calculating the window of opportunity to screen for ovarian cancer during early stages: a...
TRANSCRIPT
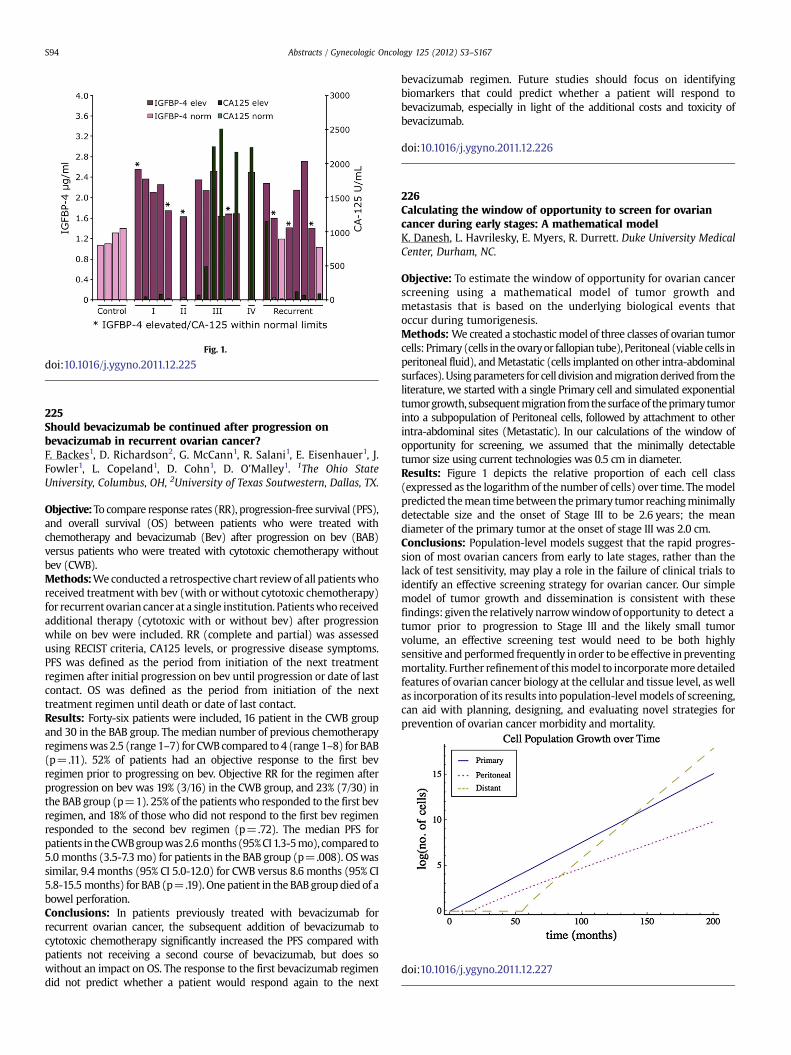
Fig. 1.
doi:10.1016/j.ygyno.2011.12.225
225Should bevacizumab be continued after progression onbevacizumab in recurrent ovarian cancer?F. Backes1, D. Richardson2, G. McCann1, R. Salani1, E. Eisenhauer1, J.Fowler1, L. Copeland1, D. Cohn1, D. O'Malley1. 1The Ohio StateUniversity, Columbus, OH, 2University of Texas Soutwestern, Dallas, TX.
Objective: To compare response rates (RR), progression-free survival (PFS),and overall survival (OS) between patients who were treated withchemotherapy and bevacizumab (Bev) after progression on bev (BAB)versus patients who were treated with cytotoxic chemotherapy withoutbev (CWB).Methods:Weconducted a retrospective chart reviewof all patientswhoreceived treatmentwith bev (with or without cytotoxic chemotherapy)for recurrent ovarian cancer at a single institution. Patientswho receivedadditional therapy (cytotoxic with or without bev) after progressionwhile on bev were included. RR (complete and partial) was assessedusing RECIST criteria, CA125 levels, or progressive disease symptoms.PFS was defined as the period from initiation of the next treatmentregimen after initial progression on bev until progression or date of lastcontact. OS was defined as the period from initiation of the nexttreatment regimen until death or date of last contact.Results: Forty-six patients were included, 16 patient in the CWB groupand 30 in the BAB group. The median number of previous chemotherapyregimenswas 2.5 (range 1–7) for CWBcompared to 4 (range 1–8) for BAB(p=.11). 52% of patients had an objective response to the first bevregimen prior to progressing on bev. Objective RR for the regimen afterprogression on bev was 19% (3/16) in the CWB group, and 23% (7/30) inthe BAB group (p=1). 25% of the patients who responded to the first bevregimen, and 18% of those who did not respond to the first bev regimenresponded to the second bev regimen (p=.72). The median PFS forpatients in theCWBgroupwas2.6 months (95%CI1.3-5mo), compared to5.0 months (3.5-7.3mo) for patients in the BAB group (p=.008). OSwassimilar, 9.4 months (95% CI 5.0-12.0) for CWB versus 8.6 months (95% CI5.8-15.5 months) for BAB (p=.19). One patient in the BAB groupdied of abowel perforation.Conclusions: In patients previously treated with bevacizumab forrecurrent ovarian cancer, the subsequent addition of bevacizumab tocytotoxic chemotherapy significantly increased the PFS compared withpatients not receiving a second course of bevacizumab, but does sowithout an impact on OS. The response to the first bevacizumab regimendid not predict whether a patient would respond again to the next
bevacizumab regimen. Future studies should focus on identifyingbiomarkers that could predict whether a patient will respond tobevacizumab, especially in light of the additional costs and toxicity ofbevacizumab.
doi:10.1016/j.ygyno.2011.12.226
226Calculating the window of opportunity to screen for ovariancancer during early stages: A mathematical modelK. Danesh, L. Havrilesky, E. Myers, R. Durrett. Duke University MedicalCenter, Durham, NC.
Objective: To estimate the window of opportunity for ovarian cancerscreening using a mathematical model of tumor growth andmetastasis that is based on the underlying biological events thatoccur during tumorigenesis.Methods: We created a stochastic model of three classes of ovarian tumorcells: Primary (cells in theovaryor fallopian tube), Peritoneal (viable cells inperitoneal fluid), andMetastatic (cells implanted on other intra-abdominalsurfaces). Usingparameters for cell division andmigrationderived fromtheliterature, we started with a single Primary cell and simulated exponentialtumorgrowth, subsequentmigration fromthesurfaceof theprimary tumorinto a subpopulation of Peritoneal cells, followed by attachment to otherintra-abdominal sites (Metastatic). In our calculations of the window ofopportunity for screening, we assumed that the minimally detectabletumor size using current technologies was 0.5 cm in diameter.Results: Figure 1 depicts the relative proportion of each cell class(expressed as the logarithm of the number of cells) over time. Themodelpredicted themean timebetween theprimary tumor reachingminimallydetectable size and the onset of Stage III to be 2.6 years; the meandiameter of the primary tumor at the onset of stage III was 2.0 cm.Conclusions: Population-level models suggest that the rapid progres-sion of most ovarian cancers from early to late stages, rather than thelack of test sensitivity, may play a role in the failure of clinical trials toidentify an effective screening strategy for ovarian cancer. Our simplemodel of tumor growth and dissemination is consistent with thesefindings: given the relatively narrowwindowof opportunity to detect atumor prior to progression to Stage III and the likely small tumorvolume, an effective screening test would need to be both highlysensitive and performed frequently in order to be effective in preventingmortality. Further refinementof thismodel to incorporatemore detailedfeatures of ovarian cancer biology at the cellular and tissue level, as wellas incorporation of its results into population-level models of screening,can aid with planning, designing, and evaluating novel strategies forprevention of ovarian cancer morbidity and mortality.
doi:10.1016/j.ygyno.2011.12.227
Abstracts / Gynecologic Oncology 125 (2012) S3–S167S94