c diff powerpoint session 3 140722 - · pdf filesession 3 –symptom ... vancomycin, for...
TRANSCRIPT

10/16/2014
1
IHI ExpeditionReducing Clostridium difficile Infections Session 3: Symptom Recognition, Precautions, and the Role of the Environment
July 23, 2014
These presenters have
nothing to disclose
Brian Koll, MDCarolyn Gould, MDDiane Jacobsen MPH, CPHQ
Expedition Coordinator2
Kayla DeVincentis, CHES, Project Coordinator, Institute for Healthcare Improvement, currently manages web-based Expeditions and the Executive Quality Leaders Network. She began her career at IHI in the event planning department and has since contributed to the State Action on Avoidable Rehospitalizations (STAAR) Initiative, the Summer Immersion Program, and IHI’s efforts for Medicare-Medicaid enrollees. Kayla leads IHI’s Wellness Initiative and has designed numerous activities, challenges, and educational opportunities to improve the health of her fellow staff members. In addition to implementing the organization’s first employee health risk assessment, Kayla is certified in health education and program planning. Kayla is a graduate of Northeastern University in Boston, MA, where she obtained her Bachelors of Science in Health Science with a concentration in Business Administration.

10/16/2014
2
Audio Broadcast3
You will see a box
in the top left hand
corner labeled
“Audio broadcast.”
If you are able to
listen to the
program using the
speakers on your
computer, you
have connected
successfully.
Phone Connection (Preferred)4
To join by phone:
1) Click the
button on the right
hand side of the
screen.
2) A pop-up box will
appear with call in
information.
3) Please dial the phone
number, the event
number and your
attendee ID to connect
correctly .

10/16/2014
3
Audio Broadcast vs. Phone Connection
If you using the audio broadcast (through your
computer) you will not be able to speak during the
WebEx to ask question. All questions will need to come
through the chat.
If you are using the phone connection (through your
telephone) you will be able to raise your hand, be
unmuted, and ask questions during the session.
Phone connection is preferred if you have access to a
phone.
5
WebEx Quick Reference
• Welcome to today’s
session!
• Please use chat to “All
Participants” for questions
• For technology issues only,
please chat to “Host”
• WebEx Technical Support:
866-569-3239
• Dial-in Info: Communicate /
Join Teleconference (in
menu)
6
Raise your hand
Select Chat recipient
Enter Text

10/16/2014
4
7
When Chatting…
Please send your message to
All Participants
Expedition Director8
Diane Jacobsen, MPH, CPHQ, Director, Institute for Healthcare Improvement (IHI) is currently directing the CDC/IHI Antibiotic Stewardship Initiative, NSLIJ/IHI Reducing Sepsis Mortality Collaborative. Ms. Jacobsen served as IHI content lead and improvement advisor for the California Healthcare-Associated Infection Prevention Initiative (CHAIPI) and directed Expeditions on Antibiotic Stewardship, Preventing CA-UTIs, Reducing C.difficle Infections, Sepsis, Stroke Care and Patient Flow. She served as faculty for IHI’s 100,000 Lives and 5 Million Lives Campaign and directed improvement collaboratives on Sepsis Mortality, Patient Flow, Surgical Complications, Reducing Hospital Mortality Rates (HSMR) and co-directed IHI’s Spread Initiative. She is an epidemiologist with experience in quality improvement, risk management, and infection control in specialty, academic, and community hospitals. A graduate of the University of Wisconsin, she earned her master’s degree in Public Health- Epidemiology.

10/16/2014
5
Today’s Agenda9
Introductions
Action Period Assignment
Debrief
Symptom Recognition,
Precautions, and the Role of the
Environment
Action Period Assignment
Expedition Objectives
At the end of this Expedition, participants will be able to:
Explain the impact of the increasing incidence and
severity of C. difficile on hospitals
Discuss key approaches to preventing the spread of C.
difficile in the hospital setting
Identify and begin improving at least one key process for
impacting C. difficile in their hospital
10

10/16/2014
6
Schedule of Calls
Session 1 – Making the Case for Reducing Clostridium difficileInfections (CDI)
Date: Wednesday, June 25, 2:00 – 3:30 PM ET
Session 2 – Rapid Detection and IsolationDate: Wednesday, July 9, 2:00 – 3:00 PM ET
Session 3 – Symptom Recognition, Precautions, and the Role of the EnvironmentDate: Wednesday, July 23, 2:00 – 3:00 PM ET
Session 4 – Antibiotic StewardshipDate: Wednesday, August 6, 2:00 – 3:00 PM ET
Session 5 – The Role of LeadershipDate: Wednesday, August 20, 2:00 – 3:00 PM ET
Session 6 – Transitions and Long- term CareDate: Wednesday, September 3, 2:00 – 3:00 PM ET
11
Action Period AssignmentRapid detection and precautions for C diff – test a process:
To expedite patients being placed on contact precautions when C diff is suspected or confirmed
- Test a flag, prompt, etc. to automatically initiate contact precaution when CDI test is ordered. (one unit, one nurse/unit clerk, refine based on initial test)
- Test a process to review patient placed on oral metronidazole or oral vancomycin, for need for contact precautions (one unit, one pharmacist/nurse, one day on MDR’s – refine based on initial test)
- Test a process to enhance STAT reporting of CDI, ie: critical value(one unit, one week, partner with laboratory – refine based on initial test)
What did you test/learn? Insights? Surprises?
12

10/16/2014
7
Faculty13
Brian Koll, MD, FACP, FIDSA, Executive Director for Infection Prevention, the Mount Sinai Health System, New York, NY, is a nationally-renowned and award-winning infection prevention expert. He has been featured on CBC Evening News for successful efforts to reduce central line associated bloodstream infections, on World News Tonight for successful efforts to control C. difficile, and in a national public service announcement regarding this disease by the Peggy Lillis Memorial Foundation.
Faculty14
Carolyn Gould, MD, MSCR, is a board-certified
Infectious Diseases physician and Medical
Epidemiologist in the Division of Healthcare Quality
Promotion at CDC. Dr. Gould joined the CDC and the
Commissioned Corps of the US Public Health Service
in December 2006. Her primary roles involve
responding to and preventing healthcare-associated
infections in acute care settings, with a special
expertise in C. difficile infections, catheter-associated
urinary tract infections (CAUTI), and antimicrobial
stewardship.

10/16/2014
8
A Tiered Approach to
Reduce Hospital Onset C.
difficile
Brian Koll, MD, FACP, FIDSA
Executive Director, Infection Prevention and Control, Mount Sinai Health System
Professor of Medicine, Icahn School of Medicine
Tiered Approach
1. Hand hygiene
2. Contact precautions
3. Sign placement
4. PPE readily available and used
5. Dedicated rectal thermometers
16

10/16/2014
9
Tiered Approach
6. Patient placement
7. Commodes
8. Environmentalcleaning protocols
9. Chlorhexidine bathing
17
Tiered Approach
10. Antibiotic stewardship
11. Pharmaceutical stewardship
18

10/16/2014
10
Begins with Leadership
•Accountability
•Link infection prevention
with organizational strategy
and resources
•Link a culture of safety to
outcomes
•Engage and facilitate
teamwork
•Goal setting and
measuring and assessing
effectiveness19
Begins with Leadership
▶ All Formal Authority Positions
– Chairs, Chiefs, Managers,
Directors, Supervisors
▶ All Physicians
▶ Informal Leaders
20

10/16/2014
11
Begins with Those on the Front Line
21
Begins with Diarrhea
22

10/16/2014
12
Isolation and Precautions
• Signage
• Availability of gowns, gloves, masks and N95
respirators
• Dedicated storage
• Monitoring of isolation rooms
• Cleaning of equipment between patients
• Hand hygiene
• Patient placement
• Private Room
• Cohorting23
Begins with Those on the Front Line
Ownership
24

10/16/2014
13
MDRO Infection Prevention Bundles
2011 – 2013
20
30
40
50
60
70
80
90
100
J2011 M M
J S N
J2012 M M
J S N
J2013 M M A O D
Co
mp
lia
nce
Ra
te %
Time
MSBI
MSBIB
25
Environmental Contamination
• Environmental cultures:
• 100% of CDAD rooms with >1 positive culture.
• 33% of non-CDAD rooms with >1 positive culture.
• C. difficile has been recovered from up to 58% of
individual samples from patient rooms.
• Beds, stretchers, wheelchairs, sinks, toilets, walls, iv poles,
blood pressure cuffs.
• Outbreaks have been associated with reusable rectal thermometers.
Dubberke. Am J Infect Control 2007;35:315-8
Martirosian. J Clin Microbiol 2006;44:1202
Walker. J Hosp Infect 2006;epub April 6

10/16/2014
14
Environmental Contamination
27
Environmental Contamination
28

10/16/2014
15
Environmental Disinfection
Eckstein et al. BMC Infectious Diseases 2007 7:61
Percentage of positive environmental cultures before and after housekeeping
cleaning and after research team disinfection with 10% bleach. (9 rooms)
Impact of Environmental Disinfection
Mayfield JL. Clin Infect Dis 2000;31:995-1000
Quaternary
ammonium
10% bleach Quaternary
ammonium
8.6* 8.1*3.3*
*cases per
1000 pt-days

10/16/2014
16
Monitoring of Environmental Cleaning
31
Begins with Those on the Front Line
Ownership
32

10/16/2014
17
Environmental Cleaning
Ownership by the Department
0
10
20
30
40
50
60
70
80
90
2011 2012H1 2012H2 2013Q1
Cleaning Compliance Rate EVS
IC
33
A Picture Says One Thousand Words
34

10/16/2014
18
Handling of Linen
35
Must be covered
No overflowing linen bins
Linen bins should be separated from clean equipment
Sani Cloths and Dispatch
36
•Two minute kill time – CDI kill time is five minutes
•Tops must be covered
•Check expiration dates
10/16/2014
19
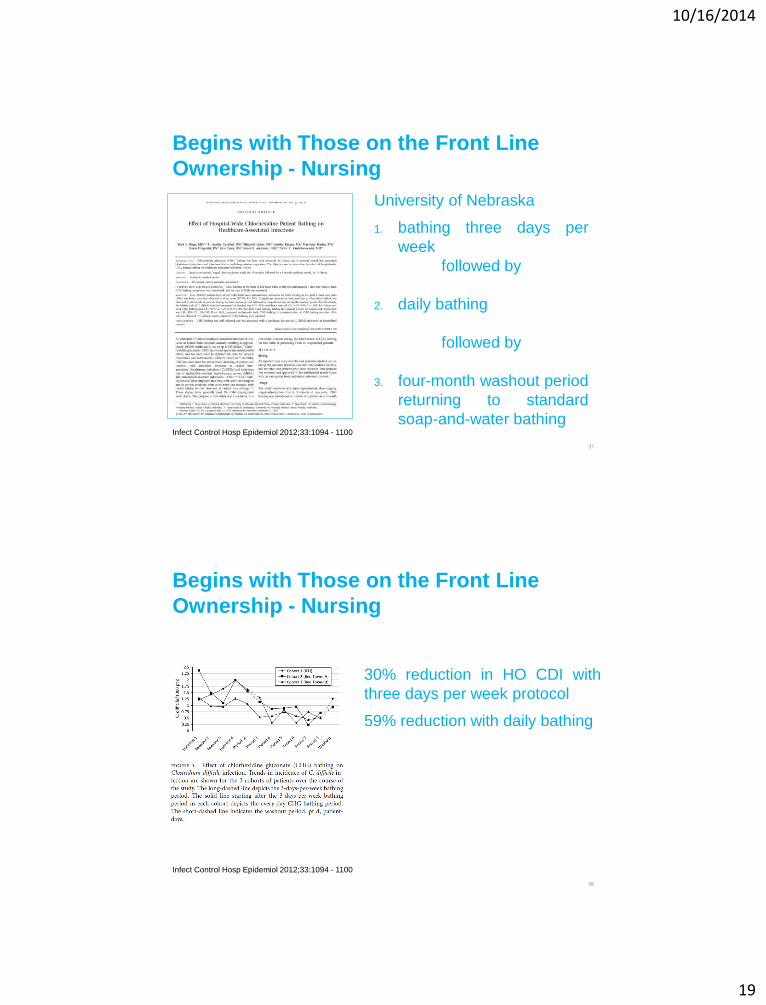
Begins with Those on the Front Line
Ownership - Nursing
University of Nebraska
1. bathing three days per
week
followed by
2. daily bathing
followed by
3. four-month washout period
returning to standard
soap-and-water bathing
37
Infect Control Hosp Epidemiol 2012;33:1094 - 1100
Begins with Those on the Front Line
Ownership - Nursing
30% reduction in HO CDI with
three days per week protocol
59% reduction with daily bathing
38
Infect Control Hosp Epidemiol 2012;33:1094 - 1100

10/16/2014
20
HO CDI
39
Tiered Approach
1. Successful
2. Involvement at all
levels of the
organization
3. Sustainable results
4. Assure continued
improvement
40

10/16/2014
21
Questions?41
Raise your hand
Use the Chat
Carolyn Gould, MD, MSCR
Division of Healthcare Quality Promotion
Centers for Disease Control and Prevention
IHI CDI Expedition Session 3: Symptom Recognition, Precautions, Role of the Environment
Prevention of Clostridium difficile Infections
National Center for Emerging and Zoonotic Infectious Diseases
Division of Healthcare Quality Promotion

10/16/2014
22
CDC highlights preventing CDI
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6109a3.htm
Vital Signs: 6 Key Components of Prevention
Prescribe and use antibiotics carefully
Focus on an early and reliable diagnosis
Isolate patients immediately
Wear gloves and gowns for all contact with patient
and patient care environment
Assure adequate cleaning of the patient care
environment, augment with EPA-registered C.
difficile sporicidal disinfectant
Notify facilities upon patient transfer
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6109a3.htm

10/16/2014
23
Vital Signs: 6 Key Components of Prevention
Prescribe and use antibiotics carefully
Focus on an early and reliable diagnosis
Isolate patients immediately
Wear gloves and gowns for all contact with patient
and patient care environment
Assure adequate cleaning of the patient care
environment, augment with EPA-registered C.
difficile sporicidal disinfectant
Notify facilities upon patient transfer
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6109a3.htm
Early Detection and Isolation
Screen
patients for
new-onset
diarrhea on
admission and
on a regular
basis
Facilitate early
testing
Consider
nurse-driven
protocols
Pair testing with
order for Contact
Precautions
Use more
sensitive testing
methods

10/16/2014
24
Optimizing Testing
Enzyme immunoassay (EIA) for toxin sensitivity 48%-
67%
More sensitive tests:
Nucleic-acid amplification tests (NAAT)
• Polymerase chain reaction (PCR)
• Loop-mediated amplification (LAMP)
2- or 3- step testing algorithms using GDH + toxin testing of
positive specimens
• GDH less sensitive (79%-98%) compared to NAAT or toxigenic
culture in a recent meta-analysis
Tenover FC, Novak-Weekley S, Woods CW, et al. J Clin Microbiol 2010; 48:3719–24
Tenover et al. J Mol Diagn 2011;13:573-82
Peterson et al. Clin Infect Dis 2007;45:1152-60
Shetty et al. J Hosp Infect 2011;77:1-6
First and Foremost…
• For any testing method, you need a favorable pre-
test probability of disease for optimal performance
– Diagnostic accuracy improves with increasing
prevalence of disease in the population tested
• That means testing appropriately:
– Watery/unformed stool (conforms to shape of
container)
– At least 3 unformed stools in 24 hours
– Avoidance of repeat testing, tests of cure

10/16/2014
25
Potential Benefits of More Sensitive Testing
Fewer isolation days for negative patients
Fewer repetitive tests performed (46% at one institution
with restriction rules in place)
In theory, earlier treatment initiation, reduced
complications, and improved infection control
Gould et al. CID 2013;57:1304
Moehring et al. ICHE 2013;34:1055-61
Loo VG, Frenette C. Presented at ICAAC 2011. Abstract D-1273
Morgan M, Grein J, Ochner M, Hoang H, Jin A, Murthy R. Presented at ICAAC 2011
Belmares J, Pua H, Schreckenberger P, Parada J. [abstract 150]. Presented at SHEA 2011 Annual Scientific Meeting, 1–4 April, 2011; Dallas, TX
Goldenber g SA et al. ICHE 2011
Environmental Cleaning:
use of Sporicidal Agents
• EPA registered disinfectants with sporicidal claim:
http://www.epa.gov/oppad001/chemregindex.htm
• Limited data suggest disinfecting with bleach (1:10
dilution prepared fresh daily) reduces C. difficile
transmission in units with high endemic rates
• Therefore, sporicidal agents may be most effective
in reducing burden where CDI is highly endemic
Mayfield et al. Clin Infect Dis 2000;31:995-1000
Wilcox et al. J Hosp Infect 2003;54:109-14

10/16/2014
26
Current list of Agents with C. difficile EPA
Sporicidal Claim (list K) (N=25)
Product: ACTIVATE 5.25% INSTITUTIONAL BLEACH
Registrant: DEARDORFF FITZSIMMONS CORPORATION
Active Ingredient: Sodium hypochlorite 5.25%
Product: AUSTIN A-1 ULTRA DISINFECTING BLEACH
Registrant: JAMES AUSTIN COMPANY
Active Ingredient: Sodium hypochlorite 6%
Product: BUSTER
Registrant: CLOROX PROFESSIONAL PRODUCTS
COMPANY
Active Ingredient: Sodium hypochlorite 8.5%
Product: CLOROX ULTRA BLEACH 2
Registrant: CLOROX PROFESSIONAL PRODUCTS
COMPANY
Active Ingredient: Sodium Hypochlorite 6.15%
Product: CONCENTRATED CLOROX GERMICIDAL
BLEACH1
Registrant: THE CLOROX COMPANY
Active Ingredient: Sodium hypochlorite 8.25%
Product: CPPC TSUNAMI
Registrant: CLOROX PROFESSIONAL PRODUCTS
COMPANY
Active Ingredient: Sodium hypochlorite .55%
Product: DISPATCH HOSPITAL CLEANER
DISINFECTANT WITH BLEACH
Registrant: CLOROX PROFESSIONAL PRODUCTS
COMPANY
Active Ingredient: Sodium hypochlorite .65%
Product: DISPATCH HOSPITAL CLEANER
DISNEFECTANT WITH TOWELS
Registrant: CLOROX PROFESSIONAL PRODUCTS
COMPANY
Active Ingredient: Sodium hypochlorite .65%
Product: FF-ATH
Registrant: ECOLAB INC.
Active Ingredient: Ethaneperoxoic acid 5.8%,
Hydrogen Peroxide 27.5%
Product: GERONIMO 160A
Registrant: KIK INTERNATION INC.
Active Ingredient: Sodium hypochlorite 8%
Product: HASTE-SSD-COMPONENT A
Registrant: STERIS CORPORATION
Active Ingredient: Tetraacetylethylenediamine
61.6%
Product: HASTE-SSD-COMPONENT B
Registrant: STERIS CORPORATION
Active Ingredient: Hydrogen Peroxide 1%
Product: KIMTECH GERMICIDAL WIPE
Registrant: KIMBERLY-CLARK GLOBAL SALES,
LLC
Active Ingredient: Ethaneperoxoic acid .23%,
Hydrogen Peroxide 4.4%
Product: MASSASOIT A
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 8%
Product: METACOMET 160B
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 8.25%
Product: OSCEOLA 160C
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 8.5%
Product: PERIDOX RTU ™
Registrant: BIOMED PROTECT, LLC
Active Ingredient: Ethaneperoxoic acid .23%, Hydrogen Peroxide 4.4%
Product: PURE BRIGHT GERMICIDAL 160 BLEACH
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 6%
Product: PURE BRIGHT GERMICIDAL ULTRA BLEACH
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 6%
Product: RESTROOM CLEANER & DISINFECTANT
Registrant: ECOLAB INC.
Active Ingredient: Sodium hypochlorite 2.15%
Product: SANI PROFESSIONAL BRAND NOROCLOTH GERMICIDAL DISPOSABLE
Registrant: PROFESSIONAL DISPOSABLES INTERNATIONAL, INC.
Active Ingredient: Sodium hypochlorite .63%
Product: STERIPLEX SD PART A
Registrant: SBIOMED, LLC
Active Ingredient: Silver .015%
Product: TECUMSEH B
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 8.25%
Product: VIRASEPT
Registrant: ECOLAB INC.
Active Ingredient: Ethaneperoxoic acid .05%,
Caprylic acid .099%, Hydrogen Peroxide 3.13%
Product: WAMPATUCK C
Registrant: KIK INTERNATIONAL INC.
Active Ingredient: Sodium hypochlorite 8.5%
http://www.epa.gov/oppad001/list_k_clostridium.pdf Updated August, 2012
Assess Adequacy of Cleaning Before
Changing to New Cleaning Product
Carling et al. Clin Infect Dis 2006;42:385-8.
10/16/2014
27
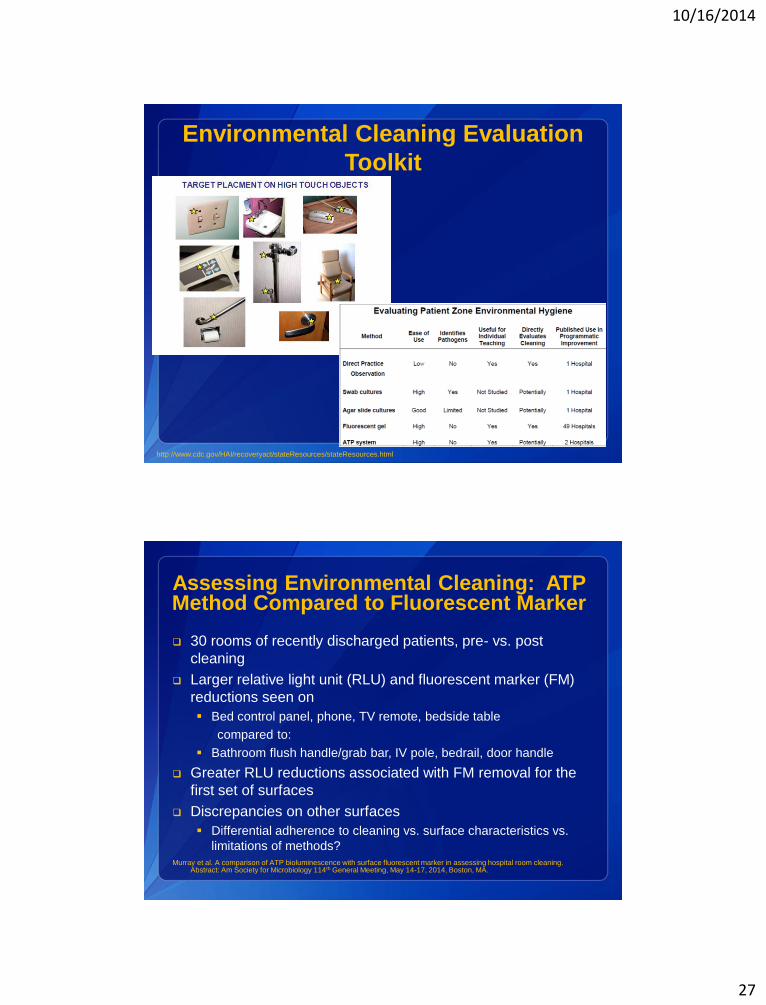
http://www.cdc.gov/HAI/recoveryact/stateResources/stateResources.html
Environmental Cleaning Evaluation
Toolkit
Assessing Environmental Cleaning: ATP Method Compared to Fluorescent Marker
30 rooms of recently discharged patients, pre- vs. post
cleaning
Larger relative light unit (RLU) and fluorescent marker (FM)
reductions seen on
Bed control panel, phone, TV remote, bedside table
compared to:
Bathroom flush handle/grab bar, IV pole, bedrail, door handle
Greater RLU reductions associated with FM removal for the
first set of surfaces
Discrepancies on other surfaces
Differential adherence to cleaning vs. surface characteristics vs.
limitations of methods?
Murray et al. A comparison of ATP bioluminescence with surface fluorescent marker in assessing hospital room cleaning. Abstract: Am Society for Microbiology 114th General Meeting, May 14-17, 2014, Boston, MA.

10/16/2014
28
Mechanical Spore Removal: Though
Much Can be Achieved, Still More to Be
Done• Wiping alone (25 sq.cm.)
– Nonsporicidal disinfectant: 2.90 log reduction
– Sporicidal disinfectant: 3.70 log reduction
• Spraying alone
– Sporicidal disinfectant: 3.40 log reduction
– Prolonged drying times and no removal of debris
“We believe the use of a wiping procedure with a sporicidal agent provides excellent removal and inactivation of spores and is an integral part of C. difficile control measures.”
Rutala et al. Infect Control Hosp Epidemiol 2012;33(12):1255-1258
How Could Non-sporicidal Disinfectants
Fail in Practice?
• “Clean bench top surface” inoculated with 105 dried spores
• 10 second wipe with:
– Fresh hypochlorite wipe
– Used hypochlorite wipe (expended on 25 sq.ft. surface)
– Wipe saturated with quaternary ammonium agent
• Wipe (10 sec) of 4 successive “clean sites”
• 5 minute contact/drying
• Swab sampling of “sites”
– vortex in neutralizer,
– plated on agar
Cadnum JL et al. Infect Control Hosp
Epidemiol 2013;34(4):441-2

10/16/2014
29
Success in Reducing CDI Using a
Sporicidal Wipe for Daily and Terminal
Cleaning• Before/after study in two high-risk medical wards
• Intervention:
– Daily and terminal cleaning of ALL rooms with ATP monitoring
before/after (similar pass rate)
– Quaternary ammonium compound before
– Hypochlorite wipes with 10 minute contact time after
• Results: 24.2 to 3.6 cases per 10,000 patient-days (85% decline)
Orenstein et al. Infect Control Hosp Epidemiol 2011;32(11):1137-1139
Role of asymptomatic shedders in C. difficile transmission?
To what degree do asymptomatic carriers spread spores
to the environment?
How long do patients continue to shed after treatment?

10/16/2014
30
Asymptomatic carriers are a Potential Sourcefor Transmission of C. difficile among LTCF
Residents
Riggs et al. Clin Infect Dis 2007;45:992–8
Post Symptomatic CDI Carriage: Particularly Contagious Asymptomatic Carriers?
Sethi AK et al. Infect Control Hosp Epidemiol 2010; 31:21-27

10/16/2014
31
Only ~30% of Hospital-associated CDI Linked to Previous Symptomatic Cases
Using advanced, highly discriminatory typing
At least 29% definitively linked to asymptomatic
carriers
Transmission between wards common
Limitation: study did not use molecular diagnostics
Expect a greater proportion linked to prior symptomatic patients
(CDI) with increased sensitivity
Implications?
Should we test for asymptomatic carriage?
Special measures for asymptomatic carriers – e.g., gloves,
sporicidal disinfectants?
Curry et al. CID 2013, McDonald CID 2013
Contaminated Hands: Remember the Patients!
Donskey et al. Infect Control Hosp Epidemiol 2014;35:204

10/16/2014
32
Photo Title – Myriad Pro, Bold, Shadow,
20pt
Caption for photo, references, citations, or credits – Myriad Pro,
14pt
For more information please contact Centers for Disease Control and
Prevention1600 Clifton Road NE, Atlanta, GA 30333
Telephone, 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348
E-mail: [email protected] Web: www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official
position of the Centers for Disease Control and Prevention.
Thank you!
Questions?
National Center for Emerging and Zoonotic Infectious Diseases
Place Descriptor Here

10/16/2014
33
Questions?65
Raise your hand
Use the Chat
Action Period Assignment
Role of the environment:
Test a checklist to assess terminal Environmental cleaning: |* your current internal checklist and/or:“CDC Environmental Checklist for Monitoring Terminal Cleaning”
- Does your current process/procedure address all the components of the CDC checklist? (ie: are there additional that your organization has identified as necessary/important? Are there components you can add to enhance your current process?)
- Request input/feedback on current process from:1) Environmental Services: current barriers/constraints they encounter in completing terminal cleaning (ie: adequate time to turn around room? Reliable notification of patient w/C diff being moved/discharged? Other? )
2) Nursing: are there current constraints(ie: ensuring Env Services are promptly & reliably notified if C diff? High census? Lack of private rooms? Other?)
Incorporate input from Nursing and/or Environmental Services to test a change to your current process
66

10/16/2014
34
Expedition Communications
Listserv for session communications:
– To add colleagues, email us at [email protected]
– Pose questions, share resources, discuss barriers or successes
67
Next Session
Session 4: Antibiotic Stewardship
Wednesday, August 6, 2:00 PM – 3:00 PM ET
Faculty: Belinda Ostrowsky MD & Phillip Chung PharmD
68