calculating the position of the joint line of the knee ... · between the joint line and each...
TRANSCRIPT
NOVEMBER/DECEMBER 2016 | Volume 39 • Number 6
n Case Report
Of the commonly accepted techni-cal goals of a total knee arthro-plasty (TKA), restoration of the
joint line of the knee is important. Failure to restore the joint line of the knee to ana-tomical position can lead to mid-flexion instability, a reduction in range of motion, impingement of the patellar tendon against the tibial tray, and gap imbalance.1-5 Unfor-
tunately, successful restoration of the joint line relies heavily on the presence and in-tegrity of bone and soft tissue landmarks. Unlike in primary TKA, in revision TKA, the necessary landmarks are often missing or obscured, making restoration of the joint line both difficult and unreliable.
Numerous methods, ranging from relative references, including “2 finger
breadths from the tibial tubercle,” to ab-solute distances, including “10 mm from the fibular styloid,” have been described for joint line restoration, yet a lack of con-sensus remains.1,6,7 Alternatively, the joint line of the knee can be estimated on a preoperative radiograph by measuring the distance from the joint line of the knee to either the medial epicondyle, fibular head, or tibial tubercle.1,8 These methods cannot
Calculating the Position of the Joint Line of the Knee Using Anatomical LandmarksGavin C. Pereira, MBBS, FrCS (Tr & OrTh); eriCka vOn kaePPler, BS; MiChael J. alaia, MD; kenneTh MOnTini, MD; MaTThew J. lOPez, MD; Paul e. Di CeSare, MD; Derek F. aManaTullah, MD, PhD
abstract
Restoration of the joint line of the knee during primary and revision total knee arthroplasty is a step that directly influences patient outcomes. In revision total knee arthroplasty, necessary bony landmarks may be missing or obscured, so there remains a lack of consensus on how to accurately identify and restore the joint line of the knee. In this study, 50 magnetic resonance images of normal knees were analyzed to determine a quantitative relationship between the joint line of the knee and 6 bony landmarks: medial and lateral femoral epicondyles, medial and lateral femoral metaphyseal flares, tibial tubercle, and proximal tib-io-fibular joint. Wide variability was found in the absolute distance from each landmark to the joint line of the knee, including significant differences between the sexes. Normalization of the absolute distances to femoral or tibial diameters revealed reliable spatial relationships to the joint line of the knee. The joint line was found to be equidistant from the lateral femoral epicondyle and the proxi-mal tibio-fibular joint, representing a reproducible point of reference for joint line restoration. The authors propose a simple 3-step algorithm that can be used with magnetic resonance imaging, computed tomography, or radiography to reliably determine the anatomical location of the joint line of the knee relative to the surrounding bony anatomy. [Orthopedics. 2016; 39(6):381-386.]
The authors are from the Department of Or-thopaedic Surgery (GCP, MJL), University of Cal-ifornia, Davis Medical Center, Sacramento, and the Department of Orthopaedic Surgery (EvK, DFA), Stanford Hospital and Clinics, Palo Alto, California; the Department of Orthopaedic Sur-gery (MJA), New York University—Hospital for Joint Disease, New York, New York; the Depart-ment of Radiology (KM), The Mayo Clinic, Scott-sdale, Arizona; and the Department of Orthopae-dic Surgery (PED), New York Hospital Queens, Queens, New York.
Ms von Kaeppler, Dr Alaia, Dr Montini, Dr Lopez, and Dr Di Cesare have no relevant fi-nancial relationships to disclose. Dr Pereira has received research grants from Zimmer. Dr Ama-natullah is a paid consultant for Sanofi and has received research grants from Acumed.
Correspondence should be addressed to: Derek F. Amanatullah, MD, PhD, Department of Orthopaedic Surgery, Stanford Hospital and Clin-ics, 450 Broadway St, Redwood City, CA 94063-6342 ([email protected]).
Received: January 5, 2016; Accepted: July 14, 2016,
doi: 10.3928/01477447-20160729-01
381

Copyright © SLACK inCorporAted
n Case Report
be employed if there is no radiograph prior to TKA or if there is previous ipsilateral or contralateral tibial tubercle osteotomy. In another method, the inferior pole of the patella with the knee in 90° of flexion can serve as a guide to joint line position.9 This method, however, cannot be employed in the setting of patellar baja, tibial tubercle osteotomy, patellectomy, or prior TKA.
Anatomical studies have evaluated the distances from the femoral epicondyles, fibular head, and tibial tubercle to the joint line of the knee, in addition to the ratios of these absolute distances to femoral or tibial widths, compensating for sex and size differences.10,11 Although these previ-ous studies yielded valuable anatomical relationships, the absolute distances can be variable. Also, during revision TKA, the identification of the necessary anatomical landmarks can be exceedingly difficult. The purpose of this study was to determine a reproducible, quantitative relationship between the position of the joint line of the knee and identifiable anatomical land-marks about the knee.
Materials and MethodsFollowing institutional review board
approval, 50 randomly selected magnetic resonance images (MRIs) of normal adult human knees, originally obtained to rule out meniscal or cruciate ligament pathol-ogy after low-energy trauma, were exam-ined by 2 independent observers (M.J.A., K.M.). Joints reported by radiologists to have ligamentous pathology, degenera-tive articular cartilage, or osteochondral defects were excluded. The experimental group consisted of 50 adults between 24 and 49 years old, including 24 men be-tween 24 and 46 years old and 26 women between 24 and 49 years old. Each ana-tomical landmark was marked using a digital caliper, included as part of the MRI software.
The following anatomical landmarks were identified on MRI (Figure 1):
1. Joint line of the knee (JL): the line through the most distal points of the medial and lateral femoral condyles in the coronal plane, or the line through the most distal point of the femur perpendicular to the ana-
tomical axis of the tibial shaft in the sagittal plane.
2. Medial epicondyle (ME): the medial-most point on the femur from which the medial collateral ligament orig-inated; coronal section (ME to the joint line of the knee: MEJL).
3. Lateral epicondyle (LE): the most prominent bony point of the femur from which the lateral collateral ligament origi-nated; coronal section (LE to the joint line of the knee: LEJL).
4. Medial flare (MF): the point at which the medial femoral metaphyseal flare met the medial condylar cortex and also where the epiphyseal scar met the medial cortex; coronal section (MF to the joint line of the knee: MFJL).
5. Lateral flare (LF): the point at which the lateral femoral metaphyseal flare met the lateral condylar cortex and also where the epiphyseal scar met the lateral cortex; coronal section (LF to the joint line of the knee: LFJL).
6. Tibial tubercle (TT): the proximal-most corner of the junction between the tuberosity and the anterior cortex of the tibia8; sagittal section. If this corner was not identifiable, the most proximal point of the patellar tendon insertion was chosen (TT to the joint line of the knee: TTJL).
7. Proximal tibio-fibular joint (PTFJ): the center of the horizontal portion of the proximal tibio-fibular joint; coronal sec-tion (PTFJ to the joint line of the knee: PTFJJL) (Figure 2).
The absolute perpendicular distance between the joint line and each anatomi-cal landmark was measured and reported.
The following diameters were mea-sured (Figure 1):
A. Interepicondylar diameter of the femur (IED): the distance between the ME and the LE in the coronal plane, also known as the surgical transepicondylar axis; coronal section.
B. Intermetaphyseal diameter of the fe-mur (IMD): the distance between the MF and the LF in the coronal plane.
Figure 1: Coronal (A) and sagittal (B) diagrams of anatomical landmarks. Arrows: LE, lateral epicondyle; LF, lateral flare; ME, medial epicondyle; MF, medial flare; PTFJ, proximal tibio-fibular joint; TT, tibial tubercle. Red line: CTD, coronal tibial diameter; IED, interepicondylar diameter; IMD, intermetaphyseal diameter; STD, sagittal tibial diameter. The blue line represents the joint line of the knee in the coronal and sagittal planes.
A B
382

NOVEMBER/DECEMBER 2016 | Volume 39 • Number 6
n Case Report
C. Coronal tibial diameter (CTD): the diameter of the tibia at the level of the PTFJ in the coronal plane, perpendicular to the tibial shaft.
D. Sagittal tibial diameter (STD): the diameter of the tibia at the level of the TT in the sagittal plane, perpendicular to the tibial shaft.
To control for variation due to differ-ences between the sexes, the absolute dis-tances were normalized to their respective bony diameters by dividing the appropri-ate diameter by the corresponding abso-lute distance (eg, IED:MEJL).10,11 These were termed either “femoral ratios” or “tibial ratios.” To quantify the overall spa-tial relationship of the femoral and tibial landmarks about the joint line of the knee, the ratios between absolute femoral and tibial distances were reported. These were termed “femoro-tibial ratios.”
All measurements were repeated twice by each of the 2 observers. The mean of the 4 measurements was reported and the error was reported as SD. Statistically relevant results were determined via a 2-tailed Student’s t test and the signifi-cance level was chosen to be P<.005 after Bonferroni correction.
resultsThe absolute distances between each of
the anatomical landmarks and the joint line of the knee are presented in Table 1. With the exception of the TTJL, all of the mea-sured absolute distances were statistically different between the sexes (P<.005; Table
1). The absolute femoral and tibial diame-ters are listed in Table 2. All of the absolute diameters were also statistically different between the sexes (P<.005; Table 2).
To negate the effect of the difference between the sexes, the absolute distances between the anatomical landmarks and the joint line of the knee were normalized to their respective femoral or tibial diameters. The LEJL was found to be one-third of the IED (IED:LEJL=3.2±0.2). The femoral and tibial ratios for all of the landmarks are provided in Table 3. After normalization, no statistically significant differences in the femoral and tibial measurements remained
between the sexes (P>.05; Table 3). The CTD:TTJL and the STD:PTFJJL ratios were not calculated because it is not pos-sible to measure these absolute distances in the same plane of an MRI.
Finally, the overall spatial relationship of the femoral and tibial landmarks about the joint line of the knee was determined by calculating the ratios between absolute femoral distances and absolute tibial dis-tances. The LEJL was found to be equal to the PFTJJL (LEJL:PTFJJL=1.0±0.1), suggesting these landmarks are equidistant from the joint line. The femoro-tibial ra-tios for all of the landmarks are presented
Figure 2: Coronal magnetic resonance image show-ing the proximal tibio-fibular joint landmark. Abbrevi-ation: PTFJJL, proximal tibio-fibular joint to joint line.
Table 1
Absolute Distance From Each Anatomical Landmark to the Joint Line of the Knee
Mean±SD, mm
Current Study
Distance Overall Males Females Servien et al11 Mountney et al12
MEJL 27.6±3.2 29.1±3.2 26.2±2.6a 28.3±2.6 26.4±2.8
LEJL 23.6±2.3 25.1±2.0 22.4±1.8a 23.6±2.3 25.8±3.5
MFJL 41.5±4.0 44.0±3.8 39.3±2.8a
LFJL 35.1±3.8 38.0±3.0 32.6±2.4a
PTFJJL 22.2±3.2 23.5±3.1 21.1±2.9a
TTJL 20.9±4.4 21.5±4.4 20.5±4.5 22.3±2.8
Abbreviations: LEJL, lateral epicondyle to joint line of the knee; LFJL, lateral flare to joint line of the knee; MEJL, medial epicondyle to joint line of the knee; MFJL, medial flare to joint line of the knee; PTFJJL, proximal tibio-fibular joint to joint line of the knee; TTJL, tibial tubercle to joint line of the knee. aStatistically different from males (P<.005).
Table 2
Absolute Femoral and Tibial DiametersMean±SD, mm
Diameter Overall Males Females
IED 77.6±6.4 82.9±3.9 72.6±3.9a
IMD 72.7±6.1 77.7±3.9 68.2±3.7a
CTD 67.0±6.0 71.7±4.2 62.7±4.0a
STD 40.8±6.1 45.2±5.0 36.8±3.9a
Abbreviations: CTD, coronal tibial diameter; IED, interepicondylar diameter; IMD, intermetaphyseal diameter; STD, sagittal tibial diameter. aStatistically different from males (P<.005).
383

Copyright © SLACK inCorporAted
n Case Report
in Table 4. None of the femoro-tibial ra-tios showed statistically significant differ-ences between the sexes (P>.05; Table 4). Although the ratios using the TTJL require measurements in 2 different planes of an MRI, the authors included the TTJL in their femoro-tibial ratios because it is a po-tentially visible intraoperative landmark.
discussionThis study has defined the position of
the joint line with respect to the anatomi-cal landmarks about the knee and has in-
troduced the concept that the joint line is at a constant ratio from both the femoral and the tibial anatomical landmarks.
The authors confirmed the following absolute distances: MEJL (27.6±3.2 mm), LEJL (23.6±2.3 mm), PTFJJL (22.2±3.2 mm), and TTJL (20.9±4.4 mm). These data are comparable to those of previously published anatomical studies as reported in Table 1 and Table 3.10-12
Previous anatomical and radiographic studies have attempted to establish a re-producible relationship between the fibu-
lar head and the tibial plateau, but a con-sensus point of reference on the fibular head from which to make observations is lacking.13,14 In addition, the fibular sty-loid is variable in morphology.11 Further, the fibular styloid can be excised intraop-eratively, during the proximal tibial cut, and is not always available as a reference during revision TKA. The fibular head is highly variable and unreliable as an ana-tomical landmark.11,13,14
Compared with the fibular head, the PTFJ used in this study is a superior anatomical landmark. Unlike the fibular head, the PTFJ is a clearly defined ana-tomical landmark that can be seen on a plain radiograph, making it a widely us-able point of reference regardless of pre-operative imaging modality. If it is not visible because of fibular rotation, the PTFJ can be found at the intersection of the lateral prominence of the fibular head and the fibular styloid.
The authors observed that the LEJL has the lowest SD (2.3 mm) compared with the other landmarks (ie, MEJL, MFJL, LFJL, PTFJJL, and TTJL). This observation confirms previous reports that, despite statistically significant inter- and intraobserver variability, the mean LEJL intraobserver deviation was the most precise at 1.7 mm.15-17 This precision
Table 3
Femoral and Tibial RatiosCurrent Study
Ratio Overall Males FemalesRajagopal and
Nathwani10 Mountney et al12 Servien et al11
IED:MEJL 2.8±0.3 2.9±0.3 2.8±0.2 3.0±0.3 3.1±0.2
IED:LEJL 3.2±0.2 3.3±0.3 3.3±0.3 3.3±0.2 3.4±0.2 3.5±0.3
IMD:MFJL 1.7±0.2 1.8±0.2 1.7±0.1
IMD:LFJL 2.1±0.2 2.1±0.2 2.1±0.2
CTD:PTFJJL 3.3±0.5 3.1±0.5 3.0±0.5
STD:TTJL 1.9±0.6 2.2±0.6 1.9±0.6 2.0±0.1a
Abbreviations: CTD, coronal tibial diameter; IED, interepicondylar diameter; IMD, intermetaphyseal diameter; LEJL, lateral epicondyle to joint line of the knee; LFJL, lateral flare to joint line of the knee; MEJL, medial epicondyle to joint line of the knee; MFJL, medial flare to joint line of the knee; PTFJJL, proximal tibio-fibular joint to joint line of the knee; STD, sagittal tibial diameter; TTJL, tibial tubercle to joint line of the knee. aOriginally reported as TTJL:STD=0.5±0.1.
Table 4
Femoro-Tibial RatiosRatio Overall Males Females
MEJL:TTJL 1.4±0.3 1.4±0.3 1.3±0.3
LEJL:TTJL 1.2±0.2 1.2±0.3 1.1±0.3
MFJL:TTJL 2.0±0.4 2.1±0.5 2.0±0.5
LFJL:TTJL 1.7±0.3 1.8±0.4 1.7±0.4
MEJL:PTFJJL 1.3±0.2 1.3±0.3 1.3±0.2
LEJL:PTFJJL 1.0±0.1 1.1±0.2 1.1±0.2
MFJL:PTFJJL 1.9±0.3 1.9±0.3 1.9±0.3
LFJL:PTFJJL 1.6±0.3 1.6±0.3 1.6±0.3
Abbreviations: LEJL, lateral epicondyle to joint line of the knee; LFJL, lateral flare to joint line of the knee; MEJL, medial epicondyle to joint line of the knee; MFJL, medial flare to joint line of the knee; PTFJJL, proximal tibio-fibular joint to joint line of the knee; TTJL, tibial tubercle to joint line of the knee.
384

NOVEMBER/DECEMBER 2016 | Volume 39 • Number 6
n Case Report
is likely a direct result of the anatomy of this structure. The LE is readily identified as the most prominent point on the lateral distal femur, whereas, in contrast, the ME, for example, is actually a sulcus between 2 prominences on the medial distal femur. As such, the LEJL is the most reliable of the authors’ measured distances for accu-rate joint line reconstruction.
Individual variation related to sex renders absolute measurements of ana-tomical landmarks irrelevant.10,11 With the exception of the TTJL (P>.05), the authors found that all of the absolute dis-tances and diameters were significantly different between the sexes (P<.005). Normalization to diameter negates sta-tistically significant differences between the sexes, offering a more reliable metric for localizing the joint line. In addition, normalization eliminates susceptibility to magnification or positional distortion, which is present in all imaging formats. Normalization allows the authors’ MRI-based technique to be employed more broadly with either plain radiographs or computed tomography scans, as all of the landmarks used in this study are visible with these modalities as well.
The current authors’ data corroborate published computed tomography and MRI data (Table 3)10-12 that the LEJL was one-third of the IED (IED:LEJL=3.2±0.2) (Figure 3). This anatomical relationship is thus a valid and useful ratio for joint line determination. Further, the authors independently verified previous reports (Table 3)11 that the TTJL was one-half the STD (STD:TTJL=1.9±0.6) (Figure 3).
Among the authors’ most function-ally useful findings was the establish-ment of a novel femoro-tibial ratio of 1.0 between the LEJL and the PTFJJL (LEJL:PTFJJL=1.0±0.1). This suggests that the joint line of the knee is halfway between the LE and the PTFJ, 2 readily identifiable landmarks (Figure 3). This is the first description of an equidistant spa-tial relationship of anatomical landmarks around the joint line of the knee.
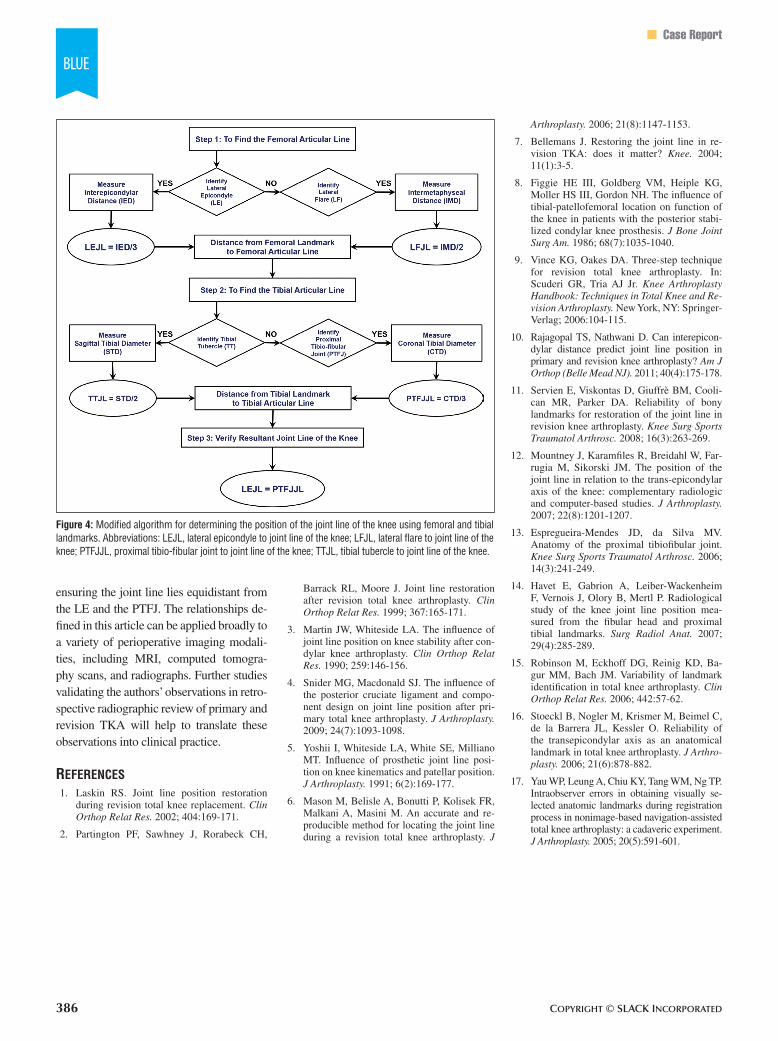
Servien et al11 first introduced the idea that normalization of absolute distances to femoral or tibial diameters can control for the high individual variability observed in absolute measurements about the joint line. They described the use of an epicon-dylar to femoral width ratio to determine the relative location of the joint line of the knee.11 On the basis of their own results, the current authors propose the following modification to the Servien et al11 algo-rithm for establishing the location of the joint line of the knee (Figure 4).
First, if the epicondyles are visible, determine the IED of the femur. The femoral articular line is approximately one-third this distance from the LE. If the epicondyles are difficult to identify, determine the IMD of the femur. The femoral articular line is one-half this dis-tance from the LF. Second, if the TT is visible, determine the STD. The tibial ar-ticular line is one-half this distance from the TT. If the TT is not visible, determine the CTD. The tibial articular line is ap-proximately one-third this distance from the PTFJ. Finally, the location of the joint line of the knee can be reliably verified using the authors’ novel reported LEJL to PTFJJL femoro-tibial ratio, as the joint
line should be equidistant from the LE and the PTFJ.
Incorporation of this algorithm into computer-assisted orthopedic surgery, especially when a preoperative MRI has been obtained (eg, patient-specific instru-mentation), may prove more useful than gross estimation. Further, the same spatial relationships used to calculate the position of the joint line of the knee relative to ana-tomical landmarks can be used in reverse to calculate the position of anatomical landmarks relative to the joint line of the knee. This reversal may be useful in es-timating ligament insertion points during reconstruction, especially when the iden-tification of an anatomical landmark (eg, ME and LE) is subject to high interob-server and intraobserver variability.15-17
conclusionThe purpose of this study was to deter-
mine a quantitative relationship between an-atomical landmarks about the knee and the joint line of the knee. The authors have pre-sented a modified algorithm for successful restoration of the joint line of the knee dur-ing TKA using the novel LEJL to PTFJJL femoro-tibial ratio. In TKA, successful res-toration of the joint line can be verified by
Figure 3: Relevant anatomical relationships about the joint line. Ratio of lateral epicondyle to joint line dis-tance (LEJL) to interepicondylar diameter (IED) (A). Ratio of tibial tubercle to joint line distance (TTJL) to sag-ittal tibial diameter (STD) (B). Ratio of LEJL to proximal tibio-fibular joint to joint line distance (LEJL:PTFJJL) (C). The blue line represents the joint line of the knee in the coronal and sagittal planes. Abbreviations: LE, lateral epicondyle; ME, medial epicondyle; PTFJ, proximal tibio-fibular joint; TT, tibial tubercle.
385
Copyright © SLACK inCorporAted
n Case Report
ensuring the joint line lies equidistant from the LE and the PTFJ. The relationships de-fined in this article can be applied broadly to a variety of perioperative imaging modali-ties, including MRI, computed tomogra-phy scans, and radiographs. Further studies validating the authors’ observations in retro-spective radiographic review of primary and revision TKA will help to translate these observations into clinical practice.
references 1. Laskin RS. Joint line position restoration
during revision total knee replacement. Clin Orthop Relat Res. 2002; 404:169-171.
2. Partington PF, Sawhney J, Rorabeck CH,
Barrack RL, Moore J. Joint line restoration after revision total knee arthroplasty. Clin Orthop Relat Res. 1999; 367:165-171.
3. Martin JW, Whiteside LA. The influence of joint line position on knee stability after con-dylar knee arthroplasty. Clin Orthop Relat Res. 1990; 259:146-156.
4. Snider MG, Macdonald SJ. The influence of the posterior cruciate ligament and compo-nent design on joint line position after pri-mary total knee arthroplasty. J Arthroplasty. 2009; 24(7):1093-1098.
5. Yoshii I, Whiteside LA, White SE, Milliano MT. Influence of prosthetic joint line posi-tion on knee kinematics and patellar position. J Arthroplasty. 1991; 6(2):169-177.
6. Mason M, Belisle A, Bonutti P, Kolisek FR, Malkani A, Masini M. An accurate and re-producible method for locating the joint line during a revision total knee arthroplasty. J
Arthroplasty. 2006; 21(8):1147-1153.
7. Bellemans J. Restoring the joint line in re-vision TKA: does it matter? Knee. 2004; 11(1):3-5.
8. Figgie HE III, Goldberg VM, Heiple KG, Moller HS III, Gordon NH. The influence of tibial-patellofemoral location on function of the knee in patients with the posterior stabi-lized condylar knee prosthesis. J Bone Joint Surg Am. 1986; 68(7):1035-1040.
9. Vince KG, Oakes DA. Three-step technique for revision total knee arthroplasty. In: Scuderi GR, Tria AJ Jr. Knee Arthroplasty Handbook: Techniques in Total Knee and Re-vision Arthroplasty. New York, NY: Springer- Verlag; 2006:104-115.
10. Rajagopal TS, Nathwani D. Can interepicon-dylar distance predict joint line position in primary and revision knee arthroplasty? Am J Orthop (Belle Mead NJ). 2011; 40(4):175-178.
11. Servien E, Viskontas D, Giuffrè BM, Cooli-can MR, Parker DA. Reliability of bony landmarks for restoration of the joint line in revision knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2008; 16(3):263-269.
12. Mountney J, Karamfiles R, Breidahl W, Far-rugia M, Sikorski JM. The position of the joint line in relation to the trans-epicondylar axis of the knee: complementary radiologic and computer-based studies. J Arthroplasty. 2007; 22(8):1201-1207.
13. Espregueira-Mendes JD, da Silva MV. Anatomy of the proximal tibiofibular joint. Knee Surg Sports Traumatol Arthrosc. 2006; 14(3):241-249.
14. Havet E, Gabrion A, Leiber-Wackenheim F, Vernois J, Olory B, Mertl P. Radiological study of the knee joint line position mea-sured from the fibular head and proximal tibial landmarks. Surg Radiol Anat. 2007; 29(4):285-289.
15. Robinson M, Eckhoff DG, Reinig KD, Ba-gur MM, Bach JM. Variability of landmark identification in total knee arthroplasty. Clin Orthop Relat Res. 2006; 442:57-62.
16. Stoeckl B, Nogler M, Krismer M, Beimel C, de la Barrera JL, Kessler O. Reliability of the transepicondylar axis as an anatomical landmark in total knee arthroplasty. J Arthro-plasty. 2006; 21(6):878-882.
17. Yau WP, Leung A, Chiu KY, Tang WM, Ng TP. Intraobserver errors in obtaining visually se-lected anatomic landmarks during registration process in nonimage-based navigation-assisted total knee arthroplasty: a cadaveric experiment. J Arthroplasty. 2005; 20(5):591-601.
Figure 4: Modified algorithm for determining the position of the joint line of the knee using femoral and tibial landmarks. Abbreviations: LEJL, lateral epicondyle to joint line of the knee; LFJL, lateral flare to joint line of the knee; PTFJJL, proximal tibio-fibular joint to joint line of the knee; TTJL, tibial tubercle to joint line of the knee.
386