by lucy abdel mabood suliman lecturer of chest diseases faculty of medicine, mansoura university
TRANSCRIPT
APAPAutomatic positive air way
pressure for OSABy
Lucy Abdel Mabood sulimanLecturer of Chest Diseases
Faculty of Medicine, Mansoura University

Obstructive Sleepapnea (OSA) is avery common disorder affecting 2%-4% of the adult population.
CPAP is a standard, safe, and efficacious treatment for the obstructive sleep apnea syndrome
Introduction

CPAP APAP fixed BIPAP Auto BIPAP AVAPS IVAPS ASV
PAP DEVICES USED IN OSAS

TECHNOLOGY OF APAP

TECHNOLOGY OF APAP
The functioning of APAP devices can be broken down into three components:
sensing of events of SRBD (sensors) automated computing and analysis of
the sensed signals (analysis) set of algorithms that will determine
the action taken by the APAP device in response to the conditions exposed (effectors).

TECHNOLOGY OF APAP In the older generation of APAP devices,
the sensors were simplistic and measured only the pressure inflections (vibrations) of a certain frequency and amplitude that were caused by snoring.
The next generation of APAP devices became more sophisticated and were able to sense flow-based changes such as apnea, hypopnea, or inspiratory flow limitation based upon the inspiratory flow contour.

Indictions of Auto CPAP
1-Auto-titration PAP to determine an
effective fixed level of CPAP)
2-Auto-adjusting CPAP for chronic
treatment with the advantage of
delivering the lowest effective
pressure in any circumstance.

The devices typically monitor one or more of the following: airflow (or motor speed), airflow profile (flattening), snoring (airway vibration), or airway impedance (forced oscillation technique).
The algorithms used to adjust pressure are proprietary Depending on the type of respiratory event that is detected the delivered pressure is increased by a certain amount.
Technique of Auto-Titration

Open unrestricted airway

Silent partial airway obstruction

Noisy partial airway obstruction

Complete airway obstruction
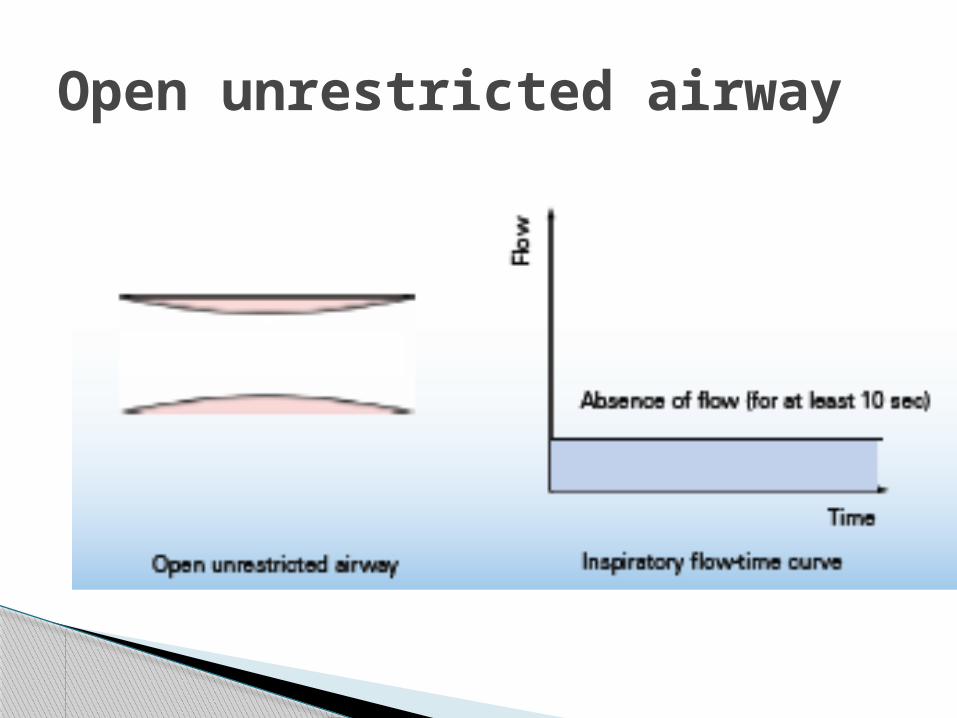
Open unrestricted airway

Most APAP devices start with a baseline pressure (usually around 3-4 cm H2O) and then titrate upward as needed.
An absence of monitored events then prompts a gradual decrease in pressure. This allows the minimum effective pressure to be delivered
The APAP devices usually allow the clinician to set maximum and minimum pressure limits.
Technique of Auto-Titration

APAP devices allow transfer of pressure over time information to a computer for:-
percentage of time at each pressure (Pmean, P95, and Pmaximum)
detailed information such as leak and persistent apnea/hypopnea counts
The ability to store more than one night of data is useful, as more than one night may be needed to effectively select an appropriate
fixed pressure

This mode allows a reduction in pressure during early expiration with a return to the current set pressure at end expiration.
This feature could improve patient tolerance to pressure.
Expiratory pressure relief
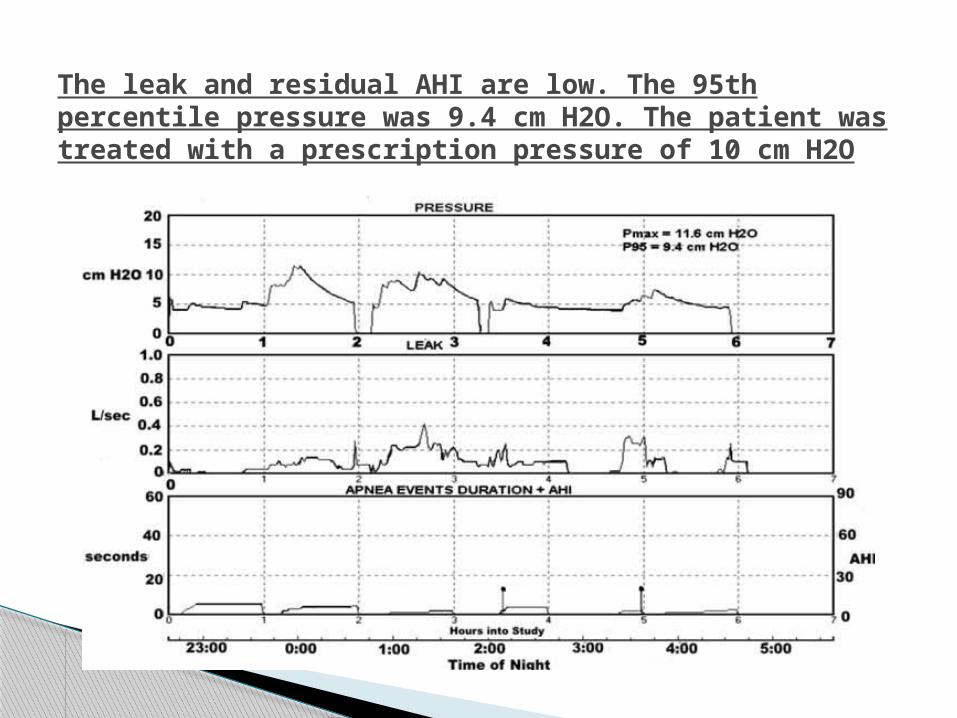
The leak and residual AHI are low. The 95th percentile pressure was 9.4 cm H2O. The patient was treated with a prescription pressure of 10 cm H2O

The leak is very high. The pressure increased to the upper limit (16 cm H2O) and remained there for most of the night. The AHI was also elevated. This titration would need to be repeated with a better mask seal.


Problems of APAP
mask/mouth leak Tend to raise the baseline flow delivered by
blower units and diminish the variations in flow during inspiration and expiration, The resulting airflow signal may be interpreted as an apnea or hypopnea and prompt an increase in pressure that may further increase leak
APAP estimated that leak exceeded 0.4L/s on average for 10% of a supervised night and 15% on an unsupervised night.

Central apneas Central apnea during APAP ,Central apneas
of the Cheyne-Stokes type are common in patients with severe congestive heart failure (CHF) and also can occur in patients with neurological diseases.

Many devices have algorithms that limit pressure increases when leak exceeds certain values or when increases in blower speed no longer result in increases in mask pressure.
some devices have leak alarms that could prompt the patient/staff to readjust the mask.
Mouth leaks could be approached by treating nasal congestion, using heated humidification, chin straps, or using a mask covering the nose and mouth.
How to solve mask leak problem?????

Some device manufacturers have attempted to identify central apnea by detecting cardiac oscillations in the airflow tracing (open airway apnea).
However, the airway can close in central apnea.
Others have designed algorithms that limit the pressure increases for apnea in the absence of associated snoring or airflow limitation.
However, the problem persists in some patients and many of the reviewed clinical trials excluded patients with congestive heart failure.
Central apnea problem solving

When an apnea has been detected, small oscillations in pressure (1 cm H2O peak-to-peak at 4 Hz) are added to the current device pressure. The CSA algorithm uses the resulting flow and pressure (determined at the mask) to measure the airway patency.
Forced oscillation technique
This could be performed as an attended study (which allows technologist intervention)
or as an unattended study either in the sleep laboratory or at home
Interventions for mask leaks and the treatment of persistent hypoxemia despite apatent airway with supplemental oxygen would be possible.
However, performing unattended CPAP titration in the sleep laboratory or home is potentially the most useful application of APAP devices.

The second potential use for APAP devices is for chronic treatment of OSA.
The difference in pressures needed in REM and NREM (body position , sleep stages)also determines the potential for differences in mean pressure between APAP and CPAP treatment
Chronic Treatment of OSA with APAP


Recommendations

APAP is not recommended to diagnose OSA. (Standard)
Patients with congestive heart failure, significant lung disease such as chronic obstructive pulmonary disease, patients expected to have nocturnal arterial oxyhemoglobin desaturation due to conditions other than OSA (e.g., obesity hypoventilation syndrome), patients who do not snore (either naturally or as a result of palate surgery), and patients who have central sleep apnea syndromes are not currently candidates for APAP titration or treatment. (Standard)

APAP devices are not currently recommended for split-night titration. (Standard)
Certain APAP devices may be used during attended titration with polysomnography to identify a single pressure for use with standard CPAP for treatment of moderate to severe OSA. (Guideline)

Certain APAP devices may be initiated and used in autotitration and unattended treatment of patients with moderate to severe OSA without significant comorbidities (CHF, COPD, central sleep apnea syndromes, or hypoventilation syndromes). (Option)

A reevaluation and, if necessary, a standard attended CPAP titration should be performed if symptoms do not resolve or if the APAP treatment otherwise appears to lack efficacy .(Standard)
