaceutical Ingredient
ARIPO Arica Regional Intellectual Property Organization
ARV antiretroviral drug
BA/BE Bioavailability/BioequivalenceAU Arican Union
AUC Arican Union Commission
BRIC Brazil, Russia, India and China
CCATP Collaborating Centre or Advocacy and Training in Pharmacovigilance
CHAI Clinton Health Access Initiative
CL Compulsory Licence
CMS Central Medical Store
COHRED Council on Health Research or Development
CSIR Council or Scientic and Industrial Research (RSA)
CTD Common Technical Document
DE Data Exclusivity
DFI Development Finance InstitutionDFID Department or International Development (UK)
DNDi Drugs or Neglected Diseases Initiative
DRC Democratic Republic o Congo
EAC East Arican Community
ECCAS Economic Community o Central Arican States
ECOWAS Economic Community o West Arican States
EDL Essential Drugs List
EGA European Generic Medicines Association
EIU Economist Intelligence Unit
EMA European Medicines Agency
EML Essential Medicines List
FDA Food and Drug Administration (U.S.)
FDC Fixed Dose Combination
FEAPM Federation o East Arican Pharmaceutical Manuacturers
FKPM Federation o Kenyan Pharmaceutical Manuacturers
GDP Good Distribution Practice
GIZ Deutsche Gesellschat uer Internationale Zusammenarbeit
GLP Good Laboratory Practice
GMP Good Manuacturing Practice
GWP Good Warehousing Practice
GPO Government Pharmaceutical Organization (Thailand)
HAI Health Action International
HAT Human Arican Trypanosomiasis

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 10/119
viii
ICH International Conerence on Harmonisation o Technical Requirements
or Registration o Pharmaceuticals or Human Use
IDMA Indian Drug Manuacturers’ Association
IFC International Finance Corporation
IFHA Investment Fund or Health in Arica
IPA Indian Pharmaceutical Association
IPO Initial Public Oering
HR Human Resource
ICT Inormation and Communications Technology
KEMRI Kenya Medical Research Institute
KETAM Kenya chapter o the Pan Arican Treatment Access Movement
KSP Kilimanjaro School o Pharmacy
LEAP Leishmaniasis East Arica Platorm
LDC Least Developed Country
LNCPP Laboratoire National de Contrôle des Produits Pharmaceutiques (Algeria)
MASC Medicines and Allied Substances ControlMDR-TB multidrug-resistant tuberculosis
M & A Mergers and Acquisitions
M & E Monitoring and Evaluation
MCAZ Medicines Control Authority o Zimbabwe
MCC Medicines Control Council (RSA)
MeTA Medicines Transparency Alliance
MMV Medicines or Malaria Venture
MoF Ministry o Finance
MoH Ministry o Health
MRC South Arican Medical Research Council
MSF Medecins sans Frontieres
MUHAS Muhimbili University o Health and Allied Sciences (Tanzania)NAFDAC National Agency or Food and Drug Administration and Control (Nigeria)
NEPAD New Partnership or Arica’s Development
NGO Non-Governmental Organisation
NIPER National Institute o Pharmaceutical Education and Research
NMRA National Medicines Regulatory Authority
NRF National Research Foundation (RSA)
OECD Organisation or Economic Co-operation and Development
PDP Product Development Partnership
PE Private Equity
PEPFAR U.S. President’s Emergency Plan or AIDS Relie
PIC/S Pharmaceutical Inspection Co-operation Scheme
PMAG Pharmaceutical Manuacturers Association o GhanaPMI Presidents’s Malaria Initiative (U.S.)
PMPA Pharmaceutical Manuacturing Plan or Arica
PPP Public Private Partnership
QC Quality Control
QMS Quality Management System
R & D Research and Development
REC Regional Economic Community
RoK Republic o Korea
RSA Republic o South Arica
SADC Southern Arican Development Community
SAGMA Southern Arican Generic Medicines Association
SARPAM Southern Arican Regional Programme on Access to Medicines andDiagnostics
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 11/119
ix
SEZ Special Economic Zone
SLF Saint Luke Foundation (Tanzania)
SMZ Sulamethoxazole
SPC Supplementary Protection Certicate
SRA Stringent National Medicines Regulatory Authority
SSA sub-Saharan Arica
TA Technical Assistance
ToR Terms o Reerence
TPI Tanzanian Pharmaceutical Industries
TPM Total Productive Maintenance
TPS Toyota Production System
TRIPS Trade and Related Aspects o Intellectual Property Rights
UK United Kingdom
US United States o America
USP U.S. Pharmacopeial Convention
XDR-TB extensively drug-resistant tuberculosisUNAIDS Joint United Nations Programme on HIV/AIDS
UNCTAD United Nations Conerence on Trade and Development
UNDP United Nations Development Programme
UNICEF United Nations Children’s Fund
UNIDO United Nations Industrial Development Organization
VC Venture Capital
WAHO West Arican Health Organisation
WAPMA West Arican Pharmaceutical Manuacturers Association
WHO World Health Organization
WIPO World Intellectual Property Organization
WTO World Trade Organization

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 12/119
x
LisT OF FiGuREs
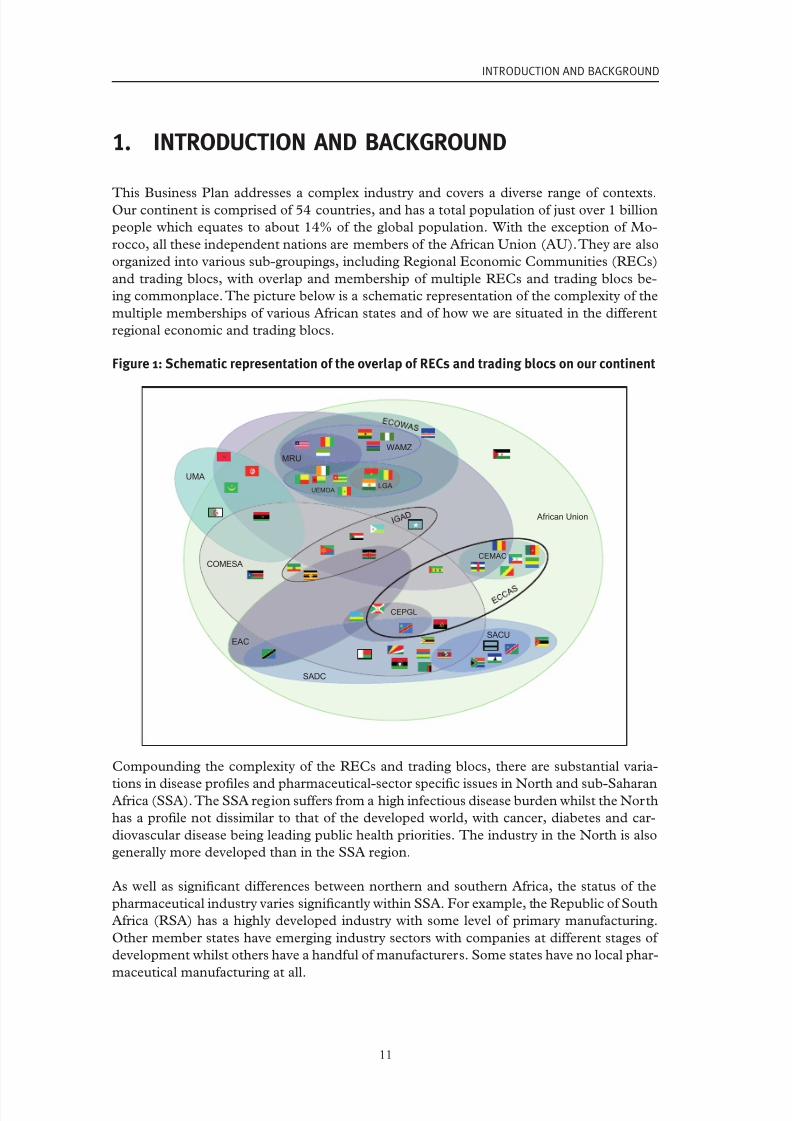
Figure 1: Schematic representation o the overlap o RECs and trading blocs onour continent ...................................................................................................................11
Figure 2: Arican Pharma Growth Drivers, ............................................................................... 14
Figure 3: Table rom AEI working paper by R. Bate ................................................................. 17
Figure 4: Schematic representation o the small molecule ‘Pharmaceutical manuacturing
system’.......................................................................................................................26
Figure 5: Typical operations o a local oral solid dosage orm manuacturer ......................... 31
Figure 6: Illustration o challenges across the manuacturing value chain .............................. 54
Figure 7: Illustration o oundations required, key interventions and ultimate ambition
or the Business Plan ................................................................................................57
Figure 8: Schematic indicating the interdependence o critical aspects o the system ...........58
Figure 9: Indicative package o solutions to address the wide ranging issues involved ........60
Figure 10: Proposed structure or implementation o the Business Plan .................................. 94

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 13/119
xi
LisT OF TAbLEs
Table 1: Summary o fndings rom WHO report on 26 National Medicines RegulatoryAuthorities in Arica .....................................................................................................38
Table 2: Key challenges identifed by the pharmaceutical sector in achieving universal
GMP standards ............................................................................................................48
Table 3: Status o partnerships impacting on the pharmaceutical sector in Arica .................. 53
Table 4: Indicative list o the broad array o stakeholders in areas related to
pharmaceutical manuacturing in Arica ...................................................................... 92
Table 5: Indicative estimate o resource requirements or ull implementation o the
Business Plan ..............................................................................................................96
Table 6: Potential indicators or national and continent level M & E ..................................... 100

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 14/119
xii

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 15/119
1
EXECuTivE suMMARY
This Business Plan addresses a complex industry and covers a diverse range o contextsacross our 54 member states. Strengthening our ability to produce high quality, aordable
pharmaceuticals across all essential medicines will contribute to improved health outcomes
and the realization o direct and indirect economic benets. This is the vision o the Phar-
maceutical Manuacturing Plan or Arica (PMPA) endorsed by our Heads o State and
Government at the summit in Accra in 2007. This Business Plan outlines a recommended
approach or achieving these aims. It is designed to benet all our member states through
contributing to improved access to aordable, sae and ecacious essential medicines.
In Arica, we bear a disproportionate burden o disease with, or example, 75% o the world’s
HIV/AIDS cases and 90% o the deaths due to malaria. Our people suer more than most
rom tuberculosis and there are many other inectious diseases that cause substantial mor-
bidity and mortality. The extreme impact o inectious diseases is largely elt in sub-Saharan
Arica (SSA) as our countries in the North have disease proles that are more closely re-
lated to those o industrialized countries, with cardiovascular disease, diabetes and cancer
being public health priorities. Non-communicable diseases are also becoming increasingly
prominent across the rest o the continent given the demographic changes that are taking
place and they are predicted to overtake inectious diseases as the leading causes o death
in Arica by 2030.
These orecasts refect the changing liestyles that are associated with economic prosperity,
a uture that is predicted or much o our continent over the coming years. The uture will
also likely see a reduction in the level o donations in support o our healthcare systems as
the global nancial crisis plays out. Thereore, it is imperative that we implement a plan ordeveloping our industry so that we can ensure access to quality aordable medicines inde-
pendent o donations. Furthermore, there is the need to improve the quality o products to
which our people are exposed across the Essential Medicines List (EML) as evidence sug-
gests that there is signicant penetration o sub-standard and countereit products in our
markets.
The 4th Conerence o Arican Ministers o Health directed the Arican Union Commission
(AUC) to develop a Business Plan or the operationalization o the PMPA, a directive that
was urther re-emphasised at the 5th meeting in Namibia in 2011. The AUC duly convened
a stakeholders meeting in Chad to review terms o reerence which have guided the develop-
ment o this Plan. That meeting reconrmed that the objectives o the Business Plan should
be to develop a sustainable supply o aordable, quality essential medicines; to improve
public health outcomes; and to contribute to industrial and economic growth.
This Business Plan is premised on the belie that industrial development o the pharmaceuti-
cal sector will contribute to improved public health outcomes, provided that the development
o the industry is based on the principle that all manuacturers supplying pharmaceuticals to
our people should ultimately meet international standards o production. However, it is also
recognized that we need to be pragmatic and that change cannot happen overnight. In view
o this, we propose a road map approach where the industry is both supported and required
to reach international standards o production over a period o time. Furthermore, the impact
o ‘sub-standard’ production will be mitigated through ensuring that critical products that
would have serious public health consequences should they be o unsatisactory quality areonly manuactured by those o our companies that have reached certain requisite standards.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 16/119
2
Pharmaceutical manufacturing Plan for africa - Business Plan
The context in which pharmaceutical manuacturing takes place is determined by a num-
ber o actors who orm the ‘pharmaceutical manuacturing system’. These entities include
the manuacturers themselves, national medicines regulatory authorities (NMRAs), various
government ministries, trade associations and an array o distribution channels. Other key
players include institutions that develop the human capital or this knowledge intensive sec-
tor.
Moreover, given the capital intensive nature o the pharmaceutical industry, manuacturers
need to access investment. An appetite rom various dierent sources o investment capital
or the sector is essential i companies are to be able to make the signicant investments
required to reach and maintain international standards.
The combined impact o these dierent actors determines the ability and desire o com-
panies to manuacture products to international standards and the degree to which such
manuacturing can be sustainable. The regulator should play a key role in ensuring that
products are manuactured according to Good Manuacturing Practices (GMP). It shouldalso oversee the distribution o products to ensure adherence to Good Distribution Prac-
tices (GDP) and Good Warehousing Practices (GWP), as well as oversee the market place
through pharmaco-vigilance and post marketing surveillance. Various government minis-
tries have policy tools at their disposal that can be used to support the development and
sustainability o the industry sector in a country.
The level o development o the manuacturing system in our countries varies dramatically.
The number o companies that are registered ranges rom over 200 in Nigeria to none in
a number o our countries. In total, it is estimated that some orm o manuacturing takes
place in 38 countries. There is wide divergence in the level o regulatory oversight, with the
Republic o South Arica (RSA) and countries such as Algeria and Tunisia in the Northhaving strong institutions. A World Health Organization (WHO) survey o 26 o our coun-
tries ound that many regulatory authorities lacked the capacity to ull the basic unctions
required or the satisactory protection o public health. Given this limited capacity, it is im-
possible or many o our regulators to oversee the supply o products rom a thousand plus
companies spread across dierent continents. In view o this, the proximity o high quality
production through developing our industries in situ is a means by which our resource-
constrained regulators can establish secure sources o supply.
In other developing countries, such as China and India where there are fourishing phar-
maceutical sectors, the industry is reputed to benet rom a number o policy measures
including protection through tari regimes and procurement preerences as well as direct
support such as interest subsidies, export credits, cheap utilities, working capital credits andtax holidays. Consequently, imports into our continent have oten been subsidized through
signicant support rom their respective governments. Furthermore, they oten enjoy zero
taris when they come into our countries.
Conversely, in some o our nations, domestic manuacturers have to pay up to 25% duty on
imported raw materials. Thereore, whilst a number o Ministries o Health and/or NMRAs
have, or example, identied strengthening the local manuacturing sector as an important
objective, there is oten policy incoherence across government ministries. This creates an
overall environment that is not conducive to the development o our pharmaceutical indus-
tries.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 17/119
3
EXECUTIVE SUMMARY
There is very limited manuacturing o Active Pharmaceutical Ingredients (APIs) in Arica
(limited exceptions being RSA, Egypt and Ghana) and most o our companies are involved
in nal ormulation and packaging o drugs. The quality standards to which our manuac-
turers adhere vary signicantly between countries and within countries. As mentioned, RSA
and most North Arican countries have strong, well developed industries. We have examples
o companies across our continent that have reached or are striving or international stan-
dards. We have others that have the ambition to do so but who have, as yet, not been able to
access the detailed technical know-how or the investment needed to progress towards this
mark. There are other entities that are happy to continue with the current status quo given
that they operate with a relatively low cost base and there is limited political power or capac-
ity or NMRAs to take action against them.
The industry does ace serious challenges i it is to achieve and maintain the standards that
should be required. These challenges include limited access to nance; limited availability o
skilled human resources; inability to access the detailed know-how necessary to implement
an upgrading programme or design a new plant; signicant costs involved in the properdevelopment o new products; the aorementioned policy incoherence; and underdeveloped
supporting industries.
The perspective o individual manuacturers is somewhat dependent on where they stand
in terms o ambition and progress towards improved quality standards. A major actor ham-
pering achievement o the overarching goal o universal high quality production is insu-
cient regulatory oversight. Such oversight is a key actor since lack o it can result in sub-
standard products (both domestically produced and imported) and countereit products
taking market share rom domestic rms genuinely aspiring to high quality production. This
has knock-on eects and it is, or example, one o the issues that investors cite as limiting
their appetite or the sector.
In addition to the challenges aced by the industry, there are underutilized opportunities to
assist and promote the development o pharmaceutical manuacturing on our continent and
or it to contribute to improved public health outcomes. For example, the Trade Related As-
pects o Intellectual Property Rights (TRIPS) fexibilities have generally not been utilized;
there are limited links between industry and academia; and collaboration between compa-
nies in Arica, as well as with international manuacturers, is quite rare. In most countries,
the range o products is limited to a small proportion o those required by a ully unctioning
health system. These underutilized opportunities oer substantial potential benets, includ-
ing expansion o the current range o locally manuactured products.
Given the diverse range o contexts and the array o aspects that need to be addressed to agreater or lesser extent in each country, this Business Plan proposes an approach where a
generic package o solutions is developed. This can then be tailored to the specic needs o
each o our countries. The solutions package includes guidance on incentives in support o
the sector; a Good Manuacturing Practice (GMP) road map and associated risk assessment
o WHO’s Essential Medicines List (EML); a syllabus or developing the human resources
required or the long term sustainability o the industry; various mechanisms or accessing
know-how in the short term, including a Partnership and Business Linkages Platorm (that
would also assist companies to, or example, establish relationships with local, regional and
international players in order to increase product ranges, mobilize investment, etc.); and
includes technical assistance to enable regulators to devise and implement organizational
development plans. It also proposes a process by which the dierent stakeholders in a coun-try can come together to develop a shared strategy or the sector and a means by which this
strategy can be implemented.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 18/119
4
Pharmaceutical manufacturing Plan for africa - Business Plan
Key to the sustainability o manuacturing on the continent is the degree to which our
manuacturers can compete with imports. As pointed out, remedying the policy incoher-
ence will go some way to improving competitiveness and achieving ecient production by
using modern production management techniques has the potential to increase capacity
utilization o plants. Evidence suggests that our companies can compete with, or example,
schedule M compliant manuacturers in India whilst still operating according to interna-
tional GMP. Thereore, another key part o the solutions is assisting companies to embrace
such approaches and constantly look to improve the eciency with which they produce.
As well as the generic solutions package or implementation at country level, we will under-
take activities at the regional and continent wide levels, such as lobbying or an extension to
the TRIPS fexibilities beyond 2016. Also, upon request, we will assist Regional Economic
Communities (RECs) to develop strategies and will work with centres o excellence to de-
velop novel ormulations or dissemination to companies that have reached international
GMP standards. There is also the need or urther deliberation on issues such as traditional
medicines, expanded manuacturing o APIs on the continent, and the need or improvedsupply o blood products. Recommendations on such issues will be developed in the course
o implementing the Business Plan (e.g. WHO is proposing to conduct a easibility study
into blood products in Arica, the ndings o which could be incorporated into the PMPA
in the uture).
This Business Plan puts orward a comprehensive package o solutions or the development
o pharmaceutical manuacturing on our continent. The broad range o disciplines that need
to be covered and the expertise required mean that no one entity can deliver all the neces-
sary aspects and a range o organizations will need to collaborate to ull the ambition. An
important issue to be addressed is the ragmentation o our markets and work under the
Arican Medicines Regulatory Harmonization initiative (AMRH) is well advanced. It willbe critical that the broader work under this Business Plan is coordinated closely with the
AMRH work in order to advance towards the objectives set by the PMPA.
As well as collaboration with AMRH, we propose to establish a consortium o key partners
who will assist us in this undertaking. Initial discussions have taken place with various A-
rican and international bodies that could come together to cover the ull range o interven-
tions required. Under the implementation approach or this Business Plan, a key rst step
will be to establish the legal basis or the consortium and to develop the chemistry between
the dierent actors so that genuine progress can be made. We have invited the United Na-
tions Industrial Development Organization (UNIDO) to assist us in setting up the con-
sortium and to play a coordinating role as we move orward. In addition to establishing
the consortium, we will need to mobilize signicant resources or the implementation o this Business Plan. A detailed budget will be prepared once the consortium has designed a
shared action plan. However, an indicative budget has been prepared and it is estimated that
implementation will cost US$ 54mn over a ve year period.
Other activities during the early stages o implementation will include urther renement o
the generic solutions package and inviting expressions o interest rom member states who
wish to engage with the Arican Union Commission (AUC) or the development o their in-
dustry or o their regulatory systems. This would enable those states to realize public health
gains rom access to regional sources o high quality medicines. During a scale up phase,
agents acting on behal o the PMPA will work with national level stakeholders to develop
strategies to achieve their shared ambitions. Once dened, these ambitions will be translatedinto a detailed action plan based on the expertise within the consortium which will also as-
sist in national level implementation.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 19/119
5
EXECUTIVE SUMMARY
This Business Plan does not represent a source o unding or public or private sector play-
ers but is a package o technical assistance which countries can access. Initial discussions
with the World Bank have suggested that there could be interest in supporting investment
in, or example, National Medicines Regulatory Authorities (NMRAs) although ultimately
it will be the responsibility o individual countries to nance the recommended investments
(whether in terms o bricks and mortar or through support to the industry in the orm o
incentives).
The nature o the manuacturing industry and the complexity o the system within which
it operates mean that it will take time or the ull benets to be realized. There will also be
the need or coordination o many dierent actors at the country level and at the interna-
tional community level. In view o this, a prerequisite or the success o this Business Plan
is the ongoing political will at the highest level to bring parties into alignment and to enable
sustainable progress to be made. Only then will the vision o increasing access to essential
medicines or our people, through a strengthened Arican pharmaceutical industry, become
reality.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 20/119
6
Pharmaceutical manufacturing Plan for africa - Business Plan
sWOT ANALYsis
This Business Plan puts orward a detailed approach to strengthening pharmaceuticalmanuacturing in Arica in order to improve public health outcomes and to contribute to
economic development o our continent. Public health will benet rom improved security
o supply and robust regulatory oversight (easible due to proximity o production) as well
as providing a basis rom which novel ormulations and new products can be developed to
tackle specic diseases and treatment challenges that are to be ound on our continent. As
the global nancial crisis continues to evolve, the development o the sector will provide
a basis or sustainable treatment programmes as the contribution that donors can make
plateaus or even begins to diminish. The sector can also make a contribution to economic
growth through enhanced exports, increased intra-Arican trade, emergence o supportive
industries and the reduced reliance on imports that use up precious hard currency and or
which only limited regulatory oversight by our national regulatory authorities is possible.
The situation across our countries varies dramatically, however general themes apply to a
greater or lesser extent. The ollowing chart summarizes the top line strengths, weaknesses,
opportunities and threats that are pertinent to the sector’s ability to contribute to progress
across public health and economic development dimensions.
Strengths Weaknesses
•Heightenedpoliticalinterest(andwill)tosup -
portthelocalproductionofmedicines.
•Demonstratedthathighqualityproductionof
essentialmedicinesisfeasibleacrossourconti-
nent.•Strengtheningoflegal/regulatoryframework(off
aweakbase).
•Existenceofscienticandtechnicalinstitutions
withtherelevantskillsinanumberofcountries
(asyetunderutilized).
•Increasingpoliticalstabilityandrapideconomic
developmentprovideastrongbasisfordevel-
opmentoftheindustry.
•Developmentsinhealthinsuranceschemesand
healthsystemswithincreasinginvestmentin
publichealth.
•Somecountrieshavewellestablishedpharma-
ceuticalsectorsandregulatoryinstitutionsthat
arerelativelystrong.
•Comparativelylowlabourcosts,especiallyas
Indianlabourcostsbegintoescalate.
•Somecountriesalreadyexportingtoindustrial -
izedmarkets.
•Levelof regulatory oversightvaries but ingen-
eralitisinsufcienttoprotectourcitizensand
toallowfair competition in our pharmaceutical
markets.
•Currentlyheavilydependentonimportswhichoftenbenetfromexportincentivesaswellas
favorable dutiesand tariffs when compared to
domesticallymanufacturedproducts.
•Policy incoherence and absent sector develop-
ment strategiesleadto anenvironmentthatis
notconducivefortheindustrytoourish.
•Highutilitycostsandunreliablesupply.
•Limited availability of affordable nance of suf -
cient magnitude and duration constrains the
sector’sabilitytoinvestinnecessaryupgradesto
achieveestablishedqualitystandards.
•Smalldomesticmarketsandfragmentedregional
marketshampercompanies’abilitytomanufac-
tureefciently.
•Situation varies dramatically, but in for many
companiesthesystems,processes,premisesand
equipmentatplantlevelareinsufcienttoassure
qualityofproduction.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 21/119
7
SWOT ANALYSIS
Strengths Weaknesses
•Limitedsupportingindustriesincludinglocalpro -
duction of inputs such as APIs, packaging and
excipients, as well as availability of services tomaintainandrepairequipmentandtoconduct
necessarytrialstoattesttosuitabilityofproducts.
•WHOprequalicationschemecoversonlyalim-
ited range ofproducts whilst thequalityassur -
anceformostmedicinesisundertheauthority
ofourhighlyresourceconstrainedNMRAs.
Opportunities Threats
•Awareness of importance of local production
amongstinternationalpartnersanddonors,and
growingcommitmenttosupportthisagenda.
•Evidence suggests given a conducive environ-
mentourmanufacturerscancompetewithim-
portsandproducehighqualityproducts.
•Time limitedsupport toindustry coupledwith
requirements(andregulatoryoversight)tode -
velopprovidesviablerouteforbuildinganinter -
nationalstandardindustry.
•Creatingmorefavorablemarketconditionswill
encourageinvestmentinthesector.
•Development of the sector (and requisite na-
tional and regional level legislation) will enable
TRIPSexibilitiestobeutilizedforimprovedac -
cesstokeymedications.
•Increasedprevalenceoflifestylediseasescanbemore comprehensively addressed through en-
hanced local production and they represent a
growingmarketopportunity.
•Training programmes and institutions exist but
needtobeexpandedandscaledup.
•More advanced countries can look to export
drugstointernationalmarkets.
•On-going work under the African Medicines
RegulatoryHarmonizationinitiativecouldleadto
defragmentedmarketsatthesub-regionallevel.
•Stronginterestfrominternationalgenericindus-
tryandthereforethepossibilityforlocalcompa-
niestoformallianceswithinternationalplayers.
•Without a holisticandrobustapproachto de-
veloping the sector efforts from committed
manufacturerswillbeunderminedbyon-going
penetration of sub-standard and counterfeit
medicines.•Anon-goinglack ofevidenceas tothe preva-
lenceandimpactofsubstandardandcounterfeit
medicationscouldunderminethelongtermpo -
liticalwillrequiredtodeveloptheindustry.
•Development of the sector requires coordina-
tionacross publichealth andindustr ialdevelop-
mentcomponentsotherwiseobjectivesonboth
frontswillnotbeachieved.
•WithoutconcertedactionrelianceonAsianim-
portsmayincreaseandqualityofproductsmay
beincreasinglysuspect.
•Ifdonorassistanceplateausapossibleincreaseinsub-standardproductsforthepandemicdiseases
couldjeopardizethehealthofpatientsandlead
toacceleratedresistancegenerationagainstcriti-
calproducts.
•Donorinitiativesthatcaninadvertentlyhavedet-
rimentalconsequencesfortheAfricanpharma-
ceuticalindustry.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 22/119
8
I N D I C A T I V
E A C T I V I T I E S T H A T C O U L D B E C O N D U C T E D D U R I N G T H E I M
P L E ME N T A T I O N O F T H I S B U S I N E S S P L A N
A r e a o f w o
r k
T i m e f r am e ( Y r s . )
K e y a c t i vi t i e s
K e y s u c c e s s f a c t or s
S e t t i n g u p t h e pr o g r a mm e
1
E s t a b l i s h c on s or t i um
R e s o ur c em o b i l i z a t i o
n
I n v i t e c o un t r i e s i n t er
e s t e d i n w or k i n g wi t h
t h eP MP A t o ex pr e s s t h ei r i n t er e s t
G en ui n e c ol l a b or a t i v e s pi r i t b e t w e en c on s or t i um
p a r t i e s
A l l p a r t n e
r s i n v ol v e d i n d e t a i l e d d e s i g n of pr o-
g r a mm e
C r e d i b i l i t y of pr o p o s a l f or d on or s
D e v el o p t h e s ol u t i on s p a c k a g e
1
D e s i g n a g en er i c GM
P r o a d m a p
C on d u c t r i s k a s s e s s m
en t of t h eE s s en t i a l
M e d i c i n e s L i s t
D e v el o p t h eHR d e v
el o pm en t p a c k a g e
C ol l a b or a
t i on b e t w e en p a r t i e s ( p a r t i c ul a r l y i nH
R
d e v el o pm
en t )
A d d r e s s i n
g c om pl ex t e c h ni c a l i s s u e s ( e. g .E ML r i s k
a s s e s s m en t ) i n a pr a g m a t i c b u t s c i en t i c a l l y s o un d
w a y
E s t a b l i s h P M
P A el d r e pr e s en t a t i v e s
1
A p p oi n t r e g i on a l c o or d i n a t or s t o o v er s e e
t h e c o un t r y l e v el d e s i g n a n d i m pl em en t a t i on
of s t r a t e g i e s
S u b j e c t t oi n v i t a t i on s f r omi n d i v i d u a l
m em b er s t a t e s ,r e c r ui t n a t i on a l ex p er t s t o
c o or d i n a t e s t r a t e g y d e s i g n a n d i m pl em en t a -
t i on
G o v er nm en t p ol i t i c a l wi l l
I ni t i a l s e e d f un d i n g f or P MP A m o b i l i z e d
H um a nR e s o ur c eD e v el o pm en t
1 -> 5
D e v el o p t r a i ni n g pr o
g r a mm e s
Of f er t r a i ni n g
−R e g ul a t or y a f f a i r s
−P h a r m a c e u t i c a l b u s i n e s s m a n a g em en t
−P h a r m a c e u t i c a l m a n uf a c t ur i n g
−P l a n t o p er a t i on s &
m a i n t en a n c e
F a c i l i t a t e s h or t t er m
a c c e s s t ok n o wh o w
( e. g . b u s i n e s s p a r t n er s h i p s / c i t i z en s en c o ur -
a g e d t or e t ur nf r om
Di a s p or a )
E a s y a c c e s s t o v i s a s a n d w or k p er mi t s f or ex p a t r i -
a t e s t a f f a n d P MP A t e a m of ex p er t s
C ol l a b or a
t i on wi t h S t r i n g en t R e g ul a t or y A u t h or i -
t i e s ,I C H ,P I C S
I n d u s t r y - a
c a d emi a -r e s e a r c h i n s t i t u t e s i n t er f a c e
&
p a r t n er s h
i p s
O v er a l l c r e d i b i l i t y of c o un t r y c ommi t m en t
s t i m ul a t e s
i n t er e s t f r om p a r t n er s a n d en c o ur a g e s
c i t i z en s t o
r e t ur n
A d v i s e g o v er nm en t s on d e s i g n a n d
i m pl em en t a
t i on of a h ol i s t i c s t r a t e g y
f or b ui l d i n g
s u s t a i n a b l ei n d u s t r y a n d /
or b en e t t i n g f r omr e g i on a l s o ur c e s of
h i g h q u a l i t y
m e d i c i n e s
1 - 3
C on d u c t ex t en s i v e c
on s ul t a t i on s wi t h i n d u s -
t r y a n d a l l r el e v a n t k e y s t a k eh ol d er s
I ni t i a l s t r a t e g y s u b mi t t e d f or c on s i d er a t i on
b y s t a k eh ol d er r o un d t a b l e pr o c e s s
I m pl em en t a t i on u t i l i z i n g t h e ex p er t i s e
wi t h i n t h e c on s or t i um a s d e s c r i b e d i n t h e
“ s ol u t i on s p a c k a g e”
t a i l or e d t o t h e s p e c i c
n a t i on a l c on t ex t
F ul l p a r t i c
i p a t i on b y a l l s t a k eh ol d er s
On g oi n g p ol i t i c a l s u p p or t a n d b u y -i n
C ommi t m
en t b y m em b er s t a t e s t h r o u g h t h e a p-
p oi n t m en t of mi ni s t r y l i a i s on of c er s

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 23/119
9
A r e a o f w o r k
T i m e f r a m e ( Y r s . )
K e y a c t i v i t i e
s
K e
y s u c c e s s f a c t o r s
A s s i s t a n c e w i t h r e g u l a t o r y s y s t e m s
s t r e n g t h e n i n g & b u i l d i n g r e g u l a t o r y
c a
p a c i t y a t c o u n t r y l e v e l
1 - > 5
T A
t o N M R
A s o n o p t i m u m o r g a n i z a t i o n a l
s t r u c t u r e &
d e v e l o p m e n t
S u
p p o r t A M R H w o r k o n r e g u l a t o r y h a r m o -
n i z a t i o n
P o
l i t i c a l s u p p o r t
R
e g u l a t o r a u t o n o m y
R
e g u l a t o r w e l l - r e s o u r c e d
A s s i s t a n c e t o l e a d i n g c o m p a n i e s t o
a c
h i e v e s t r i n g e n t r e g u l a t o r y a p p r o v a l
2 -
3
S u
b j e c t t o c r i t e r i a e s t a b l i s h e d b y t h e T A ,
i d e n t i f y l e a d i n g c o m p a n i e s i n a c h i e v i n g p r e -
q u a l i c a t i o n o f p r o d u c t s
I d e
n t i f y i n d i v i d u a l r e q u i r e m e n t s a n d s e t
u p a p p r o p r
i a t e t e c h n i c a l a s s i s t a n c e p r o -
g r a m m e s
C
o m p a n i e s w i l l n e e d t o t a k e a d v a n t a g e o f t h e a s -
s i s t a n c e ( w h i c h w i l l m a i n l y b e i n k i n d )
S u
s t a i n a b i l i t y o f s u c h c o m p a n i e s w i l l a l s o d e p e n d
o n o t h e r a s p e c t s o f t h e B u s i n e s s P l a n s u c h a s s p e -
c i c g o v e r n m e n t s u p p o r t i n t h e s h o r t
t e r m
F a
c i l i t a t e a n d p r o m o t e a c c e s s t o p r o d -
u c
t s a n d t e c h n o l o g y f o r i n t e r n a t i o n a l
G M P c o m p l i a n t l o c a l m a n u f a c t u r e r s
2 - 5
W
o r k i n g w
i t h c e n t r e s o f e x c e l l e n c e a n d
p a r t n e r s , a c c e l e r a t e r e s e a r c h i n t o n e w
p r o d u c t a n d f o r m u l a t i o n d e v e l o p m e n t ,
s e l e c t p r o d
u c t s f o r d e v e l o p m e n t b a s e d o n
E M L
D
i f f u s e p r o
c e s s & o t h e r t e c h n o l o g y t o l e a d -
i n g c o m p a n
i e s
A
c c e s s t o e x p e r t i s e – A N D I C o E ’ s a n d A m e r i c a n
p a r t n e r s
A
b i l i t y t o g e t V o l u n t a r y L i c e n c e s o r t o
e x p l o i t
T R I P S e x i b i l i t i e s
T e
c h t r a n s f e r t e a m s
F a
c i l i t a t e a c c e s s t o a f f o r d a b l e n a n c e
2 - > 5
T
h r o u g h t h
e P a r t n e r s h i p a n d B u s i n e s s
L i n k a g e s P l a t f o r m a d v o c a t e f o r D F I s s u c h a s
t h e A f r i c a n
D e v e l o p m e n t B a n k & A f r i c a n
E x p o r t - I m p
o r t B a n k ( A f r i E x i m ) t o i n v e s t i n
t h e p h a r m a
s e c t o r
A
s p a r t o f h o l i s t i c a p p r o a c h , a
d v i s e g o v e r n -
m e n t s o n a
p p r o p r i a t e i n i t i a t i v e s t o a t t r a c t
i n v e s t m e n t
i n t o t h e s e c t o r
P o
l i t i c a l l e a d e r s h i p
P a
r t n e r s h i p s w i t h n a n c i a l e x p e r t s
G
o v e r n m e n t c r e a t e s a c o n d u c i v e e n v i r o n m e n t f o r
i n v e s t m e n t
A t t a i n i n g i n t e r n a t i o n a l q u a l i t y s t a n d a r d s
1 - > 5
A
s p a r t o f c o u n t r y l e v e l i m p l e m e n t a t i o n o f
h o l i s t i c s t r a t e g y , a s s i s t r e g u l a t o r s t o t a i l o r
a n d e x e c u t e a G M P R o a d M a p t o g u i d e t h e
m i g r a t i o n t o i n t e r n a t i o n a l G M P s t a n d a r d s
I n
c e n t i v e s a n d n a n c i n g a v a i l a b l e f o r i n
d u s t r y t o
u p g r a d e
R
e g u l a t o r h a s p o l i t i c a l a u t h o r i t y a n d c a p a c i t y t o
e n f o r c e r e q u i r e m e n t s
F a
c i l i t a t e p a r t n e r s h i p s , c o l l a b o r a t i o n a n d
b u
s i n e s s l i n k a g e s
1 - > 5
E s
t a b l i s h p l a t f o r m s f o r f a c i l i t a t i n g m a t c h -
m a k i n g
M
o n i t o r d e
a l o w a n d a d v i s e g o v e r n m e n t s
o n k e y c o n s i d e r a t i o n s f o r F D I
M
u t u a l l y b e n e c i a l r e l a t i o n s h i p s c a n b e e s t a b l i s h e d
P l a
t f o r m d e s i g n e d t o a l l o w f o r w i d e v a r i e t y o f r e l a -
t i o n s h i p s b e t w e e n a s s o r t e d t y p e s o f s t a k e h o l d e r

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 24/119
10
A r e a o f w o
r k
T i m e f r am e ( Y r s . )
K e y a c t i vi t i e s
K e y s u c c e s s f a c t or s
E nh a n c i n g m a r k e t d a t a c ol l e c t i on
1 - 5
A p pr o a c h I M S I n s t i t u
t e t o p a r t n er a n d of f er
t r a i ni n g onm a r k e t d a t a c ol l e c t i on t o ol s
I m pl em en t t r a i ni n g
Wi l l i n g n e s s t o s h a r e d a t a b y a l l s t a k eh ol d er s
I M S s e e s p o t en t i a l g a i nf r om t h e p a r t n er s h i p
F a c i l i t a t i n g m a r k e t a c c e s s & pr om o t i n g
i n t r a -r e g i on
a l t r a d e
2 -> 5
S u p p or t a s r e q ui r e d
t oA MR Hi nm o v i n g
t o w a r d s r e g ul a t or y h
a r m oni z a t i on
P ol i t i c a l w
i l l
H a r m oni z
er e g i s t r a t i onr e q ui r em en t s
P r o v i d i n g a s s i s t a n c e t o ex pl oi t T R I P S
F l exi b i l i t i e s
1 -> 5
A p pr o a c h A R I P O , UNDP , UN C T A Dr e
of f er i n g T A a n d s u p p
or t f or a m en d i n g I P R
l e g i s l a t i on t oi n c or p o
r a t eT R I P S exi b i l i t i e s
L o b b y f or ex t en s i on
of T R I P S d e a d l i n e of
0 7 / 0 1 / 1 6
A p pr o a c h R E C ’ s onh a r m oni z a t i on of I P R
P ol i t i c a l w
i l l
Wi l l i n g n e s s t o a m en d n a t i on a l l e g i s l a t i on t oi n c or -
p or a t e t h eT R I P S exi b i l i t i e s
C om p a ni e s s h o wi n t er e s t i n ex pl oi t i n g T R I P S
P r om o t i n g a n d c a t a l y z i n g A P I P r o d u c -
t i on
1 -> 5
I d en t i f y pr o d u c t s f or
l o c a l pr o d u c t i on
M o b i l i z ef un d i n g a n d
en t i c e en t r e pr en e ur s
t oi n v e s t i nA P I pr o d
u c t i on
C a n v a s s u p p or t f or l o c a l A P I pr o d u c er f r om
l o c a l f or m ul a t or s
F un d i n g
P r o d u c t i o
n of c om p e t i t i v eA P I ( pr i c e a n d q u a l i t y )
P r o v i d i n g a s s i s t a n c e t o a c c el er a t er e-
s e a r c h a n d
d e v el o pm en t i n t o t r a d i t i on a l
m e d i c i n e s
1 -> 5
I d en t i f y p a r t n er s a l r e
a d y en g a g e d i n t h e a r e a
a n d of f er s u p p or t
W or k i n g wi t h i d en t i e d p a r t n er s , c o d i f y
t h ek n o wl e d g e b a s e
a n d c r e a t e a l i b r a r y of
pl a n t s wi t h m e d i c i n a l pr o p er t i e s
F un d i n g
R e s e a r c h
ex p er t i s e a n d c ol l a b or a t i on s
P a r t n er s h
i p s wi t h t r a d i t i on a l h e a l er s
E s c or t i n g t h ef or m a t i on a n d s t r en g t h en-
i n g of ph a r m a c e u t i c a l t r a d e a s s o c i a t i on s
1 -> 5
F a c i l i t a t ef or m a t i on o
f n a t i on a l a n d r e g i on a l
t r a d e a s s o c i a t i on s
C on s ul t wi t h i n d u s t r y s t a k eh ol d er s
E x t en s i v e
c on s ul t a t i on s wi t h i n d u s t r y a n d r el e v a
n t
s t a k eh ol d er s
I n d u s t r y w
i l l i n g n e s s t o p a r t i c i p a t e
G o v er nm en t a n d R E C l e v el s u p p or t
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 25/119
11
INTRODUCTION AND BACKGROUND
1. iNTRODuCTiON AND bACKGROuND
This Business Plan addresses a complex industry and covers a diverse range o contexts.Our continent is comprised o 54 countries, and has a total population o just over 1 billion
people which equates to about 14% o the global population. With the exception o Mo-
rocco, all these independent nations are members o the Arican Union (AU). They are also
organized into various sub-groupings, including Regional Economic Communities (RECs)
and trading blocs, with overlap and membership o multiple RECs and trading blocs be-
ing commonplace. The picture below is a schematic representation o the complexity o the
multiple memberships o various Arican states and o how we are situated in the dierent
regional economic and trading blocs.
1: S ps vp recs d d bs
UMA
African Union
WAMZ
LGAUEMOA
COMESA
MRU
EAC
SADC
SACU
CEPGL
CEMAC
Compounding the complexity o the RECs and trading blocs, there are substantial varia-
tions in disease proles and pharmaceutical-sector specic issues in North and sub-SaharanArica (SSA). The SSA region suers rom a high inectious disease burden whilst the North
has a prole not dissimilar to that o the developed world, with cancer, diabetes and car-
diovascular disease being leading public health priorities. The industry in the North is also
generally more developed than in the SSA region.
As well as signicant dierences between northern and southern Arica, the status o the
pharmaceutical industry varies signicantly within SSA. For example, the Republic o South
Arica (RSA) has a highly developed industry with some level o primary manuacturing.
Other member states have emerging industry sectors with companies at dierent stages o
development whilst others have a handul o manuacturers. Some states have no local phar-
maceutical manuacturing at all.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 26/119
12
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
The level o regulatory oversight o medicines varies dramatically across our continent.
A ew member states have strong regulatory authorities; others have institutions in place
which, to a greater or lesser extent, ull the unctions necessary to oversee the pharma-
ceutical markets; and some have virtually nonexistent regulatory systems. This multiplicity
o regulatory environments and widely varying capacities make regulatory harmonization
on the continent a massive challenge and continue to hamper access to aordable quality
essential medicines. It is against this background that the Arican Heads o State and Gov-
ernment adopted the Pharmaceutical Manuacturing Plan or Arica (PMPA) in May 2007.
The PMPA was adopted with the explicit aim o contributing to a sustainable supply o
quality essential medicines to improve public health and promote industrial and economic
development on the continent1. Broadly speaking then, the objective is to improve the qual-
ity o medicines even in countries that are neither involved in nor contemplating local phar-
maceutical production. The Arican Union Commission (AUC) is o the view that, even in
such countries, the PMPA will be o benet in contributing to access and security o sup-
plies o regionally produced high quality medicines. Such high quality regional sources willallow or a speedier response to country needs. Moreover, the proximity o producing coun-
tries will enable closer oversight o the quality o products compared with oversight o those
derived rom numerous plants across dierent continents. The quality o products available
in such countries will also benet rom strengthened supply chains and the development o
post marketing surveillance competencies.
1.1 the Strategic conteXt o arica’S healthcarechallengeS
Arican healthcare systems ace severe challenges which negatively impact on access to a-
ordable quality healthcare and lead to morbidity and mortality rom eminently treatable
conditions. The challenges are complex and, amongst others, include a disproportionately
high inectious disease burden, a growing chronic disease burden, a shortage o the requisite
human resources and the necessary inrastructure to deliver healthcare services, as well as
signicant unding and budgetary constraints.
1.1.1 High infectious disease burden
The International Finance Corporation (IFC)2 estimates that Arica accounts or:
• 25% o the global disease burden
• More than 50% o the global deaths o children under ve
• 3% o the world’s healthcare workers deployed
• Consumes only 1% o global healthcare expenditure
Specically, Arica accounts or the bulk o the global inectious disease burden with about
75% o the HIV/AIDS pandemic, 90% o the malaria cases and deaths. In addition, nine
Arican countries (excluding North Arica) rank among the 15 countries with the highest
1 Pharmaceutical Manuacturing Plan or Arica – CAHM_MIN._8(111) 20072 IFC – The Business o Healthcare in Arica 2007

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 27/119
13
INTRODUCTION AND BACKGROUND
tuberculosis (TB) burden in the world. The incidence o multidrug-resistant tuberculosis
(MDR-TB) and extensively drug-resistant tuberculosis (XDR-TB) in Arica is one o the
highest in the world.3
Furthermore, according to the World Health Organization (WHO), 90% o child deaths
in Arica are attributable to neonatal causes, pneumonia, diarrhoea, measles and HIV and
AIDS4 whilst the major causes o adult mortality are also related to HIV/AIDS, TB and
Malaria.
1.1.2 Growing chronic and non communicable disease burden
In addition to the pandemics and other uniquely Arican inectious diseases, the continent
aces a signicant and growing non communicable disease burden. These diseases are major
public health issues in the North already and are projected to increase dramatically in SSA
due to improving social conditions and rapid urbanisation; environmental issues like air
pollution; and an increase in the consumption o alcohol and tobacco products. The rise inchronic diseases will also be exacerbated by sedentary liestyles. It is estimated that by the
year 2020 Arica could have5:
• 60 million people with hypertension
• 1 million cases o cancer annually
• 18.6 million people with diabetes
Along with the specic conditions mentioned above, there will be an explosion o other
cardiovascular conditions, chronic respiratory diseases and neuro-psychiatric conditions.
For example, predictions are that by 2030 non-communicable diseases will have surpassedinectious diseases as the leading cause o death in Arica6.
1.1.3 The changing economic context and pharmaceutical industry growth
As well as the changing epidemiology o diseases and demographic changes, the Business
Plan will be implemented over a period o time when Arica is expected to undergo substan-
tial economic development. Various commentators have predicted that the continent will
experience substantial growth and economic development. For example, the World Bank in
November 20107 envisioned Arica’s prospects thus:
‘’We conclude that Arica could be on the brink o an economic takeo, much like China was 30
years ago, and India 20 years ago.”
The McKinsey Global Institute also made the ollowing observation:
“Arica’s growth acceleration resulted rom more than a resource boom. Arguably more important
were government actions to end political conficts, improve macro-economic conditions, and create
better business climates, which enabled growth to accelerate broadly across countries and sectors” 8 .
3 WHO Global Tuberculosis Report 20114 WHO Global Tuberculosis Report 20115 WHO & DFID (UK)6 Colin D Mathers & Dejan Loncar. Projections o Global Mortality and Burden o Disease rom 2002-2030. PloS
Medicine Nov 2006, Vol. 3, Issue 117
The World Bank; Arica’s uture and the World Bank’s role in it - http://siteresources.worldbank.org/INTAFRICA/Re-sources/Arica_s_Future_and_the_World_Bank_s_Role_in_it.pd
8 McKinsey Global Institute – Lions on the Move: The progress and potential o Arican economies. June 2010

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 28/119
14
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Thereore, the industry, like that o other emerging markets, is expected to grow tremen-
dously in the coming years. The expected growth will largely be driven by economic and
medical actors as presented in Figure 2 below. This Business Plan articulates an approach
or the PMPA that is designed to catalyse the development o the industry, shorten the time
needed or the progressive realization o international quality standards and lead to an in-
crease in product portolios to address the needs o the continent.
2: a P gw Dvs9 10,
The growth of the pandemics and
increasing numbers of people on
treatment
An improving health insurance
and coverage environment, and a
consequent increase in the
number of people with access to
healthcare
An ageing population leading to
increased prevalence of geriatric
disorders
An increase in lifestyle diseases
associated with growing
economic prosperity and
urbanization
Pharma
industry
growth
1.3 billion population by 2020
A combined GDP of 2.9 trillion
USD
Healthcare expenditure of around 200 billion USD
A pharmaceutical market
valued at an estimated 23
billion USD,
50 percent of households will
have a disposable income of
more than 20 USD per day;
Investments in healthcare
reforms
The patent expiries of many
leading medicines
Economic factors Medical factors
1.1.4 Shortage of the requisite human resources and infrastructure
The delivery o healthcare requires more than just medicines. There are widespread reports
o understaed health centres and acilities are oten not situated where they are most need-
ed. When they are present, they oten lack the essential medicines that are needed. It is ur-
ther estimated that more than a third o the available highly skilled Arican scientists are now
living in the developed world11. A recent survey on the nancial cost o doctors emigrating
rom sub-Saharan Arica revealed that a large number o doctors in sub-Saharan countries
were, in act, working in the United Kingdom, Australia, Canada and the United States.
The actual numbers are estimated by various parties to be in the thousands and accountor an estimated loss o return on investment or the nine countries o almost US$2.17bn
whilst the net gain or the developed countries to which they emigrated was estimated at
US$4.55bn12.
This points to the act that the training capability and talent in the basic and advanced sci-
ences is there. However, a key problem or the continent is the high attrition rate and the
brain drain although we also need to increase the output o skilled scientists. It also means
that there is a large pool o people who can be tapped to support the continent’s objectives
and that, as in the case o India and China, it may be possible to repatriate skills rom the Di-9 Arica Progress Report 2010.10McKinsey Global Institute – Lions on the Move: The progress and potential o Arican economies. June 2010.
11Joint Statement by the Network o Arican Science Academies July 2009 - www.nationalacademies.org/includes/NA-SACbraindrain09.pd (accessed December 2011.)
12Edward J. Mills et al. The nancial cost o doctors emigrating rom sub-Saharan Arica: human capital analysis. Brit-
ish Medical Journal publication. BMJ 2011;343:d7031 doi: 10.1136/bmj.d7031 (published 24 November 2011.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 29/119
15
IntroductIon and Background
aspora when the environment in Arica becomes conducive to the expression o such skills.
1.1.5 Inadequate distribution infrastructure
The lack o proper inrastructure also contributes to poor health outcomes. For example,
there is anecdotal evidence that due to the distribution diculties caused by insucient
inrastructure in some countries, a percentage o donated drugs expire on shelves in govern-
ment central medical stores without ever reaching the areas o greatest need in rural clinics
and hospitals. Conversely, there is a body o evidence that suggests that locally manuactured
products are more readily available in the remote rural parts than imported products13, 14.
This is an important development and speaks to the potential impact o assisting the devel-
opment o local industry.
1.1.6 Chronic healthcare underfunding
Arican healthcare systems have historically been severely underunded. Despite the Abuja
Declaration in which Arican Heads o State and Government committed to spending 15%
o GDP on healthcare, very ew countries have done so and many still grapple with chronic
underunding and very limited healthcare budgets. Inevitably, this unding gap compromises
care since the delivery o healthcare in Arica is largely dependent on public sector unding
albeit that a ew markets have airly developed private sector healthcare delivery platorms.
Even in instances where the public sector is the primary method o health delivery, various
sources estimate that out o pocket spending, especially or medicines, is as high as 60% as a
result o requent medicine shortages at public institutions. As a consequence o the unding
gap, many donors have come orward and today a large proportion o the health budgets and
treatment programmes on the continent are nanced or subsidized by international donors.
The over reliance on donor unding, especially or the pandemic conditions, is laden with di-
culties especially in the current setting o reducing donor commitments and increasing treat-
ment gaps. O necessity, this calls into question the sustainability o treatment programmes
and healthcare delivery. The Economist Intelligence Unit (EIU) makes this observation:
“By 2022 continued global economic instability will lead to cuts in oreign aid budgets and leave
many donor organisations overstretched, with the result that many o them are orced to pull out o
Arican countries. The migration o skilled medical personnel to developed countries is likely to ac-
celerate. The initial consequences o such a development could be empowering or many countries, as
well as catastrophic or a smaller number. Countries with greater resources will use the opportunity
or emancipation rom charity to build up their own local manuacturing capability or basic drugs
and medical equipment. In the medium term, booming economies in these more ortunate countries
will attract international companies rom high-growth markets to develop generic drugs locally, to
train local medical sta, to oer new insurance products and to set up research and development
centres on the continent” 15 .
This view is supportive o similar sentiments raised by various other sources that have spo-
ken o the need or Arica to begin planning and preparing or health provision post the aid
boom. Attention is drawn to the urgent need to develop local pharmaceutical production ca-
13 Mackintosh M, Mujinja P.GM. Pricing and competition in essential medicines markets: the supply chain to Tanzania
and the role o NGOs - IKD Working Paper No. 32 July 2008.14Mackintosh M. Essential Medicines, supply chain and inequalities - DIME / FINNOV / IKD Workshop
INNOVATION AND INEQUALITY: The Need or New Indicators rom Pharma and Beyond: Sant’Anna School o Advanced Studies, Pisa, Italy 15 - 16 May 2010. May 2010.
15 The Economist Intelligence Unit - The Future o Healthcare in Arica 2011.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 30/119
16
Pharmaceutical manufacturing Plan for africa - Business Plan
pacity to help ease the problem o access in the long term. For example, UNAIDS published
an Issue Brie in January 2012 in which it identied local production o HIV treatments as
being critical or the long term sustainability o the HIV/AIDS response16.
1.1.7 Limited access to essential medicines
Compounding the disease burden and the shortage o human resources or health is the act
that many people still do not have access to the essential medicines they need. This is a result
o a multitude o actors, including the lack o local production capacity, weak institutional
capacity and poorly regulated supply chain systems that enable sub-standard products (lo-
cally produced and imports) to reach patients, and the emerging scourge o Arica’s insidi-
ous public health crisis - countereit drugs. As a consequence, access to essential medicines
in Arica has been hampered because products are not available, not aordable, or ineec-
tive, amongst other reasons.
For example, the availability o medicines at the retail pharmacy level in most Organisationor Economic Co-operation and Development (OECD) countries is over 90%. In Arica, it
is estimated that the availability o essential medicines (excluding North Arica) is way be-
low 40% in the public sector, which caters or the bulk o the population, and less than 60%
in private sector medicines outlets17. The end result is poor access to essential medicines
with the resultant poor health outcomes. Notwithstanding the act that there has been con-
siderable progress – especially in the treatment o HIV/AIDS, TB and malaria - anecdotal
evidence rom across the continent suggests that the observation made in 2001 in a WHO/
World Trade Organization (WTO) brieng paper, as captured below, still holds:
“In Arica and South East Asia, prompt diagnosis and treatment could save an estimated our mil-
lion lives each year. Two-thirds o all deaths o children under 15 are due to seven diseases or whicheective prevention and treatment exist. Put simply, people are dying because the drugs they need
are not available to them. The opportunities or rapid health gain through better access to health
technology are immense” 18 .
It is a matter o concern that, even when medicines are available, their quality is suspect due
to the weak nature o regulation and widespread non compliance with international Good
Manuacturing Practice (GMP) and other critical components o the quality system. There
have been a limited number o surveys on the quality o drugs in Arica with most ocusing
on products or the high prole pandemic diseases such as tuberculosis and malaria19, 20. De-
spite the lack o inormation across the much broader range o drugs required or a unction-
ing health system, there is already a critical mass o evidence to suggest that the impact o
sub-standard drugs is grave. For example, a recent WHO study21 looking at product quality
o anti-malarial products in selected Arican countries ound that 39% o products tested
in Ghana were sub-standard and the proportion was as high as 64% o products tested in
Nigeria (the samples taken included imported as well as locally produced drugs).
16 AIDS Dependency Crisis, Sourcing Arican Solutions – UNAIDS publication. January 201217 Rockeeller Foundation, Dalberg and MIT Zaragoza; 2008. Private sector role in health supply chains. Report avail-
able online at http://www.dalberg.com/html/PDFs/Health_Supply_Chains.pd (accessed October 2011)18 WHO Secretariat. 2001. More Equitable Pricing or Essential Drugs. Background paper or the WHO-WTO Secre-
tariat workshop on dierential pricing and nancing o essential drugs.19 A summary o the major prevalence surveys or sub-standard drugs can be ound in J. M. Caudron et al’s paper –
Substandard medicines in resource-poor settings: a problem that can no longer be ignored. Tropical Medicine and
International Health Volume 13 No. 8, pp 1062-1072, August 2008.20 A non-exhaustive list o publications on poor quality medicines can be ound on QUAMED’s website: http://www.
quamed.org/en/news-articles/quamed-actsheet-on-access-and-quality.aspx21Survey o the Quality o Selected Antimalarial Medicines circulating in Six Countries in Sub-Saharan Arica. WHO,
January 2011
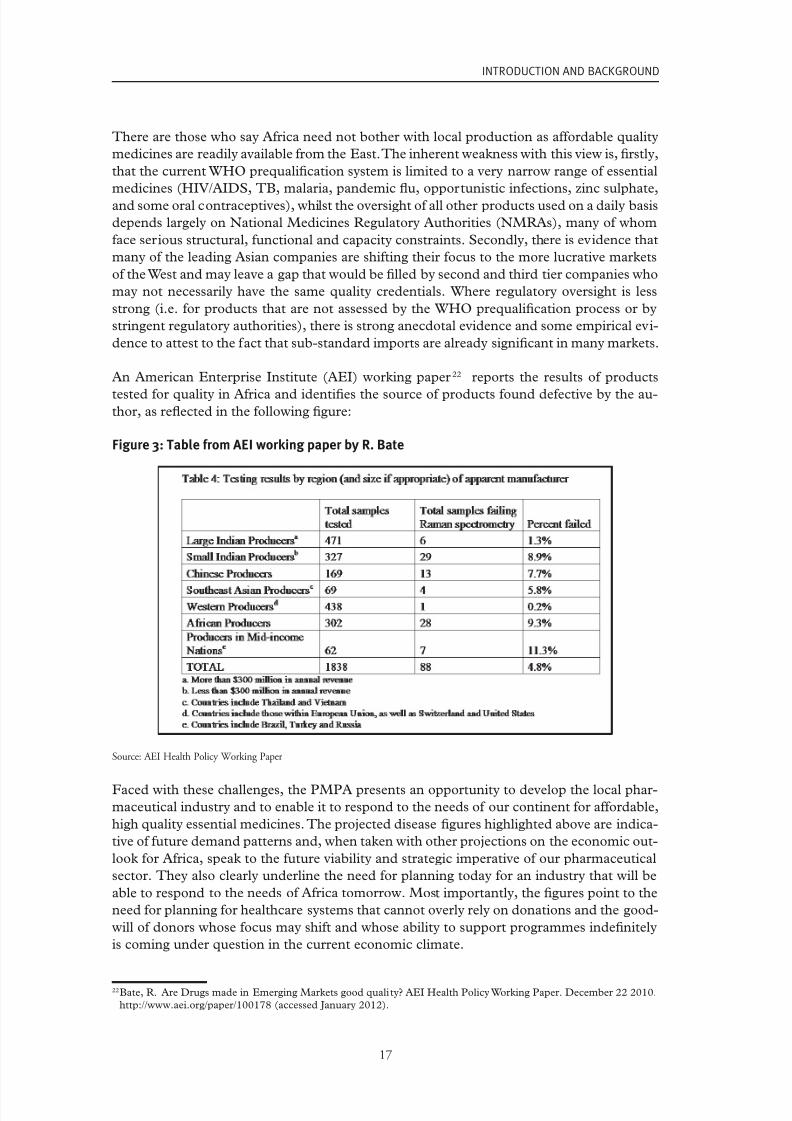
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 31/119
17
INTRODUCTION AND BACKGROUND
There are those who say Arica need not bother with local production as aordable quality
medicines are readily available rom the East. The inherent weakness with this view is, rstly,
that the current WHO prequalication system is limited to a very narrow range o essential
medicines (HIV/AIDS, TB, malaria, pandemic fu, opportunistic inections, zinc sulphate,
and some oral contraceptives), whilst the oversight o all other products used on a daily basis
depends largely on National Medicines Regulatory Authorities (NMRAs), many o whom
ace serious structural, unctional and capacity constraints. Secondly, there is evidence that
many o the leading Asian companies are shiting their ocus to the more lucrative markets
o the West and may leave a gap that would be lled by second and third tier companies who
may not necessarily have the same quality credentials. Where regulatory oversight is less
strong (i.e. or products that are not assessed by the WHO prequalication process or by
stringent regulatory authorities), there is strong anecdotal evidence and some empirical evi-
dence to attest to the act that sub-standard imports are already signicant in many markets.
An American Enterprise Institute (AEI) working paper22 reports the results o products
tested or quality in Arica and identies the source o products ound deective by the au-thor, as refected in the ollowing gure:
3: tb aei wk pp by r. B
Source: AEI Health Policy Working Paper
Faced with these challenges, the PMPA presents an opportunity to develop the local phar-
maceutical industry and to enable it to respond to the needs o our continent or aordable,
high quality essential medicines. The projected disease gures highlighted above are indica-
tive o uture demand patterns and, when taken with other projections on the economic out-
look or Arica, speak to the uture viability and strategic imperative o our pharmaceutical
sector. They also clearly underline the need or planning today or an industry that will be
able to respond to the needs o Arica tomorrow. Most importantly, the gures point to the
need or planning or healthcare systems that cannot overly rely on donations and the good-
will o donors whose ocus may shit and whose ability to support programmes indenitely
is coming under question in the current economic climate.
22Bate, R. Are Drugs made in Emerging Markets good quality? AEI Health Policy Working Paper. December 22 2010.
http://www.aei.org/paper/100178 (accessed January 2012).
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 32/119
18
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
1.2 the Pharmaceutical manuacturing Plan or arica
In recognition o the enormous challenges acing healthcare systems, including lack o ac-
cess to essential medicines, and the reliance on others or solutions, our Heads o Statedirected the Arican Union Commission to develop a pharmaceutical manuacturing plan
or the continent. The PMPA was duly developed and adopted by the Conerence o Arican
Ministers o Health held in Johannesburg, South Arica in April 2007 and endorsed by the
Heads o State and Government in Accra, Ghana in July 2007.
The PMPA is premised on the inalienable principle that access to quality healthcare, in-
cluding access to all essential medicines that are aordable, sae, ecacious, and o good
quality, is a undamental human right. The PMPA proposes that the promotion o industrial
development and the saeguarding and protection o public health are not mutually exclu-
sive priorities and that the production o quality medicines and the development o an in-
ternational GMP compliant industry in Arica are possible, desirable and eminently doable.
This Business Plan is based on the belie that industrial development and the development
o the pharmaceutical sector is not in confict with public health imperatives and that the
industry should in act be developed with the long term aim o promoting access to quality
essential medicines.
The core objective o the PMPA is to support local pharmaceutical manuacturing in order
to contribute to the ollowing outcomes:
• Increased access to aordable quality medicines
• Sustainable supply o essential medicines
and it should have the ollowing impact:
• Improved public health outcomes
• Industrial and economic development
This vision, as articulated in the inception report adopted by the AUC PMPA Technical
Committee in December 2011, is to develop a competitive and enduring integrated phar-
maceutical manuacturing industry in Arica able to respond to the continent’s need or a
secure and reliable supply o quality, aordable, accessible, sae and ecacious medicines.
The vision calls or the planning o today to be inormed by the Arica o the uture; an Aricathat is on a high-speed train to prosperity and that will be able to aord to pay or medicines
needed by its peoples. It also recognizes the ongoing human tragedy on our continent regard-
ing the limitations in access to medicines and seeks to help address this situation through the
development o the pharmaceutical industry. It is a vision that demands courage, oresight
and the willingness to take tough decisions now in order to deal with the myriad o challenges
that the pharmaceutical manuacturing system currently aces. Such initiatives will enable the
industry to make the contribution to improved public health on the continent o which it is ca-
pable and will contribute to Arica truly becoming sel sucient in the provision o healthcare.
This is a plan that oresees the entry o Arica into new drug discovery and the development
and commercialisation o Arican developed and researched blockbuster drugs. It also recog-
nizes the critical need or governments to play a catalytic role in order to kick-start the growth
o the industry and to put a brake on overreliance on imports.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 33/119
19
INTRODUCTION AND BACKGROUND
This vision leads to a path that calls orth Aricans in the Diaspora to come back home and
invites people o goodwill and unders o research to invest in Arican research and devel-
opment work. It requires that governments give the upstream support needed to grow the
industry and to assist it to realize its ull potential. The vision calls or a path that leads to
success, sustainability and sel-suciency in the provision o aordable quality medicines.
The key actors that will enable our pharmaceutical industry to be successul in delivering
on this vision include:
• Strong independent and predictable regulatory systems
• Availability o the requisite human skills and access to know-how in the short term
• Increased competition leading to continuous product improvements, increased pro-
duction and distribution eciencies, enhanced sales and marketing eorts and ser-
vice and business model innovation
• Reduced demand uncertainty and accurate orecasting
• Enhanced regulatory oversight
• Investment and access to aordable nance
• Provision o time-limited, easily understood, and accessible incentives
Finally, the success o the PMPA vision will depend on a recognition that, whilst this is the
overarching continental sector strategy document and road map, there are multiple ongoing
eorts on the ground and that some Regional Economic Communities and countries havealready developed and are implementing strategies and plans or developing the industry in
their regions. The package o solutions proposed here is not intended to supplant or take
precedence over the work already being done but will be deployed, as requested, to augment
and plug into regional and country specic initiatives. Where there are no sector strategies
in place, the AUC and our partners, subject to invitation, will look to assist in developing
and implementing them.
Similarly, it is recognized that there are a host o development partners, Non Governmental
Organizations (NGOs), Arican centres o excellence and others already engaged in various
activities including regulatory harmonization, skills development, technology transer and
so orth. The AUC believes that in implementing this Business Plan, the coordination and
integration o these various initiatives will be critical.
1.3 BuSineSS Plan
The 4th Conerence o Arican Ministers o Health directed the AUC to develop a Business
Plan or the ‘operationalization’ o the PMPA, a directive which was urther emphasized by
the 5th Conerence held in Namibia in 2011. The Arican Union Commission convened a
stakeholder workshop in N’Djamena, Chad, to review the Terms o Reerence (ToR) which
should guide the development o the Business Plan or ‘operationalizing’ the PMPA.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 34/119
20
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
The Chad workshop reconrmed that the overall objective o the PMPA is to support local
pharmaceutical manuacturing in order to contribute to:
• A sustainable supply o aordable quality essential medicines
• Improved public health outcomes
• Industrial and economic development
Although there is recognition o the importance o this Business Plan to achieving the stated
objectives o the PMPA, the AUC acknowledges that it is not a panacea that will solve all
challenges and that its impact will ultimately also depend on other initiatives, including the
strengthening o health systems, developing human resources or health, and upgrading the
distribution inrastructure in order to be able to eectively deliver drugs to all points o care.
1.3.1 Partnerships
Given the need to coordinate and integrate work on the PMPA, the AUC invited UNIDO
to partner it in developing this Business Plan and to assist in the planning, organisation and
coordination o the Plan’s implementation. However, the Commission is acutely aware that
there is no single organisation with the breadth o expertise to deliver on the Business Plan
on its own. The AUC will thereore need the support and collaboration o various partners
in this endeavour. Initial discussions are ongoing with potential core partners including
the World Health Organization (WHO), the United Nations Joint Programme on HIV/
AIDS (UNAIDS), the U.S. Pharmacopeial Convention (USP), the Arican Network or
Drugs and Diagnostics Innovation (ANDI) and some o its centres o excellence, Saint Luke
Foundation / Kilimanjaro School o Pharmacy and various academic entities (in Arica and
beyond).
One component o the overall PMPA is the work being conducted by the New Partnership
or Arica’s Development (NEPAD), the World Bank, WHO and the Bill and Melinda Gates
Foundation on registration harmonization through the Arican Medicines Regulatory Har-
monization (AMRH) initiative. This work is well advanced with, or example, the launch o
the regional strategy or the East Arican Community (EAC) which took place in March
2012.
Deragmentation o our markets through harmonization o registration requirements and
urther progress toward regulatory harmonization is vital or the long term sustainability o
local production. With this in mind, the broader requirements or strengthening local pro-duction on our continent, as outlined in this Business Plan, will be closely coordinated with
the ongoing work under the AMRH initiative.
The AUC recognizes the critical importance o political commitment and leadership at the
highest levels and the need or inclusivity and proper coordination as prerequisites or suc-
cess. We will thereore seek to align and integrate the eorts o all key partners behind the
PMPA vision and the Business Plan since history suggests that ‘isolated’ and/or vertical pro-
grammes do not have the sustainable and substantive impact that can be achieved through
cooperation. The nature o the pharmaceutical industry is such that manuacturers’ viability
is dependent on, amongst others, a product portolio that cuts across a range o therapeutic

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 35/119
21
INTRODUCTION AND BACKGROUND
categories. Moreover, the sustainability o aordable high quality local production is depen-
dent on coordinated change across the whole pharmaceutical manuacturing system.
The PMPA is a vehicle through which the AUC will mobilize the requisite resources and
behind which various partners will align to provide technical support and insights in order
to assist those member states who aspire to high quality sustainable local production. For
those countries that do not have the ambition or capacity or developing their pharmaceuti-
cal industry, the PMPA will work on other initiatives to help strengthen quality and market
surveillance systems. This approach will improve access to medicines in those countries that
could source high quality, quality assured products rom manuacturing hubs in the region.
It is envisaged that, in order to realize the ultimate vision o the PMPA, concerted action
will be required over an extended timerame (15+ years). Nonetheless, signicant progress
is still possible over the next ve years. This Business Plan is weighted towards the near to
medium term, keeping the long term objectives as the target, and it represents an approach
or the rst ve year phase starting in 2013.
1.3.2 Methodology and Structure
The purpose o this Business Plan is to present the proposed approach or the operational-
ization o the PMPA. It outlines a number o interventions or a ‘package o solutions’ to ad-
dress the various challenges aced by stakeholders associated with the industry i they are to
contribute to the development o a sustainable pharmaceutical sector capable o responding
to our continent’s need or aordable essential medicines o good quality.
The proposed package o solutions is based on the ndings o extensive desk research and
consultations with stakeholders in various member states and with international experts. Italso refects consultations with various institutions engaged in one way or another with the
pharmaceutical industry. Fact nding missions were undertaken to various member states
in all parts o the continent. These visits incorporated consultations with a broad array
o stakeholders, including national medicine regulators; ocials rom ministries o trade,
industry, and health; government ocials responsible or pharmaceutical policy and plan-
ning and industrial strategy; procurement ocials and government central medical stores
or tender boards; investment promotion agencies; pharmaceutical trade associations; and
individual manuacturers.
The solutions are also inormed by UNIDO insights acquired through activities carried
out, including advisory services on policy and sector strategy development in countries like
Ghana and Kenya; institutional support to organisations like the Southern Arican Generic
Medicines Association (SAGMA), the West Arican Pharmaceutical Manuacturers Associ-
ation (WAPMA), assisting the Saint Luke Foundation / Kilimanjaro School o Pharmacy in
Tanzania in the development o human resources; and support to companies in Ghana and
Cameroon. It is urther inormed by the work o the World Health Organization, the Arican
Network or Drugs and Diagnostics Innovation (ANDI), the various AUC Technical Com-
mittee reports and the AUC PMPA Chad workshop; by AMRH and knowledge acquired
through the New Partnership or Arica’s Development (NEPAD); the work o the USP;
and ongoing work to explore the economics o production and to establish partnerships
with organisations like the World Bank, USP, WHO, and various Arican and international
universities.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 36/119
22
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
The Business Plan incorporates knowledge gained rom this research and it has identied
challenges and problems that will be addressed by the PMPA. There are general themes
that, to a greater or lesser extent, are relevant in specic contexts but there is also a large
degree o heterogeneity o the pharmaceutical manuacturing systems across our continent
and these are refected in the fexible structure that is proposed.
The remaining parts o this document are structured as ollows:
Chapter 2 ocuses on the current state o Arican pharma and key challenges and opportu-
nities or its development.
Chapter 3 discusses proposed interventions (‘package o solutions’) to be undertaken un-
der the PMPA.
Chapter 4 outlines the implementation plan and estimated resource requirements.
1.4 SummarY o chaPter 1
Key messages rom Chapter 1 include:
• The status o the pharmaceutical sector varies dramatically across our continent
• In sub-Saharan Arica, we ace a huge inectious disease burden and a growing prev-
alence o chronic and non-communicable diseases
• In the North, the disease prole is similar to that o the West, with cardiovascular
disease, cancer and diabetes being key public health concerns
• Our continent is predicted to experience strong economic growth over the com-
ing years which should enable us to address some o the current limitations o our
healthcare systems and to improve access to essential medicines
• At present, many o our healthcare systems ace major challenges including un-
derunding, overreliance on donors, shortage o human resources, limited access
to essential medicines and signicant penetration o sub-standard and countereit
products
• As a means o addressing the access to medicines challenges in Arica, the Pharma-
ceutical Manuacturing Plan or Arica was adopted by the Conerence o Arican
Ministers o Health in April 2007 and was endorsed by the Heads o State and Gov-
ernment in Accra in July 2007
• The objectives o the PMPA are to increase access to aordable quality medicines
and to ensure a sustainable supply which will provide improved public health out-
comes as well as deliver associated economic development
• Following the directive rom the Conerence o Arican Ministers o Health held in
Namibia in 2011, the AUC was tasked with developing a Business Plan to operation-alize the PMPA

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 37/119
23
INTRODUCTION AND BACKGROUND
• A stakeholder workshop in N’Djamena in June 2011 established the Terms o Reer-
ence or the development o the Business Plan
• UNIDO was invited to assist the AUC in developing this Business Plan
• Partnerships with various institutions and ongoing initiatives are essential or the
genuine progress o our pharmaceutical industry. This Business Plan recognizes the
progress made by the AMRH initiative as well as other Arican initiatives and institu-
tions such as ANDI, the Kenya Medical Research Institute (KEMRI) and the Saint
Luke Foundation, as well as by international development partners such as UNIDO,
WHO, UNAIDS, and USP
• The Business Plan has been developed based on established expertise rom various
actors and through a consultative process that involved discussions with a wide range
o stakeholders (ministries, regulators, academia, private sector) in member states
rom all parts o our continent

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 38/119
24

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 39/119
25
OVERVIEW OF PHARMACEUTICAL MANUFACTURING IN AFRICA
2. OvERviEW OF PhARMACEuTiCAL
MANuFACTuRiNG iN AFRiCA
2.1 introDuction: the Pharmaceutical manuacturingSYStem
The context within which pharmaceutical manuacturing operates in a country is determined by
a number o stakeholders. Figure 4 provides a schematic representation o the roles and infu-
ence o key actors. This gure identies the unctions o the regulator who should ideally provide
oversight o the quality systems throughout the value chain o pharmaceutical production and
distribution. It also provides indicative examples o the tools that various government ministries
have at their disposal or infuencing the context within which the industry operates and rec-
ognizes that trade associations have an important role to play. In addition, it demonstrates that
the system is not sel contained within a country as imports compete with nationally producedproducts and the nature o export markets is dened by a similarly complex interplay o dierent
institutions that set policy, provide regulatory oversight and possibly oer support to local actors.
The impact o the international donor unded markets is also taken into account. For products
supplied to these markets, regulatory approval and oversight is largely a unction o international
actors (although registration at the national level should be required as well) and procurement
policies are dened by unding entities such as the Global Fund and the U.S. President’s Emer-
gency Plan or AIDS Relie (PEPFAR).
It should be noted that Figure 4 deals only with the system relating directly to the in situ
value chain o generic drug manuacturing. For example, in order not to overcomplicate the
picture, other stakeholders who play a less direct (although oten extremely important) role
have been omitted. Specically, the manuacturing processes, regulatory unctions, and pol-
icy making in this eld all involve specialized skills. Thereore human capital and the institu-
tions that develop and provide that human capital or the system are o great importance.
Pharmaceutical manuacturing is also a capital intensive activity and access to capital is
another key aspect that, or simplicity, has been omitted. There are a variety o sources and
mechanisms by which companies can access capital and, to some extent, the appetite o
those dierent sources (e.g. equity investors, providers o debt, oreign direct investment,
etc.) or engaging with the pharmaceutical industry is dependent on the dynamics o the rest
o the pharmaceutical manuacturing system in a country.
The actual manuacturing systems in place in dierent countries vary rom this schematic,which shows a somewhat idealized representation given that, or example, most NMRAs do
not have the capacity to ull the range o unctions that should be in place. Similarly, trade
associations may not exist, and policies rom dierent government entities may not be aligned
behind a strategy in support o the sector. The current status o the key dimensions o the phar-
maceutical manuacturing system across our continent is described in the ollowing section.
It is the interplay o the dierent components o the manuacturing system that determines as-
pects o pharmaceutical production, including competitiveness and quality o production. These
particular aspects are key i the undamental objective o the PMPA o improving access to high
quality drugs, whose production is sustainable (i.e. competitive with alternative sources o sup-
ply) is to be achieved. They are also critical or countries that aspire to export to developed mar-kets. Further, a unctioning manuacturing system has the potential to produce a broader range
o drugs than is currently produced by most o our countries engaged in local manuacturing.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 40/119
26
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
g u e 4 :
S c e c r e p e s e e
s l l l e c u l e ‘ P c e u c l u c u g s y s e ’
I n p u t s
L o c al
M an uf a c t ur i n g
Di s t r i b u t i on
M ar k e t
Trade Associations*
N a t i on al M e d i c i n e s R e g
ul a t or y A u t h or i t i e s
e. g. ov er s i gh t of
c l i ni c al t r i al s an d
GL P
e. g. d o s s i er r ev i ew ,
pl an t i n s p e c t i on ,
GMP c er t i f i c a t i on &
m oni t or i n g
e. g.
ov er s i gh t an d
enf o
r c em en t of GDP
an d
GWP
e. g.P h ar m a-
c ov i gi l an c e an d
a d v er s e ev en t s
r e p or t i n g s y s t em
M a t er i al i n p u t s ( e. g.
A P I , ex c i pi en t s )
O t h er s u p p or t i n g
i n d u s t r i e s e. g.
M ai n t en an c e an d r e p ai r
of e q ui pm en t
C l i ni c al r e s e ar c h f or
B A / B E
U t i l i t i e s
B u s i n e s s p ar t n er s
- a c c e s s t of or m ul a t i on s
an d k n owh ow
- S u p pl y a gr e em en t s
- e t c
N a t i on al S t an d ar d s
B o ar d e. g. c al i b r a t i on of
e q ui pm en t
M
an uf a c t ur er s
F
or m ul a t i on
d
ev el o pm en t
F
i n al f or m ul a t i on
P
a c k a gi n g
Di s t r i b u t i on
- ar r a y of p u b l i c &
pr i v a t e s y s t em
s
Di s t r i b u t i on
-r an g e of
m e c h ani s m s
i n c l u d i n gn a t i o
n al
s y s t em s an d d
on or
o p er a t e d s u p p
l y
c h ai n s
N a t i on al M ar k e t s
P u b l i c pr o c ur em en t
P r i v a t em ar k e t
N G O pr o c ur em en t
S u b -r e gi on al ex p or t s
• P u b l i c pr o c ur em en t
• P r i v a t em ar k e t
• N G O pr o c ur em en t
D on or f un d e d
m ar k e t f or
p an d emi c s ( b o t h
n a t i on al an d
ex p or t ) , e. g.
• Gl o b al F un d
• P E P F A R
• P MI
e. g. d o s s i er
r ev i ew , pl an t
i n s p e c t i on an d
GMP c er t i f i c a t i on
an d m oni t or i n g
O t h er NMRA s
O t h er M oF
O t h er M oH
I n t er n a t i on al r e g ul a t or y
b o d i e s e. g.
-WH O pr e q u al i f i c a t i on
pr or g amm e
- S t r i n g en t r e g ul a t or y
a u t h or i t i e s ( e. g.F DA )
P r e q u al i f i e d pr o d u c t s
f r om o t h er c o un t r i e s
l ar g el y f r omI n d i a
P r o d u c t s f r om o t h er
c o un t r i e s
p ar t i c ul ar l y I n d i a a s w el l
a s i n t r aA f r i c anT r a d e
E x t er n al
P l a y er s
V ar i o u s N a t i on al Mi n
i s t r i e s i n c l u d i n gH e al t h ,F i n an c e ,I n d u s t r y ,T r a d e
e. g.T ar i f f s onI n p u t s ,
F DI i n c en t i v e s
e. g.I n c en t i v e s t o
s u p p or t i n d u s t r y
e. g. pr o c
ur em en t
p ol i c i e s an d f un c t i on s
of t h e C M S
e. g. c on t en t of E ML ,n a t i on al
d r u g p ol i c y , ex p or t i n c en t i v e s ,
i n c l u s i on of T RI P S f l ex i b i l i t i e
s i n
n a t i on al l e gi s l a t i on
* -N o
t e t r a d e a s s o c i a t i on s c an p er f or m ar an g e of f u
n c t i on s on b eh al f of t h ei r m em b er s t o
i nf l u en
c e t h e b u s i n e s s env i r onm en t , s u c h a s d i s s emi n a t i on of b e s t pr a c t i c e , p ar t n er s h i p b r ok er i n g ,
l o b b y i n g
K e y :
=M a t er i al f l ow s
= s u p pl y of s er v i c e s / a c c e s s t ok n owl e d g e
=i nf l u en c e ,i n c l u d i n g t h r o u gh r e g ul a t or y ov er s i gh t , p ol i c y ,l o b b y i n g e t c .

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 41/119
27
OVERVIEW OF PHARMACEUTICAL MANUFACTURING IN AFRICA
2.1.1 The manufacturing system and quality
The ‘quality’ o pharmaceuticals is a unction o many dimensions including, or example:
• The level o active pharmaceutical ingredient (API) content
• Appropriate ormulation impacting on the pharmaco-kinetics o the drug (e.g. peak
concentration, dissolution prole o drug)
• Degradation o the product due to many possible actors such as poor production or
inappropriate storage and distribution
• Contamination o the product with other drugs, with impurities, or ollowing the
degradation o the API, or example, during transport or once it has been ormulated
•
Mislabelling o products
• Microbial contamination o product
This is only an indicative list o some o the areas where product quality can be compromised.
In the developed world, the risk o such ailures occurring and o sub-standard products actu-
ally reaching patients is minimized by a complex interplay o regulatory oversight that enorces
concepts such as Good Manuacturing Practice (GMP) and other aspects o the quality sys-
tem including Good Laboratory Practice (GLP), Good Distribution Practice (GDP), etc., as
well as conducting pharmaco-vigilance activities to monitor products on the market.
Another vital element is having a unctioning and ecient adverse event reporting mecha-
nism such that problems can be rapidly identied and resolved. A undamental philosophyrequired or the pharmaceutical supply chain is that quality is manuactured into the prod-
uct at all stages and that inspection and quality control at the end o the production process
is not sucient; it is just one part o an integrated approach to quality assurance.
The saety and ecacy o a product are not only a unction o the processes ollowed in its
production and distribution and their regulatory oversight. These processes are intended
to ensure that products are manuactured consistently according to the specications de-
scribed in the product dossier reviewed and approved by the regulator prior to marketing
authorization being granted. Consequently, review o detailed evidence to conrm the man-
ner in which the product behaves when given to patients is another important component o
ensuring that products are sae and eective.
Most products on the Essential Medicines List (EML) are no longer covered by patent pro-
tection and generic versions can be legally produced without the need or voluntary licences
rom originator companies. A generic product is given marketing authorization on the basis
that it is therapeutically equivalent to the originator product. This means that large scale
clinical trials o generics are not required but that evidence to attest to their equivalence to
the originator product is. In most cases, the necessary evidence is a bioequivalence study in
which clinical trials are conducted to show that the generic product behaves in the same way
as the originator when given to patients. In some cases where, or example, an active ingredi-
ent is highly soluble, approval can be granted on the basis o a biowaiver, where non-clinical
evidence o the physical and chemical properties o the product are shown to be equivalent
to the originator. Samples o products also need to be tested at quality control laboratoriesprior to marketing approval being granted.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 42/119
28
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Thereore, the components o the manuacturing system required to ensure quality o pro-
duction and saety o the product are adherence to GMP by the manuacturer (which in-
cludes design o the plant, maintenance and integrity o equipment, established and vali-
dated processes and procedures or all aspects o production and quality control at various
stages o the production cycle); development o the ormulation that is to be manuactured
with accompanying evidence to attest to the equivalence o the product to the originator;
detailed review o the dossier and sample testing by the regulator prior to marketing ap-
proval; and regular inspection o production processes by the NMRA at the manuacturing
site. Following production, the regulator also plays a key role in ensuring that the product
reaches the patient in an appropriate condition through oversight o Good Distribution and
Wholesaling Practices. A urther post production unction o the regulator is overseeing the
market through pharmaco-vigilance activities and the establishment o adverse event report-
ing mechanisms. This is required to identiy instances o sub-standard products reaching the
market so that product recalls can be rapidly enacted and countereit products identied
and removed rom the market.
2.1.2 The manufacturing system and competitiveness
The increased investment and operating costs involved in setting up and running a GMP
compliant acility do not mean that international standard production on our continent
cannot be competitive or that very large manuacturing plants are required to achieve cost
eective production. Research commissioned by UNIDO indicates that the economics o
pharmaceutical production are highly complex. This as yet unpublished working paper indi-
cates that xed costs associated with upgrades are generally directly correlated to the output
o the acility such that technical economies o scale are not particularly signicant beyond
certain airly low volumes. In act, established wisdom that a capacity o 1.5 billion tablets is
necessary or competitive production is not borne out by the analysis.
Further, the signicance o xed costs means that capacity utilization has a critical impact
on the cost o each unit o production. The nature o pharmaceutical production is that it
is a batch process where dierent products are manuactured with the same machinery.
Changeover time required between batches o dierent products represents downtime when
assets are not being productively utilized. Machine downtime can also occur where a pro-
duction line is not balanced. For example, one piece o equipment may have a greater output
per unit o time than another leading to a bottleneck situation where the machine with the
greater output remains idle or periods o time. Downtime can also occur due to breakdown
o equipment but preventative maintenance programmes can minimize the impact o this.
Modern business practices have evolved methods by which downtime o equipment can
be kept to a minimum and capacity utilization optimized. This can, or example, involve
campaigning batches o the same product so that limited changeover time is required. The
degree to which campaigning can take place to achieve eciency o production is to some
extent also a unction o the market (size and procurement agreements) as another impor-
tant component o the economics o production is working capital requirements, in which
inventory carrying costs (inputs, work in process, and retained nal products) are critical.
The above comments reer to the manuacturing o approved products. However, the cost o devel-
oping new products is signicant, particularly i bioequivalence studies are required. Companies
can buy dossiers on the open market and go through a technology transer process to set up produc-
tion in their acility. However, the cost o high quality dossiers can run to US$100,000 and more.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 43/119
29
Overview Of Pharmaceutical manufacturing in africa
These issues and the mechanisms by which the PMPA Business Plan can take them into
account and instigate solutions that enable competitive high quality production are explored
urther in the ‘challenges’ part o this chapter and in the ‘solutions’ chapter (Chapter Three).
2.1.3 The manufacturing system and breadth of product portfolio
The pharmaceutical manuacturing system described above can produce most o patent
pharmaceutical products (excluding, or example, biological products and blood products).
Moreover, by using TRIPS fexibilities or voluntary licences, even critical health products
still under patent protection, like second and third line antiretroviral drugs (ARVs), can be
manuactured. Products that involve novel combinations o active ingredients or new or-
mulations (e.g. paediatric ormulations) can also be produced through this system.
From a public health perspective, key products that a country’s health system needs to
source are listed in the WHO Model List o Essential Medicines, which countries can adapt
to their specic circumstances. The EML lists over 300 products across many disease indi-cations including analgesics, anti-allergy medicines, antibiotics, anti-helminthics, anti-TB
drugs, anti-ungal drugs, ARVs, malaria treatments, various products or tropical diseases
such as those to treat Arican trypanosimiasis, anti cancer agents, treatments or cardio-
vascular disease, gastrointestinal medicines, treatments or psychiatric disorders, drugs or
respiratory disorders, products or the treatment o diabetes and others. The WHO also has
a Model List o Essential Medicines or Children, which includes over 250 products across
a similarly broad range o indications.
These products cover dierent ormulation types including tablets, capsules, syrups, oint-
ments, gels, small and large volume parenterals, and dispersibles. The underlying quality
principles and the economics o production remain similar across ormulations (althoughor parenterals, or example, the need or sterility requires enhanced GMP). However, the
equipment required or various product types varies and the market dynamics or dierent
medications (e.g. volume requirements, level o competition, etc.) also vary. Over and above
the EML, there are many other products that are o patent and which Arica-based manu-
acturers could produce or local consumption and ultimately or export to other develop-
ing and developed markets. Some companies in countries such as South Arica and Tunisia
have, or example, been certied by American and European regulators.
2.2 the current StatuS o the Pharmaceutical inDuStrY anD other StaKeholDerS
This section describes the size and current levels o activity in the dierent segments o
the pharmaceutical industry. It also details the status o the various components o the
manuacturing system as they stand today, beore outlining the challenges aced by dierent
industry players.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 44/119
30
Pharmaceutical manufacturing Plan for africa - Business Plan
2.2.1 Industry size and participants
The Arican pharmaceutical market accounts or only a small portion o the global pharma-
ceutical industry. In 2007, the International Finance Corporation (IFC) estimated that sub-Saharan Arica accounted or just under 0.6% o the global market or US$3.8bn23, whilst
the North Arican market is valued at several more billions. Recent estimates or the whole
continent put the market at between US$8bn to US$10bn. IMS Health recently estimated
that the Nigerian market was worth US$2.5bn in 2011 and that the Arican market as a
whole will be worth about US$24bn by 201424. The pharmaceutical market in the Republic
o South Arica is now worth over US$4bn25. Estimates o the value o the pharmaceutical
market on our continent vary signicantly as a result o dierent methodologies and this is
also indicative o the paucity o data.
Although, by any measure, the Arican pharmaceutical market is small compared with the
global market, it plays host to some o the leading global innovator and generic manuactur-
ers and has a growing number o local manuacturers. The majority o Arican manuactur-ers are small privately owned companies that mostly serve their national markets. However,
there are also examples o publicly listed companies (e.g. Ayrton and Starwin in Ghana)
and some companies that have invested in their acilities through accessing international
equity nancing (e.g. Universal in Kenya). There are also domestic manuacturers that are
comparable in size to leading international generic manuacturers. For example, Aspen
in South Arica is in the top ten largest generic manuacturers in the world. Furthermore,
manuacturing o pharmaceuticals on our continent is not exclusively the purview o the
private sector. We have public sector manuacturers such as Saidal (80% state owned) in
Algeria and Saphad in Tunisia, which is also majority government owned. Mozambique has
a government owned liquid acility and is currently in the process o constructing an ARV
plant with the help o Brazil.
A urther example o direct government involvement in pharmaceutical manuacturing is a
recent development which saw a US$211mn joint venture (Ketlaphela) being ormed be-
tween Lonza, a leading global API manuacturer rom Switzerland, and the South Arican
government (through Pelchem) or the production o ARV APIs in South Arica. In the eld
o vaccine production, the South Arican Government has also ormed a Public Private
Partnership called The Biovac Institute.
Currently, there are an estimated 38 countries that have pharmaceutical manuacturing
entities on the continent. The size o the sectors in these countries is widely divergent. For
example, Nigeria has more than 200 registered pharmaceutical manuacturers, South A-
rica has roughly 30 domestic producers, and Ghana and Kenya have an estimated 20 and40 active registered manuacturers respectively. Algeria has roughly 30 manuacturers and
Tunisia about 20. Other countries such as Uganda, Tanzania, Zambia and Zimbabwe have
dynamic but relatively small sectors with between ve to ten active companies. There are
also countries such as Cameroon, Namibia, Swaziland, Lesotho, Malawi and others that
have just one or two active manuacturers.
In addition to local manuacturers, there are many importers and distributors o medicines
who import rom and represent companies rom across the world, with India and Chi-
na being the predominant suppliers. Further, the leading global innovator (Pzer, Sano,
GSK, Merck) and generic (Ranbaxy, Aspen, Mylan, Cipla) companies either have a direct
23
IFC – The Business o Healthcare in Arica 200724 IMS Health Market Prognosis 201025 IMS Health TPM 2011 and South Arican National Treasury Contract Management gures

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 45/119
31
Overview Of Pharmaceutical manufacturing in africa
presence or work through agencies and distributors. Some o these leading pharmaceutical
companies have manuacturing acilities in various Arican countries. They include, among
others, GSK, Johnson and Johnson, Sano (with plants in six Arican countries), Sandoz
and Ranbaxy. The latter now has three manuacturing acilities situated in South Arica,
Nigeria and Morocco.
A ew international companies are also involved in joint ventures with local manuacturers
and some o these have involved the transer o technology and the licensing o products
to Arican players. They include leading global generic companies like Cipla, which has an
arrangement with Quality Chemicals o Uganda, Zydus Cadila, which is in collaboration
with Almeta Impex o Ethiopia, and Ranbaxy, which is working with Community Invest-
ment Holdings o RSA. This trend is not conned to local companies only. Whilst not a
ully-fedged joint venture, Sano Aventis in South Arica recently announced an agreement
wherein Hetero o India will supply it with raw materials or the manuacture o ARVs or
local consumption26. Sano Pasteur (the vaccine arm o Sano Aventis) has recently an-
nounced a technology transer agreement with the The Biovac Institute in South Arica.
Figure 5 is a schematic that represents the typical activities o local manuacturers and dem-
onstrates that the industry is largely involved in ormulating imported raw materials. In act,
some companies even procure ready-made granules and simply start at the compression
stage. This is just one example and other types o ormulations are produced including cap-
sules, liquids, large and small volume parenterals and ointments. The exceptions to the ocus
on nal ormulation and packaging are South Arica27 and Egypt28, which have commercial
scale production o a limited range o APIs29. There is also small scale API manuacturing
or internal consumption in Ghana or the production o azithromycin API30.
5: typ ps sd ds
2.2.2 Range of products manufactured in Africa
As with other areas covered by this Business Plan, the range o products varies signicantly
across our countries. The Republic o South Arica and North Arican countries have well
developed industries with participants producing a broad range o products. The majority o 26 http://www.businessday.co.za/articles/Content.aspx?id=16889527 Fine Chemical Corporation – www.cc.co.za28 The Pharma Letter - Egypt’s pharma market set or 11.4 per cent CAGR to 2014 - http://www.thepharmaletter.
com/le/95304/egypts-pharma-market-set-or-114-cagr-to-2014-helped-by-drug-pricing-reorm-that-will-boost-
generics.html (accessed October 2011).29 Personal conversations with Dr. Alexandra Graham and Paul Lartey o Lagray Chemical Company30
A lieline to treatment: the role o Indian generic manuacturers in supplying antiretroviral medicines to developingcountries; Brenda Waning, Ellen Diedrichsen and Suerie Moon. Journal o the International AIDS Society 2010,
13:35

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 46/119
32
Pharmaceutical manufacturing Plan for africa - Business Plan
manuacturers in the rest o SSA produce a limited range generally covering nutraceuticals,
cough and cold preparations, simple analgesics and sedatives, anti-malarials, older genera-
tion antibiotics, anti-helminthics and rst generation anti-hypertensives, anti-diabetics and
neuro-psychiatric drugs.
This mismatch between the EML and actual product portolios supplied by local manu-
acturers represents a signicant latent potential market or locally manuactured products
in many parts o the continent. So long as quality standards are enhanced to meet inter-
national GMP (see solutions Chapter or a pragmatic approach), this would also represent
an important opportunity or improved public health given the regulatory limitations and
supply chain challenges that orm the basic philosophy or why local production has such
an important role to play. Expanding the range o high quality locally made products is an
important dimension towards realizing this objective.
Arguably the most signicant public health issue on a large part o our continent is HIV/
AIDS. The majority o the market or ARVs is controlled by the international donor enti-
ties and Non Governmental Organisations (NGOs). Without exception, they require that
products be prequalied by WHO or approved by a stringent regulatory authority. To date,
ew o our companies have supplied the international donor markets and it is estimated that
80% o ARV nished ormulations on our continent are imported, with the majority coming
rom India31.
There are pockets o ARV production that serve markets other than those o international
donors. For example, Danadams o Ghana won a tender rom the West Arican Health Or-
ganisation (WAHO) to supply ARVs to The Gambia, Togo, Côte d’Ivoire and Burkina Faso.
Danadams has also received emergency orders to ll requirements or donor unded pro-
grammes when supply chain and procurement ailures have led to risks o stock outs o keyproducts. Furthermore, there are a number o manuacturers in South Arica that supply
ARVs to the national government-unded market. There are also other Arican manuactur-
ers, who (despite operating to international GMP standards) have not yet applied or WHO
prequalication as the international donor unded markets are viewed as unattractive. One
reason given or this is the advantages rom which Indian manuacturers in particular ben-
et in terms o government support. One company that has achieved international certica-
tion or an ARV commented that it could compete on price with Indian companies i there
was a level playing eld and the opportunity to campaign production batches.
Malaria is another critical public health concern. The range o products or treating the
disease includes artemisinin-based combination therapy (ACT), such as artemether/lume-
antrine (AL) and artesunate/amodiaquine (AA) now identied by WHO or rst line treat-
ment, as well as older generation products such as suladoxine/pyrimethamine (recom-
mended or intermittent preventative treatment during pregnancy). There is a signicant
donor unded market or these products (with prequalication/stringent regulatory approval
requirements) but also substantial private and government unded markets. Only one com-
pany in Arica is certied by WHO or an anti-malarial and thereore able to access the do-
nor unded markets although many others have been supplying older generation products
and, latterly, the ACTs to the other market segments.
Unlike most other product types, there have been a number o in-depth studies into the
quality o drugs or the treatment o malaria. The output o such studies is very detailed and31
A lieline to treatment: the role o Indian generic manuacturers in supplying antiretroviral medicines to developingcountries; Brenda Waning, Ellen Diedrichsen and Suerie Moon. Journal o the International AIDS Society 2010,
13:35

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 47/119
33
Overview Of Pharmaceutical manufacturing in africa
some o the specic results are recognized as lacking statistical signicance. In view o this,
sweeping generalizations need to be avoided. However, in the non-donor unded markets,
evidence suggests that the quality o products is a serious concern (although there is sub-
stantial variance among countries). The evidence also suggests that signicant proportions
o imported products are sub-standard as well as some locally produced drugs.
The quality standards o our manuacturers vary dramatically and it would be unortunate
to conclude that all sources o domestic production o anti-malarials pose a public health
threat. We need to make sure that all companies reach the standards o the leading players
to ensure a reliable, sustainable source o eective anti-malarials. We cannot rely on imports
rom a diverse range o geographies since a signicant proportion o such products have
been ound to be sub-standard (although, again, signicant variance is seen among compa-
nies in terms o their ailure rate).
Many commentators have identied the recent Aordable Medicines Facility or malaria
(AMFm) as damaging to the long term sustainability o supply o quality medicines to ghtmalaria. In the short term, the Facility has led to more prequalied products being available
in the countries in which it has been active. However, this has, in turn, severely reduced
the anti-malarials market or our manuacturers, including or those who are demonstrably
superior to some o the companies rom which we have imported. The danger is that, when
the AMFm ceases to subsidize these products, our local capacity will no longer be in place
and we will have to rely on imports that cannot be properly regulated and have been seen in
some instances to pose a risk to public health.
The international malaria community recognized the unintended consequences o this ini-
tiative and, in May 2011, the Arican Leaders Malaria Alliance (ALMA) convened a coner-
ence in Nairobi, Kenya to discuss the implications and appropriate action to minimize thelong term potential downsides. Support or local industry to reach international standards
and remain competitive across its product portolios was a key recommendation o the
meeting, a message that is consistent with the proposed approach o this Business Plan.
2.2.3 Access to inputs
Arican manuacturers depend on imports or the bulk o their production inputs. Further-
more, practically all the machinery and equipment, laboratory equipment and reagents, and
production raw materials including API, aluminium oil or blister packaging, other label-
ling materials, and excipients are imported. The local contribution to inputs is conned in
some countries to starches and sugars and it is estimated that almost 95% o the continent’s
API needs are met by imports.
This reliance on imports has very real and signicant nancial implications. The lead time
required or goods to arrive rom Asia means that credit terms oered by suppliers may be
used up prior to the inputs even reaching manuacturers’ warehouses let alone being con-
verted into nished products and distributed to the market. The implications or working
capital can be dramatic and, given the high cost o trade nancing in many o our countries,
ways o addressing this cash fow and cost issue will be one area where government interven-
tion (or a dened period o time) could make a meaningul contribution to the viability o
companies as the economic structure o the industry evolves into one that is sustainable in
the long term.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 48/119
34
Pharmaceutical manufacturing Plan for africa - Business Plan
2.2.4 Quality of production
There have been no published systematic studies on the range o quality standards to which
manuacturers on our continent adhere. We know that production in RSA and North Aricais generally close to international standards with a signicant proportion o players actually
reaching international standards. Companies such as Medis in Tunisia are exporting products
to the highly regulated European market and a company like Aspen Pharmacare exports to
North America, Europe, South America and Australia among others. However, in other coun-
tries in SSA, the range o quality standards is more varied. There are two companies in the
rest o SSA that have achieved WHO prequalication o a product (Varichem in Zimbabwe
and Universal in Kenya) and Quality Chemicals in Uganda has been approved by WHO as an
additional manuacturing site or some products that have been prequalied by Cipla in India.
There are also a number o companies that are striving to achieve international manuactur-
ing standards with LaGray in Ghana, or example, having eectively achieved this as evi-
denced by the approach to the company o the United Nations Children’s Fund (UNICEF)and PEPFAR or possible supply o products such as zinc sulphate and a lamivudine/zid-
ovudine xed dose combination ARV. Cosmos in Kenya has received certication rom the
Pharmaceutical Inspection Co-operation Scheme (PIC/S). In Nigeria, the National Agency
or Food and Drug Control (NAFDAC) has been working with WHO and eleven compa-
nies, including May and Baker and Juhel Nigeria, to achieve international GMP standards
and to have products prequalied by WHO.
There are other examples o companies in SSA striving to achieve international standards,
with Cinpharm in Cameroon being an example o a company that is investing in upgrading.
Further, there are a number o companies that are investing in new plants which are be-
ing purpose built with international GMP requirements in mind. These include TanzanianPharmaceutical Industries (TPI) which has constructed a state o the art acility in Arusha,
Tanzania, and Azee Aqua and Lab and Allied, both in Kenya, which are constructing a large
and small volume parenterals acility and an oral solid dosage orms acility respectively.
Danadams is also in the process o constructing a new acility that is internationally GMP
compliant.
There is evidence then that production to international standards is possible across our con-
tinent and that we have entrepreneurs with the appetite or risk, energy, and commitment
to achieve these goals. However, as well as these (and other) leading players, we know that
there are many other companies licensed to manuacture products whose quality systems
all in some cases way below what should be acceptable. Whilst there has been no systematic
study, experts who have visited plants, and comments by regulators with access to conden-
tial GMP inspection reports, provide categorical evidence that this is the case.
There are genuine challenges conronting companies that aspire to improve quality and to
realize their ambition o achieving international GMP status. However, there are other man-
uacturers who are happy to maintain the status quo and produce to their current standards.
Discussions with various regulators revealed that, in certain cases where they were aware o
signicant non-compliance, they were either reluctant to act or were prevented rom doing
so due to political intererence.
It is encouraging that some NMRAs are working with industry to resolve such issues in a
pragmatic manner and to eect corrections gradually in order to reach acceptable interna-tional standards. One such example is the work o NAFDAC in Nigeria and the Medicines
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 49/119
35
Overview Of Pharmaceutical manufacturing in africa
Control Authority o Zimbabwe (MCAZ). However, the operating environment o compa-
nies is aected by many interrelated aspects o the pharmaceutical manuacturing system o
a country, many o which all outside the mandate o the regulatory authority. This Business
Plan proposes a systemic approach to developing the sector and identies solutions to the
various interrelated issues which, i implemented in a coordinated ashion, could support
and perhaps accelerate these initiatives. Such solutions could also enable regulators in other
countries, which aspire to become centres o excellence or pharmaceutical manuacturing,
to take similar steps.
2.2.5 Efciencyofproduction
As already pointed out, the economics o pharmaceutical manuacturing are more com-
plex than is perhaps generally realized. Key to the competitiveness o the industry is the
eciency o production. Various principles on achieving eciency have been developed in
countries like Japan and the US over the last ew decades (across industry sectors) and they
include approaches such as lean manuacturing, Total Productive Maintenance (TPM), 6Sigma and the Toyota Production System (TPS). UNIDO has conducted pilot work with
the aim o understanding how such approaches could impact on the competitiveness o the
pharmaceutical sector in Arica.
Unpublished initial reports have been shared and, although the ndings are based on a
very limited sample and top-level analysis o leading companies (rom a quality perspec-
tive), the output provides evidence that substantial eciency gains could be achieved i
Japanese-style production approaches were to be introduced. Rough estimates based on
this analysis indicate that productivity levels could be improved by around 30%. However,
the potential improvement will depend on the starting point o the company. One organiza-
tion interviewed in the course o research or this Business Plan claimed to have been ableto improve output veold through optimizing its production scheduling process, instituting
a change management process, and training all employees on the imperatives or quality and
eciency o production.
There is then substantial scope to improve the competitiveness o production through im-
plementing approaches such as TPM. However, actually realizing the benets o such ap-
proaches requires expertise, ‘buy in’ across the organization rom senior management to
production sta, and the embedding o a culture o ecient production.
2.2.6 Status of regulatory oversight
Oversight o the market is a unction o Medicines and Allied Substances Control regula-
tions. These pertain to the regulation and control o various aspects o the pharmaceutical
value chain, rom medicine registration to how the end users access medicines. The regula-
tions also speak to the unctional and operational structures o the NMRA and dene re-
sponsibilities, reporting structures, unding and so orth.
The unctions o a regulator are many and include the ollowing minimum unctions32:
• Making sure that the manuacture, import and export, distribution and wholesal-
ing o all medicines are properly licensed and that there is conormance with Good
Manuacturing Practice (GMP) and that Good Distribution Practice (GDP) is ob-
served in all activities and on all premises32 WHO Policy Perspectives on Medicines. No 7, 2003.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 50/119
36
Pharmaceutical manufacturing Plan for africa - Business Plan
• Assessing the saety, ecacy and quality o all medicines prior to granting a market-
ing authorisation
• Conducting ongoing monitoring and surveillance o the quality and saety o mar-
keted medicines to guard against harmul, sub-standard and countereit medicines
being used by members o the public
• Inspecting and controlling the inormal market, including internet-based trade, in
order to prevent illegal trade in medicines
• The monitoring o the advertising and promotion o medicines and the dissemina-
tion o independent inormation on the rational use o medicine to public sector and
health proessionals
• Participation in orums in order to promote collaboration and acilitate the sharing
o inormation and discussion o issues o common interest with other regulators at
regional and international levels
• The continual monitoring and evaluation o perormance to identiy weaknesses,
review whether objectives have been realized and to take corrective action where
needed
Most Arican countries are not yet in a position to meet these basic minimum requirements.
The key ndings o a 2010 WHO Assessment o Medicines Regulatory Systems in 26 sub-
Saharan countries33 are summarized in Table 1 below.
The study concluded that there was adequate legal provision or:
• NMRAs’ unctions
• Medicines registration, relevant documents or applicants and assessors, advisory
committees, and use o external assessors/expertise
• Licensing (manuacture, wholesale, distribution, etc.)
• Monitoring o saety, ecacy and quality o marketed medicines
but identied the ollowing weaknesses:
•Complex legal rameworks, unclear denitions o responsibilities, and regulatorygaps and overlaps; some NMRAs are not ully established and in some countries
they are not perorming all regulatory unctions
• Lack o unding, shortage o sta, lack o operational resources, no quality manage-
ment systems, no sta development programmes
• Guidelines and assessment procedures not up to WHO standards
• Poor coordination among the various authorities/bodies involved in regulating the
industry
33 WHO. Assessment o medicines regulatory systems in sub-Saharan Arican countries. An overview o ndings rom
26 assessment reports 2010.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 51/119
37
Overview Of Pharmaceutical manufacturing in africa
Nonetheless, there are countries on our continent that have more robust and ully unc-
tioning regulatory systems (although none is regarded as being stringent by international
donors). For example, the Medicines Control Council (MCC) in South Arica is a member
o PIC/S. Algeria has a rigorous inspection process whereby all batches manuactured in the
country are tested by the Laboratoire National de Contrôle des Produits Pharmaceutiques
(LNCPP), the national quality control laboratory which employs over 400 people.
Yet most Arican NMRAs ace immense challenges, inter alia a severe shortage o unding
and human resources, a high sta turnover and the consequent lack o experience in many
core unctions. They also suer rom antiquated ling and other administrative systems. The
capacity issues in most regulatory authorities go beyond a shortage o inspectors and in-
clude lack o laboratories or monitoring (or ill-equipped laboratories) as well as the skilled
personnel to operate them.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 52/119

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 53/119
39
Overview Of Pharmaceutical manufacturing in africa
In addition, the vast challenge o overseeing many thousands o products rom numerous
plants spread across dierent geographies (e.g. products rom over 1,000 production sites
registered in Kenya where the Pharmacy and Poisons Board has just six ull time GMP
inspectors) is impossible to meet the desirable level given the resource constraints. Simi-
larly, the monitoring o the market through pharmaco-vigilance and post market surveil-
lance is ar rom robust in most countries. This provides opportunities or countereit and
sub-standard products, leads to adverse events oten going unreported or undetected, and
results in ailures to recall deective products. International development partners such as
USP and WHO have been helping to improve post marketing surveillance and, as part o
this Business Plan, these initiatives will be built upon and augmented to rapidly enhance the
oversight o the market place.
The entities charged with regulation o the pharmaceutical industry have a critical role to
play in the pharmaceutical manuacturing system. International stringent regulators have
substantial resources and a wealth o experience to mobilize in conducting the ull range o
regulatory unctions. However, even the US’ FDA aces capacity limitations as evidenced bythe ever increasing time taken to approve Abbreviated New Drug Applications (ANDAs).
Given the inherent capacity challenges aced by all regulators, and the particular resource
constraints in many o our countries, we need to work together to maximise synergies (un-
der the AMRH work) and to invest in the regulatory unctions critical or public health pro-
tection and a market place that is air and competitive. The proximity o high quality local
production, coupled with targeted investment in our NMRAs, is a means by which we can
maximise the ability o regulators to protect our people, especially when we are less and less
reliant on donations.
2.2.7 Policy and legislative landscape
There are many policy and legislative tools that impact on pharmaceutical manuacturing
and they are implemented by dierent ministries within government. One key instrument
specic to pharma is a national drug policy, which is in place in most o our countries and
normally has two core objectives:
• to promote access to sae, eective quality medicines at aordable prices
• to promote the rational use o medicines and EMLs
A urther objective is oten that o developing local industry via the promotion o local pro-
duction o essential medicines. However, Ministries o Health (MoH) in isolation do not
control the ull range o instruments that impact on the ability o the local pharma industryto develop. Consequently, whilst promoting local production may be an ambition, without
coordinated action across dierent ministries, there can be policy incoherence. Moreover,
the objectives o the MoH may not be refected in the activities o, or example, national
revenue authorities or ministries o trade and industry.
Historically, where dierent priorities guide the work o dierent government ministries
and departments, this has resulted in conficting approaches to the pharmaceutical industry.
Not many countries on our continent have an explicit strategy or the pharmaceutical sector
which coordinates the tools at the disposal o dierent government ministries. As a result,
there are requent examples o conficts in policy as implemented by dierent government
actors. There are many dierent policy and incentive tools that governments can employ or
various objectives yet, without specic consideration o how these tools aect the pharma

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 54/119
40
Pharmaceutical manufacturing Plan for africa - Business Plan
sector, policy incoherence is somewhat inevitable.
Countries with thriving pharmaceutical industries like India and China provide signicant
government support to their producers in the orm o incentives and protectionist policies.
Policy instruments that have been used to protect pharmaceutical sectors in developing
regions include:
• High taris on imported nished products. For example, India is reported to have
duties or nal ormulations o up to 56%; Brazil has a 15% tari or nished or-
mulations; and China has recently imposed import taris o up to 37% on Sula-
methoxazole (SMZ) imported rom India34
• Procurement preerences. Brazil has a 25% price preerence and Russia has intro-
duced measures to ensure that 70% o products procured by the state are locally
manuactured. This has apparently led to many Indian companies considering put-
ting up manuacturing plants in Russia35. South Arica has local production preer-ence points in tenders and is in the process o replacing these with a new system
where a percentage o designated products will be procured only rom domestic pro-
ducers. Procurement preerences legislation is in place in a number o other coun-
tries in Arica but is not always utilized
These examples highlight that some emerging countries have taken active steps to protect
and support their pharmaceutical industries. Manuacturers oten also benet rom other
means o support. In India, it is claimed that producers o nal ormulations receive sub-
stantial government assistance to promote exports including:
• Duty ree imports o equipment and raw materials or export products
• Ten year tax holidays i located in Special Economic Zones (SEZs)
• Export credits
• Low utility rates
• Working capital credits
• Enhanced depreciation allowances
The result is that nal ormulation imports to our continent have beneted rom substantial
government support in their country o origin and then oten do not attract duty. Con-versely, Arican manuacturers requently have to pay up to 25% taris on imported APIs
(and other inputs).
This situation is obviously working against local industry. The lack o a level playing eld
poses a genuine threat to the sustainability o high quality pharmaceutical production in
Arica and limits the ability o companies to make the investments required to upgrade their
plants. It is imperative that this imbalance is addressed i the enabling environment needed
or sustainable high quality production o nished products in Arica is to be achieved. Only
in this way will the dire consequences o relying on imported drugs rom a quality (and pos-
sibly price) perspective be avoided.34
http://www.thehindu.com/business/article2366488.ece35 Pharma exports to grow 35% this year. http://www.business-standard.com/india/news/pharma-exports-to-grow-
35-this-year/451194/

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 55/119
41
Overview Of Pharmaceutical manufacturing in africa
In other developing regions and some parts o Arica, protectionist tools such as restricted
lists have been used in support o the industry. These lists involve import prohibition on
identied products and have been used in countries such as Nigeria and Ghana. According
to local actors, these lists have been instrumental in the development o domestic industry.
For example, it appears that, until Ghana introduced a restricted list o 13 products, it
had ve local manuacturers and that today it has 22 active manuacturers. In Algeria and
Tunisia, once a locally manuactured generic is registered, the innovator is given two years
in which to commence local production. Failure to do this, results in a ban on importation
o the nished product and the market can then only be served through locally produced
products. This strategy has been important or local industry growth in both these countries
where, in addition to government owned laboratories, the market has seen the entry o a
number o private sector players in the last ten years.
However, the context in which restricted lists and other protectionist tools are introduced is
critical. In considering such steps, it is imperative that public health implications are priori-
tized. Direct support to industry to take advantage o the opportunities arising provides achance to upgrade to international standards over a dened period o time and to level the
playing eld or our manuacturers. Once a critical mass o companies has reached requisite
standards, a restricted list can be put in place.
Nonetheless, a recent study published by WHO36 (which supports development o local
production o essential medicines) nds that the evidence to link local production to im-
proved access (in terms o the range o dimensions) is ambiguous. Evidence is taken rom,
or example, India where the emphasis has perhaps been more on developing industry or
its export potential than on national public health. This is a cautionary observation since a
undamental objective o the PMPA is improved public health.
This Business Plan is premised on the view that high quality local production will benet
public health across our continent as well as provide economic benets. For this to be
achieved, industrial development tools must be utilized and coordinated with health priori-
ties in a coherent policy and regulatory ramework that supports and requires the industry
to meet established standards. Chapter Three will elaborate on how a pragmatic and holistic
approach can enable companies to continue to operate and have improved access to ac-
tors needed to upgrade whilst risk to public health rom short term non-GMP standards o
production is minimized.
2.2.8 Supporting industries and associated infrastructure
Well developed related and supporting industries and inrastructure are crucial or the phar-
maceutical sector. The supporting unctions encompass the creation o the appropriate sci-
entic and knowledge base and include educational and training institutions; laboratories
and research institutes involved in preclinical and clinical testing (clinical research organ-
isations and research labs); suppliers o all manuacturing equipment and inputs; as well
as a sound logistical system or distributing both inputs and the nished products. Other
supportive inrastructure includes legal and nancial systems; developed inormation and
communications technology (ICT); and a reliable and aordable supply o utilities.
Lack o related and supporting industries poses signicant challenges or the Arican phar-
maceutical sector. For example:
36 Local Production or Access to Medical Products: Developing a Framework to Improve Public Health. WHO publi-
cation. 2011.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 56/119
42
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
• Whilst in some member states there are world-class research acilities, the majority
o Arican states lack clinical research organisations and bioequivalence centres. As
a consequence, companies have to seek out these services globally (many products
currently on the market have not been through such studies or provided similar evi-
dence – e.g. biowaiver)
• Distribution chains are ragmented and grossly inecient with as many as 724 li-
censed medical distributors in Nigeria37, over 200 in Zimbabwe38 and 296 in Sudan
and South Sudan39
• Utilities are unreliable and prohibitively expensive and supply interruptions are a
regular occurrence
• The nancial and legal inrastructure in the majority o Arican countries is not sup-
portive o the development o Arican pharma
• Specialised skills and know-how are required in areas including tooling and abrica-
tion, clinical research, instrumentation and equipment calibration to name but a ew.
The absence o these skills in some markets results in a situation where local compa-
nies oten incur additional and unavoidable costs or the maintenance o advanced
technologies because they have to fy in experts rom abroad
• The lack o a reliable supply o market intelligence services is also problematic as
it limits manuacturers’ ability to make decisions on product choice, portolio opti-
misation and production and supply chain planning. Investors have cited a lack o
credible market data as being an important issue that limits their enthusiasm or the
sector
2.2.9 Skilled human resources
The pharmaceutical manuacturing system requires specialized skills in a number o disci-
plines, including pharmacy, chemistry (analytical, organic, synthetic, medicinal), the bio-
logical sciences (biochemistry, microbiology, molecular biology), engineering (mechanical,
electrical, chemical, industrial, process), the lie sciences (medicine, pharmacology, toxicol-
ogy), and management (strategy, nancial and management accounting, operations, logis-
tics, commercial law, etc.) and Inormation and Communications Technology. The current
training and education landscape consists o various providers with the key partners being
traditional universities which oer various science, engineering and technology degrees.
These degrees are relevant only to the extent o providing solid grounding in scientic
theory which is crucial or industry. However, they lack industry applicability and practical-
ity. Thereore, a chemistry graduate will still need industry-specic training to gain the skills
which will render him/her productive in a manuacturing environment.
Stakeholders report, or example, that it takes up to three years to train a new recruit who
has a basic qualication in the various relevant disciplines and to convert him/her into a
skilled pharmaceutical operator. This is not uncommon and experience rom around the
world shows that there are a number o institutions that oer training to bridge such a
gap. Stakeholders also report that the lack o available skilled human resources across the
broad array o disciplines identied above is a major constraint and that the resources and
37
IFC38Personal communication with pharmaceutical executives39WHO

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 57/119
43
Overview Of Pharmaceutical manufacturing in africa
expertise needed to enhance the skills o workers across the industry system are insucient.
Furthermore, there is limited access to the know-how required to implement international
GMP. A number o companies who have sought guidance rom international consulting
rms have ound that guidance to be, at times, o questionable value and oten prohibitively
expensive.
There are a number o ongoing initiatives aimed at increasing the supply o skilled human
resources or the pharmaceutical manuacturing system. They include:
• WHO’s Essential Medicines Group which organizes ongoing training activities in
support o the industry as well as capacity building or regulators
• USP, which has been working with a number o regulators to enhance post market-
ing surveillance capabilities and has also developed a set o modules or training in
dierent technical aspects o production that could be developed or and rolled out
in Arica
• The collaboration between Saint Luke Foundation in Tanzania and Howard and
Purdue Universities in the US. This collaboration has already established a valuable
model or the training o industry actors and regulators at the Foundation’s indus-
trial pharmacy training centre in Moshi, Tanzania
• Various Arican universities and research institutes involved in training science un-
dergraduates
• Other Non-Governmental Organisations, such as Action Medeor, which run cours-
es on various aspects o the disciplines involved in pharmaceutical manuacturing
These and other worthy initiatives need to be built upon so that the requisite skills or the
sector can be developed and models rom other continents adopted in a concerted and com-
prehensive approach. In other geographies, there are specialized training institutions which
oer programmes specic to the pharmaceutical industry across many o the requisite skills.
Examples include institutions like Purdue University and Stephens Institute o Technology
in the United States and the National Institute or Pharmaceutical Education and Research
(NIPER) in India.
The Saint Luke Foundation/Kilimanjaro School o Pharmacy and Muhimbili University in
Tanzania are examples o specialized centres in Arica that have demonstrated a valuable
model or the training o industry actors. Expanding this and strengthening other entities
with the potential to provide specialist training is critical to the long term sustainability and
viability o the industry on the continent.
2.2.10Accesstonance
Access to aordable investment capital is regularly identied by the industry as a key chal-
lenge that limits its ability to make requisite investment in upgrading to international GMP
standards. In 2011, UNIDO conducted some research into the capital requirements o com-
panies and the availability o dierent types o unding. The options covered included tradi-
tional bank debt nancing, various types o equity nancing, and the opportunity or access-
ing nance rom international sources (including the well developed nancial community in
South Arica and Development Finance Institutions (DFIs) based in the developed world).
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 58/119
44
Pharmaceutical manufacturing Plan for africa - Business Plan
From a demand perspective, most companies in SSA (outside South Arica) wanting to in-
vest in upgrading acilities required long term capital (5+ years) to the tune o multi-million
dollar sums (specic cases vary dramatically but typically US$5mn as a bare minimum).
This research established that traditional bank debt nancing was problematic given the
high interest rates involved (15% to 30+% depending on the country or local currency
denominated loans). An added deterrent, which made such approaches unattractive in the
current context, was the risk o dollar-denominated debt, appreciating against the local cur-
rency. It also ound that loans in excess o US$3mn were rarely available and that the term
was usually less than ve years.
However, there are alternative sources o unds available (to a greater or lesser extent), in-
cluding:
• Local private equity (PE) and venture capital (VC) investors
• Some (though very limited) Initial Public Oerings (IPOs) on certain national stock
exchanges
• International private equity and venture capital investors
• DFIs
• Not-or-prot international organizations (both generalists and healthcare ocused)
• Pharmaceutical collaborative (technical) partners (including capital injection aspect
through to overall deal structure)
Nonetheless, these entities identied various concerns that limit their appetite or the do-
mestic pharmaceutical industry, including corporate culture, exit opportunities or equity
investors, and general pharmaceutical industry considerations.
Corporate culture
With regard to corporate culture, the issues most commonly cited included:
• Businesses generally controlled by one shareholder or amily
• Focus on retaining the business to pass on within the amily
• Reluctance to view exits such as M & A (Mergers and Acquisitions) or a stock mar-
ket listing positively
• Poor corporate governance
• Poor record and account keeping, lack o audited accounts and other records
• Poorly unctioning Boards o Directors – lack o outside independent business experts
• Poor planning; lack o long term strategy and vision

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 59/119
45
Overview Of Pharmaceutical manufacturing in africa
• Personnel issues (e.g. amily-owned companies hesitant to recruit external senior
management)
Exits or equity investors
For equity investors, the exit options are o concern. The most likely are:
• Initial Public Oering (IPO)
• Trade sale/M & A
• Buy-back by majority shareholder o equity stake
• Purchase o shares by strategic nancial investor (e.g. larger private equity group)
The IPO market is oten limited due to both immature public markets and aversion o
companies to seek a listing. In view o this, an IPO is oten not high on any investor’s list as
an exit strategy. M & A opportunities are also oten limited although, with time, increasing
demand, and evolving business models and management culture, this may change.
Given the current dynamic and limited opportunities or IPO and M & A, some venture
capital groups structure their exit into the initial investment agreement, aiming to allow the
investment to match both their requirements and to appeal to amily shareholders by using,
or example, call and/or put options (i.e. share buy-back clauses) and by dening upront
exactly what growth and increase in value is required. In other words, this share buy-back
structure entails purchase o the venture und’s stake by the major shareholder – generally
the controlling amily – at a pre-agreed price premium.
This creative deal structuring addresses the exit issues inherent in the local market. Im-
portantly, it also addresses a key concern o amily-owned businesses who want to retain
long-term ownership within a tight circle o shareholders since it gives them the ability to
buy out the investor. However, a negative aspect o this structure is that, should the major
shareholders not be in a position to buy back the shares, there are likely to be contractually
agreed penalties enorced by the investor.
The nal option, purchase o the share stake by a new private equity investor, is currently
relatively unlikely. However, with improved market conditions and the increasing attrac-
tiveness o local manuacturers, such exits may be more likely with time, especially wheninternational PE houses acquire stakes in these companies as a means o rapid expansion
into sub-Saharan Arica.
Pharmaceutical industry concerns
The industry specic issues most oten raised included:
• Need to recruit specialized, highly trained sta and the limited local availability
• Inability to manuacture quality products that are competitive with subsidized im-
ports

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 60/119
46
Pharmaceutical manufacturing Plan for africa - Business Plan
• Lack o accurate, comprehensive market data, analysis and orecasts
• Weak regulation and consequent penetration o sub-standard and countereit prod-
ucts which then erode the market
Overall implications or accessing capital
Sources o equity do exist and could be accessed by the dierent industry players although
no one capital structure or source o unding will be appropriate or all players. The observa-
tions rom this work are that an improved market context and evolving nancial systems will
increase options. However, it is also clear that direct government intervention in addressing
the weaknesses o the pharmaceutical system will be an important actor that encourages
all orms o investor to show greater enthusiasm or the industry. It would also be helpul i
international entities such as the IFC were to review their current policies on investment in
the sector in Arica (e.g. requirement or WHO prequalication). Such policies hinder themin ullling a role in supporting the development o high quality manuacturing o essential
medicines on our continent with the associated health and economic benets.
2.2.11 Status of intra Africa trade in pharmaceuticals
The ability to access regional markets depends on a number o actors, including com-
petitiveness, product portolio, product quality and price, as well as the ability to meet the
regulatory requirements and processes o regional NMRAs. Market penetration and access
also refect the ability to adapt to dierent circumstances and speak to the need to revise
and amend business models, orm partnerships and do what is necessary to succeed in other
markets. Access to markets is also reliant on the sector having ecient internal regulatoryprocesses, eective supply chains and willing buyers.
It is generally dicult or local manuacturers to access external markets because o poten-
tial buyers’ perception that their products may be o poor quality and the general lack o
aith in the competencies o other regulatory agencies. Furthermore, registration delays and
the peculiarities o regulatory rameworks in external markets are problematic. Improved
trade among our countries in the realm o pharmaceuticals is dependent on increasing the
links between our companies and on supporting local industry to compete with imports in
the short term whilst it evolves to a point o long term sustainability.
Data on trade in pharmaceutical products among our member states is limited, mainly be-
cause the ocial trade statistics are not suciently disaggregated to allow the precise iden-
tication o most pharmaceuticals. However, it is oten quoted that 30% o pharmaceuticals
used in Arica are made on the continent, suggesting that there is signicant room or expan-
sion. Outside the donor unded markets, the regulation o imports rom other continents is
extremely problematic. Consequently, increasing market share o products manuactured
under close scrutiny by our NMRAs through increased intra Arica trade in pharmaceuticals
will contribute to improved access to quality, aordable essential medicines.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 61/119
47
Overview Of Pharmaceutical manufacturing in africa
2.2.12 International development assistance for local production
Our development partners have, until recently, adopted dierent stances on the importance
and imperative o strengthening local production o essential medicines. Now, however, thegeneral consensus is shiting towards our own position, which was publicly ormalized in
2005. Yet, despite this historical lack o consensus, many initiatives have already been taken
by the international community to support local production or in support o our health
systems (e.g. through improving pharmaco-vigilance). Actors have included multilateral or-
ganisations, bilateral arrangements between countries, universities, and non-governmental
organisations. The areas o intervention have included regulatory capacity strengthening,
regulatory harmonization, skills development, and technology transer.
However, despite concerted eorts on many ronts, we have still not seen the hoped or
development o the sector. In part, this may be due to lack o coordination among initia-
tives, a somewhat inevitable consequence o dierent institutional priorities, mandates and
time perspectives. Now that we have developed the PMPA Business Plan, this will provide acentral unction to acilitate coordination and cooperation so that there is a genuine impact
on improving health outcomes (and associated economic benets) through developing the
local pharmaceutical industry.
2.3 challengeS anD oPPortunitieS or local ProDuction
The previous section described the current status o the pharmaceutical manuacturing
system across our continent. It highlighted the diverse contexts but also embarked on iden-
tiying some general trends and issues that represent both challenges and opportunities orthe sector i it is to deliver on the vision o high quality, aordable essential medicines and
associated economic benets. Here, we lay out the specic challenges and opportunities
aced by the industry.
2.3.1 Challenges of achieving universal GMP
As demonstrated, achieving GMP standards is technically possible across our continent but
genuine challenges ace the industry i companies are to reach and maintain this level.
In general, these challenges can be broken down into technical considerations regarding
the expertise needed in setting up and running high quality plants; nancial considerations,
such as mobilizing investment capital; achieving and maintaining competitiveness given the
cost implications o setting up and running a GMP compliant acility; and inrastructure
to assist local production, such as access to bioequivalence acilities and other supporting
industries.
The current situation on many o these issues has already been described and a summary
o key challenges as perceived by the industry is now given in Table 2. However, pharma-
ceutical manuacturing companies currently display a wide range o attitudes. They include
companies that have already demonstrated their commitment to international standards
and achieved them; those who are currently in the process o upgrading their operations;
companies who aspire to improved quality but have so ar not been able to mobilize the
necessary range o expertise and resources; and those that are happy to continue producingat standards signicantly below GMP.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 62/119
48
Pharmaceutical manufacturing Plan for africa - Business Plan
tb 2: Ky s dfd by p s v vs gmPsdds
Technical Expertise Financial Considerations Infrastructure Requirements
•Accesstoknow-howforde-
signing,upgradingtoandrun-
ningGMPcompliantfacilities
•Accesstoskilledhuman
resourcessuchasindustrial
pharmacists,microbiologists
andanalyticalchemists
•Accesstoaffordableinvest-
mentcapital
•Policyincoherence(e.g.taxon
inputsversustaxfreeimpor -
tationofnishedproducts,
restrictedlists,capitalcontrols,
etc.)
•Marketcontext(e.g.penetra -
tionofcounterfeits,uneven
playingeldversusimports–
tosomeextentafunctionof
policyincoherence)
•Variabilityinqualityamongstmarketplayers
•Accesstoexportmarkets
andtheircurrentfragmented
nature
•Competitiveproductiongiven
coststructure(functionofef -
ciency)
•Reliableutilities(implications
forcostaswellascompliance
withGMP)
•Accesstobioequivalence
centres
•Regulatoryoversight(impact
onaccesstocapitalandmar -
ketcontextconsiderations)
•Underdevelopedsupporting
industries(implicationsforcost
andquality)
•Lackofmarketdata(implica -
tionsforstrategicplanningandaccesstocapital)
•Uncoordinatedand/orvertical
approachestodevelopingthe
sector
Depending on where companies are positioned along the production chain, rom very low
to international standards, unsurprisingly, they have diering views on the challenges theyace and their ability to reach and maintain competitive production to international stan-
dards. For those that have achieved the mark, or are well on their way to it, concerns relate
to sustainability as technical challenges have already been addressed. For example, leading
manuacturers cite limited regulation o the market as a key challenge given that they have to
compete with rms with lower standards and thereore a lower cost base. For others, there
are concerns that the sector’s reputation or variable quality standards could limit the op-
portunity or exports and even create a preerence in their domestic market or international
products. They also cite ‘unair’ competition rom companies overseas who benet rom sig-
nicant government support and may also be manuacturing to standards below their own.
Furthermore, the lack o coherence in policies previously described is also a cause or con-
cern given the advantage that imports oten enjoy. Companies that aspire to manuacture
to international standards also cite lack o regulatory oversight as an important barrier. This
is one o the issues identied by investors as currently limiting their enthusiasm or the in-
dustry in many countries. Pharma companies oten also cite the challenges in accessing the
necessary know-how to implement upgrading programmes. However, or some companies,
these barriers and the lack o regulatory enorcement mean that they neither need nor aspire
to improve production standards.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 63/119
49
Overview Of Pharmaceutical manufacturing in africa
2.3.2 Specicopportunitiesforstrengtheninglocalproductionofmedicines
This sub-section describes three particular areas - utilizing the TRIPS fexibilities; synergies
with R & D initiatives; and greater linkages between manuacturers as well as other actors – rom which local pharmaceutical manuacturing could benet in order to become a critical
public health asset or the continent.
Intellectual property rights and ull use o TRIPS exibilities
Many Arican countries belong to the World Intellectual Property Organization (WIPO) and
the World Trade Organization (WTO) and consequently observe international norms and
standards with respect to Trade-related aspects o Intellectual Property Rights (TRIPS).
Protection o such rights is enshrined in national legislation and, in cases o inringement,
intellectual property right holders can seek relie rom courts and assert their rights in cases
o patent, trademark and copyright inringements. Most Arican countries enjoy the early
working provision (Bolar) that allows companies to research and develop a product beore
patent expiry. Further, there are no data exclusivity (DE) provisions and no supplementary
protection certicates (SPCs).
Thus, market entry in non-LDC Arica can occur immediately upon patent expiry. How-
ever, despite these provisions and largely because o small markets and delays in medicine
registrations, many international companies rarely register patents in Arican jurisdictions
or launch generic equivalents already developed ahead o later patent expiries in Europe and
North America. Because many countries on the continent are classied as Least Developed
(LDCs), in line with WTO rules, they have until January 2016 to comply ully with the
TRIPS provisions. Furthermore, there is a strong possibility that the 2016 deadline may beextended. The TRIPS fexibilities include the ollowing:
• Exemptions rom patentability (Article 27.1, 27.3)
• Provisions to issue compulsory licences and authorize parallel imports (Article 31)
• Exhaustion o rights (Article 6)
• Limitations on data protection (Article 39.3)
• Bolar provision or early working (Article 30)
Article 31 grants governments the right to license third parties to use patents without the
consent o the rights holder i it is in the public interest; in cases o national emergency; i
there is ailure by the rights holder to exploit the patent or there is insucient working; and,
lastly, as a remedy to anti-competitive practices. This provision is mainly or the supply o
the local market but it does not preclude use or exports to LDCs without any manuactur-
ing capacity. It was introduced ollowing the adoption o Paragraph 6 o 2003 which waived
the requirement o Article 31() o TRIPS which stipulated that compulsory licences (CLs)
could only be issued or domestic use and was in recognition o the act that many LDCs
that needed to make use o the fexibilities had no domestic manuacturing capacity. Lastly,
it is important to emphasize that Article 31 is not intended or use only in emergencies and
is not limited to certain diseases.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 64/119
50
Pharmaceutical manufacturing Plan for africa - Business Plan
For various reasons, only a ew member states have exploited the fexibilities. One o the
most important reasons is that many LDCs have not incorporated the fexibilities into their
national legislation as they are required to do prior to exploitation o the provisions. In act,
a review o many LDCs’ intellectual property laws reveals that they not only ully comply
with the WTO’s Trade-related aspects o Intellectual Property Rights (TRIPS) agreement
but, in some cases, ar exceed the protections o intellectual property rights expected o
them (TRIPS+).
Other reasons why LDCs and other Arican countries (with productive capacity) have not
taken advantage o the TRIPS fexibilities include:
• A lack o political will to enact the necessary amendments to intellectual property
rights law to enable countries to exploit the fexibilities
• A general lack o knowledge among the technocrats tasked with dealing with IPR
and access to medicine issues about the fexibilities and how to go about creating anenabling environment; and, nally
• Capacity constraints such as weak legal and regulatory rameworks and weak sup-
porting technical know-how and administrative capacity which remove any incentive
or inclination to act on the fexibilities
Arica thereore aces a simple choice in the next our years - to ully exploit the TRIPS
fexibilities and accelerate the ongoing negotiations or an extension to the 2016 transition
period or ace the prospect o paying more or drugs in the uture. The global economic
crisis has seen the scaling down o treatment programmes and the cancellation o Round 11
o the Global Fund. It is clear that in the long term the sustainability o treatment regimes
in Arica may well depend on the ability to ully utilize the fexibilities and to develop the
competencies to make our own medicines. Chapter Three o this document will propose
how the Business Plan can endeavour to acilitate the utilization o these fexibilities or the
benet o the peoples o the continent and or local manuacturers who are international
GMP compliant.
Research and development
Arica lags behind other regions o the world when it comes to innovation and knowledge
creation. In 2002, the continent spent just 0.3% o GDP on R & D versus the global average
o 1.7% and had only 1.2% o the world’s researchers40. The Organisation or Economic Co-
operation and Development (OECD) reers to research and development (R & D) as the
“creative work undertaken on a systematic basis in order to increase the stock o knowledge,
including knowledge o man, culture and society, and the use o this stock o knowledge to
devise new applications”41.
R & D activities broadly cover three areas o activity: basic research, applied research, and
experimental development, all with the sole intention o discovering and generating new
knowledge and products and ultimately providing solutions to problems.
The capabilities needed or R & D are important or innovation and the discovery o new
products, or reverse engineering current products, and or creating new ormulations and
40 A World o SCIENCE, Vol. 2, No. 1, January–March 200441 OECD denition

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 65/119
51
Overview Of Pharmaceutical manufacturing in africa
delivery systems. The shortage o researchers on the continent is exacerbated by the loss o
skills to the developing world. For example, it is estimated that more than a third o practis-
ing highly skilled Arican scientists are now living in the developed world42.
However, the situation is changing, with greater emphasis now being put on R & D and
with the ormation o key institutions like the Arican Network or Drugs and Diagnostics
Innovation (ANDI). At continent level, the need to promote research and development is
refected in a number o documents, including:
• Arica Health Strategy 2007-2015
• Global Strategy and Plan o Action on Public Health, Innovation and Intellectual
Property (WHA 61.21 o May 2008), a WHO document
• Abuja Declaration o March 2006
• Accra Declaration on Health Research o June 2006; and
• Algerian Declaration on Research or Health in the Arican Region o June 2008
Furthermore, various countries have national research strategies and are investing signi-
cant resources to scale up R & D. Government owned institutions and medical research
institutes now have active medicinal and drug discovery programmes and some leading
teaching institutions have also created drug discovery and development programmes, as well
as clinical trial centres which can be used or bioequivalence testing.
Local pharmaceutical companies on the other hand are not involved in any original R & D
work. A ew companies do have research and development programmes but most have onlysmall ormulation departments where reverse engineering o marketed medicines is done.
Innovator companies that are active on the continent do not undertake any direct original
research work in Arica although they outsource some parts o the development work to
institutions on the continent and spend considerable resources on clinical trials or new
chemical entities.
The PMPA and other Arican imperatives recognize the critical importance o original and
basic research (drug discovery and development) and its overall strategic importance to the
uture and long term viability o the industry on the continent. However, or the purposes
o this Business Plan, R & D is used broadly to reer to experimental development which
entails the use o existing scientic, technological and other knowledge and skills in order to
produce modied or improved products, processes and services. This is particularly relevant
to the creation o new ormulations, delivery systems, combination products and paediatric
ormulations, areas in which Arican manuacturers are ar behind their counterparts in
other developing countries.
Nonetheless, novel R & D should become an increasingly important ocus area or our
continent and competencies in this eld will have to be built up signicantly. This need is
evidenced by the act that less than one per cent o all the thousands o new chemical entities
developed in the last 30 years are or treating the neglected diseases which predominantly
aect Arica43. Consequently, organisations like ANDI need to be supported in their work so
42
Joint Statement by the Network o Arican Science Academies. July 2009 - www.nationalacademies.org/includes/NA-SACbraindrain09.pd (accessed December 2011)
43 Pierre Chirac, Els Torreele. Global ramework on essential health R & D. The Lancet Vol. 367 May 13 2006

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 66/119
52
Pharmaceutical manufacturing Plan for africa - Business Plan
that they can respond to the needs o the continent or eective medicines or the diseases
that plague us. Furthermore, ANDI has set up a network o 32 centres o excellence across
Arica involved in drug discovery, pre-clinical and clinical work.
The AUC believes that our continent should tap these skills sets and competencies to re-
spond to the needs o industry or innovative ormulations, improved delivery systems and
paediatric ormulations among others. Consequently, the AUC will, in partnership with
ANDI and others, seek to ast track the development o technologies and the speedy diu-
sion o these technologies to international-GMP-compliant Arican manuacturers.
There are a number o research partnerships between Arican and international organisa-
tions and they include:
• The National Research Foundation o South Arica/Emory University/SCYNEXIS
Advanced Drug Discovery Program
• The Drugs or Neglected Diseases initiative’s (DNDi) clinical research platorms:
Leishmaniasis East Arica Platorm (LEAP) in Kenya, Ethiopia, Sudan, and Ugan-
da; and the Human Arican Trypanosomiasis (HAT) Platorm based in the Demo-
cratic Republic o Congo (DRC) or ghting sleeping sickness
• The Medicines or Malaria Venture (MMV) network o clinical trial sites in malaria-
endemic countries
These partnerships need to be encouraged and accelerated and the AUC is keen to engage
with them and others to explore how work under the PMPA can assist in making new prod-
ucts widely available.
Partnerships, collaboration and improved business linkages
Partnerships and collaboration between industry and various players such as R & D institu-
tions, education and training providers are critical or the growth o the industry. Moreover,
partnerships between manuacturers themselves are needed to realize economies in product
development, raw material procurement, equipment servicing and maintenance among oth-
ers. In our industry, the practice o partnering is not well entrenched. Table 3 reviews the
current status o such partnerships which are critical or the growth o the industry and or
increased access to medicines.
The current limited number o relationships between regional and international entities
represents an opportunity or the sector. Facilitating partnerships between companies on
our continent, as well as with international rms, could enable access to various industry
needs including know-how, enhanced product portolios and investment capital. There is
also the potential to strengthen relationships between the corporate sector and academia on
the continent and via Product Development Partnerships (PDPs) among others.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 67/119
53
Overview Of Pharmaceutical manufacturing in africa
tb 3: Ss psps p p s a
Partnership type Functions Status
R&Dpartnershipsbetweenin -
dustry,universitiesandresearch
institutes
Importantforinnovation,discov-
ery,developmentandcommer -
cialisationofnewproductsand
newgenericformulationand
deliverysystems
Nonexistent
ANDIseekstollthisspace
Technologytransferpartnerships
betweenlocalcompaniesand
externalpartners
Importantfortheintroduction
ofnewtechnologiesandprod-
uctsquicklyandtosignicantly
reducedevelopmentcostsand
timetomarketinthecaseof
generics
Afewexamples:
•CiplaandQualityChemicals
(Uganda)
•ZydusCadilaandAlmeta
Impex(Ethiopia)
•AspenGSK(RSA)
•SanoPasteurandTheBiovac
Institute(RSA)
Educationandtrainingprovision
partnershipsbetweenindustry
andinstitutionsofhigherlearning
Fortheprovisionofadequate
trainingandeducationrelevant
totheskillsrequirementsofthe
pharmaceuticalindustry
Scarce:
•MuhimbiliUniversity(TZ)
•SaintLukeFoundation(TZ)
Partnershipsbetweendevelop -
mentpartners
Forcoordinatedandintegrated
supportresponsivetotheneeds
ofindustry
Present:
•WHO&USP
•UNorganizations(UNIDO,
UNCTAD,UNDP,WHO,
WorldBank)
•UNIDO,
Cooperationbetweenindustry
andvariousstakeholdersin
government
Forthecreationofanenabling
andsupportiveenvironmentas
wellasasharedvisionforthe
industry
Weak–alotofworkneedsto
bedone
Businesslinkagesbetweenlo-
cal,regionalandinternational
companies
Thisisfortechnologytransfer,
accesstonewproductsandfor -
eigndirectinvestmentintothe
localpharmaceuticalsector
Multipleagenciesandproductor
distributionlicensingagreements

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 68/119
54
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
2.4 SummarY o chaPter 2
6: is s ss v
Research &
development
Capacity & skills shortages
Poor quality & counterfeit drugs
Facilites not GMP compliant
Weak regulatory framework
Lack of/poor technology
Limited access to markets
No market data
Lack of partnerships & linkages
• Conflicting policies & regulations
(trade, health & industrial)
• Absence of shared pharma vision amongst
stakeholders
• Lack of funding & government support
• Mismatch between industry needs & education
provision
ManufacturingSales &
Marketng Distributon
• Rigid IPR laws
• Weak supporting industries
• Poor business practices
O t h e r
C h a l l e n g e s
Key messages rom Chapter Two include:
• Pharmaceutical manuacturing occurs within a complex system with a wide range
o stakeholders
• The status o the ‘pharmaceutical manuacturing system’ in those o our countries
where manuacturing occurs is unique
• The current status o manuacturing activities on our continent varies dramatically
across countries
• In North Arica and RSA a broad range o products are manuactured but in most
o SSA product portolios are generally limited
• There are ew internationally certied (WHO prequalication or approval by a
‘stringent’ regulator) manuacturers or products against HIV and malaria
• Most inputs are imported, with an estimated 95% o APIs coming rom overseas,
largely rom India and China
• It has been demonstrated that production to international standards is possible on
our continent
• However, the quality standards to which companies on our continent produce vary
both across dierent countries and regions and also within individual countries

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 69/119
55
OVERVIEW OF PHARMACEUTICAL MANUFACTURING IN AFRICA
• Companies have a wide range o perspectives with regard to upgrading production
standards
• The issue o sub-standard products has grave implications or public health; we
thereore need to take steps to increase quality standards across the board
• Concerns exist as to whether international standard production can be competitive
on our continent
• Research and real world insights show that the economics o pharmaceutical pro-
duction are complex (and go beyond traditional notions o economies o scale) and
are impacted by eciency o production
• Simulation exercises and insights rom leading companies show that high quality
production can be competitive with imports rom India i there is a more level play-
ing eld (rom a policy perspective) and i eciencies in production can be realized
• The level o regulatory oversight in many countries is insucient
• The policy and legislative landscape in most countries is not supportive o local
industry and oten coners a disadvantage versus imports o nished ormulations
rom countries which provide signicant support to their sectors
• The sustainability o high quality local production will benet rom development o
supportive industries and associated inrastructure
• The dierent activities across the manuacturing system require signicant skilled
human resources and know-how but current availability is limited
• Access to nance is a challenge or many industry players given that long term bank
debt o the order o magnitude required is oten not available and the appetite o
equity investors or the sector is somewhat limited
• Intra Arica trade in pharmaceuticals is limited due to various obstacles rom a regu-
latory perspective as well as the reluctance o companies to work together. There is
a substantial opportunity or increased trade in high quality essential medicines and
or this to lead to improved health outcomes
• There are a number o untapped opportunities that could assist the industry and
enable it to become an important public health asset. These include ull utilizationo the TRIPS fexibilities, the output rom the increasing ocus on novel R & D, and
acilitating business linkages and partnerships with multiple aims, including access-
ing new products, investment capital and know-how

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 70/119
56
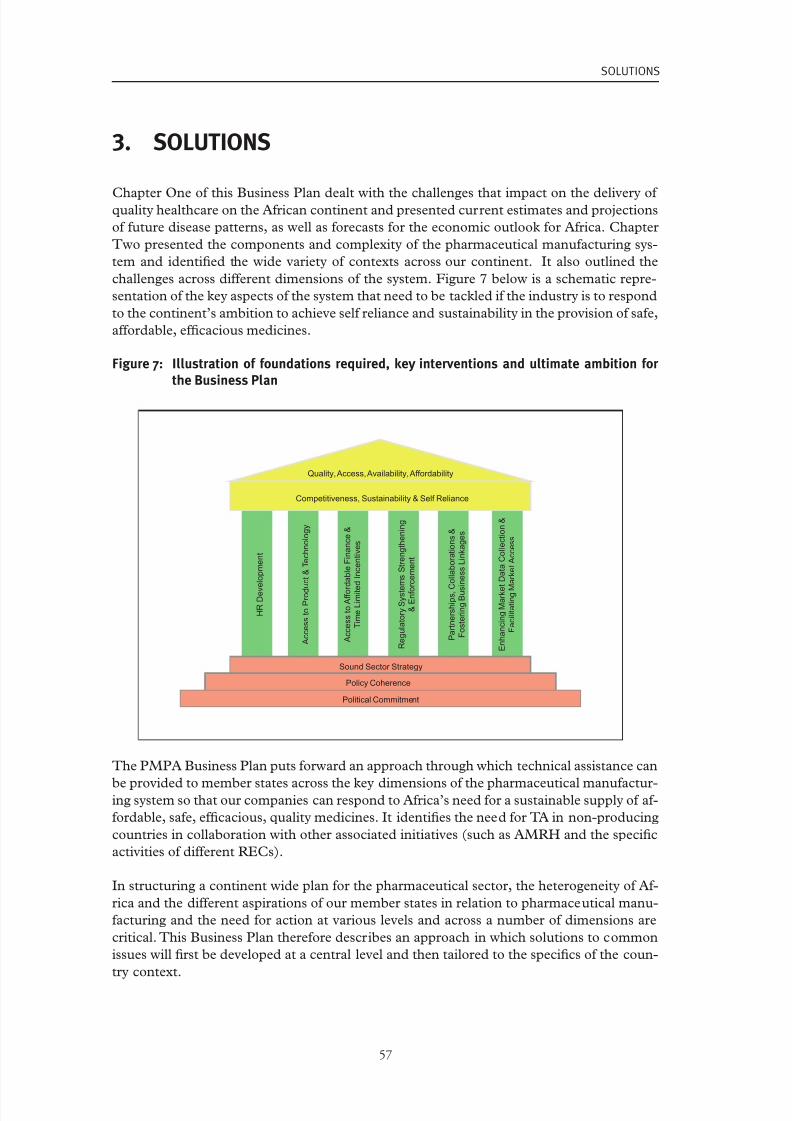
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 71/119
57
SOLUTIONS
3. sOLuTiONs
Chapter One o this Business Plan dealt with the challenges that impact on the delivery o quality healthcare on the Arican continent and presented current estimates and projections
o uture disease patterns, as well as orecasts or the economic outlook or Arica. Chapter
Two presented the components and complexity o the pharmaceutical manuacturing sys-
tem and identied the wide variety o contexts across our continent. It also outlined the
challenges across dierent dimensions o the system. Figure 7 below is a schematic repre-
sentation o the key aspects o the system that need to be tackled i the industry is to respond
to the continent’s ambition to achieve sel reliance and sustainability in the provision o sae,
aordable, ecacious medicines.
7: is ds qd, ky vs d b Bsss P
Policy Coherence
Political Commitment
Sound Sector Strategy
H R
D e v
e l o p m e n t
A c c e s s t o P r o d u c t & T e c h n o l o g y
A c c e s s t o A f f o r
d a b l e F i n a n c e &
T i m e L i m i t e
d I n c e n t i v e s
R e g u l a t o r y S y s t e
m s S t r e n g t h e n i n g
& E n f o
r c e m e n t
P a r t n e r s h i p s , C
o l l a b o r a t i o n s &
F o s t e r i n g B u s
i n e s s L i n k a g e s
E n h a n c i n g M a r k e
t D a t a C o l l e c t i o n &
F a c i l i t a t i n g M
a r k e t A c c e s s
Competitiveness, Sustainability & Self Reliance
Quality, Access, Availability, Affordability
The PMPA Business Plan puts orward an approach through which technical assistance can
be provided to member states across the key dimensions o the pharmaceutical manuactur-ing system so that our companies can respond to Arica’s need or a sustainable supply o a-
ordable, sae, ecacious, quality medicines. It identies the need or TA in non-producing
countries in collaboration with other associated initiatives (such as AMRH and the specic
activities o dierent RECs).
In structuring a continent wide plan or the pharmaceutical sector, the heterogeneity o A-
rica and the dierent aspirations o our member states in relation to pharmaceutical manu-
acturing and the need or action at various levels and across a number o dimensions are
critical. This Business Plan thereore describes an approach in which solutions to common
issues will rst be developed at a central level and then tailored to the specics o the coun-
try context.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 72/119
58
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Implementation o the PMPA will largely take place at the country level although there are
also specic aspects o policy and international development assistance that lend themselves
to action at the level o the RECs and the continent. Critical to success is the recognition
that the pharmaceutical manuacturing system involves a broad array o players and that
strengthening the dierent components requires a similarly broad range o expertise. No
one entity contains the necessary insights, capacity, mandate or skills to address the ull
range o requirements. Consequently, the need or collaboration between dierent parties
is o paramount importance. In view o this, building a consortium o partners is recom-
mended and the AUC will provide the central authority under which these parties can work
together. Further details o the nature o the envisaged consortium and how it will unction
are described in more detail in Chapter Four.
3.1 the generic SolutionS PacKage 8: S d dpd sps sys
Overall Market Context
Regulatory
environment
Government
Policy
Credibility of
Long Term
Commitment
Contribution of Development
Partners
Developments
in Sub-regions
Quality
StandardsKnow How
Skilled
Human
Resources
Infrastructure
e.g.
Bioequivalence
Facilities
Access to
Capital
Cost
Structure of
the Industry
Market
Opportunity
Individual
Company
Characteristics
Key: A B = B is dependent on A
Figure 8 illustrates the interconnectedness o key dimensions and requirements o the man-
uacturing system. It is a schematic simplication that provides some examples o how issues
are connected. The specics in each context dier depending on numerous variables, in-
cluding current status, ambition, level o development and access to capital markets, status
and capacity o the regulator and more.
The generic solutions will constitute a central repository o expertise, knowledge, skills and
capacity which can be accessed and tailored to the various contexts. This section will ocus
on a description o the solutions package, building on existing interventions and exper-tise. In the context o the PMPA, new tools and approaches will be developed that can be

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 73/119
59
SOLUTIONS
implemented with genuine collaboration between partners. The generic solutions package
includes:
• Development o Human Capital
• Development o a GMP road map in conjunction with a risk assessment o the Es-
sential Medicines List
• Insights and guidance on time limited incentive options which governments can em-
ploy to support industry given the specic country context as well as identication
o non-scal support such as acilitating access to know-how
• Recommendations and advocacy to acilitate access to aordable long term invest-
ment capital o sucient magnitude to enable upgrading o acilities to international
standards
• Insights into legislative and policy requirements, tools and options or development
o the local pharmaceutical sector and an understanding o which issues are to be
dealt with at country level and where regional level coordination/negotiation is in-
volved
• Technical assistance to regulators to identiy critical regulatory unctions on which
they should ocus (not just in the context o the PMPA but also in assuring product
quality in the market place) and to develop and implement an organisational devel-
opment plan or achieving these objectives
• A partnership or business linkages platorm which could cover an array o dierent
relationships, including those that provide access to capital and/or technology andknow-how
• Working with centres o excellence to develop ormulations to take advantage o
the TRIPS fexibilities and to assist companies that have reached GMP standards
to access aordable high quality dossiers or established generic products that have
signicant public health importance
• Development o new ormulations or transer to international GMP compliant
manuacturers
• Guidance or strengthening national and regional pharmaceutical manuacturers’
associations
• Developing options and recommendations or improved market data collection and
availability
The range o the solutions package is shown in Figure 9 below and a proposed mechanism
by which a tailored approach or each country context can be developed is also described
below.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 74/119
60
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
9: idv pk ss ddss wd sss vvd
Package of Solutions
Business
Linkages
Platform
Expertise on
time limited
incentives and
policy coherence
Human Resource
Development:
Across actors
TA for strengthening
regulatory
infrastructure
Model GMP road
map and risk
assessment of
EML
Strengthening
Trade Association
as key portal for
dissemination of
expertise to
industry
Best practice
module for
efficient pharma
manufacturing
Assistance to
leading companies
to achieve WHO PQ
Liaison with e.g.
AMRH, ANDI, GF,
CHAI
Develop new formulations for
dissemination to leading
companies (e.g. 2nd line ARVs
and novel FDCs & pediatric
formulations)
Enhanced
market Data
Inputs Manufacturing Distribution Market
Inputs – Material,know how, HR,capital, utilities,service etc.
LocalManufacturers:
• Formulationdevelopment
• Final formulation
• Packaging
• Distribution-array of public & privatesystems
• Distribution -rangeof mechanisms
• National Markets
• Sub-regionalexports
• Donor fundedmarket for pandemics
T
r a d e A s s o c i a t i o n s
E x t er n al A c t or s
National Medicines Regulatory Authorities
Government / Ministries
Pharmaceutical Manufacturing System
3.1.1 Human resource development
One o the most critical aspects o the long term sustainability o the pharmaceutical in-
dustry on our continent is developing the human resources necessary to ull the dierent
unctions within the pharmaceutical manuacturing system. Historically, there have been
many worthy initiatives to develop skills. However, they have been uncoordinated and have
not had the impact they could have had had the HR requirements or dierent aspects o the
system been developed in a deliberate and considered way. The system requires enhanced
human capital in regulatory unctions, technical aspects o manuacturing, business and
management aspects o manuacturing, and in the policy making sphere across dierent
ministries.
There are various mechanisms available or building the skills o those already involved inthe sector and there is a need to increase the availability o skilled proessionals or long term
sustainability to be achieved. In view o this, the human resource development component
o this Business Plan identies both ormal academic training o sector participants at cen-
tres o excellence and a structured set o modules to be made available to industry actors
at individual country and/or country cluster levels. The importance o the country/cluster
level training cannot be overestimated. The progress o the industry requires not only the
dry technical skills involved but also a shit in industry culture across the system such that
quality and eciency become concepts embedded within the psyche o all practitioners.
At the enterprise level, those companies that have reached international standards have
repeatedly emphasized the need to adjust the internal culture o the company and haveutilized many mechanisms to do this. Experts in ecient manuacturing also emphasize

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 75/119
61
SOLUTIONS
the need or eciency to be part o a company’s core culture or continuing improvements
which lead to evermore competitive production. Best practice in terms o enterprise level
training programmes will be developed and disseminated to companies through trade as-
sociations. Companies themselves will be responsible or taking advantage o such materials
but sector level training will also be conducted as part o the PMPA. This will orm a basis
rom which enterprise level initiatives can be designed and implemented.
It is also necessary to recognize that, or the sector to embark on a new trajectory, we will
need to augment our current human resources through accessing know-how in the short to
medium term via various mechanisms. For example, the Partnership and Business Linkages
Platorm described later would provide a mechanism through which companies could en-
gage partners to assist in areas such as plant design. There are many skilled people in other
parts o the world whose expertise could be brought in and those in the Diaspora could be
encouraged to return.
For example, there are thousands o highly skilled pharmaceutical personnel currently un-employed ollowing the large scale retrenchments by multinational pharmaceutical com-
panies during the global recession. Pharmalot estimates the number o people retrenched
at 19,076 in 2011, 53,636 in 2010, 61,109 in 2009, and 43,014 in 2008. Means by which
governments could consider acilitating quick access to such expertise include increasing
the quota o expatriate working visas or pharmaceutical companies.
The specialized skills sets required to support local manuacturing are described in Chapter
Two where there is also a non-exhaustive list o organisations involved in training or the
pharmaceutical sector. The AUC, with the assistance o UNIDO, has had initial discussions
with WHO, USP, and the Saint Luke Foundation/Kilimanjaro School o Pharmacy about
building on their ongoing activities to accelerate human resource development or the in-dustry. Although these entities can assist in the development o human resources already
involved in the manuacturing system, the long term supply o skilled graduates who will
be vital or sustainability and sel reliance in the production o high quality medicines also
needs urther development. In view o this, the training curricula o schools o pharmacy
should be revised so that they incorporate industrial training although this is outside the
specic mandate o the PMPA. However, the technical partnership envisaged in the Plan
would make experts available to assist those institutions o higher learning that are inter-
ested in revising their curricula.
There is also a need to develop urther business skills, business culture, and expertise in
manuacturing eciency i the sector is to become sustainable in the long term. Thereore,
as well as developing the technical human resources or regulation and production, the con-sortium will also build on initial insights and establish training modules to provide materials
and guidance on which companies can draw to improve their operations and develop busi-
ness models and structures that are attractive to investors and increasingly competitive in
the medium term.
As already pointed out, developing human resources requires dierent models to develop a
strong basis o technical skills and to ensure that this knowledge is then reinorced through
continual learning and dissemination to other industry participants. This Business Plan will
seek to provide a comprehensive education syllabus through centres o excellence and ongo-
ing training at sector level. It will also be necessary or individual companies to recognize the
importance o ongoing training and corporate culture development and to take responsibil-ity or such activities (with sector level guidance rom the PMPA).

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 76/119
62
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Technical manuacturing, regulatory and policy skills
Human resource development will involve dierent levels o intervention by the consortium
engaged to do the detailed design and implementation o this Business Plan. At a technical
level, training at academic institutions will include:
• A comprehensive syllabus o short term courses or current employees and those
aspiring to join the sector. This could initially be conducted at the Saint Luke Foun-
dation (with its partners) and then be subject to expanded roll out as the model is
extended (see above).The syllabus would include documentation (drug product/
substance, mock drug master le compilation), ormulation, design, excipients, coat-
ing, bioequivalence, method validation, equipment calibration, ling with the FDA/
WHO-PQ (SRAs). Muhimibili University is already oering short courses on these
modules as well as courses on validation and qualication, granulation, tableting and
coating; quality control o medicines; and coating and sustained release ormulations
• A syllabus o pharma-specic long term courses or regulators and industry. The
Saint Luke Foundation/Purdue and Howard universities collaboration oers a two
year Industrial Pharmacy Advanced Training Programme which will be expanded to
other regions o our continent. The ocus includes drug development and regulatory
quality compliance, drug manuacturing process (GMP), regulatory documents and
generic drug approval submissions, and drug discovery. The training is oered in the
Industrial Pharmacy Teaching Unit which boasts a ully equipped and GMP com-
pliant production line with 50kg batch size equipment. This programme is based on
Purdue University’s leading Industrial and Physical Pharmacy Programme
These training courses will be supplemented with the running o in-country/country cluster
courses made available to various industry actors. It is imperative that technical knowledge
rom academic courses is built upon and that there is a structured approach to developing
the broad understanding o the range o requirements or high quality production. Equally
important is the ability and awareness o all actors o the need to ull their particular op-
erational unction according to these standards. These in-country/country cluster courses
will include:
• A structured approach to building knowledge o GMP and associated processes,
practices and requirements
• Specic training aimed at changing the management culture o companies and o-
cusing on quality aspects. As with other courses, this training will be conducted ata sector level although companies requiring specic in-house training will be able
to access the AUC panel o vetted experts independently. Mechanisms or assisting
countries with limited numbers o manuacturers wishing to access such training
will need to be established, or example, via regional cluster approaches. However,
the PMPA will seek to develop materials to assist companies in their internal ongo-
ing training programmes around GMP, culture change and the importance o qual-
ity to the business
• Specic training or NMRAs over and above academic courses will also be necessary
to enable regulators to build on this knowledge and current expertise to enhance
their ability to oversee the market (dependent on inrastructure as well as human re-
sources – see below). WHO and USP activities in this space have already been men-

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 77/119
63
SOLUTIONS
tioned. However, it is recognized that these initiatives need to be enhanced and that
development o regulatory skills would benet rom more additional and perhaps
more extensive programmes o support. USP and WAHO have, or example, pro-
posed a ‘training o trainers’ approach or the ECOWAS region, where experienced
regulators who have retired could mentor individuals and transer their knowledge to
the next generation who should then act as agents or change within their NMRAs.
Such a concept could be developed and rolled out to other RECs. Furthermore,
many stringent regulatory authorities and related organisations oer training pro-
grammes or regulators rom developing countries. The PMPA will seek coopera-
tion with organisations such as the International Conerence on Harmonisation o
Technical Requirements or Registration o Pharmaceuticals or Human Use (ICH),
the U.S. Food and Drug Administration (FDA), the European Medicines Agency
(EMA) and WHO with a view to oering continuous development programmes or
participating Arican NMRAs. Any initiatives in this area will be coordinated with
the ongoing approach to training o regulators that is being developed by the AMRH
initiative
• Training or policy makers is a key area that needs to be addressed head on to in-
crease the industry specic knowledge o the technocrats tasked with ormulating and
implementing policies impacting on the pharmaceutical industry. Given the broad ar-
ray o ministries involved and the number o sta who will have input, whilst discrete
external courses may be appropriate or senior government ocials, it is anticipated
that a series o workshops and seminars to inorm policy makers o the reality o the
sector, its complexity, its potential or public health benets and its need or cohesive
policy rameworks will be oered at country level. Some leading Arican universities
have been approached and have already indicated a willingness to design and oer the
required training. The AUC will also approach other international training institutions
and development partners with the requisite know-how to develop and oer such a
programme and will endeavour to twin them with the interested Arican institutions
• Short term courses or engineering teams, artisans and machine operators. It has be-
come clear through interactions with various industry stakeholders that a key challenge
conronting manuacturers relates to the shortage o the requisite skills and experience
in tooling and abrication as well as in optimal plant maintenance and operations. The
AUC thereore proposes to start a series o short term courses or technical teams in
industry in order to disseminate international best practice and to equip companies to
be able to service, maintain and repair their own equipment. This is particularly urgent
since one o the causes o long downtimes is equipment breakdown which necessitates
the importation o skills, normally rom abroad. This is a major disruption in continu-ous plant operations and is costly or many cash strapped companies
Business skills or the pharmaceutical industry
The development and sustainability o the pharmaceutical sector is dependent not only
on the technical skills associated with manuacturing but also the business skills o the
entrepreneurs and corporate managers involved. Competitiveness is not only a unction o
a number o structural aspects o the industry or the development o an enabling environ-
ment rom a policy, regulatory and legislative perspective. It is also dependent on the ability
o entrepreneurs and corporate managers to take advantage o opportunities arising and toachieve their business objectives. The inherent skills o successul entrepreneurs, such as
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 78/119
64
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
energy, dynamism, and risk taking should not be underestimated. However, these skills can
be urther enhanced through the teaching o some key dimensions o doing business in the
pharmaceutical sector.
There is potential or establishing industry training programmes at institutions o learning
which, or example, could replicate the MBA in Pharmaceutical Management oered by
institutions like NIPER in India. The need or such programmes has been endorsed by vari-
ous pharma proessionals who identied the ollowing courses as relevant:
• Accounting and Financial Management
• Pharmaceutical Business Environment
• Business Law
•
Production and Operations Management in Pharma
• Strategic Management in Pharmaceuticals
• Pharmaceutical Sales Management
• Marketing Management
• Brand Management in Pharmaceuticals
• Logistics and Supply Chain Management or Pharmaceuticals
• Corporate Governance and Board Leadership
It should also be recognized that many entrepreneurs and corporate managers will not have
the time to participate in such extensive training. Nonetheless, the need or specic aspects
o business management to be disseminated to the industry is urgent since the time needed
or moving rom initial planning to mobilizing investment and to upgrading established
plants or building new plants is substantial. In view o this and to enable companies to take
action rapidly, training in the key skills required or the sector’s development will be pro-
vided, as requested, through entities such as trade associations.
A key component o this training will ocus on changing the prevailing business culture and
governance practices in the industry. The management and governance culture o Arican
pharmaceutical companies has consistently been identied as one o the major weaknesseso the industry and is a key reason why investors are unwilling to invest in the industry. This
is hardly surprising given that the investment community is understandably not keen to in-
vest in businesses where its views may not be heard and where record keeping, governance
structures and roles and responsibilities are not well dened. Thus it is imperative to oer
a number o modules or executive training and or building the requisite general manage-
ment skills and expertise.
Improving competitiveness is another key area or business managers. It is clear that achiev-
ing eciencies requires incorporation o eciency into the corporate culture but managers
need to be given the tools with which to identiy the opportunity and to eect change within
their organisations.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 79/119
65
SOLUTIONS
3.1.2 GMP road map and risk assessment of the EML
The ultimate objective o the PMPA is that all production in Arica should adhere to inter-
national GMP standards. There are a number o guidelines set out by dierent regulatorsand agencies to dene what constitutes GMP but the PMPA recommends that WHO GMP,
as established in the WHO compendium on quality assurance 2006, should be the target to
which all countries aspire.
Where companies are developing new production acilities, it is recommended that coun-
tries immediately require WHO GMP standards but, where there already is an established
pharmaceutical sector, a trajectory towards GMP requirements needs to be established.
In an ideal world, all companies would immediately upgrade their standards to GMP but
this is not practical as substantial expertise is required to address all the aspects involved.
Moreover, signicant investment is oten needed, time is required to adjust the corporate
culture towards one that has quality as a central tenet, and processes and procedures need
to be dened and validated.
These and other actors mean that a pragmatic approach is warranted since most companies
will need to make improvements in order to reach GMP standard and they will require vari-
ous orms o assistance to do this (see section on other solutions involving both technical
support and incentives). Firms also need time to implement change whilst continuing to do
business. By the same token, most regulators will also have to increase their capacity and
capabilities i GMP is to be enorced widely. This, again, will take time and resources.
Recognizing this situation, the Business Plan recommends the establishment o a ‘GMP
road map’. Initial work with USP has resulted in the development o a prototype assessment
tool that seeks to quantiy the level o a company’s adherence to GMP. This could be usedunder the authority o the NMRA as part o country level PMPA implementation to assess
the level o compliance with GMP o manuacturers operating in a country. The purpose o
the assessment would be to establish a baseline rom which a GMP road map or the sector
can be established. During the set up phase, the AUC, in conjunction with core partners,
will develop a generic road map.
The objective or the uture is that all companies should be GMP compliant across all prod-
uct categories. However, as already pointed out, this is neither possible nor practical right
now. The implications o sub-standard production vary depending on the product type in
terms o implications or health i contaminated, i products are not eective, or i products
were to be mislabelled. Thereore, in the interim, it is proposed that those companies that
are not at GMP levels should be restricted to manuacturing only products that are deemed
to pose a minimal risk in the event o their quality being compromised. To identiy products
that would pose minimal risk, a technical review o the WHO Essential Medicines List will
be conducted (initial discussions with WHO regarding this undertaking have taken place).
Such a risk assessment would be used as a basis or NMRAs to determine which products
could be produced by which companies (it may be that there would be a number o tiers
below the ully GMP compliant status).
Despite the PMPA recommending a pragmatic approach to improving standards over time,
the implications o quality should not be underestimated and the GMP road map will in-
clude recommended prerequisites or certain product types (even in the minimal risk cat-
egory) which must be in place beore production can start or continue. For example, pro-duction o syrups should not be allowed without proper water treatment plants in place. The

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 80/119
66
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
risk o anaphylactic shock in people allergic to penicillin means that beta lactam production
should always be in a separate acility to other products. Further suggested prerequisites will
be recommended as part o the road map.
In summary, where there is an established industry with varied production standards, the
Business Plan espouses a pragmatic approach to improving quality standards with the ul-
timate goal being international GMP standards across the board. This requires a holistic
approach where regulatory capacity development, human resource development, access to
know-how and incentives/support to industry are coordinated to enable and require compa-
nies to adhere to a GMP road map which will:
• Consist o a series o milestones setting out specic components o GMP that com-
panies would need to have in place by a certain point in time. This would be leading
towards a point in the uture (probably established by the NMRA ollowing consul-
tations) where all components o GMP would need to be in place
• Need to be pragmatic but also identiy critical issues o GMP that should be ad-
dressed as an imperative at the outset
• Dierentiate between the dierent GMP requirements or dierent dosage orms
and certain product categories
• Need to be pragmatic, as certain aspects will take some time to implement (e.g.
where construction and/or capital mobilization is required)
• Be implemented in conjunction with a risk assessment o the EML whereby com-
panies operating below GMP standards would be limited to production o those
products that represent the minimum risk
3.1.3 Insights and guidance on time limited incentives to support industry
A key objective o the PMPA is that international standard production o essential medi-
cines in Arica should be sustainable. Some commentators have suggested that sustainability
in terms o competitiveness can only be achieved with large scale plants that are able to
‘achieve economies o scale’. However, the economics o production o nal ormulations
are much more complex, with many actors to consider.
As pointed out in Chapter Two, UNIDO has commissioned various pieces o research into
the economics o production or nal ormulations. They indicate that, with appropriatesupport and changes in business practices, local manuacturing o high quality products can
be competitive with Asian companies.
Long term sustainability o high quality production is possible on the continent and will be
a unction both o how well companies are run and o progress on a number o ronts (such
as harmonization o registration which is being pursued by AMRH). The human resource
development solutions outlined in this Business Plan provide assistance to companies on
how to run plants eciently and achieve competitiveness. However, time limited incentives
are required to assist companies to make the necessary investments and to protect and sup-
port those that have already done so.
The work being done on the economics o pharmaceutical production, coupled with in-sights as to the current status o production, the investment requirements or upgrades and
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 81/119
67
SOLUTIONS
the nature o the pharmaceutical industry provide the basis or advising governments on ap-
propriate time limited incentives. These will support the industry as it learns to be competi-
tive and strives to produce to international standards. The recommendations on a package
o incentives will be dependent on the specic country context since numerous variables will
need to be taken into account, including:
• Interest rates
• Liquidity o equity markets
• Currency volatility
• Current status o the industry in terms o investment requirements
• General and industry specic industrial policy tools and incentives that are already
in place (e.g. Special Economic Zones, export incentives, restricted lists, sot loans,
etc.)
• The specics o the tax regime
• Current production capacity and standards in the country
• The specics o the GMP road map as determined by the NMRA (with advice rom
the PMPA)
• Public health priorities
These and other variables will inorm the design o the package o incentives. Experience
rom within Arica, as well as other geographies and industries, provides examples o mecha-
nisms that can be utilized to provide scal support to manuacturers. They can be largely
divided into two categories: direct support and protective measures. Mechanisms or provi-
sion o direct support could include:
• Interest subsidies
• Working capital credits
• Underwriting Letters o Credit to improve the credit terms that companies can ob-
tain rom suppliers
• Zero rating/exemption or taxes/ taris on imported inputs or the industry
• Special depreciation provisions (e.g. in India, companies could allow or 150% de-
preciation o capital investments)
• Utility subsidies
• Subsidies to support training
• Export incentives
Protectionist approaches could include:

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 82/119
68
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
• Increased taris on imported nished products
• Restricted lists
• Marginal preerence or procurement o locally produced products
The likelihood is that a combination o dierent tools should be incorporated in an incen-
tives package and, as mentioned, the specics will inevitably vary rom country to country.
In advising on an incentives package, we will be mindul o certain considerations. These
include:
• Depending on the status o the industry, protectionist policies could be detrimental
to public health, or example, i they lead to price increases (e.g. through increased
taris) or i the local industry is not developed to the point where competition keeps
prices down i a restricted list is introduced
• The incentives package will need to recognize the dierent business models and
capital structures that exist and that are desirable or long term sustainability (or ex-
ample, interest subsidies alone would avour debt nanced operations when a blend
o debt and equity may be more appropriate)
• The incentives should keep in mind the medium term goal o stand-alone competi-
tiveness and should seek to encourage ecient production (India had price controls
in place so that companies had to be competitive rom the start but received support
in other orms)
• The incentives are intended to be time limited in duration
• Manuacturers are all starting rom dierent points and those that have already made
investments should not be penalized. They should receive some orm o protection in
the short term
• Any measures should be developed to work within the ramework o existing indus-
trial policy incentives and mechanisms
• The incentive package should not be overly complicated but should recognize the
complexity o the situation
• Measures should be coordinated with the GMP road map (and vice versa)
• The incentives will need to consider oreign investment and joint ventures as mecha-
nisms or sourcing investment and accessing technology as well as the degree to
which they should be encouraged through the package
• The incentives should not be token gestures and (based on the evidence) should
represent meaningul and appropriate support levels
• The incentives should not represent an unnecessary subsidy to the private sector
• It will be necessary to refect on the possible “unoreseen” consequences and per-
verse incentives that could result
• Finally, it should be recognized that incentives cannot resolve all things or all people.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 83/119
69
SOLUTIONS
The importance o business skills, energy, initiative, appetite or risk, and ability to
adjust o entrepreneurs and corporate managers should not be underestimated, un-
dermined or devalued. Further, these attributes need to be enhanced (as described
above) in order to achieve long term sustainable manuacturing across our continent
3.1.4 Insights and guidance on legislative and policy considerations
Policy incoherence has been identied as a major impediment to the development o the
pharmaceutical sector. Later in this chapter, we present a proposed approach or developing
country specic plans or the sector. The consultative approach across stakeholders and di-
agnosis o the policy and legislative landscape, ollowed by development o a shared strategy,
are the means by which incoherence can be identied and resolved.
3.1.5 Technical assistance to regulators
Chapter Two identied the critical role o the regulator in the pharmaceutical manuactur-ing system and pointed to evidence rom a recent WHO study that shows that many o our
NMRAs (or equivalents) are not able to carry out the necessary unctions. The human re-
source development section o this Business Plan identies means by which human capacity
can be developed and more skills brought into the rame. However, as well as human capital
requirements, NMRAs require the inrastructure to ull their mandate to protect the public
and ensure that medicines on the market are quality assured, sae and ecacious.
Thereore, partners within the consortium will oer technical assistance to produce organi-
zational development plans, including the necessary regulatory inrastructure, and to guide
their implementation. This assistance will be provided to both producing and non-produc-
ing countries (within the context o ongoing AMRH activities) in order that all nation stateshave the opportunity to benet rom local sources o high quality production o aordable
essential medicines.
The specic unctionalities on which the regulator in each country should ocus will be de-
pendent on manuacturing aspirations, level o cooperation with other NMRAs, and critical
weaknesses in current systems directly relating to protection o public health. There is substan-
tial expertise within WHO and USP that can be brought to bear and the University o Ghana
Medical School (designated a WHO Collaborating Centre or Advocacy and Training in Phar-
macovigilance (CCATP) in 2010) has developed expertise and a pharmaco-vigilance ‘tool kit’
which could be utilized by the PMPA. However, technical assistance can only deliver progress
in this area i there is high level political commitment to invest in the regulatory authorities.
Accessing unding or such institutional development programmes will be the responsibil-
ity o member states. However, development banks such as the World Bank have inormally
indicated that there would be strong interest in requests rom governments or loans, sot
loans and grants (depending on country status and other priorities) or investment in this
critical public health unction.
3.1.6 Assistance to leading companies
The long term sustainability o treatment programmes or the pandemic diseases will ben-
et rom establishing high quality WHO certied production. There are three companies in
SSA outside South Arica that have reached this standard and a number o others who areworking hard towards this (and other stringent regulatory certication).

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 84/119
70
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Fundamentally, this Business Plan adopts a philosophy whereby the whole sector should be
supported and required to improve GMP standards and advocates achieving this through
building capacity across the manuacturing system. However, there is a public health neces-
sity to rapidly increase local production o international standard drugs or the pandemic
diseases. Consequently, the Plan includes support to those leading companies that have
already taken bold steps towards achieving international GMP standards. Thereore, some
plant level support (based on application to and approval rom the PMPA) will be appropri-
ate to assist those that are close to prequalication to reach the requisite standard or prod-
ucts included on the WHO prequalication list. Support will also be oered to those who
already have prequalied products so that they can increase their portolio and access new
markets. Achieving WHO approval alone does not guarantee that products will be procured
so, in addition to assistance on issues such as dossier preparation, these companies would
warrant bespoke plant level assistance to improve their production eciencies. This would
enable them in the short term to be competitive with imports.
Other aspects o the solutions package also provide opportunities or leading companies thathave attained WHO standards, including access to new ormulations developed under the
PMPA and the business linkages platorm, under which advanced companies are more likely
to be interesting partners or leading international players.
3.1.7 New formulations
Initial discussions have been held with Arican (e.g. KEMRI and MUHAS) as well as inter-
national (Purdue and Howard) universities and centres o excellence regarding their interest
in developing ormulations or dissemination through the PMPA to companies that achieve
WHO GMP standards. Initial interest has been expressed and a model by which such work
will be unded and the priorities or ormulation development established is under develop-ment. It is suggested that the PMPA could provide seed unding or the development o
initial ormulations and that these would be disseminated to leading companies using a cost
recovery model.
This component o the solutions package serves to address some critical weaknesses in the
short to medium term, including:
• Expanding the product portolios o leading companies on the continent to include
more than just basic ormulations o old products. This will be an important public
health contribution
• Developing ormulations and then spreading the cost across a range o companies(through charging a ee to each refecting only a proportion o the real cost) would
be a means by which companies could aord to expand their portolios
• New ormulations or Arica are required in some critical areas. Ongoing work by
various Product Development Partnerships is looking to address this but the ANDI
centres o excellence could coordinate with these other entities to develop, or ex-
ample, paediatric ACT ormulations and novel FDCs or adults and children in the
realm o HIV
• Second and third line HIV therapy is largely still under patent protection and pro-
hibitively expensive or many programmes and countries. I TRIPS fexibilities are
properly incorporated in our legislation, then we could utilize these centres o excel-
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 85/119
71
SOLUTIONS
lence to reverse engineer these products and make the technology available to lead-
ing Arican manuacturers. They would then be able to provide such products to the
Least Developed Countries on our continent
There is thus a need to assist industry to access products and ull common technical docu-
ment (CTD) ormat dossiers and to make these high quality dossiers aordable to industry
through a ‘shared cost’ model. The AUC does not intend to provide this service indenitely.
It regards this as an urgent and time limited intervention that will taper o within ve to
ten years as companies acquire the capability and the nancial resources needed to develop
their own products.
It is critical to highlight that access to developed technology will be conned to companies
who have attained international GMP and will be used as a motivation or companies to
work towards international GMP certication. The ollowing key activities will be involved:
• Selecting products or development based on essential medicines lists and secondline antiretroviral medicines
• Signing product and technology development agreements
• Reverse engineering products and working with partners to compile CTD ormat
dossiers
• Setting up technology transer teams and recruiting experts
• Transerring technology to GMP compliant companies
To acilitate commercialisation o the technologies developed by the technology transercentres, licensing agreements will be directly negotiated with various IPR holders or the is-
sue o voluntary licences or international GMP compliant Arican manuacturers. Further,
given that technology transer is not a straightorward matter, it is proposed that, on comple-
tion o the process and ormulation development in various laboratories, the process should
then be transerred to Muhimbili University’s PharmD R & D Lab, whose laboratory-scale
production capacity is up to 5 kg. Ater this, the process would then be transerred to the
Saint Luke Foundation which has a pilot plant with a production scale o 50kg – sucient
to allow bridging rom laboratory production to commercial scale. Where such technology
transer is conducted, it will be necessary or a tech transer team to be established to ensure
that the highly involved and complex process is conducted correctly and that recipient com-
panies receive the appropriate training o production sta.
3.1.8 Partnership and Business Linkages Platform
Chapter Two describes the underutilized opportunities or business relationships and vari-
ous types o collaboration that could strengthen local production. There are a myriad o di-
erent relationships that could be entered into and the Business Plan suggests a platorm via
which these can be brokered. The opportunities or cooperation exist at country and region-
al levels as well as or intercontinental arrangements to be established to the mutual benet
o both/all parties. Country level collaboration between manuacturers can perhaps best be
acilitated through the strengthening o trade associations. Other regional and international
linkages could be acilitated through a Partnership and Business Linkages Platorm.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 86/119
72
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
There is evidence as to the mutual benet that various types o relationship could deliver
and o the need or our companies to access various inputs, including know-how, capital,
products and technology. Despite the evident need and the latent interest in this, the num-
ber o relationships that have materialized is limited and the degree to which companies can
access investment (through equity joint ventures, proessional investors, or bank debt) and
know-how (through collaboration or on a ee or service basis) has been reported as a key
challenge.
We recommend that an experienced lie sciences investment and business development pro-
essional be recruited with a dedicated role to manage the various activities that would
constitute the Partnership and Business Linkages Platorm. The Platorm would use various
modalities to acilitate partnerships and business arrangements covering the diverse range
o potential structures and participants. They include:
• A web portal to include corporate proles, details o a pool o experts identied or
various orms o assistance that companies might require, dissemination o inorma-tion about upcoming industry conerences, and publication o materials or in-house
corporate development programmes.
• Active monitoring and engagement in the fow o business deals in the pharmaceuti-
cal sector. This could be achieved through attending conerences and building an
extensive network across geographies and types o institution (e.g. research entities,
manuacturers, service providers, equipment manuacturers, etc.) with the intention
o identiying opportunities or collaboration and promoting opportunities arising
out o pharmaceutical manuacturing in Arica.
• In coordination with consortium partners, monitoring the progress made by the sec-
tor in mobilizing investment and accessing technology, and identiying opportunities
or evolution to the action plan.
• Working with international unding entities such as the Investment Fund or Health
in Arica (IFHA), the IFC’s Health or Arica Fund and the Arican Development
Bank to mobilize enthusiasm or the sector and to encourage adjustments in invest-
ment requirements such as the IFC’s prerequisite or WHO prequalication beore
investing in Arican manuacturers.
• Holding two matchmaking events over the ve year period to provide opportunities
or stakeholders to meet and establish initial interest in working together
• Working with strategy development and implementation processes at country level
to identiy opportunities and recommend approaches designed to acilitate collabo-
ration and to diagnose the investment climate and recommend strategy components
that could improve access to investment (e.g. specic aspects o the incentives pack-
age that investors would need to see in place)

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 87/119
73
SOLUTIONS
3.1.9 Strengthening industry trade associations
Most in-country interventions and inormation dissemination workshops and training ses-
sions will be organized and delivered through large group settings. The AUC and partnerswill prioritise the strengthening o trade associations both at a regional and country level
since they will be valuable partners in the organization o such training programmes and as
inormation dissemination portals.
UNIDO has signicant experience in supporting the ormation and development o trade
associations both in the pharmaceutical sphere and in the wider industrial context. For ex-
ample, it supported the oundation o the Southern Arican Generic Medicines Association
(SAGMA) and has worked closely with the West Arican Pharmaceutical Manuacturers
Association (WAPMA), the Pharmaceutical Manuacturers’ Association o Ghana (PMAG)
and the Federation o Kenyan Pharmaceutical Manuacturers (FKPM). Knowledge gained
through this experience, together with its institutional strengthening skills, will be brought to
bear in assisting the strengthening o industry associations under the auspices o the PMPA.
Trade associations can provide valuable services to their members and can act as a mouth-
piece or the industry to raise awareness o the challenges that exist or areas where interven-
tion by government is needed. The associations are also an important means or dissemi-
nation o best practice. However, it should be recognized that associations are de acto a
collaboration o competitors (creating some internal tensions) and that their job is to rep-
resent the interests o their members. It will thereore be important that, whilst the PMPA
should seek to assist such associations to develop capacity, their undamental mandate
means that, even when strengthened, they will remain independent rom the PMPA core
partners. The PMPA is not a mechanism or promoting the wishes o the private sector but
it can perorm an honest broker unction between parties across public and private sectors.
3.1.10 Indirect impact of the PMPA solutions package and opportunities for col-
laboration
As repeatedly emphasized in this Business Plan, the pharmaceutical manuacturing system
is complex and interventions at a number o key points are recommended. However, this
Plan cannot and should not attempt to resolve every aspect o the system directly. As de-
scribed, access to capital and strong related and supporting industries are also imperative to
both the short term development o the sector and its long term sustainability.
Certain specic initiatives have been articulated to address these particular aspects. For
example, the provision o time limited support, which may include interest subsidies, is
intended to enhance access to capital. Similarly, support to artisans and other relevant ac-
tors is proposed under the training programme. However, these catalytic initiatives need to
be just that - catalytic - with the intention o the plan being to provide the opportunity or
governments to address the key dimensions o the manuacturing system and, in doing so,
to create new enthusiasm or the sector rom associated actors. For example, investors have
expressed caution about the sector or a variety o reasons that credible commitment rom
government in this area (or example, regulatory oversight) would help to address. Those
involved in supportive industries may also see new opportunities or establishing capacity on
our continent (e.g. in Tunisia, it is viable or international equipment suppliers to maintain
oces or servicing their manuacturing equipment given the density o pharmaceutical
manuacturers and the advanced nature o the machinery that is used across the board).

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 88/119
74
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Other areas where the PMPA does not look or direct intervention are where there are ongo-
ing initiatives that will provide valuable opportunities or the manuacturing systems on the
continent. For example, ANDI has a network o 32 centres o excellence (and is establishing
more), some o which already have the competencies and requisite skills to become ully
fedged bioequivalence study centres. Through the business linkages activities, and as new
ormulations are developed under the PMPA, these centres will be engaged or carrying out
the clinical component o product development activities. The centres will also be able to
assist regulatory authorities with market surveillance activities where these are weak.
The need or less ragmented markets to enable manuacturers to achieve eciencies o
production is a vital long term requirement or sustainable local production. The AMRH
work being conducted under the overall ramework o the PMPA will be supported, where
necessary, under the activities described in this Business Plan. However, the registration
and regulatory harmonization components are the mandate o the established parties inthis initiative and whilst (as requested) the activities described in this Business Plan can
help capacity building at individual regulatory authorities, the Plan deers to AMRH and its
partners in the realm o regional integration.
Another area where increased enthusiasm or the sector should provide a virtuous eect
is market data. This Business Plan will endeavour to explore means by which data can be
collected and disseminated. However, this is an area where substantial expertise is required
and, in the developed world, the unction is generally conducted by private sector service
providers. The implementation o the PMPA and the growing interest in our markets rom
overseas players may well create a market opportunity or inormation providers. In view
o this, the PMPA will explore interest amongst the likes o IMS Health (through the IMSInstitute) as to whether a viable business case can be made or building a platorm or data
collection and dissemination.
3.1.11 Country level implementation
The previous sections have described the generic solutions to be developed under the PMPA.
The specics o how these are implemented at country level will vary depending on the in-
dividual country context and its ambitions and aspirations. Thereore, as well as providing
a repository o expertise, the Business Plan proposes a process that can assist country level
stakeholders to establish their nation’s ambitions or pharmaceutical manuacturing and
to develop a bespoke strategy and implementation plan or realizing them. Further, once
an implementation plan has been developed, the PMPA will (as required) escort the actual
execution o the dierent components o the Plan through accessing the requisite expertise
and coordinating the implementation in collaboration with national level stakeholders. De-
veloping national level strategies requires processes to be adopted so that the complex array
o considerations and perspectives can be incorporated. Whilst the specics will vary, an
indicative approach that could be adopted at the country level is described here.
In Chapter Two, a schematic representation shows the complexity o the pharmaceutical
manuacturing ‘system’ and identies the roles o the many types o stakeholders involved.
Historically, it has been suggested that there are mutually exclusive, non-compatible, per-
spectives amongst this diverse range o actors. However, experience suggests that, through
a consultative process and a thorough diagnosis o the specic objectives, mandates andchallenges aced by individual actors, it is possible to develop a comprehensive strategy that

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 89/119
75
SOLUTIONS
can be endorsed by all parties. Experience also suggests that high level political engagement
rom the outset is critical i rapid progress is to be made rom the time o initial engagement
between parties through to strategy development and implementation.
The nature o the process or designing and implementing a strategy at national level is
thereore a critical part o the ‘package’ o solutions. As with all other areas o the PMPA, the
specics will depend on the context. However, an indicative approach is described below.
Stage 1: Project set up
On receipt o an invitation rom the government o a country, PMPA representatives will have
initial discussions with the key stakeholders to determine an agreed approach or diagnosis,
consultation and strategy development. The key stakeholders are likely to include the Minis-
tries o Health, Industry, and Finance (or their equivalents), the NMRAs, academia, and indus-
try representatives. The discussions would likely include the establishment o a working group
with high level representation rom the key stakeholders. This group would provide oversight
or the development o the strategy and its implementation and would also establish the activi-
ties to be conducted and milestones to be set and draw up a timeline or their completion.
The stages now outlined would be dependent on these initial discussions, so, once again,
they should be seen as indicative rather than cast in stone.
Stage 2: Situational analysis
A situational analysis will involve collection o hard data on, or example:
• Health budgets
• Pharmaceutical expenditure
• Current industrial policy rameworks and industry development support, as well as
other pertinent policies and legislation such as IPR and national procurement rules
• Taxes and taris applicable to the industry
• Imports and exports
• Range o products produced
• Access to capital considerations (such as interest rates, currency volatility, equity
markets)
It will also include a qualitative component in which the dierent stakeholders (including
entities such as civil society and the donor community) are engaged to garner their perspec-
tives on the pharmaceutical sector, including the major challenges aced.
Consequently, the situational analysis will capture key hard data but, more importantly, will
be a consultative process whereby the dierent perspectives and the consequent implica-
tions and concerns about strategic direction are captured at the outset.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 90/119
76
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
In collaboration with the working group, PMPA representatives would produce a report on
the ndings to be submitted to key stakeholders or consideration prior to a ‘round table’
where stakeholders would discuss the ndings and initial proposals on ways orward.
Stage 3: Detailed strategy design
Subject to the conclusions o the round table, the expertise outlined in the PMPA ‘solu-
tions package’ would be mobilized to work with specic stakeholders to tailor a package
o interventions based on the strategic vision articulated by the round table. The detailed
work (such as developing a package o incentives or determining the needs o the regulator
regarding its capacity) will need to be conducted separately. However, a key unction o the
PMPA representative will be to ensure that the specic deliberations are put together in a
manner that ensures that they are mutually reinorcing and represent a coherent holistic ap-
proach to developing the sector.
For example, detailed work on industry incentives that may need to take place with the
Ministries o Finance and Industry should be coordinated with the detailed work with the
regulator and industry on establishing a GMP road map. The incentives (and other aspects
o the strategy) will need to be aligned with the requirements o the road map. This is the
case both rom a timing perspective and in terms o reinorcing the regulatory requirements
whereby incentives may be triggered upon achieving certain milestones. Unless this is done,
progress at the implementation stage is likely to be highly problematic.
Where there is an established industry, subject to approval by the regulator and other gov-
ernment bodies, a diagnostic (as opposed to regulatory) GMP audit should be considered at
this stage. This will provide a baseline or purposes o monitoring and evaluation and a basiso understanding or developing an upgrading schedule and programme or the country.
A generic GMP road map will be developed as a central solution but, unless it is tailored
according to the specic country reality, its value may be compromised. Similarly, the risk
assessment o the EML will be a guide and local considerations will need to be refected in
any specic limitations adopted on manuacture.
This detailed strategy design phase will produce an overarching articulation o the strategy
and an implementation plan. This plan will, where appropriate, involve specic organiza-
tional development plans or the regulator and the industry association. It will also identiy
any policy or legislative requirements that need putting in place. The strategy will involve a
detailed cost benet analysis or consideration by government, whose authority at the high-
est level would be required to move to implementation. Following consultation with govern-
ment, it will also include indicators by which progress towards the vision can be assessed.
Stage 4: Implementation
The pharmaceutical industry is complex, capital intensive, and, at the plant level, calls or
detailed expertise and sophisticated processes, equipment and acilities. I these are not
already in place, they will take time to develop. Similarly, the capacity o the National Medi-
cines Regulatory Authority is critical to the development o the industry. However, putting
in place the appropriate regulatory systems is likely to require enhanced human resources
and organisational development, neither o which can take place overnight. Consequently,

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 91/119
77
SOLUTIONS
the implementation phase o the work will need to recognize that momentum and political
will must be maintained over a period o years.
It is expected that, through coordination under the PMPA, the partners will be able to move
rom talk to demonstrable action at the country level and that this will be an important
component in maintaining momentum. Appropriate government structures should also be
established and specic aspects o the national pharmaceutical industry development plan
should be incorporated into the perormance metrics or organizations and individuals.
In Chapter Four, a proposed structure or implementation o the Business Plan is outlined.
It recommends that regional PMPA coordinators should oversee activities in individual
countries that would be managed on a day to day basis by national experts. It would be the
role o these regional coordinators to access the expertise o the consortium and the generic
solutions package in order to ensure that national level implementation plans are conducted
as approved by the governments o each country. The representatives o the PMPA based at
regional and country levels would also, where invited by the Government, be responsible orensuring that developments are coordinated. In addition, they will be empowered to identiy
specic challenges present in any particular country and to mobilize expertise under the
PMPA to address them.
The specic activities carried out under the implementation phase will take place over a
period o years and will represent combinations o generic solutions described earlier and
tailored to the country context as well as bespoke solutions where necessary.
This central package o solutions is intended to provide the fexibility to advise and as-
sist countries acing very dierent contexts. Whilst the complete range o activities may
be required in some hubs that aspire to enhance manuacturing, other aspects may not be
relevant in all contexts. For example, the GMP road map component will have no relevance
to a country such as Botswana, which is looking to establish pharmaceutical manuactur-
ing capacity rom scratch and thereore does not require a quality upgrading road map.
Similarly, the availability o a central repository o expertise will enable the PMPA to assist
other non-producing countries or those with very small pharmaceutical sectors to consider
their options. For example, technical insights and understanding o the business and public
health aspects o local production could be mobilized to support countries such as Chad
and others to determine whether they wish to develop a strategic asset in this space and
to develop the model (perhaps a Public Private Partnership - PPP) by which one could be
achieved.
3.2 other actiVitieS
In addition to the generic solutions package, there are other initiatives proposed by this
Business Plan including the need or certain activities at the sub-regional and continent
level, as well as urther work on developing strategies or parts o the Essential Medicines
List and production value chain not already covered by the central solutions.
The manuacturing o ormulations is part o a value chain which extends back to the pro-
duction o raw materials including APIs. The core o this Business Plan looks at enhancing
the ormulations component o the value chain on the continent. However, long term sus-
tainability, competitiveness and innovation aspirations need to take into account enhanced

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 92/119
78
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
API capabilities at the continent level. In the shorter term, there are also likely to be oppor-
tunities or local production o other inputs.
This Business Plan covers various ormulation types but ocuses largely on small molecule
products. There are other products on the Essential Medicines List or which local produc-
tion is very desirable, particularly blood products.
3.2.1 Initiatives at continent level
There is a growing interest in local production o generic pharmaceuticals amongst our
development partners, an evolution in approach that is to be welcomed. We established the
concept o the PMPA as early as 2005 and the plan itsel was endorsed in 2007. As em-
phasized earlier, the PMPA respects the sovereignty o individual nations to take decisions
and to work bilaterally with institutions as desired. Similarly, the autonomy o our Regional
Economic Communities is also respected by this Business Plan and interventions at both
levels under the PMPA would be subject to invitation rom the respective political bodies.
However, the AUC will provide a central hub where those interested in continent level plans
which impact on the pharmaceutical industry will be able/expected to discuss their plans
and to align behind the PMPA. For example, the AUC, working with a consortium o part-
ners able to provide expertise and insights on many ronts, would have been an appropriate
partner in advising on the design o the AMFm, which has implications or the sustainability
o our local industry. The malaria community is to be congratulated that it recognized this
issue and took steps to address the concerns o local industry and seek solutions through its
conerence in Nairobi.
In uture, those working on public health initiatives and policy changes at, or example, theGlobal Fund, will be able to seek input rom the AUC (with advice rom the consortium)
when they consider the impact o initiatives on the long term sustainability o local produc-
tion. For example, the Global Fund’s market dynamics committee may wish to coner with
the AUC and its partners as it considers procurement policies that could assist in increasing
access to essential medicines and looks to transition to a uture model where we will take an
increasingly large share o the responsibility or providing essential medicines or our people.
The TRIPS fexibilities issue is another area where a continent wide position and the ability
to speak with one voice will have increased weight in discussions on extending the fexibili-
ties. Working together with international organisations like ARIPO, UNDP and UNCTAD,
the PMPA partnership will join the eort to lobby or the extension o the January 2016
TRIPS fexibilities window. The partnership will also mobilize all those involved to lobby or
the simplication o requirements to exploit the fexibilities given that the current onerous
and time consuming process has seen many companies either abort or elect not to partici-
pate, even when an opportunity presents itsel.
3.2.2 Regional level initiatives
There are a number o legislative, policy and trade issues that need resolving at the regional
level. They include the regional ramework or incorporating TRIPS fexibilities, registration
harmonization, and strategy rameworks under which national level progress can be made.
Equally important is the need or cooperation to maximise the benets o pharmaceuti-
cal trade among our countries and to minimise the impact o protectionist policies amongpartner states that could stand in the way o mutual benet and progress. In view o this,

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 93/119
79
SOLUTIONS
the consortium o partners would be available to assist regions to resolve some o these is-
sues, subject to invitation, and could orge links between national level strategies and the
rameworks put in place at regional level. Moreover, where regional level strategies are as
yet incomplete, the AUC and its partners could also work with the regional departments o
health, industry and trade to assist various counterparts to work together to establish policy
coherence at the regional level.
3.2.3 Regulatory harmonization
Lack o regulatory harmonization presents a serious challenge to manuacturers and inad-
vertently leads to reduced access and higher prices due to reduced competition when some
companies opt out o certain markets. Resolving this conundrum is thus critically impor-
tant. There are a number o very good ongoing initiatives under the auspices o the AMRH
initiative led by NEPAD among others.
The AMRH initiative has been working in the area o medicines regulatory harmonizationsince 2006 and has to date developed a number o regional proposals or harmonization in a
number o RECs. The harmonization processes or RECs like the Southern Arican Devel-
opment Community (SADC), Economic Community o Central Arican States (ECCAS)
and Economic Community o West Arican States (ECOWAS) are at an advanced stage and
the East Arican Community (EAC)’s plan has been nalized and was ormally launched in
March 2012. Lastly, the AMRH has also been mobilizing political support and the nancial
and technical resources needed to bring this to ruition.
Given that the lack o capacity in some NMRAs is partly responsible or the low levels o
trust among respective Authorities, the training o regulators is a key intervention on which
the partnership will ocus. The remaining harmonization initiatives will continue to be ablymanaged by the AMRH and it is envisaged that the role o this Business Plan will be con-
ned to supporting the development o country policies and strategies conducive to regula-
tory harmonization and to oering support to the activities o the AMRH through ongoing
technical assistance and training and capacity building o NMRA employees.
3.2.4 TakingadvantageofTRIPSexibilities
One o the key policy and legislative changes needed in order to benet our continent, its
patients and local industry is in the domain o intellectual property rights. Most countries
have ailed to take advantage o current opportunities presented by TRIPS fexibilities. A
ew have enacted the TRIPS provisions but the common consensus is that the requirements
are too onerous and too time consuming. Exploitation o the provisions is only permissible
i they are written into national laws yet many LDCs have not even incorporated TRIPS
fexibilities into their national legislation or the reasons cited above. In act, not only have
LDCs not incorporated the fexibilities, some actually have ar stricter IPR than required
under the TRIPS agreement.
Furthermore, negotiations to extend the window period beyond January 2016 should be
intensied and Arica should push or another ten year transition period. The AUC rmly
believes that the TRIPS fexibilities present the same opportunity or Arican pharma as did
the Indian Patent Act o 1970 or Indian industry. The Commission is convinced that ull
exploitation o the fexibilities would lead to a transormation o local industry. Thereore,
working together with ARIPO, UNDP and UNCTAD, the PMPA will:
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 94/119
80
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
• Lobby or simplication o the means by which fexibilities can be exploited. The
current system is onerous and wasteul
• Advise and assist governments to revise and amend their patent laws to incorporate
the fexibilities
• Assist international GMP compliant Arica based companies wishing to make ull
use o the fexibilities in order to supply LDC markets with the documentation and
in negotiating the legal mineeld
• Work with RECs to harmonize national patent laws to acilitate exploitation o the
fexibilities or the benet o the continent
This initiative creates an avenue to partner with European and North American companies
who oten develop molecules considerably ahead o time. Some o these companies have
already developed molecules whose patents will expire in 2017 and beyond. Given that they
have already committed the unds and invested in product development, they could transer
the technology to international GMP compliant Arican manuacturers who can then ex-
ploit the TRIPS fexibilities and market these much needed drugs in LDC markets.
3.2.5 API production
Measures to enhance API production capability on the continent are worthy o detailed
consideration in view o their potential to impact on the sustainability o production and
to become an asset or innovation (e.g. through novel synthetic pathways). The level o API
production on the continent at the moment is minimal but due consideration will be given
to enhancing capabilities and the models by which this could be achieved (such as the PPP
approach with Lonza in RSA) as a discrete part o the PMPA.
Whilst the production o various APIs remains a long term ambition, in order to exploit the
TRIPS fexibilities, our continent will need to develop the competencies to manuacture its
own APIs or products like second line ARVs. This is necessary given that the large Asian
bulk drug producers would, in the absence o voluntary licences, be unable to manuacture
and supply API to local ormulators. Similarly, the owners o the intellectual property would
be unlikely to provide API to our manuacturers even though our market contributes only
a miniscule amount to their revenues or any given products. Our partnership with leading
academics who have the expertise and have already developed a number o environmentally
riendly, more ecient and less costly processes or developing various molecules will be
very valuable.
3.2.6 Blood products
The collection o blood, and the separation o dierent components into plasma, various
blood actors, platelets and red blood cells is a specialized process that has limited correlation
to the generic pharmaceutical production which is the ocus o this Business Plan. However,
the availability o blood products in Arica would benet greatly rom local capacity or col-
lection, ractionation, etc. WHO is proposing to conduct easibility studies on the expansion
o blood product production on the continent. This work is welcomed by the AUC and, once
initial ndings are developed, could be incorporated as a component o the PMPA.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 95/119
81
SOLUTIONS
3.2.7 Vaccines and biological products
An area that will require urther work is establishing a model or enhancing the production
o human vaccines. Vaccines are a cornerstone o any primary healthcare programme andare an essential tool in preventing disease. The signicance o vaccines in public health in
general, coupled with the requirement to be able to respond rapidly to pandemics (note the
limited availability o fu vaccines during the 2009 infuenza crisis) mean that developing
our own capability to provide or our vaccine needs will be explored. The Arican Vaccine
Manuacturers’ Initiative is currently being ormulated. Historically, much emphasis has
been placed by international agencies and donors on the supply o vaccines and in doing so
many lives have been saved. However, we should build production capacity on the continent
so that, in the medium to long term, we will be able to rapidly respond to our needs and will
have a sustainable source o high quality products to address vaccine preventable diseases.
Developing our continent’s ability to produce biological products also needs urther con-
sideration. A number o important medicines based on recombinant DNA technology weredeveloped with the advent o biotechnology in the latter part o the 20th century and the
eld continues to be a source o novel treatments. In the realm o diabetes, recombinant
human insulin and epithelial growth actor are critical or managing the disease and associ-
ated symptoms; biological products have improved ecacy or many diseases compared to
some earlier generation treatments (e.g. tumor necrosis actor inhibitors or the treatment
o rheumatoid arthritis and betaintererons or treating multiple sclerosis); and a number o
the o latest generation cancer treatments are biological products (e.g. trastuzamab – trade
name Herceptin – a monoclonal antibody or the treatment o breast cancer). As ‘Western’
and non-communicable diseases become more prevalent having aordable, quality assured
sources o such products and others will be vital or providing our people with the best
treatment options or some emerging public health issues. We currently have very limitedcapacity or production o biological products and will need to consider dierent models or
the development o this segment o the industry given the unique manuacturing, distribu-
tion and market considerations that apply. Biotechnology may also hold the key to treating
uniquely Arican diseases and provide an option or optimizing traditional medicines, thus
building R&D expertise in this eld as well as production capacity should be part o the
objective.
3.2.8 Traditional medicines
Our continent is home to a large and diverse plant lie, much o which has ormed the basis
or many o our traditional medicine systems. It is also a act that these plant based remedies
remain the treatment o choice or many people in Arica. The AUC is acutely aware o this
and, o course, the PMPA itsel recognizes the important role that traditional medicines play
in healthcare delivery on our continent. Whilst research has been carried out on some o the
most well known treatments, and notwithstanding the act that some have even been com-
mercialized by international companies, there is an urgent need to accelerate research into
the extensive fora, especially those or which medicinal claims are made.
This process would lead to the codication o the traditional medicines and an elucidation
o properties, side eects and related aspects o the plant lie, as well as the creation o a li-
brary or these ndings. The AUC is very aware o the potential value o such medicines and
believes that the diverse Arican fora may well provide the world with another wonder drug
to replicate the importance o artemisinin, which has been used in traditional Chinese medi-cine or centuries. The USP is proposing to establish a Medicines Compendium or drugs

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 96/119
82
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
used outside the US and this would include traditional medicines. Moreover, initial discus-
sions have taken place with experts in the eld about approaches that could be adopted to
enhance availability and consistency o eective traditional Arican remedies.
3.3 SummarY o chaPter 3
The key messages rom this Chapter include:
• The heterogeneity o contexts across our continent requires that a solutions package
is designed to be fexible and able to assist countries at various stages o development
in the pharmaceutical eld and with diering ambitions
• The various dimensions o the pharmaceutical manuacturing system and the ‘inter-
connectedness o issues’ mean that implementation o dierent ‘solution modules’
in a country must be coordinated as part o a holistic strategy or development o
the sector
• The Business Plan proposes a Generic Solutions Package across dimensions that in-
clude approaches or strengthening human resources, guidance on incentives to the
industry, the utilization o a GMP road map and associated risk assessment o the
EML, brokering o partnerships and business linkages, and assistance to strengthen
regulatory capacity
• A process or developing and implementing national level strategies upon invitation
rom governments would likely include initial discussions with key stakeholders, adetailed consultative and diagnostic process, detailed strategy design, and imple-
mentation
• This process and the solution packages could be implemented in all countries rang-
ing rom those with no ambition to enter into manuacturing but with a desire to
improve regulatory oversight and to benet rom high quality local production rom
neighbours to advanced countries in the North who wish to urther develop their
industries or public health and economic development objectives
• This Business Plan espouses an approach whereby the industry as a whole is as-
sisted and required to improve standards to eventually achieve international GMP.
However, in the short term, individual assistance to leading companies to prequaliyproducts is also a critical requirement
• There is the need or novel ormulations such as new FDC ARVs and paediatric
ACTs. The opportunity also exists to take advantage o TRIPS fexibilities through
reverse engineering o second and third line ARVs. In view o this, research centres
will be assisted to develop such products or transer to companies that meet inter-
national GMP standards
• Implementation o solutions and genuine commitment rom partners and govern-
ments will lead to indirect improvements in the business context or the pharmaceu-
tical industry by, or example, making it more attractive to investors and through the
establishment o supporting services and industries

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 97/119
83
SOLUTIONS
• As well as country level activities, this Business Plan identies some additional areas
o work at regional and continent level (such as lobbying or an extension to the
TRIPS fexibilities) and identies associated areas such as API production, blood
products and traditional medicines where ongoing work will need to be built upon
and insights incorporated under the PMPA

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 98/119
84

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 99/119
85
IMPLEMENTATION PLAN
4. iMPLEMENTATiON PLAN
The earlier Chapters o this Business Plan have detailed the ambitions or pharmaceuticalmanuacturing on our continent, outlined the current situation in the sector and the chal-
lenges and opportunities in realizing the vision o the PMPA. They have also proposed an
indicative ‘package o solutions’ that will be developed to address the complexity o the vari-
ous dimensions o the pharmaceutical manuacturing system in a holistic and coordinated
ashion. This package o solutions will represent a central repository o expertise that can be
tailored to implementation at the country level.
The main thrust o the document is that, whilst ambitions and aspirations vary amongst our
member states, there are generic themes that apply to a greater or lesser extent across coun-
tries that are actively engaged in pharmaceutical production or in those that may wish to en-
ter the sector. Critical to the design o this proposal or implementation is that the solutions
required cover a diverse range o skills, expertise and capabilities which no one organisation
or entity can provide. In view o this, a consortium approach, with core partners contrib-
uting to the design and implementation o the solutions package, is recommended. Initial
discussions have taken place with organisations identied as having the critical expertise
and mandates to cover the range o requirements. During the initial stages o implementa-
tion, detailed discussions will be necessary to lay the oundations o the consortium and to
establish the specic roles and responsibilities o the dierent parties.
I this Business Plan is to translate into genuine sustainable progress to the benet o our
continent, it is imperative that the partners (both Arican entities and international develop-
ment bodies) within the consortium genuinely collaborate over an extended period o time
and that a positive dynamic is established between the various organisations. The achieve-ment o a unctioning consortium will be dependent on a number o actors, including:
• The degree to which partners have the opportunity to provide input into the details
o what this Business Plan will deliver and how this will be achieved
• The availability o central resources to und the activities o various parties under
the PMPA
• Establishing mutual trust between organisations and between the individuals who
represent them
• Establishing the legal basis or the consortium
• Developing a detailed shared work plan with roles and responsibilities identied
along with the measures by which organisations will be held accountable or their
contribution
• The governance and reporting structures or the consortium
• The degree o fexibility or the work plan such that learning over time can be in-
corporated and activities adjusted according to the evolving reality on the ground
(subject to oversight rom the PMPA governance structures)
• The central authority o the Arican Union Commission as the leading entity which‘owns’ the plan on behal o our member states
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 100/119
86
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
This implementation plan is crated with a clear recognition o the multiplicity o eorts
and initiatives across the various RECs and countries on the continent. Whilst it recognizes
the need or some regional interventions, it also appreciates the crucial importance and
centrality o country level implementation. Key to real progress at the country level will be
the coordination o activities on the ground and the collaboration between a diverse range
o national level stakeholders. As well as coordination at the central level, this Business Plan
proposes a mechanism by which (subject to invitation by individual member states) agents
acting on behal o the PMPA will be able to ull an ‘honest broker’ role as national level
stakeholders come together to ormulate, develop and implement a shared national strategy
or the development o the ‘Pharmaceutical Manuacturing System’.
The PMPA is an Arican initiative and is the responsibility o the AUC on behal o our
member states. We have invited UNIDO to be a core partner in accelerating the implemen-
tation o the PMPA and it has agreed to continue in this role as we move to implement this
plan. UNIDO will also work with us as we set up the consortium o partners and seek to
mobilize the necessary resources.
Moving orward, it will be imperative that the consortium is a partnership under the leader-
ship and authority o the AUC. UNIDO has been asked to provide planning and coordina-
tion unctions at the central and eld level as part o the role it will ull in this partnership.
The Organization has indicated that, backed by nancial support rom the German govern-
ment, it will be sel-nanced as it works with us through the initial phase o the Business
Plan.
In the longer term, central unds (mobilized or the implementation o the PMPA) will be
allocated and disbursed according to the shared work plan developed by the partnership on
condition that this work plan is endorsed by the governance structures o the PMPA/AUCand the respective donors.
A phased approach to the implementation o the Business Plan is envisaged. This chapter
rst describes the various phases to be worked through. It then details specic components
o implementation such as the nature o the resources required, a proposed structure, ap-
proaches or engaging the broad range o stakeholders operating in this eld, and nally
discusses the monitoring and evaluation dimension o the plan.
4.1 PhaSeD aPProach to imPlementationFour main phases or the implementation o the plan are envisaged:
• Set up phase
• Pilot phase
• Scale up phase
• Full scale implementation
The ollowing sub-sections describe in more detail the activities to be conducted duringeach phase. It should be noted that a strict linearity is not anticipated and, or example,

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 101/119
87
IMPLEMENTATION PLAN
given that a ew countries and regions have already developed plans that are ready or ur-
ther elaboration, the pilot phase is likely to overlap with the set up phase. Moreover, whilst
it has been designated as a specic ‘phase’, perhaps an alternative way o perceiving the pilot
phase is that it provides or the launching o ull scale implementation in countries that have
already developed plans o action and where the solutions developed in the set up phase can
be implemented without the need or the consultative process required in most countries.
4.1.1 Set up phase
The set up phase will involve the ollowing key aspects:
• Building the consortium and establishing its legal basis
• Detailed discussions to develop a shared work plan
• Resource mobilization
• Development o solutions or which urther work is required (e.g. GMP roadmap,
EML risk assessment, detailed design o syllabus or HR development across the
dierent dimensions o human capital requirements)
• Identication o member states and, i appropriate, RECs who wish to actively en-
gage with the PMPA
• Identication o experts and service providers
• Interaction with other stakeholders involved in activities related to pharmaceutical
manuacturing in order to derive inputs and identiy opportunities or collaboration/alignment with the PMPA
• Setting up eld representation or the PMPA
Establishing the central consortium
Initial discussions have taken place with prospective partners in the central consortium that
would assist the AUC in the implementation o this Business Plan. This consortium should
include partners with sucient expertise to cover the ull range o disciplines required or
the pharmaceutical manuacturing system, including regulation o the industry, industrial
development, GMP, human resource development, and ormulation development/R & D,
as well as political authority in the realm o public health. It will comprise Arican organiza-
tions and international development partners but should consist o a limited number such
that it does not become unwieldy. Consequently, whilst some overlap in expertise is inevi-
table, duplication o expertise will be limited.
The introduction to this chapter identied some o the aspects needed or the consortium
to become a genuine partnership with positive internal dynamics so that it is able to eect
change. One component o this is establishing the legal basis or the consortium and urther
legal advice will be required as to the specics o the appropriate legal structures. Partners
will also be expected to sign memoranda o association or letters o agreement that identiy
the undamental role that each organization will play.
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 102/119
88
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
Whilst a legal basis or the relationship between the parties is required, it should also be
borne in mind that extended deliberations should be avoided as there is an urgent need or
progress on the ground. The legal documents will outline the core role o each constituent
but will in all likelihood also reer to the action plan or identication o the detailed ac-
tivities to be undertaken by each partner. Such an approach will enable fexibility since the
action plan should be a ‘living document’ that will be reviewed regularly with substantive
changes submitted to the Technical Committee and respective donors or approval. Further-
more, it should acilitate a relatively ecient approach to establishing the legal basis or the
consortium.
Developing a shared action plan
Once agreements in principle have been reached with partners, the development o a shared
action plan will be a top priority. Initial bilateral discussions will be held between the AUC/
UNIDO and dierent potential partners prior to a proposed retreat when the consortium
will meet to discuss and agree on the details o the shared action plan. This plan should rep-
resent a common understanding o the detail required or each component o the solutions
package and will probably include indicative (depending on resource mobilization progress)
timelines or production o concrete deliverables. The specics o the action plan will enable
a detailed understanding o the magnitude, nature and timing o resource requirements and
will eed into the resource mobilization activities conducted by the AUC and UNIDO.
Resource mobilization
A description o the resource requirements or the Business Plan is given later in this chap-ter. AUC/UNIDO will take the lead in developing and implementing a resource mobiliza-
tion strategy. This will involve initial contact with donors to explain the philosophy and
recommended approach o the Business Plan or the PMPA and to explore their level o
interest. This Plan provides indicative gures as to the timing and magnitude o resources
required over the next ve years and this will orm the basis or discussions. However, the
action plan will need to be nalized beore detailed negotiations can take place and in order
to establish the monitoring and evaluation requirements o the unders o this initiative.
Further development o the solutions package
The current status o the individual components o the indicative solutions package varies.
For example, deep insights into regulation o the industry are inherent within the expertise
o potential partners such as WHO, although the implementation o this Business Plan will
require the scaling up o ongoing activities and identication o technical expertise that can
be mobilized (probably on a ee or service basis) in order or technical assistance (TA)
across dierent countries to be delivered in parallel. Similarly, UNIDO has extensive expe-
rience in working with countries to develop strategies across the manuacturing system and
a proposed stepwise approach to engaging with stakeholders is described in this document.
However, other aspects, such as the development o a generic GMP roadmap, need more
work. WHO has (in another context) identied the risk assessment o the EML as being a
potential activity or the near uture and discussions as to how this can be supported by the

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 103/119
89
IMPLEMENTATION PLAN
PMPA will be necessary. Various academic institutions in Arica have the capability to de-
velop new ormulations but the products to be developed will need prioritizing. A compre-
hensive syllabus or developing human resource capacity across the manuacturing system
largely exists across dierent stakeholders. However, the critical issue is to ensure coordina-
tion o the syllabus in such a way that it builds on itsel over time. This will require urther
deliberation during the set up phase.
In view o this, during the set up phase it will be necessary to rene existing tools and ex-
pertise as well as to ensure that substantive progress is made on certain specic elements o
the solutions package.
Identifcation o interested member states and RECs
We will invite expressions o interest rom our member states to establish which countries
and possibly RECs would like to work with the AUC and its partners. The Business Plan
is designed to benet all countries on our continent whether through strengthening the
manuacturing system itsel or through providing secure sources o high quality aordable
medicines across much o the Essential Medicines List. The PMPA is not intended to be
a unding mechanism or public or private sector investment but is a proposed package o
technical assistance that would be provided to enable countries to ull their ambitions in
this eld and to help develop and implement tailored strategies that take into account the
specic context o a country or region.
For countries that do not seek to become manuacturing hubs, the PMPA would look to pro-
vide guidance on improvement in regulatory oversight to enable them to take advantage o
high quality regional sources o supply. Such activities would be conducted in coordinationwith other ongoing initiatives (such as the AMRH work and regional strategies) and will not
seek to override these endeavours. However, improved market oversight is a key requirement
i the benets o local production are to be realized and the AUC and its partners would
seek, where necessary, to increase the emphasis on this aspect and to mobilize the requisite
support such as loans rom development banks or investing in regulatory inrastructure.
Subject to the number o requests received, as well as available resources and the timing
o those resources, it is likely that some means o prioritizing requests will be necessary.
Depending on the volume o demand, the AUC would seek guidance rom the Technical
Committee as to the criteria to be applied when scheduling support or individual countries.
Ultimately, the prioritization would only be relevant during the set up, pilot and scale up
phases as, at ull implementation (subject to available resources), the AUC and its consor-
tium partners would look to work with all countries requesting support to establish their
priorities and develop and implement the strategy or achieving them.
Identifcation o service providers
In addition to the consortium o partners, there will be a need to engage external expertise
rom service providers in the realm o, or example, improving production eciencies, ad-
vice on accessing the best technologies, and so orth. The AUC will, through the business
linkages platorm, identiy a number o experts who are available to work with trade as-
sociations to disseminate best practice and, secondly, to assist companies willing to pay or

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 104/119
90
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
additional in-house training which would build on the sector level modules and materials
developed or manuacturers to utilize.
Interaction with other stakeholders
O necessity, the size o the central consortium will be kept to a limited number o organiza-
tions. However, many entities are active in areas related to local production and their part-
nership with the PMPA and alignment with its approach will be critical to the success o this
endeavour. Thereore, as well as the establishment o a consortium, mechanisms by which
other partners can be engaged or inputs and or coordination will be explored. In the initial
set up phase, or example, bilateral discussions between the AUC (and/or UNIDO acting
on behal o the AUC) and the many entities involved would be appropriate. A stakeholders’
conerence would also be a possible mechanism or building awareness, seeking inputs and
allowing or constructive debate as to how dierent parties could align with the overarching
objectives o the PMPA.
It is also likely that, although not members o the central consortium, other stakeholders
could become directly involved in implementing activities through direct unding o their
activities rom central PMPA resources. For example, there are a number o academic orga-
nizations in Arica that have expressed interest in working with the PMPA and it is essential
that Arica’s academia should be represented within the consortium. However, it will not be
possible to have all such institutions represented even though they may be conducting criti-
cal unctions under the PMPA (training, ormulation development, etc.).
Setting up feld presence or the PMPA
Experience suggests that there is a need or an ‘honest broker’ unction at the country level
to bring dierent stakeholders together to develop shared strategies or the manuacturing
system. It has also been established that such collaboration requires close escorting so that
momentum is built and maintained. It is thereore proposed that a dedicated (though mini-
mal) eld presence be established, with coordinators covering a number o dierent coun-
tries. A proposed structure or implementing the PMPA is elaborated later in this chapter.
4.1.2 Pilot phase
Given that various organizations have already been working in some o the identied priorityareas in some countries, the package o PMPA solutions will be mobilized in those territories
where there is already broad consensus among stakeholders about what needs to be done.
USP, UNIDO and WHO have, or example, all been actively engaged in Ghana and Kenya
on various dimensions o the local production agenda. Furthermore, through a stakeholder
consultative process, strategies have been developed that are supported by the dierent na-
tional actors across public and private sectors. In view o this, these countries would be well
positioned to benet immediately rom implementation o solutions and could thereore be
considered or assistance as part o the pilot phase.
It should be highlighted that the pilot phase is not envisaged as reaching a ‘conclusion’ prior
to scaling up o activities as progress in the pharmaceutical sector will materialize over an
extended timerame. However, there will be the opportunity to learn how the consortium

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 105/119
91
IMPLEMENTATION PLAN
works at the country level and to seek to adjust the model as experience is gained. It is in-
tended that the scale up phase (subject to resources) will take place in parallel with activities
in these countries although strategy development at the national level will be needed prior
to detailed implementation.
4.1.3 Scale up phase
Ultimately, the PMPA is designed to be a mechanism by which real progress can be made
on the ground in our member states. Many countries do not have strategies or the pharma-
ceutical system. Consequently, prior to delivering change, national (and regional) strategy
development exercises will be necessary.
In view o this, the scale up phase reers largely to the need to enter into detailed strategy
design at the country level prior to implementation. Subject to demand rom our member
states, resource mobilization, and the level o capacity available or eld level coordination
under the PMPA, it is likely that some means o prioritizing countries will be necessary asalready pointed out. The Technical Committee’s guidance on this matter will be sought.
However, it is worth reiterating that such prioritization is purely a scheduling issue and that
the development o national level strategies or all interested countries would be initiated as
expeditiously as possible.
4.1.4 Full scale implementation
Some countries have already developed strategies that can be built on through a detailed
implementation planning process ollowed by the implementation itsel. Thereore, it is pro-
posed that the PMPA move rapidly to conduct this work under what is described as the
pilot phase. Full scale implementation will eectively be the phase when strategy designrom other interested countries comes on stream and the PMPA is mobilized to deliver the
tailored package o solutions in-country.
4.2 StaKeholDer engagement
This section identies the broad range o stakeholders and reviews the steps needed to en-
gage them and align eorts behind the PMPA. It will also outline a plan or maintaining the
channels o communication with all stakeholders.
The AUC recognizes that one o the reasons why various pharmaceutical development ini-
tiatives have not achieved the desired success is the lack o participation and coordination
across various stakeholders. To ensure that there is widespread support and buy-in rom all
stakeholders and that their activities are consistent with objectives, the AUC will seek to in-
volve all interested parties throughout the various phases outlined in the Business Plan. The
Commission has thus undertaken a stakeholder mapping and analysis which takes into con-
sideration the current initiatives in place to support local manuacturing on the continent. It
also includes direct beneciaries such as industry trade associations, individual companies
and the patients who will benet rom the realization o the PMPA’s goals.
We propose to develop a plan to establish and maintain channels o communication with
all stakeholders such that they are kept inormed and can provide insights and eedback on

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 106/119
92
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
their activities. We at the AUC will also be a ocal point with which any organizations whose
activities in Arica are relevant to the sustainability o pharmaceutical manuacturing on our
continent will be able to/expected to engage. In this way, we will seek to ensure that policy
incoherence at the continent level as a result o uncoordinated initiatives does not material-
ize. The AUC is nonetheless aware o a number o good initiatives on the ground and has
no intention o interering with bilateral initiatives at a country or regional level that have
been entered into by our member states or RECs; we will only seek to augment eorts on
the ground and not to supplant them.
The Arican Union Commission will thereore develop a stakeholder engagement strategy
which will likely involve communicating inormation on developments under the PMPA
and the establishment o mechanisms by which stakeholders can come together to provide
eedback and to discuss their activities under the overarching PMPA ramework. Table 4 lists
some o the present and potential stakeholders (but is by no means the denitive list) and
the areas in which they are active.
tb 4: idv s bd y skds s d p a
Area of Work Organization
Humancapitaldevelopmentandcapacitybuilding
(productionandbusinessmanagement)
•ActionMedeor
•Africanacademicinstitutions
•AfricanMedicinesRegulatoryHarmonization
initiative(AMRH)
•HowardUniversity
•InternationalConferenceonHarmonisation
•PurdueUniversity•SaintLukeFoundationinTanzania
•StringentRegulatoryAuthorities(e.g.FDA)
•U.S.PharmacopeialConvention(USP)
•WorldHealthOrganization(WHO)
Intellectualproperty •Afr icanRegionalIntellectualPropertyOrganiza-
tion(ARIPO)
•DeutscheGesellschaftfuerInternationale
Zusammenarbeit(GIZ)
•UnitedNationsConferenceonTradeandDe-
velopment(UNCTAD)
•UnitedNationsDevelopmentProgramme
(UNDP)•WorldIntellectualPropertyOrganization
(WIPO)
Procurement • ClintonHealthAccessinitiative(CHAI)
•GlobalTBDrugFacility
•MedecinsSansFrontieres(MSF)
•NationalTenderBoards
•President’sEmergencyPlanforAIDSRelief
(PEPFAR)U.S.
•TheGlobalFundtoFightAIDS,Tuberculosisand
Malaria
•UNICEF
•UNITAID
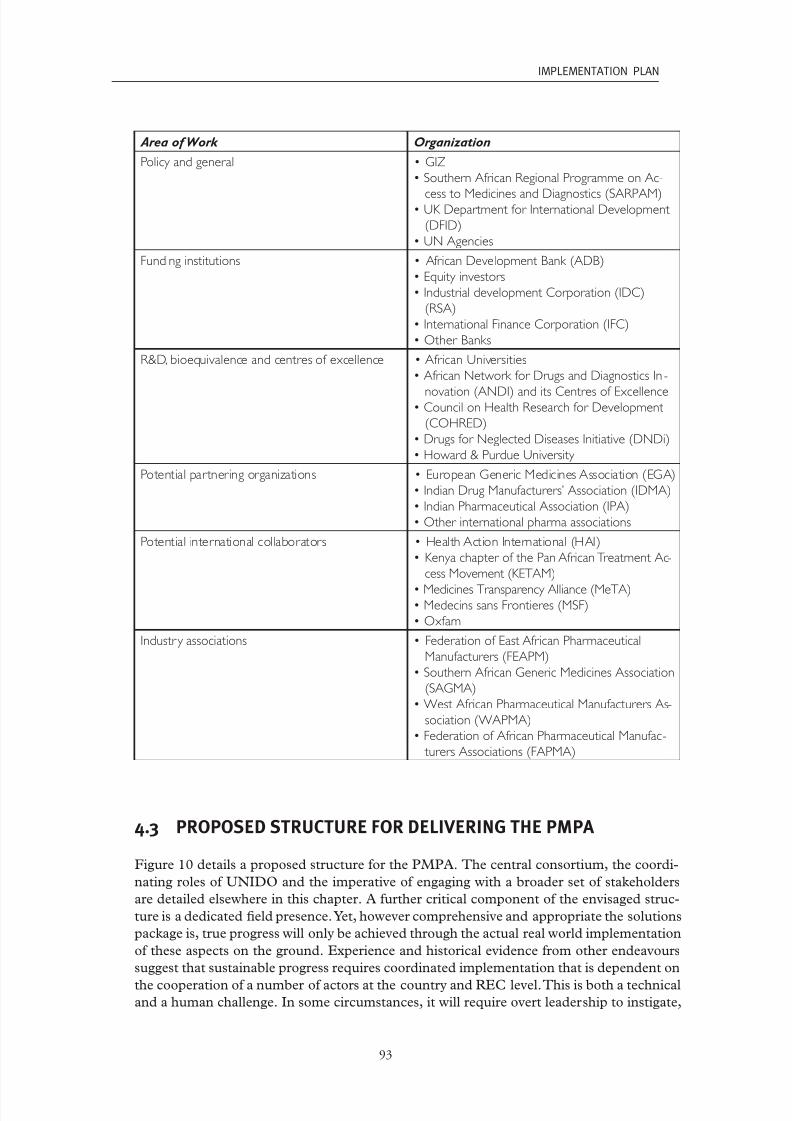
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 107/119
93
IMPLEMENTATION PLAN
Area of Work Organization
Policyandgeneral •GIZ
•SouthernAfricanRegionalProgrammeonAc-
cesstoMedicinesandDiagnostics(SARPAM)•UKDepartmentforInternationalDevelopment
(DFID)
•UNAgencies
Fundinginstitutions • AfricanDevelopmentBank(ADB)
•Equityinvestors
•IndustrialdevelopmentCorporation(IDC)
(RSA)
•InternationalFinanceCorporation(IFC)
•OtherBanks
R&D,bioequivalenceandcentresofexcellence •AfricanUniversities
•AfricanNetworkforDrugsandDiagnosticsIn -
novation(ANDI)anditsCentresofExcellence•CouncilonHealthResearchforDevelopment
(COHRED)
•DrugsforNeglectedDiseasesInitiative(DNDi)
•Howard&PurdueUniversity
Potentialpartneringorganizations •EuropeanGenericMedicinesAssociation(EGA)
•IndianDrugManufacturers’Association(IDMA)
•IndianPharmaceuticalAssociation(IPA)
•Otherinternationalpharmaassociations
Potentialinternationalcollaborators •HealthActionInternational(HAI)
•KenyachapterofthePanAfricanTreatmentAc-
cessMovement(KETAM)
•MedicinesTransparencyAlliance(MeTA)•MedecinssansFrontieres(MSF)
•Oxfam
Industr yassociations • FederationofEastAfricanPharmaceutical
Manufacturers(FEAPM)
•SouthernAfricanGenericMedicinesAssociation
(SAGMA)
•WestAfricanPharmaceuticalManufacturersAs-
sociation(WAPMA)
•FederationofAfricanPharmaceuticalManufac -
turersAssociations(FAPMA)
4.3 ProPoSeD Structure or DeliVering the PmPa
Figure 10 details a proposed structure or the PMPA. The central consortium, the coordi-
nating roles o UNIDO and the imperative o engaging with a broader set o stakeholders
are detailed elsewhere in this chapter. A urther critical component o the envisaged struc-
ture is a dedicated eld presence. Yet, however comprehensive and appropriate the solutions
package is, true progress will only be achieved through the actual real world implementation
o these aspects on the ground. Experience and historical evidence rom other endeavours
suggest that sustainable progress requires coordinated implementation that is dependent on
the cooperation o a number o actors at the country and REC level. This is both a technicaland a human challenge. In some circumstances, it will require overt leadership to instigate,

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 108/119
94
PHARMACEUTICAL MANUFACTURING PLAN FOR AFRICA - BUSINESS PLAN
motivate, and coordinate dierent parties. In other instances, where initiatives are already
underway, it will be imperative that the PMPA supports ongoing eorts and does not try to
replicate and/or take over the agenda.
Experienced individuals with the credibility and ability to recognize and adapt to the di-
erent dynamics as well as to infuence high level oce bearers will be imperative or the
success o the programme. It is proposed that our regional coordinators be placed in the
eld with responsibility or managing the implementation o the PMPA (whether as a ‘go it
alone’ or as a supporting initiative) at country and regional level. They would be responsible
or accessing the package o solutions rom the central hub on behal o the stakeholders in
the eld both at the REC level and in individual countries that have engaged the PMPA to
help develop their industries.
It would not be easible or necessarily appropriate (as capacity building or the long term
should also be an objective) to engage such individuals or each and every country and na-
tional level experts would be employed to manage the administration o the solutions. Theregional coordinators will provide the high level support as and when necessary. Figure 10
below gives a schematic representation o the relationships between the dierent aspects o
the proposed structure.
10: Ppsd s p Bsss P
Regional
Expert A
African
Union
Commission
PMPA Technical Committee
Consortium
of
Partners
Country
Expert B
Country
Expert C
Country
Expert D
Regional
Expert B
Country
Expert E
Country
Expert F
Regional
Expert C…
… ……………Country
Expert A
Additional temporary expertise will be required and will include the pool o experts that
will be recruited to oer various services to the industry and to assist the PMPA programme
team when needed. This pool o experts will be assisted in the regions and at country level
by the permanent team members leading the various interventions.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 109/119
95
ImplementatIon plan
4.4 reSource reQuirementS
The AUC and UNIDO will take the lead in mobilizing the resources required to deliver this
Business Plan. It is proposed that UNIDO hold a trust und or central PMPA resourceswhich would be disbursed to dierent consortium partners and the broader range o stake-
holders according to the action plan developed (including identication o expertise beyond
the consortium to be nanced rom central programme unds). The details o the resource
requirements in terms o dierent components, timing and magnitude will be developed in
line with the action plan. However, at this stage it is possible to identiy the major compo-
nents o the plan which will require unding and to provide some indicative gures or the
overall resource requirements as well as the expected timing o those resources.
There will be some elements o xed cost in setting up the human ‘inrastructure’ required
or the Business Plan and or the operation o the central consortium. There will also be
xed costs associated with urther work on developing the solutions package. In addition,
there will be variable costs that will depend on the number o countries and (RECs) that ac-
tively engage with the PMPA and the level o activity required in each country. For example,
the complexity o the situation in countries with well established industry sectors is likely to
require more detailed and wide ranging activities at the dierent stages o the country level
process than in a country that has limited or no pharmaceutical manuacturing.
A signicant proportion o the overall cost o the Business Plan is expected to be incurred
in the process o developing human resources or the pharmaceutical manuacturing sys-
tem. Investment in acilities or training will be beyond the scope o the PMPA so estab-
lished centres o excellence will be utilized and the PMPA will actively lobby or expanding
the model o training provision, or example, at the Saint Luke Foundation. The nature o
sponsorship or participants on these courses will also need to be considered. For example,UNIDO currently sponsors participants on the extended course at Saint Luke Foundation
providing 50% o ees or private sector actors and 100% o ees or public sector represen-
tatives (travel and subsistence costs are covered by the individual or his/her organization).
Similarly, an extensive syllabus o in-country training modules is anticipated and the degree
to which these are ully unded under the PMPA or whether some ees will be recouped will
need urther consideration and may vary depending on the specic nature o the module
and the resource requirements.
This Business Plan also proposes utilizing the expertise o research entities or the devel-
opment o new ormulations and or developing synthetic pathways or APIs required in
products covered by patents that could be developed or production under the TRIPS fex-
ibilities. These APIs would be used in ormulations that would also need to be developed.
It is envisaged that these initiatives would require initial seed unding and that their ongo-
ing activities to develop urther products would be nanced by recouping the investment
through charging ees to GMP-compliant companies and taking a cost sharing approach.
The ollowing table lists the main cost components described above and provides guid-
ance on the expected timing implications as well as, where possible, indicative gures. The
total resource requirements identied in this indicative budget are roughly US$54mn over
ve years, with an annual breakdown o US$4mn, US$16mn, US$14mn, US$10mn and
US$10mn in years 1 to 5 respectively.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 110/119

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 111/119
97
ImplementatIon plan
C o s t C o m p o n e n t
T i m i n g I m p l i c a t i o n s
A s s u m p t i o n s
E s t i m a t e d m a g n i t u d e
I n - c o u n t r y / c o u n t r y c l u s t e r t r a i n i n g
c o
u r s e s a c r o s s v a r i o u s d i m e n s i o n s .
W i l l d e p e n d o n d e v e l o p m e n t o f s y l -
l a b u s a n d f u n c t i o n i n g o f T r a d e A s s o c i a -
t i o n s
A s s u m e s :
C o u r s e s i n - c o u n t r y i n 1 0 c o u n t r i e s a n d
f o r 4 c o u n t r y c l u s t e r s . 2 0 s e s s i o n s p e r
y e a r f u n d e d b y P M P A ( o t h e r t r a i n i n g
p r o v i d e r s w i l l a u g m e n t w i t h t h e
i r o w n
f u n d i n g ) w i t h c o s t s l i m i t e d t o v e n u e ,
m a t e r i a l s a n d t r a v e l a n d p r o f e s s i o n a l
f e e s o f t r a i n e r . T o t a l p e r s e s s i o n
U S $ 4 k
( p o s s i b i l i t y o f c h a r g i n g f e e s b u t
a s s u m e s
f u l l c o s t b o r n e b y P M P A ) . S c a l e
u p w i t h
5 0 % i n 1 s t y e a r , 7 5 %
i n 2 n d y e a
r a n d
1 0 0 % i n 3 r d , 4 t
h a n d 5 t h y e a r s
Y e a r 1 : U
S $ 5 6 0 k
Y e a r 2 : U
S $ 8 4 0 k
Y e a r 3 : U
S $ 1 . 1 2 m n
Y e a r 4 : U
S $ 1 . 1 2 m n
Y e a r 5 : U
S $ 1 . 1 2 m n
T o t a l : U S $ 4 . 7 6 m n
I m
p l e m e n t a t i o n p h a s e
T A
a c r o s s m a n u f a c t u r i n g s y s t e m i n a c -
c o
r d a n c e w i t h a g r e e d s t r a t e g y
S u g g e s t e d t h a t i n G h a n a a n d K e n y a
i m p l e m e n t a t i o n s t a r t s b e g i n n i n g
2 0 1 3 . O
t h e r c o u n t r i e s b e g i n t o e n t e r
i m p l e m e n t a t i o n p h a s e i n 2 0 1 4 w i t h
a l l
s t r a t e g i e s i n 3 0 c o u n t i e s c o m p l e t e b
y
e n d 2 0 1 5
R e s o u r c e r e q u i r e m e n t s f o r i m p
l e m e n t a -
t i o n s u p p o r t w i l l v a r y w i d e l y b u
t a v e r -
a g e e s t i m a t e d a t U S $ 2 5 0 k p e r y e a r p e r
c o u n t r y . A s s u m e 5 y e a r s s u p p o r t f o r
r s t t w o c o u n t r i e s . A f u r t h e r 8
c o u n -
t r i e s r e c e i v e 4 y e a r s a n d 2 0 c o u n t r i e s 3
y e a r s T A
Y e a r 1 : U
S $ 5 0 0 k
Y e a r 2 : U
S $ 2 . 5 m n
Y e a r 3 : U
S $ 7 . 5 m n
Y e a r 4 : U
S $ 7 . 5 m n
Y e a r 5 : U
S $ 7 . 5 m n
T o t a l : U S $ 2 5 . 5 m n
N e w f o r m u l a t i o n d e v e l o p m e n t
O n e o f f p a y m e n t ( a l t h o u g h c o u l d b e
p h a s e d ) . w i t h r e v o l v i n g f u n d m o d e l
A s s u m e s :
F i v e e n t i t i e s r e c e i v e s e e d f u n d i n
g i n 2 n d
y e a r o f p l a n
E a c h o r g a n i s a t i o n r e c e i v e s ' w o r
k i n g
c a p i t a l ' o f U S $ 1 m n T e c h n o l o g y
t r a n s f e r
c o s t s w i l l b e b o r n e b y t h e r e c i p
i e n t
c o m p a n y
T o t a l c o s t i n y e a r 2 : U
S $ 5 m
n
B u s i n e s s l i n k a g e s p l a t f o r m
D e d i c a t e d P M P A s t a f f m e m b e r ( i n -
c l u d e d a b o v e ) b u t a n n u a l o p e r a t i n g
c o s t s w i l l r e l a t e t o s t a f f t r a v e l a n d P R
a c t i v i t i e s . A s s u m e o n e p a r t n e r i n g e v
e n t
i n 2 n d a n d 4 t h y e a r s
W i l l i n c l u d e a w e b p o r t a l m a n a
g e d b y
c e n t r a l P M P A s t a f f . M a r k e t i n g o f s e r v i c e
r e q u i r e d s o P M P A s t a f f t o t r a v e
l t o
c o n f e r e n c e s f o r a w a r e n e s s b u i l d i n g . 5
c o n f e r e n c e s p e r y e a r a t U S $ 6 k
e a c h .
A l s o t r a v e l t o B R I C S c o u n t r i e s a n d E u -
r o p e f o r p r o m o t i o n o f s e r v i c e - 3 t r i p s
p e r y e a r a t U S $ 8 k p e r t r i p
E v e n t i n y e a r 2 a n d 4 a t U S $ 1 5
0 k e a c h .
Y e a r 1 : U
S $ 5 4 k
Y e a r 2 : U
S $ 2 0 4 k
Y e a r 3 : U
S $ 5 4 k
Y e a r 4 : U
S $ 2 0 4 k
Y e a r 5 : U
S $ 5 4 k
T o t a l : U S $ 5 7 0 k

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 112/119
98
Pharmaceutical manufacturing Plan for africa - Business Plan
C o s t C om p
on en t
T i mi n g
I m pl i c a t i on s
A s s
um p t i on s
E s t i m a t e d m a gni t u d e
P MP A s t a k e
h ol d er e v en t s
On e e v en t d ur i n g t h e s e t u p ph a s e ; on e
i n y e a r
3 a n d on ei n y e a r 5 . On g oi n g
d i a l o g u
e wi l l b e c on d u c t e d b y c or e
P MP A s t a f f t om a i n t a i n c omm uni c a t i on
E a c h e v en t U S $ 1 5 0 k
Y e a r 1 : U S $ 1 5 0 k
Y e a r 2 : U S $ 0
Y e a r 3 : U S $ 1 5 0 k
Y e a r 4 : U S $ 0
Y e a r 5 : U S $ 1 5 0 k
T o t a l : U S $ 4 5 0 k
T e c h ni c a l C
ommi t t e em e e t i n g s
A nn u a l m e e t i n g s of t h eT e c h ni c a l C om-
mi t t e e
wi l l t a k e pl a c e , pl u s a n ex c e p-
t i on a l m
e e t i n g ex p e c t e d f or a p pr o v a l of
a c t i on pl a nh a l f w a y t h r o u g h y e a r 1 .
2 d
a y m e e t i n g s wi t h s i m ul t a n e o u s
t r a
n s l a t i on ,f a c i l i t i e s a n d t r a v el f or T C
m e
m b er s a n d P MP A s t a f f c o v er e d .A s -
s um e2 0 T C m em b er s p er e v en t , wi t h
c o s t s p er i n d i v i d u a l U S $ 2 . 5 k .
P l u
s f a c i l i t i e s e t c . U S $ 1 0 k p er e v en t
Y e a r 1 : U S $ 1 2 0 k
Y e a r 2 : U S $ 6 0 k
Y e a r 3 : U S $ 6 0 k
Y e a r 4 : U S $ 6 0 k
Y e a r 5 : U S $ 6 0 k
T o t a l : U S $ 3 6 0 , 0 0 0
C on s or t i um
m e e t i n g s
R e g ul a r m e e t i n g s of t h e c on s or t i um
a r e ex p
e c t e d t o t a k e pl a c e e v er y s i x
m on t h s a n d i n t h e s e t u p ph a s e wi l l b e
s el f n a n c e d . Wh enr e s o ur c e s m o b i -
l i z e d , c o s t s s h o ul d b e c o v er e d b y P MP A
A s s um e1 0 t r a v el l i n g p a r t i c i p a n t s wi t h
v en u e c h a n g i n g b u t a v er a g e c o s t of
$ 2 . 5 k p er t r a v el l i n g p a r t i c i p a n t
Y e a r 1 : U S $ 5 0 k
Y e a r 2 : U S $ 5 0 k
Y e a r 3 : U S $ 5 0 k
Y e a r 4 : U S $ 5 0 k
Y e a r 5 : U S $ 5 0 k
T o t a l : U S $ 2 5 0 k
S u p p or t t o
l e a d i n g c om p a ni e s t o
a c h i e v e pr e
q u a l i c a t i on
W ei g h t e d t o w a r d s t h e r s t h a l f of t h e
B u s i n e s s P l a n
A s s i s t a n c e d e p en d en t on s p e c i c n e e d s
of c om p a n y b u t b a s e d on t e c h ni c a l
a s s
i s t a n c en o t c a pi t a l i n v e s t m en t .A s -
s um e1 0 c om p a ni e s b en e t a n d e a c h
c om p a n y r e c ei v e s s u p p or t e q ui v a l en t t o
U S
$ 2 0 0 k s pr e a d o v er r s t 2 y e a r s
Y e a r 1 : U S $ 1 mn
Y e a r 2 : U S $ 1 mn
T o t a l : U S $ 2 mn
On g oi n g r e
s e a r c h i n t o d i m en s i on s of
ph a r m a m a
n uf a c t ur i n g s y s t em a n d c on-
t i n en t a l s t r a
t e g y d e v el o pm en t f or A P I
pr o d u c t i on , t r a d i t i on a l m e d i c i n e s , e t c .
( n o t e: b l o o d pr o d u c t w or k b ei n g c on-
d u c t e d s e p a r a t el y b y WH O.F i n d i n g s
c o ul d b ei n c or p or a t e d un d er P MP A a s
a d d i t i on a l a
c t i v i t y b u t n o t i n c l u d e d i n
t h i s i n d i c a t i v e b u d g e t )
R e s e a r c h f un c t i onh a s c on s i s t en t a nn u a l
b u d g e t
t h a t s t a r t s i n y e a r 2 .
D e
d i c a t e d P MP A s t a f f m em b er t o
m a
n a g er e s e a r c h a c t i v i t i e s ; wi l l r e q ui r e
ex p er t c on s ul t a n c i e s a n d ex p er t g r o u p
m e
e t i n g s . S u g g e s t e d b u d g e t of U S $ 2 5 0 k
p er y e a r .
Y e a r 1 : U S $ 0
Y e a r 2 : U S $ 2 5 0 k
Y e a r 3 : U S $ 2 5 0 k
Y e a r 4 : U S $ 2 5 0 k
Y e a r 5 : U S $ 2 5 0 k
T o t a l : U S $ 1 mn

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 113/119
99
ImplementatIon plan
4.5 monitoring anD eValuation
It would be premature to provide a detailed logical ramework or the PMPA as the spe-
cic activities to be conducted are subject to a number o variables including the detailedoutcome o discussions on the agreed action plan. That plan will include specic activities
to be undertaken by each party and metrics or assessing progress. However, a Monitoring
and Evaluation (M & E) philosophy, indicative key objectives and possible means by which
progress can be measured are identied in this section based on the undamental objectives
o the PMPA as articulated in the rst section o this Business Plan.
The key objectives should orm the basis o an approach to monitoring and evaluation
which should take into account that:
• This programme is intended to benet all member states
• The quality o pharmaceutical production should be raised to international GMP
standards and ultimately it should be a non-negotiable requirement that manuac-
turers must meet i they are to supply our people
• There is a need to expand the range o drugs that our manuacturers produce (sub-
ject to the manuacturer meeting international GMP standards)
• The industry must be sustainable in the long term and competitive whilst operating
to international standards
• NMRAs will be advised to limit the range o products that companies can produce
unless they meet GMP requirements
• There is a need to develop and implement coordinated strategies at the national level
• A undamental long term requirement is that regulatory capacity is strengthened
and that, in resource constrained environments, eorts are targeted at those aspects
o regulatory activities that are critical to protecting public health
• Some o our more advanced member states have well developed manuacturing sys-
tems but wish to reduce their reliance on imports and possibly develop/expand their
export markets to include those overseen by stringent regulatory authorities
• We have some companies that are prequalied or manuacture o products by WHO
and/or other stringent regulatory authorities and there are others who are striving
to achieve this milestone. We need to increase the number o internationally certi-
ed products rom Arican manuacturers (increased number o manuacturers and
broader product range)
This Business Plan underlines the act that the dierent countries on our continent cur-
rently ace a diverse range o realities. In view o this, the M & E approach should report
inormation at the national level as well as at continent level so that a true picture o the
progress in diverse situations is not lost through amalgamation o results at the continent
level. National level data will be a necessary component o strategy design and implementa-
tion in individual member states and it is important that this level o detail is also refected
in the overarching M & E or the PMPA.
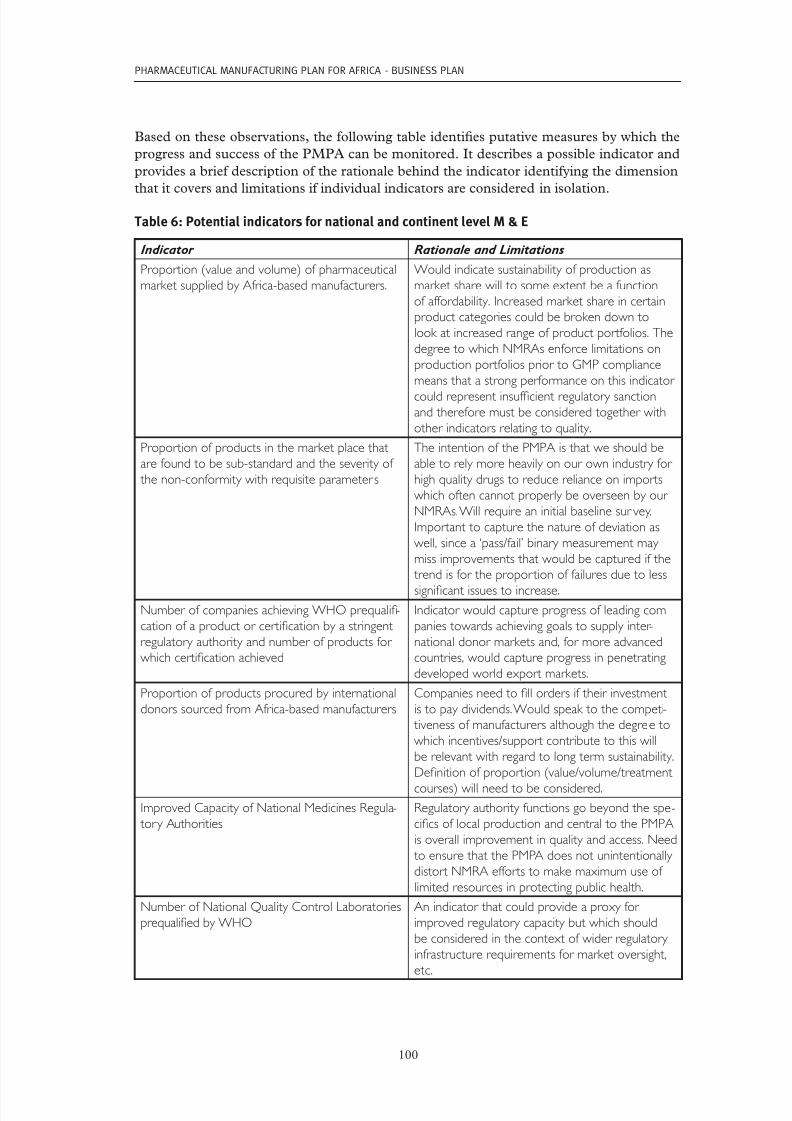
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 114/119
100
Pharmaceutical manufacturing Plan for africa - Business Plan
Based on these observations, the ollowing table identies putative measures by which the
progress and success o the PMPA can be monitored. It describes a possible indicator and
provides a brie description o the rationale behind the indicator identiying the dimension
that it covers and limitations i individual indicators are considered in isolation.
tb 6: P ds d v m & e
Indicator Rationale and Limitations
Proportion(valueandvolume)ofpharmaceutical
marketsuppliedbyAfrica-basedmanufacturers.
Wouldindicatesustainabilityofproductionas
marketsharewilltosomeextentbeafunction
ofaffordability.Increasedmarketshareincertain
productcategoriescouldbebrokendownto
lookatincreasedrangeofproductportfolios.The
degreetowhichNMRAsenforcelimitationson
productionportfoliospriortoGMPcompliance
meansthatastrongperformanceonthisindicator
couldrepresentinsufcientregulatorysanctionandthereforemustbeconsideredtogetherwith
otherindicatorsrelatingtoquality.
Proportionofproductsinthemarketplacethat
arefoundtobesub-standardandtheseverityof
thenon-conformitywithrequisiteparameter s
TheintentionofthePMPAisthatweshouldbe
abletorelymoreheavilyonourownindustryfor
highqualitydrugstoreducerelianceonimports
whichoftencannotproperlybeoverseenbyour
NMRAs.Willrequireaninitialbaselinesur vey.
Importanttocapturethenatureofdeviationas
well,sincea‘pass/fail’binarymeasurementmay
missimprovementsthatwouldbecapturedifthe
trendisfortheproportionoffailuresduetoless
signicantissuestoincrease.
NumberofcompaniesachievingWHOprequali-
cationofaproductorcerticationbyastringent
regulatoryauthorityandnumberofproductsfor
whichcerticationachieved
Indicatorwouldcaptureprogressofleadingcom-
paniestowardsachievinggoalstosupplyinter -
nationaldonormarketsand,formoreadvanced
countries,wouldcaptureprogressinpenetrating
developedworldexportmarkets.
Proportionofproductsprocuredbyinternational
donorssourcedfromAfrica-basedmanufacturers
Companiesneedtollordersiftheirinvestment
istopaydividends.Wouldspeaktothecompeti-
tivenessofmanufacturersalthoughthedegreeto
whichincentives/supportcontributetothiswill
berelevantwithregardtolongtermsustainability.
Denitionofproportion(value/volume/treatment
courses)willneedtobeconsidered.
ImprovedCapacityofNationalMedicinesRegula-
toryAuthorities
Regulatoryauthorityfunctionsgobeyondthespe-
cicsoflocalproductionandcentraltothePMPA
isoverallimprovementinqualityandaccess.Need
toensurethatthePMPAdoesnotunintentionally
distortNMRAeffortstomakemaximumuseof
limitedresourcesinprotectingpublichealth.
NumberofNationalQualityControlLaboratories
prequaliedbyWHO
Anindicatorthatcouldprovideaproxyfor
improvedregulatorycapacitybutwhichshould
beconsideredinthecontextofwiderregulatory
infrastructurerequirementsformarketoversight,
etc.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 115/119
101
ImplementatIon plan
Numberofcountriesthathavedevelopedandare
implementingstrategies
Implicitassumptionthatastrategyhasbeendevel-
opedthroughconsensusbuildingandthatthere
isdetailedengagementofallstakeholdersasthe
presenceofastrategyalonedoesnotmeasure thevalueoftheapproach.
Amountofcapitalinvestmentinpharmaceutical
manufacturingactivities
Aproxymeasureforthecredibilityoftheongoing
progressofthesectoranditsfutureviabilityas
providersofcapitalwillweighriskssuchasthreat
fromcounterfeitandsub-standardproductsin
theirinvestmentdecisions.
Numberofcountriesamendinglegislationto
incorporateTRIPSexibilitiesandthenumber
ofproductsonthemarketasaresultofexploit-
ingtheexibilitiesandpriceofproductsversus
originators
TRIPSexibilitiesrepresentanimportantoppor -
tunityforimprovingpublichealthandincorporat-
ingthelegislationisonestep;butthedegreeto
whichthistranslatesintoavailabilityofaffordable
versionsofpatentprotectedproductsinLeast
DevelopedCountries(LDCs)onourcontinentshouldalsobecaptured.Themeasureof‘price’
needscarefulconsiderationtoensurethatagenu-
inecomparisonismade.
Numberofindustryprofessionalstrainedacross
differentdisciplinesrequiredbythepharmaceutical
manufacturingsystem
Humanresourcedevelopmentiskeyandempiri-
calevidenceofprogresscanbecapturedthrough
thisindicator ;however,theabilityofthosetrained
toeffectchangeintheirrespectiveorganisa-
tionswillalsodependonintangibleaspectssuch
aschanging‘culture’oftheorganisationwhichis
implicitinanumberofmetricsrelatedtoquality
andcompetitiveness.
NumberofPartnershipsandBusinessLinkagesfacilitated
ThePartnershipandBusinessLinkagesPlatformwillcoveradiverserangeofpossiblerelationships.
TheimpactofthePMPAisintendedtoadjustthe
operatingcontextoftheindustrytomakeitmore
attractivetoinvestorsandencouragepartnerships,
etc.Anappropriatemetrictocapturethisdiversity
andtheindirectimpactofthePMPAwillrequire
furtherdeliberation.
Emergenceofsupportiveindustries Appearanceoflocalindustriesthat,forexample,
manufactureexcipientsandpackagingmaterialand
areabletoserviceandretoolequipment.These
supportiveindustrieswillbeessentialforthelong
termsustainabilityandcompetitivenessofourpharmaceuticalmanufacturers.
4.6 riSK management
This section reviews some key considerations and assumptions about the programme, iden-
ties potential risks or the successul implementation o the PMPA, and presents a risk
mitigation strategy including the necessary legal agreements and provisions and protections,
as well as the management and control o programme unds.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 116/119
102
Pharmaceutical manufacturing Plan for africa - Business Plan
The AUC is acutely aware that implementing a programme o this nature, with the myriad
o contexts on the continent, and the various ambitions and stages o development o com-
panies, is a challenging undertaking. This is especially so because most interventions will be
carried out by partners who have their own governance and internal dynamics. The poten-
tial risks to the success o the PMPA implementation thereore derive rom the ollowing:
• The risk that external players do not align behind the PMPA given that uncoordi-
nated vertical programmes can create distortions
• Interactions with stakeholders will lead to the evolution o the programme, the addi-
tion o new partners, the expansion o the package o solutions, and result in modi-
cations o partner roles. Some may nd the increasing or reducing responsibility
unacceptable
• The challenge o a number o organisations engaging in genuine collaboration and
maintaining this over the long term
• Funding shortalls leading to the abandonment o some key interventions or even
the inability to commence PMPA implementation
Ways in which the above risks can be mitigated include:
• Continuous stakeholder interactions and consultations
• Continuous monitoring and evaluation o project implementation and reporting to
ensure that adjustments and corrective actions are taken or that interventions that
do not work are abandoned
• Open communication and reporting to the AUC PMPA Technical Committee and
all partners and stakeholders so that they are kept abreast o all developments
• Regular coordination meetings
• Governance and controls should be in place and should regulate all aspects o pro-
gramme management, including use o nancial resources
4.7 SummarY o chaPter 4Key messages rom this Chapter include:
• The implementation o this Business Plan will require a diverse range o skills, ex-
pertise and organisational mandates; no one entity can cover them all
• It is recommended that a consortium is established and genuine collaboration be-
tween partners will be essential
• UNIDO has been requested to assist the AUC to build the consortium
•
Initial discussions have taken place with potential partners; during the initial phaseo the Business Plan, detailed negotiations will take place, legal arrangements will be
7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 117/119
103
ImplementatIon plan
established and the consortium will work together to establish a detailed work plan
• The initial or ‘set up’ phase o this Business Plan will also involve urther develop-
ment o the solutions package, resource mobilization and an invitation to our mem-
ber states to express interest in working with the AUC and its partners under the
PMPA
• The consortium will o necessity be limited in size so inevitably there will be many
stakeholders who are conducting related work and with whom collaboration and
alignment with the PMPA will be important. In view o this, the AUC and its part-
ners will ensure during implementation that channels o communication with the
wide array o players are kept open and that there are opportunities or regular ace-
to-ace-interaction
• A pilot phase is suggested as there are a number o countries that have already devel-
oped strategies or the sector and who would be in a position to benet rom detailedimplementation by the consortium
• Prior to implementation in other countries, a detailed strategy development process
will be conducted in each one (as described in Chapter 3) prior to ull scale imple-
mentation
• Experience suggests that coordination across stakeholders at the national level is
necessary and an implementation structure that includes dedicated PMPA eld co-
ordinators is recommended
• A complete budget proposal or the implementation o the Business Plan will de-
pend on the details o the action plan to be developed by the consortium partners.However, an indicative budget is proposed which estimates that over a ve year pe-
riod US$54mn will be required
• Indicative indicators have been suggested and the rationale and limitations o these
indicators discussed. A detailed logical ramework will be produced to capture the
details o the action plan and the measures by which it will be monitored and evalu-
ated
• Risks to the eectiveness o this Business Plan are highlighted and include the chal-
lenge o maintaining a unctioning consortium o parties over an extended period
o time. This is an issue that will benet rom continuous dialogue, regular meetings
and monitoring and evaluation activities.

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 118/119
104

7/28/2019 Business Plan Nov2012 eBook
http://slidepdf.com/reader/full/business-plan-nov2012-ebook 119/119
Printed in AustriaV1-November 2012