c hoeffel, p rousset imaging of peritoneal carcinomatosis jfim hanoi 2015
TRANSCRIPT

Imaging of peritoneal carcinomatosis
C.HOEFFEL, Reims P.ROUSSET, Lyon
HANOI, NOV 2015

ObjecHves
• Understand why evaluaHon of carcinomatosis is necessary
• Understand where to look for and how to quanHfy carcinomatosis
• Know the protocol of CT and MR examinaHons for evaluaHon of carcinomatosis
• Know the role and added value of involved imaging modaliHes in evaluaHon of carcinomatosis

General consideraHons
• Primary – GI : colo-‐rectal, pancreaHc, gastric – Ovary/Breast
• Outcome – Median survival: 7 months, OS-‐2 years : 15% – Limited penetraHon of systemic chemotherapy

• New agressive treatment= standard [ for paHents with disease confined to peritoneum and CRC – Removal of macroscopical – HIPEC: high local concentraHon of chemotherapy, increased in drug toxicity
with heat, for microscopical – OS-‐3 years: 53 % and OS-‐5 years: 48.5 % – 30 % morbidity, 4 % mortality
General consideraHons

ROLE OF IMAGING
• Not only Diagnosis but • Extension for strategy – selecHon of paHents for surgery +++, even if perop evaluaHon= ref – PCI = peritoneal cancer index=> score 0 to 39 (12 regions), ex Sugarbaker score
• Diameter : score 1 = 0-‐5 mm, score 2= 5 mm-‐5 cm, score 3 > 5 cm
– Probability to obtain R0 surgery and taken into account as CI to surgery when too high for a type of cancer
Sugarbaker PH, De Bree E., Jour Surg Oncol, 2004

• Extension necessitaHng expert centre: – ResecHon of diaphragm for diaphragmaHc nodule – HepaHc parenchymal invasion from implants, Bowel implants
– Bladder or ureteral invasion • Idea of length and morbidity • No current consensus on criteria for subopHmal resecHon but some lesions suggest non resectability
ROLE OF IMAGING
Low AJR 2008 Low. Ann Surg Oncolo.2013 Nougaret. Radiographics 2013

Alert surgeons to to the presence of disease that may complicate surgery or may preclude opHmal debulking . Extensive involvement of small bowel-‐ diffuse mesenteric infiltraHon or retracHon of the root of mesentery

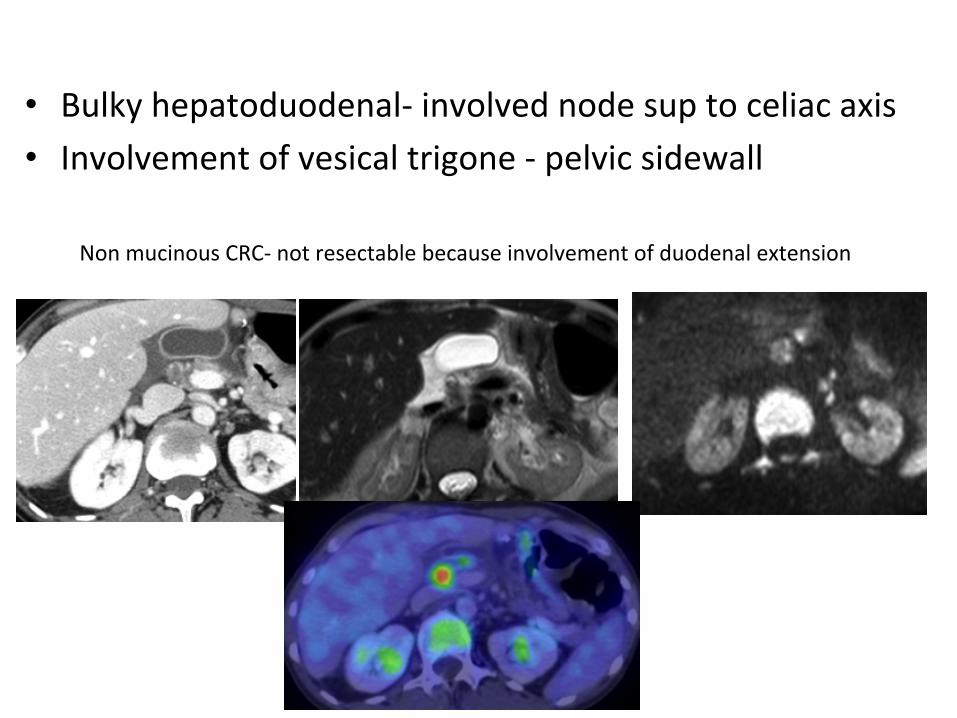
• Bulky hepatoduodenal-‐ involved node sup to celiac axis • Involvement of vesical trigone -‐ pelvic sidewall
Non mucinous CRC-‐ not resectable because involvement of duodenal extension

• IdenHfy extraperitoneal lesions – Liver small or central mets in liver , spleen not seen with lap
– Lymph nodes – Abdominal wall – Pleura – Bone
Role of Imaging

– Liver – Lymph nodes – Abdominal wall – Pleura-‐ inaccessible with lap – Bone

– Liver – Lymph nodes – Abdominal wall – Pleura-‐ inaccessible with lap – Bone

Where to look for carcinosis?
– Gravity dependent areas or of arrested flows • Pelvic recesses (rectouterine, lateral paravesical, RLQ), Right paracolic gu[er (phrenicocolic lig upward on the lel), ACE, Morisson’s recess, Right subdiaphragmaHc space
• RS J, Ileocaecal juncHon, pylorus – Peritoneal folds containing fat
• Ligaments : reflexion area between visceral and parietal p • Mesos : mesentery, transverse meso colon, mesosigmoïd • Omentum
Nougaret et al. RadioGraphics 2012. 32, No. 6: 1775-‐1800

PCI SCORE-‐Features
• Involvement of parietal serosa : peritoneal thickening-‐ nodules
• Involvement of fa[y areas (omental cake)
Nougaret et al. RadioGraphics 2012 Vol. 32, No. 6: 1775-‐1800
plaques
infiltration
Reticulonodular lesions
Mass (confluent nodules)

• Involvement of visceral serosa – Extrinsic tumoral infiltraHon (ileocaecal, right colonic angle, RSJ)
– Distorsion SB (retracHon of mesentery)-‐ Thickening
– ObstrucHon

PCI SCORE-Features
Pr Valette PJ. Lyon

Adhesions= deviaHon of a structure to another or thickening between
two structures without fat interface.

nodules of the mesentery if >7mm, and/if irregular hypodense nodules
and/if numerous : grouped and > 8 on one slice

Other signs
• Ureteral dilataHon without any obstacle
• Cardiophrenic lymph node – 550 pts with CRC – 30 % proven PC – VPN 85 %/VPP 49 %
Caramella. Eur J Cancer 2013
Two years after surgery for CRC. Ureteral dilatation due to carcinomatosis

Pseudomyxoma • Intraperitoneal seeding of mucin secreHng cells responsible for mucin in
the peritoneum – Low grade and high grade according to OMS 2010 – From mucinous appendicular, ovary
• Features: – Diffuse involvement – Thick asciHs with scalloping or septas – Possibility of calcificaHons – Rarely nodules and masses, associated organ involvement or extent to
pleura

ROLE of CT • Reference imaging for staging and restaging of paHents:
>90 % /paHent • Easily available, quick, large FOV
– SpaHal resoluHon (1 mm thick slices) and 3D reformats: reconstrucHon using 3 mm slices-‐
– Anayze coronal reformats : Nodule in at least two planes increases confidence in diagnosis
• Protocol: IV +±1 l water IV-‐ for ovary and CRC (30 % with calcificaHons)
Chandrashekhara. BJR.2011 Mazzei 2013. Abdominal imaging

• PCI: underscores staging compared with surgery
• Depends on size – Se < 15% for T< 0.5 cm (miliary in liniHs)
– Se < 25% for T < 1 cm – Se around 40% for T = 0.5 -‐ 5 cm
– Se 60 to 94% for T > 5 cm
De Bree. JSO 2004 Koh Ann. Surg Oncol .2009
Esquivel. JSO 2010 Sala. Radiology. 2010
ROLE OF CT-‐ Limits
small lesion on mesentery
plaque like lesion
ROLE OF CT-‐ Limits
• Depends on site – Se< 20% for small bowel and mesentery – Se poor for diaphragmaHc lesions – Se variable for pelvis
• Depends on level of experience • Depends on type of lesion : nodule (k=0.8)/ thickening (k=0.4)/distorsion (k=0.2)
• Depends on amount of fat De Bree. JSO. 2004

ROLE OF CT-‐ Limits
• CharacterizaHon of nodules and of asciHs

Role of CT-‐Limits Limits= specificity

ROLE OF MRI • Few studies available, parHcularly in paHents without
neoadjuvant treatment • MRI versus CT
– Qayyum. Gynecol oncol 2005: 137 pts, CT = MRI – Torkzad. JSO 2015: 39 pts, PCI radio CT = MRI, EXCEPT junior
– Low. Ann surg oncol. 2015: 22 pts: Acc = 85 vs 63%
• MRI versus PET – Soussan. Eur radiol 2012: 30 pts (13/33 (43% opérés)
Ac = 83 vs 80% per p[ per site MRI + per lesion
– Klumpp. abdo imaging 2012: 15 pts: 88 vs 94%. MRI without diffusion
• MRI alone – pseudomyxoma – Low. Ann Surg Oncol 2012: 33 p[s (25 PMP) Acc 0.84

MR PROTOCOL
• Fast/PEG 500 cc? • AnHperistalHc agents before gadolinium injecHon = glucagon
• MRI of abdomen and pelvis -‐ 2 stacks to cover the whole peritoneal cavity – Axial T2 single shot FSE (trigger free breathing, not as good with echo nav), 5-‐6 mm, sans Fatsat
– Axial Diffusion (b 0-‐800) – Axial post gadolinium-‐enhanced T1-‐weighted art/portal/late phase (5 minutes).
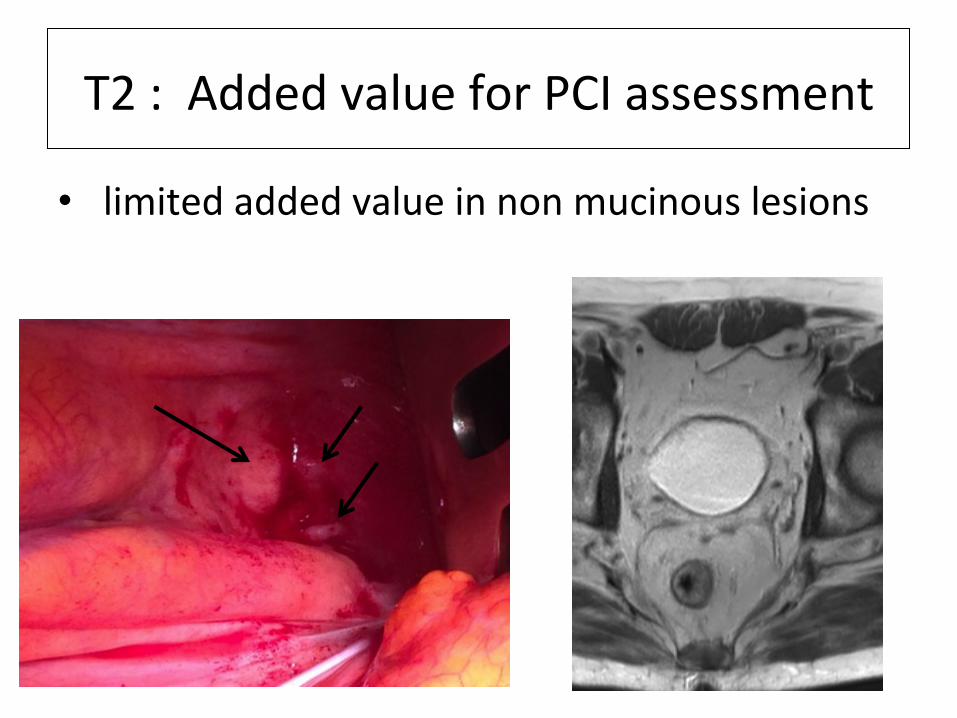
T2 : Added value for PCI assessment
• limited added value in non mucinous lesions

T2 : Added value for PCI assessment
• added value ++ for mucinous lesions

Gadolinium: Added value for PCI assessment
• non mucinous lesions-‐ peritoneal thickening

Gadolinium: Added value for PCI assessment

Gadolinium: Added value for PCI
assessment
Mucinous lesions

Tissu sain Tissu tumoral
Diffusion: Added value for PCI assessment-‐Contrast resoluHon-‐
detecHon
Diffusion: Added value for PCI assessment-‐DetecHon
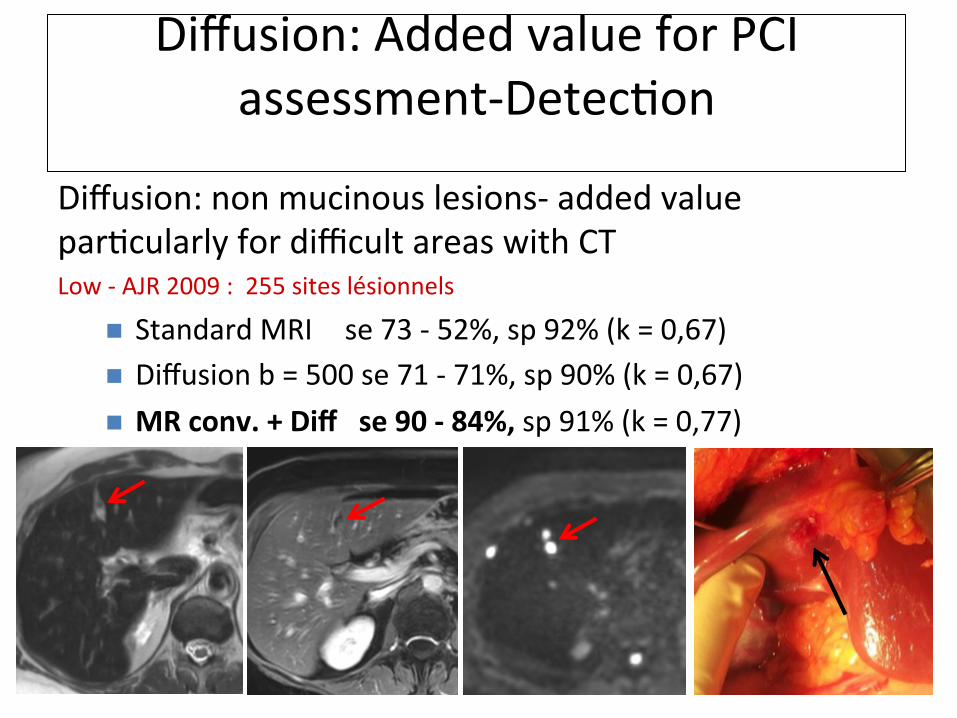
Diffusion: non mucinous lesions-‐ added value parHcularly for difficult areas with CT Low -‐ AJR 2009 : 255 sites lésionnels
n Standard MRI se 73 -‐ 52%, sp 92% (k = 0,67) n Diffusion b = 500 se 71 -‐ 71%, sp 90% (k = 0,67) n MR conv. + Diff se 90 -‐ 84%, sp 91% (k = 0,77)



Small bowel serosa < 5 mm
Added value for pelvis and small bowel WARN SURGEON => morbidity

Abdominal wall lesion < 10 mm
Added value for special sites such as abdominal wall

Diffusion: Added value for PCI assessment-‐CharacterizaHon
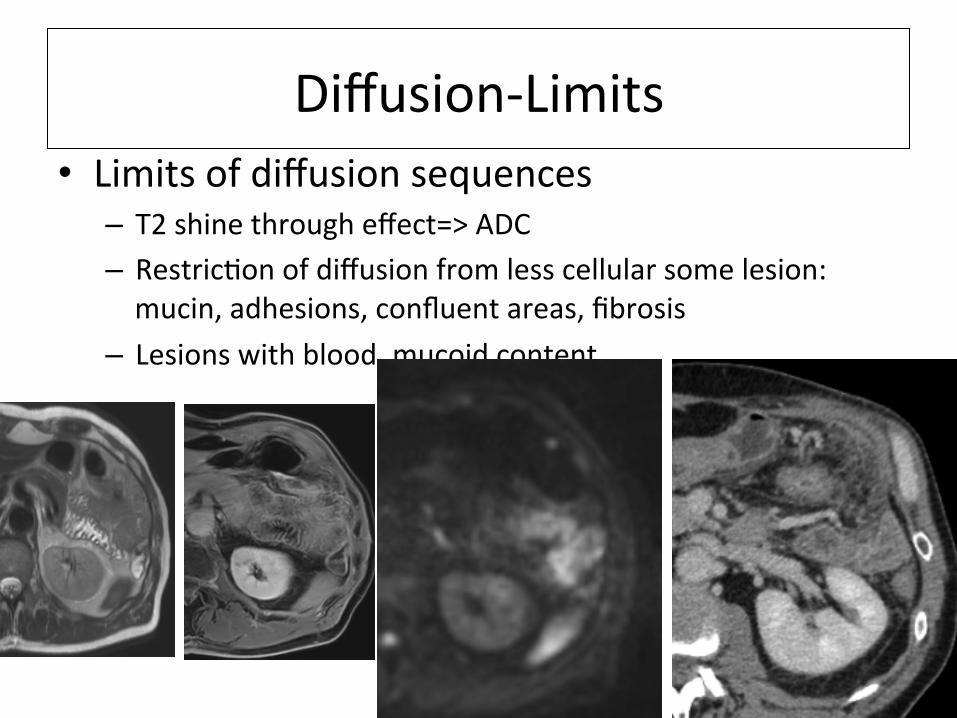
Diffusion-‐Limits • Limits of diffusion sequences
– T2 shine through effect=> ADC – RestricHon of diffusion from less cellular some lesion: mucin, adhesions, confluent areas, fibrosis
– Lesions with blood, mucoid content

MR Technique-‐Limits
• PaHent-‐dependent • PeristalHsm • Black hole effect-‐ get rid of the asciHs before MRI
• ParHal volume effect-‐spaHal resoluHon • Interobserver Variability (per site)-‐ learning curve

PET CT-‐ Main IndicaHons
• Strong Clinical suspicion of PC or increase in markers level with normal CT
• DetecHon of recurrence versus fibrosis • Assessment before HIPEC
– Underscores PCI but complementary to CT/MRI – Rules out extraperitoneal lesions contraindicaHng surgery

– False negaHve • Mucinous tumors, low grade pseudomyxoma and gastric liniHs
PET CT-‐ Limits
Passot.Eur J Surg Oncol. 2010 Anthony. AJR.2009 Hymnimen. Gynecol oncol. 2013

PET CT-‐ Limits • False negaHve
– Size < 1cm
– Hidden lesions by respiratory and GI movements
• False posiHve: specificity < CT – Inflammatory reacHon of peritoneum around large or numerous implants – Foreign body or inflammatory reacHon related to previous surgery – Physiological uptake of bowel and vessels
Pierandrea de Iaco. EJR. 2011

Conclusion
– CT= reference imaging – Before deciding upon treatment MRI ±PET scanner needed
• For assessment of PCI • Detect lesions needing expert center
• Detect non resectable disease – Added value of diffusion for small bowel, pelvis , hepaHc hilum, pseudomyxoma ++
– PET/CT for extraperitoneal disease – COMBINE modaliHes

Peritoneal Thickening