by prof. el sayed abdel fattah eid lecturer of internal
TRANSCRIPT

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Endocrinology
By
Prof. El Sayed Abdel Fattah Eid
Lecturer of Internal Medicine Delta University
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Diabetes Mellitus
Definition: Diabetes mellitus comprises a heterogeneous group of metabolic diseases that arecharacterized by chronic hyperglycemia anddisturbances in carbohydrate, lipid, andprotein metabolism. Its Prevalence is increased worldwide (epidemic) because of obesity and sedentarylife in both adults, adolescent and children. These adolescents may present in DKA,and then behave like type 2 Presentation:
Type 1: classic acute symptoms:
- Hyperglycemia - Polydipsia - Polyuria - weight loss - polyphagia - blurred vision - and pruritus - 25% present the first time with DKA.
Type 2:
the disease is often present for many years before diagnosis: - Chronic hyperglycemia - impairment of growth - susceptibility to infections - slow wound healing.
Classification: - Type 1 diabetes (Immune mediated or Idiopathic) - Type 2 diabetes: (Insulin resistance) - Gestational diabetes mellitus - Other specific types : * Genetic defects of β-cell function * Genetic defects in insulin action * Diseases of the exocrine pancreas (chronic pancreatitis) * Endocrinopathies (cushing, acromegaly, thyrotoxicosis ) * Drug- or chemical-induced (steroid ) * Infections * Anti-insulin receptor antibodies * Other genetic syndromes sometimes associated with diabetes
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
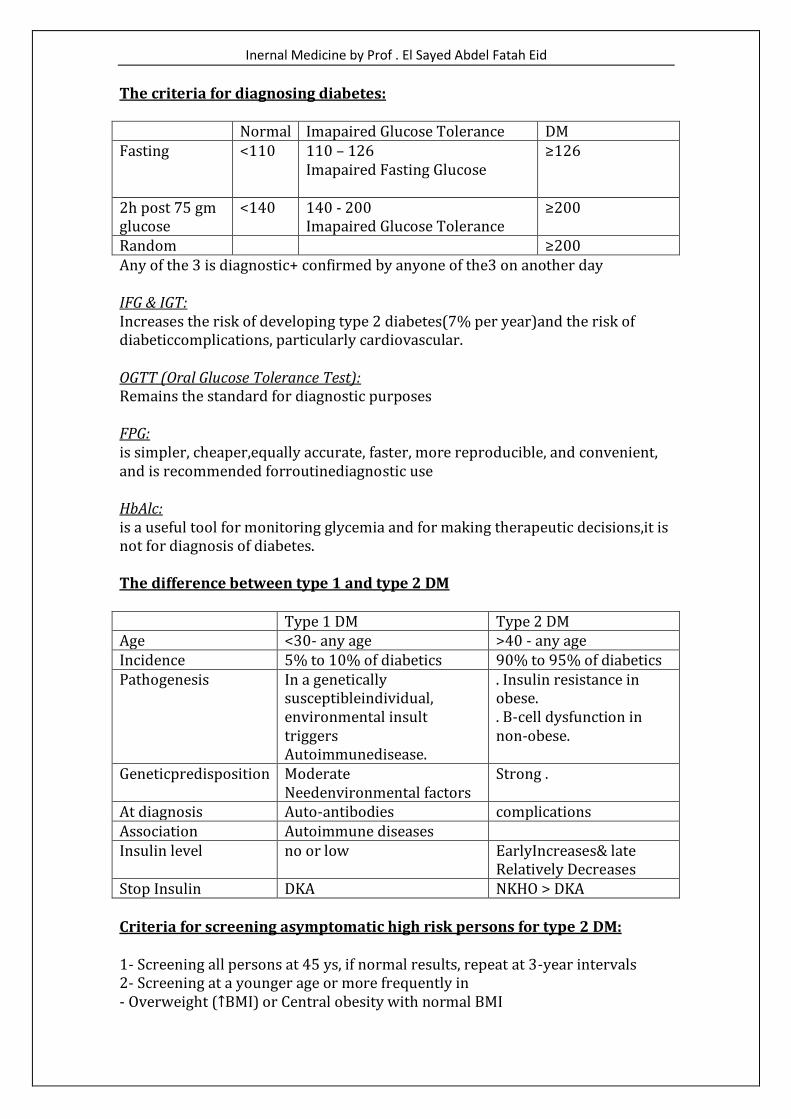
The criteria for diagnosing diabetes: Normal Imapaired Glucose Tolerance DM Fasting <110
110 – 126 Imapaired Fasting Glucose
≥126
2h post 75 gm glucose
<140 140 - 200 Imapaired Glucose Tolerance
≥200
Random ≥200 Any of the 3 is diagnostic+ confirmed by anyone of the3 on another day IFG & IGT: Increases the risk of developing type 2 diabetes(7% per year)and the risk of diabeticcomplications, particularly cardiovascular. OGTT (Oral Glucose Tolerance Test): Remains the standard for diagnostic purposes FPG: is simpler, cheaper,equally accurate, faster, more reproducible, and convenient, and is recommended forroutinediagnostic use HbAlc: is a useful tool for monitoring glycemia and for making therapeutic decisions,it is not for diagnosis of diabetes. The difference between type 1 and type 2 DM Type 1 DM Type 2 DM Age <30- any age >40 - any age Incidence 5% to 10% of diabetics 90% to 95% of diabetics Pathogenesis In a genetically
susceptibleindividual, environmental insult triggers Autoimmunedisease.
. Insulin resistance in obese. . B-cell dysfunction in non-obese.
Geneticpredisposition Moderate Needenvironmental factors
Strong .
At diagnosis Auto-antibodies complications Association Autoimmune diseases Insulin level no or low EarlyIncreases& late
Relatively Decreases Stop Insulin DKA NKHO > DKA Criteria for screening asymptomatic high risk persons for type 2 DM: 1- Screening all persons at 45 ys, if normal results, repeat at 3-year intervals 2- Screening at a younger age or more frequently in - Overweight (↑BMI) or Central obesity with normal BMI

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
- First-degree relative with diabetes - Members of a high-risk ethnic population - Bad Obstetric History(delivering a large baby, perinatal death or GDM) - Hypertensive - HDL cholesterol<35 mg/dL and/or TG >250 mg/dL - IFG or IOT Screening for Gestational diabetes mellitus 50 gm glucose (Screening) 100 gm glucose (Diagnostic) FBS 95 1h 140 180 2h 155 3h 140 (Any 2 are diagnostic). Gestational diabetes mellitus (GDM)
- GDM affects 2% to 5% of all pregnancies (up to 14%) - Screening between 24 and 28 weeks - For all women> 25 years old - For younger women with high risk to develop type 2 - Women at very high risk should be screened at their initial obstetric visit. - A Positive 50-g glucose screening test indicates 3-hour, l00 gm OGTT - Follow up after 6 weeks postpartum - 25% of lean women & 50% of obese women develop diabetes over a
2Oys.
Management: l-Nutrition: Balanced, healthy diet: - 10% to 20% protein + < 30% fat + 50% to 60% carbohydrate. - Soluble fiber delays carbohydrate absorption and improves lipid profiles. 2-Weight management therapy 3-Exercise management therapy : - Regular, moderate physical activity for at least 30 minutes/day. - No Exercise if FPG >250 mg/dL with ketones, or >300 mg/dL without ketones - Self blood glucose montoring (SBGM) should be performed befor& after exercise. 4-Tight control of blood pressure to 130/85 5-Tight control of blood sugar : - DCCT Study (type 1 diabetes) showed that intensive treatment prevented or slowed theonset and/or progression of the microvascularcomplications:
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
retinopathy by 76%,neuropathy by 60%, and proteinuria by 54% with increase in hypoglycemia. - UKPDS Study (type 2 diabetes) showed an overall reduction inmicrovascularcomplications of 25% with tight control. Insulin therapy: Indication 1. Type 1 diabetics 2. Type 2 not responding to oral treatment 3. Infections 4. Surgery. 3. Gestational diabetes. Insulin regimens
- Starting doses 0.15 to 0.5 U/kg/day up to 1.5 U/kg in severe IR. - The dose is increased during intercurrent illness, pregnancy & growing
child. - A split or mixed regimen of NPH/regular twice daily (2/3 of the dose
beforebreakfast and 1/3 before dinner; at each time 2/3 NPH and 1/3 regular)
- Bedtime insulin (NPH) and daytime sulfonylurea therapy for type 2 diabetes
Other Antihyperglycemic agents Sulfonylureas: - insulin secretagogue - Glibenclamide, Glicilazide, Glipizide&Glimipride - They stimulate beta cells to secrete insulin - Side effect: Hypoglycemia & Weight gain. Biguanides (Metformin) - Insulin Sensitizers - Increases Hepatic glucose production by inhibiting gluconeogenesis. - Increases Glucose uptake and utilization by muscle. - Decreases Intestinal glucose absorption. - Decreases Weight & Lipids - Side effects: Gastrointestinal upsets & Lactic acidosis with advanced
hepatic & renal disease
Alpha-Glucosidase inhibitors - Antagonizing pancreatic amylase; so they Decrease Postprandial glucose. - It is taken with the first bite of a carbohydrate-containing meal - Side effects: Diarrhea and flatulence.
Thiazolidinediones (Insulin Sensitizers) - Decreases Insulin resistance so used in obese patients - Pioglitazone & roseglitazone - Decrease lipids - No hypoglycemia.
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
- Side effects: Liver dysfunction (elevate liver enzymes), edema & weight gain .
Meglitinides: - Insulin secretagogue - As sulfonylureas so not combined with sulfonylurea. - taken with meals and is omitted in the absence of a meal Complications of DM: Acute complications of DM:
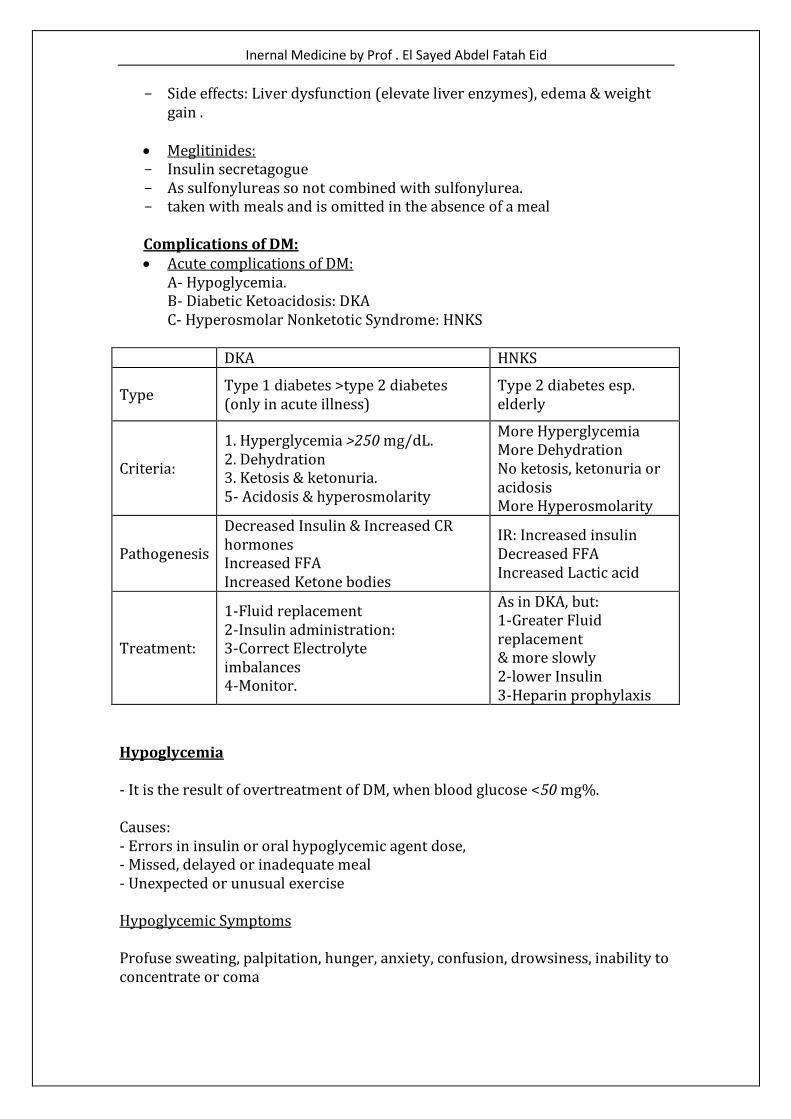
A- Hypoglycemia. B- Diabetic Ketoacidosis: DKA C- Hyperosmolar Nonketotic Syndrome: HNKS
DKA HNKS
Type Type 1 diabetes >type 2 diabetes (only in acute illness)
Type 2 diabetes esp. elderly
Criteria:
1. Hyperglycemia >250 mg/dL. 2. Dehydration 3. Ketosis & ketonuria. 5- Acidosis & hyperosmolarity
More Hyperglycemia More Dehydration No ketosis, ketonuria or acidosis More Hyperosmolarity
Pathogenesis
Decreased Insulin & Increased CR hormones Increased FFA Increased Ketone bodies
IR: Increased insulin Decreased FFA Increased Lactic acid
Treatment:
1-Fluid replacement 2-Insulin administration: 3-Correct Electrolyte imbalances 4-Monitor.
As in DKA, but: 1-Greater Fluid replacement & more slowly 2-lower Insulin 3-Heparin prophylaxis
Hypoglycemia - It is the result of overtreatment of DM, when blood glucose <50 mg%. Causes: - Errors in insulin or oral hypoglycemic agent dose, - Missed, delayed or inadequate meal - Unexpected or unusual exercise Hypoglycemic Symptoms Profuse sweating, palpitation, hunger, anxiety, confusion, drowsiness, inability to concentrate or coma
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Hypoglycemia Management - It depends on the severity and whether the pt. is conscious and able to swallow - Oral carbohydrates if hypoglycemia is recognized early - IV glucose (30-50 ml of 50% dextrose) glucagone (1 mg I.M) should be given - As soon as the pt. is able to swallow, glucose should be given orally Chronic Complications of DM - Diabetes is the sixth leading cause of death - Diabetes is a cause of 18% of all deaths in people over 25s of age - Diabetes is the leading cause of ESRD, New cases of blindness and non-traumatic lower limb amputations. - Cardiovascular disease is the major cause of diabetes-related death - Cardiovascular disease is 2-4 times in diabetics >normal population - In diabetics; Increased risk of stroke - In diabetics; Life expectancy reduced by 5 to 10 years. Microvascular Complications They are either diabetic neuropathy,diabetic nephropathy or diabetic retinopathy Mechanisms: - Accumulation of sorbitol - Advanced glycation end products (AGE) - Increased oxidative damage - Hyperinsulinemia, hyperviscosity & platelet dysfunction - Activation of various growth factors
Diabetic Retinopathy (DR) - Either proliferative or non-proliferative DR - Comprehensive fundus exam at time of diagnosis as evidence shows some patients may have retinopathy at diagnosis (type 2 and after 5 years in type 1 DM) - The frequency of follow-up- consensus is yearly with more frequent follow-up of abnormal findings
Diabetic Neuropathy - Peripheral neuropathies either sensory (commonest), motor or autonomic - Sensory neuropathy may be presented by pain, paresthesias or loss of sensation - Autonomic neuropathy may be presented by postural hypotension, gastroparesis, diarrhea or impotence
Diabetic Nephropathy - It may be presented glomerular lesions lesdmg to persistent albuminuria which progress to end stage renal failure - Yearly screening for microalbuminuria is essential for early detection
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Treatment of Microvascular Complications - Prevention is the Key - Good Glycemic control - Hypertension control < 135/75 mm Hg - Smoking cessation - Weight reduction - Lipid control - Aggressive treatment of co-risk factors - Regular Exams (fundus, sensory, MIA, ECG, KFT) - Low-dose aspirin
Macrovascular Complications of DM They are either cardiovascular disease, cerebrovascular disease or peripheral vascular disease. Mechanism: Atherosclerosis & Risk factors: • Dyslipidemia • Hypertension • Obesity • Hyperglycemia Management of chronic diabetic Complications: • Aggressive treatment of hypertension <130/85 mm Hg, • Use ACEI or ARB for renal protection. • B-Blockers • Low-dose aspirin • Cessation of smoking • Management of obesity • Treat Dyslipidemia:
- goals: . LDL cholesterol <100 mgldL . TG <200 mg/dL . HDL >45 mg/dL for men &>55mg/dL for women
• Safe exercise .
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
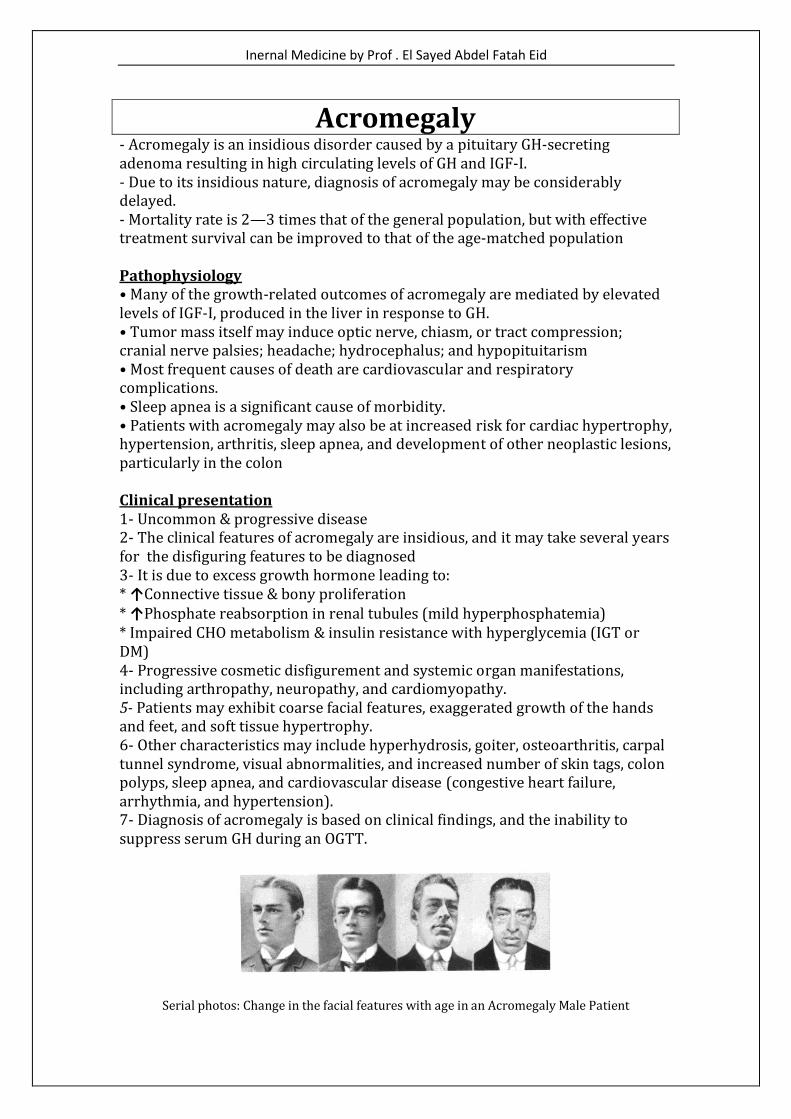
Acromegaly - Acromegaly is an insidious disorder caused by a pituitary GH-secreting adenoma resulting in high circulating levels of GH and IGF-I. - Due to its insidious nature, diagnosis of acromegaly may be considerably delayed. - Mortality rate is 2—3 times that of the general population, but with effective treatment survival can be improved to that of the age-matched population Pathophysiology • Many of the growth-related outcomes of acromegaly are mediated by elevated levels of IGF-I, produced in the liver in response to GH. • Tumor mass itself may induce optic nerve, chiasm, or tract compression; cranial nerve palsies; headache; hydrocephalus; and hypopituitarism • Most frequent causes of death are cardiovascular and respiratory complications. • Sleep apnea is a significant cause of morbidity. • Patients with acromegaly may also be at increased risk for cardiac hypertrophy, hypertension, arthritis, sleep apnea, and development of other neoplastic lesions, particularly in the colon Clinical presentation 1- Uncommon & progressive disease 2- The clinical features of acromegaly are insidious, and it may take several years for the disfiguring features to be diagnosed 3- It is due to excess growth hormone leading to: * ↑Connective tissue & bony proliferation * ↑Phosphate reabsorption in renal tubules (mild hyperphosphatemia) * Impaired CHO metabolism & insulin resistance with hyperglycemia (IGT or DM) 4- Progressive cosmetic disfigurement and systemic organ manifestations, including arthropathy, neuropathy, and cardiomyopathy. 5- Patients may exhibit coarse facial features, exaggerated growth of the hands and feet, and soft tissue hypertrophy. 6- Other characteristics may include hyperhydrosis, goiter, osteoarthritis, carpal tunnel syndrome, visual abnormalities, and increased number of skin tags, colon polyps, sleep apnea, and cardiovascular disease (congestive heart failure, arrhythmia, and hypertension). 7- Diagnosis of acromegaly is based on clinical findings, and the inability to suppress serum GH during an OGTT.
Serial photos: Change in the facial features with age in an Acromegaly Male Patient

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Serial photos: Change in the facial features with age in an Acromegaly Female Patient
Symptoms of Acromegaly
Normal foot vs. Acromegalic foot Normal hand vs. Acromegalic hand
Investigation 1- Blood glucose & serum phosphate levels 2- Plain x ray skull, hands and feet 3- Serial photos
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
4- Elevated GH level non-suppressible after OGTT’ (GH levels will remain above 2 ng/mL). 5- In contrast to GH levels, plasma levels of IGF-I are more stable, and an elevated IGF-I level in a patient with appropriate clinical suspicion is almost always indicative of acromegaly. 6- Other pituitary hormones 7- Pituitary Imaging: pituitary adenoma should be confirmed using MRI. 90% of acromegalic patients have tumors larger than 1 cm. Treatment Goals Primary goal of treatment is to normalize GH levels. Surgical Treatment Surgical tumor excision (trans-sphenoidal) is indicated for most patients with small, well localized microadenomas unless there is a contraindication to surgery Nonsurgical Treatment Options for Acromegaly Medical therapy with somatostatin analogs or dopamine agonists and radiotherapy. These therapies have been most effective when used in conjunction with surgery.
1- Somatostatin analogs Somatostatin is an endogenous molecule that exerts a variety of physiological effects, including inhibition of GH secretion.
2- Dopamine agonists Dopamine agomsts (bromocriptine and pergolide) bind to pituitary dopamine type 2 receptors and suppress GH secretion in some patients with acromegaly. Tumor shrinkage occurs in a minority of patients
3- Radiotherapy Both conventional and heavy particle (proton beam) irradiation has been used. The beneficial effects of radiotherapy on GH levels are dose dependent Side Effects of Radiotherapy Hypothyroidism and gonadal dysfunction, visual disturbances, development of a secondary brain malignancy, brain necrosis, and brain damage.
Trans-sphenoidal Surgery

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
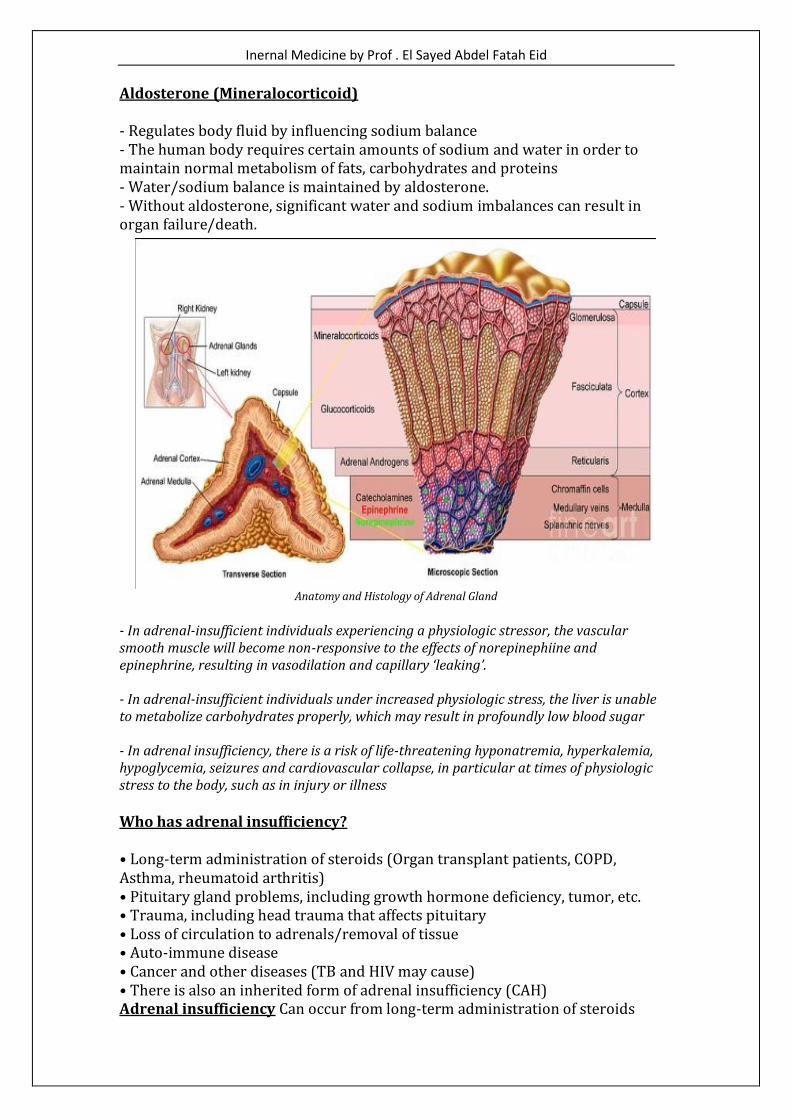
Adrenal Insufficiency Adrenal Anatomy & Physiology The adrenals are endocrine organs that sit on top of each kidney Each adrenal gland has two parts : Adrenal Medulla (inner area) • Secretes catecholamines which mediate stress response (help prepare a person for stress). • Hormones (Norepinephrine, Epinephrine & Dopamine) Adrenal Cortex (outer area, encloses Adrenal Medulla) • Secretes steroid hormones • Glucocorticoids: exert effect on metabolism of carbohydrates and proteins • Mineralocorticoids: are essential to maintain sodium and fluid balance • Sex hormones (secondary source) The Essential Steroids Primary glucocorticoid: Cortisol (hydrocortisone) Primary mineralocorticoid: Aldosterone A functioning adrenal cortex is essential for survival. Adrenal Cortex consists of 3 anatomic zones:
1- The outer zone (zona glomerulosa): secretes mineralocorticoid aldosterone.
2- The intermediate zone (zona fasciculata): secretes cortisol. 3- The inner zone (zona reticularis): secretes adrenal androgens.
Cortisol (Glucocorticoid) - Frequently referred to as the stress hormone. Released in response to physiological or psychological stress - Critical actions on many physiologic systems, including: - Maintains cardiovascular function - Provides blood pressure regulation - Enables CHO metabolism (acts on the liver to maintain normal glucose levels) - Immune function actions (reduces inflammation & suppresses immune system) - When cortisol is not produced or released by the adrenal glands, humans are unable to respond appropriately to physiologic stressors.
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Aldosterone (Mineralocorticoid) - Regulates body fluid by influencing sodium balance - The human body requires certain amounts of sodium and water in order to maintain normal metabolism of fats, carbohydrates and proteins - Water/sodium balance is maintained by aldosterone. - Without aldosterone, significant water and sodium imbalances can result in organ failure/death.
Anatomy and Histology of Adrenal Gland
- In adrenal-insufficient individuals experiencing a physiologic stressor, the vascular smooth muscle will become non-responsive to the effects of norepinephiine and epinephrine, resulting in vasodilation and capillary ‘leaking’. - In adrenal-insufficient individuals under increased physiologic stress, the liver is unable to metabolize carbohydrates properly, which may result in profoundly low blood sugar - In adrenal insufficiency, there is a risk of life-threatening hyponatremia, hyperkalemia, hypoglycemia, seizures and cardiovascular collapse, in particular at times of physiologic stress to the body, such as in injury or illness Who has adrenal insufficiency? • Long-term administration of steroids (Organ transplant patients, COPD, Asthma, rheumatoid arthritis) • Pituitary gland problems, including growth hormone deficiency, tumor, etc. • Trauma, including head trauma that affects pituitary • Loss of circulation to adrenals/removal of tissue • Auto-immune disease • Cancer and other diseases (TB and HIV may cause) • There is also an inherited form of adrenal insufficiency (CAH) Adrenal insufficiency Can occur from long-term administration of steroids

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Why long-term administration of steroids causing adrenal insufficiency? Adrenal glands tend to get ‘lazy’ when steroids are regularly administered by mouth, I.M. injection or I.V. infusion. To illustrate how quickly; Just 4 weeks of daily oral cortisone administration is sufficient to cause the adrenals to be slightly less responsive to stressors.
Primary Adrenal Insufficiency - Glucocorticoid insufficiency can be primary, resulting from the destruction or dysfunction of the adrenal correx, or secondary, resulting from ACTH hypo secretion. - Usually both Glucocorticoids & mineralocorticoid secretion are diminished - 80% of the time, damage is caused by an auto-immune response that destroys the adrenal cortex Causes - Autoimmune (Atoimmune disease (Addison’s disease)) - Infectious (Tuberculosis, Fungal, cytomegalovirus, HIV) - Vascular (Bilateral adrenal hemorrhage, Sepsis, Coagulopathy, Thrombosis, embolism, Adrenal infarction) Clinical manifestations Weight loss, increasing fatigue, postural dizziness may also occur. Vomiting, diarrhea or anorexia with salt craving Muscle and joint pain, abdominal pain, Signs of increased pigmentation (initially most marked on the extensor surfaces, palmar creases, and buccal mucosa)

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Diagnosis Laboratory tests: - ACTH & ACTH stimulation tests - Blood chemistries (hyponatremia, hyperkalemia, hypoglycemia, ft BUN) - CBC (ft Eosinophils & lymphocytes) - Serum cortisol (am and pm) - 24 hour urines for 17-hydroxycorticosteroids ECG: Hyperkalemia Changes Abdominal CT Treatment Life long hormone replacement — Glucocorticoids: Dexamethasone 0.5mg or Prednisone 5mg daily — Mineralocorticoids: Fludrocortisone with adequate salt intake Patient & Family teaching CRITICAL: — Hormone replacement therapy- LIFELONG — Use of patient Card — ft corticosteroids during illness & stress Acute manifestation of Addison’s (Addison Crisis) - Severe vomiting/diarrhea, dehydration - Sudden, severe pain in back, belly or legs - The patient may present with any illness or injury as the precipitating event. - Hypotensive, often unresponsive to fluids/pressors - Hypoglycemia, often refractory to glucose - May have neurologic deficits (Headache/confusion/seizure, lethargy /unresponsive ) - Cardiovascular collapse & Death - Children may deteriorate into adrenal crisis from a simple fever, a gastrointestinal illness, a fall from a bicycle or some other injury - For these patients, standard shock management requires supplementation with corticosteroid medication (Solu-Cortef or Solu-Medrol) Patient Management - Follow standard ABC and shock management treatment. - Notify ALS intercept as soon as possible; transport without delay - ALS: administer steroid IM/IV/Oral as soon as possible after initial life-threat and shock management have been initiated. - Transport without delay to appropriate hospital with early notification .
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Obesity & Metabolic Syndrome Definition Increasing the amount of body fat leading to increasing body weights Prevalence of Obesity - 1/3 - 1/2 of USA citizens are overweight - In an Egypt: 21.5 % in 1994 (endemic) 30 % in 2003 - The risk of death ↑2 - 4% for each ↑1 kg in body Weight Increased Risk for Adult Obesity — Gender/Ethnicity: Women, blacks — Family History — Childhood Obesity — In lower socioeconomic status — Sedentary lifestyle — Increased time-spent watching TV & computer Etioloy of Obesity 1- Sedentary lifestyle : — ↓ energy expenditure & promotes weight gain — ↓physical education in school, sports less participation or TV, computers, cars 2- Diet: ↑ energy intake (overeating) & the composition of diet — Night eating syndrome — Frequency of eating or dietary fat intake — Artificial feeding babies tend to gain weight in later life — Progressive hyperphagic obesity (↑ caloric requirement) — Smoking Cessation (Nicotine withdrawal lead to overeating) 3- Drug-induced weight gain - Glucocorticoids = fat redistribution - Drugs ↑ appetite: progestin, phenothiazines, insulin, sulfonylureas, antidepressants, antiepileptic (gabapentin & carbemazepine) lithium, 4- Socioeconomic state: Lower Socioeconomic state 5- Neuroendocrine obesity (hypothalamic obesity, cushing syndrome, hypothyroidism, polycystic ovary syndrome) 6- Genetic Causes: abnormal gene as primary factor ± Environmental factors. Classification of obesity

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
1- Android (or abdominal or central, males) — Collection of fat mostly in the abdomen (above the waist) - apple-shaped — Associated with insulin resistance & IHD 2- Gynoid (below the waist, females) — Collection of fat on hips and buttocks - Pear-shaped — Associated with mechanical problems Diagnosis of Obesity 1- The easiest to diagnose (spot Diagnosis) & most difficult to manage 2- Simple inspection 3- Weight / Height ratio: BMI= weight (kg)/height (m) 2 5- Fat distribution (WC, HG, WHR, abdominal CT & MRI) — WC = horizontal plane at natural waist (narrowest part of torso) — HC = horizontal plane at maximum extension of the buttocks posterior 6- Waist / Hip ratio 7- Skin fold thickness 8- Methods to quantitative for adipose mass Squeal of Obesity - Obesity of a group of diseases rather than a single disease - Once diagnosed, the complications are there - No system is exempted!!! (CVS; chest; metabolic; GIT, musculoskeletal; GU, skin & neuropsychatric) Morbidity & Mortality with Obesity - Hippocrates (relationship between obesity & sudden death) - ↑ DM,HTN - ↑ The incidence of ischemic stroke
- ↑The incidence of Cancer: ♂(colon, rectum & prostate) in ♀(uterus, breast) - ↑ Health costs to patient & healthcare system & .L workforce productivity - BMI>27.5 = 2 folds risk of death from all causes Squeal of Obesity General: fatigue, pain, disability, lower socio- economic status, poorer quality of life Obesity and hypertension —In extreme obesity 2/3 are hypertensive — Why? Hyperinsulinemia & IR; genetic factors &↑ Sympathetic tone

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Obesity and psychiatric disorders — Poor self-image; emotional liability; indoor lifestyle or depression — Psychological factors as the cause or the results
Obesity and coronary heart diseases - Central or abdominal obesity → Atherosclerosis due to hyperinsulinemia & insulin resistance, dyslipidemia, atherogenic Lipid profile & HTN Diabetes and obesity — ↑ Incidence of both (epidemic) allover the world — Metabolic syndrome, Cola lifestyle syndrome — 90 % of type 2 DM are obese Obesity and some endocrinopathies — Delay Puberty, lipomastia, concealed external genitalia, some striae — Polycystic ovary & hirsuitism Obesity and dyslipidemia — ↑ TG; ↑ FFA; ↑ LDL; ↑ VLDL; ↓HDL &↑ Lpa — Xanthelasma & Atherosclerosis Obesity and Thrombogenesis — Dyslipidemia, defective endothelial factors — ↑ Plasma homocysteine level, fibrinogen, & oxidative stresses Obesity and musculoskeletal System — ↑ Hyperuricemia — Osteoarthritis: (knees, hips & back) — Disc prolapse & root compression Obesity and gastero-intestinal tract — Fatty liver ± Liver fibrosis; gasterOesophageal reflux disease — Gall bladder dyspepsia & stones; Cancer colon; Hernias — Dyspepsia: Simply over eating — Hemorrhoids — Difficult Surgery &↑ Postoperative complications Obesity and gynecological system — Endometrial & Breast Cancer (Hyperestrogenic states) — PCO & Infertility — Gestational DM — Macrocosmic fetus; Obesity is commonest cause — Pregnancy (GDM, HTN,↑Pre-eclamsia and ↑ CS, congenital defects, polyhyromanus) Obesity and skin — Moniliasis, intertrigo, acanthuses Nigerians, panniculitis

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
— Varicose veins, hirsuitism & striae Obesity and chest —Sleep Apnea syndrome (SAS): Obesity is the commonest cause of SAS — Respiratory failure: Pickwickian syndrome Obesity and CNS — Cerebrovascular stroke, idiopathic intracranial hypertension, paresthesia
Obesity Management Program Treatment goals — Prevention of further weight gain — Weight loss to achieve target BMI Team Approach (Surgeons; Physician; Nurse Specialist; Dietitians; Exercise Physiologist & Psychologist) * Mild obesity — Diet, exercise & behavior therapy * Moderate obesity — Diet, exercise, behavior therapy, psychotherapy & medical therapy * Gross obesity — Consider surgery (gastroplasty) 1- Conventional Therapy * Diet control & modification — Low caloric diet: reduce calories by 500-1,000 calories/day — High fiber diet — Very low caloric diet<800 kCal/day, need supervision * Exercise program (↑Physical activity) — Reduces risk of T2DM, dyslipidemia, HTN — Assists weight management — Need 20-30 mins constant exercise — Not useful in: severely obese, elderly, arthritic * Behavior modification (change sedentary life style) * Pharmacotherapy : helps maintain weight loss best in combination with behavioral, diet and exercise interventions
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
- Appetite suppressants Adrenergic agents (amphetamine, or phentermine) Serotonergic agents (fenfluramine, sertraline, fluoxetine) - Thermogenic agents (ephedrine, thyroid hormones) - Drugs acting on GIT Bulk forming agents (methylcellulose) Glucosidase inhibitor (acarbose) Lipase inhibitors. Orlistat (Xenical) decreases fat absorption. 2- Surgical methods (when all other therapies fail or in gross obesity) — Jaw wiring — Gastroplasty, gastric banding — Gastric bypass loop or Roux-en-Y — Intestinal bypass Who Is a Surgical Candidate? — Failed medically supervised weight loss attempts — No endocrine cause of obesity or no uncontrolled psychological conditions — Understands surgery & risks
Benefits of surgery - Improvement of Co-Morbid Conditions - 86% of diabetes resolved or improved - 70% of hyperlipidemia improved - 78.5% of hypertension resolved improved - 83.6% of sleep apnea resolved or improved - 400% Reduced incidence of cancer
Insulin resistance (Metabolic) Syndrome
Definition A decreased ability of endogenous insulin to stimulate glucose clearance mainly into the skeletal muscle and to suppress hepatic glucose production Hyperinsulinemia is the physiological consequence of insulin resistance as the pancreas maintains glucose homeostasis by secreting higher amount of insulin Metabolic Syndrome: Three or more of the following present: 1- Abdominal obesity (>102cm M/88cm F) 2- Elevated triglycerides (>1 5Omg/dl) 3- Low HDL (<40 for men mg/dl; <50 for mg/dl for women) 4- Hypertension

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
5- High fasting blood sugar Etiologic Factors It is due to interaction between multiple factors including genetic, hormonal, obesity, age and ↓ Physical Activity Metabolic dysregulation: — Insulin resistance or glucose intolerance - also called the insulin resistance syndrome — Hyperinsulinemia — Pro-inflammatory state (elevated C-reactive protein) — Pro-coagulant changes (elevated fibrinogen and plasminogen activated inhibitor-1) — Dyslipidemia (hypertriglyceridemia and low HDL levels) — Premature atherosclerosis and type 2 diabetes — Hypertension

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Calcium Homeostasis and Its Disorders Calcium Metabolism & Regulation - 99% body calcium in skeleton (0.9 % intracellular and 0.1 % extra cellular) - 50% bound (Mostly albumin) Parathyroid Gland Anatomy - Parathyroid glands are four small glands near, attached to, or embedded in the thyroid gland. Total weight of parathyroid tissue is about 150mg - They regulate the calcium levels - Serum Ca++: 8.5-10.5 mg/dl
Anatomy
Parathyroid hormone (PTH) - PTH is synthesized as the preprohormone by parathyroid gland - PTH secretion in response to the level of Ca++ in the blood - The active PTH is cleaved from the preprohormone before release from the gland - PTH is synthesized continuously. It is released by exocytosis in response to reduced plasma Ca++ & Vitamin D feeds back to reduce PTH secretion Biological Activity of PTH 1-Bone - Stimulates bone osteoblasts to increase growth & metabolic activity - ↑ Bone resorption releases Ca++ & PO4 into blood 2- Kidney - ↑ Reabsorption of Ca++ & ↓ reabsorption of PO4 - Net effect of its action is ↑ Ca++ & ↓ PO4 in plasma

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
2- Intestine => ↑ Ca++ reabsorption via vitamin D Function of Calcium — Bone mineralization — Cofactor for factors VII, IX, X — Enzyme regulation — Skeletal & cardiac muscle contraction — Neural excitation. — Cellular secretion — Cell growth & division. — Maintenance of plasma membrane stability Calcium homeostasis — PTH => ↑ Ca++, ↓ PO4, ↑ Vitamin D — Vitamin D : ↑ Ca++, ↑ P04, ↓PTH (slow) — Ca++ control: Kidney, Bones, GI Tract Vitamin D - two sources (Skin and Diet) - 25 (OH) Vitamin D: Storage form Vitamin D and synthesized in the Liver - 1, 25 (OH) Vitamin D: Active form Vitamin D. - It activated by PTH and hypophosphatemia through 1-alpha hydroxylase in the kidney - It promotes absorption of calcium and phosphorous from small intestine - It activates osteoblasts/osteoclasts leading to bone resorption and release of calcium and phosphorous - It promotes calcium and phosphate excretion from the kidneys
Calcitonin - Little role in calcium homeostasis (↓ serum calcium) - Secreted by C cells of thyroid gland. Also; it has neural cell origin - It is elevated in cases of thyroid medullary hyperplasia/Cancer - Most sporadic case (MEN IIA or IIB)
Hyperparathyroidism Types Primary — Loss of regulatory relationship between serum Ca++ & PTH — ↑ Activity of the PTH gland — Parathyroid tumor or idiopathic hyperplasia (adenoma common) — ↓ Bone Ca - loss of PO4
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
Secondary - ↑ PTH due to hypocalcaemia - ↓ Plasma Ca++: ↓ Vit D, CRF - CRF (↓ GFR = ↑ serum P04 & ↓ serum Ca++ → PTH secretion is stimulated Tertiary In cases of CRF; persistant hypocalcemia change secondary hyperparathyroidism to autonomus noule causing very high level of PTH → ↓ serum Ca++ Etiology: Single Adenoma 85% Multiple Adenomas 5% Hyperplasia 10% Carcinoma <1%. ↑ Incidence with age & Postmenopausal women. - Prevalence 1/1000. Female: male = 2-3:1 Primary Hyperparathyroidism - Solitary adenoma is the commonest of 1ry HPT - Common in postmenopausal women - Usually asymptomatic - Fatigue and weakness - Bone & joint pain, stones & hematuria (↓ bone density & nephrolithiasis) - Osteitis fibrosa cystica (Brown tumor) and nephrocalcinosis are rare - Calciphylaxis Etiology of Hypercalcemia 1- Hyperparathyroidism - Primary (Adenoma, hyperplasia or carcinoma) or tertiary 2- Familial Hypocalciuric Hypercalcemia 3- Lithium therapy 4- Malignancy 5- Granulomatous Disease 6- Endocrinopathy (thyrotoxicosis, adrenal insufficiency, pheochromocytoma (ectopic PTH secretion) 6- Drug induced (Vitamin A and D, Milk-Alkali syndrome, Thiazide diuretics) 7- Immobilization 8- Paget’s disease Manifestation of HPT &Hypercalcemia 1- Asymptomatic (75%) 2- Constitutional: fatigue, weight loss, anorexia 3- Bone disease — Pam, weakness (Ostetitis fibrosa, osteoporosis or arthritis) — Osteitis fibrosa cystica, subperiosteal resorption (phalanges), bone Cysts (Brown tumors), Osteopenia/Osteoporos is, Pathological fracture
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
— Dental resorption of lamina dura 4- Renal disease - Renal Stones, polyuria, polydipsia, uremia - Calcification, degeneration, and necrosis of the tubular cells → tubular atrophy, interstitial fibrosis & calcification → nephrocalcinosis 5- Gastrointestinal: constipation, peptic ulcer, indigestion, nausea, vomiting, pancreatitis 6- Neuromuscular: headache, proximal muscle weakness, lethargy, gait disorders, hyperreflexia, fatigue, stupor and coma 7- Corneal deposition CaPO4 (band keratopathy), conjunctivitis 8- Hypertension (↑ risk CV mortality) 9- Skin: pruritus and brittle nails 10- Neuropsychiatric: depression, irritability, emotional liability, memory loss, psychoses, personality change, neurosis, insomnia, poor concentration 11- Parathyroid Tumors: neck mass 12- Hypercalcemic Crisis — Predisposing factors: inter-current illness/dehydration — Usually severe serum Ca> 14 mg% — Marked hypercalcemia symptoms especially CNS & Polyuria Diagnosis of HPT &Hypercalcemia 1- Clinical Diagnosis: Symptoms & Signs of hypercalcmia 2- Laboratory Diagnosis — ↑serum Ca (total, ionized) & ↓ Serum P04 — ↑ PTH level by radio-immunoassay with ↑ serum Ca (most specific test) — Others: (albumin, serum creatinine & BUN,↑Urine ca & PO4 levels and ↑Alkaline Phosphatase (associated bone disease) 3- Imaging Diagnosis — X-ray → osteoporosis, bone cysts — Bone Mineral Density — Localization: Ultrasound, CT, MRI, FNA, angiography with venous sampling 4- Parathyroid Laboratory Profile (serum PTH level) Management of HPT & Hypercalcemia Asymptomatic HPT (indications for medical monitoring) — Mild hypercalcemia — No episodes of life-threatening hypercalcemia — Normal renal & bone status Severe Hypercalcema: - Saline + diuresis - Bisphosphonates (onset 24-48h) - Calcitonin (immediate onset)

Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
- Hemodialysis Drugs to Lower Calcium Levels - ↓Ca intake, hydration, diuresis & calciuria - Alendronate (Fosamax) - Antiresorption Agents: plicamycin, gallium nitrate, phosphates & calcitonin - Oral phosphate (May precepitate calciphylaxsis) - Calcimimetic agents: Ca receptor agonists Surgical treatment (Parathyroidectomy): indicated in — Markedly elevated serum Ca level — Previous episode of life-threatening hypercalcemia — Reduced creatinine clearance (>30%) or presence of kidney stones — Increased urinary Ca excretion (>400 mgld) — Reduced bone mass (>2 SD below controls) — Patient requests surgery Secondary HPT: - Treat underlying cause - CRF → Ca salts &Vit. D - HRT in post-menopausal women
Hypoparathyroidism Definition Hyposecretion of the parathyroid glands →↓serum ca levels & ↑serum PO4 levels → ↑ neuromuscular irritability (tetany) Etiology of Hypoparathyroidism 1- latrogenic (thyroidectomy) 2- Injury, Ischemia or accidental neck radiation 3- Autoimmune disorder 4- Hereditary — DiGeorge’ s syndrome — agenesis — Pseudohypoparathyroidism: Albright’s hereditary osteodystrophy (peripheral resistance to PTH). Short stature, round faces, obesity, mild MR, dental abscesses, short digits, ectopic calcification 5- Idiopathic 6- Hypomagnesaemia Causes of Hypocalcaemia
Inernal Medicine by Prof . El Sayed Abdel Fatah Eid
1- PTH deficiency (the same causes of hypoparathyroidism) 2- PTH Resistance (Pseudohypoparathyroidism) - Congenital defect - Absent metacarpal, short stature, round face, mental disability - Target organ unresponsiveness to PTH - Serum PTH levels high 3- Vitamin D Deficiency - Nutritional deficiency and lack of skin exposure; Adult (osteomalacia & proximal muscle weakness) - Rickets Type 1 (hereditary vitamin D deficiency due to lack of 1-alpha hydroxylase) - Renal insufficiency 4- Vitamin D Resistance (Rickets Type II) - Target organ unresponsiveness to vitamin D due to defect in receptor 5- Calcium Deposition - Hyperphosphatemia due to tumor lysis, rhabdomyosis, renal failure - Pancreatitis - Acute Hypocalcaemia after parathyroidectomy (Hungry bone syndrome) - Citrate in blood transfusion - Lactate therapy Clinical manifestation (symptoms & signs of of Tetany) Symptoms: - Paresthesia (lips, fingers, toes), fasciculation muscle cramps & Laryngeal spasm, respiratory paralysis, tetany, irritability, movement disorder & seizure - Emotional changes, confusion or psychosis - Chvostek’s sign & Trousseaus sign - Abnormal Dentition, intracranial calcifications (basal ganglia) & mental changes - Visual: Cataracts, optic neuritis, papilledema - Pulmonary: Bronchospasm - Cardiovascular: arrhythmias, prolonged QT, CHF, Hypotension, digitalis resistance - Gastrointestinal: Dysphagia, abdominal pain, biliary colic - Obstetric: Preterm labor