calcific tendonitis james wilson
TRANSCRIPT
1
James Wilson Upper Limb Fellow Teaching
30/09/2014
Calcific Tendonitis
2
• Calcific tendonitis / calcific perarthritis • Predominantly in the shoulder • Can be manifest throughout the body
• (Longus coli)
!
• Due to deposition of poorly calcified Hydroxyapatite
Ca10(PO4)6(OH)2
Definition
3
• Exact pathogenesis unclear. • ? association with endocrine disorders (Harvie) • ? matrix vesicles (Gohr) • ? due to tendon degeneration and necrosis
• Peak age earlier • Calcific tendinitis may resolve • Dystrophic calcification occurs in necrotic tissue • Different chemical composition
Aetiology
Harvie P, Pollard TC, Carr AJ. Calcific tendinitis: natural history and association with endocrine disorders. J Shoulder Elbow Surg 2007; 16:169–173 Gohr CM. Fahey M. Rosenthal AK. Calcific tendonitis: a model. Connect Tissue Res 2007:48:286-91.
4
!
• Formative • Calcific • Resorptive • Reparative !
• Natural History
Cell Mediated Process
Uhthoff HK. Loehr JW, Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg 1997:5:183-91.
5
• Age of onset typically 30-60 yrs • Slight female preponderance
!
• Location • supraspinatus - 80% • infraspinatus - 15% • subscapularis - 5% • periarticular soft tissues - ligaments, capsule, bursae
Clinical Presentation
Speed CA. Hazleman BL. Calcific tendinitis of the shoulder, N Engl J Med 1999:340:1582-4.
6
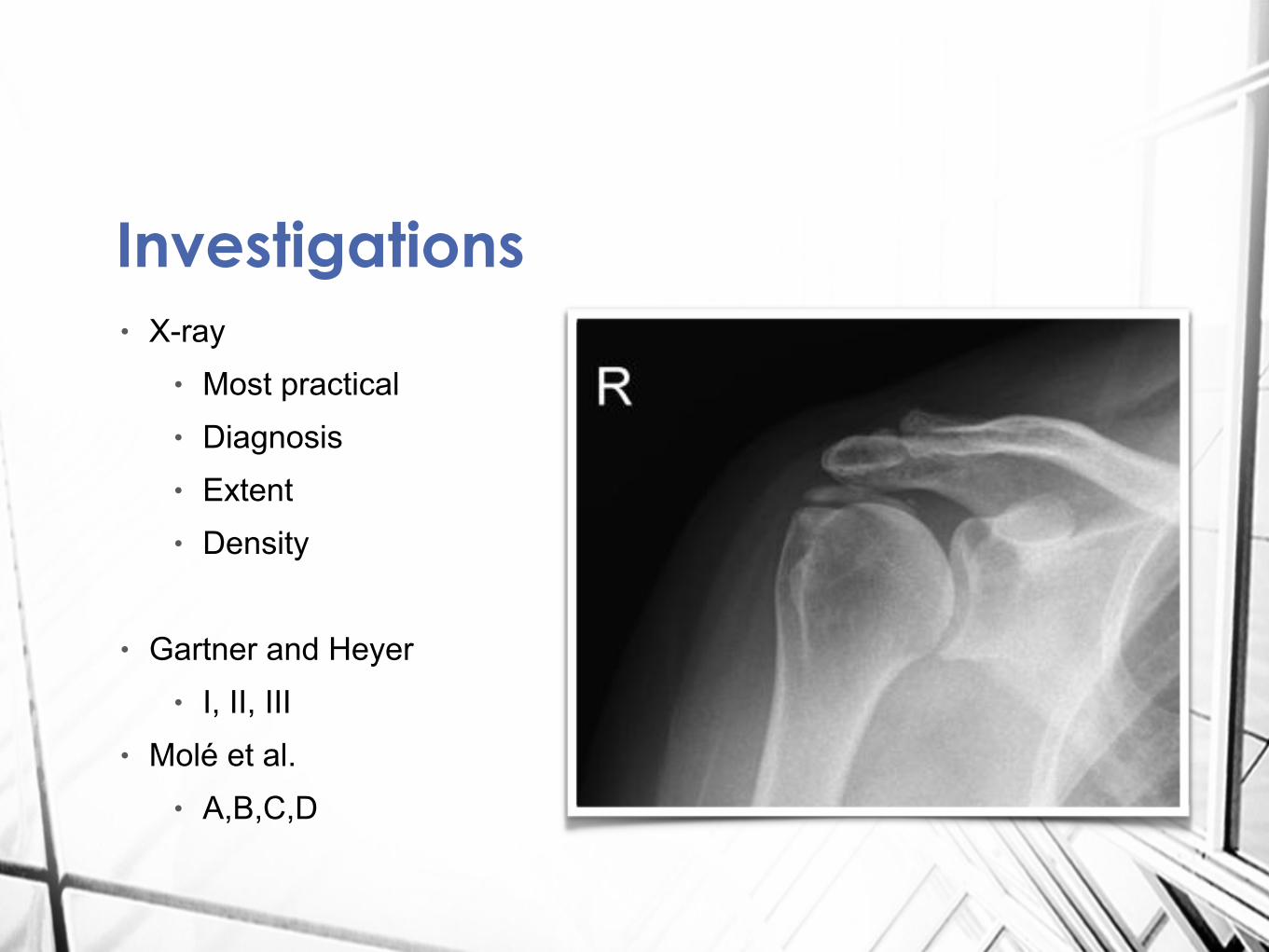
• X-ray • Most practical • Diagnosis • Extent • Density !
• Gartner and Heyer • I, II, III
• Molé et al. • A,B,C,D
Investigations
7
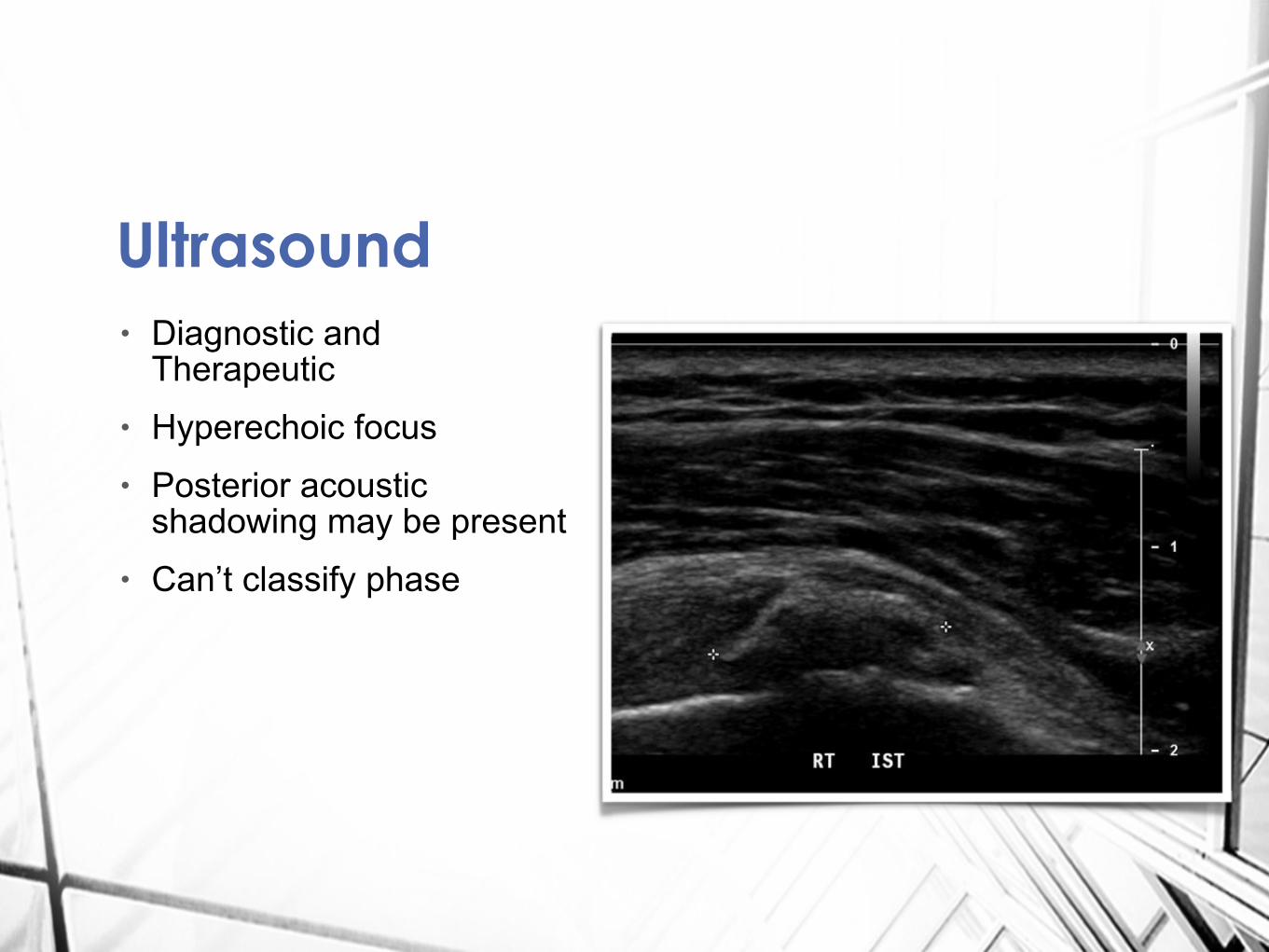
• Diagnostic and Therapeutic
• Hyperechoic focus • Posterior acoustic
shadowing may be present • Can’t classify phase
Ultrasound
8
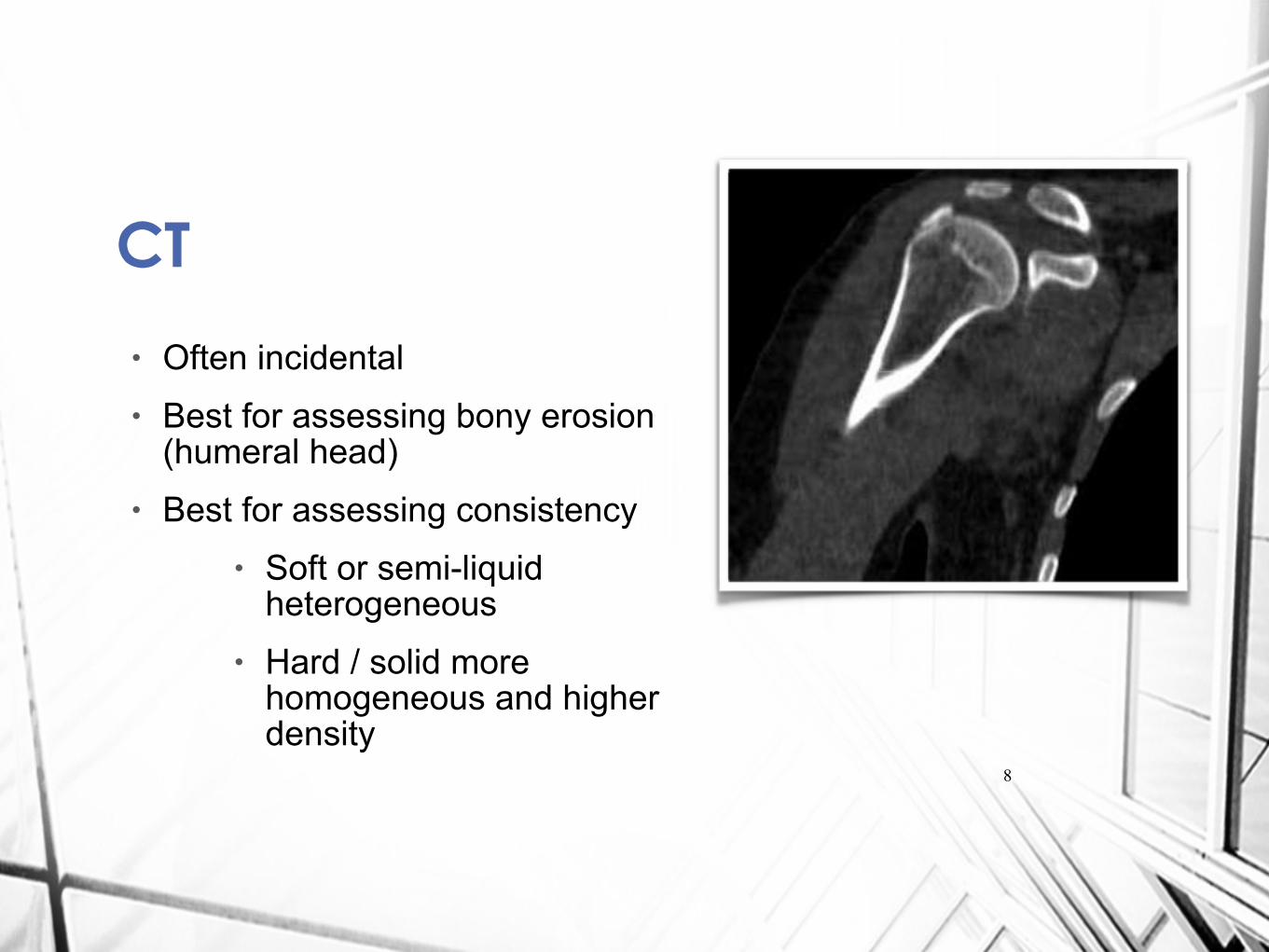
• Often incidental • Best for assessing bony erosion
(humeral head) • Best for assessing consistency
• Soft or semi-liquid heterogeneous
• Hard / solid more homogeneous and higher density
CT
9
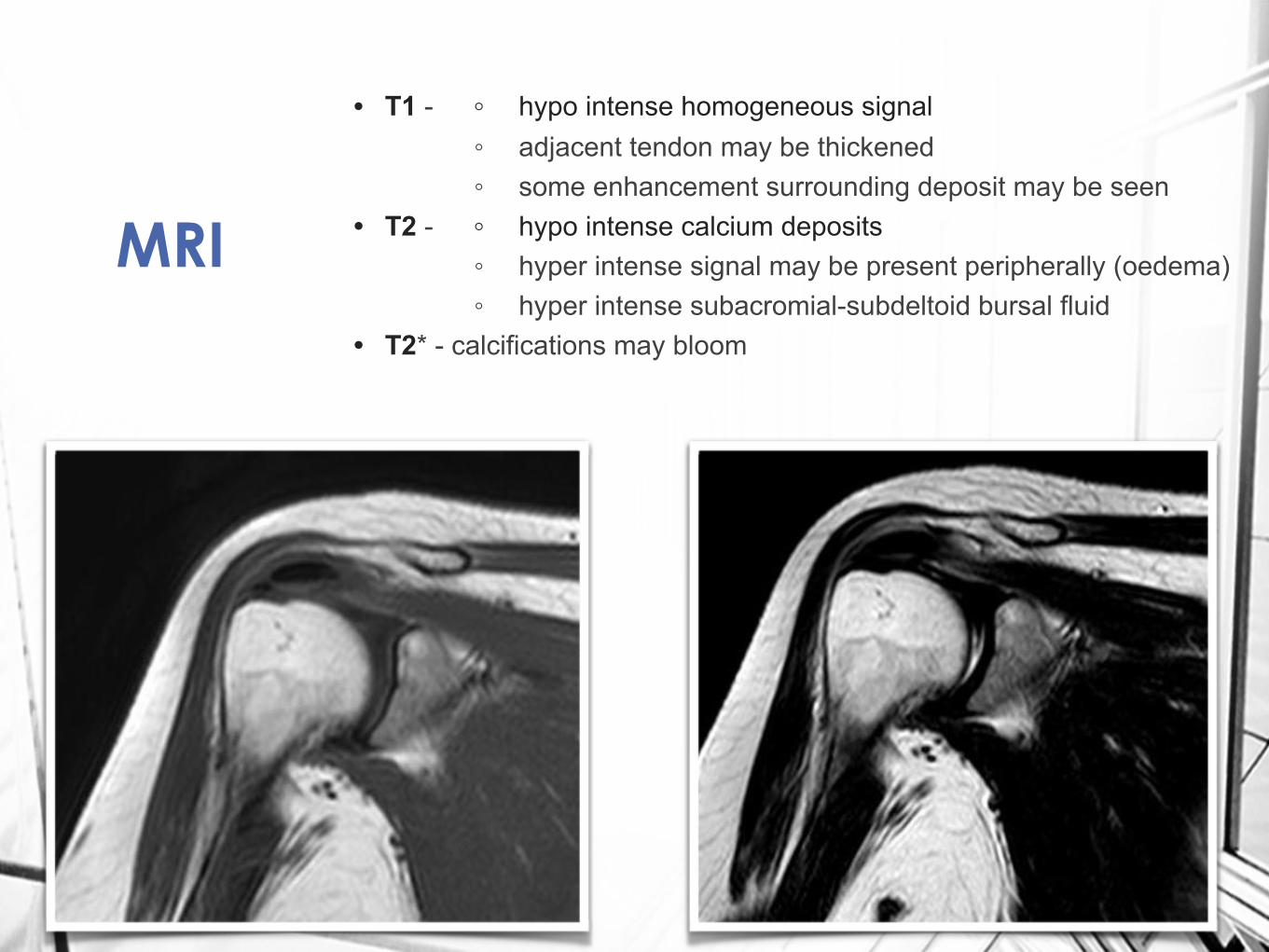
MRI
• T1 - ◦ hypo intense homogeneous signal ◦ adjacent tendon may be thickened ◦ some enhancement surrounding deposit may be seen • T2 - ◦ hypo intense calcium deposits ◦ hyper intense signal may be present peripherally (oedema) ◦ hyper intense subacromial-subdeltoid bursal fluid • T2* - calcifications may bloom
10
• Rest • NSAIDs • Physiotherapy • Subacromial steroid injection • Radial or traditional ESWT • Needling / Barbotage (better if not solid) • Surgical release
Treatment
11
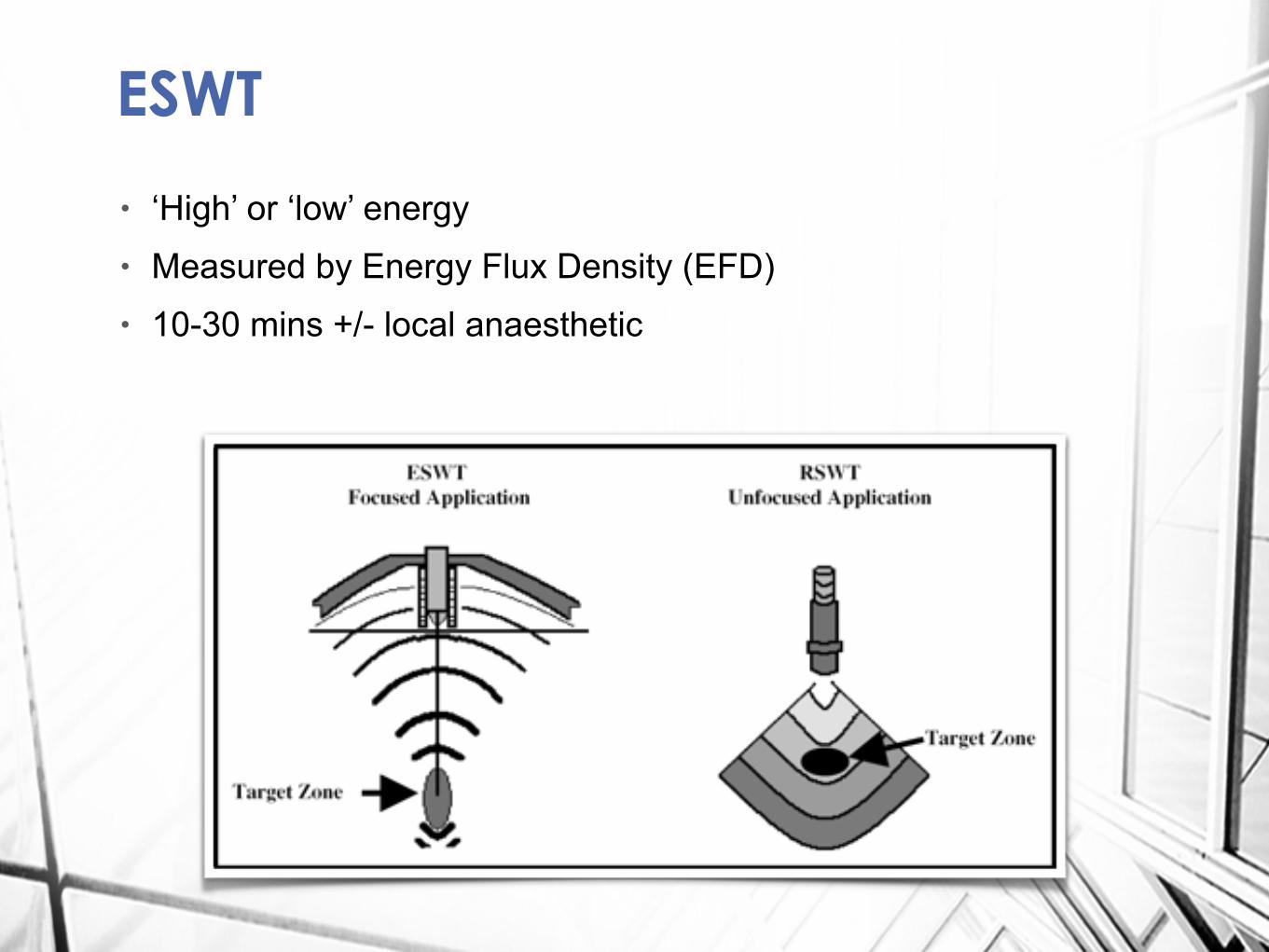
• ‘High’ or ‘low’ energy • Measured by Energy Flux Density (EFD) • 10-30 mins +/- local anaesthetic
ESWT
12
ESWT• High energy ESWT effective
for pain and function • High energy > 0.28 mJ/mm2 • No useful comparisons with
surgery • (? equivalence for non-homogenious
deposits)
• No benefit in treating non-calcific tendinitis
13
• Case series - n=35 • Combined with Subacromial
steroid injection • 71% improved within 6 months • Constant scores 54 - 88 • 6 failed and had Surgery • (mean Constant - 92)
U/S guided Needling
14
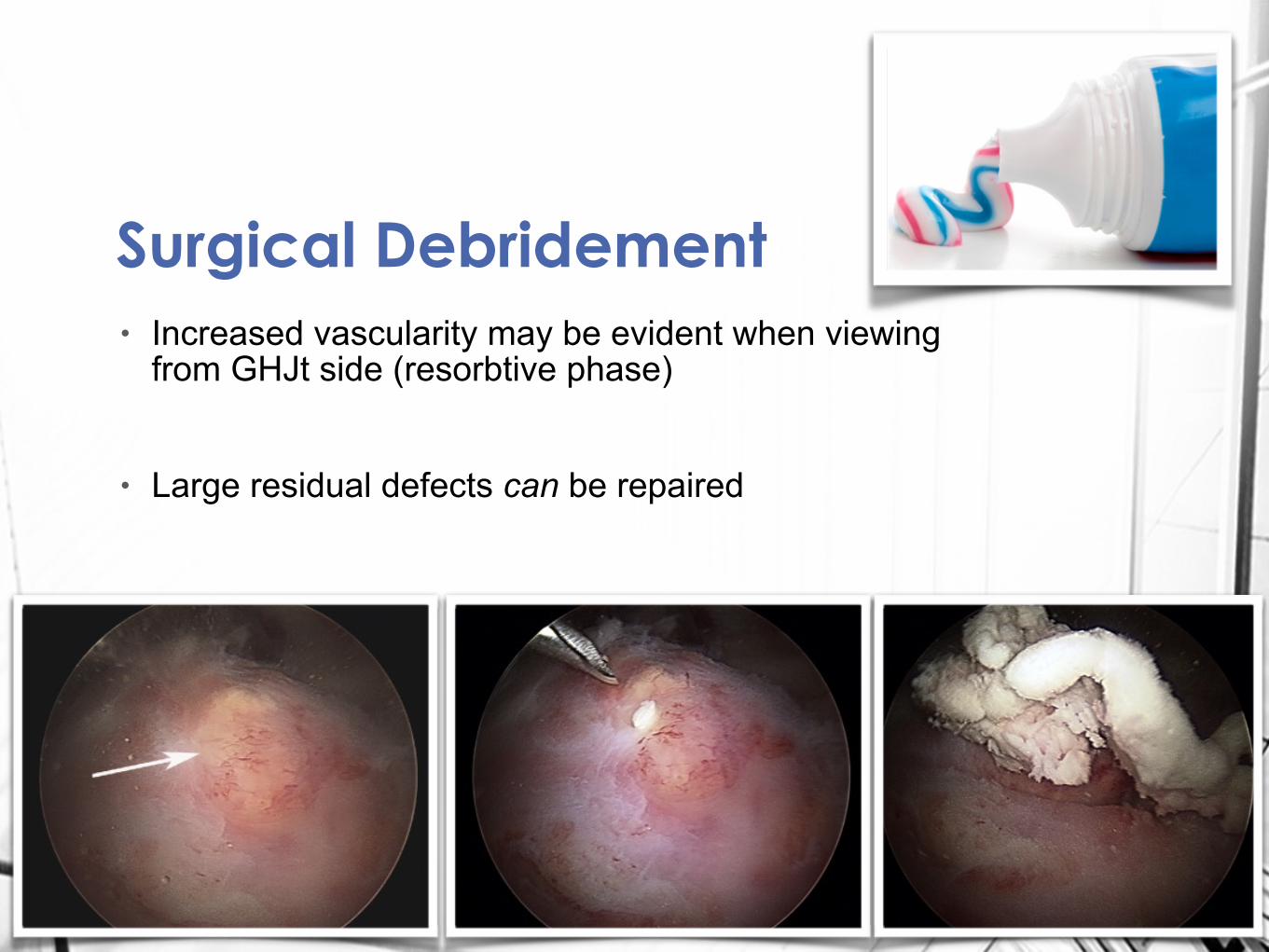
• Increased vascularity may be evident when viewing from GHJt side (resorbtive phase)
!
• Large residual defects can be repaired
Surgical Debridement
15
• Case-control study • 50 patients, 25 in each arm • 2 surgeons with different
techniques • data collected over 10 yrs • Outcome measures - return to
full activity • Found no difference in long
term outcome but sooner return to full activity.
Surgical debridement