by : m. sha`bani md tb is caused by bacteria of the m. tuberculosis complex & usually affects...
TRANSCRIPT


TUBERCULOSISBY : M. SHA`BANI MD

TB is caused by bacteria of the M. Tuberculosis complex & usually affects lung.
If treated,is curable
If unreated ,may fatal within 5 y/o in 50-65% of cases

M. Tuberculosis is a rod shape ,nonspore-forming,aerobic
Acid- fast bacili (AFB )

TB is spread person to person through the air via droplet nuclei
M. tuberculosis may be expelled when an infectious person:◦ Coughs◦ Sneezes◦ Speaks ◦ Sings
Transmission occurs when another person inhales droplet nuclei
FROM EXPOSURE TO INFECTION
The most infectious patients :cavitary, laryngeal,sputum containing 105 – 107
AFB/ml Q: Are co-infected patients(HIV + TB) highly
infectious?

Depends on innate immunologic and non –immuonologic defenses and function of CMI
Primary disease : children and immunocompromsed persons
Secondary ( postprimary) TB dormant bacilli may persist for years before reactivation to produce this type .
Up to 10% of infected persons will develop active TB ( esp. in HIV patients)
FROM INFECTION TO DISEASE

Pathogenesis is defined as how an infection or disease develops in the body.
TB Pathogenesis (1)
Occurs when tubercle bacilli are in the body, but the immune system is keeping them under control
Detected by the Mantoux tuberculin skin test (TST) or by blood tests such as interferon-gamma release assays (IGRAs) which include:
◦ QuantiFERON®-TB Gold test (QFT-G)◦ QuantiFERON®-TB Gold In-Tube (QFT-GIT)◦ T-Spot®.TB test (T-SPOT)
People with LTBI are NOT infectious
TB Pathogenesis (2)Latent TB Infection (LTBI)

Develops when immune system cannot keep tubercle bacilli under control
◦ May develop very soon after infection or many years after infection
About 10% of all people with normal immune systems who have LTBI will develop TB disease at some point in their lives
People with TB disease are often infectious
TB Pathogenesis (3)TB Disease

Tubercle bacilli multiply in alveoli, where
infection begins
bronchioleblood vessel
tubercle bacilli
a lveoli
2
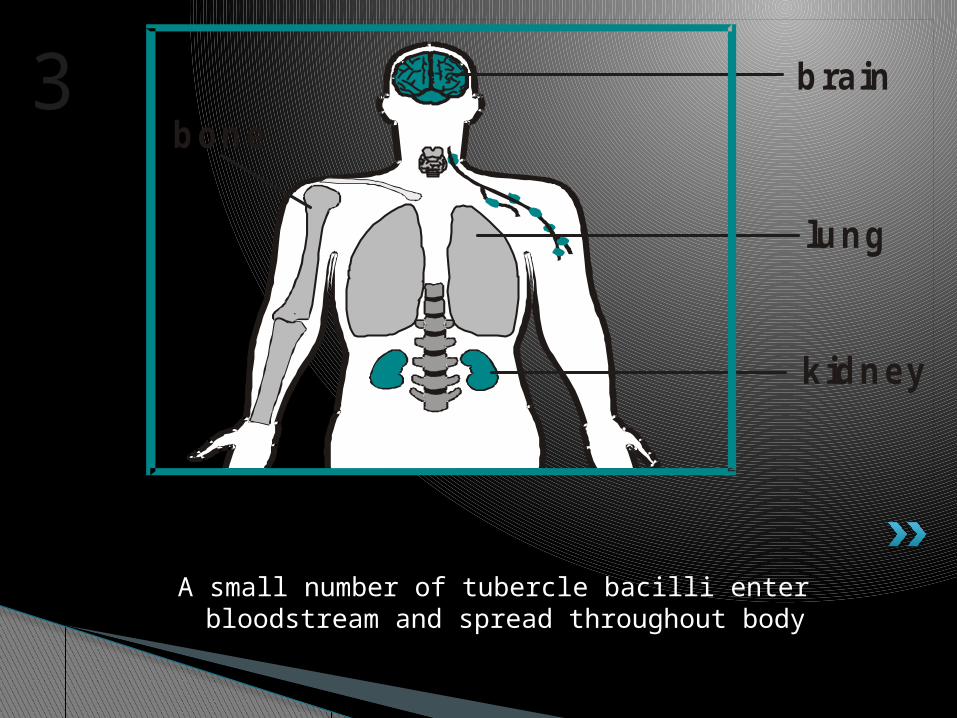
A small number of tubercle bacilli enter bloodstream and spread throughout body
brain
lung
kidney
bone3
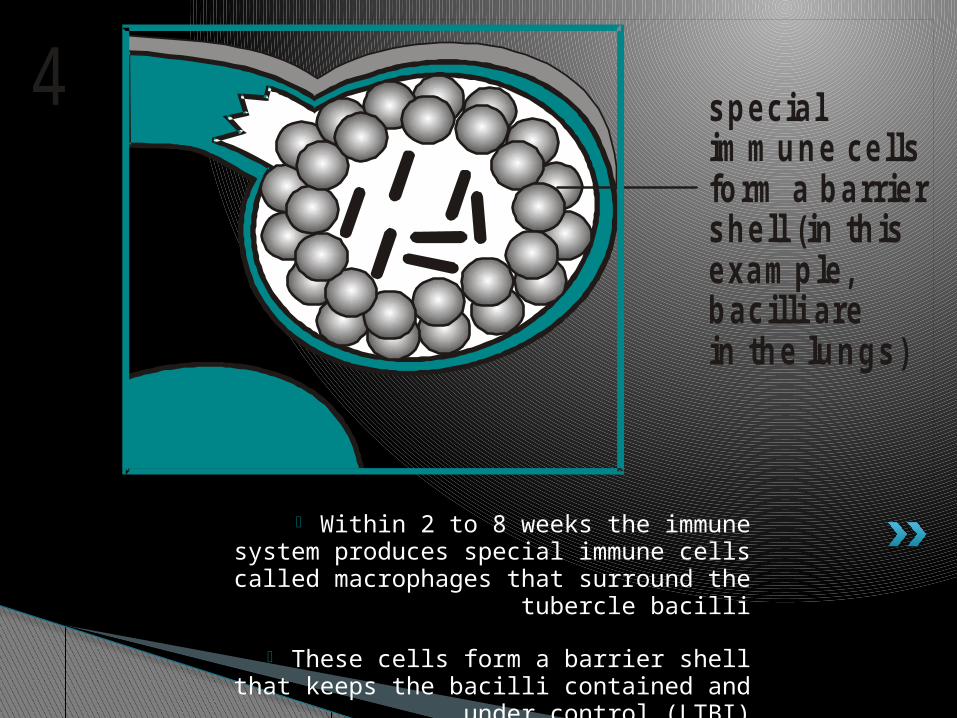
• Within 2 to 8 weeks the immune system produces special immune cells called
macrophages that surround the tubercle bacilli
• These cells form a barrier shell that keeps the bacilli contained and under control
(LTBI)
specialim m une cells form a barrier shell (in th isexam ple,bacilli arein the lungs)
4

• If the immune system CANNOT keep tubercle bacilli under control, bacilli begin
to multiply rapidly and cause TB disease
• This process can occur in different places in the body
shell breaks down and tuberclebacilli escape
m ultip ly(in th is exam ple,TB d isease develops in the lungs)
and
5

Latent TB Infection (LTBI) TB Disease (in the lungs)
Inactive, contained tubercle bacilli in the body
Active, multiplying tubercle bacilli in the body
TST or blood test results usually positive
TST or blood test results usually positive
Chest x-ray usually normal Chest x-ray usually abnormal
Sputum smears and cultures negative Sputum smears and cultures may be positive
No symptoms Symptoms such as cough, fever, weight loss
Not infectious Often infectious before treatment
Not a case of TB A case of TB

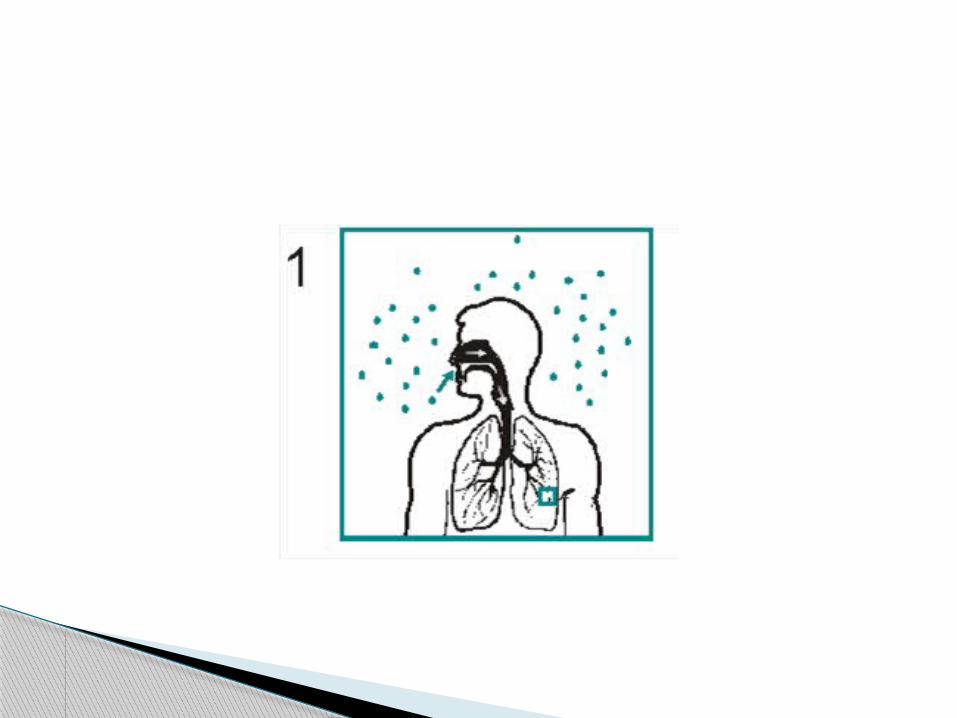
When a person inhales air that contains droplet nuclei containing M. tuberculosis, where do the droplet nuclei go? (pg. 15)
• Most of the larger droplet nuclei become lodged in the upper respiratory tract, where infection is unlikely to develop
• However, droplet nuclei may reach the small air sacs of the lung (the alveoli), where infection begins
TB PathogenesisStudy Question

After the tubercle bacilli reach the small air sacs of the lung (the alveoli), what happens to them? (pg. 15)
Tubercle bacilli multiply in alveoli and some enter the bloodstream and spread throughout the body
Bacilli may reach any part of the body
Within 2 to 8 weeks, the immune system usually intervenes, halting multiplication and preventing further spread
TB PathogenesisStudy Question

In people with LTBI (but not TB disease), how does the immune system keep the tubercle bacilli under control? (pg. 15)
The immune system produces special immune cells that surround the
tubercle bacilli. These cells form a shell that keeps the bacilli contained and under control.
TB PathogenesisStudy Question
How is LTBI detected? (pg. 16)
LTBI is detected by the Mantoux tuberculin skin test (TST) or blood tests such as interferon-gamma release assays (IGRA), which include the QuantiFERON®-TB test (QFT-G), QuantiFERON®-TB Gold In-tube (QFT-GIT), or T-SPOT.
TB PathogenesisStudy Question

Some conditions increase probability of LTBI progressing to TB disease

In an HIV-infected person,
TB can develop in one oftwo ways:
Person with LTBI becomes infected with HIV and then develops TB disease as the immune system is weakened
Person with HIV infection becomes infected with M. tuberculosis and then rapidly develops TB disease
Progression to TB Disease TB and HIV

PULMONARY dis.: Primary dis.: 1-asymptomatic 2-fever and pleuritic c.p. -in children -middle and lower lobes -Ghon focus(after initial inf. –peripheral-hilar
or paratracheal LAP-heals spontaneously and calcified noduls)
-EN in legs
CLINICAL MANIFESTATIONS
In young child or immunosuppressed person pulmonary TB (Primary ) progress to clinical illness
PE :2/3 Cavity+ LAP Enlarged LN then... Rupture of LN and ... Hematogen distribution

Post-primary dis. : Reactivation Apex Small infiltrations to large cavities What happens? up to 1/3 will be severe others (ends to
remission or chronicity)

symptoms: -nonspecific and slowly -eventually up to 90% ,cough -C.P. -dyspnea Signs:most of them ,normal but may have
inspiratory rales and occasionally rhonchiThe most common hamatologic findings:
Mild anemia, leukocytosis, thrombocytopenia

In order of frequency: L.N., pleura, GU, skeletal, mening, peritonum and pericardium
Lympadenitis: nontender swelling ,posterior cervical and supraclavicular( scrofula) ,
Systemic signs are ucommon unless in HIV FNA or excisional Bx
EXTRAPULMONARY TB

Pleural TB : 1-postprimary 2-chronic 3-with miliary 4-empyema Dx: thoracentesis, needle bx of pleura The first one responds rapidly to chemo. For empyema surgical drainage + chemo.

Genitourinary TB Skeletal TB Meningitis and tuberculoma Gastrointestinal TB

Miliary TB -Hematogenous spread of bacilli -granuloma 1-2 mm lesions ( as millet
seeds) Nonspecific manifestations Fever,night sweat, anorexia,wt loss 1-acute 2-cryptic 3-nonreactive Dx: BAL, TBB, Bx of involved organs

A person with a pos. PPD who acquires HIV has a risk of 3-13% /year for active TB
prsentation depends onstage of HIV Extrapulmonary TB is common Dx is difficult because...(smear,radiography
granuloma,PPD)
HIV- associated TB
1-AFB MICROSCOPY ( microscopic exam of a diagnostic
specimen,e.g. sputum,tissue) Sputum: x3 in morning ( but 2 sample on
the same visit is better than 3 samples) Tissue: in normal saline( not in
formaldehyde)
DIAGNOSIS

CULTURE : because most mycobacterias grow slowly 4-
8 weeks may be required The most sensitive test PCR, radiography,invasive procedures

PPD: False negative in
immunosuppression ,malnutrition False positive in non-TB mycobacteria , BCG
vaccination IFN-gamma release assay( IGRA): It measures T cell release of IFN-gamma in
response to stimulation with the highly TB-specific antigen ESAT-6 AND CFP-10
It is more specific than PPD esp. in low-incidence setting
DIAGNOSIS OF LATENT INFECTION

4 major drugs are the first line agents : Isoniazid,rifampin ,pyrazinamide,ethambuto
l Monitoring : bacteriologic evaluation( if cx
not possible then AFB smear) Serial CXR is not recomended Drug toxicity: (patient should be educated
about hepatitis , hypersensitivity reaction, hyperuricemia and arthralgia,thrombocytopenia,optic neuritis
TREATMENT

For preventing active dis.( chemoprophylaxis) Candidates are : 1- HIV, recieving immunosuppressive
drugs,close contact, fibrotic lesions on CXR with at least 5 mm
2- recently infected persons, high risk condition( DM,hematologic dis., IDU, ESRD,,rapid wt loss) with at least 10 mm
3-low risk persons with at least 15 mm( except for employment purposes TST is not indicated for low-risk group)
Tx of latent TB infection
THANK YOU
QUESTION?



















