california journal of health-system pharmacy · subscription rate for non-members is $75 per year;...
TRANSCRIPT

Perspective: Sacramento’s Fall Rhythm
Continuing Pharmacy Education (CPE): Recent Laws, Rulings and Programs Affecting the Practice of Pharmacy in California
Clinical Pearls: Inpatient Antiretroviral Prescribing for HIV-Positive Patients: Analysis of Error Rate and Associated Factors
Proposals to the 2011 CSHP House of Delegates
Call for Innovative Pharmacy Practice Project Examples
2011 CSHP Seminar Award Winners
September/October 2011 Volume 23, Number 5
www.cshp.org
California Journal of HealtH-SyStem PHarmaCy
Review of Last Year:This was a fantastically well done and unique event that successfully put together an opportunity to educate, network, and ski in one of the most beautiful places on earth. Please count me in for next year! - Grant Lackey, CSHP Member
Harvey’s/Harrah’s in South Lake Tahoecontinuing education • networking • fun in the snow
Register Now!
Visit www.cshp.org to learn more or register!
January 27 - 29, 2012

California Journal of Health-System Pharmacy
Official Journal of the California Society of Health-System Pharmacists1314 H Street, Suite 200, Sacramento, CA 95814
(916) 447-1033 FAX (916) 447-2396 www.cshp.org E-Mail [email protected]
Vol. 23 No. 5September/October 2011
CJHP (ISSN 1097-6337) is published bimonthly by the California Society of Health-System Pharmacists, 1314 H Street, Suite 200, Sacramento, CA 95814, under the guidance of the Editorial Advisory Board. The CJHP is distributed as a regular membership service, paid through allocation of membership dues. Subscription rate for non-members is $75 per year; single copies are $15. Periodicals postage paid at Sacramento, CA. Postmaster: Send address change to California Society of Health-System Pharmacists, 1314 H Street, Suite 200, Sacramento, CA 95814 (email: [email protected]).
The views expressed by authors of contributions in the California Journal of Health-System Pharmacy do not necessarily reflect the policy of CSHP or the institution with which the author is affiliated, unless this is clearly specified. Policy statements and official positions of CSHP are clearly labeled as such. The editor and publisher assume no responsibility for material contained in articles and advertisements published, nor does publication necessarily constitute endorsement by them. Letters to the editor are encouraged. Publisher reserves the right to edit, reject or publish whole or part of manuscripts submitted. No portion of this magazine may be reproduced, in whole or in part, without written consent of CSHP. © 2011 by the California Society of Health-System Pharmacists. Payments to CSHP are not deductible as charitable contributions for federal income tax purposes; however, they may be deductible under other provisions of the Internal Revenue Code.
For display and employment advertising, please contact Rebecca Brover, CSHP Director of Development at [email protected] or (916) 447-1033.
EditorDawn Benton
Managing EditorRebecca Brover, MBA
Contributing EditorJeanne Winnick Brennan
Design ConsultantHareLine Graphics
Editorial Advisory Board
CAlIfOrNIA SOCIEty Of HEAltH-SyStEm PHArmACIStS
Officers Maria Serpa [email protected] President Christine Antczak [email protected] President–electNancy Korman [email protected] Chair, Board of DirectorsVicky Ferraresi [email protected], House of DelegatesKenn Horowitz [email protected]
Directors Sylvia Banzon [email protected] Carr-Lopez [email protected] Daniel Dong [email protected] Goodrich [email protected] Kawahara [email protected] Perrin [email protected] Raff [email protected] Serrano Adams [email protected] Schneider [email protected]
Student Section Executive Committee Susan Cho [email protected] (Southern CA)
Ian Ford [email protected] (Northern CA)
Ex-OfficioDawn Benton [email protected] Vice President/CEO
Marcus Ravnan, ChairRon Floyd, Past-chairGary BesinqueAlexander CaoRochelle Castro-LeggKathy Daly
Bruce ManzoCathlene RichmondDan RossJessica SongDoris Wong
to complete the CPE self-assessment exams, go to www.HealthSystemCE.org.
You will be asked to log in and enter your password. Choose Journal CE and proceed with the exam. Once you complete the exam, you will be able to download/print your statement of credit for your records. HealthSystemCE.org is available for CSHP members.
Perspective: Sacramento’s Fall Rhythm ................................................................................4
Continuing Pharmacy Education: Recent Laws, Rulings and Programs Affecting the Practice of Pharmacy in California ............................................................5
Clinical Pearls: Inpatient Antiretroviral Prescribing for HIV- Positive Patients: Analysis of Error Rate and Associated Factors. ...............................................12
Proposals to the 2011 CSHP House of Delegates. .................................................17
Call for Innovative Pharmacy Practice Project Examples ......................................25
2011 CSHP Seminar Award Winners .......................................................................... 27

Sacramento’s Fall Rhythm Dawn Benton, mBA Executive Vice President and CEO
Perspective California Society of Health-System Pharmacists
fall is one of our busiest times of the year in Sacramento. After a long summer of combining work and vacation days with politi-
cians out of the Capitol and kids out of school, people return rested and ready to ratchet up their schedules. The rhythm of Sacramento picks up dramatically. The governor and his staff are racing the clock to sort out pending legislation that must be acted upon, and legislators are hovering over their pet bills’ final moments to see if they will fly or die by the governor’s pen. Against this backdrop, it’s crunch time for our staff as we finalize a multitude of details for our annual Seminar. And if this wasn’t enough, October is now when we officially draw attention to our industry with a planned event or activity for “National Hospital and Health-System Pharmacy Week”.
I am pleased to tell you that our staff is once again participating in the U.S. Drug Enforcement Agency’s national take back initiative to collect unused or expired medication and promote its safe disposal. The National Prescription Drug Take Back Day this fall is Saturday, October 29, 2011, from 10:00 a.m. to 2:00 p.m. across the country. With our local chapter of the California National Guard, we are hosting a site in downtown Sacramento in Cesar Chavez Park in front of city hall.
According to the 2009 Substance Abuse and Mental Health Services Administration’s National Survey on Drug Use and Health, more than seven million Americans currently abuse prescription drugs. Each day, approximately, 2,500 teens use prescription drugs to get high for the first time according to the Partnership for a Drug Free America. Studies show that a majority of abused prescription drugs are obtained from family and friends, including the home medicine cabinet. Events like these offer a tremendous opportunity to educate the public, and they also link us more directly with the average consumer. Can you think of a home without a medicine cabinet? In conjunction with state and local law enforcement agencies through-out the United States, the DEA conducted two drug take back days last spring and fall, and 309 tons of pills were collected.
At this fall’s event, Megan Blackwell on our staff has made it a priority also to include other pharmacy educational opportunities for consumers with representatives from the California Poison Control
System and a health fair with screening services provided by CNCP. This type of awareness provides a great customer service to thepublic and underscores the expertise of hospital pharmacy.
When we return to the Disneyland Hotel & Resort this fall for Seminar 2011 – A Whole New World of Healthcare, November 3-6 – we will have a program that will not disappoint. You can review the complete program and supporting documents at seminar.CSHP.org. Specifically, I’m delighted to remind pharmacy directors that we our holding the 2nd annual presentation breakfast on Saturday, November 5, from 7:30 to 9:00 a.m. that focuses on topics of key concern to you. Rita Shane, PharmD, FCSHP, FASHP, Director of Pharmacy at Cedars-Sinai Medical Center, will provide an update on her work with the California Board of Pharmacy regarding compounding regulations, and Dan Dong, PharmD, FCSHP, Area Pharmacy Director for Kaiser Permanente, will present on CSHP’s Title 22 Task Force recommen-dations to CDPH’s Licensing and Certification Division. Following these presentations, we will discuss the challenges you are facing and review how CSHP can assist you. I hope you will consider attending; this is a session you won’t want to miss. See you at Seminar! u
Spotted in the Sacramento area...Promoting Pharmacists and their contributions to patient safety.
4 cjhp: California Journal of Health-System Pharmacy September/October 2011

Learning Objectives:After reading this article, the reader should be able to:
1) Identify what the purpose of the Risk Evaluation and Mitigation Strategy (REMS) program entails for enhancing improved patient understanding of specific medications they have been prescribed.
2) List the types of drugs that the REMS Program provides information for and why.
3) Discuss new pharmacy-related laws introduced within the last year.
4) Describe the importance of the new labeling requirements as well as pending law that will place additional demands on pharmacists.
5) Identify proposed pharmacy-related laws that are being considered by the California legislature during the 2011 session period.
Accreditation Information0126-0000-11-112-H03-T0126-0000-11-112-H03-PRelease Date: November 1, 2011Expiration Date: November 1, 2014One credit hour
Requests for Information:Dr. Weissman is Associate Dean, Academic & Clinical Affairs, and Associate Professor of Pharmacy Practice at the Univ. So. Calif. School of Pharmacy. Email: [email protected]: (323) 442-1383
Continuing Pharmacy Education
recent laws, rulings, and Programs affecting the Practice of Pharmacy in California
fred G. Weissman, PharmD J.D.
IntroductionIn 2011, the federal government has expanded both the drugs involved in the Risk Evaluation and Mitigation Strategy (REMS) Program and the expectations placed upon health care professionals in follow-ing the Program’s requirements. The REMS Program further requires that Patient Medication Guides be a major information source to be provided to patients taking drugs that pose a higher than normal risk.
California has initiated new laws that deal with the Board of Pharmacy issuing “cease practice” orders if a licensee tests positive for any substance that is prohibited under the terms of the licensee’s probation or diversion program.1 The requirements upon the renewal of one’s license have gone through some regulatory changes.2 Besides the new prescription labeling requirements, there are upcoming rul-ings that will require ensuring that patients who do not comprehend information in English be provided interpretive services in the patient’s language.3 There is also the new statutory requirement pertaining to the pharmacist-in-charge notification to the Board.4 There have also been recent regulations on general non-sterile compounding of drug products.5 There are also several California Assembly and Senate bills that are up for consideration and possible passage
The Federal FDA Risk Evaluation and Mitigation Strategy (REMS) ProgramIn 2007, as a result of increasing concerns about medication safety, and building a system that better educates patients about the medi-cations they are taking, the FDA established the Risk Evaluation and Mitigation Strategies (REMS) Program. The REMS Program essen-tially is a post-marketing surveillance program that allows the FDA to review reports of adverse events, drug-drug interactions, and other drug related incidences, and to formulate written documentation of these events to be provided to health care professionals and ultimately patients where necessary.
Prior to REMS programming, the FDA established approaches to drug risk management by utilizing Risk Minimization Plans (RiskMaps) to alter unsafe prescribing and self-care practices by pre-scribers and patients. The RiskMap concept has been incorporated into the REMS regulatory thinking. As an example, isotretinoin was one of the high priority drugs to be dealt with under the RiskMap plan strategy in consideration of its use during pregnancy by the female or prior to pregnancy by the male partner.6,7
The FDA’s role associated with the REMS program is to create methods in which patients are to be informed about specific drugs and the risks versus the benefits associated with those drugs. In con-
sideration of potential risks associated with the taking of a drug or combination of drugs, there will be an increased role and extended expectation on the part of members of the health care team, and very much including pharmacists, to ensure that the patient is not only aware of the risks a drug can impose, but the need to monitor the patient while he or she is taking the drug.
Pharmacists will obviously play a major role in the developing REMS Programming as a result of the growing patient instructional resources that are being made available: 1) medication guides; 2)
September/October 2011 cjhp: California Journal of Health-System Pharmacy 5

CPE: Recent Laws
“Black Label” warnings; 3) patient package inserts; 4) medication counseling protocols that are being established; and 5) sources to sup-port “elements to assure safe use (ETASU)” of medications by patients.
Not every drug product has been subjected to review by the REMS program. At present, those drugs that appear to present the greatest concerns regarding patient safety have been placed at the forefront requiring special patient attention on the part of health care profes-sionals. Certainly, the inclusion of more drugs will follow.
The ultimate questions posed are: 1) What is the expected role of practicing pharmacists in ensuring the expectations of REMS program-ming is successful, and 2) Will the REMS program be able to achieve the purpose for which it was intended – to reduce patient medication problems?
The Material Resources To Help Make The REMS Program WorkIn order for the REMS Program to work, not only must there be appropriate resource materials available to aid medication users to fully understand what issues exist with the specific medications they are taking, but there must be trained health care profession-als, such as the pharmacist, who will not only ensure that patients receive written resource information, but also work with patients to make sure they thoroughly understand important matters associated with the use of their medications, and provide avenues of follow-up while patients are on their medications. What we have available as so-called “tools-of-the-trade” are medication guides, medica-tion communication plans and patient counseling, and elements to assure safe use (ETASU).8,9
Medication Guides: The FDA has approved printed medication guides as handouts, required by law, to be provided to a patient when the patient receives a medication. This guide is to be provided in order to: a) help prevent serious adverse effects resulting from the taking of the drug; b) help enhance informed patient decision-making once the patient understands the risks versus the benefits associated with the drug; and c) help the patient understand the importance of adhering to the directions for the use of the drug product in order to achieve optimum therapeutic benefit from the drug. Medication guides are considered one of the basic building blocks of REMS.10
While medication guides are required to be provided to outpatients receiving drugs, inpatients receiving drugs that have corresponding medication guides usually are not under the same standard since the drug is mainly administered by a healthcare professional that can both monitor and answer questions the patient may have about a drug they are receiving. However, the FDA may eventually develop policy requiring even inpatients to be recipients of medication guides. Medication Guides are to be made available to inpatients or their representatives if requested.11
Medication Communication Plans and Patient Consultations: The communication of information is crucial if REMS programming is to succeed. Health care providers such as prescribers and phar-macists need to know just about everything that is known about a given drug. The drug manufacturers need to ensure a network of constantly upgraded information about their drugs that includes both new information as well as older information that needs to be rein-forced as part of the patient’s understanding when they take a given drug. Prescribers and pharmacists need to be kept up to date about important information that is required to be passed onto the patient
regarding the taking of a specific drug, especially such information that suggests potential dangers or risks in the taking of a given drug. Thus, the channels of new drug information must be improved upon so that access is simple, timely, and uniform to the members of the health care team. At the same time, members of the health care team in a hospital setting should have open access to as much information about the patient’s medical condition, including laboratory results and other test procedures, as well as the treatment plan.
Elements To Assure Safe Use (ETASU): Because the REMS pro-gramming appears to be a presently accepted concept, factors such as special training, certification, and evaluation of practitioners may become requirements in order to ensure that members of the health care team are familiar with the educational materials available, risks of the drugs assigned to the REMS program, and the conditions required for safe use that would include appropriate patient counsel-ing. Some rather interesting outcomes might develop from ETASU concepts such as limit those drugs, or groups of those drugs where risks in taking are high, to only certified pharmacy operations that have been trained and certified regarding designated REMS-related drugs. Having patients sign agreements of understanding after a pharmacist’s intervention, to ensure that they, the patient, are fully aware of risks associated with a given drug and methods in which to hopefully mitigate those risks. Pharmacists involved in the dispens-ing of drugs that pose a high risk, should work in association with a health care unit that can provide necessary laboratory testing, and other assessment determinations to ensure the proper monitoring of a high risk drug that is to be self-administered by a patient. Pharmacists should acquire training in outcome studies related to data collected on patients who are receiving high risk drugs, so that such information can be shared within the pharmacy and medical community. The end result of such ETASU programming is to make health care profession-als more aware of better managing patients who are placed on high risk medications, and hopefully lessening the adverse problems that might otherwise be occurring.
The American Society of Health-System Pharmacists (ASHP) – Provision of A REMS Resource Center The ASHP has established an online REMS Resource Center that pro-vides basic information for pharmacists, patients and other healthcare professionals regarding over a hundred prescription medications that are adjudged by the FDA to be associated with a potential serious risk.12 The data base provided by ASHP lists the risk-related drugs alphabetically and provides a basic template that follows the format for the example noted below for Oxycodone (OxyContin®) in Table 1. The FDA continues to assess other drugs, both new and old to add to the REMS program. Recently a REMS review was conducted on a variety of opioid products.13 In April of 2011, the FDA released a REMS statement regarding long-acting and extended-release opioid products that includes the provision of new medication guides, but no other added responsibilities for pharmacists.14 Further, inpatient pharmacists in hospital settings will not be required to distribute opi-oid medication guides to patients at this time.15
A number of prescription drugs in the REMS Program require that the hospital/pharmacy, patient, and/or prescriber enroll in a program along with the possible verification by the pharmacy that the patient and/or the prescriber have also enrolled in a training program. It is important for pharmacists to be familiar with the prescription
6 cjhp: California Journal of Health-System Pharmacy September/October 2011

CPE: Recent Laws
drugs assigned to the REMS Program in order to follow the required mandates of the Program, with the major one being the provision of medication guides to patients that receive those drugs. As noted previously, medication guides that have been prepared per the requirements of the FDA are by law to be provided when the REMS-identified drug is dispensed to the patient.16
To determine what drugs the FDA has designated as being serious risk factors, the ASHP Website displaying the REMS Resource Center is an excellent source for identifying those drugs that are part of the REMS Program.
Recent California Pharmacy Laws Passed Or Being Considered
Pharmacist-In-Charge (PIC) Approval By The Board Of PharmacyThe California Board of Pharmacy now wants to grant approval to all future PIC assignments. This is a law that was passed in 2009 that you may not have encountered yet. All new PIC recommendations for assignment must be submitted to the Board.17 When a pharmacist vacates his or her position as a PIC, he or she must notify the Board within 30 days of leaving the PIC position. The management of that pharmacy must then submit the name, and other information about a new potential PIC candidate to the Board. The Board will then do a background check on the intended replacement. If the Board finds the new PIC recommendation unacceptable after doing a background check, the Board will send back a disapproval notice, and the phar-
macy management is then required to propose another replacement within 15 days of the date of the disapproval, and shall continue to name proposed replacements until a PIC is approved by the Board.
If a pharmacy is unable, in the exercise of reasonable diligence, to identify within 30 days a permanent or replacement PIC to propose to the Board, the pharmacy may instead provide the name of any phar-macist who is an employee, officer, or administrator of the pharmacy to act as the interim PIC for a period not to exceed 120 days.18
New Pharmacist License Renewal RequirementWhen a California pharmacist receives his or her license renewal form, two major changes will have taken place that must be complied with:19
1. There will be a space on the renewal form requesting disclosure of whether or not the licensee has been convicted of any viola-tion of the law in this or another state, omitting traffic infractions under $300 that do not involve alcohol, dangerous drugs, or controlled substances. Based upon the wording of the law, it will require the licensee to report traffic infractions of $300 or more regardless of what the infraction is for. Keep in mind this will be a reporting requirement for any violation that occurred within a two year period between each license renewal time.
2. Pharmacists licensed prior to 2002, when electronic fingerprint-ing was not available, are on notice that they need to submit electronic fingerprint records to the Board before their license renewal date. The fingerprints to be submitted require that they be done through an electronic scanning system to be forwarded to the California Department of Justice. It is important to com-ply with this electronic fingerprint requirement to prevent delay in receiving your license renewal. Remember, if your license is not renewed when due, or the requirement of electronic finger-printing is not met, it is possible that you might be practicing pharmacy without a license, and generally the Board places such an individual’s license in an “inactive status” until all renewal requests are met.
New Rules Regarding Prescription LabelsThe new rules regarding prescription labeling must be followed for outpatient prescription services. The new prescription label require-ment was put into effect on January 1, 2011. The purpose of the new labeling requirement is to emphasize on the label information of greatest importance (to be highlighted possibly using a colored back-ground along with using bolder or larger type) which shall include: the patient’s name, the name of the drug and strength, the directions for use, and the purpose for it being prescribed (if entered onto the prescription by the prescriber). This latter point of noting the purpose is being considered as a future requirement for all prescription labels that will require that the prescriber be contacted to provide that infor-mation if it does not appear on the prescription. Fifty percent (50%) of the label must be dedicated to the items of importance noted, and that information, as it is suggested, must be printed in at least 10 point sans serif font, and if requested by the patient, in 12-point font to accom-modate for vision deficiencies. The intent of this legislation is to make the prescription labels easier for patients to read, easier for patients to locate key information, and to improve patient understanding and compliance on how they are to take their medications.20
It is further important that patient’s understand the directions in a way that they properly administered the drugs prescribed. As an
TABLE 1 - Oxycodone
Q. A.
Why is this medication required to have a REMS?
The goal is to inform patients and health-care professionals about the potential for abuse, misuse, overdose, and addiction of Oxycontin.
Do I or my hospital/pharmacy have to enroll in a certain program?
No
Does the patient have to enroll in a certain program?
No
Does the prescriber have to enroll in a certain program?
No – but the prescriber must complete the “Oxycontin training” offered by Purdue Pharmaceuticals.
Do I have to verify that the patient and/or prescriber are enrolled?
No
Do I have to dispense a Med Guide or any other material to the patient?
Yes (however, not required in an inpatient setting)
Is there monitoring involved with this medication?
No
Can I order this medication through my usual supplier?
Yes
What do I have to document? Nothing
Am I required to complete CEs? No
Are there restrictions on amount of this medication (i.e., quantity dis-pensed, refills)?
No
Am I or my pharmacy subject to an audit by the manufacturer/FDA/or 3rd party?
No
September/October 2011 cjhp: California Journal of Health-System Pharmacy 7

CPE: Recent Laws
example, the regulation involved attempts to give clarity to such direc-tions as one tablet twice a day, or one tablet three or four times a day by stating that the medication needs to be taken in the morning and in the evening for a twice a day direction; and in the morning, afternoon, and evening for a three times a day direction; or in the morning, after-noon, early evening, and at bedtime for a four times a day direction.21
There are additional requirements in place to ensure that patients who do not ordinarily communicate in English, or do not understand English will need to be communicated with in their non-English language. The applicable regulation states that the pharmacy shall have policies and procedures in place to help patients who are not proficient in English, and to have interpretive services available in the language that the patient understands by phone or in-person dur-ing the pharmacy’s operational hours.22 Further, it is being proposed under a pending regulation recently considered by the Board of Pharmacy (Title 16, Calif. Code of Regs., Sec. 1707.6(c)) that a non-English speaking patient receiving a prescription will be able to point
California Assembly Bills Having An Effect On Pharmacy Practice Proposed For 2011*
The Bills Proposed For This Legislative Session Are Still In Committee
AB 310 Would prohibit health care service plans and health insurers that offer outpatient prescription drug coverage from requiring coinsurance, as defined, from the enrollee as a basis for cost sharing. The bill would also impose certain limitations on copayments, as defined, and out-of-pocket expenses for outpatient prescription drugs. The bill would make these provisions inoperative upon a determination by the department and commissioner that these provisions would result in additional costs to the state as a result of laws governing federal health care reform.
AB 369 Would impose specified requirements on health care service plans or health insurers that restrict medications for the treatment of pain pursuant to step therapy or fail first protocol. The bill would authorize the duration of any step therapy or fail first protocol to be determined by the prescribing physician and would prohibit a health care service plan or health insurer from requiring that a patient try and fail on more than two pain medications before allowing the patient access to other pain medication prescribed by the physician, as specified.
AB 377 Would require if passed that any unit-dose medication produced by a hospital pharmacy under common ownership be barcoded to be readable at the patient’s bedside. The hospital pharmacy would be able to prepare and store a limited quantity of unit-dose medications in advance of receipt of a patient-specific prescription in a quantity as is necessary to ensure continuity of care for an identified population of patients of the hospital based on a documented history of prescriptions for that patient population.
AB 1280 Would prevent the retail sale of any nonprescription products containing ephedrine, pseudoephedrine, norpseudoephedrine, or phenylpropanolamine to a person, via an alert system, where an alert is generated to not sell such products to a given purchaser.
California Senate Bills Having An Effect On Pharmacy Practice Proposed for 2011*
The Bills Proposed For This Legislative Session Are Still In Committee
SB 260 Would make it a felony punishable by imprisonment to possess, without regard to intent, 1⁄2 pound or more of ephedrine or pseudoephedrine, or any salts, isomers, or salts of isomers of ephedrine or pseudoephedrine, or 1⁄2 pound or more of a substance containing ephedrine or pseudoephedrine, or any salts, isomers, or salts of isomers of ephedrine or pseudoephedrine.
SB 360 Existing law requires that prescription forms for controlled substance prescriptions be obtained from security printers approved by the Dept. of Justice. The bill would require security printers to obtain photo identification from the customer and maintain a log of the information, and to report any theft or loss of controlled substance prescription forms to the department via fax or e-mail within 24 hours of the incident.
SB 393 Would establish the Patient-Centered Medical Home Act of 2011 and would define medical home and other terms, as specified.
SB 514: Would restrict the sale of nonprescription drug products containing dextromethorphan to persons under 18 years of age. To sell a dextromethorphan product to anyone under the age of 18 would constitute an infraction, punishable by a fine not to exceed $250.
SB 632 Would prohibit a pharmacist from interchanging or substituting an opioid analgesic drug, as defined, for an opioid analgesic drug incorporating a tamper resistant technology, as defined, unless the opioid analgesic drug to be interchanged or substituted is described on a list to be prepared by the Board of Pharmacy. In those situations where the drug is not on the Board’s list, the bill would require the pharmacist to obtain consent from the prescriber prior to an interchange or substitution.
to a notice posted in a conspicuous position or on a video display screen in the outpatient pharmacy and show the pharmacist what language they understand, and that an interpreter will be provided at no cost. The proposed notice (either posted or available in a flyer) shall have interpretation services available in at least the following languages: Arabic, Armenian, Cambodian, Cantonese, Farsi, Hmong, Korean, Mandarin, Russian, Spanish, Tagalog, and Vietnamese.23
Other languages shall also be added over time. There is additional consideration to possibly have the prescription labels printed in the language and script of the non-English language requested. This would require special language writing interactive programming.
The Use Of Mobile PharmaciesThe use of mobile pharmacy units is not necessarily a new concept. The VA and other states have employed the use of mobile pharmacies especially in association with major disasters such as what occurred during hurricane Katrina.24 In California the Board has recently made
*Current at time of publication
8 cjhp: California Journal of Health-System Pharmacy September/October 2011

CPE: Recent Laws
the requirement to obtain a special sterile compounding license from the Board.”29
Some recent requirements have been established by the Board of Pharmacy for non-sterile compounding in pharmacies. While phar-macies that compound non-sterile products do not require separate licensing by the Board, they are now required to operate such com-pounding services consistent with recently formulated regulations as noted below. These same compounding standards are also required for sterile compounding pharmacy operations as well.30
Keeping a master formula record: If a drug product is routinely compounded by a pharmacy, the pharmacy will be required to main-tain a written master formula record that shall include the following elements: a) active ingredients to be used; b) inactive ingredients to be used; c) process and/or procedure used to prepare the compounded product; d) quality reviews required at each step in the preparation of the compounded product; e) post-compounding process or proce-dures required, if any; and f) expiration dating requirements.31 Where a pharmacy does not routinely compound a particular drug product, the master formula record for that product may be recorded on the prescription document itself.32
A filled-out non-sterile self-assessment form must be maintained: The compounding self-assessment form is a two-part document, one section for sterile compounding, and the second section for non-sterile compounding. The applicable forms, along with the general pharmacy operations self-assessment form, must be completed by the PIC before July 1 of each odd-numbered year, or within 30 days of the start of a new PIC, or within 30 days of the issuance of a new phar-macy license.33 These self assessments are kept within the pharmacy, and to be made available if requested by the Board of Pharmacy or Board inspector.
Record requirement for each compounded product: For each compounded drug product, the pharmacy records shall include: a) the master formula record; b) the date the drug product was compound-ed; c) the identity of the pharmacy personnel who compounded the drug product; d) the identity of the pharmacist reviewing the final drug product; e) the quantity of each component used in compounding the drug product; f) the manufacturer and lot number of each component used (exempt from this requirement are sterile products compounded on a one-time basis for administration within 24 hours to an inpatient in a health care facility); g) the equipment used in compounding the drug product; h) a pharmacy assigned reference or lot number for the compounded drug product; i) the expiration date of the final com-pounded drug product (cannot exceed 6 months); and j) the quantity or amount of drug product compounded. Records produced shall be maintained in the pharmacy for at least three years from the date the record was created.34
Compounding Policies and Procedures required: The policy and procedure manual to be created for compounding operations shall contain procurement of drug procedures, methodologies for the formulation and compounding of drugs, facilities and equipment cleaning, maintenance, operation, and other standard operating pro-cedures related to compounding. The policy and procedures manual shall be reviewed on an annual basis by the PIC and shall be updated whenever changes are implemented.35
Training of compounding staff: The pharmacy for those pharmacy staff members involved in drug compounding, shall maintain written documentation that demonstrates that the personnel involved have
provisions for allowing the use of mobile pharmacies in two circum-stances: a) during a declared federal, state, or local emergency; and b) where a pharmacy operation is destroyed or made non-accessible.
During a declared state of emergency, the Board shall allow for the placement of mobile pharmacy units to operate in impacted areas provided the following conditions are met:25
a) The mobile pharmacy shares common ownership with at least one currently licensed pharmacy in good standing.
b) The mobile pharmacy retains records of dispensing.c) A licensed pharmacist is on the premises and the mobile pharma-
cy is under the control and management of a pharmacist while the drugs are being dispensed.
d) Reasonable security measures are taken to safeguard the drug supply maintained in the mobile pharmacy.
e) The mobile pharmacy is located within the declared or affected emergency area.
f) The mobile pharmacy ceases the provision of services within 48 hours following the termination of the declared emergency.
The second provision allows for maintaining a mobile pharmacy as a result of a pharmacy’s inability to function due to such cir-cumstances as a fire, flood, or other situations that will render the pharmacy inaccessible. If such is the case, the requirements noted above in a declared state of emergency would be followed with some further considerations:26
a) The mobile pharmacy shall provide services only on or imme-diately contiguous to the site of the damaged or destroyed pharmacy.
b) The mobile pharmacy will continue to be under the control and management of a PIC.
c) The pharmacy operating the mobile pharmacy provides the Board with records of the destruction of, or damage to, the pharmacy and expected restoration date.
d) Within three calendar days of restoration of pharmacy services, the Board is provided with notice of the restoration of the per-manent pharmacy, and that the mobile pharmacy is not to be in operation for more than 48 hours following the restoration of the permanent pharmacy.
Pharmacy Compounding UpdateBeginning in 2010, community pharmacies that intended to do compounding of sterile products were required by the Board to have special licensing for this purpose.27 In order for a community pharmacy to be licensed to do sterile compounding, the Board upon inspection of the pharmacy mandated that there be strict adherence to a host of requirements: a) a well-developed policy and procedure manual; b) an area sufficient to perform sterile compounding; c) nec-essary equipment to perform sterile compounding; d) special labeling of compounded products; e) proper and accurate recordkeeping of all compounded sterile products; f) description of attire to be worn while compounding; g) outlines of training programs for staff, patients, and caregivers; h) provisions for the methods of disposal of waste materials; i) quality assurance programming; and j) the maintenance of appropriate reference materials.28 “Pharmacies operated by entities that are licensed by either the Board or the State Department of Public Health and that have current accreditation from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO), or other pri-vate accreditation agencies approved by the Board, are exempt from
September/October 2011 cjhp: California Journal of Health-System Pharmacy 9

CPE: Recent Laws
the skills and training required to properly and accurately perform their assigned responsibilities relating to drug compounding. There shall also be on-going competency evaluations for all pharmacy involved in drug compounding, and there shall be maintained docu-mentation of any and all training related to compounding undertaken by pharmacy personnel.36
Drug compounding quality assurance: The pharmacy shall main-tain as part of its written policies and procedures, a written quality assurance plan designed to monitor and ensure the integrity, potency, quality, and labeled strength of all compounded drug products. The quality assurance plan should further include written procedures for verification, monitoring, and review of the adequacy of the com-pounding process and shall also include written documentation of review of those processes by pharmacy personnel. There should be included qualitative and quantitative analysis reports for compounded products, along with an action plan in the event any compounded drug product is ever found to be below minimum standards for integ-rity, potency, quality, or labeled strength.37
Changes In The California Controlled Substances ActFor decades the drug substance apomorphine had been assigned as a Schedule II controlled substance in California. Federally, the drug was never identified as a controlled substance, primarily because of its intense emetic effect. Apomorphine has been removed from the Schedules, and is no longer recognized as a Schedule II controlled substance in California.38
Proposed California Legislature Bills Affecting PharmacyThe California legislative session for 2011 has introduced a number of bills in both the Assembly and the Senate, and those bills are pres-ently in a committee of the Assembly or Senate for review. In the tables below is a sampling of those bills that if passed may directly or indirectly affect the practice of pharmacy in California.39
Conclusion2011 is perhaps the test year for how well the REMS Programming operates, and how well patients respond to understanding the dan-gers imposed by the higher-risk drugs they are taking. While written information is both important and now required in the form of Patient Medication Guides, the role of the prescriber and the pharmacist may become more demanding in ensuring that patients not only compre-hend the risks that may be involved with regarding the drug or drugs they are taking, but what action they are to take when the drug poses an experienced serious adverse effect. At the same time, prescribers and pharmacists need to also ensure the patients of how important the drug they are taking is in achieving the necessary therapeutic effect intended. While we do not as health care practitioners wish to scare patients about the drugs they are prescribed, it will be the manner in which we convey important information that will count, and to let the patient know that we are available, care and should be called upon whenever they have a question or concern about a medication they are taking.
Passed California statutes and regulations for 2011, while not unusually extraordinary, tend to put more controls in place (PIC approval by the Board, license renewal information regarding vio-lations of the law within the two year renewal period, new patient labeling requirements, and adopted non-sterile compounding require-ments). Other laws provide more access to pharmacy services in case of declared states of emergency or a pharmacies inability to operate (the use of mobile pharmacy laws).
Laws being proposed will probably add to the requirements associ-ated with the prescription label (placement on the label the medical condition for which the drug was prescribed, and possible directions to the patient in a non-English language that the patient will under-stand). The possible bar-coding of all drugs that are administered to a patient in a hospital setting, the restriction of over-the-counter sales of dextromethorphan to individuals under the age of 18 years old, and the method in which the FDA will require prescription drugs placed in the stream of commerce to be authenticated as labeled, will all be both some of the up-coming concerns that will need to be dealt with over the next couple of years.u
to complete the CPE self-assessment exam for this article, go to www.HealthSystemCE.org.
1. Calif. Bus. & Prof. Code, Sec. 315.2
2. Title 16, Calif. Code of Regs., Sec. 1702
3. Ibid. at Sec. 1707.5(b)(d)
4. Calif. Bus. & Prof. Code, Sec. 4113(d)
5. Title 16, Calif. Code of Regs. Secs. 1735-1735.7
6. Soller, R. William, The REMS Primer: Understanding the Strategies for Risk Management Medscape CE Program, Dec. 28, 2010
7. Food and Drug Administration. Isotretinoin (marketed as Accutane) capsule information. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm094305.htm Updated October 22, 2010. Accessed November 2, 2010.
8. 110th Congress. FDA Administrative Amendment Act (FDAAA). Title IX: Enhanced Authorities Regarding Postmarket Safety of Drugs. Public law 110-85., September 27, 2007. Available at: http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?dbname=110_cong_pub-lic_laws&docid=f:publ085.110.pdf Updated February 9, 2009. Accessed November 2, 2010.
9. Food and Drug Administration. Guidance for Industry Format and Content of Proposed Risk Evaluation and Mitigation Strategies (REMS), REMS Assessments, and Proposed REMS Modifications. Draft Guidance. September 2009. Available at: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM184128.pdf.
10. Soller, R. William, The REMS Primer: Understanding the Strategies for Risk Management Medscape CE Program, Dec. 28, 2010.
11. FDA Drug Safety Report. Guidance For Industry, Medication Guides – Distribution Requirements and Inclusion in Risk Evaluation and Mitigation Strategies (REMS), Draft Guidance. February 2011.
12. ASHP Website, REMS Resource Center, 2011.
13. Drug Industry Daily, FDA Unveils New Opioid REMS, Could Include Prescriber Education, Vol. 10 No.78, April 20, 2011.
14. Thompson, CA. Long-awaited Opioid REMS Affects Prescribers More Than Dispensers. Am J Health-Syst Pharm; Vol. 68, June 1, 2011, pg. 963.
15. Ibid. at pg. 967.
16. 21 CFR 208.24 (c) and 21 CFR 208.26(b)
17. Calif. Bus. & Prof. Code, Sec. 4113(d)
18. Ibid. at Sec. 4113(e)
19. Title 16, Calif. Code of Regs., Sec. 1702
20. Calif. Bus. & Prof. Code, Sec. 4076.5
21. Title 16, Calif. Code of Regs., Sec. 1707.5
22. Ibid. at Sec. 1707.5
23. Proposed as Title 16, Calif. Code of Regs., Sec. 1707.6
24. Mosquera, M. Mobile Pharmacies To Help In Emergencies. Federal Computer Week. March 19, 2008.
25. Calif. Bus. and Prof. Code, Sec. 4062(c)
26. Ibid. at Sec. 4110
27. Ibid. at Secs. 4127 and 4127.1(a)(b)
28. Title 16, Calif. Code of Regs., Secs. 1751 thru 1751.8
29. Calif. Bus. & Prof. Code, Sec. 4127(d)
30. Title 16, Calif. Code of Regs., Sect 1751(a)
31. Title 16, Calif. Code of Regs., Sec. 1735.2(d)
32. Ibid. at Sec. 1735.2(e)
33. Ibid. at Sec. 1735.2(j)
34. Ibid. at Sec. 1735.3(a)(d)
35. Ibid. at Sec. 1735.5(a)(b)
36. Ibid. at Sec. 1735,7(a)(b)
37. Ibid. at Sec. 1735.8(a)(b)(c)(d)
38. Calif. Health & Safety Codes, Sec. 11055
39. A major portion of the wording contained in the two tables for both Calif. Assembly and Senate Bills was primarily the result of it being available from the CSHP website, under the section entitled, “Advocacy News,” and from the bills themselves.
References
10 cjhp: California Journal of Health-System Pharmacy September/October 2011

IntroductionThe use of highly active antiretroviral therapy (HAART) has dra-matically improved morbidity and mortality in patients infected with human immunodeficiency virus (HIV)1,2. Since there remains no cure, treatment aims for maximal suppression of viral load.3,4 It is widely believed patient adherence to prescribed HAART regimens is central to achieving this goal.5 While consumption of at least 80% of prescribed doses is considered an acceptable level of adherence for most drugs, previous studies indicate that for HIV-infected patients, adherence of 95% or greater is significantly associated with superior virologic outcome as compared to lower adherence rates.6
Maximal viral suppression also requires initiation and con-tinuation of guideline-appropriate antiretroviral (ARV) medication regimens.7 The continuation of appropriate regimens are often inter-rupted upon transfer of care, which may result in drug toxicities, treatment failure, and viral resistance.8-13 In the hospital setting, medication errors are generally common11 but are especially costly to HIV-infected patients who depend on high adherence rates for treatment success. The need to continue a patient’s current medi-cations upon admission to the hospital is highlighted by the Joint Commission’s National Patient Safety Goal 8, which is to accurately and completely reconcile medications across the continuum of care.14 However, previous studies have shown increasing com-plexity in ARV medications and poor prescriber knowledge place HIV-positive patients at risk for inpatient prescribing errors upon hospital admission.8-9,12-13,15 In these studies, the most common errors in ARV prescribing were incorrect dosage or frequency and incomplete regimens per established guidelines. Another study found most ARV errors occur at the time of admission to the hospital, and are most often due to inadvertent omission.16
At our institution, a retrospective review of ARV order-entry at the time of admission was conducted in order to determine the ARV error rate, frequency of guideline-inappropriate regimens pre-scribed, and factors associated with ARV errors.
MethodsPopulationThe University of California, San Francisco (UCSF) Medical Center is a tertiary care, 610-bed teaching hospital in San Francisco, California. All patient visits were included in the analysis if the patient was HIV-positive, 18 years of age and older, admitted to UCSF Medical Center during a 12 month period, and had at least one ARV entered in the UCSF order-entry program (WORx, Mediware Information Systems, Lenexa, KS). Patients were excluded if they were less than 18 years old, used ARVs for indications other than HIV infection (i.e., post-exposure prophylaxis, hepatitis B infection, vertical transmission prophylaxis), or had ARVs entered in their medication profiles erroneously. This study was granted approval by the Committee on Human Research, UCSF’s Institutional Review Board.
Data CollectionDemographic information was collected from the electronic medical record (UCARE), which included admission and discharge dates, admit-ting service, age, weight, height, gender. Laboratory test data obtained upon admission included international normalizing ratio (INR) and serum creatinine. Ideal body weight and estimated creatinine clearance (using the Cockcroft-Gault formula) were calculated if the necessary parameters were available (serum creatinine, height, weight, age). ARV orders in WORx were evaluated for time of entry and discontinuation, dose, route, and frequency.
Each patient’s WORx profile was evaluated for each visit that occurred during the 12-month study period for ARV errors and HAART regimen appropriateness according to the 2006 Guidelines for the Use of Antiretrovirals Agents in HIV-1-Infected Adults and Adolescents (Department of Health and Human Services - DHHS).3 Errors in ARV prescribing associated with delayed timing were defined as any dis-pensing of an ARV that took place 24 hours after the initial ARV was prescribed. The types of errors searched for is listed in Table 1.
inpatient antiretroviral Prescribing for HiV- positive Patients: analysis of error rate and associated factors
Christie A. Robinson Health Sciences Assistant Clinical Professor University of California San Francisco
Grace C. Lin, PharmD General Medicine Clinical Pharmacist University of California San Francisco Medical Center
Julie Shih, PharmD Pediatric Clinical Pharmacist San Francisco General Hospital Medical Center
• • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • Clinical Pearls
Helen Wang, PharmD Ambulatory Care Pharmacist Kaiser Permanente Specialty Pharmacy
Conan MacDougall, PharmD, MAS, BCPS Associate Professor of Clinical Pharmacy University of California San Francisco
September/October 2011 cjhp: California Journal of Health-System Pharmacy 11

Pearls: Inpatient Antiretroviral Prescribing
Data AnalysisA retrospective electronic medical record review and electronic medication-order entry system review were performed. Data was entered into an Excel spreadsheet (Microsoft Corp., Redmond, WA) and analyzed with Stata SE (Stata Corp, College Station, TX). The primary outcomes of interest were the rate of prescribing errors in ARVs ordered upon admission and whether the initial regimen was guideline-appro-priate. Unadjusted comparison of error likelihoods according to patient demographics was performed using Chi-square analysis. Multivariable logistic regression analysis of drug level errors was performed incorpo-rating presence of a pharmacist on service, performance of medication reconciliation upon admission, gender, age, and renal function.
ResultsA total of 558 hospital admissions were identified as having been prescribed at least one ARV medication during the 12-month study period and 377 of those admissions had ARVs prescribed for the treatment of an HIV infection (Figure 1). The mean age of the patients was 49 years with a standard deviation of 9.6 years. The study included 211 males (83.3%). Most patients were admitted into the Medicine service (35.8% of visits), followed by Kidney Transplant (8.5%), Vascular Surgery (7.7%), and General Surgery and Cardiology (6.9% each). Seventy-eight percent of patients were in services with clinical pharmacists.
A total of 1,159 ARV medications were ordered throughout the study period, with 3.07 ARVs per admission. The most commonly used regimens were standard regimens; a single protease inhibitor (PI) and two nucleoside reverse transcriptase inhibitors (NRTIs) was seen in 136 (36.1%) admissions, and a single non-nucleoside reverse tran-scriptase inhibitor (NNRTI) and two NRTIs was seen in 100 (26.5%)
admissions. Nonstandard and salvage regimens ordered include two or more PIs (14 patients), a PI and an NNRTI (24 patients), and three or four PIs (73 patients).
A total of 177 (15.3%) dosing errors were detected from the 1,159 ARV medications ordered in total, with the most seen in PIs (18.3% of PIs; p=0.07 for likelihood of dosing error across the drug classes). Adjusting for admissions, dosing errors were seen in 129 (34.2%) admissions with one error in 90 admissions, two errors in 30 admis-sions, and three errors in nine admissions. On univariate analysis, dosing errors were more common among the >65 year old age group (18/30 drugs, 60%), compared to the 45-65 group (75/235, 32%) and the <45 year old age group (36/112, 32%, p<0.001 for comparison between groups).
A subgroup analysis, including 350 admissions with complete information allowing for the calculation of creatinine clearance (CrCl), was completed to determine the percentage of dosing errors in patients with normal renal function (CrCl > 50 ml/min), intermediate renal dysfunction (CrCl 20-50 ml/min), and severe renal dysfunction (CrCl <20 ml/min) (Table 2). Within this subgroup, the intermediate and severe renal dysfunction groups had significantly higher ARV dosing errors compared to patients in the normal renal function group (70.6%, 56.1%, 23.3%, respectively; p < 0.001). The likelihood of an error was not significantly different between services normally assigned a clinical pharmacist and those where a clinical pharmacist was not normally present (33.3% vs 37.4%, p=0.49). Among patients where records indi-cated that medication reconciliation had been performed, an error was noted in 71/230 (30.9%) compared to 58/147 (39.5%) cases without performance of medication reconciliation (p=0.09)
A multivariable regression model of dosing errors (Table 3) incorporating patient age, presence of a pharmacist on service, per-
Figure 1. Study Inclusion Criteria Flowchart
12 cjhp: California Journal of Health-System Pharmacy September/October 2011
Pearls: Inpatient Antiretroviral Prescribing
formance of medication reconciliation, and renal function found that compared to patients with an estimated creatinine clearance (CrCl) of >50 mL/min, patients with intermediate renal impairment (estimated CrCl 20-50 mL/min) had 8.0 times the odds of a dosing error (95% confidence interval 3.8 – 16.5) and those with severe renal impair-ment (CrCl <20 ml/min) had 4.3 times the odds (95% confidence interval 2.1 – 8.6). Other factors were not associated with likelihood of a dosing error after adjustment.
Guideline-inappropriate regimens were found in 15.9% of all admissions. They were found in 14.6% in services with a pharmacist versus 20.5% in services without a pharmacist (p = 0.19). Medication reconciliation, a process of comparing patients’ home medications with those ordered while under the care of an institution,1 was performed for 61.0% of all admissions. Guideline-inappropriate regimens were associated with 13.0% of admissions with medication reconciliation versus 20.4% of admissions without medication reconciliation (p = 0.06). On adjusted analysis incorporating patient age, presence of a pharmacist on service, and performance of medication reconciliation, the odds of a guideline-inappropriate regimen were 1.6 times higher (95% confidence interval when a medication reconciliation was not performed (p = 0.09).
Discussion The development of new ARV agents and the increasing complex-ity of HAART regimens leads to the potential for more prescribing errors.8-9,12-13,15 In addition, medication discrepancies and interruption in appropriate therapy have been shown to be common at the time of hospital admission.16 This was also found to be the case at the UCSF Medical Center. In this study, there was at least one ARV dosing error in 34.2% of the admissions, and a guideline-inappropriate regimen in
15.9% of the admissions. These results are helpful in estimating the incidence of initial ARV prescribing errors for the UCSF Medical Center because previous studies have shown that anywhere from 5.8% to 86% of HIV-positive hospitalized patients experience at least one ARV drug-related error.8,9,12,13
In general, studies looking at ARV-related errors in hospitalized patients identify the most common errors as incorrect dosage amount or frequency, drug-drug interactions between an ARV and another medication, and incomplete ARV regimens.8,9,12,13 While this study did not identify the specific types of errors that occurred, the multivariable model of drug-level errors did show a difference in drug error rate in patients with varying levels of renal function (Table 3).
Interestingly, most ARV drug errors occurred in patients with inter-mediate renal function. One explanation could be that patients who had intermediate renal function were undergoing acute renal failure upon admission, and dosages were based on their prior renal function. In addition, patients with severe renal dysfunction may have had better documentation of their renal failure, leading to heightened awareness of the need for renal dose-adjustment. Even so, patients with severe renal dysfunction were still more likely than those with normal renal function to have ARV dosing errors.
The failure to dose-adjust for renal insufficiency is well documented. One study found that 45% of patients with chronic kidney disease (CKD) stages 3 to 5 received higher than recommended medication doses based on their estimated creatinine clearance.17 Another study found that the doses for patients with CKD were on average 2.5 times
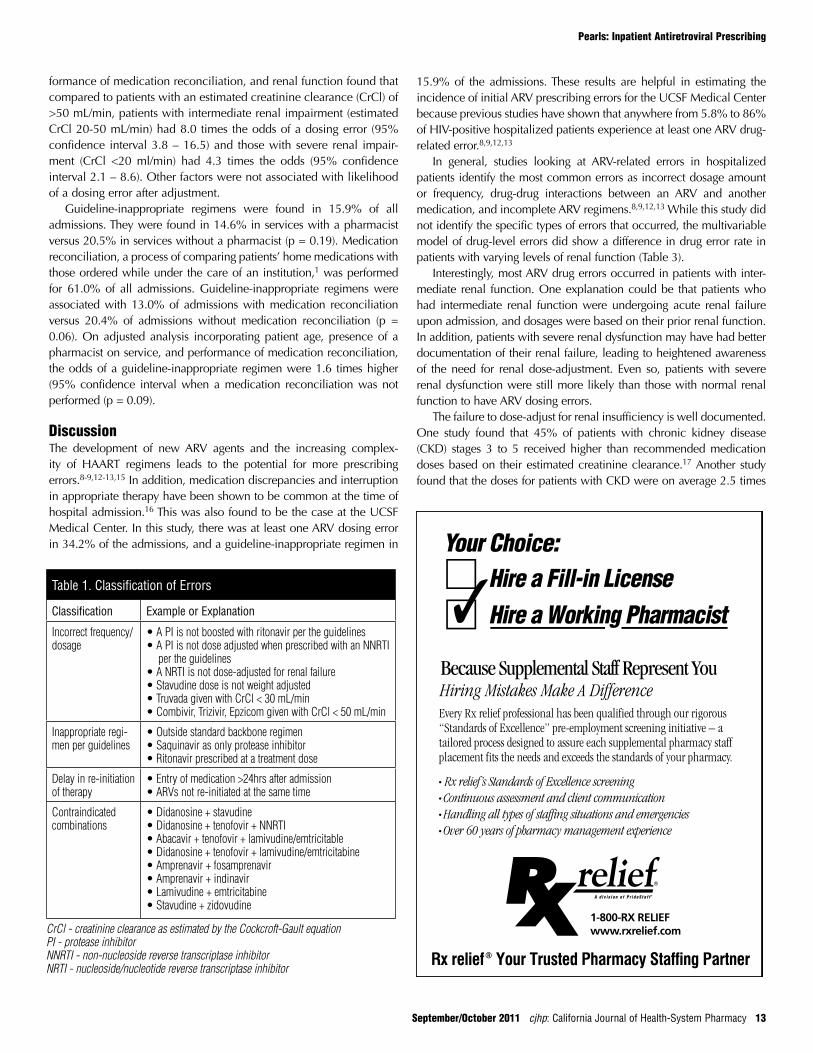
Table 1. Classification of Errors
Classification Example or Explanation
Incorrect frequency/dosage
• A PI is not boosted with ritonavir per the guidelines• A PI is not dose adjusted when prescribed with an NNRTI
per the guidelines• A NRTI is not dose-adjusted for renal failure• Stavudine dose is not weight adjusted• Truvada given with CrCl < 30 mL/min• Combivir, Trizivir, Epzicom given with CrCl < 50 mL/min
Inappropriate regi-men per guidelines
• Outside standard backbone regimen• Saquinavir as only protease inhibitor• Ritonavir prescribed at a treatment dose
Delay in re-initiation of therapy
• Entry of medication >24hrs after admission• ARVs not re-initiated at the same time
Contraindicated combinations
• Didanosine + stavudine• Didanosine + tenofovir + NNRTI• Abacavir + tenofovir + lamivudine/emtricitable• Didanosine + tenofovir + lamivudine/emtricitabine• Amprenavir + fosamprenavir• Amprenavir + indinavir• Lamivudine + emtricitabine• Stavudine + zidovudine
CrCl - creatinine clearance as estimated by the Cockcroft-Gault equationPI - protease inhibitorNNRTI - non-nucleoside reverse transcriptase inhibitorNRTI - nucleoside/nucleotide reverse transcriptase inhibitor
September/October 2011 cjhp: California Journal of Health-System Pharmacy 13
higher than the maximum recommended doses based on their glo-merular filtration rate.18 In this study, the patient population receiving ARVs was no exception.
Inpatient ARV dosing errors have major consequences. In all of the aforementioned studies, the most common dosing error was failure to adjust dosages based on renal function.8,9,12,13 Failure to dose-adjust for renal insufficiency increases the risk of toxicity and adverse effects, which may lead to decreased compliance.7,19 Decreased compliance often results in treatment resistance, increased viral load, and decreased CD4 cell counts, which in turn increases the risk for opportunistic infec-tions.7,19 Delays in therapy or an incomplete regimen may also induce treatment resistance, since patients need to be on an optimized regimen for adequate viral suppression, as specified by the DHHS Antiretroviral Guidelines.3 Furthermore, drug interruptions have been shown to increase the risks of cardiovascular, hepatic, and renal complications.19
Given the number of errors seen at the UCSF Medical Center, it is important that strategies are developed to minimize inappropriate prescribing of ARVs. One possibility is to develop an ARV dosing form, similar to the antibiotic dosing form currently in use at the Medical Center. An infectious diseases pharmacist reviews the antibiotic dos-ing form for correctness prior to being processed by the pharmacy. A specialized HIV pharmacist could similarly review the ARV dosing form to reduce ARV prescribing errors. Furthermore, the dosing form could mandate the calculation of the patient’s creatinine clearance in order to encourage proper dose adjustment for renal insufficiency.
Pearls: Inpatient Antiretroviral Prescribing
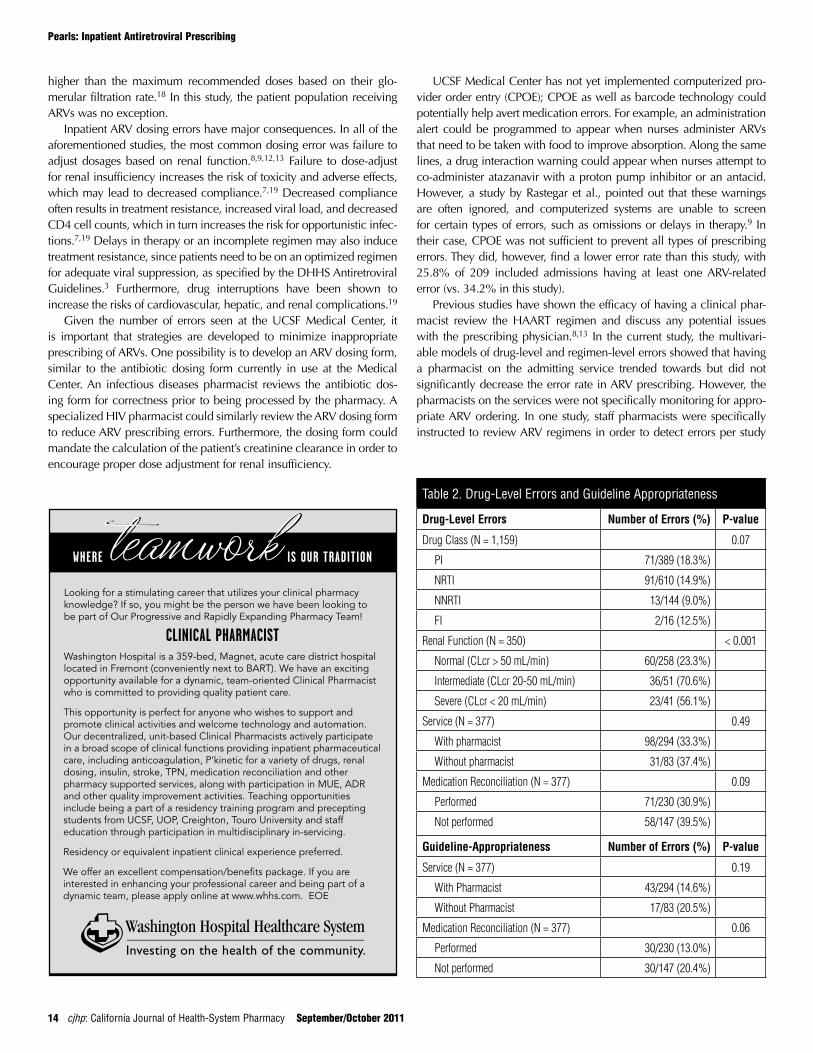
Table 2. Drug-Level Errors and Guideline Appropriateness
Drug-level Errors Number of Errors (%) P-value
Drug Class (N = 1,159) 0.07
PI 71/389 (18.3%)
NRTI 91/610 (14.9%)
NNRTI 13/144 (9.0%)
FI 2/16 (12.5%)
Renal Function (N = 350) < 0.001
Normal (CLcr > 50 mL/min) 60/258 (23.3%)
Intermediate (CLcr 20-50 mL/min) 36/51 (70.6%)
Severe (CLcr < 20 mL/min) 23/41 (56.1%)
Service (N = 377) 0.49
With pharmacist 98/294 (33.3%)
Without pharmacist 31/83 (37.4%)
Medication Reconciliation (N = 377) 0.09
Performed 71/230 (30.9%)
Not performed 58/147 (39.5%)
Guideline-Appropriateness Number of Errors (%) P-value
Service (N = 377) 0.19
With Pharmacist 43/294 (14.6%)
Without Pharmacist 17/83 (20.5%)
Medication Reconciliation (N = 377) 0.06
Performed 30/230 (13.0%)
Not performed 30/147 (20.4%)
UCSF Medical Center has not yet implemented computerized pro-vider order entry (CPOE); CPOE as well as barcode technology could potentially help avert medication errors. For example, an administration alert could be programmed to appear when nurses administer ARVs that need to be taken with food to improve absorption. Along the same lines, a drug interaction warning could appear when nurses attempt to co-administer atazanavir with a proton pump inhibitor or an antacid. However, a study by Rastegar et al., pointed out that these warnings are often ignored, and computerized systems are unable to screen for certain types of errors, such as omissions or delays in therapy.9 In their case, CPOE was not sufficient to prevent all types of prescribing errors. They did, however, find a lower error rate than this study, with 25.8% of 209 included admissions having at least one ARV-related error (vs. 34.2% in this study).
Previous studies have shown the efficacy of having a clinical phar-macist review the HAART regimen and discuss any potential issues with the prescribing physician.8,13 In the current study, the multivari-able models of drug-level and regimen-level errors showed that having a pharmacist on the admitting service trended towards but did not significantly decrease the error rate in ARV prescribing. However, the pharmacists on the services were not specifically monitoring for appro-priate ARV ordering. In one study, staff pharmacists were specifically instructed to review ARV regimens in order to detect errors per study
IS OUR TRADITIONWHERE teamworkteamworkLooking for a stimulating career that utilizes your clinical pharmacy knowledge? If so, you might be the person we have been looking to be part of Our Progressive and Rapidly Expanding Pharmacy Team!
CLINICAL PHARMACISTWashington Hospital is a 359-bed, Magnet, acute care district hospital located in Fremont (conveniently next to BART). We have an exciting opportunity available for a dynamic, team-oriented Clinical Pharmacist who is committed to providing quality patient care.
This opportunity is perfect for anyone who wishes to support and promote clinical activities and welcome technology and automation. Our decentralized, unit-based Clinical Pharmacists actively participate in a broad scope of clinical functions providing inpatient pharmaceutical care, including anticoagulation, P’kinetic for a variety of drugs, renal dosing, insulin, stroke, TPN, medication reconciliation and other pharmacy supported services, along with participation in MUE, ADR and other quality improvement activities. Teaching opportunities include being a part of a residency training program and precepting students from UCSF, UOP, Creighton, Touro University and staff education through participation in multidisciplinary in-servicing.
Residency or equivalent inpatient clinical experience preferred.
We offer an excellent compensation/benefits package. If you are interested in enhancing your professional career and being part of a dynamic team, please apply online at www.whhs.com. EOE
14 cjhp: California Journal of Health-System Pharmacy September/October 2011

Pearls: Inpatient Antiretroviral Prescribing
Requests for Information:Christie A. RobinsonHealth Sciences Assistant Clinical ProfessorUniversity of California San Francisco, School of Pharmacy, Department of Clinical Pharmacy San Francisco, CA 94143(415) 476-1339 (work) (415) 476-6632 (fax)[email protected]
protocol.8 They were able to detect and prevent 108 significant ARV medication prescribing errors involving 86 patients during a 34-month study period. Another study evaluated the median length of time until an error was corrected, comparing periods when a clinical pharmacist was monitoring patients receiving HAART to periods without pharma-cist monitoring.13 They found that 21% of the HIV-infected patients receiving ARVs during the study period had at least one error in their HAART regimen. When a clinical pharmacist intervened, the median time to correction of the errors was reduced from 84 hours to 15.5 hours. Specialized HIV pharmacists may be even more efficient at detecting and preventing ARV-related errors.
The multivariable models done in this study found that having a medication reconciliation performed by a pharmacist upon admission did not significantly reduce the risk of having an ARV error at the indi-vidual drug level, although there was a trend towards decreased errors. It seemed as if patients were also more likely to have a guideline-appro-priate regimen if a pharmacist performed a medication reconciliation. Although not statistically significant either, this suggests a benefit in performing a medication reconciliation on admission to reduce guide-line-inappropriate ARV regimens. Medication reconciliations could increase the continuity of care between outpatient and inpatient set-tings if they are performed in a timely manner, and is one of the Joint Commissions’ National Patient Safety Goals.14
This study had several limitations. First, this study focused on the frequency of errors rather than characterization of the specific types of ARV prescription errors. Second, the prescribing of medications other than ARVs was not taken into consideration, so any drug-drug interactions or contraindicated drug combinations were not detected. Therefore, it is likely that this study underestimated the number of ARV-related errors that occurred during the study period. Third, since the study population was based on whether or not the patients were prescribed ARVs, patients who should have been on a HAART regimen but had their HAART regimen omitted completely upon admission
were not detected. Fourth, the cause of renal insufficiency in patients was not evaluated. Hence, it is uncertain why a larger percentage of patients with intermediate renal function experienced dosing errors compared to patients with severe renal impairment. Sixth, the clinical impact of the ARV dosing errors on the patients, such as subsequent adverse effects or sequelae, was not studied. This study was retrospec-tive and only looked at the frequency with which ARV-related errors occurred; it was not designed to evaluate strategies which could poten-tially decrease the rate of errors. Further studies are needed to review the efficacy of interventions such as an ARV dosing form or the clinical impact of an HIV-specialized pharmacist.
ConclusionIt has been shown in prior studies that dosing errors and guideline inappropriate regimens are commonly found in ARV regimens when patients are first admitted into the hospital. This was also true at the UCSF Medical Center. Most dosing errors occurred as a result of failing to adjust ARV medications for renal function. Although not statistically significant, pharmacists and medication reconciliation showed some benefits in reducing dosing errors and guideline inap-propriate regimens.u
1. Palella FJ Jr, Delaney KM, Moorman AC et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med 1998; 338: 853-860.
2. Hogg RS, Yip B, Kully C, et al. Improved survival among HIV-infected patients after initiation of triple-drug antiretro-viral regimens. CMAJ 1999; 160: 659-665.
3. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. November 3, 2008; 1-139. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed 3/29/09.
4. Wood E, Yip B, Hogg RS, et al. Full suppression of viral load is needed to achieve an optimal CD4 cell count response among patients on triple drug antiretroviral therapy. AIDS 2000; 14: 1955-1960.
5. Montaner JS, Hogg R, Raboud J, et al. Antiretroviral treatment in 1998. Lancet 1998; 352: 1919-1922.
6. Paterson DL, Swindells S, Mohr J, et al. Adherence to Protease Inhibitor Therapy and Outcomes in Patients with HIV Infection. Ann Intern Med 2000; 133:21-30.
7. Wainberg MA, Friedland G. Public health implications of antiretroviral therapy and HIV drug resistance. JAMA 1998; 129 (12 Pt 2): 1079-1100.
8. Purdy BD, Raymond AM, Lesar TS. Antiretroviral Prescribing Errors in Hospitalized Patients. Ann Pharmacother 2000. 34: 833-838.
9. Rastegar DA, Knight AM, Monolakis JS. Antiretroviral medication errors among hospitalized patients with HIV infec-tion. CID 2006. 43: 933-938.
10. Harrigan PR, Hogg RS, Dong WWY, et al.: Predictors of HIV drug resistance mutations in a large antiretroviral-naïve cohort initiating triple antiretroviral therapy. The Journal of Infectious Diseases 2005, 191:339-47.
11. Committee on Identifying and Preventing Medication Errors: Institute of Medicine Report 1996.
12. Mok S, Minson Q. Drug-related problems in hospitalized patients with HIV infection. Am J Health Syst Pharm 2008; 65: 55-59.
13. Heelon M, Skiest D, Tereso G, Meade L, Weeks J, Pekow P, et al. Effect of a clinical pharmacist’s interventions on duration and antiretroviral-related errors in hospitalized patients. Am J Health Syst Pharm 2007; 64:2064-68.
14. The Joint Commission on Accreditation of Healthcare Organizations. Accreditation Program: Hospital National Patient Safety Goals. Available at http://www.jointcommission.org/hap_2011_npsgs/. Accessed 1/8/11.
15. Arshad S, Rothberg M, Rastegar DA, et al. Survey of physician knowledge regarding antiretroviral medications in hospitalized HIV-infected patients. Journal of the International AIDS Society 2009; 12:1.
16. Cornish PL, Knowles SR, Marchesano R, et al.: Unintended medication discrepancies at the time of hospital admis-sion. Arch Intern Med 2005; 165:424-429.
17. Cantu TG, Ellerbeck EF, Yun SW, et al. Drug prescribing for patients with changing renal function. Am J Hosp Pharm 1992;49:2944-8.
18. Gabardi S, Abramson S. Drug dosing in chronic kidney disease. Med Clin N Am 2005;89:649-87.
19. Hammer SM, Eron JJ, Reiss P, et al. Antiretroviral Treatment of Adult HIV Infection: 2008 Recommendations of the International AIDS Society – USA Panel. JAMA 2008;300(5):555-70.
References
September/October 2011 cjhp: California Journal of Health-System Pharmacy 15

Proposals to be Considered by the California Society of Health-System Pharmacists House of DelegatesNovember 3 & 6, 2011
DISCLAIMER:All proposals have been fully developed and submitted by the CSHP Board of Directors for distribution to CSHP members. The proposals are correct as of October 1, 2011. Please go to the “About” section of the CSHP website (cshp.org) and select “House of Delegates” under “Resources” for the most up-to-date, accurate information concerning any and all proposals to the 2011 CSHP House of Delegates.
Note: The Open Forum provides an opportunity for discussion of all pro-posals. The BOD strongly recommends attendance by one (1) delegate from each chapter at the Open Forum, 3:30–5:30 PM on Friday, November 4, 2011.
PROPOSAL A
PROPOSAL: To Modify CSHP Bylaws for Executive Committee of the
Technician Division to include Technician Director
SUBMITTED BY: Maria Serpa, President
DATE: June 2, 2011
SITUATION: 1. CSHP Bylaws currently state there are 2 pharmacists members on the
Executive Committee of the Technician Division. One of which is the Board Liaison.
2. There is no mention of the Technician Director as a member of the Executive Committee of the Technician Division.
TARGET:Technician Director to be a member of the Executive Committee of the Technician Division and liaison to the Board of Directors.
PROPOSAL: 1. Bylaws changes as below
ARTICLE VI
DIRECTORS
SECTION 1. POWERS (b) (ix) Directors shall serve as members of the Board of Directors of the Society. A Director shall be appointed by the President as a liaison to Councils, Committees, and/or Task Forces as described in Article IX, Section 3 (d) of these Bylaws. A Director shall also be appointed by the President as a liaison to each Regional Chapter. The Technician Director shall also be appointed to serve as a liaison to the Executive Committee of the Technician Division.
ARTICLE XIV TECHNICIAN DIVISION
SECTION 1. MEMBERSHIP The membership of the Technician Division (hereafter referred to as “the Division”) shall consist of all technician members of the California Society of Health-System Pharmacists.
SECTION 2. RESPONSIBILITIES The responsibilities of the Division shall be to: (a) Plan and implement continuing education programs for technicians. (b) Expand and maintain membership recruitment services for technicians. (c) Provide guidance, and make proposals to the Board of Directors on
policy issues involving technicians. (d) Develop guidelines and practice standards for pharmacy technicians. (e) Promote and foster the standards and objectives of the Society. (f) Participate in activities for the advancement of the profession of phar-
macy. (g) Report, consolidate and delineate problems, issues and programs of
general importance to the profession of pharmacy and pharmacy tech-
nicians through its representation of the House of Delegates.
SECTION 3. RESTRICTIONS (a) The Division shall not make political contributions of any kind to fed-
eral, state or local candidates or campaigns. (b) The Division may have the privilege of using the insignia of the Society
in accordance with guidelines established by the Board of Directors.
(c) Acts of the Division shall in no way commit or bind the Society.
SECTION 4. OPERATIONAL STRUCTURE (a) Officers.
(i) The Officers of the Division shall be members of the Division. (ii) The elected Officers of the Division shall be a Chairperson, a
Chairperson-Elect, an Immediate Past Chairperson, and a Secretary. The Chairperson-Elect shall be elected annually and shall ascend successively to the offices of Chairperson and Immediate Past Chairperson, serving one (1) year in each of these positions. The Secretary shall be elected every two (2) years.
(iii) Duties of the Officers. (A) Chairperson: The Chairperson shall be the principal elected offi-
cial of the Division. With approval of the Executive Committee, the Chairperson shall appoint committees as needed; shall be a member of the Division’s Executive Committee and shall serve as its Chairperson; shall serve as one of the technician delegates; and shall report at least annually on the Division activities to the Board of Directors.
16 cjhp: California Journal of Health-System Pharmacy September/October 2011

(B) Chairperson-Elect: The Chairperson-Elect shall be a member of the Division Executive Committee and shall perform the duties of the office of Chairperson whenever the Chairperson is unable to do so.
(C) Immediate Past Chairperson: The Immediate Past Chairperson shall be a member of the Division Executive Committee and shall serve as Chairperson of the Executive Committee in the absence of both the Chairperson and the Chairperson-Elect.
(D) Secretary: The Secretary shall be a member of the Division Executive Committee; and shall serve as Secretary of the Executive Committee.
(b) Executive Committee. There shall be an Executive Committee of the Division consisting of the officers, one technician member at-large, and onetwo active pharmacist- member-at-large,s as appointed by the President, and the Technician Director, who. One of the pharmacist members must also be on the Board of Directors and shall serve as liaison to the Board of Directors.
The pharmacist member at-largeExecutive Committee members and Technician Director shall be voting members of the Committee.
(c) Elections. A Committee on Nominations, appointed by the Chairperson, shall select two (2) candidates for Chairperson-Elect and two (2) candi-dates for each Delegate position other than the Chairperson each year. The Committee shall select two (2) candidates for Secretary every two (2) years and two (2) candidates for the at-large technician member of the Executive Committee on alternating two years. The at-large techni-cian member would be elected for a one year term in 1990 and then for two year terms beginning in 1991.
The Chairperson-Elect and Delegates shall be elected by the Division members. The ballots shall be mailed to all Division members in con-junction with established election procedures for other Society Officers and Directors.The results of the election shall be certified by the Secretary of the Society.
Persons nominated as delegates but not elected will serve as alternate delegates.
(d) Vacancies. If the office of an elected member of the Division Executive Committee becomes vacant, the Executive Committee shall fill such vacancy until such time as a duly elected replacement is installed. During its next annual nomination cycle, the Committee on Nominations of the Division shall present candidates for election to serve the remaining portion of the unexpired term.
(e) Meetings. The Division Executive Committee shall meet at least four (4)
times per year.
SECTION 5. AUTHORITY (a) The Division may not adopt, publicize, promote or otherwise convey
any policy or principle in the name of the Society which has not been approved by the Board of Directors.
(b) The Division may pursue any activity that is authorized by the Society. (c) The Board of Directors shall have authority to assign a specific matter to
the Division for its consideration. (d) Any matter presented for consideration directly to the Board of Directors
may, prior to action by the Board of Directors, be referred for consid-eration and recommendation to the Division. In the event the Board of Directors does not act favorably upon a recommendation received
from the Division, the matter shall be returned with explanation to the Division for its further consideration.
(e) The Board of Directors shall approve an annual Division budget and have authority to establish guidelines for the expenditure of Division funds.
(f) The Board of Directors shall have final authority over the proposals of the Division and the determination of which proposals require approval by the House of Delegates.
(g) The Division shall not secure nor attempt to secure funds independently from sources outside the Society without prior approval from the Board of Directors.
(h) The Division shall not independently contact other organizations unless authorized by the Board of Directors or the President.
(i) If a matter is presented to the Division, in a called meeting, merely for the information of the Division, only acknowledgment of the informa-tion in the form of informal statements or suggestions shall be required
in the records of the meeting.
RESOURCES REQUIRED FOR PROPOSED ACTION(S) Financial: none EVP time: 0 hours Staff time: 5 hours (to take to HOD and add to elections; update
bylaws document)
CSHP BOARD ACTION:At its July 8-9, 2011 meeting, the board approved the proposal.
PROPOSAL B
PROPOSAL: To Modify CSHP Bylaws for New Practitioner Executive Committee
SUBMITTED BY: 2011 NPEC, Elaine Law, Chair Maria Serpa, Board Liaison
DATE: June 8, 2011
SITUATION: 1. New Practitioner Executive Committee (NPEC) was established by the
CSHP BOD in October 2010 and the 1st year was tasked to develop governance, policies, and goals. Administrative Policy A20154.
2. The chair of NPEC is represented on the CSHP BOD as a non-voting member per current policy.
3. Current policy states that a Vice-Chair is appointed in case of geo-graphic or employment changes of the Chair.
4. CSHP currently has 2 Student Section Executive Committee co-chairs, with one (1) co-chair attending BOD meetings as a voting member.
5. ASHP currently has a New Practitioner Forum and Student Forum. A delegate from each forum sits in the ASHP House of Delegates but they do not sit on the ASHP Board of Directors.
6. CPhA has a student member from each school as voting members on the CPhA Board of Trustees. There is no formal subgroup of new practi-tioners.
TARGET: 1. Invest in New Practitioners and provide them with a voice in the gover-
nance of CSHP. 2. Increase and retain membership by getting new practitioners involved
and helping them transition.
September/October 2011 cjhp: California Journal of Health-System Pharmacy 17

Proposals to the 2011 CSHP House of Delegates
3. Generate increased interest from new practitioners regarding gover-nance and development of leadership in the pharmacy profession.
4. Provide clarification of the number of NPEC meetings per previous STP which asks for an additional face-to-face meeting.
5. Remove the need for Vice-Chair as geographic or employment location is not relevant to the appointment of NPEC Chair and would not affect the status of Chair.
6. Correct for current bylaws errors and/or omissions in number and type of current Board of Director members.
7. Update CSHP bylaws to provide governance documentation of NPEC..8. Update CSHP bylaws to add voting privileges to NPEC Chair representa-
tion on the CSHP Board of Directors.
PROPOSAL:1. Bylaws addition as below to add New Practitioner Executive Committee
(see below)2. Bylaws corrections to include and correct references to total number
of directors on the Board (e.g. corrections for Technician director and co-chair SSEC board member). This is not changed as a part of this STP
but correcting previous errors or omissions.
RESOURCES REQUIRED FOR PROPOSED ACTION(S) Financial: No additional costs (NPEC expenses in previous STPs) EVP time: 5 hours Staff time: 20 hours
PROPOSED Bylaws CHANGES
ARTICLE VI DIRECTORS
SECTION 2. NUMBER AND QUALIFICATIONS OF DIRECTORSThe authorized number of Directors of the corporation shall be sev-
enteen (17) fifteen (15) until changed by amendment of these Bylaws. The Board of Directors shall consist of the President, the Immediate Past President, the President-Elect, the Treasurer, the Chairperson of the House of Delegates, the Executive Vice President (Secretary), Chairperson of New Practitioner Executive Committee, one (1) co-chairperson of Student Section Executive Committee and nine (9) eight (8) elected Directors. Directors must be Active Members of the Society. No Director elected by the general mem-bership shall be eligible to serve more than two (2) consecutive terms in the same elected office, except as provided for the Chairperson of the House of Delegates in Article VI, Section 3 (d). No Director shall be entitled to hold more than one elected position on the Board of Directors at any one time.
SECTION 3. ELECTION, DESIGNATION AND TERM OF OFFICE(a) Elected Directors. There shall be a total of nine (9) elected Directors
(including the Technician Director) who shall serve staggered three (3) year terms or until their respective successors are elected and take office. Two (2) Directors shall be elected for installation at the next annual meeting of the Society each calendar year commencing with the 1990 annual meeting and every third calendar year thereafter. Three (3) Directors shall be elected for installation at the annual meeting every in all other calendar years. with the technician director being elected as one (1) of the three (3) Directors commencing with the 2011 annual
meeting and every third calendar year thereafter. Nominations and vot-ing for elected Directors shall be conducted consistent with Sections 4 and 5 of this Article VI of these Bylaws.
(b) Technician Director. There shall be a total of one (1) Technician Director who shall serve a three (3) year term until his/her respective successor is elected and takes office. The Technician Director shall be elected from the general membership of the Technician Division.
(c) Chairperson of New Practitioner Executive Committee. There shall be a total of one (1) Chairperson of New Practitioner Executive Committee, who shall serve a two (2) year term until his/her respective successor is elected and takes office. The Chairperson of New Practitioner Executive Committee, shall be elected from the active members of CSHP and be qualified as a New Practitioner for the duration of their term.
(d) Co-chairpersons of Student Section Executive Committee. There shall be a total of two (2) co-chairpersons who shall be appointed by the President from the Student Section Executive Committee and serve a term of one (1) year. Only one (1) co-chairperson can vote during board
meetings.
ARTICLE XIII (New Article XIII and renumbering of subséquent articles)
Article XIII - NEW PRACTITIONER EXECUTIVE COMMITTEE
SECTION 1. MEMBERSHIP(a) The President-elect shall annually appoint 7 (seven) active members
qualifying as new practitioners to the New Practitioner Executive Committee. They shall represent the diverse practice settings and geog-raphy of CSHP membership.
(b) A chairperson will be elected from the active members of CSHP. The term of office for Chairperson will be for two years and shall not exceed one term.
SECTION 2. RESPONSIBILITIES(a) Promote and foster the mission, vision and standards of the California
Society of Health-System Pharmacists.(b) Represent and provide for the membership needs of new practitioner.(c) Provide guidance and make proposals to the Board of Directors on
policy issues.
SECTION 3. AUTHORITY(a) The Chairperson shall represent the interests of the New Practitioner
Executive Committee and CSHP New Practitioners as a voting member of the Board of Directors
ARTICLE XVIII AMENDMENT TO BYLAWS
SECTION 2. APPROVAL BY MEMBERSHIPThe provisions of Section 1 of this Article XVIII notwithstanding, no vote
to amend any provision of Articles I, II, III, IV, XVII or XIXVIII, Sections 1 or 2 of Article VIII, or Sections 1 or 3 of Article XX IX shall become effective unless approved by a majority of the voting members of the Society by mail ballot in the same manner as election of officers and Directors as provided in these Bylaws.
CSHP BOD ACTION:At its August 31, 2011 meeting the board approved the proposal.
18 cjhp: California Journal of Health-System Pharmacy September/October 2011

Proposals to the 2011 CSHP House of Delegates
PROPOSAL C
PROPOSAL: To reaffirm, modify and reaffirm, or delete CSHP profes-sional policies which are five (5) years or older
SUBMITTED BY: Christine Antczak, Susan Cho, Vicky Ferraresi, Ian Ford, Kenn Horowitz, and Nancy Korman
DATE: June 6, 2011
SITUATION:
1. CSHP Professional Policies have been catalogued since 1980. 2. One of the duties of Board of Directors is to review any professional
policy that is 5 years old or older. For this review, each professional policy that is five years old was reviewed for applicability and current relevance and recommendations to reaffirm, modify and reaffirm, or delete were outlined.
3. While analyzing professional policies, ASHP’s professional policy cata-logue was checked for any policies that relate to the topic.
TARGET:
1. A mechanism exists to periodically review CSHP policies for their con-tinued relevance and applicability (CSHP Board of Directors action is generally guided by existing policy.)
2. CSHP’s professional policies accurately reflect current practice and professional standards.
3. The annual review process of professional policy is continued as an opportunity for CSHP to reflect the most current and contemporary positions on pharmacy practice and organizational guidelines for our members.
PROPOSAL:
1. The following CSHP professional policies be reaffirmed as CSHP pro-fessional policy.
2. The following CSHP professional polices to be modified & reaffirm as CSHP professional policy.
3. The following CSHP professional policies be deleted as CSHP profes-sional policy.
CSHP BOARD ACTIONS:At its July 8-9, 2011 meeting, the board approved the proposal.
Policy #: P-200601 Assigned to: Christine Antczak
Recommended Action: £ Reaffirm, £Delete,S Modify & Reaffirm
Current Policy Wording
#2006-01 Internet: Pharmacy Practice (#2006-01)Source: HOD 10/29/00Note: This is former policy #2000-11 approved by the HOD in 2000; modi-fied and reaffirmed by the HOD in 2006 as #2006-01).1. The California Society of Health-System Pharmacists supports pharmacy
practice via the Internet only by sites that adhere to professional stan-
dards of pharmacy consistent with our mission and:
a. Meet all federal and state regulations and statutes, including those on patient consultation, consumer safeguards (e.g. drug-drug inter-actions) and good business practice.
b. Have been certified as a Verified Internet Pharmacy Practice Site (VIPPS) by NABP and are listed on the NABP Website www.nabp.org.
c. This information is disseminated to consumers.
2. Decisions to utilize the Internet should be predicated on compliance with federal and state laws and regulations, including those on patient consultation and licensure criteria;
3. Where appropriate, CSHP shall initiate and participate in regulatory discussions involving the technological advances of the Internet and implications to the practice of pharmacy in maximizing patient care;
4. CSHP will support activities that disseminate information to consumers and key publics regarding reputable Internet pharmacy sites and drug/
disease information on the Internet.
If Modify & Reaffirm, Recommended Wording 1. The California Society of Health-System Pharmacists supports pharmacy
practice via the Internet only by sites that adhere to professional stan-
dards of pharmacy consistent with our mission and:
a. Meet all federal and state regulations and statutes, including those on patient consultation, consumer safeguards (e.g. drug-drug inter-actions) and good business practice.
b. Have been certified as a Verified Internet Pharmacy Practice Site (VIPPS) by NABP and are listed on the NABP Website – www.nabp.netwww.nabp.org.
c. This information is disseminated to consumers.
2. Decisions to utilize the Internet should be predicated on compliance with federal and state laws and regulations, including those on patient consultation and licensure criteria;
3. Where appropriate, CSHP shall initiate and participate in regulatory discussions involving the technological advances of the Internet and implications to the practice of pharmacy in maximizing patient care;
4. CSHP will support activities that disseminate information to consumers and key publics regarding reputable Internet pharmacy sites and drug/
disease information on the Internet.
Rationale for RecommendationThe website address has changed.
Policy #: P-200604 Assigned to: Vicky Ferraresi
Recommended Action: £ Reaffirm, £Delete,S Modify & Reaffirm
Current Policy Wording
# 2006-04 Precepts of Palliative Care (#2006-04)
Source: HOD 10-28-01
CSHP endorses Last Acts’ Precepts of Palliative Care(Full text of Precepts follows).
Last Acts Care and Loving at the End of Life Precepts of Palliative Care Developed by The Task Force on Palliative Care December 1997
Palliative care refers to the comprehensive management of the physical, psychological, social, spiritual, and existential needs of patients. It is espe-cially suited to the care of people with incurable, progressive illness.
Palliative care affirms life and regards dying as a natural process that is a profoundly personal experience for the individual and family. The goal of palliative care is to achieve the best possible quality of life through relief of suffering, control of symptoms and restoration of functional capacity while remaining sensitive to personal, cultural and religious values, beliefs and
September/October 2011 cjhp: California Journal of Health-System Pharmacy 19

Proposals to the 2011 CSHP House of Delegates
practices.Palliative care can be complementary to other therapies that are available
and appropriate to the identified goals of care. The intensity and range of palliative interventions may increase as illness progresses and the complex-ity of care and needs of the patients and their families increase. The priority of care frequently shifts during this time to focus on the dying process with an emphasis on end-of-life decision making and care that supports physical comfort and a death that is consistent with the values and expressed desires of the patient. Palliative care guides patients and families as they make the transition through the changing goals of care, and helps the dying patient who wishes to address issues of life completion and life closure.
Palliative care has become an area of special expertise within medicine, nursing, social work, pharmacy, chaplaincy and other disciplines. However, advances in palliative care have not yet been integrated effectively into standard clinical practice. The fundamental precepts of palliation should be a basic component of the attitudes, knowledge base and practice skills of all clinicians.
The Last Acts Palliative Care Task Force believes that acknowledgment and incorporation of the following core precepts into all end-of-life care can serve as a starting point for needed reform.
Precepts of Palliative Care
Respecting Patient Goals, Preferences and Choices
Palliative Care:Is an approach to care that is foremost patient-centered and addresses
patient needs within the context of family and community.Recognizes that the family constellation is defined by the patient and
encourages family involvement in planning and providing care to the extent the patient desires.
Identifies and honors the preferences of the patient and family through careful attention to their values, goals and priorities, as well as their cultural and spiritual perspectives.
Assists patients in establishing goals of care by facilitating their under-standing of their diagnosis and prognosis, clarifying priorities, promoting informed choices and providing an opportunity for negotiating a care plan with providers.
Strives to meet patients’ preferences about care settings, living situations and services, recognizing the uniqueness of these preferences and the bar-riers to accomplishing them.
Encourages advance care planning, including advance directives, through ongoing dialogue among providers, patient and family.
Recognizes the potential for conflicts among patient, family, providers and payers, and develops processes to work toward resolution.
Comprehensive Caring
Palliative Care:Appreciates that dying, while a normal process, is a critical period in the
life of the patient and family, and responds aggressively to the associated human suffering while acknowledging the potential for personal growth.
Places a high priority on physical comfort and functional capacity, including but not limited to: expert management of pain and other symp-toms, diagnosis and treatment of psychological distress and assistance in remaining as independent as possible or desired.
Provides physical, psychological, social, and spiritual support to help the patient and family adapt to the anticipated decline associated with
advanced, progressive, incurable disease.Alleviates isolation through a commitment to non-abandonment, ongoing
communication and sustaining relationships.Assists with issues of life review, life completion and life closure.Extends support beyond the lifespan of the patient to assist the family in
their bereavement.
Utilizing the Strengths of Interdisciplinary Resources
Palliative Care:Requires an interdisciplinary approach drawing on the expertise of,
among others, physicians, nurses, psychologists, pharmacists, pastoral caregivers, social workers, ancillary staff, volunteers and family members to address the multidimensional aspects of care.
Includes a clearly identified, accessible and accountable individual or team responsible for coordinating care to assure that changing needs and goals are met and to facilitate communication and continuity of care.
Incorporates the full array of inter-institutional and community resources (hospitals, home care, hospice, long-term care, adult day services) and promotes a seamless transition between institutions/settings and services.
Requires knowledgeable, skilled and experienced clinicians, who are provided the opportunity for ongoing education, professional support and development.
Acknowledging and Addressing Caregiver Concerns
Palliative Care:Appreciates the substantial physical, emotional and economic demands
placed on families caring for someone at home, as they attempt to fulfill caregiving responsibilities and meet their own personal needs.
Provides concrete supportive services to caregivers such as respite, round-the-clock availability of expert advice and support by telephone, grief counseling, personal care assistance and referral to community resources.
Anticipates that some family caregivers may be at high risk for fatigue, physical illness and emotional distress, and considers the special needs of these caregivers in planning and delivering services.
Recognizes and addresses the economic costs of caregiving, including loss of income and non-reimbursable expenses.
Building Systems and Mechanisms of Support
Palliative Care:Requires an environment that supports innovation, research, education
and dissemination of best practices and models of care.Needs an infrastructure that promotes the philosophy and practice of
palliative care.Relies on the formulation of responsible policies and regulations by insti-
tutions and by state and federal governments.Promotes equitable and timely access to the full array of interdisciplin-
ary services necessary to meet the multidimensional needs of patients and caregivers.
Demands ongoing evaluation, including the development of research-based standards, guidelines and outcome measures.
Assures that mechanisms are in place at all levels (e.g., systems, direct care services) to guarantee accountability in provision of care.
Requires appropriate financing, including the development of new methods of reimbursement within the context of a changing health care financing system.
Precepts of Palliative Care for Children, Adolescents and Their Families
20 cjhp: California Journal of Health-System Pharmacy September/October 2011

Proposals to the 2011 CSHP House of Delegates
Respecting Patient Goals, Preferences and Choices
Palliative Care:Emphasizes family-centered care and addresses the child’s needs in the
context of the child’s physical condition, developmental stage, family, and community.
Recognizes that the family constellation is defined by the child, the family and their culture and beliefs and encourages child and family involvement in planning and providing care.
Identifies and honors the preferences of the child and family through careful attention to their values, goals and priorities as well as their cultural and spiritual perspectives.
Assists the child and family in establishing goals of care by facilitating their understanding of the diagnosis and prognosis, clarifying priorities and providing an opportunity to collaborate with providers on the creation of a care plan. This process takes into account the child’s developmental stage, chronological age and the family’s wishes.
Respects the roles of parent or surrogate by presenting a model of shared decision-making.
Strives to meet the child’s and family’s preferences about care settings, living situations and services, recognizing the uniqueness of these prefer-ences and assisting the family to work through any barriers to achieving their goals.
Encourages advance care planning through ongoing dialogue among health care professionals, the child and family.
Recognizes the potential for conflicts among the child, family, providers, and payers and develops processes to work toward resolution.
Comprehensive Caring
Palliative Care:Responds to the inherent human suffering and grief associated with living
with serious illness and life-threatening conditions.Appreciates differences among children and families regarding the mean-
ing of their experience; for some children and families, this experience can be a period for inner growth.
Places a high priority on physical comfort and functional capacity, including, but not limited to, expert management of pain and other symp-toms, diagnosis and treatment of psychological and spiritual distress, and assistance in remaining as independent as possible, if so desired.
Provides comprehensive interventions and support to help the child and family adapt to living with serious illness and/or life-threatening conditions.
Alleviates isolation through a commitment to non-abandonment, ongoing communication and sustaining relationship.
Assists with reaffirmation of the child’s life and the parents’ role in that life as well as helping to bring about completion and closure within the context of family culture and values.
Extends support beyond the life span of the child to assist the family and others in their bereavement through ongoing support, guidance and remembrance.
Using the Strengths of Interdisciplinary Resources
Palliative Care:Requires an interdisciplinary team of knowledgeable, skilled and experi-
enced pediatric health care professionals, who are provided the opportunity for ongoing education, professional support and development.
Includes a clearly identified, accessible and accountable individual or
team responsible for coordinating care to ensure that changing needs and goals are met and to facilitate continuity of care and ongoing communica-tion among team members, the child and family.
Incorporates the full array of inter-institutional and community resources (e.g., schools, hospitals, home care, hospice) and promotes a seamless tran-sition between institutions/settings and services.
Determines what services are available for the child and family and that the hospice/palliative care staff are knowledgeable about the unique needs of the seriously ill child and the family.
Acknowledging and Addressing Caregiver Concerns
Palliative Care:Recognizes that the well-being of seriously ill or injured children and that
of their family caregivers are intertwined.Appreciates the substantial physical, emotional and economic demands
placed on a family caring for the child at home or during prolonged and/or repeated hospitalizations as they attempt to fulfill care-giving responsibili-ties and to meet the entire family’s needs.
Provides concrete supportive services to caregivers such as respite care, and around-the-clock availability of expert advice and support by tele-phone, grief counseling, personal care assistance and referral to community resources.
Anticipates that some family caregivers may be at high risk for fatigue, physical illness and emotional distress and considers the special needs of these caregivers in planning and delivering services.
Recognizes and addresses the economic costs of care giving including loss of income and non-reimbursable expenses.
Acknowledges that family grief begins during the child’s illness and con-tinues after a child dies.
Building Systems and Mechanisms of Support
Palliative Care:Requires an environment that supports innovation, research, education
and dissemination of best practices and models of care.Needs an infrastructure that promotes the philosophy and practice of
pediatric palliative care.Relies on the formulation of responsible policies and regulations by insti-
tutions and by state and federal governments.Promotes equitable and timely access to the full array of interdisciplinary
services necessary to meet the multidimensional needs of patients and their caregivers.
Demands ongoing evaluation including the development of evidence-based standards, guidelines and outcome measures.
Assures that mechanisms are in place at all levels (e.g., systems, direct care services) to guarantee accountability in the provision of care.
Requires appropriate financing including the development of new meth-ods of reimbursement within the context of a changing health care financing system.
See other References not included here: National Hospice and Palliative Care Organization Palliative Care Precepts Crosswalk, JCAHO Standards, CMS (Medicare) Conditions of Participation.
If Modify & Reaffirm, Recommended Wording
September/October 2011 cjhp: California Journal of Health-System Pharmacy 21

Proposals to the 2011 CSHP House of Delegates
Precepts of Palliative Care The Pharmacist’s Role in Hospice and Palliative Care
Source: HOD 10-28-01 CSHP endorses Last Acts’ Precepts of Palliative Care the 2009 Clinical
Practice Guidelines for Quality Palliative Care developed by the National Consensus Project for Quality Palliative Care These guidelines are for all health care professionals to help address the growing population of patients with advanced illness. CSHP believes that pharmacists have a pivotal role and should be integral members of all hospice and palliative care interdis-ciplinary teams.
See (www.nationalconsensusproject.org ) for the full text of the Clinical Practice Guidelines and the ASHP Statement on the Pharmacist’s Role in Hospice and Palliative Care (www.ashp.org/DocLibrary/BestPractices/SpecificStHospice.aspx )
Rationale for RecommendationThe original policy is a statement of support for palliative care. It is time
to redirect our professional statement to pharmacist involvement in hospice and palliative care.
40 professional organizations have endorsed the 2004 guidelines, and 20 (as of 3/25/11) have endorsed the 2009 guidelines; none of them are pharmacy organizations.
Although the guidelines acknowledge the input of 7 pharmacist leaders in the field, there is only passing mention of the pharmacist twice in the document (as an optional part of the interdisciplinary team, pages 9 and 72):
…a core group of professionals from medicine, nursing and social work, and may include some combination of volunteer coordinators, bereavement coordinators, chaplains, psychologists, pharmacists, nursing assistants and home attendants, dietitians, speech and language patholo-gists, physical, occupational, art, play, music, and child-life therapists, case managers, and trained volunteers.
Drug therapy is the mainstay of the palliation of pain and other symp-toms. Other palliative care cannot take place in the face of unremitting symptoms (e.g. pain or nausea). This is a great opportunity for CSHP to support this practice area and to advocate for pharmacist involvement in these areas of practice.
Policy #: P-200606 Assigned to: Susan Cho
Recommended Action: S Reaffirm, £Delete,£ Modify & Reaffirm
Current Policy Wording
#2006-06 Off-Label Use of Medication (#2006-06)Source: HOD 10/15/2006
1. CSHP supports the practice of prescribing medications for off-label uses that are documented in the medical literature in a system that:
a. Maintains patient access to pharmacist review of all medications.b. Protects the pharmacist’s right of refusal of an off-label use of a
medication.c. Preserves the patient-pharmacist-prescriber relationship.d. Provides adequate patient counseling and education, particularly to
patients taking medications for off-label use.e. Recognizes the prescriber’s responsibility in assuring the appropri-
ate and safe use of all medications; and
f. Encourages evidence-based decision making and prescribing.
2. CSHP opposes efforts to restrict the off-label use of medication when the usage is medically appropriate, evidence-based and in the patient’s best
interest.
If Modify & Reaffirm, Recommended Wording
Rationale for Recommendation
Policy #: P-200607 Assigned to: Christine Antczak
Recommended Action: £ Reaffirm, SDelete,£ Modify & Reaffirm
Current Policy Wording
#2006-07 Pharmaceutical Care (#2006-07)
Source: HOD 10/15/2006The California Society of Health-System Pharmacists supports the
practice of pharmaceutical care (pharmacist cognitive services) that seeks to achieve optimal therapeutic outcomes for patients and improves their quality of life. This care may or may not occur in conjunction with the pro-vision of a medication product. This care supports collaborative efforts of a multi-disciplinary patient care team, which includes the patient, physicians, pharmacists, nurses, dieticians, respiratory care providers, and others.
If Modify & Reaffirm, Recommended Wording
Rationale for RecommendationASHP has an existing policy under their Governement, Laws and
Regulations section titled the ASHP Statement on the Principles of Including Medications and Pharmaceutical Care in Health Care Systems.
PROPOSAL D
PROPOSAL: Update and Move A-200618: Volunteers: State and Chapter Level to Professional Policy Catalogue
SUBMITTED BY: Maria Serpa, President Nancy Korman, Chair of the Board
DATE: June 21, 2011
SITUATION:
1. CSHP Professional and Administrative Policies have been catalogued since 1980.
2. One of the duties of Board of Directors is to review any administrative policy that is 5 years old or older.
3. During the Committee on Finance review of the Administrative Policy STP, it was determined that A-200818. Volunteers: State & Chapter Level was a Professional Policy and should be moved from the Administrative Policy catalogue to the Professional Policy catalogue.
TARGET:
1. A mechanism exists to periodically review CSHP policies for their con-tinued relevance and applicability (CSHP Board of Directors action is generally guided by existing policy.)
2. CSHP’s professional policies accurately reflect current practice and professional standards.
3. The annual review process is an opportunity for CSHP to reflect the most current and contemporary positions on pharmacy practice and
organizational guidelines for our members.
22 cjhp: California Journal of Health-System Pharmacy September/October 2011
Proposals to the 2011 CSHP House of Delegates
PROPOSAL:
Modify and Move A-200618 to the Professional Policy catalogue:
A-200618 Volunteers: State & Chapter LevelCSHP is a member-centric organization as defined in the organization’s
Mission, Vision and Values.Volunteerism is to be promoted and supported throughout the CSHP
organization in order to provide opportunities for personal growth and advancing the professional growth.
CSHP BOARD ACTIONS:At its July 8-9, 2011 meeting, the board approved the proposal.
PROPOSAL E
PROPOSAL: To Adopt CSHP Professional Policy on Hospice and Palliative Care
SUBMITTED BY: Victoria Ferraresi (Chair, House of Delegates) DATE SUBMITTED: June 17, 2011
SITUATION:1. In 2001 the CSHP House of Delegates approved Professional Policy,
Precepts of Palliative Care. The policy was reaffirmed in 2006 (P-20064).2. ASHP has a Statement on the Pharmacist’s Role in Hospice and Palliative
Care (www.ashp.org/DocLibrary/BestPractices/SpecificStHospice.aspx) This document states:
Medicare regulations state that the hospice must “employ a licensed pharmacist; or have a formal agreement with a licensed pharmacist to advise the hospice on ordering, storage, adminis-tration, disposal, and record keeping of drugs and biological”.
This is only applicable for a hospice inpatient unit where drugs are purchased, stored and dispensed (42 CFR §418.106(2). The majority of hospice care in the United States is provided in patient homes or in the long-term care or assisted living facilities where they reside. There is no mandate for pharmacist services of any kind in these settings in Medicare regulations
3. ASHP Policy Statement 0307, Pharmacist Support for Dying Patients promotes the role of pharmacists in providing care to these patients but does not address the pharmacist as part of the hospice or palliative care interdisciplanary group.
4. In 2004 the National Quality Consensus Project for Quality Palliative Care pu blished Clinical Practice Guidelines for Quality Palliative Care. This was updated in 2009, available at www.nationalconsensus-project.org.
5. Although the 2009 guidelines acknowledge the input of seven phar-macist leaders in palliative care, there is only passing mention of pharmacists twice in the document, as an optional part of the interdisci-plinary team (on pages 9 and 72, bolded font added for emphasis here):
…a core group of professionals from medicine, nursing and social work, and may include some combination of volunteer coordinators, bereavement coordinators, chaplains, psychol-ogists, pharmacists, nursing assistants and home attendants,
dietitians, speech and language pathologists, physical, occu-pational, art, play, music, and child-life therapists, case managers, and trained volunteers.
6. In 2008, the Medicare Hospice Conditions of Participation were updat-ed to add:
42 CFR §418.106(a) The hospice must ensure that the interdisciplanary group confers with an individual with education and training in drug management as defined in hospice policies and procedures and State law…to ensure that drugs and biologicals meet each patient’s needs.
7. The Medicare Hospice Conditions of Participation currently specify the following as required members of the interdisciplanary group—a doc-tor of medicine or osteopathy, a registered nurse, a social worker, and a pastoral or other counselor (42CFR §418.56).
8. Current CSHP Professional Policy 2006-07, Pharmaceutical Care, sup-ports the collaborative efforts of the multi-disciplinary patient care team
which includes pharmacists.
TARGET:
1. Endorse the 2009 Clinical Practice Guidelines for Quality Palliative Care from the National Quality Consensus Project for Quality Palliative Care.
2. Acknowledge and educate other health care providers and stakeholders on the role of pharmacists in the provision of hospice and palliative care.
3. Advocate for the inclusion of pharmacists as active members of hospice and palliative care interdisciplinary teams. (And eventually in hospice
as core providers specified in the Medicare Conditions of Participation.)
PROPOSAL:1. Create new Professional Policy, Hospice and Palliative Care CSHP endorses the 2009 Clinical Practice Guidelines for Quality
Palliative Care (from the National Quality Consensus Project for Quality Palliative Care) and advocates for the active participation of pharmacists as integral members of hospice and palliative care interdisciplinary teams.
Full text of the guidelines (76 pages) is available at www.national-
consensusproject.org/guideline.pdf
ESTIMATED RESOURCES REQUIRED FOR PROPOSED ACTION(S)
Financial: EVP time:
Staff time:
CSHP BOARD ACTION:At its July 8-9, 2011 meeting, the board approved the proposal.
September/October 2011 cjhp: California Journal of Health-System Pharmacy 23

Proposals to the 2011 CSHP House of Delegates
PROPOSAL F
PROPOSAL: To Adopt CSHP Professional Policy on the “California Health Benefit Exchange.”
SUBMITTED BY: Joanne Whitney, Council on Professional Affairs DATE: June 6, 2011
SITUATION:1. In September 2010, as the first law passed in the United States relat-
ing to the federal statute (Patient Protection and Affordable Care), the California Health Benefit Exchange was passed into law by Assembly Bill AB 1602 and Senate Bill SB 900.
2. The law sets up an exchange where the approximately 7 million unin-sured and thousands of underinsured California residents will be able to purchase affordable quality health insurance from member health plans starting in 2014.
3. To date four meetings have been held to determine the exact structure of the exchange and the methods by which the exchange provid-ers will comply with federal quality measures that may include care coordination, chronic disease management and medication and care compliance.
4. Medication Therapy Management (MTM) by pharmacists is recognized as a key element in improving patient health and reducing the costs of health care, has been endorsed by both state and national pharmacy organizations and is compensated as professional services in many venues.
5. The inclusion of compensated MTM by pharmacists as in the services and benefits that must be provided by insurers in the Exchange ensures that federal mandates for clinical quality measures are met.
TARGET:1. To support and advocate for the inclusion of MTM compensated ser-
vices by pharmacists in the package of benefits provided by insurers in the CaliforniaHealth Benefit Exchange.
PROPOSAL:1. To adopt CSHP Professional Policy on the “California Health Benefit
Exchange” as follows: The California Society of Health-System Pharmacists supports compen-
sation for pharmacist cognitive services.
RESOURCES REQUIRED FOR PROPOSED ACTION(S) Financial: N/A EVP time: N/A Staff time: N/A
CSHP BOARD ACTION:At its July 8-9, 2011 meeting, the board approved the proposal as amended.
PROPOSAL G
PROPOSAL: To Adopt CSHP Professional Policy on “Assisting Pharmacy Schools on Tailoring Pharmacy Education”
SUBMITTED BY: Council on Professional Affairs DATE: June 6, 2011
SITUATION:1. The California Society of Health-System Pharmacists shall seek an
active role in assisting California schools of pharmacy and proposed schools of pharmacy to tailor pharmacy education in pharmacy schools, so that pharmacy students are better prepared to meet the needs of the profession. Examples may include identification or strengthening the educational content on pharmacy leadership, clinical specialties, or fields of pharmacy needed for the future of pharmacy practice (such as informatics).
2. Both ASHP and AACP have reports stating the need to promote lead-ership development beginning at the schools (early in a pharmacist’s career) so that pharmacists may be better prepared to serve as health-care leaders.
3. No similar policy relating to this matter is evident in current CSHP policy.
TARGET:1. To increase activities related to assessing pharmacy education. 2. To collaborate with schools of pharmacy in California to align curricu-
lum with the identified future needs and expectations of pharmacists. Examples include, but are not limited to, the following:
a. Strengthening of the educational content on pharmacy leadership and management;
b. Informatics; c. Pharmacoeconomics; d. Medication safety, or; e. Ambulatory care roles where the pharmacist is a primary care pro-
vider of medication therapy management.
PROPOSAL: To adopt CSHP Professional Policy on “Assisting Pharmacy Schools on
Tailoring Pharmacy Education” as follows:
The California Society of Health-System Pharmacists supports acollabo-rative relationships with Pharmacy Schools and proposed Pharmacy Schools providing feedback on traditional, as well as emerging, roles of the pharmacist on provisions of pharmaceutical care so that pharmacy students are better prepared to meet the needs of the profession and the patients we serve.
RESOURCES REQUIRED FOR PROPOSED ACTION(S) Financial: N/A EVP time: N/A Staff time: N/A
CSHP BOARD ACTION:At its July 8-9, 2011 meeting, the board approved the proposal as amended.
24 cjhp: California Journal of Health-System Pharmacy September/October 2011

PROPOSAL H
PROPOSAL: To Modify CSHP Bylaws on Vision and Mission Statements
SUBMITTED BY: Maria Serpa, President DATE: August 3, 2011
SITUATION: 1. Every three (3) years CSHP reviews its vision and mission statements as
a part of the Strategic Planning process.2. Mission and Vision Statements are typically short and meant to be easily
stated by leadership and membership.3. The concepts in the old Mission Statement are covered in CSHP Specific
Purposes and CSHP Values.
TARGET: 1. Update CSHP Vision and Mission statements
PROPOSAL: 1. Bylaws changes as below
ARTICLE III
PURPOSES AND MISSION STATEMENT
SECTION 2. VISION STATEMENT The Leader in Wellness, Patient Safety and the Optimal Use of
Medications Leading Pharmacy Practice in Patient Safety and Medication Therapy Management.
SECTION 3. MISSION STATEMENT To Promote Wellness, Patient Safety and Optimal Use of Medications CSHP is a professional society of pharmacists, pharmacy technicians,
student pharmacists and associates who promote the health, safety, and appropriate use of medication therapy f or patients and the public by: (a) Serving as an organization through which the membership pursues
its common professional goals. (b) Providing leadership for the profession and support for its members. (c) Advocating for its members before private and public agencies and
health care professional organizations.
RESOURCES REQUIRED FOR PROPOSED ACTION(S) Financial: none EVP time: 0 hours Staff time: 3 hours (to take to HOD and add to elections; update bylaws
document)
CSHP BOARD ACTION:At its strategic planning meeting on July 31, 2011, the board developed and
approved a new CSHP Mission and Vision Statement. u
the Council on Professional Affairs (COPA) is seeking examples of innovative pharmacy practice projects in
order to share them with other CSHP members via InfoSource, the California Journal of Health-System Pharmacy, discussion at regional chapter meetings, and the CSHP Website. To date, COPA has identified many innovative practice examples that include: transition care pharmacists, expert witnesses, drug take back, immunization administration, automation and technology, medication safety pharmacists, and MTM. COPA recognizes that there are many more innovative practice proj-ects and would request that you provide additional examples. Please forward your examples along with your contact infor-mation to [email protected] or fax them to (916) 447-2396.
In addition to providing this information as a catalyst for improvement and expansion in different practice areas, CSHP believes these innovative practices would be great educa-tional materials for legislators and consumers as they promote the pharmacy practice.
One of the Council on Professional Affairs’ (COPA) charges this year includes identifying innovative pharmacy practice projects that our members might find useful. COPA wanted to share with you one innovative project that occurred in San Diego in December 2009. The San Diego Patient Safety Council’s (consisting of 11 healthcare institutions and com-panies) charter was to coordinate care to improve patient experience and outcomes. The project was to provide rec-ommendations and tools to Intensive Care settings for the development and implementation of an evidence-based stan-dard for safe and effective management of pain, sedation, and delirium in adult intensive care unit (ICU) ventilated patients. For more information and for the full document titled “ICU Sedation Guidelines of Care,” please visit www.cshp.org and click on Newsroom.u
Call for innovative Pharmacy Practice Project examples
September/October 2011 cjhp: California Journal of Health-System Pharmacy 25

Kathleen Hill Besinque, PharmD, MSEd, FASHP, FCSHPDistinguished Service Award
Kathleen Hill Besinque has been named the 2011 CSHP Distinguished Service Award recipient. Dr. Besinque is currently the Associate Professor of Clinical Pharmacy at the University of Southern California in Los Angeles, CA.
Dr. Besinque has been an extremely active member of CSHP and has served on numerous committees and boards including Chair of the House of Delegates, CSHP Foundation Board Member, and multiple Seminar Management Teams. Additionally, she has been President, Treasurer, and Pharmacist of the Year of her local chapter, the Southern California Society of Health-System Pharmacists. Currently, Dr. Besinque is serving as the CSHP Foundation Treasurer.
Dr. Besinque received her Doctor of Pharmacy degree from the University of Southern California School of Pharmacy. She completed her residency at the Veterans Administration Outpatient Clinic and the USC School of Pharmacy in Los Angeles, CA.
Brian Hodgkins, PharmD, FASHP, FCSHP said, “Her prolific contribution to this profes-sion is manifest in her tireless collaboration with others across the profession with varying view points and opinions to develop a sense of professional one-ness and to showcase the value of pharmacist efforts which has resulted in tremendous recognition by her peers and colleagues in every specialty of healthcare.”
Terry T. Hashimoto, PharmD Pharmacist of the Year
Terry T. Hashimoto has been named the 2011 Pharmacist of the Year by CSHP. Dr. Hashimoto is currently the Director of Pharmacy at Consonus Health in Vacaville, CA.
Dr. Hashimoto has nearly 4 decades of managerial and direct patient care experience in community, hospital, mail order, and home infusion pharmacy. He was one of the pioneers in home infusion by establishing the first home infusion pharmacy (Option Care) in the Sacramento area in 1982.
Dr. Hashimoto received his Doctorate of Pharmacy at UCSF School of Pharmacy. He was Treasurer of CSHP from 1986-1988, President in 1989, and has sat on multiple committees including Council on Organization Affairs, and Seminar Management Teams. Dr. Hashimoto has also been Treasurer, President, and Pharmacist of the Year of his local chapter, Sacramento Valley Society of Health-System Pharmacists
Max Ray, PharmD, MS, LHD said “Terry’s professional accomplishments are quite remarkable. In addition to being a seasoned health-system pharmacy manager/director, he has established himself as an expert, with a national reputation, in the area of infusion therapy and care delivery. He has brought a standard of care to this area of practice that reflects the highest professional standards. And he has generously shared his knowledge and expertise in this area with professional colleagues, residents and students.”
California SoCiety of HealtH-SyStem PHarmaCiStS
2011 award recipients
26 cjhp: California Journal of Health-System Pharmacy September/October 2011

CSHP 2011 Awards Recipients
Kathy Daly, CPhT, FTCSHPTechnician Achievement Award and Practitioner Recognition Program, Technician Fellow
Kathy Daly is the lead pharmacy technician at Scripps Mercy Hospital in San Diego, CA. She has been extremely active in CSHP as the chair of the Technician Division Executive Committee (TDEC), technician delegate to the CSHP House of Delegates, mem-ber of the Government Affairs Advisory Committee and Editorial Advisory Committee, Technician Co-Chair for the 2009 Seminar Management Team, and Technician Liaison to her local chapter, the San Diego Society of Health-System Pharmacists (SDSHP) since 2004. Additionally, she received SDSHP Technician of the Year in 2004 and 2008.
Daly is a certified Pharmacy Technician (PTCB) and a California Registered Pharmacy Technician through the California Board of Pharmacy. She has contributed seven techni-cian focused articles to the California Journal of Health-System Pharmacy.
Jason Lam, PharmD said “Kathy’s ability to inspire others through her energetic passion for pharmacy and CSHP sets her apart from others. She commands respect and admiration from fellow pharmacy technicians and pharmacists through her understanding of SDSHP, CSHP, and hospital practice.”
Peter Ambrose, PharmD, FASHP, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Ambrose played a critical role in convincing the Board of Pharmacy to adopt California’s patient medication safety regulation, “Tech-Check-Tech”. Additionally, he has been involved with CSHP as co-chair of the 2008 Seminar Management Team, sat on the Board of Directors, represented California in the ASHP House of Delegates, and served as President of his local chapter, the South Bay/Long Beach Society of Health-System Pharmacists. He was also named an ASHP Fellow in 1996.
Dr. Ambrose received his Doctorate of Pharmacy from UCSF School of Pharmacy and completed his residency in Hospital Pharmacy and Fellowship in Pharmacokinetics at Long Beach Memorial Medical Center. He is currently the Professor of Clinical Pharmacy at the UCSF School of Pharmacy and resides in Long Beach, CA.
Jason Bandy, PharmD, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Bandy has been a member of the CSHP Government Affairs Advisory Committee since 2007 and served as Chair in the 2009-2010 term. He also served as the Membership Chair for his local chapter, CSHP-Sacramento Valley since 2008. He has stood out for his work as a preceptor over the past nine years. In 2007, Dr. Bandy was named the Preceptor of the Year from the University of the Pacific, Thomas J. Long School of Pharmacy and Health Sciences.
Dr. Bandy received his Doctorate of Pharmacy from the University of the Pacific, Thomas J. Long School of Pharmacy and Health Sciences and completed his pharmacy residency at St. Joseph’s Medical Center in Stockton, CA. Currently, Dr. Bandy is working at UC Davis Medical Center as a Senior Pharmacist in Pharmacy Ambulatory Care Clinics and resides in Sacramento, CA.
September/October 2011 cjhp: California Journal of Health-System Pharmacy 27

CSHP 2011 Awards Recipients
Julianna Burton, PharmD, BCPS, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Burton stood out for her work at UC Davis Medical Center, where she started an ambulatory care residency program, created an anticoagulation class for patients, and started a cardiovascular and refill clinic among many other things.
She has been very active in CSHP through her service on the Board of Directors, Chair of the Committee on Goals, and member of the Medication Therapy Management Committee, as well as President, Secretary, and Delegate of her local chapter, the Sacramento Valley Society of Health-System Pharmacists.
Dr. Burton received her Doctorate of Pharmacy from the University of the Pacific, Thomas J. Long School of Pharmacy and Health Sciences and completed a pharmacy practice residency at St. Joseph’s Medical Center in Stockton, CA. She currently works as the Supervisor of the Ambulatory Care Clinical Section of the Department at UC Davis Medical Center.
Donna Dare, PharmD, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Dare has been a member of CSHP since 1997 and has served at her local chapter, CSHP-Golden Gate, as treasurer and public relations committee member. Additionally, Dr. Dare has served on the UCSF Pharmacy Alumni Board of Governors since 2006.
Dr. Dare received her Doctorate of Pharmacy from the UCSF School of Pharmacy and currently works at the San Francisco VA Medical Center as the Chief of Pharmacy Services. She has worked at the VA since 1984. Most recently, Dr. Dare designed and coordinated the new USP-797-compliant inpatient pharmacy to include robotic automa-tion. Since 1989, Dr. Dare has received the Outstanding Performance Award from the San Francisco VA Medical Center nine times.
“Donna has truly achieved a lot in advancing the profession of pharmacy over the years. She continues to help shape the direction of pharmacy practice by being on vari-ous national committees within the VA system that helps to expand the scope of practice and maintain the quality standards for pharmacists,” said Dan Dong, PharmD, FCSHP.
Jerika Lam, PharmD, AAHIVE, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Lam graduated from the University of Southern California (USC) School of Pharmacy, completed a pharmacy practice residency at the San Francisco VA Medical Center and an HIV Research Fellowship at USC. Nancy Korman, PharmD, FCSHP said “Dr. Lam’s completion of a post-doctoral research fellowship at USC and recognition as an HIV Expert in the American Academy of HIV Medicine is a testament to her pursuit of excellence as a practitioner.”
Dr. Lam has served as the CSHP Faculty Student Liaison Committee Chair since 2008. She specializes in HIV/Infectious Diseases, and is currently an Assistant Professor in the Department of Pharmacotherapy and Outcomes Science at the Loma Linda University School of Pharmacy.
28 cjhp: California Journal of Health-System Pharmacy September/October 2011

Melissa Mantong, PharmD, MS, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Mantong is an Assistant Professor at the University of the Pacific, Thomas J. Long School of Pharmacy & Health Sciences. She has been a member of CSHP since 1994 and an active member of her local chapter, the Sacramento Valley Society of Health-System Pharmacists. She has served as their President, Technician Committee Chair, and Membership Committee Member and received the Pharmacist of the Year award in 2003.
Dr. Mantong received her Doctorate of Pharmacy from the UCSF School of Pharmacy. She completed a pharmacy practice residency at the California Pacific Medical Center, a pediatric residency at UC Davis Medical Center, and a patient safety fellowship at VHA West Coast. Additionally, she completed the Pharmacy Leadership Academy through the American Society of Health-System Pharmacists Foundation.
Robert L. Poole, PharmD, FPPAG, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Poole has been a member of CSHP since 1977 and served as President of his local chapter, the Quatra County Society of Health-System Pharmacist. He has authored/co-authored over 40 journal articles and has authored/co-authored 30 plus other publications, including articles in non-peer reviewed journals, book chapters, abstracts and contribu-tions to on-line references.
“Beyond his own personal contributions via his publications and presentations, Dr. Poole’s contributions to the profession and health care must include the fact that he has made education and training a priority,” said Donald Kishi, PharmD, FCSHP.
Dr. Poole received his Doctorate of Pharmacy and completed a residency at the UCSF School of Pharmacy. He is currently the Director of Pharmacy at the Lucile Packard Children’s Hospital at the Stanford University Medical Center. He is also a Clinical Professor at the UCSF School of Pharmacy, an Adjunct Professor of Pharmacy Practice at the University of the Pacific School of Pharmacy, an Adjunct Clinical Professor at the Touro University College of Pharmacy and a Clinical Professor of Pharmacy Practice at the Western University of Health Sciences College of Pharmacy.
Sarah Scarpace Lucas, PharmD, BCPS, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Lucas stood out for her work as the Pediatric Clinical Pharmacist at the UCSF Benioff Children’s Hospital, where she started a PGY2 Pediatric Specialty Residency Program which she currently co-directs, among many other accomplishments. She graduated with a Doctorate of Pharmacy from University of Wisconsin – Madison and completed a specialty residency in pediatric pharmacy practice at the St. Louis Children’s Hospital.
Dr. Lucas has been a member of CSHP and Faculty Student Liaison to the UCSF School of Pharmacy since 2005. According to Julie Ganz, PharmD, “Dr. Lucas strives to optimize medication safety and patient center pharmaceutical care. The degree to which she leads by example is impressive indeed. I recall circumstances where she felt it neces-sary to challenge a parent’s decision when it meant such a decision could compromise their child’s care. She has conviction and will respectfully intercede with families to ensure the safety of patients.”
CSHP 2011 Awards Recipients
September/October 2011 cjhp: California Journal of Health-System Pharmacy 29
CSHP 2011 Awards Recipients
Join the dynamic Pharmacy Department at Madera Community Hospital! We are a 106-bed acute care hospital located in the heart of Central California. Our area offers affordable housing and excellent schools. We are close to the mountains, the ocean, and Yosemite National Park!
The ideal candidate will provide comprehensive pharmaceutical care which includes: clinical, distribution, educational, informational, quality assurance and supervisory functions for Madera Community Hospital Pharmacy Department. This person must have a current State of California Pharmacist License. This person may interact with all other patient care providers including physicians, nurses, respiratory therapists, physical therapists, dietitians, pharmacist, pharmacy technicians, pharmacy buyer, and patients.
For immediate consideration, please apply online with resume: www.maderahospital.org or contact:
Human Resources 1250 East Almond Avenue Madera, CA 93637 (559) 675-2728 EOE
CLINICAL PHARMACISTFULL TIME POSITION
Competitive Compensation Package
Barbara Uenaka, PharmD, MHA, FCSHPPractitioner Recognition Program, Pharmacist Fellow
Dr. Uenaka has been extremely active in CSHP, where she has served as the Membership Committee Chair and Seminar Management Team 2009 Secretary, as well as President of the Education Committee Chair, Secretary, Director, and Night Out with Industry Chair of her local chapter, the Diablo Society of Health-System Pharmacists. She has been a CSHP member since 1979.
“Dr. Uenaka has been a key member of the Diablo Society of Health Systems Pharmacists for many years. She has served DSHP in numerous capacities, including President. She has always been active in our local chapter as well as all CSHP state wide events. Her professionalism and accomplishments serve as an outstanding example of how a pharmacist can utilize their membership in CSHP to advance the practice of pharmacy,” said Alfonso Becerra, PharmD.
Dr. Uenaka retired from the VA Medical Center in 2008 after over 30 years. She cur-rently resides in Walnut Creek, CA. u
Health-system pharmacists can now count on the Pharmacy Professionals of California Political Action Committee (PPC-PAC) to represent their interests in California and help establish vital relationships with aspiring and existing elected officials.
Founded by the CSHP Board of Directors in January 2009, the PPC–PAC is a bipartisan committee that supports candidates and legislators at the state level who understand the challenges of practicing as a pharmacist in California. With your donation to the PPC–PAC, CSHP can ensure that public officials are educated about the vital role pharmacists play in the healthcare arena. Please see CSHP membership materials and the CSHP Website at www.cshp.org for additional information on the PPC–PAC and to learn how you can donate.
PPC-PACPharmacy Professionals of California Political Action Committee (PPC-PAC)
30 cjhp: California Journal of Health-System Pharmacy September/October 2011

CJHP: Now Featuring Your Research!Submit your article to CJHP and share your research.
Not ready to submit your article yet? Register to review for a colleague.
To register as a reviewer or submit an article for consideration, please visit cshpjournal.msubmit.net.

The mission of the California Society of Health-System
Pharmacists Research and Education Foundation
(CSHP Foundation) is to promote public health and the
safe use of medication through research and education.
You may donate to the Foundation in a number of ways.
You may choose to donate to the Joseph H. Beckerman
Memorial Scholarship Fund, make an unrestricted
donation to the Foundation, or donate in honor of a
friend, colleague, or loved one.
For more information or to make your gift, visit
www.cshpfoundation.org.
The CSHP Foundation is a 501(c)(3) corporation.
Donations are tax-deductible.
Today’s Research for Tomorrow’s BreakthroughsSupport the CSHP Foundation
www.cshpfoundation.org