calcineurin inhibitor toxicity in kidney allograft protocol biopsies neeraja kambham m.d. stanford...
Post on 19-Dec-2015
219 views
TRANSCRIPT
Calcineurin Inhibitor Toxicity In Kidney Allograft Protocol
BiopsiesNeeraja Kambham M.D.
Stanford University
Calcineurin Inhibitor Toxicity (CNIT)
• CNI toxicity is a very important cause of chronic allograft nephropathy (CAN)
• Later phase of CAN (i.e. > 1 year post txp) is likely due to CNIT, and it’s contribution progressively increases (Nankivell et al.)
• Acute phase of CNI toxicity is reversible, but chronic phase is probably irreversible
CNI Toxicity
• Functional• Structural:
– Acute: tubulopathy (proximal tubules), endothelial injury (thrombotic microangiopathy)
– Chronic: arteriolopathy, tubular atrophy, striped fibrosis, glomerulosclerosis
Calcineurin Inhibitor (CNI) Toxicity
• Can it it be scored objectively?• Is it clinically useful?• Does it correlate with subsequent
graft function?• Is it better than Banff Chronicity
score?
Study Design
• 50 consecutive pediatric renal transplant patients (November 1999- December 2004)
• Patients on Steroid free immunosuppression protocol*
• Immunosuppression: Extended Daclizumab induction; Tacrolimus and Mycophenolate mofetil maintenance
• Biopsies: Protocol 3, 6, 12 and 24 months (P); also as indicated clinically (NP)
(Sarwal MM et al: Transplantation. 76 (9): 2003)
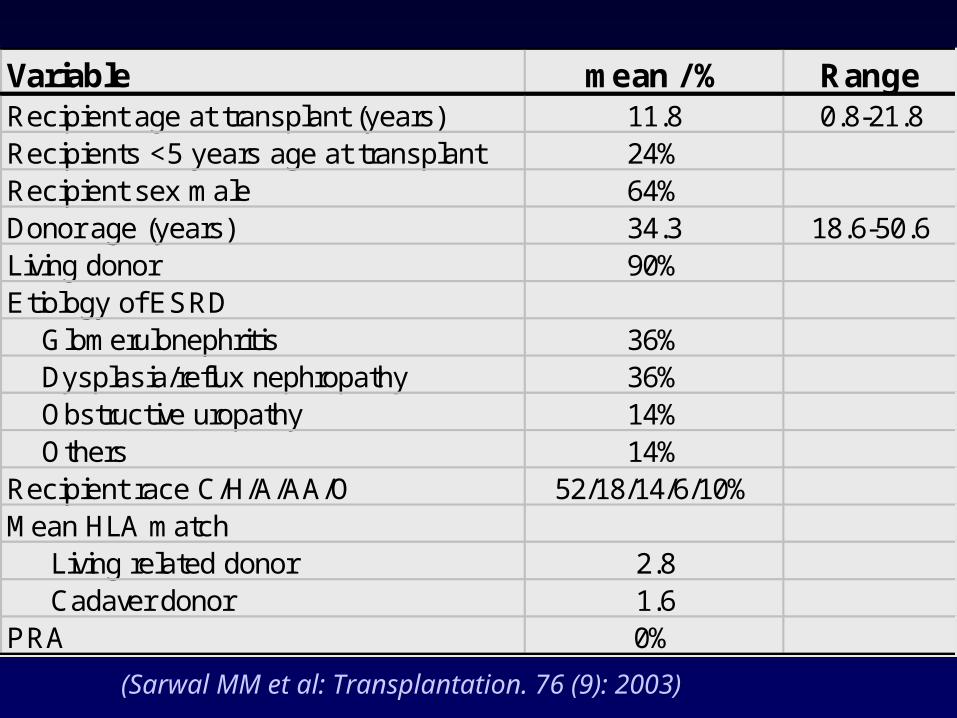
Variable mean / % RangeRecipient age at transplant (years) 11.8 0.8-21.8Recipients <5 years age at transplant 24%Recipient sex male 64%Donor age (years) 34.3 18.6-50.6Living donor 90%Etiology of ESRD Glomerulonephritis 36% Dysplasia/reflux nephropathy 36% Obstructive uropathy 14% Others 14%Recipient race C/H/A/AA/O 52/18/14/6/10%Mean HLA match Living related donor 2.8 Cadaver donor 1.6PRA 0%
(Sarwal MM et al: Transplantation. 76 (9): 2003)
Study Design…
• 231 biopsies (P+NP) scored in a blinded fashion– 27 were inadequate (diagnosis rendered on 5)
• CNI toxicity (CNIT) score in biopsies with histological evidence of CNI toxicity
• Banff chronicity score (BChS): cg, ct, ci, cv• Modified Banff chronicity score (MBChS): gs,
ct, ci, cv• Chronic Allograft Damage Index (CADI)• C4d Stains on paraffin embedded tissue
Diagnostic Categories• CNI Toxicity• Acute Rejection
– graded by Banff criteria
• Chronic Allograft Nephropathy– Unclear etiology of chronic damage– Any tubular atrophy or interstitial fibrosis >
5%
• No Significant Abnormality– No tubular atrophy; interstitial fibrosis < 5%
• Other: ATN, glomerulonephritis, reflux
Acute Rejection (n=29)
• Non-protocol Biopsies: 21 (9 %)– Borderline: 13– IA: 6– IB: 2
• Protocol Biopsies: 8 (4.8 %)*– Borderline: 4– IA: 3– IB: 1
* Includes clinical & subclinical acute rejections
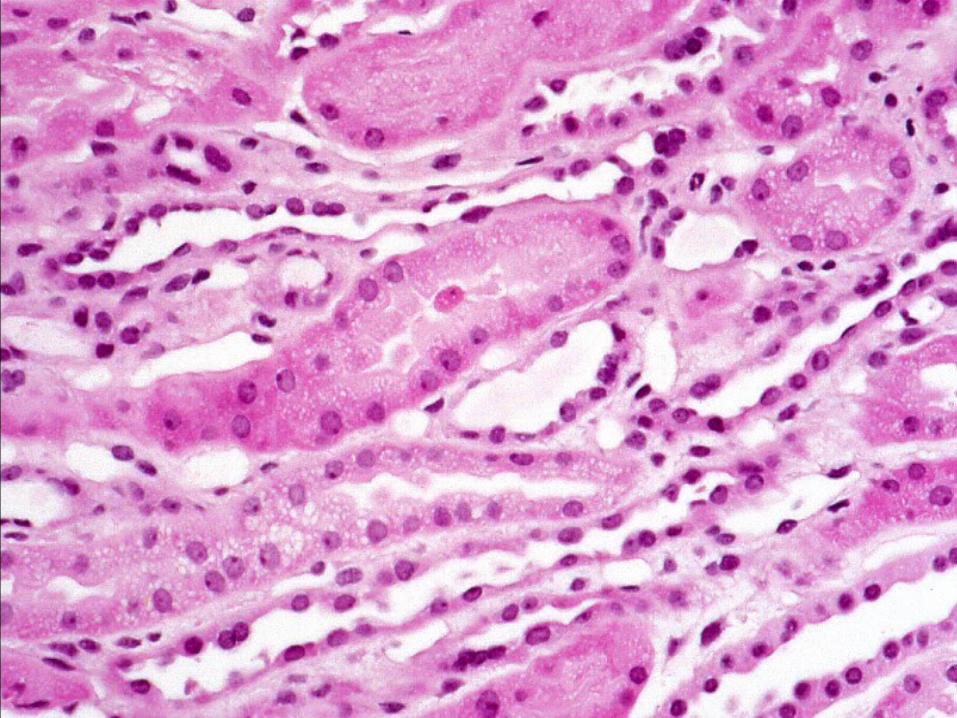
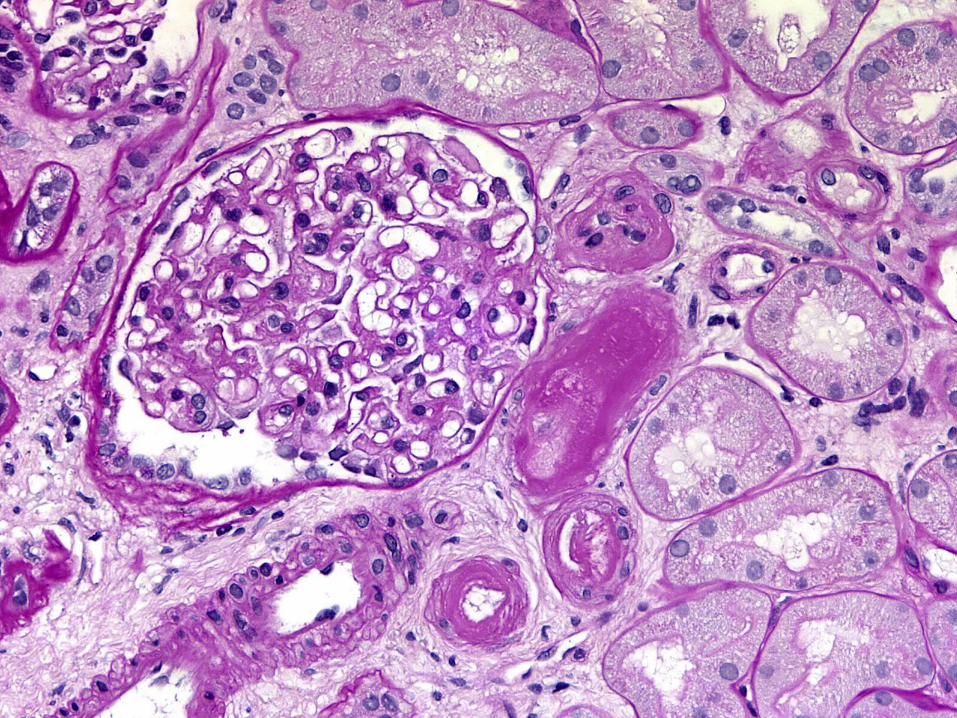
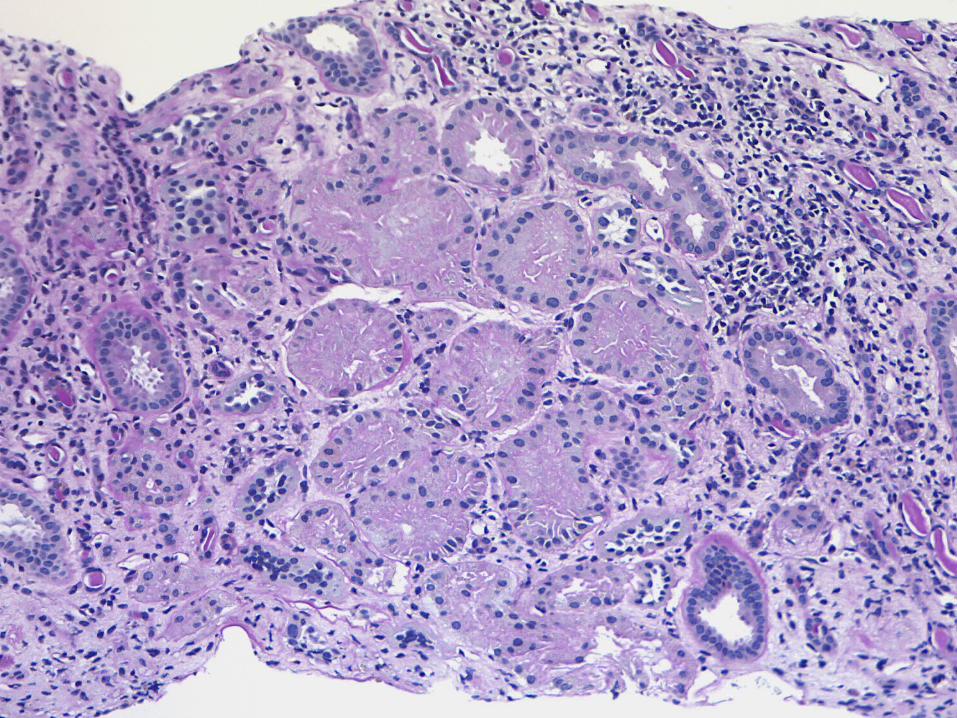
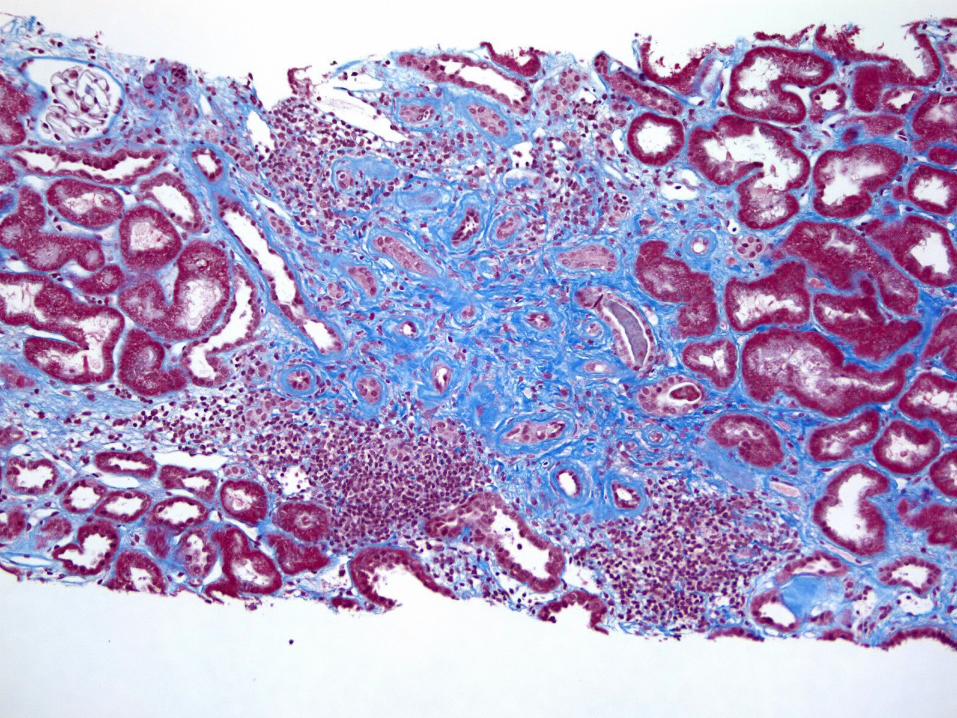
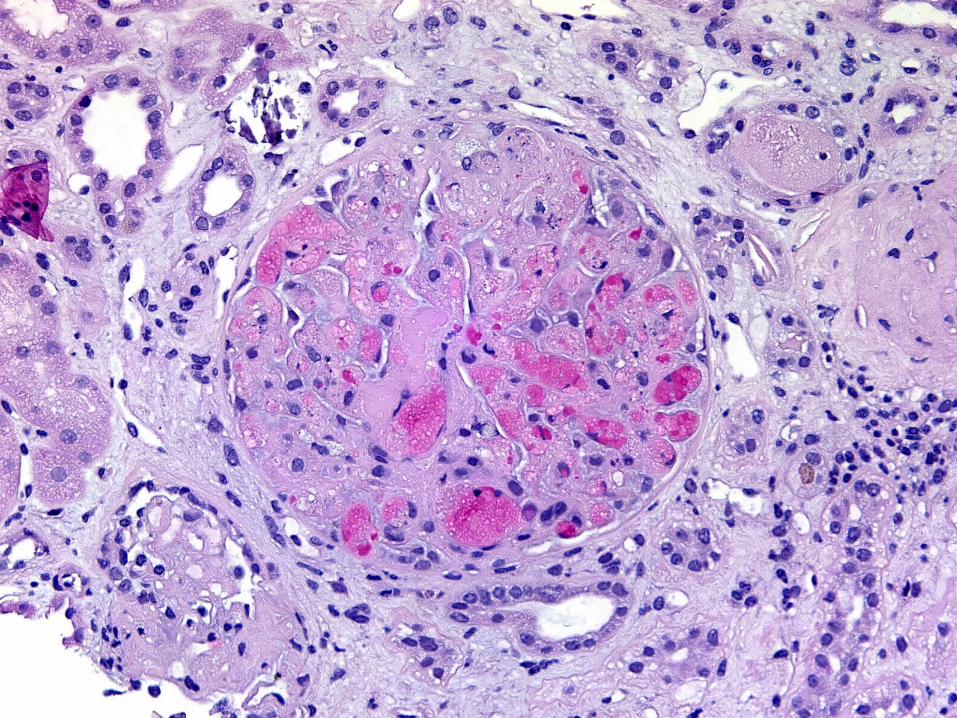
Features of CNI Toxicity
• Tubular isometric vacuolization• Arteriolar medial/peripheral
hyaline• Striped pattern of tubular atrophy
and interstitial fibrosis
* Ischemic collapse of glomeruli, Tubular dystrophic calcifications, juxtaglomerular apparatus hyperplasia
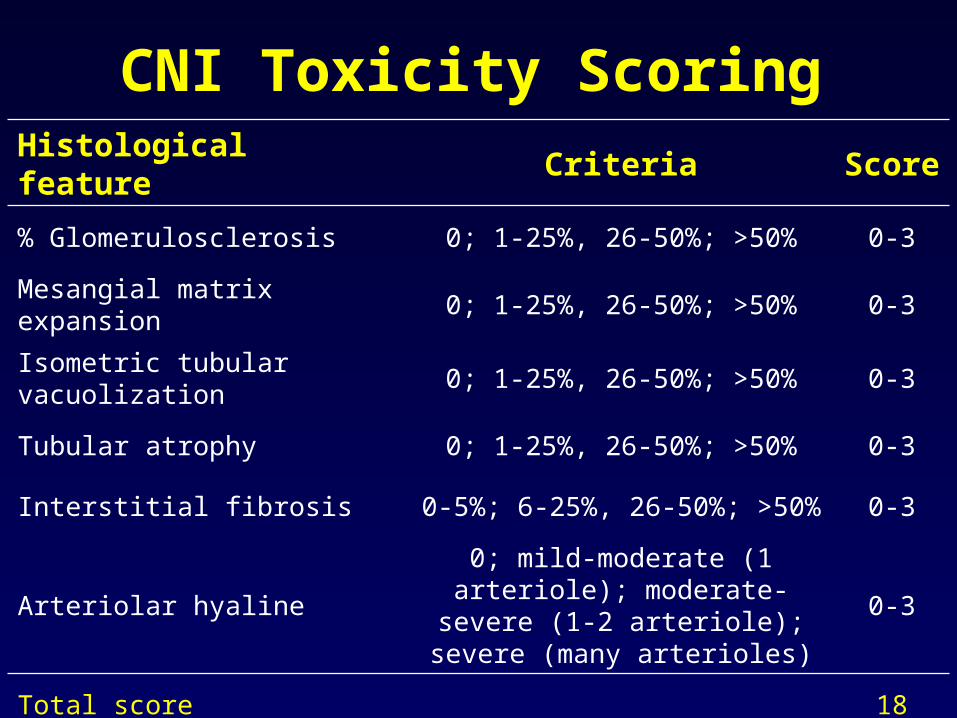
CNI Toxicity ScoringHistological feature Criteria
Score
% Glomerulosclerosis 0; 1-25%, 26-50%; >50% 0-3
Mesangial matrix expansion 0; 1-25%, 26-50%; >50% 0-3
Isometric tubular vacuolization
0; 1-25%, 26-50%; >50% 0-3
Tubular atrophy 0; 1-25%, 26-50%; >50% 0-3
Interstitial fibrosis 0-5%; 6-25%, 26-50%; >50% 0-3
Arteriolar hyaline
0; mild-moderate (1 arteriole); moderate-severe (1-2
arteriole); severe (many arterioles)
0-3
Total score 18
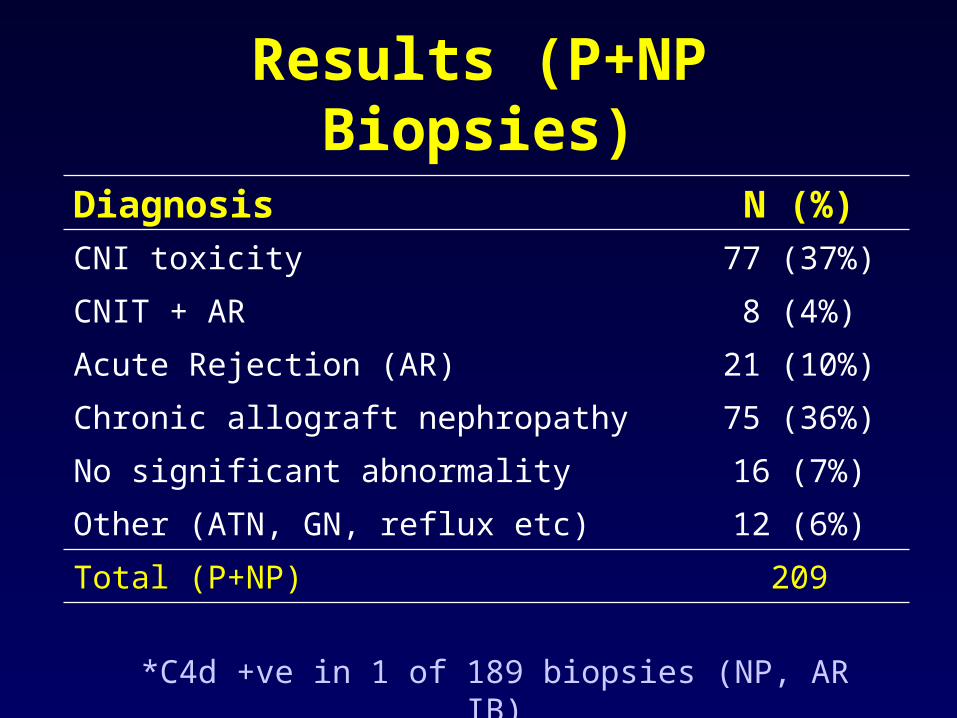
Results (P+NP Biopsies)
Diagnosis N (%)CNI toxicity 77 (37%)
CNIT + AR 8 (4%)
Acute Rejection (AR) 21 (10%)
Chronic allograft nephropathy 75 (36%)
No significant abnormality 16 (7%)
Other (ATN, GN, reflux etc) 12 (6%)
Total (P+NP) 209
*C4d +ve in 1 of 189 biopsies (NP, AR IB)
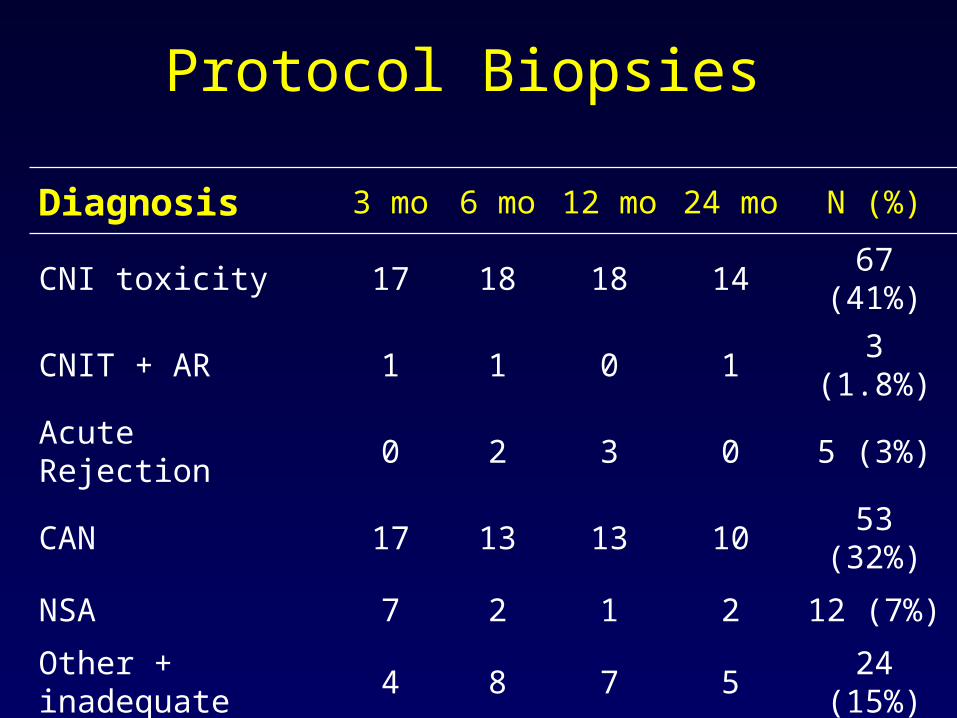
Protocol Biopsies
Diagnosis 3 mo 6 mo 12 mo 24 mo N (%)
CNI toxicity 17 18 18 14 67 (41%)
CNIT + AR 1 1 0 1 3 (1.8%)
Acute Rejection 0 2 3 0 5 (3%)
CAN 17 13 13 10 53 (32%)
NSA 7 2 1 2 12 (7%)
Other + inadequate
4 8 7 5 24 (15%)
Total 46 44 42 32 164
0
5
10
15
20
25
30
35
40
TV AH SF 2 or more
Diagnostic features
TV
AH
SF
2 or more
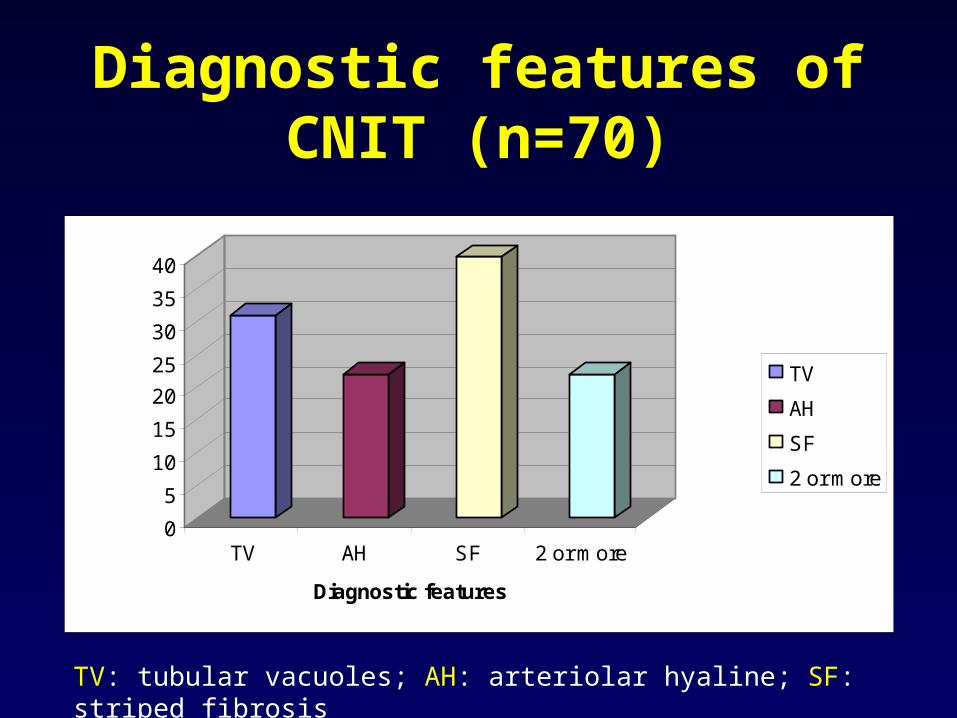
Diagnostic features of CNIT (n=70)
TV: tubular vacuoles; AH: arteriolar hyaline; SF: striped fibrosis
End points for graft function
• CNIT, BChS, MBChS and CADI correlated with– Creatinine Clearance (by Schwartz method)– Hypertension: # of anti-HTN agents to
normalize blood pressure– Proteinuria
• CNIT score also correlated with Tacrolimus trough levels (ng/ml) and dosage (mg/kg)
Follow up
• Mean follow up period: 25.7 months (range 24-44 months)
• 2 patients died with functioning grafts• None had urine protein/creatinine ratio >
1• Mean Creatinine Clearance at 24 months:
88.2 ml/min (range: 46-135)• Mean # anti-HTN agents: 0.27 (range 0-
2)
Results
• By Pearson parametric correlation (one side test)– CNI Toxicity Score at 3 months
significantly correlates with 12 mo CrCl (p=0.021, r2=-0.54) and 24 mo CrCl (p=0.03, r2 =-0.58)
Results…
– No correlation with hypertension, Tacrolimus dose or levels
– CADI, BChS and MBChS did not correlate with outcome
– CNIT and MBChS seem to correlate with each other*
* gs, ct and ci are common parameters in both
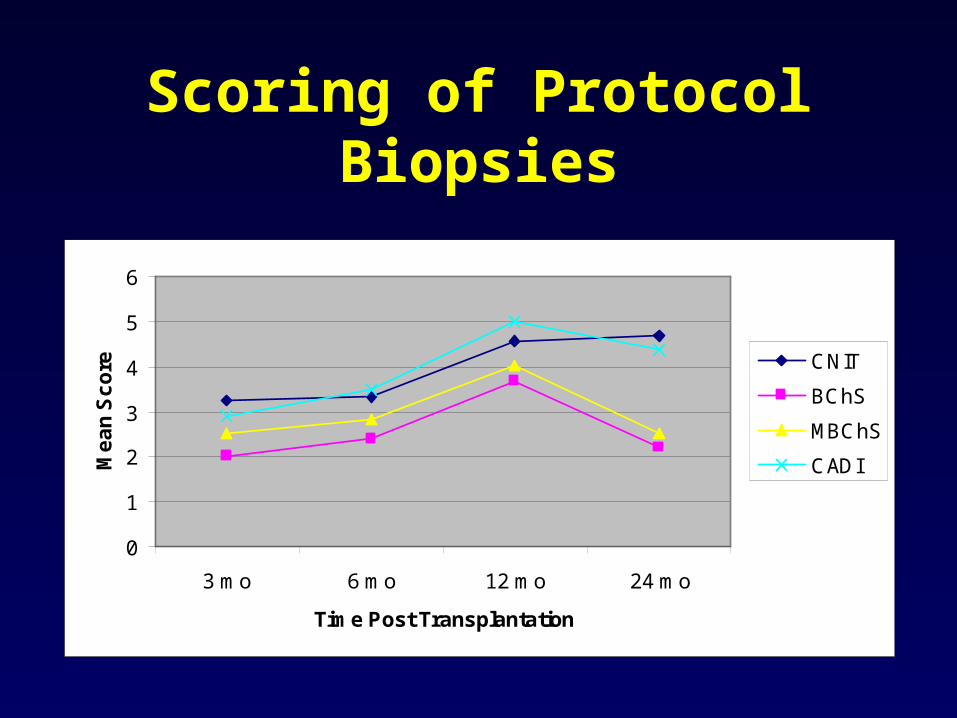
0
1
2
3
4
5
6
3 mo 6 mo 12 mo 24 mo
Time Post Transplantation
Me
an
Sc
ore CNIT
BChS
MBChS
CADI
Scoring of Protocol Biopsies
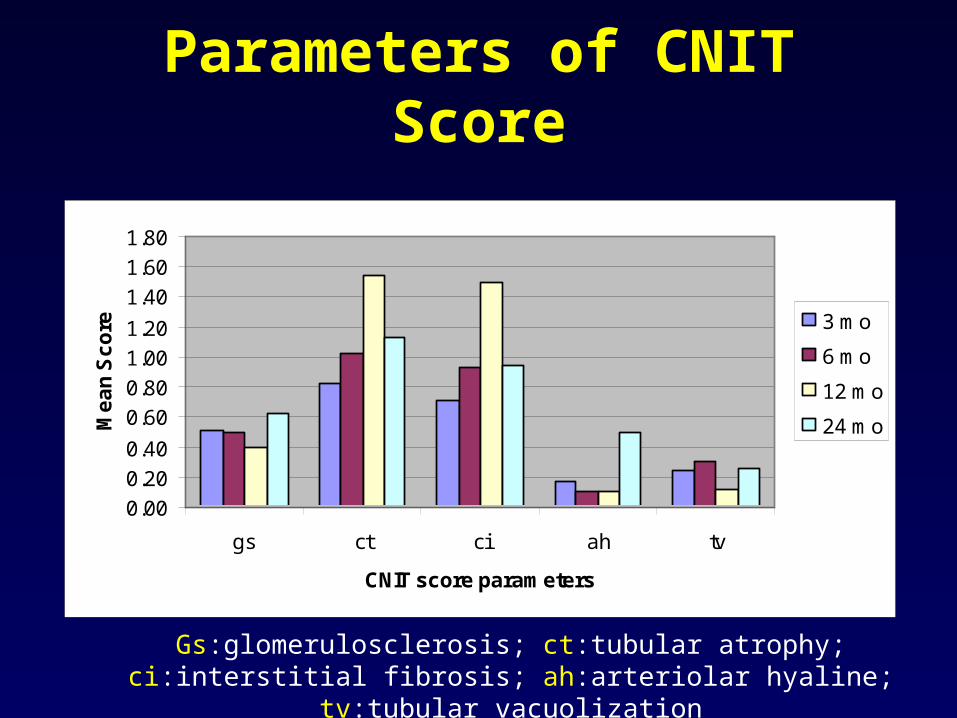
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
1.60
1.80
gs ct ci ah tv
CNIT score parameters
Me
an
Sc
ore 3 mo
6 mo
12 mo
24 mo
Parameters of CNIT Score
Gs:glomerulosclerosis; ct:tubular atrophy; ci:interstitial fibrosis; ah:arteriolar hyaline; tv:tubular vacuolization
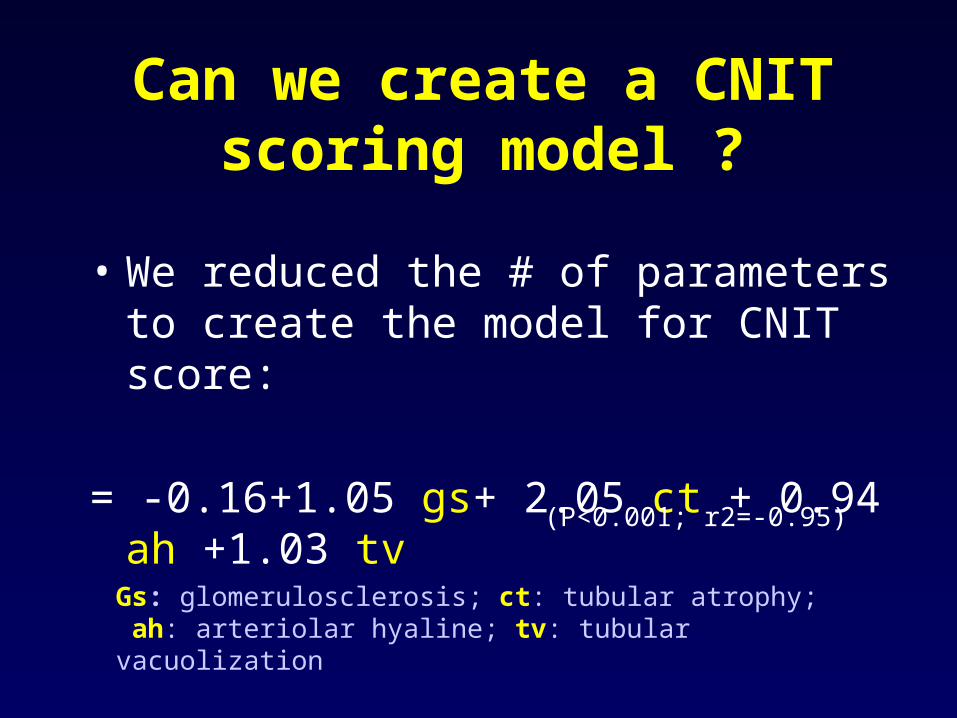
Can we create a CNIT scoring model ?
• We reduced the # of parameters to create the model for CNIT score:
= -0.16+1.05 gs+ 2.05 ct + 0.94 ah +1.03 tv
Gs: glomerulosclerosis; ct: tubular atrophy; ah: arteriolar hyaline; tv: tubular vacuolization
(P<0.001; r2=-0.95)
Testing the validity of the model
• Identified 14 patients with CNI toxicity on 3 month protocol biopsy with at least 12 months follow up
• Patients on steroid based (3) and steroid free (11) immunosuppression
• 11 patients had 24 mo post- txp follow up
Validity..
• Mean CNIT score (calculated using model): 4.08 (range 1.97-9.28)
• 3 month CNIT score correlated significantly – 12 mo CrCl (p= 0.02; r2 =-0.54) – 24 mo CrCl (p= 0.004; r2 =-0.75)
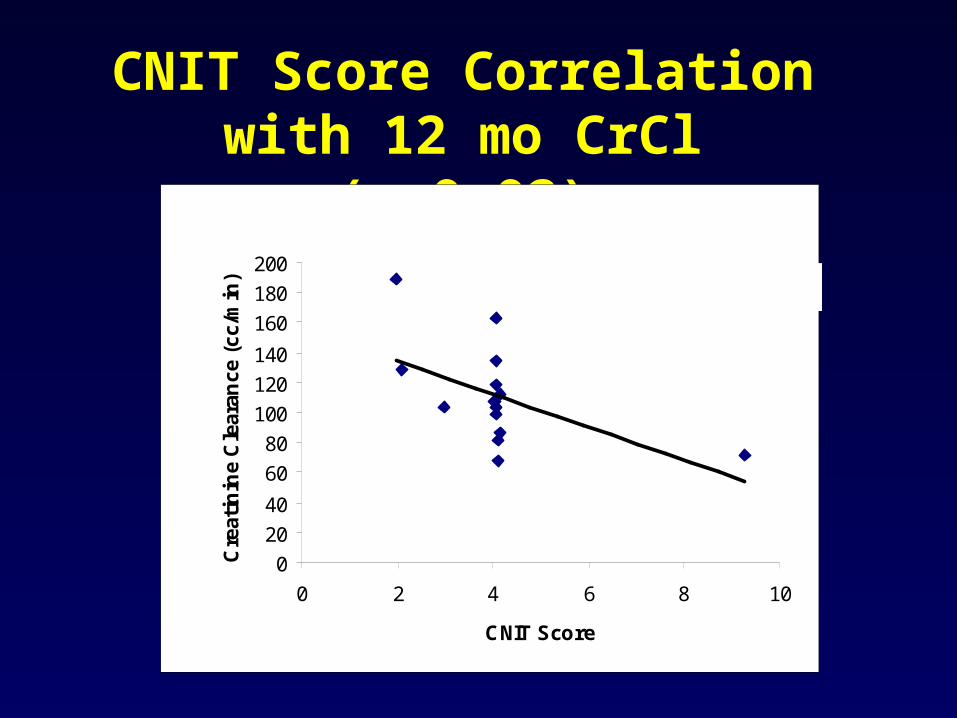
CNIT Score Correlation with 12 mo CrCl (p=0.02)
y = -10.97x + 156.69R2 = 0.2957
0
20
40
60
80
100
120
140
160
180
200
0 2 4 6 8 10
CNIT Score
Cre
atin
ine
Cle
aran
ce (
cc/m
in)
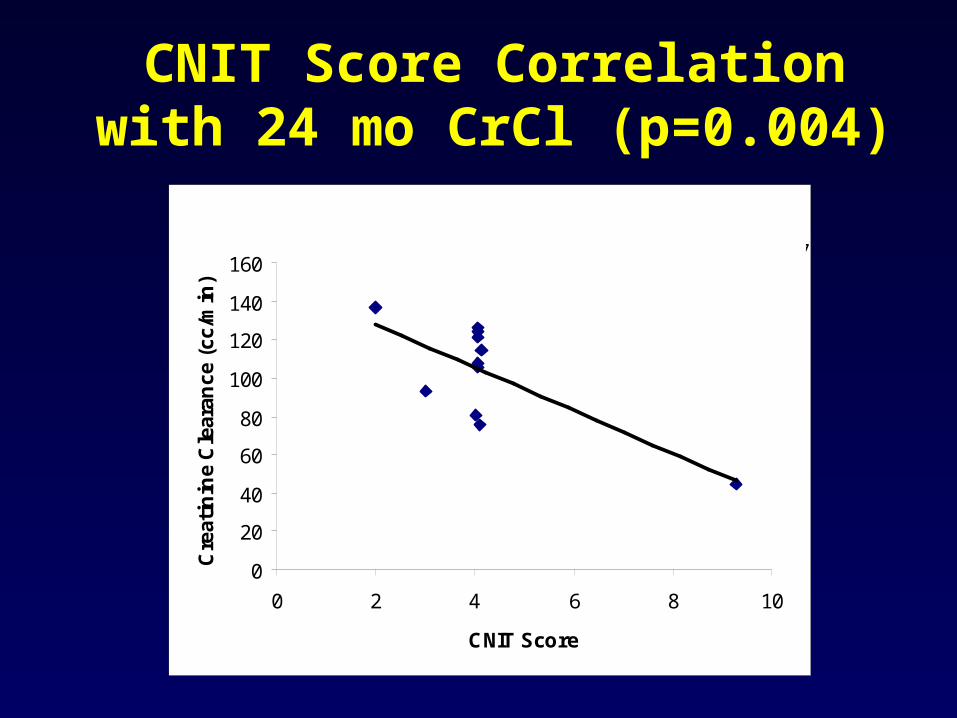
CNIT Score Correlation with 24 mo CrCl (p=0.004)
y = -11.194x + 150.37R2 = 0.5556
0
20
40
60
80
100
120
140
160
0 2 4 6 8 10
CNIT Score
Cre
atin
ine
Cle
aran
ce (
cc/m
in)
Scoring System
• Is linear scoring of parameters better?
• Image analysis may be helpful• Need to validate the data with more
protocol biopsies (steroid free and steroid based regimens)
• We are probably underestimating the incidence of CNI toxicity
Conclusions• CNIT score: helpful in objective
grading • A diagnosis of CNIT requires
aggressive monitoring of CNI therapy• Need to modify maintenance
immunosuppression • Arteriolar hyaline: most important
factor and likely irreversible cause of progressive loss of graft function
Minnie Sarwal M.D., Ph.D.– Suja Nagarajan, M.D.– Sheryl Shah– Li Li
Acknowledgements