camilla c.u. zimmermann€¦ · quality of life (hrql) and satisfaction with care in patients with...
TRANSCRIPT

EFFECTIVENESS OF SPECIALIZED PALLIATIVE CARE FOR
PATIENTS WITH ADVANCED CANCER
Camilla C.U. Zimmermann
A thesis submitted in conformity with the requirements
for the degree of Doctor of Philosophy
Institute of Medical Science
University of Toronto
© Copyright by Camilla C.U. Zimmermann 2010
ii
Effectiveness of specialized palliative carefor patients with advanced cancer
Ph.D. 2010, Camilla C.U. ZimmermannInstitute of Medical Science, University of Toronto
ABSTRACT Despite the rapid development of palliative care teams, evidence for their effectiveness in
oncology care is lacking. This thesis reviews and contributes towards this evidence, focusing on
the randomized controlled trial as a research method.
We conducted a systematic review of 22 trials reviewed that measured effectiveness of specialized
palliative care. Family satisfaction with care improved in seven of 10 studies, but only four of 13
trials assessing quality of life and one of 14 assessing symptoms showed a benefit of the
intervention. Conclusions were limited by methodologic problems in all of the trials.
We conducted a phase II study of the efficacy of a palliative care team for symptom control and
satisfaction of 150 patients with advanced cancer. Symptom severity (Edmonton Symptom
Assessment System Distress Score) improved at one week and one month, as did patient
satisfaction (all p<0.0001).
We investigated factors associated with symptom severity and response for patients enrolled in the
phase II study. Symptoms at baseline were worse for women and those with worse performance
status (both p<0.005); female gender and worse baseline symptom severity independently
predicted symptom improvement (both p<0.05).
We planned and initiated an RCT of the effectiveness of an early palliative care intervention for
improvement of health-related quality of life (HRQL) and satisfaction with care. Using baseline
data from this RCT, we examined factors associated with HRQL in patients with advanced cancer.
The strongest determinants of overall HRQL (combined FACT-G total score and FACIT-Sp

iii
Meaning and Peace subscore) were increased age (p<0.001), good performance status (p<0.001)
and survival time >6 months (p=0.001). Compared to patients receiving cancer treatment, those
awaiting new treatment had worse emotional well-being (p<0.001) while those on surveillance or
whose treatment had been stopped had worse existential well-being (p=0.03). Male gender
predicted better emotional and physical well-being and lower income predicted worse social well-
being.
Lastly, we developed recommendations for those planning an RCT in a palliative care population,
incorporating information from the studies presented. Although such RCTs are challenging to
conduct, they are feasible and necessary to improve the evidence base for the treatment of patients
with advanced cancer.
iv
ACKNOWLEDGEMENTS
I have many people to thank. First and foremost, I thank my thesis supervisor, Ian
Tannock and my committee members, Gary Rodin and Malcolm Moore. Many thanks to
my research coordinators, Debika Burman and Nadia Swami, as well as to other research
staff who recruited patients and performed data entry for the studies herein: Kristina
Wakimoto, Shazeen Bandukwala, Jennifer Kottler and Priya Bhola. Thank-you to the
residents and fellows who made contributions to the papers in the thesis: Matthew
Follwell, Rachel Riechelmann and Christopher Lo. Thanks to my clinical palliative care
team for participating in the palliative care intervention, and for facilitating recruitment
for the phase II trial: Dori Seccareccia, John Bryson, Giovanna Sirianni, Ebru Kaya,
Subrata Banerjee, Catherine Purcell, Terri Vanderkooy, Janet Partanen, and Elizabeth
Dougherty. Thank-you to all the medical oncologists in the Department of Medical
Oncology at Princess Margaret Hospital for allowing randomization of their clinics and
for facilitating recruitment to the randomized trial; special thanks to Monika
Krzyzanowska and Natasha Leighl for their contributions to papers in this thesis. Many
thanks to Allan Donner for his statistical mentorship and help with planning the analyses
for the randomized controlled trial, and to Lisa Le for her help planning and carrying out
the analyses for the phase II trial. Personal thanks to Richard Wennberg for being such a
supportive husband and to my children Erica, Hendrik and Karl for putting up with my
long work hours. The research in this thesis was supported by grants from the National
Cancer Institute of Canada, with funds from the Canadian Cancer Society (NCIC #017257
and CCS #020509; CZ). Co-investigators on both grants were: Gary Rodin, Malcolm
Moore, Allan Donner, Amit Oza, Andrea Bezjak, Natasha Leighl, Monika Krzyzanowska,

v
and Anne Rydall. Dr. Ian Tannock wrote a letter of support for both grants, and provided
help and advice throughout.

vi
TABLE OF CONTENTS
Chapter 1 1
Introduction
Chapter 2 4
Aims and hypotheses
Chapter 3 7
Literature review
Chapter 4 10
Phase II study of an outpatient palliative care intervention
in patients with metastatic cancer
Chapter 5 31
Predictors of symptom severity and response in patients with metastatic cancer
Chapter 6 46
Design and methodology for a randomized controlled trial of a palliative careintervention for patients with metastatic cancer

vii
Chapter 7 70
Determinants of health-related quality of life in patients with advanced cancer
Chapter 8 89
Summary of findings
Chapter 9 94
General discussion
Chapter 10 107
Conclusions
Chapter 11 109
Future directions
Appendix 1 113
Appendix 2 125
References 143

1
Chapter One
Introduction
2
INTRODUCTION
Patients with advanced cancer have many physical symptoms and psychosocial
needs, which may begin long before the patient’s death.1-3 Palliative care teams developed
in response to this suffering, first focussing on the needs of patients with terminal cancer
who were dying in hospitals or at home,4,5 and more recently expanding to include the care
of patients earlier in the course of disease and in ambulatory settings.6-13 The structure and
membership of such teams may vary among countries, health care systems and specific care
settings, and at present it is not clear what is the best model for the delivery of specialized
palliative care.14
The evaluation of the effectiveness of specialized palliative care began in 1980 with
the National Hospice Study, a large multi-site American study with a quasi-experimental
design in which the impact of hospice care on quality of life and cost was compared to non-
hospice (conventional) terminal care.15 Results showed that although patients were more
likely to die at home, quality of life was similar for hospice and non-hospice care. Costs
were reduced only for hospice care that did not include an inpatient hospice facility.16 The
first randomized controlled trial of hospice care was published in 1984, and showed no
difference between hospice and conventional care for symptom control or cost, but greater
satisfaction of patients and caregivers in the hospice group.17 In the last decade, there has
been a surge in the number of RCTs assessing the effectiveness of specialized palliative
care.18 These have been of increasing methodologic quality,18 and are often preceded by
pilot studies to assess the feasibility of the study and the efficacy of the intervention.8,13,19
The purpose of this thesis is to make a contribution towards the rigorous assessment
of the effectiveness of specialized palliative care for the care of patients with advanced
3
cancer. Because randomized controlled trials (RCTs) are considered to represent the gold
standard for the assessment of the effectiveness of health care interventions,20 this thesis
will concentrate on the RCT as a research method. Specifically, the research presented in
this thesis includes: (1) a systematic review of RCTs assessing the effectiveness of
specialized palliative care; (2) a phase II study of the efficacy of a palliative care team for
symptom control and satisfaction of patients with advanced cancer; (3) an analysis of
factors associated with symptom severity and response, using data from the phase II study;
(4) a description of the design and methodology of an ongoing RCT of an early palliative
care team intervention for patients with advanced cancer; (5) an analysis of the baseline data
of this ongoing RCT, investigating determinants of health-related quality of life for patients
with advanced cancer; and (6) a summary of recommendations for the planning of an RCT
in a palliative care population, incorporating information from all of these studies. The
thesis concludes with a discussion of future directions for this research.

4
Chapter Two
Aims and hypotheses

5
The overall aim of this research was to make a contribution towards the assessment
of the efficacy and effectiveness of specialized palliative care to improve health-related
quality of life (HRQL) and satisfaction with care in patients with advanced cancer. Specific
aims were:
1. To examine systematically the evidence for effectiveness of specialized palliative
care in improving quality of life, satisfaction with care and/or economic cost. This was done
by conducting a systematic review.
2. To assess prospectively the efficacy of a palliative care clinic consultation in
improving symptom control and satisfaction with care. This was done by means of a phase
II trial. The hypothesis was that one week and one month after consultation in a palliative
care clinic, patients would report improved symptom control and improved patient
satisfaction with care.
3. To present the methodology and plan for analysis of a cluster randomized study of
palliative care. The hypotheses for this study are that, compared to conventional cancer care,
early intervention (at a prognosis of > 6 months) of a multidisciplinary symptom
management and palliative care team in patients with metastatic cancer will be associated
with (i) better patient health related quality of life (HRQL) (primary outcome measure); (ii)
greater patient and caregiver satisfaction with care; (iii) better symptom control; (iv)
6
improved communication with health care providers; and (v) improved caregiver quality of
life (ii-v are secondary outcomes).
4. To examine determinants of HRQL for patients with metastatic cancer. This was
done by examining baseline data of patients recruited for the cluster-randomized trial. We
hypothesized that better HRQL would be associated with demographic factors such as
increased age, male gender, and higher income, and with disease-related factors such as
better performance status, lower comorbidity and increased survival time.
5. To use information from all of these studies, to develop recommendations for
those planning RCTs in palliative care populations.

7
Chapter Three
Literature review
Published previously as:
Zimmermann, C., Riechelmann, R., Krzyzanowska, M.K., Rodin, G, Tannock, I.
Effectiveness of specialized palliative care: A systematic review.
JAMA. 2008; 299(14):1698-1709
Copyright © 2008 American Medical Association. All rights reserved.
A link to the published paper can be found at:
http://jama.ama-
assn.org/cgi/content/full/299/14/1698?ijkey=fQCAC4W598zlY&keytype=ref&siteid=amajnls

8
ABSTRACT
Context: Specialized palliative care teams are increasingly providing care for the terminally
ill. However, the impact of such teams on quality of life of patients, satisfaction with care
and economic cost has not been examined systematically using detailed criteria for study
quality.
Objective: To systematically review the evidence for effectiveness of specialized palliative
care.
Data sources: We performed a keyword search of the following databases from inception to
January 2008: Medline, Ovid Healthstar, CINAHL, EMBASE and the Cochrane Central
Register of Controlled Trials.
Study selection: We included all randomized controlled trials in which specialized
palliative care was the intervention and for which outcomes included quality of life,
satisfaction with care and/or economic cost.
Data extraction: Data on population, intervention, outcome, methodology and
methodological quality were extracted in duplicate by two investigators using standardized
criteria.
Results: Of 396 reports of randomized controlled trials, 22 met our inclusion criteria. There
was most consistent evidence for effectiveness of specialized palliative care in improvement
of family satisfaction with care (seven of ten studies favored the intervention). Only four of
thirteen studies assessing quality of life and one of fourteen assessing symptoms showed a
significant benefit of the intervention; however most studies lacked statistical power to
report conclusive results, and quality of life measures were not specific for terminally ill
patients. There was evidence of significant cost savings of specialized palliative care in only
one of the seven studies that assessed this outcome. Methodological limitations were

9
identified in all trials, including contamination of the control group, failure to account for
clustering in cluster randomization studies, and substantial problems with recruitment,
attrition and compliance.
Conclusions: The evidence for benefit from specialized palliative care is sparse and limited
by methodological shortcomings. Carefully planned trials, using a standardized palliative
care intervention and measures constructed specifically for this population, are needed.
Please go to the journal’s website to read the contents of Chapter 3. A toll-free weblink to
the published article is provided below.
http://jama.ama-
assn.org/cgi/content/full/299/14/1698?ijkey=fQCAC4W598zlY&keytype=ref&siteid=amajnls

10
Chapter Four
Phase II study of an outpatient palliative care intervention
in patients with metastatic cancer
Published previously as:
Follwell, M., Burman, D., Le, L., Wakimoto, K., Seccareccia, D., Bryson, J., Rodin, G.,
Zimmermann, C. Phase II study of an outpatient palliative care intervention for patients
with metastatic cancer, J Clin Oncol. 2009 Jan 10; 27(2):206-213.
For this paper, I designed the study, supervised data collection and analyses, and wrote the
original draft of the submitted manuscript as well as the revisions thereof.

11
ABSTRACT
Purpose: Although there is increasing advocacy for timely symptom control in patients
with cancer, few studies have assessed outpatient palliative care clinics. This study assessed
prospectively the efficacy of an Oncology Palliative Care Clinic (OPCC) in improving
patient symptom distress and satisfaction.
Patients and Methods: Eligible patients were new referrals to an OPCC, had metastatic
cancer, were at least 18 years old, and were well enough and able to speak and read English
sufficiently to provide informed consent and complete questionnaires. Patients received a
consultation by a palliative care team. The primary endpoints of symptom control and
patient satisfaction were assessed using the Edmonton Symptom Assessment Scale (ESAS)
and FAMCARE scales at baseline, one week and one month. Initial and follow-up scores
were compared using paired t-tests.
Results: Of 150 patients enrolled, 123 completed one-week and 88 completed four-week
assessments. At baseline, the mean ESAS distress score was 39.5. The mean improvement
in ESAS distress score was 8.8 (P<.0001) at one week and 7.0 (P<.0001) at one month.
Statistically significant improvements were observed for pain, fatigue, nausea, depression,
anxiety, drowsiness, appetite, dyspnea, insomnia and constipation at one week (all P≤.005)
and one month (all P≤.05). The mean improvement in FAMCARE score was 6.1 (P<.0001)
at one week and 5.0 (P<.0001) at one month.
Conclusion: This phase II study demonstrates efficacy of an OPCC for improvement of
symptom control and patient satisfaction with care. Randomized controlled trials are
indicated to further evaluate the effectiveness of specialized outpatient palliative care.

12
INTRODUCTION
The symptom and psychosocial needs of patients with advanced cancer are increasingly
acknowledged,1-3 resulting in the development and expansion of palliative care programs in
cancer settings.21-24 The purview of such programs traditionally encompassed inpatient
consultations, palliative care units and home hospice care.4,5 However, with increasing
importance placed on timely management of symptoms and advance care planning,25,26
there has been a growing interest in interventions in the ambulatory care setting.6-13
Research evaluating the effectiveness of specialized palliative care has been limited
by methodological difficulties,18,27-29 and few randomized trials have shown a benefit of
specialized palliative care for quality of life11,30 or symptom control.9 Moreover, few trials
have evaluated palliative care in the outpatient setting9-11 and those that have did not assess
specialized palliative care clinics, which are a new development in cancer care. Therefore,
the current evidence for effectiveness of palliative care clinics for symptom control is
limited to a few retrospective studies.6-8
The primary objective of this uncontrolled, phase II study was to assess
prospectively the efficacy of a palliative care clinic consultation in improving symptom
control and satisfaction with care. Secondary objectives were to assess the feasibility of
enrolling patients in a study at the initial visit at a palliative care outpatient clinic; to
determine whether telephone follow-up at one week or one month would be appropriate for
measuring outpatient palliative care effectiveness; and to explore the responsiveness of
specific symptoms to the intervention.

13
PATIENTS AND METHODS:
Patient selection
The study received approval from the University Health Network Research Ethics Board,
and all patients provided written, informed consent. Participants were recruited upon initial
referral to the Oncology Palliative Care Clinic (OPCC) at Princess Margaret Hospital
(PMH), a comprehensive cancer center in Toronto, Canada. Eligible patients had metastatic
cancer, were at least 18 years old, and were well enough and had sufficient English
proficiency to provide informed consent and complete questionnaires. All newly referred
patients were considered for participation; this included both patients who continued to be
followed at PMH, and those whose follow-up would take place elsewhere (e.g. with home
palliative care physicians, in palliative care units, or in hospices).
Palliative care team intervention
The OPCC is a component of a larger palliative care service at PMH.23 Outpatients are
referred to the OPCC by PMH oncologists, for management of pain, other symptoms and
end-of-life planning.23,31
The consultation process has been described previously.23 The initial consultation
lasts approximately 90 to 120 minutes; patients are seen first by a palliative care registered
nurse (RN) case manager, who assesses the patient and collects the names of their
medications. The palliative care physician then conducts a full medical, physical and
psychosocial assessment, following which recommendations are made for symptom and
palliative care treatment, education, counseling, and home support. The palliative care team
includes a social worker and psychiatrists, who are involved depending on patient need and
preference; other specialists are consulted as necessary. Referrals to home care and

14
community hospice and palliative care agencies are made as appropriate. A complete note is
dictated for the patient’s electronic medical record and is also sent to the patient’s
oncologist and family physician.
Follow-up appointments at the OPCC are tailored to the needs of each patient.
Patients with uncontrolled symptoms are called by their palliative care physician or nurse
within one week. All patients are given contact information for the nurse and physician, and
the number for the 24-hour on-call service staffed by palliative care physicians; patients are
encouraged to call if their symptoms are poorly controlled. The average time to follow-up is
approximately one month, but medications are titrated over the telephone in the interim.
Follow-up time can range from a few days (e.g. patients with poorly controlled symptoms)
to months (e.g. symptom-free patients referred for planning). Patients who are too ill to
return are referred to home palliative care physicians in the community.
Study procedures
Patients were recruited in the palliative care clinic waiting area. Those consenting were
interviewed briefly by research staff to evaluate Eastern Cooperative Oncology Group
(ECOG) performance status,32 and completed the Edmonton Symptom Assessment Scale
(ESAS)33 and FAMCARE measures.34 The ESAS is normally completed by all patients
attending the OPCC, with the assistance of the RN Case Manager. For this study, research
staff administered the ESAS, before any contact with the palliative care team. One copy of
the ESAS was retained by research staff, and another was used in the clinical assessment by
the nurse and physician, as is usual in the OPCC.23 The FAMCARE was not shown to the
palliative care team.

15
After the completion of baseline measures, research staff completed the chart review
to extract data including age and tumor type. Research staff telephoned patients one week
and one month following the initial visit, and readministered the ESAS and FAMCARE by
telephone. Information on source and reason for referral to palliative care, comorbidity, and
palliative care interventions was abstracted from the chart and clinical database.
Measures
We chose measures that were validated in patients with advanced cancer and quick to
complete. Brevity was important, since patients were providing consent and completing
measures during the waiting time before their palliative care consultation, and by telephone.
The ESAS is a 0-10 numerical scale (0=best, 10=worst) to rate severity of 9
individual symptoms: pain, fatigue, drowsiness, nausea, anxiety, depression, appetite,
dyspnea, and sense of well-being and one “other” symptom chosen by the patient.33 It is a
simple, validated, self-report tool that assesses the intensity of the most common symptoms
in patients with advanced incurable illness.35,36 For this study, the “other” symptoms item
was replaced by two items rating insomnia and constipation, which were graded using the
same 0-10 scale. Since no time window is stipulated on the ESAS form, we added
instructions that symptoms were to be rated based on the previous 24-hour period.
The FAMCARE is a 20-item scale that measures satisfaction with information-
giving, availability of care, psychological care and physical patient care in patients with
advanced cancer.34,37 Although it is usually completed by the closest family member, it has
also been completed by patients themselves;38 we modified it for patient completion and
used 17 of the 20 items. We chose this measure because it was specifically designed for the

16
evaluation of palliative care,34 and has been validated for outpatients with advanced
cancer.34,37
The Charlson Comorbidity Index (CCI) generates an age-adjusted weighted score
based on the presence of various medical illnesses;39 it has good reliability and validity, is
often used for chart review,40 and is the most commonly used measure of comorbidity for
cancer patients.40
Analyses
Our target sample size of 147 was calculated in advance using a two-sided significance
value of 0.05; power of 0.8; a minimally important difference of 5 points (6%) on the EDS;
a standard deviation of 17.9 based on previous research using this measure in the outpatient
palliative care population;7,41 and allowing for 30% drop-out at one month. A minimum
change of 5-10% has been found to be clinically significant for symptom and quality of life
analyses.42-45
The ESAS distress score (EDS) was calculated by summing the nine usual symptom
intensity scores, excluding insomnia and constipation; the Total Distress Score (TDS) was
the sum of all eleven symptom intensity scores.33 Both scores were prorated as long as more
than 50% of items were completed (5 for the EDS and 6 for the TDS), as has been
suggested for quality of life scales.46,47 Prorated scores were calculated by summing the
individual scores, multiplying by the number of possible items (9 and 11, respectively), and
dividing by the total number of items completed.
The primary outcomes were the EDS and the FAMCARE total score; the individual
symptom scores and TDS were secondary outcomes. For TDS, EDS, individual symptoms
and FAMCARE, the statistical significance of the differences between scores at baseline,

17
and scores at one week and one month, was assessed using paired t-tests. Follow-up
completed at one week was considered acceptable for analysis if conducted between 6 and
14 days following completion of the baseline measures; for one month, a 25 to 45 day
interval was considered acceptable.
An exploratory analysis compared the proportions of patients with individual
symptom scores that improved (decrease of ≥1 point for that symptom), were maintained
(decrease or increase of <1 point) or deteriorated (increase of ≥1 point) at the one-week and
one-month time points. Such analyses have been encouraged and used in trials with quality
of life or symptom control as the primary endpoint.48-50 Further exploratory analyses were
performed for patients at one week to determine proportions improving by ≥1 (small clinical
change)44,49 or ≥2 points (moderate clinical change)44,49 within subgroups according to
baseline severity.
Efficacy and feasibility criteria
Recruitment of patients at the time of initial consultation in the palliative care clinic was
deemed feasible if a recruitment rate of at least 60% was achieved. Target completion of
measures at one week and one month was at least 60% for each time interval. Determination
of efficacy was based on statistically significant change in the primary end points (EDS and
overall FAMCARE score) at one week or one month. Clinical efficacy was evaluated for
individual symptoms and defined as an improvement in ESAS score by at least one unit in
at least 40% of patients for that symptom.

18
RESULTS
Patient Characteristics
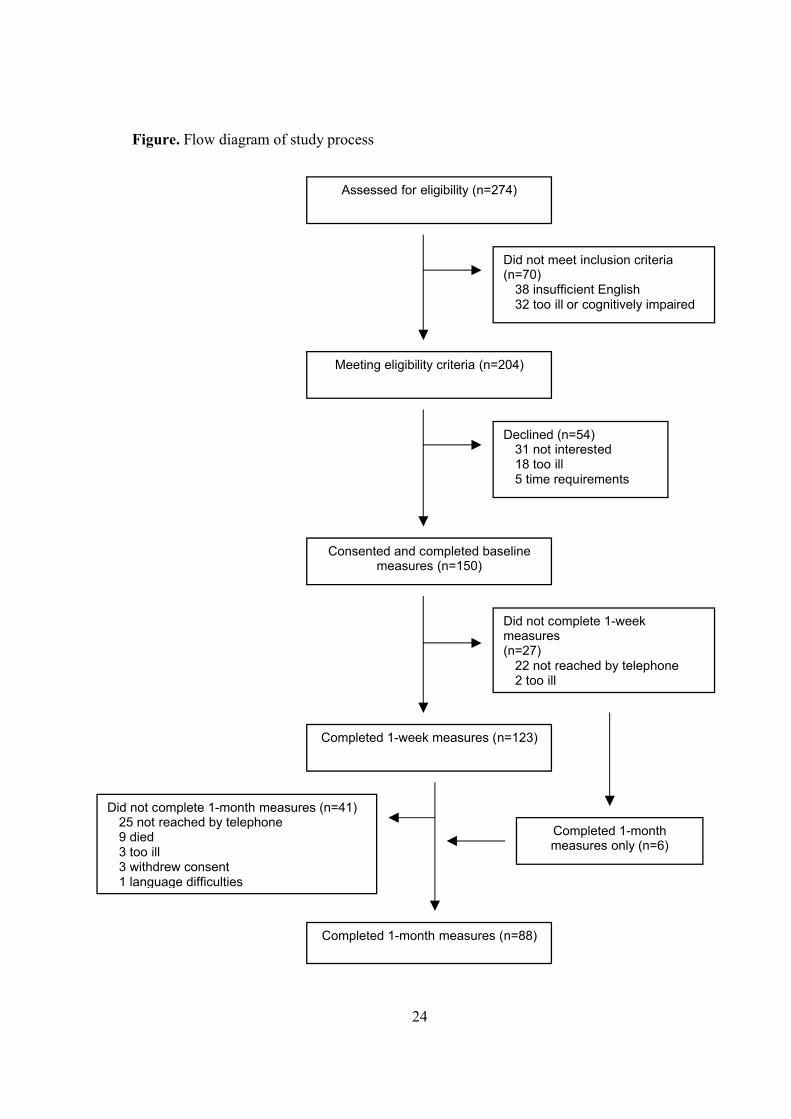
Between 5 July 2006 and 5 April 2007 (9 months), 204 patients were approached, of whom
150 consented (74% recruitment); 31 (58%) of those who declined were not interested, 18
(33%) were too ill, and 5 (9%) cited time requirements (Figure). Baseline characteristics of
participants and non-participants are shown in Table 1. Non-participants were older than
participants (median 67 vs 60 years, P=0.07) but had a similar gender distribution. The
mean CCI score for participants was 0.43 (median 0; range, 0-6). The most prevalent
coexisting medical diagnoses were hypertension (n=40) and diabetes (n=15); psychiatric
diagnoses included depression (n=5), bipolar disorder (n=1), panic disorder (n=1) and
paranoid disorder (n=1). Referrals to the OPCC were made by medical oncologists (n=106,
71%), radiation oncologists (n=32, 21%), surgical oncologists (n=5, 3%) or psychiatrists
(n=7, 5%) for management of pain (n=48, 32%), other symptoms (n=43, 29%), or end-of-
life planning (n=59, 39%).
Retention of participants was 82% (123/150) at one week and 58% (88/150) at one
month (Figure). Interventions initiated by the palliative care team are described in Table 2.
Of 150 participants, 106 continued follow-up in the OPCC after the initial consultation. The
median time interval between the initial visit and the follow-up visit was 21 days (range 4-
388 days).
Symptom control
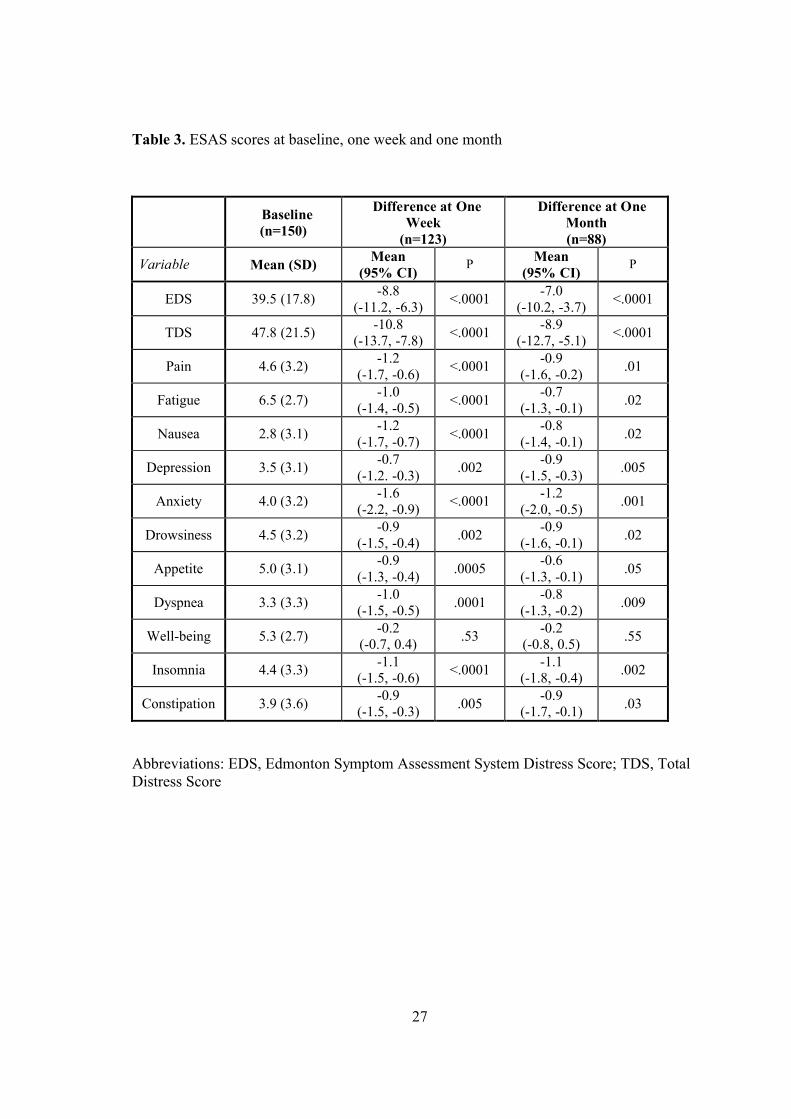
At baseline, the mean EDS was 39.5 and the mean TDS was 47.8 (Table 3). In the 123
patients with one-week follow-up data, there was a mean improvement in EDS of 8.8
(9.8%; P<.0001) and in TDS of 10.8 (9.8%; P<.0001). Statistically significant

19
improvements occurred for all symptoms except well-being, including pain, fatigue, nausea,
anxiety, dyspnea and insomnia (all P≤.0001), as well as depression, drowsiness and
constipation (all P≤.002). More than 40% of the 150 patients enrolled had a reduction of
symptom score by at least one point at one week for pain, fatigue, anxiety and insomnia
(Table 4), and more than 60% of those scoring 8-10/10 had an improvement of at least 1
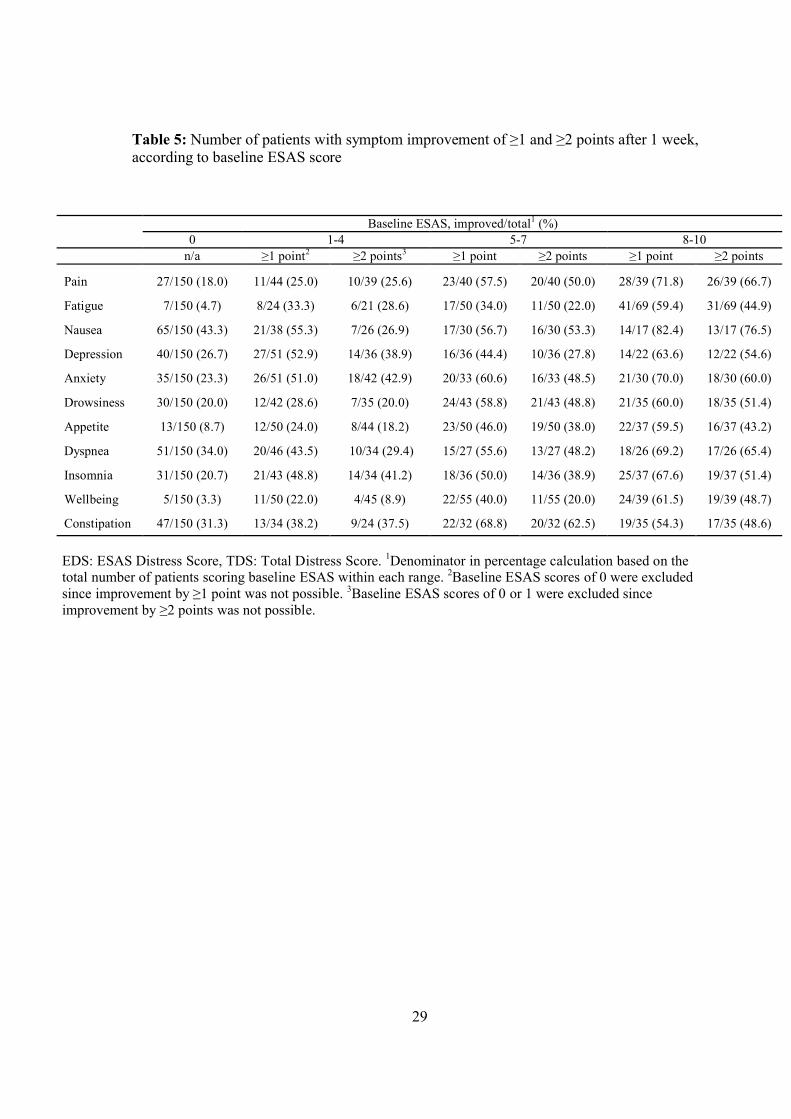
point for all symptoms except fatigue, appetite and constipation (Table 5).
In the 88 patients who were evaluable at one month, there was a significant
improvement in TDS (-8.9, P<.0001) and EDS (-7.0, P<.0001) and statistically significant
improvement in symptom control for anxiety, insomnia, dyspnea, depression and pain
(Table 3). However, the attrition at this time point was greater than 40%, and less than 40%
of the 150 patients enrolled had a reduction of any symptom score by at least one point
(Table 4).
To investigate whether loss to follow-up was related to symptom severity, we
compared baseline EDS of patients who completed assessments at one week (n=123) and
those who did not (n=27). Those patients who completed questionnaires at one week had a
higher (worse) baseline EDS than those who did not (40.9 vs 33.1, P=.04). We also
compared ESAS scores at one week for those completing questionnaires at one month
(n=82) and those who did not (n=41), which revealed no significant difference (37.0 vs
39.5, P=.52). The above analyses were repeated for ECOG score. There was no significant
trend for difference in baseline performance status between those who were missing, or not,
at one week (Cochran-Armitage trend test: P=.09), and no trend for difference in
performance status at one week between those who were or were not missing at one month
(P=.2).
20
Patient satisfaction
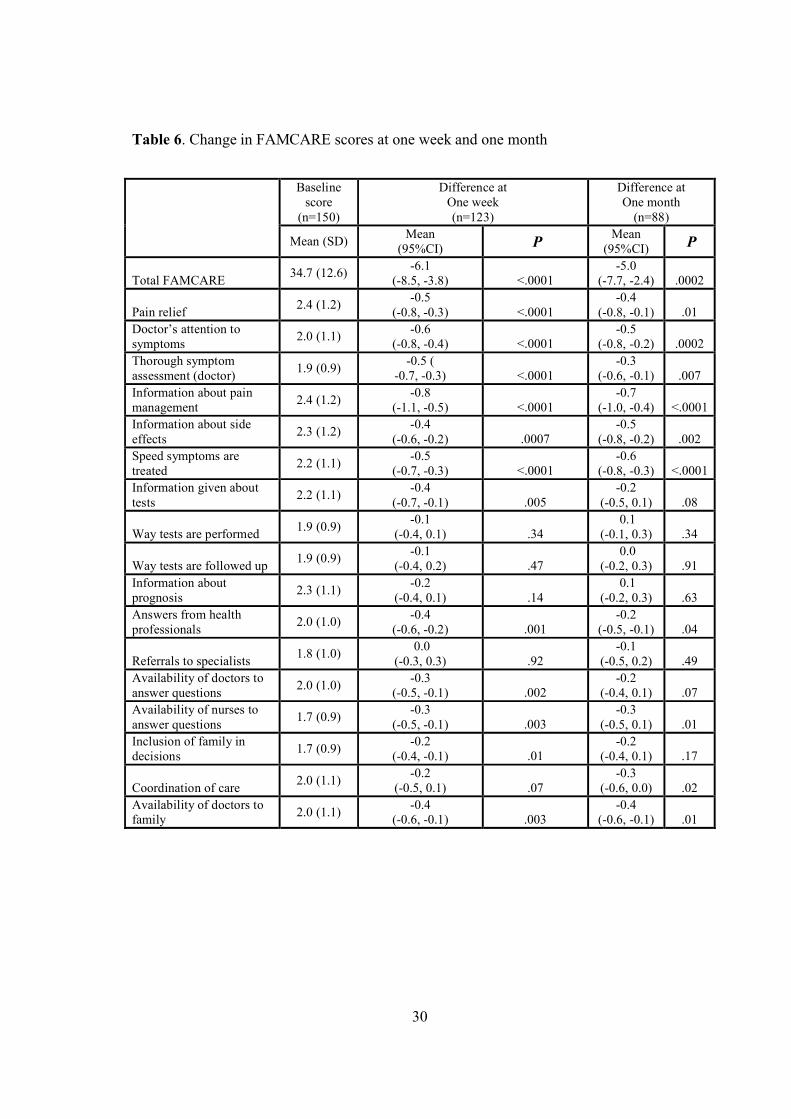
The mean baseline total FAMCARE score was 34.7 (Table 6), with a mean improvement
score of 6.1 (P<.0001) at one week, and 5.0 at one month (P=.0002). FAMCARE domains
that showed the greatest improvement were “Information given about how to manage pain”,
“Doctor’s attention to symptoms”, “Pain relief”, “How thoroughly the doctor assesses
symptoms” and “Speed with which symptoms are treated” (all P<.0001).
DISCUSSION
The primary objective of our study was to assess the efficacy of an outpatient palliative
oncology clinic for improvement of symptom control and satisfaction with care. One week
after the palliative care consultation, there was a 10% improvement in overall symptom
control, including statistically significant improvements in all ten individual symptoms
assessed, which were sustained at one month. Although there is no information on clinically
significant improvement for the ESAS Distress Score, recent reviews have concluded that
the minimal clinically important difference for symptom and quality of life instruments is 5-
10%,43,45 suggesting that the observed improvement was also clinically significant. The
overall symptom improvement is remarkable, since physical symptoms tend to worsen as
death approaches,41,51 and the patients were not selected for symptom prevalence or
severity. The improvements demonstrated are also consistent with results of studies
assessing outpatient palliative care retrospectively.6,7
There was also significant improvement in patient satisfaction at both one week and
one month. Satisfaction with palliative care is related to other constructs such as quality of
life52 and quality of death,53 but is a distinct concept that includes accessibility and
coordination, competence in symptom management, communication and education,

21
emotional support and personalization of care, and support of patients’ needs and decision-
making.54 The specific items that improved are those relating directly to the purpose of the
palliative care clinic, such as pain and symptom relief, thoroughness of assessment, and
information about pain management and side effects. The FAMCARE scale was specifically
developed to measure satisfaction with palliative cancer care, and is generally administered
to family members one month after the death of the patient.55,56 However, there is risk of
recall bias with this method,57 perceptions of care may be influenced by grief,54 grieving
families may be difficult to contact, and the patient’s perception is not addressed. Other
studies have used the FAMCARE prospectively58,59 and in patients.38 The improved patient
satisfaction in the outpatient setting using the FAMCARE in the current study indicates that
this measure is promising for randomized trials.
Secondary objectives for our study included assessment of feasibility of recruitment
and follow-up. Our recruitment rate of 75% shows that it is possible to recruit patients at
their initial visit to the palliative care clinic, and compares favorably to another palliative
medicine feasibility study with 69.4% participation of outpatients.60 Similar to the latter
study,60 patients who did not participate in our study were slightly older and more
symptomatic than non-participants, suggesting possible recruitment bias, although these
differences were not statistically significant.
We had hoped to minimize attrition by keeping measures short and administering
follow-up measures by telephone. We achieved our feasibility target at one week but not at
one month. Attrition is one of the most significant problems in palliative care studies,18,29,61
with usual attrition rates of approximately 40% for randomized trials.18 This may result in
bias, since patients who are retained are likely to be those with better outcomes. However, a
study evaluating attrition in a palliative care setting found that drop-out was associated with

22
higher initial symptomatology but not with diminishing symptom control.61 In our study,
those who did not complete questionnaires at one week actually had less severe
symptomatology at baseline. This suggests that some patients may have dropped out not
because of poor clinical status, but because they had few symptoms to begin with and did
not perceive a symptom follow-up study to be relevant to their situation.
Another secondary objective of our study was to explore the responsiveness of
specific symptoms to the intervention. The individual symptoms that showed both a mean
improvement of at least one point, and for which at least 40% of patients improved by this
amount, were pain, fatigue, anxiety and insomnia. For nausea and dyspnea there was a mean
improvement of at least one point, but 43% and 34% of patients, respectively, rated these
symptoms as 0/10 at baseline and thus could not improve further. At high levels of symptom
severity, there was substantial improvement in the majority of patients for most symptoms,
whereas at low levels of severity less than half of patients improved. These results are
consistent with results from another study, which found that those patients with the worst
symptom control had the greatest improvement after palliative care intervention.51 While
these results suggest that it would be useful to have entry criteria for symptom severity, the
purpose of this study was to assess the efficacy of the palliative care clinic for all patients
referred, regardless of reason for referral or symptom severity. The baseline mean EDS of
39.5 is similar to symptom burden previously documented in outpatient palliative care
settings,6,7,60 suggesting generalizability of our results.
In conclusion, the results of this phase II study demonstrate feasibility of
recruitment, and efficacy of symptom control and patient satisfaction with care after a
palliative care clinic intervention. To keep assessments brief, we did not assess health-
related quality of life or outcomes in caregivers. We are currently conducting a randomized

23
controlled trial to assess the effectiveness of an early palliative care intervention on
symptom control, satisfaction and quality of life in patients and their caregivers.
24
Figure. Flow diagram of study process
Assessed for eligibility (n=274)
Did not meet inclusion criteria (n=70)
38 insufficient English 32 too ill or cognitively impaired
Meeting eligibility criteria (n=204)
Consented and completed baseline measures (n=150)
Declined (n=54)31 not interested18 too ill5 time requirements
Did not complete 1-week measures (n=27)
22 not reached by telephone2 too ill
Completed 1-week measures (n=123)
Completed 1-month measures only (n=6)
Completed 1-month measures (n=88)
Did not complete 1-month measures (n=41)25 not reached by telephone9 died3 too ill3 withdrew consent1 language difficulties

25
Table 1. Baseline characteristics of participants and non-participants
Participants(n=150)
Non-participants(n=54)
P
Characteristic No. % No. %Gender 1.00 Male 76 51 27 50 Female 74 49 27 50Age, median (range) 60 (31-90) 67 (23-87) 0.07Primary Site 0.33 Gastrointestinal 50 33 14 26 Breast 27 18 4 7 Lung 22 15 12 22 Head and Neck 10 7 3 6 Brain 8 5 3 6 Gynecological 8 5 6 11 Skin 8 5 1 2 Genitourinary 7 5 5 9 Hematological 5 3 2 4 Unknown primary 2 1 1 2 Other 3 2 3 5ECOG scorea
0 9 6
1 53 35
2 51 34
3 35 23
4 2 2
ESAS Distress Score, mean (SD)
39.5 (17.8) 42.8 (18.0) 0.25
Total Distress Score,mean (SD)
47.8 (21.5) 52.8 (20.9) 0.16
aECOG score not available for non-participantsAbbreviations: ECOG, Eastern Cooperative Oncology Group.

26
Table 2. Interventions in Oncology Palliative Care Clinic
Intervention Number (%)Prescribed new medication 99 (66.0)Change in existing medication 51 (34.0)Medication discontinued 27 (18.0)Referrals Social work 44 (29.3) Psychology/psychiatry 15 (10.0) Physical/occupational therapy 18 (12.0) Home nursing services 70 (46.7) Home palliative care physician 56 (37.3) Other services (dietician, medical/radiation oncology, ophthalmology, interventional radiology, respiratory therapy, support groups)
16 (10.7)
27
Table 3. ESAS scores at baseline, one week and one month
Baseline (n=150)
Difference at One Week
(n=123)
Difference at One Month(n=88)
Variable Mean (SD)Mean
(95% CI)P
Mean(95% CI)
P
EDS 39.5 (17.8)-8.8
(-11.2, -6.3)<.0001
-7.0(-10.2, -3.7)
<.0001
TDS 47.8 (21.5)-10.8
(-13.7, -7.8)<.0001
-8.9(-12.7, -5.1)
<.0001
Pain 4.6 (3.2)-1.2
(-1.7, -0.6)<.0001
-0.9(-1.6, -0.2)
.01
Fatigue 6.5 (2.7)-1.0
(-1.4, -0.5)<.0001
-0.7(-1.3, -0.1)
.02
Nausea 2.8 (3.1)-1.2
(-1.7, -0.7)<.0001
-0.8(-1.4, -0.1)
.02
Depression 3.5 (3.1)-0.7
(-1.2. -0.3).002
-0.9(-1.5, -0.3)
.005
Anxiety 4.0 (3.2)-1.6
(-2.2, -0.9)<.0001
-1.2(-2.0, -0.5)
.001
Drowsiness 4.5 (3.2)-0.9
(-1.5, -0.4).002
-0.9(-1.6, -0.1)
.02
Appetite 5.0 (3.1)-0.9
(-1.3, -0.4).0005
-0.6(-1.3, -0.1)
.05
Dyspnea 3.3 (3.3)-1.0
(-1.5, -0.5).0001
-0.8(-1.3, -0.2)
.009
Well-being 5.3 (2.7)-0.2
(-0.7, 0.4).53
-0.2(-0.8, 0.5)
.55
Insomnia 4.4 (3.3)-1.1
(-1.5, -0.6)<.0001
-1.1(-1.8, -0.4)
.002
Constipation 3.9 (3.6)-0.9
(-1.5, -0.3).005
-0.9(-1.7, -0.1)
.03
Abbreviations: EDS, Edmonton Symptom Assessment System Distress Score; TDS, Total Distress Score

28
Table 4. Proportions of patients with change in symptoms by at least one point
Abbreviations: N/A: not assessable
One Week (n=150)No. (%)
One Month (n=150)No. (%)
Variable
Improve Stable Deteriorate N/A Improve Stable Deteriorate N/A
Pain 62 (41) 33 (22) 28 (19) 27 (18) 49 (33) 17 (11) 22 (15) 62 (41)
Fatigue 66 (44) 29 (19) 28 (19) 27 (18) 45 (30) 16 (11) 26 (17) 63 (42)
Nausea 52 (35) 52 (35) 19 (13) 27 (18) 37 (25) 29 (19) 21 (14) 63 (42)
Depression 57 (38) 36 (24) 27 (18) 30 (20) 40 (27) 23 (15) 21 (14) 66 (44)
Anxiety 69 (46) 29 (19) 22 (15) 30 (20) 44 (29) 22 (15) 18 (12) 66 (44)
Drowsiness 57 (38) 29 (19) 37 (25) 27 (18) 44 (29) 17 (11) 26 (17) 63 (42)
Appetite 57 (38) 38 (25) 28 (19) 27 (18) 42 (28) 17 (11) 26 (17) 65 (43)
Dyspnea 53 (35) 47 (31) 23 (15) 27 (18) 40 (27) 28 (19) 19 (13) 63 (42)
Well-being 57 (38) 21 (14) 41 (27) 31 (21) 38 (25) 17 (11) 31 (21) 64 (43)
Insomnia 64 (43) 34 (23) 22 (15) 30 (20) 44 (29) 15 (10) 25 (17) 66 (44)
Constipation 54 (36) 40 (27) 24 (16) 32 (21) 43 (29) 21 (14) 21 (14) 65 (43)
29
Table 5: Number of patients with symptom improvement of ≥1 and ≥2 points after 1 week, according to baseline ESAS score
Baseline ESAS, improved/total1 (%)0 1-4 5-7 8-10
n/a ≥1 point2 ≥2 points3 ≥1 point ≥2 points ≥1 point ≥2 points
Pain 27/150 (18.0) 11/44 (25.0) 10/39 (25.6) 23/40 (57.5) 20/40 (50.0) 28/39 (71.8) 26/39 (66.7)
Fatigue 7/150 (4.7) 8/24 (33.3) 6/21 (28.6) 17/50 (34.0) 11/50 (22.0) 41/69 (59.4) 31/69 (44.9)
Nausea 65/150 (43.3) 21/38 (55.3) 7/26 (26.9) 17/30 (56.7) 16/30 (53.3) 14/17 (82.4) 13/17 (76.5)
Depression 40/150 (26.7) 27/51 (52.9) 14/36 (38.9) 16/36 (44.4) 10/36 (27.8) 14/22 (63.6) 12/22 (54.6)
Anxiety 35/150 (23.3) 26/51 (51.0) 18/42 (42.9) 20/33 (60.6) 16/33 (48.5) 21/30 (70.0) 18/30 (60.0)
Drowsiness 30/150 (20.0) 12/42 (28.6) 7/35 (20.0) 24/43 (58.8) 21/43 (48.8) 21/35 (60.0) 18/35 (51.4)
Appetite 13/150 (8.7) 12/50 (24.0) 8/44 (18.2) 23/50 (46.0) 19/50 (38.0) 22/37 (59.5) 16/37 (43.2)
Dyspnea 51/150 (34.0) 20/46 (43.5) 10/34 (29.4) 15/27 (55.6) 13/27 (48.2) 18/26 (69.2) 17/26 (65.4)
Insomnia 31/150 (20.7) 21/43 (48.8) 14/34 (41.2) 18/36 (50.0) 14/36 (38.9) 25/37 (67.6) 19/37 (51.4)
Wellbeing 5/150 (3.3) 11/50 (22.0) 4/45 (8.9) 22/55 (40.0) 11/55 (20.0) 24/39 (61.5) 19/39 (48.7)
Constipation 47/150 (31.3) 13/34 (38.2) 9/24 (37.5) 22/32 (68.8) 20/32 (62.5) 19/35 (54.3) 17/35 (48.6)
EDS: ESAS Distress Score, TDS: Total Distress Score. 1Denominator in percentage calculation based on the total number of patients scoring baseline ESAS within each range. 2Baseline ESAS scores of 0 were excluded since improvement by ≥1 point was not possible. 3Baseline ESAS scores of 0 or 1 were excluded since improvement by ≥2 points was not possible.
30
Table 6. Change in FAMCARE scores at one week and one month
Baseline score
(n=150)
Difference at One week(n=123)
Difference at One month
(n=88)
Mean (SD)Mean
(95%CI) PMean
(95%CI) P
Total FAMCARE34.7 (12.6)
-6.1 (-8.5, -3.8) <.0001
-5.0 (-7.7, -2.4) .0002
Pain relief2.4 (1.2)
-0.5 (-0.8, -0.3) <.0001
-0.4 (-0.8, -0.1) .01
Doctor’s attention to symptoms
2.0 (1.1)-0.6
(-0.8, -0.4) <.0001-0.5
(-0.8, -0.2) .0002Thorough symptom assessment (doctor)
1.9 (0.9)-0.5 (
-0.7, -0.3) <.0001-0.3
(-0.6, -0.1) .007Information about pain management
2.4 (1.2)-0.8
(-1.1, -0.5) <.0001-0.7
(-1.0, -0.4) <.0001Information about side effects
2.3 (1.2)-0.4
(-0.6, -0.2) .0007-0.5
(-0.8, -0.2) .002Speed symptoms are treated
2.2 (1.1)-0.5
(-0.7, -0.3) <.0001-0.6
(-0.8, -0.3) <.0001Information given about tests
2.2 (1.1)-0.4
(-0.7, -0.1) .005-0.2
(-0.5, 0.1) .08
Way tests are performed1.9 (0.9)
-0.1 (-0.4, 0.1) .34
0.1 (-0.1, 0.3) .34
Way tests are followed up1.9 (0.9)
-0.1 (-0.4, 0.2) .47
0.0 (-0.2, 0.3) .91
Information about prognosis
2.3 (1.1)-0.2
(-0.4, 0.1) .14 0.1
(-0.2, 0.3) .63Answers from health professionals
2.0 (1.0)-0.4
(-0.6, -0.2) .001-0.2
(-0.5, -0.1) .04
Referrals to specialists1.8 (1.0)
0.0 (-0.3, 0.3) .92
-0.1 (-0.5, 0.2) .49
Availability of doctors to answer questions
2.0 (1.0)-0.3
(-0.5, -0.1) .002-0.2
(-0.4, 0.1) .07Availability of nurses to answer questions
1.7 (0.9)-0.3
(-0.5, -0.1) .003-0.3
(-0.5, 0.1) .01Inclusion of family in decisions
1.7 (0.9)-0.2
(-0.4, -0.1) .01-0.2
(-0.4, 0.1) .17
Coordination of care2.0 (1.1)
-0.2 (-0.5, 0.1) .07
-0.3 (-0.6, 0.0) .02
Availability of doctors to family
2.0 (1.1)-0.4
(-0.6, -0.1) .003-0.4
(-0.6, -0.1) .01

31
Chapter Five
Predictors of symptom severity and response in
patients with metastatic cancer
Published previously as:
Zimmermann, C., Burman, D., Follwell, M., Wakimoto, K., Seccareccia, D., Bryson, J., Le, L., Rodin, G. Predictors of symptom severity and response in
patients with metastatic cancer. Am J Hosp Palliat Med. 2009 Sep 25 [epub ahead of print]

32
ABSTRACT
We examined determinants of symptom severity and response to treatment among 150
cancer patients participating in a Phase II trial of a palliative care team intervention.
Baseline ESAS Distress Score (EDS), Total Distress Score (TDS) and individual symptoms
were compared according to gender, age, cancer site and performance status. Univariate and
multivariate analyses assessed predictors of EDS and TDS improvement at one week.
Women had worse baseline EDS (p=0.003) and TDS (p=0.005), particularly anxiety and
appetite. Performance status was inversely associated with EDS, TDS, well-being, appetite
and fatigue (all p<0.005). Symptom improvement was independently predicted by worse
baseline EDS score and female gender. Performance status, gender and baseline symptom
severity should be accounted for in trials of palliative care interventions; inclusion criteria
based on symptom severity should also be considered.
Keywords: palliative care; symptom; gender; Edmonton Symptom Assessment Scale;
cancer; performance status

33
INTRODUCTION
Patients with metastatic cancer experience multiple symptoms, which may be alleviated by
a palliative care intervention. Numerous studies in both inpatient and outpatient settings
have documented the symptom burden of patients with advanced cancer.1 Randomized and
non-randomized studies have also assessed the effectiveness of palliative care interventions
on symptom control.6-9,11,62,63 However, not many studies have examined predictors of
symptom prevalence or severity in patients with advanced cancer,64-67 and only one of these
assessed predictors of symptom response to palliative treatment.64 Such information is
useful both for the development of palliative cancer care services and in the planning of
randomized clinical trials assessing the effectiveness of specialized palliative care for
symptom control.
We have recently completed a phase II study of an outpatient palliative care clinic
intervention in patients with metastatic cancer,68 in which we measured symptom severity
and patient satisfaction one week and one month after the intervention. There were
improvements in overall symptom distress and in the individual symptoms of pain, fatigue,
nausea, depression, anxiety, drowsiness, appetite, insomnia and constipation at one week
and at one month, as measured by the Edmonton Symptom Assessment System (ESAS).33
Similarly, there was a significant improvement in satisfaction with care, as measured by the
FAMCARE scale,34 at one week and one month.
In the current study, we used the same dataset to examine associations of symptom
burden and response to treatment with demographic and disease-related characteristics.
Based on previous research in advanced cancer populations,65 our primary hypotheses were
that younger patients, women, and those with worse performance status would have greater
symptom burden. Secondary exploratory analyses were carried out to examine differences

34
for individual symptoms if the outcomes of primary hypotheses were significant. We also
hypothesized that patients who had worse symptom control at baseline would have a greater
improvement in their symptoms. To improve the power of our analyses, we limited these to
outcomes of overall symptom distress and individual symptoms at baseline, and the
response of symptoms to the intervention at one week.
METHODS
Study participants
The methods have been described previously.68 Participants were recruited upon initial
referral to the Oncology Palliative Care Clinic (OPCC) at Princess Margaret Hospital
(PMH), a cancer center in Toronto, Canada. All newly referred patients who were assessed
in the palliative care clinic were eligible, provided that they had metastatic cancer, were at
least 18 years old, and were well enough and able to speak and read English sufficiently to
provide informed consent and complete questionnaires. Approval for this study was granted
from the University Health Network Research Ethics Board, and all patients provided
written, informed consent.
Palliative care clinic intervention
Patients are referred to the OPCC by their medical, radiation or surgical oncologist, for pain
management, treatment of other symptoms and palliative care planning.23,31 The palliative
care consultation consists of an assessment by both a palliative care Registered Nurse (RN)
Case Manager and a palliative care physician;23 a palliative care social worker and/or
psychiatrist are involved as necessary. Additional referrals may be made to other members
of the interdisciplinary team, including psychologists, spiritual care providers, dieticians,

35
wound care specialists, physiotherapists, and occupational therapists. Recommendations are
made for symptom and palliative care treatment, education, counseling, and home support.
Outreach referrals to home care and community hospice and palliative care agencies are
made as appropriate. All clinic patients have access to a 24-hour on-call service staffed by
palliative care physicians.
Study procedures
Patients were recruited in the waiting area for the OPCC. Consenting patients were
interviewed briefly by research staff to evaluate Eastern Cooperative Oncology Group
(ECOG) performance status,32 and completed the ESAS33 and FAMCARE measures.34 Only
ESAS results are presented in this paper.
The ESAS is a 0-10 numerical scale (0=best, 10=worst) for 9 individual symptoms:
pain, fatigue, drowsiness, nausea, anxiety, depression, appetite, dyspnea, and sense of well-
being and one “other” symptom chosen by the patient.33 It is a simple, validated tool that is
completed by the patient and allows for screening and monitoring for the most common
symptoms in patients with advanced incurable illness.35,69 For this study, we substituted the
“other” item with two symptoms (insomnia and constipation), which were graded using the
same 0-10 scale. Since no time window is stipulated on the ESAS form, we also added
instructions at the beginning of the form that symptoms were to be rated based on the
previous 24-hour period.
The ESAS is normally completed by all patients attending the OPCC, with the
assistance of the RN Case Manager. However, for this study research staff administered the
ESAS, so that it represented a true baseline measure before any contact with the palliative
care team. The patient was then given a copy of the ESAS, which was used in the clinical
36
assessment by the nurse and physician, as is the usual practice in the OPCC.23 After the
completion of baseline measures, research staff completed the chart review to extract data
including age and tumor type. Research staff telephoned patients one week and one month
following the initial visit, and readministered the ESAS and FAMCARE by telephone
interview.
Analyses
The ESAS distress score (EDS) was calculated using the nine usual symptom scores,
excluding insomnia and constipation.33 If there were less than 5 missing items, the EDS was
considered evaluable, and was calculated by summing the individual scores; multiplying by
the number of possible items (nine); and dividing by the total number of items completed.
The Total Distress Score (TDS) was calculated using all eleven symptom scores. The TDS
was considered evaluable if there were less than 6 missing items, and was calculated in the
same way as the EDS, but using eleven as the number of possible items. Follow-up
completed at one week was considered acceptable for analysis if conducted between six and
14 days following completion of the baseline measures.
Our primary hypotheses relate to overall symptom burden, and secondary analyses
were conducted to assess individual symptoms. Accordingly, baseline EDS and TDS were
compared for the demographic variables, and differences among individual symptoms were
subsequently investigated if the results for EDS and TDS were significant. Due to the
skewness of the individual symptom scores, the Wilcoxon Mann-Whitney test was used for
gender, and the Kruskal-Wallis test for ECOG. In order to explore predictors of
improvement in EDS at one week, univariate analyses were conducted for gender, age,
primary site, and ECOG score using ANOVA and/or student t-tests. Multivariate analysis of
37
covariance (ANCOVA) was carried out to examine the impact of independent predictors on
EDS. Variables with p ≤ 0.10 were kept in the final results. Mean improvement after one
week was compared for each symptom among three categories of baseline scores: 1-4
(mild), 5-7 (moderate) and 8-10 (severe).70
All analyses were performed using SAS v9.1 (SAS Institute, Cary, NC); all reported
p-values are two-sided. We did not adjust the p-values for multiple comparisons so as not to
compound type 2 error in a study that has a relatively small sample size.71 Instead, we
distinguish those p-values that are significant at the p<0.005 level for the 11 individual
symptoms (which is equivalent to a Bonferroni correction) from those that are significant at
the p<0.05 level. All original p-values are reported in the text to promote clarity.
RESULTS
Study sample characteristics
Between 5 July 2006 and 5 April 2007, 150 patients were entered into the trial, of whom
123 completed follow-up measures at one week by telephone (one patient had died and a
further 26 withdrew). Of the 150 patients, the median age was 60, 51% were female, and
most had primary cancers of gastro-intestinal (33%), breast (18%) or lung (15%) origin.
Performance status was 0 or 1 in 41% of patients, 2 in 34%, and 3 or 4 in 25% (Table 1).
Predictors of baseline symptom burden
Baseline symptom distress scores were higher in women than men (mean TDS: 52.6 vs.
42.9, p=0.005; mean EDS: 43.6 vs. 35.2, p=0.003). The symptoms for which there was the
greatest difference between women and men were anxiety (3.2 vs. 4.8, p=0.002) and
appetite (5.7 vs. 4.3, p=0.004; Table 1). Differences at the p<0.05 level were found for

38
depression (4.1 vs. 2.8, p=0.008), fatigue (mean: 7.0 vs. 6.0, p=0.03), sense of well-being
(5.7 vs. 4.8, p=0.03) and drowsiness (5.0 vs. 3.9, p=0.04); Table 1). However, these were
not significant with Bonferroni correction. There were no significant gender differences for
pain, nausea, dyspnea, insomnia or constipation. The severity of baseline symptoms did not
differ according to age or cancer site (all p>0.09; data not shown). Patients with worse
performance status had significantly worse EDS and TDS (Table 1), and particularly worse
fatigue (p=0.0008), appetite (p=0.0004) and well-being (p=0.0002).
Predictors of improvement in symptoms
Univariate analyses of symptom improvement showed that there was a greater decrease in
EDS for women (mean: 11.9 units vs. 5.3 units in men, p=0.007) and for patients with
higher baseline EDS (p=0.0002; Table 2). In the multivariate analysis, worse baseline EDS
score independently predicted improvement in EDS score (p=0.005), as did gender
(p=0.04); the joint effect of baseline EDS and gender did not predict symptom improvement
over and above their separate effects (p=0.08; Table 2). For all symptoms rated in the 8-10
range at baseline, there was a mean improvement of at least two units, with the greatest
improvements in nausea (mean improvement 4.7 units), anxiety (4.1 units), dyspnea (3.5
units) and pain (3.5 units). In contrast, for patients with a score of 1-4 at baseline, symptoms
stayed approximately the same (Table 3).
DISCUSSION
In a previous paper, we reported on the improvement of overall symptom distress and
individual symptoms after intervention by a palliative care team.68 The purpose of the
current analyses was to determine predictors of symptom severity and improvement. As
39
hypothesized, worse performance status and female gender both predicted baseline
symptom severity; no significant impact was found for patient age. The response of
symptoms to treatment was predicted by baseline symptom severity and also by female
gender. These results have implications for the future design of trials of palliative care
interventions, and for the treatment of patients with advanced cancer.
The relationship between performance status and symptom severity among patients
with cancer is well documented.35,65,72 In our study, this relationship was found particularly
for fatigue, appetite and well-being. In a study in a different population of patients
attending the PMH OPCC,73 we found that these same symptoms were correlated
significantly with time to death, as were drowsiness and dyspnea, which were associated
with performance status at the p<0.05 level in the current study. Another study found that
performance status and the fatigue, appetite and dyspnea items of the ESAS had a
statistically significant impact on the survival of patients after referral for palliative
radiotherapy.74 Thus fatigue, appetite, and dyspnea appear to be specifically associated with
worse performance status and prognosis. Of note, these symptoms still demonstrated a
significant improvement following palliative care intervention,68 and in the current study
symptom improvement was not related to performance status. Thus these symptoms, while
specifically associated with advancing disease, are still amenable to improvement after
intervention by a palliative care team.
Baseline symptom severity was a significant positive predictor of symptom
response. At high levels of distress, there was substantial improvement for all symptoms,
whereas at low levels of distress symptoms stayed relatively stable. These results are
consistent those of Modonesi et al.,51 who found that patients with the worst symptom
control were most likely to have the greatest symptom improvement after admission to a

40
palliative care unit. Although previous randomized trials of palliative care interventions
have tended not to show significant results for symptom control,18 they have also usually
not had entry criteria based on symptom severity. Consideration should be given to
including only patients above a certain symptom threshold in trials of palliative care
interventions where symptom control is the primary outcome.
At baseline, women reported significantly higher symptom burden than men. These
results are consistent with data from studies of the general population75,76 and of patients
with advanced cancer,65 which have shown worse quality of life in women than in men in
the areas of physical and emotional well-being. The worse symptom scores among women
for depression, anxiety, appetite, drowsiness and fatigue, are also consistent with data from
other studies that have shown lower quality of life in women with cancer than in men for
these symptoms. Studies in cancer patients have found either no gender difference for
depression77-80 or higher prevalence in women.81-85 Similar results have been found for
anxiety (one study found no gender difference83, others increased anxiety in women80,84,85)
and fatigue (no gender difference in some studies78,86, with others showing increased fatigue
in women65,67,87-89). Although there have been no studies specifically reporting on
differences in appetite between women and men, there have been studies reporting an
increased prevalence of nausea and vomiting.65,66 It is noteworthy that no studies have
shown a greater prevalence or severity for any of these symptoms in men.
Although women reported worse baseline symptom control, they also had a more
marked response to the intervention. There are few studies that have measured this
association, and one other study measuring pain with the ESAS and the EORTC QLQ-C30
found the opposite gender association, with greater improvement in men than women one
week after referral to a specialist palliative care unit.64 The largest body of literature on

41
gender as a factor influencing treatment response is on depression, but the results have been
conflicting with some studies supporting and others refuting an influence of gender on
response to antidepressants.90 Further studies with larger sample sizes are necessary to
clarify whether there is an independent effect of gender on improvement of symptoms.
A limitation of our study was its small sample size, which may have resulted in lack
of power to detect differences that otherwise might have been statistically significant. For
example, previous studies have documented a difference in symptom severity based on
cancer site,91 but this would require larger numbers of patients in each cancer site than in
our study. Similarly, studies with larger sample sizes have reported a larger symptom
burden and/or worse quality of life in younger than in older patients with cancer.65,84,92
Again the smaller number of patients may have prevented us from showing such a
difference, and the negative findings from our study should be interpreted with caution. In
interpreting gender differences, it is also important to recognize that men and women may
experience symptoms differently93 and a difference in symptom reporting does not
necessarily correspond to an actual difference in symptom perception.94 Qualitative studies
comparing themes in women and men may shed light on what dimensions each gender
considers important in reporting different symptoms.
In conclusion, our study showed that performance status is associated with symptom
severity, but only for specific symptoms that have been associated with prognosis in other
studies. Symptom severity and response were greater in women, though the latter finding
was partly due to more severe baseline symptom severity, which was a strong predictor of
symptom response. Further research is warranted regarding the relationship of gender to
symptom response, using prospective studies with cancers that are not gender specific.
Performance status and gender should be included as covariates in trials of palliative care

42
interventions. To improve sensitivity to change, trials should also consider inclusion criteria
based on intensity of symptoms.

43
TABLES
Table 1: Baseline symptom scores according to gender and performance status [mean (SD)]
Sex Performance Status (ECOG)Male Female 0-1 2 ≥3
N 74 76 62 51 37
EDS 35.2 (16.2) 2 43.6 (18.4) 34.1 (15.6) 2 39.8 (20.5) 47.9 (14.1)
TDS 42.9 (20.0)2 52.6 (21.9) 42.2 (19.9) 2 48.4 (24.3) 56.5 (16.7)
Pain 4.3 (3.0) 4.9 (3.4) 4.1 (3.1) 5.3 (3.4) 4.6 (3.0)
Fatigue 6.0 (2.9)1 7.0 (2.5) 5.7 (2.7) 2 6.4 (2.8) 7.8 (2.2)
Nausea 2.4 (2.9) 3.1 (3.3) 2.3 (2.5) 3.1 (3.5) 3.0 (3.6)
Depression 2.8 (2.6) 1 4.1 (3.3) 3.1 (2.9) 3.6 (3.1) 3.9 (3.2)
Anxiety 3.2 (2.8) 2 4.8 (3.4) 3.4 (2.8) 4.2 (3.5) 4.8 (3.4)
Drowsiness 3.9 (3.0) 1 5.0 (3.3) 4.0 (3.1) 1 4.2 (3.3) 5.6 (3.0)
Appetite 4.3 (2.8) 2 5.7 (3.2) 4.2 (2.6) 2 4.8 (3.3) 6.7 (2.9)
Dyspnea 3.4 (3.1) 3.3 (3.6) 2.8 (3.1) 1 3.0 (3.0) 4.7 (3.8)
Insomnia 4.2 (3.3) 4.5 (3.4) 4.3 (3.2) 4.5 (3.5) 4.3 (3.5)
Well-being 4.8 (2.5) 1 5.7 (2.8) 4.5 (2.5) 2 5.0 (2.7) 6.8 (2.5)
Constipation 3.5 (3.3) 4.3 (4.0) 3.7 (3.6) 4.1 (3.7) 4.1 (3.6)
EDS: ESAS Distress Score, TDS: Total Distress Score. 1 p <0.05 2 p≤0.005

44
Table 2: Univariate and Multivariate Analysis of Predictors for ESAS distress improvement after 1 week
Univariate (n=123) Multivariate
Variable Mean difference (SE) p-value p-value
Sex 0.007 0.04Male -5.4 (1.4)Female -11.9 (1.9)
Age 0.57< 60 yrs -9.5 (1.6)≥ 60 yrs -8.1 (1.9)
Primary site 0.18GI -6.4 (1.9)Breast -12.3 (2.7)Lung -13.2 (4.3)Gyne -4.6 (5.3)GU -14.3 (4.8)Other -6.1 (2.1)
ECOG at baseline 0.160-1 -9.7 (1.5)2 -5.8 (2.2)≥ 3 -11.6 (2.8)
EDS at baseline 0.0002 0.005≤ 30 -1.8 (1.4)31-50 -9.0 (1.7)> 50 -14.5 (2.6)
Sex * baseline EDS 0.08
EDS: ESAS Distress Score, GI: gastrointestinal, Gyne: gynecological, GU: genitourinary
45
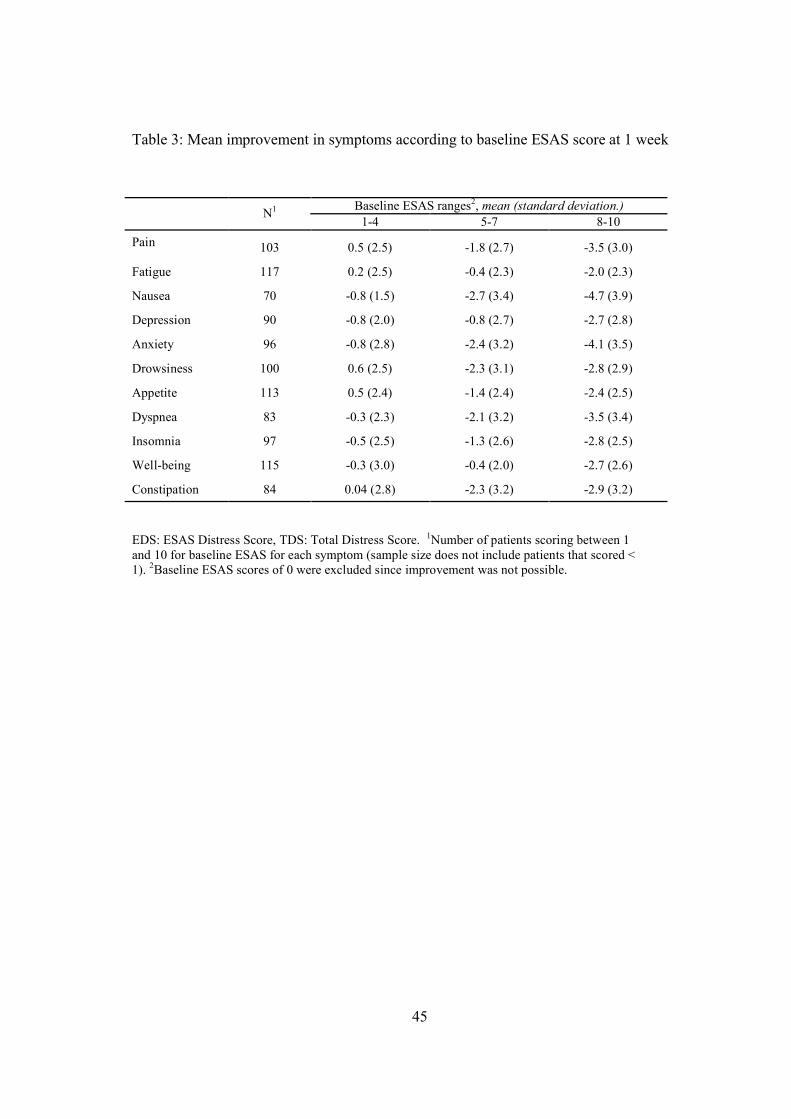
Table 3: Mean improvement in symptoms according to baseline ESAS score at 1 week
Baseline ESAS ranges2, mean (standard deviation.)N1
1-4 5-7 8-10
Pain 103 0.5 (2.5) -1.8 (2.7) -3.5 (3.0)
Fatigue 117 0.2 (2.5) -0.4 (2.3) -2.0 (2.3)
Nausea 70 -0.8 (1.5) -2.7 (3.4) -4.7 (3.9)
Depression 90 -0.8 (2.0) -0.8 (2.7) -2.7 (2.8)
Anxiety 96 -0.8 (2.8) -2.4 (3.2) -4.1 (3.5)
Drowsiness 100 0.6 (2.5) -2.3 (3.1) -2.8 (2.9)
Appetite 113 0.5 (2.4) -1.4 (2.4) -2.4 (2.5)
Dyspnea 83 -0.3 (2.3) -2.1 (3.2) -3.5 (3.4)
Insomnia 97 -0.5 (2.5) -1.3 (2.6) -2.8 (2.5)
Well-being 115 -0.3 (3.0) -0.4 (2.0) -2.7 (2.6)
Constipation 84 0.04 (2.8) -2.3 (3.2) -2.9 (3.2)
EDS: ESAS Distress Score, TDS: Total Distress Score. 1Number of patients scoring between 1 and 10 for baseline ESAS for each symptom (sample size does not include patients that scored < 1). 2Baseline ESAS scores of 0 were excluded since improvement was not possible.

46
Chapter Six
Design and methodology for a randomized controlled trial of a palliative
care intervention for patients with metastatic cancer

47
RATIONALE
Introduction
Approximately 73,800 deaths from cancer occured in Canada in 2008, of which 27,300
were in Ontario.95 The complex symptom and psychosocial needs of patients with advanced
cancer occur not only at the end of life, but may arise many months before the patient’s
death.1-3,96 Correspondingly, the World Health Organization states that palliative care is
relevant “early in the course of illness, in conjunction with other therapies that are intended
to prolong life”,97 and the Canadian Hospice and Palliative Care Association posits that
palliative care “should be available to patients and families throughout the illness”.98
However, referral to palliative care teams for most cancer patients currently occurs in the
last two months of life or not at all,99-102 and no prospective study has assessed the
effectiveness of early versus routine palliative care intervention.
We are currently conducting a cluster randomized controlled trial of early versus
routine palliative care intervention in patients with advanced cancer. Twenty-four medical
oncology clinics at Princess Margaret Hospital, Toronto, have been randomized either to
immediate consultation and follow-up by a palliative care team or to conventional cancer
care. Consenting patients and their primary caregivers complete measures of quality of life
and satisfaction with care at monthly intervals for 4 months. We present results to date and a
plan for completing this trial. At the time of the analyses conducted below, we had recruited
245 patients (114 intervention and 131 controls) and 109 caregivers (52 intervention and 57
controls).

48
Research Hypothesis: Compared to conventional cancer care, early intervention (at a
prognosis of >6 months) of a palliative care team in patients with metastatic cancer will be
associated with (i) better patient health related quality of life (HRQL) (primary outcome);
(ii) greater patient and caregiver satisfaction with care; (iii) better symptom control; (iv)
improved communication with health care providers; and (v) improved caregiver quality of
life (ii-v are secondary outcomes).
Background
Despite increasing advocacy for the early integration of palliative care into mainstream
cancer care, no randomized controlled trials (RCTs) have tested this practice. No completed
Canadian RCT has investigated the effectiveness of a palliative care team intervention, and
no previous RCT worldwide has specifically assessed early palliative care intervention.
We recently conducted a systematic review of 22 RCTs from 1984-2007 evaluating
the effectiveness of specialized palliative care, which was published in the Journal of the
American Medical Association.18 All but three studies included patients with cancer, and
eleven studied almost exclusively this population.10,11,17,63,103-109 Most were conducted in the
United States, and there was only one Canadian study,105 which was not completed due to
methodological difficulties. Palliative care was defined broadly and not all studies evaluated
a palliative care team, with interventions including a coordinating service,106,110,111 a nursing
intervention10,108,112,113 or counselling.109,114 Only four10,11,30,115 of thirteen studies assessing
HRQL and one9 of thirteen assessing symptoms had significant findings, although most
lacked statistical power, and HRQL measures were not specific for terminally ill patients.
Patient and caregiver satisfaction were each measured in ten studies, with improvements in
four10,17,110,116 and seven,17,30,104,111,112,117,118 respectively. Our review and others27,29,119,120
49
have identified recurrent methodological problems, which may account for the failure of
these studies to show a benefit in terms of HRQL.
Recent pilot studies have assessed the efficacy of early outpatient palliative care. In
one U.S. study,13 patients with advanced non-small cell lung cancer were assigned, within 8
weeks of diagnosis, to integrated care from Palliative Care and Oncology. Fifty patients
were enrolled, although the recruitment rate was not documented. Feasibility was
confirmed, based on the criteria of 88% of patients completing at least 50% of their monthly
HRQL assessments and scheduled visits. Another U.S. pilot study121 investigated the effect
of a palliative care team intervention on HRQL of patients accrued to Phase I or II
chemotherapy trials. The study was non-randomized with patients assigned to palliative
team intervention or control based on place of residence. Data were collected monthly for 4
months; 64 patients were enrolled and complete results were obtained for 59 (92%). The
trend to greater improvement in FACT-G122 HRQL scores in the intervention group was not
significant, but the study was not adequately powered.
We completed recently a phase II study evaluating the efficacy of an outpatient
palliative care team intervention, which was accepted for publication in the Journal of
Clinical Oncology68. The primary endpoints of symptom control (Edmonton Symptom
Assessment Scale) and patient satisfaction (FAMCARE scale) were assessed at baseline,
one week and one month. Of 150 patients enrolled (74% recruitment rate), 123 (82%)
completed one-week and 88 (59%) completed four-week assessments. The mean
improvement in ESAS distress score was 8.8 (P<.0001) at one week and 7.0 (P<.0001) at
one month. There were improvements in pain, fatigue, nausea, depression, anxiety,
drowsiness, appetite, dyspnea, insomnia and constipation at one week (all P≤.005) and one
month (all P≤.05). The mean improvement in FAMCARE score was 6.1 (P<.0001) at one

50
week and 5.0 (P<.0001) at one month. The results demonstrated feasibility of recruitment,
and efficacy of a palliative care clinic intervention in improving symptom control and
patient satisfaction. Our ongoing phase III study builds on these findings by enrolling
patients earlier in the disease course (at which time drop-out is also less likely); extending
follow-up to 4 months; and adding quality of life measures for both patients and caregivers.
Methodological considerations
The failure of most RCTs to demonstrate an impact on HRQL may be due to
methodological problems that we have addressed in our RCT. Many studies relied on
referrals for recruitment, whereas in our RCT, research personnel actively screen oncology
clinics. Few studies evaluated nonparticipants to judge generalizability.29,123 Many studies
lacked a formal sample size calculation, and were underpowered. HRQL scales may reach
their “floor” in the last weeks of life52 and patients may have been randomized too close to
death for a measurable difference in HRQL to occur. Our study includes inclusion criteria of
ECOG performance status of ≤2 and a clinical prognosis by the treating oncologist of >6
months. Although physicians tend to overestimate survival,124-126 their predictions are still
highly correlated with survival127 and oncologists’ estimates may be more accurate than
those of other health care professionals.126
After careful consideration and discussion, we opted for cluster rather than
individual randomization. Based on evidence from the health services literature128,129 and
advice from oncologists, it is very difficult to recruit patients to be randomized (or not) to an
intervention such as palliative care, given strong preconceived preferences among patients
and oncologists. Similar individually randomized trials have had severe problems with
recruitment and with control patients crossing over to the intervention.63,105,110,128 The main

51
limitation of cluster randomization is selection bias, due to randomization before
consent.130,131 However, this can be offset by including baseline measures as covariates and
is preferable to an underpowered trial due to poor recruitment. The design implications of
cluster RCTs were thoroughly taken into account in our trial,132,133 unlike previous cluster
RCTs of palliative care. Although our systematic review identified 4 cluster RCTs,9,62,106,112
none accounted for the intracluster correlation coefficient or cluster size in their sample size
calculations, and 3 failed to account for clustering in their analyses.9,106,112 We have
accounted for clustering in our planned analyses, and in our sample size calculation, which
also accounts for drop-out, “drop-in” and nonadherence.
RCTs evaluating palliative care have been criticized for lack of well-defined primary
endpoints, and for using measures that were not developed or validated in a cancer or
palliative care population.18,52 We have curtailed our measures to minimize patient burden.
As maximizing HRQL for patients is a central focus of palliative care,52,97,134 our main
endpoint is HRQL. Existential issues are missing in most HRQL tools and may become
more prominent at the end of life, as do perceptions of quality of care.135-137 We have
included, as secondary outcomes, measures of existential well-being and satisfaction with
care. Palliative care is directed not only at the patient, but also at the caregiver, whose
quality of life may be affected substantially by the burden of caregiving and by the
emotional strain of watching a loved one suffer.138-140 Our trial therefore includes caregiver
HRQL as a secondary outcome.

52
TRIAL PROTOCOL
Overview of trial design
The study is a cluster RCT, with oncologists as the unit of randomization and the
patient/caregiver as the unit of inference.132 Written consent was obtained from all PMH
medical oncologists in the 5 participating tumour site groups to randomize their 24 clinics
either to immediate intervention by a palliative care team, or to conventional care, with
equal numbers allocated to each group. For consenting participants, HRQL and satisfaction
with care are measured prospectively for 4 months. Blinding is not possible because
assignment is evident to the subjects and cannot feasibly be hidden from the referring
physician or palliative care team. We have stratified by tumour site: Lung, Gastrointestinal
(GI), Genito-urinary (GU), Breast and Gynaecological. This controls for major differences
in the range of symptoms and prognosis between tumour types (eg. metastatic lung cancer,
in which the prognosis is less than a year, versus breast cancer, in which it may be many
years) as well as in baseline referral patterns.
Trial setting
Princess Margaret Hospital (PMH), a member of the University Health Network (UHN), is
a cancer centre and teaching hospital in Toronto, Canada, which treats over 10,000 new
patients annually. The PMH Palliative Care Service consists of the Oncology Palliative Care
Clinic (OPCC), a 12-bed Palliative Care Unit (PCU), and an inpatient consultant team.23 In
2007, the service provided consultations to approximately 1600 oncology patients of which
800 were assessed initially in the OPCC. The palliative care team consists of seven full-time
and one part-time physicians (7.5 FTE), five advanced practice nurses (4.5 FTE), 3
registered nurse case managers (2.1 FTE), a social worker (1.0 FTE), a pharmacist (0.3

53
FTE), a physiotherapist (0.5 FTE), an occupational therapist (0.5 FTE) and a chaplain (0.5
FTE). Since starting the trial we have hired one palliative care physician and two registered
nurse case managers, and have increased the social worker’s time from 0.5 to 1.0 FTE to
accommodate increased patient volumes.
The PMH PCU is based on a model of acute palliative care in an academic
environment.23,141 Patients are admitted for acute symptom management, respite (maximum
2 weeks) or terminal care (prognosis <2 weeks). The mean length of stay is 12 days and
there are approximately 29 admissions per month, with 50% dying on the unit and the other
50% discharged home (30%) or to community-based palliative care units (20%). Priority
admission goes to outpatients (60% of admissions) for whom the wait until admission is 0-3
days.
The PMH palliative care team provides consultations and follow-up in the
OPCC,18,68 and is in regular contact with the home care nurses serving the patient’s area.
Once patients require or desire home-based care, they are transferred to a home palliative
care physician. For districts that do not have such a service, telephone contact with the PMH
team continues until death or PCU admission. Applications to PCUs in the patient’s area are
placed in a timely fashion and the patient is admitted to the PMH PCU or to other PCUs if
this is required.
Trial interventions (Table 1)
Intervention: This group receives immediate consultation and follow-up in the OPCC by
the palliative care team based on a philosophy of multidisciplinary care,6,68 which consists
of 7 main elements: (i) Referral to the PMH OPCC. Patients are seen within one week of
recruitment and receive a comprehensive multidisciplinary assessment of symptoms,

54
psychological distress, social support and home services. Symptoms are assessed according
to the Edmonton Symptom Assessment System (ESAS)33 and patients are treated according
to the Palliative Care Integration Project Symptom Management Guidelines.142 (ii) Routine
telephone call by palliative care nurse one week after first consultation. (iii) Monthly
outpatient palliative care follow-up (if possible, scheduled on the same day as oncology
appointments). (iv) 24-hour on call service for telephone management of urgent issues. (v)
Assessment of need for home nursing care and arrangement of services as necessary. (vi)
Transfer of care to a home palliative care team when the patient’s ECOG is ≥3 or when the
patient desires home-based care. (vii) Availability of the PMH PCU for urgent symptom
issues, respite and terminal care. If the patient is admitted to another service at PMH, the
palliative care team follows the patient and provides advice.
Control: This group receives no formal intervention. However, we cannot ethically deny or
delay palliative care referral for patients who wish this and patients may be referred to the
palliative care service at any later time. Whether and when this has occurred is determined
at study-end by checking with the palliative care clinic roster. Analyses will be by intention
to treat but adjustment for such co-intervention is accounted for in the sample size
calculation (Section 2.8). Controls referred to the service receive the same care, complete
the same forms (ESAS) and have access to the same resources (eg. on call service, PCU,
home care) as patients in the intervention group, as this is standard for the PMH OPCC. The
only exception (in addition to later referral) is that controls do not have the same
standardized monthly follow-up, as it is standard practice in the PMH OPCC to base the
interval of follow-up in clinic on the judgement of the individual clinician.
55
Process evaluation: Process evaluation measures are implemented to document that the
intervention is providing the services described. A Palliative Care Assessment Checklist
was developed with input from palliative care team members and is completed by the
palliative care physician for every intervention patient. The palliative care nurse keeps a log
of all telephone calls made on the patient’s behalf. This information will not be controlled
for in the analyses, as it is considered part of the intervention and analyses will be by
intention to treat.
Inclusion and exclusion criteria
Inclusion criteria: (i) Age 18; (ii) Attending PMH; (iii) Diagnosis of stage IV cancer (for
breast or prostate cancer, refractory to hormonal therapy is an additional criterion; stage III
is included for lung cancer due to short prognosis); (iv) ECOG ≤2 (by primary oncologist);
(v) Estimated prognosis by primary oncologist >6 months; (vi) Completion of the first set of
questionnaires. Exclusion criteria: (i) Insufficient English literacy to complete the
questionnaires; (ii) Inability to pass the cognitive screening test (Short Orientation-Memory-
Concentration Test (SOMC) score <20 or >10 errors).143
Measures
Primary outcome: Health-related quality of life (HRQL) as measured by the FACT-G,
QUAL-E and FACIT-Sp scales, which together measure physical, social/family, emotional,
functional and existential well-being.
(i) FACT-G (Functional Assessment of Cancer Therapy-General): The primary outcome
measure used for sample size calculation is the total FACT-G score (see section 2.7). The
FACT-G is a 27-item internationally validated questionnaire divided into four primary

56
HRQL domains: Physical Well-being (PWB), Social/Family Well-being (SWB), Emotional
Well-being (EWB) and Functional Well-being (FWB).46,122 The total FACT-G score is
calculated by summing the subscale scores (PWB, SWB, EWB, FWB). This questionnaire
is appropriate for use with patients with any form of cancer and takes approximately 5-10
minutes to complete.
(ii) QUAL-E: The QUAL-E is a brief 26-item self-report measure of quality of life at the
end of life, which contains items in four domains: life completion, symptoms impact,
relationship with health provider and preparation for end of life.144 It was developed to
evaluate the effectiveness of interventions targeting improved care at the end of life,144 is
acceptable to seriously ill ambulatory patients, and is reliable and valid.145 It takes 5-10
minutes to complete.
(iii) FACIT-Sp: The 12-item FACIT-Sp consists of 2 subscales evaluating Meaning and
Peace (8 items) and Faith (4 items), and has satisfactory reliability and validity.146 The
relationship between spiritual well-being and HRQL was accounted for more by the
Meaning and Peace subscale, which may also be more important in HRQL and more
amenable to amelioration in medical settings.135,136,147-149 We will therefore use only the
Meaning and Peace subscale as an outcome measure. The entire scale takes 2-3 minutes to
complete.
Secondary outcomes:
A. Patient and family:
(i) Satisfaction with cancer care (FAMCARE scale) This scale measures satisfaction with
information-giving, availability of care, psychological care and physical patient care in
patients with advanced cancer.34,37 It is usually completed by the closest family member, but

57
has also been completed by patients.38 Family members will complete the 19-item scale,34,37
which has previously been used in studies of patients with advanced cancer59,118 and takes
less than 5 minutes. Patients will complete a 17-item version, which we modified for patient
use and used in our pilot study.68 This measure was specifically designed for the evaluation
of palliative care,34 and has been validated in outpatients with advanced cancer.34,37
B. Patient only:
(i) Symptom control (Edmonton Symptom Assessment System; ESAS) The ESAS
consists of 0-10 visual analogue scales (0=best, 10=worst) for pain, fatigue, drowsiness,
nausea, anxiety, depression, appetite, dyspnea, insomnia, and sense of well-being. The
ESAS is a simple, validated tool that is completed by the patient and allows for screening
and monitoring for the most common symptoms in patients with advanced incurable
illness.33 It takes less than 2-3 minutes to complete.
(ii) Communication with health care providers (CARES: Medical Interaction
Subscale) This is an 11-item subscale derived from the Cancer Rehabilitation Evaluation
System.150 It assesses whether or not patients experience problems in their interactions with
their nurses and doctors, including problems related to information seeking and active
participation in medical care. It has good internal consistency and adequate reliability,
validity and sensitivity among cancer patients.151 It takes less than 5 minutes to complete.
C. Family member only:
(i) Caregiver quality of life (Caregiver QOL Index-Cancer; CQOLC) This is a scale
designed to assess HRQL in family caregivers of patients with cancer,152,153 which consists
of 35 items rated on a 5-point Likert-type scale. The instrument has undergone rigorous
58
psychometric testing,152 including in a palliative setting,139 and has good validity, internal
consistency and reliability. It takes approximately 10 minutes to complete.
(ii) Caregiver health and functioning (Medical Outcomes Study Short Form (SF-36))
This scale assesses perceived health and functioning, using eight subscales: physical
functioning, role limitation due to physical health problems, bodily pain, general health,
vitality (energy/fatigue), social functioning, role limitation due to emotional problems and
mental health154 and has been well validated.155-157 Two summary scores (physical and
mental) provide global indices of functioning. It has been an outcome in previous studies
assessing the health of caregivers of cancer patients30,59,158 and takes 5 minutes to complete.
Other measures:
(i) Chart Review Form Medical records for each patient are reviewed at recruitment and at
each follow-up in order to document demographic data, cancer diagnosis, stage, co-morbid
conditions and treatment received.
(ii) Caregiver Demographic Questionnaire This includes age, gender, ethnicity, level of
education, marital status, household income, and the nature of the patient/primary-caregiver
relationship (spouse, parent, child, etc).
Practical arrangements for recruitment and follow-up
Patients are being recruited from five tumour sites at PMH: Lung, GI, GU, Breast and
Gynaecology. These are the 5 largest solid tumour sites, and include lung, breast, prostate,
colorectal, pancreatic and ovarian cancer, which are among the most frequent causes of
cancer deaths in Canada.95 Recruitment occurs by regular screening of oncology clinics by
research personnel.

59
After obtaining permission from the attending oncologist, eligible patients are
approached for consent. Patients attending clinics randomized to the intervention arm are
asked for consent to participate in a trial evaluating the effectiveness of involvement of a
symptom management and palliative care team in their care. Those in clinics randomized to
the control arm are asked for permission to participate in a study assessing quality of life
and satisfaction with care (see Consent Forms). This differential consent process, which has
been used in cluster randomized trials of palliative care62 and other interventions,159-162
avoids bias which could result from control patients requesting the intervention or otherwise
altering their behaviour and has been approved by the UHN REB. Each patient is also asked
to identify his/her primary caregiver. If the caregiver is present, he/she is approached about
the study and consent is obtained. If the caregiver is not present, he/she is contacted by
telephone to request study participation and to seek informed consent. To allow for
inclusion of baseline data as a covariate in the analyses, consenting patients and caregivers
complete baseline measures in order to be eligible for the trial.163, p. 101 For patients who
refuse participation, we are requesting collection of baseline data and medical chart
information. The data from these patients will be analysed separately and will be used only
for the purpose of establishing generalizability and assessing selection bias.
The outcome measures are measured by self-report of the patient (FACT-G, FACIT-
Sp, QUAL-E, ESAS, modified FAMCARE, CARES) and primary caregiver (FAMCARE,
CQOLC, SF-36). All questionnaires except the baseline package are distributed by mail.
Patients who do not respond within 2 weeks receive a reminder telephone call and an offer
for a research assistant to help them to complete the forms. Patients who cannot be reached
or who decline help filling out the forms are considered lost to follow-up. Following
completion of baseline measures, a research team member completes the chart review.

60
Medical and demographic data are extracted including: i) age, gender, marital and family
status, level of education, religion; ii) medical history including comorbid diagnoses and
time of cancer diagnosis; iii) treatment recommendations and treatments received, including
list of medications. Follow-up data are collected at 1, 2, 3 and 4 months after study
enrolment. In a previous study, one month was considered consistent with an intervention
period likely to show a clinically significant treatment effect on HRQL.62
Sample size calculation (Appendix A)
To ensure sufficient power for our analyses, we have recalculated the sample size (see
Appendix A) based on the reassessed values of the standard deviation, intra-cluster
correlation coefficient, attrition and adherence. The revised sample size is 450 patients (225
per group), compared to our original calculation of 380. The minimally important difference
(MID) in HRQL score has been defined as “the smallest difference in score in the domain of
interest that patients perceive as important”.50 Our primary outcome measure is the FACT-G
total score, for which the MID is 3-7 points.46,164-166 We have used 7 points as our MID,
which corresponds to a 7% change on the overall scale. Studies have found that a 5-10%
change in quality of life scales is clinically significant.42,43,167 The standard deviation for the
FACT-G score in our sample is 15.4 which is similar to other studies in cancer patients
(range 14.5-15.9)164,168
Sample size calculations for cluster RCTs differ from those for individually
randomized trials, in that the intra-cluster correlation coefficient (ICC) must be taken into
account. The ICC measures the degree of similarity among responses within a cluster and
accounts for the fact that patients within a given cluster (i.e. clinic, in this trial) are more
likely to respond in a similar manner than patients between different clusters.133 For our
61
sample, the ICC is 0.04 (Appendix A), which is within the 0.01-0.05 range found in
previous studies of medical clinics,133 but larger than our originally estimated value of 0.03.
In order to detect a difference of 7 units, at the 2-sided significance level of 0.05, with
power 0.8, a total of 250 subjects is required, assuming a standard deviation of 15.4, a
cluster size of 20, and an intracluster correlation coefficient of 0.04 (Appendix A). We
anticipate that there will be 6% “drop-in”169 to the intervention by the control group (see
Section 2.8), which requires multiplying the sample size by 1.3.170 Further adjusting for
20% drop-out and 85% completion of questionnaires (see Section 2.8) gives a total sample
size estimate of 450 (218 per group).
Recruitment, attrition and adherence (compliance)
Between December 5, 2006 and September 10 2008 (21 months), we recruited 245 patients
(114 intervention and 131 controls) and 109 caregivers (52 intervention and 57 controls), for
whom baseline characteristics are shown in Tables 2 and 3. There was a significant
difference at baseline for HRQL and patient performance status (worse in the intervention
group); the latter explains the increased death rate in the intervention group (Table 4) and
suggests selection bias,130,131 which we will address in our analyses (Section 2.9). We have
estimated expected attrition, and adherence with questionnaire completion, based on
patients enrolled from December 2006–April 2008, as all of these patients should have
complete follow-up data as of September 2008 (Table 4). Of the 201 patients who
completed baseline (T0) questionnaires during the latter time period, 41 (20%) either died or
withdrew by T3, which is higher than the 15% estimate we used in our original sample size
calculation. In addition, 31 (15%) did not complete questionnaires at T3, which is precisely
the estimate used in our original calculation. As anticipated, there are also controls who
62
have “dropped in” to the intervention by receiving early palliative care. Of 71 patients who
have completed T3, only 6% were referred to palliative care, which is less than the
anticipated 7%. Accordingly, we have accounted for 6% “drop-in” in our
calculations.130,132,133
Planned analyses
Analyses will be by intention to treat and patients will be analysed in the groups to which
they were originally randomized. Although the unit of randomization is the clinic, the unit
of analysis is the individual patient/caregiver, since the intervention is directed at the
patient/caregiver rather than at the oncologist and the outcome of quality of life is an
individual construct.133 Standard regression methods are not appropriate, as they do not
account for the effects of clustering, resulting in spuriously low observed p-values.132,171-173
We will therefore use a mixed effects linear regression model, which will be implemented
with the PROC MIXED program in the SAS statistical software package.174 In order to
increase precision, we will include the baseline FACT-G score as a covariate in the model.
Adjustment for the stratification factors and other baseline variables (either at the cluster or
individual level) observed to be associated with the principal response measures and
showing important levels of imbalance between treatment groups will also be performed.
Since missing data in HRQL studies are frequently not random,175 sensitivity analyses will
also be conducted.176 In keeping with FACT-G scoring guidelines, missing data subscores
will be prorated using the average of the other answers, as long as more than 50% of the
items were answered. The total FACT-G will be considered appropriate to score as long as
the overall item response rate is greater than 80%.46,177

63
SIGNIFICANCE
This is the first RCT to study the effectiveness of early involvement of a multidisciplinary
palliative care team in patients with metastatic cancer. Its results are expected to have
important and wide-reaching consequences for the care of patients with cancer in Canada
and elsewhere.
Results will be disseminated according to the Pathman-PRECEED model of
knowledge translation.178 Depending on the results, potential avenues for translation of
knowledge include highlighting gaps in patient understanding of the relevance of palliative
care and/or training of health care professionals in the communication of treatment goals
and appropriateness of early palliative care intervention. Results will be disseminated at
lectures, rounds, scientific meetings and in peer-reviewed journals. Adoption and adherence
will be facilitated by the development of educational interventions such as workshops and
small group discussions. Patient-based interventions such as pamphlets, websites and
support groups will also be developed and evaluated. Implementation will be enhanced by
the inclusion as co-investigators and collaborators of influential medical oncologists, who
may serve as opinion leaders to change current practice.
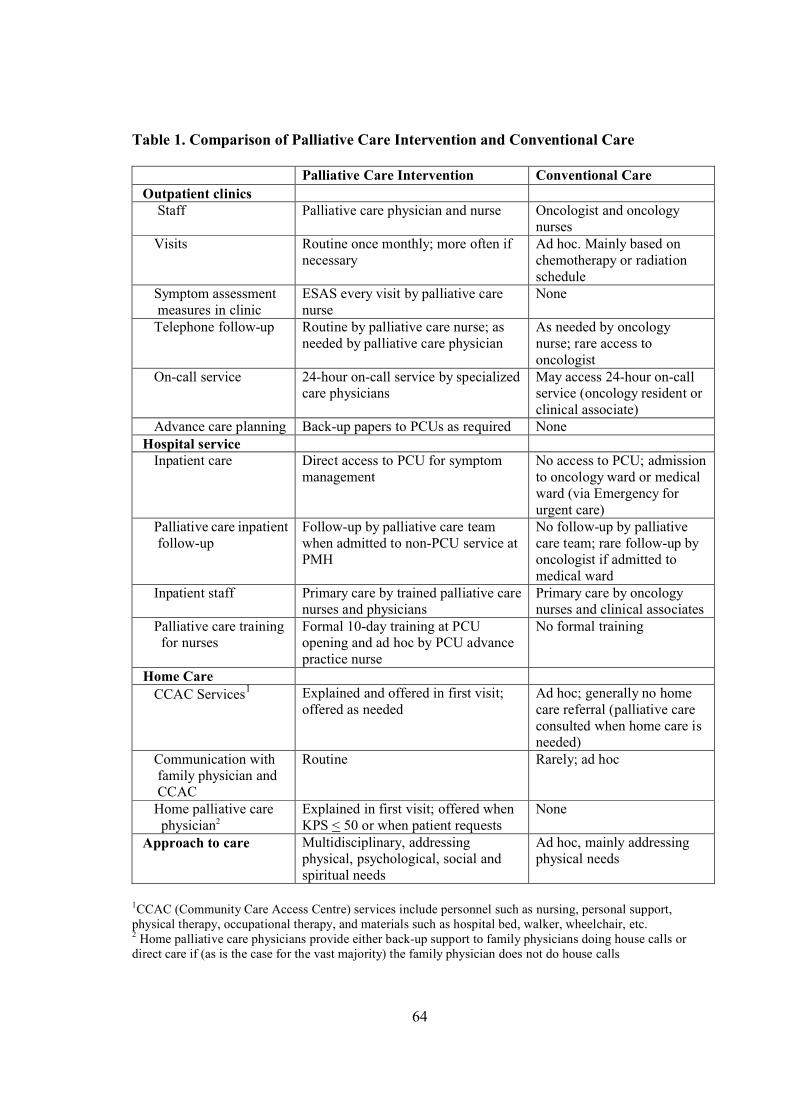
64
Table 1. Comparison of Palliative Care Intervention and Conventional Care
Palliative Care Intervention Conventional Care Outpatient clinics Staff Palliative care physician and nurse Oncologist and oncology
nurses Visits Routine once monthly; more often if
necessaryAd hoc. Mainly based on chemotherapy or radiation schedule
Symptom assessment measures in clinic
ESAS every visit by palliative care nurse
None
Telephone follow-up Routine by palliative care nurse; as needed by palliative care physician
As needed by oncology nurse; rare access to oncologist
On-call service 24-hour on-call service by specialized care physicians
May access 24-hour on-call service (oncology resident or clinical associate)
Advance care planning Back-up papers to PCUs as required None Hospital service Inpatient care Direct access to PCU for symptom
managementNo access to PCU; admission to oncology ward or medical ward (via Emergency for urgent care)
Palliative care inpatient follow-up
Follow-up by palliative care team when admitted to non-PCU service at PMH
No follow-up by palliative care team; rare follow-up by oncologist if admitted to medical ward
Inpatient staff Primary care by trained palliative care nurses and physicians
Primary care by oncology nurses and clinical associates
Palliative care training for nurses
Formal 10-day training at PCU opening and ad hoc by PCU advance practice nurse
No formal training
Home Care CCAC Services1 Explained and offered in first visit;
offered as neededAd hoc; generally no home care referral (palliative care consulted when home care is needed)
Communication with family physician and CCAC
Routine Rarely; ad hoc
Home palliative care physician2
Explained in first visit; offered when KPS < 50 or when patient requests
None
Approach to care Multidisciplinary, addressing physical, psychological, social and spiritual needs
Ad hoc, mainly addressing physical needs
1CCAC (Community Care Access Centre) services include personnel such as nursing, personal support, physical therapy, occupational therapy, and materials such as hospital bed, walker, wheelchair, etc. 2 Home palliative care physicians provide either back-up support to family physicians doing house calls or direct care if (as is the case for the vast majority) the family physician does not do house calls

65
Table 2. Patient baseline characteristics according to treatment group
Study arm n (%)Characteristic Intervention
n=114Controln=131
p-value
Age [mean (SD)] 61.5 (12.9) 58.6 (12.2) 0.08
SexMale 41 (36.0) 55 (42.0) 0.3Female 73 (64.0) 76 (58.0)
Clinic/primary tumor siteGI 32 (28.1) 31 (23.7) 0.2GU 19 (16.7) 31 (23.7)Gyne 19 (16.7) 29 (22.1)Breast 20 (17.5) 24 (18.3)Lung 24 (21.1) 16 (12.2)
Education< high school 6 (5.3) 7 (5.3) 0.7High school 27 (23.7) 29 (22.1)College/University/Other 80 (70.2) 95 (72.5)
Employment statusEmployed 25 (21.9) 36 (27.5) 0.5Unemployed 14 (12.3) 18 (13.7)On disability 20 (17.5) 26 (19.8)Retired 55 (48.2) 51 (38.9)
Income<$60,000 33 (47.1) 38 (42.2) 0.5≥$60,000 37 (52.9) 52 (57.8)
Marital statusMarried/Common law 80 (70.2) 96 (73.3) 0.4Separated/Divorced 9 (7.9) 14 (10.7)Single 15 (13.2) 16 (12.2)Widowed 10 (8.8) 5 (3.8)
Living AloneYes 22 (19.3) 23 (17.6) 0.7No 92 (80.7) 108 (82.4)
Caregiver for othersYes 36 (31.6) 47 (35.9) 0.5No 78 (68.4) 84 (64.1)
On chemotherapyYes 49 (43.4) 57 (43.8) 1.0No 64 (56.6) 73 (56.2)
ECOG performance status 0 or 1 105 (92.1) 126 (96.2) 0.003 2 9 (7.9) 5 (3.8)FACT-G total 72.23 (16.3) 78.24 (14.2) 0.002QUAL-E total 70.02 (11.1) 72.78 (11.2) 0.06

66
Table 3: Caregiver baseline characteristics according to treatment group
Study arm n (%)Characteristic Intervention
(n=52)Control(n=57)
p-value
Age [mean (SD)] 56.5 (12.8) 53.7 (10.2) 0.2
SexFemale 30 (57.7) 36 (63.2)
Recruitment clinicGI 19 (36.5) 18 (31.6) 0.9GU 9 (17.3) 12 (21.1)Gyne 9 (17.3) 9 (15.8)Breast 9 (17.3) 13 (22.8)Lung 6 (11.5) 5 (8.8)
Education< high school 2 (3.9) 4 (7.0) 0.8High school 12 (23.5) 16 (28.1)College/University/Other 37 (70.6) 36 (63.2)
Employment statusEmployed 29 (55.8) 31 (54.4) 0.6Unemployed 5 (9.6) 6 (10.5)On disability 0 2 (3.5)Retired 18 (34.6) 17 (29.8)Student 0 1 (1.8)
Marital statusMarried/Common law 49 (94.2) 54 (96.4) 0.4Separated/Divorced 0 1 (1.8)Single 3 (5.8) 1 (1.8)Widowed 0 0
Living with patientYes 46 (88.5) 50 (87.7) 0.9No 6 (11.5) 7 (12.3)
Caring for othersYes 24 (46.2) 18 (31.6) 0.1No 28 (53.8) 39 (68.4)
Relationship to patientSpouse/partner 39 (75.0) 48 (84.2) 0.3Son/daughter 5 (9.6) 6 (10.5)Sibling 3 (5.8) 1 (1.8)Parent 3 (5.8) 1 (1.8)Other 2 (3.8) 1 (1.8)
Years known patient [mean (SD)] 35.00 (13.8) 32.82 (12.5) 0.4
Hours/day spent with patient [mean (SD)] 15.06 (7.9) 16.54 (7.4) 0.3
Hours/day spent on care-giving [mean (SD)] 2.42 (4.1) 3.19 (5.8) 0.5
SF-36 v2 – Physical [mean (SD)] 54.16 (8.2) 52.43 (9.1) 0.320
SF-36 v2 – Mental [mean (SD)] 41.33 (12.8) 41.59 (10.6) 0.910
Caregiver QOL Index-Cancer – Total [mean (SD)] 82.87 (22.1) 84.04 (18.5) 0.765

67
Table 4: Recruitment, Attrition and Adherence
Table 4A: Questionnaires completed
Completed questionnaires (enrolled Dec. 2006 to Sept. 2008)
Completed questionnaires (enrolled Dec. 2006 to Apr. 2008)
Intervention Control Total Intervention Control TotalConsented 174 191 365 152 162 314
T0 114 131 245 95 106 201T1 81 105 186 69 82 151T2 68 91 159 60 77 137T3 60 82 142 57 71 128T4 50 81 131 50 80 130
T0 indicates baseline assessment; T1-T4, one-month to 4-month follow-up assessments, respectively
Table 4B : Questionnaires not completed
Did not complete questionnaires (enrolled Dec. 2006 to Sept. 2008)
Did not complete questionnaires(enrolled Dec. 2006 to Apr. 2008)
Intervention Control Total Intervention Control TotalT0 0 0 0 0 0 0T1 (total) 114-81 = 33 131-105 = 26 59 95-69 = 26 106-82 = 24 50 died* 2 0 2 2 0 2 withdrew* 8 5 13 8 5 13 skipped 20 20 40 16 19 35 pending 3 1 4 - - -
T2 (total) 114-68 = 46 131-91 = 40 88 95-60 = 35 106-77 =29 64 died* 6 1 7 6 0 6 withdrew* 15 9 24 12 9 21 skipped 17 21 38 17 20 37 pending 8 9 17 - - -T3 (total) 114-60 = 54 131-82 = 49 106 95-57 = 38 106-67 = 35 73 died* 12 1 13 11 0 11 withdrew* 19 17 34 16 15 31 skipped 12 17 34 11 20 31 pending 11 14 25 - - -T4 (total) 114-50 = 64 131-81 = 50 114 95-50 = 45 106-80 = 26 71 died* 13 1 14 12 0 12 withdrew* 36 28 64 33 26 59 pending 15 21 36 - - -
* Number of deaths and withdrawals are cumulative over each time point.

68
Appendix ASample Size Calculation
Null hypothesis: The mean change in total FACT-G score from baseline to 3 months after study enrolment is the same in patients receiving an early palliative care team intervention and patients receiving conventional cancer care.
Alternative hypothesis (two sided): The mean change in total FACT-G score from baseline to 3 months after study enrolment is different in patients receiving an early palliative care team intervention and patients receiving conventional cancer care.
For cluster randomization, the cluster size, m, and the intracluster correlation coefficient, , must be taken into account 132, p. 57. It is reasonable to assume that over 3.5 years, an average of 20 patients will be recruited per clinic (m = 20). The intracluster correlation coefficient for our sample is 0.04, which is similar to intra-cluster correlation coefficients of between 0.01 and 0.05 found in previous studies of medical clinics 133.
Intra-cluster correlation coefficient (ICC) calculation179-181
Using mean square (MS) values from a one-way analysis of variance, and assuming that cluster size is the same across clusters (i.e. 20), the equation is:
ICC = MS(between) – [MS(within)/MS(between) + (m -1)*MS(within)]
ICC = (412.759-220.240)/[412.759 + (20-1)* 220.240]
ICC = 192.519/4597.319
ICC = 0.04
Sample size calculation:
Assuming 20 patients per cluster, a minimally important difference (MID) of 7 points in the FACT-G, a standard deviation in the FACT-G of 15.4, an ICC of 0.04, a 2-sided significance level of 0.05, and a power of 0.80, the unadjusted sample size per arm is:
n = 2 [(Z2 + Z2)]2 [1 + (m – 1) ] /2
Using Z2 = 1.96, Z2 = 0.842, = 15.2, = 7, m = 20, = 0.03
n = 2 [(1.96+0.842) 15.4]2 [1+ (20-1) 0.04]/72
n = 133.76
Therefore the sample size for each study arm is 134 patients and the total sample size N is 2*133.76 = 267.52, or 268.
69
For a stratified design, the between-cluster variance component of the overall response variance will be reduced, and the power of the trial will be correspondingly increased. However, the actual gain in precision is difficult to estimate. We will adopt the conservative strategy of ignoring this aspect of design in sample size planning.132, p. 70
Of the control patients, up to 6% may, during the 3 months before the primary outcome analysis, be referred to palliative care with a subsequent survival of >6 months, effectively “dropping in”169 to the intervention. Adjustment for drop-ins can be done using Lachin’s formula,170 multiplying the sample size by a correction factor of 1/(1-R)(1-R) where R is the proportion of drop-ins. For drop-in rate of 6%, the sample size must be multiplied by a correction factor of 1/(1-0.06)(1-0.06) = 1.13.
Adjustment for loss to follow-up is necessary. This is normally done by multiplying the sample size by 1/(1-d1) where d1 is the anticipated loss rate 163, p. 78. For loss to follow-up of 20%, d1 = 0.20 and the sample size must be further multiplied by 1/(1-0.20) = 1.25
Of those who are not lost to follow-up, not all may return questionnaires. This is accounted for by using the same formula as for loss to follow-up, 1/(1- d2) where d2 is the non-compliance rate 163, p. 79. For compliance of 85%, d2 = 0.15 and the sample size must again be multiplied by 1/(1-0.15) = 1.18
The sample size, N*, accounting for loss to follow-up rate and non-compliance is:
N* = N (1.13)(1.25)(1.18)
N* = 268 (1.13)(1.25)(1.18)
N* = 446.7 rounded to 450 patients, 225 per arm

70
Chapter Seven
Determinants of health-related
quality of life in patients with advanced cancer
Submitted for publication as:
Zimmermann, C., Burman, D., Swami, N., Krzyzanowska, M., Leighl, N., Moore, M.,
Rodin, G., Tannock, I. Determinants of quality of life in patients with advanced cancer.

71
ABSTRACT
Purpose: Improving health related quality of life (HRQL) is the main goal of palliative care
and an important outcome for oncology trials. This study examines determinants of HRQL
in outpatients with advanced cancer.
Patients and Methods: Patients with metastatic gastrointestinal, genitourinary, breast, lung
or gynecological cancer, ECOG 0-2, and clinical prognosis of 6 months to 2 years were
recruited from outpatient medical oncology clinics. HRQL was measured using the FACT-
G questionnaire and the FACIT-Sp meaning and peace (existential) subscale. The influence
of demographic and medical characteristics on HRQL was determined using t-tests and
ANOVA, with Tukey correction for multiple comparisons. Multivariate linear regression
was used to determine independent predictors.
Results: Of 285 patients, 57% were female and the median age was 61 years; 44% were
alive at latest follow-up, and of those deceased, the mean survival time was 10 months. The
strongest determinants of overall HRQL were increased age (p<0.001), good performance
status (PS; p<0.001) and survival time >6 months (p=0.001). Compared to patients
receiving cancer treatment, those awaiting new treatment had worse emotional well-being
(p<0.001), while those on surveillance or whose treatment had been stopped had worse
existential well-being (p=0.03). Male gender predicted better emotional and physical well-
being and lower income predicted worse social well-being.
Conclusions: Age, PS, survival time and treatment status are important determinants of
HRQL in patients with advanced cancer. Decision aids, open communication and
involvement of supportive care specialists may improve emotional and existential distress
associated with changing or stopping cancer treatment.

72
INTRODUCTION
Maximizing health related quality of life (HRQL) for patients is a central focus of palliative
care.52,97,134 HRQL is typically measured according to physical, functional, social, and
psychological domains; in addition, the existential domain is of particular relevance in
patients with advanced cancer.182-184 HRQL is determined not only by the disease and its
treatment, but also by other medical and sociodemographic characteristics.75,76,185-187 It is
important to develop an understanding of variables that may influence HRQL for patients
with advanced cancer, so that these can be accounted for in clinical trials; it is also
important to identify vulnerable groups, so that their HRQL can be specifically addressed
and optimized.
Most studies of determinants of HRQL have been conducted in general
populations.75,76,185,186 Such studies have reported better HRQL among those who are
younger,75,76,186 male,75,186 married,76,185 and have higher education.76,185 Studies comparing
cancer and non-cancer populations have shown that a malignant diagnosis is not associated
with reduced global HRQL, although having cancer reduces physical and role
function.187,188 There have been only three studies investigating determinants of HRQL for
patients with advanced cancer.65,92,135 Two that used the European Organization for
Research and Treatment of Cancer Quality of Life Questionnaire – Core 30 (EORTC QLQ-
C30) reported less pain and better emotional functioning in older patients, more nausea and
vomiting in women, and worse social functioning in married/cohabiting patients.65,92 The
third study used the Functional Assessment of Cancer Therapy-General (FACT-G) measure
and found that HRQL in people with advanced cancer (clinical prognosis 3 months to 2
years) did not vary significantly in relation to marital status, education level, ECOG

73
performance status, or clinician-estimated life expectancy.135 Only the last study specifically
assessed outpatients, and none has used measures including the existential domain.
The purpose of our study was to examine factors associated with HRQL for
outpatients with advanced cancer, including physical, emotional, social, functional and
existential domains. We hypothesized that better HRQL would be associated with
demographic factors such as increased age, male gender, and higher income, and with
disease-related factors such as better performance status, lower comorbidity and increased
survival time. For treatment status we had no specific hypotheses, as HRQL could improve
with treatment, but could also be affected by side effects.
METHODS
Study participants
Patients were recruited from December 2006 to December 2008, as part of a cluster
randomized controlled trial of early intervention by a specialized palliative care team versus
routine oncology care in patients with advanced cancer. Recruitment took place at 24
oncology clinics at Princess Margaret Hospital (PMH), a comprehensive cancer center in
Toronto, Canada.
Eligibility criteria included a diagnosis of stage IV gastrointestinal, genitourinary,
breast or gynecological cancer, or stage III/IV lung cancer; ECOG performance status ≤2;
and a clinical prognosis of 6 months to 2 years (the latter two criteria were determined by
the patient’s primary oncologist). Patients with locally-advanced pancreatic or esophageal
cancer were also included. Those with insufficient English to complete the questionnaires,
or who did not pass the cognitive screening test (Short Orientation-Memory-Concentration
Test (SOMC) score <20 or >10 errors)143 were excluded.
74
All patients provided written informed consent; those who did not wish to proceed
with the trial were asked for written consent to complete baseline measures only. Because
this was a cluster-randomized study, randomization of clinics occurred before patient
consent. To decrease bias, patients recruited for the control group were not told about the
existence of a trial and were invited to participate in a study assessing quality of life and
satisfaction with care. This consent process has been used previously in cluster randomized
trials of palliative care62 and other interventions.159,161 The protocol was approved by the
Research Ethics Board of the University Health Network.
Measures
Consenting patients completed measures of HRQL at baseline, and at monthly intervals for
four months. For this study, baseline measures were used for all analyses.
The Functional Assessment of Cancer Therapy-General (FACT-G) is a 27-item
internationally validated questionnaire. The core of the FACIT scales, it is divided into four
primary HRQL domains: Physical Well-being, Social/Family Well-being, Emotional Well-
being and Functional Well-being.46,122 The total FACT-G score is calculated by summing
the four subscale scores. A two-point difference on the FACT-G subscale scores and a five-
point difference on the FACT-G are associated with clinically and subjectively meaningful
differences.46,168,189
The 12-item Functional Assessment of Chronic Illness Therapy-Spiritual Well-being
(FACIT-Sp) is a validated measure of spiritual well-being,136,146 which consists of two
subscales complementary to the FACT-G. One subscale measures existential well-being
(Meaning and Peace; 8 items) and includes statements such as “I have a reason for living”.
The other assesses religious well-being (Faith; 4 items), and includes items such as “I find

75
comfort in my faith or spiritual beliefs”. HRQL is reported to depend much more on the
Meaning and Peace than on the Faith subscale,135,184 which may even have a negative
impact.190 We used the 8-item Meaning and Peace subscale to measure existential well-
being.
The primary outcome was HRQL including physical, social, emotional, functional
and existential well-being, as measured by the combined score of the four FACT-G
subscales and the Meaning and Peace subscale; secondary outcomes were the individual
subscales. As suggested in the FACT-G and FACIT-Sp scoring guidelines,46 when there
were missing items, subscale scores were prorated by multiplying the sum of the subscale
by the number of items in that subscale, then dividing by the number of questions answered.
This is considered acceptable as long as more than 50% of the items are answered for that
subscale.46
The Charlson Comorbidity Index (CCI) generates an age-adjusted weighted score
based on the presence of various medical illnesses;39 it has good reliability and validity, and
is the most commonly used measure of comorbidity for patients with cancer.40
Patients completed a demographic questionnaire at the time of enrolment. This
included age, gender, ethnic origin,191 level of education, marital status, living arrangement,
employment status, household income, cancer treatment and comorbid diagnoses. In
addition, research staff reviewed medical records to document and verify demographic data,
cancer diagnosis, stage, and cancer treatment status. The latter was abstracted in duplicate
(DB, CZ) using a standardized abstraction sheet. Discrepancies were resolved by jointly
referring to the medical records.

76
Statistical analyses
The mean total and subscale scores for the HRQL scales were compared among
subgroups according to patient medical and sociodemographic characteristics using
Student’s t-test and one-way analysis of variance (ANOVA), with Tukey’s correction for
multiple comparisons. Demographic variables included those listed above; medical
variables included performance status, primary cancer site, survival time after completion of
the measures, and cancer treatment status. Treatment status was categorized as follows:
“receiving cancer treatment” (receiving chemotherapy, hormonal therapy and/or radiation);
“awaiting new treatment” (those awaiting a further line of treatment), or “no cancer
treatment” (those on surveillance or where treatment had been stopped).
The influence of medical and demographic characteristics on HRQL was examined
using multivariate linear regression. The initial model included all of the above covariates
except marital status, cancer site and employment status. Marital status was excluded due to
collinearity with living situation, and employment status due to collinearity with age.
Cancer site was excluded because certain sites are gender-specific (e.g. breast and
gynecological). Age, comorbidity and performance status were included as continuous
variables. The following variables were dichotomized: income (≥$60,000 vs. <$60,000),
education (≥high school vs. >high school), living situation (alone vs. with others) and ethnic
origin (non-European vs. European).
For survival following completion of the questionnaires, multiple dichotomous
(‘dummy’) variables were first entered into the model: ≤6 months, >6 to 12 months, >12 to
18 months, >18 to 24 months, and >24 to 30 months, with alive as the reference variable.
However, only survival ≤6 months was significantly associated with any HRQL outcomes,
and so this variable was subsequently dichotomized (≤6 vs. >6 months). Multiple
77
dichotomous variables were also created for treatment status, with receiving cancer
treatment as the referent. In total there were 10 independent variables; thus the
recommended sample size for adequate power is at least 200 subjects (20 subjects per
independent variable).192
A backwards stepwise selection process was used to build the regression models. A
two-sided p<0.05 was considered statistically significant. Analyses were performed with
SPSS, version 16.0 (SPSS Inc, Chicago, IL).
RESULTS
Patient characteristics
Of 582 eligible patients approached, 269 were enrolled in the trial, and 16 completed
baseline measures only; an additional 96 initially consented to participate but did not
ultimately complete baseline measures. The most common reasons for declining to
participate were lack of interest (n=84) and time required (n=45).
Tables 1 shows the demographic and Table 2 the medical characteristics of the study
sample (n= 285). The median age was 61 years, 57% were female, 72% were
married/common law, and 18% lived alone. Forty-four percent were alive at the time of
analysis, and of those who were deceased, the mean interval from completion of measures
to death was 10 months. Comorbidity was low with a median CCI score of 0 (range, 0-6).
The most prevalent coexisting medical diagnoses were hypertension (n=81), high
cholesterol (n=39), diabetes (n=37), ischemic heart disease (n=24) and arthritis (n=24);
psychiatric diagnoses included depression (n=13), and anxiety disorder (n=5). The mean
and median FACT-G and FACIT-Sp Subscale and Total Scores are shown on Table 3.

78
Univariate analyses
HRQL scores according to demographic and medical characteristics are shown on Table 4.
Older patients and men had better physical and emotional well-being than younger patients
and women. Patients of European background reported better physical well-being than those
of non-European origin. Patients with lower income had worse social well-being on the
FACT-G scale. Those who were employed or retired had better well-being for the physical,
functional and emotional subscales than those who were unemployed or on disability.
Patients with poor performance status had worse physical, emotional, functional and
existential well-being. Patients with lung cancer had the worst physical and functional
HRQL while emotional well-being was lowest for those with breast and gynecological
cancers. There were no significant differences for treatment status (Table 4), nor for living
situation, marital status or education (data not shown). Patients who survived less than 6
months had the worst HRQL subscores for all domains except social well-being.
Determinants of HRQL according to multivariate analyses
The strongest and most consistent determinants of overall HRQL were age, good
performance status, and a survival time of greater than 6 months. Older age was a
particularly strong predictor of physical and emotional well-being, and better performance
status and longer survival were especially associated with physical and functional well-
being. Compared to patients receiving cancer treatment, those awaiting a new treatment line
had worse emotional well-being, while those who were not receiving treatment had worse
existential well-being. Male gender predicted better emotional and physical well-being and
lower income predicted worse social well-being.
79
DISCUSSION
This study examined determinants of HRQL for outpatients with advanced cancer, using
validated measures including the existential domain. The strongest determinants of overall
HRQL were older age, good performance status, and subsequent survival of more than 6
months. Treatment status had a strong impact on emotional well-being and also affected
existential well-being. Other predictors such as male gender and higher income had a
smaller impact on particular subscales.
Younger age was associated with worse HRQL, particularly in the physical and
emotional domains. These findings are similar to those of two studies using the EORTC-
QC30 to measure HRQL in patients with advanced cancer, which found associations
between younger age, and worse emotional functioning and pain control.65,92 In contrast,
studies in general populations have consistently reported a decline in HRQL with older
age.75,76,186,187,193 This contrasting influence of age in general populations compared to
patients with advanced cancer may be explained by the fact that comorbidity contributes to
worsening HRQL with age,187 but may not be of the same relative importance for patients
with advanced cancer. A diagnosis of advanced cancer may also be more traumatizing for
younger patients, because they are less likely to expect a diagnosis of terminal illness,194 and
are more likely to have concurrent roles and responsibilities such as being the main family
wage earner or the parent of young children.195,196 There remains a dearth of literature on
the specific needs of younger patients and their families, and further research is needed in
this area.
Both performance status and survival time were independent determinants of
physical, functional, emotional and existential well-being. These findings confirm those of a

80
study using the EORTC-QLQ-C30 measure65 and demonstrate that although performance
status is a predictor of prognosis,197 it cannot be used reliably as a proxy for survival time.
Rather, survival time should also be included as a covariate in trials of advanced cancer
patients with HRQL as an outcome. This can be done by waiting at least 6 months after
completion of the study before conducting analyses, and dichotomizing by survival <6
versus ≥6 months. Another study measuring existential well-being found that this was
associated with self-rated performance status; however, it was unclear whether patients
found more meaning and peace because they were less affected by their illness, or whether
their existential well-being protected them from feeling the effects of their illness.184 Our
finding that survival time and clinician-rated performance status are associated with
existential well-being indicates that spiritual well-being decreases with advancing disease
and decline in function. Lack of existential well-being has in turn been associated with
depression148 and may be amenable to change with psychotherapeutic and palliative
interventions.149,198
Our study also reports the impact of treatment status on HRQL in patients with
advanced cancer; in another study where only 13% of patients were receiving
chemotherapy, treatment status was examined but not found to be significant.65 Controlling
for age, performance status and survival time, patients in our study who were awaiting a
new line of chemotherapy had the worst emotional well-being, while those who were
neither receiving nor anticipating treatment had the worst existential well-being. There was
no association between treatment status and functional or physical well-being. Because
patients awaiting new treatment have recently received news that their cancer is
progressing, their distress may reflect this news, combined with the uncertainty of whether
or not the next treatment will be effective. Conversely, receiving active treatment in the

81
setting of advanced disease may convey a false sense of security and prevent end-of-life
planning or the engagement in meaningful life review.199 Decision aids; open, honest
communication of expectations; and the involvement of palliative care and psychosocial
oncology specialists may help to guide patients and clinicians through the difficult decisions
associated with cancer treatment at the end of life.
Emotional as well as physical well-being was also impacted by gender. Our findings
of worse physical and emotional well-being in women are similar to those of a general
population study using the FACT-G,76 although the scores in our sample were worse, and
the gender differences more pronounced. Population studies using the EORTC-QC30 have
also found better emotional functioning in men than in women,75,186,187 and investigations in
oncology regarding specific symptoms have noted increased severity in women of
depression,81-85 anxiety,80,84,85 fatigue,65,67,87-89 and nausea.66 It is not clear whether these
findings indicate a gender disparity in symptom perception,93 reporting,94 or treatment, and
further studies are indicated to explain these differences.
Social well-being was rated consistently high, and had few significant determinants
other than level of income. Indeed, compared with general population data from the United
States,188 Austria,76 and Australia,185 social/family well-being was rated slightly better in our
sample (22 vs. 19-20), although our sample scored worse on the FACT-G total score (75 vs.
80-87). Our sample also scored worse on all domains of HRQL than those in previous
studies of HRQL of heterogeneous cancer populations (mean FACT-G total score 80.4164
and 80.9,188 respectively), but the social well-being subscore in these studies was similar to
that found for our sample (22.1 and 22.3, respectively). These findings of higher perceived
social well-being for patients with cancer, whether in the early or advanced stage, may
reflect a greater need for support from family and friends during serious illness. The
82
questionnaire contains items such as “I get emotional support from my family” and “I get
support from my friends”. This support may be more apparent in a situation where it is
explicitly required.
Limitations of our study include the generally high income, high level of education
and predominantly European ethnic origin of our sample, which has also been the case for
other studies.200 We also limited the study to those with relatively good performance status
to ensure appropriate follow-up, which may restrict generalizability. The patients we
recruited are likely representative of those who would normally participate in clinical trials;
however we did include patients who consented to complete only baseline measures. There
was a high proportion of missing data for income, which may have influenced the results.
Data for this study are cross-sectional, and further longitudinal studies are necessary to
investigate the relationship of HRQL to treatment status and survival time. Finally, we used
measures designed for cancer but not specifically for palliative care. However, although the
latter measures usually include existential well-being, they may measure inadequately
physical and functional aspects of HRQL.201 We therefore complemented the well-validated
FACT-G with a measure of existential well-being.
Our results show that for outpatients with advanced cancer, of the variables we
examined, the most influential determinants of HRQL are age, performance status, survival
time and treatment status. Although the former two are generally accounted for in trials of
palliative care interventions the latter are often omitted. The impact of treatment status on
emotional and existential well-being underscores the importance of attending to
communication of treatment decisions, and providing adequate psychological and spiritual
support. Further epidemiologic studies in ethnically diverse populations and with patients of
mixed socio-demographic and educational backgrounds are necessary. Further research is

83
also needed regarding the effectiveness of targeted interventions for specific patient
subgroups.

84
Table 1. Sociodemographic characteristics of participants (n=285)
Characteristic N %
GenderFemale 163 57.2Male 122 42.8
Age (years)Median (min-max) 61.0 28-88
Living SituationAlone 51 17.9With others 234 82.1
Marital StatusMarried/Common law 204 71.6Single 33 11.6Separated/Divorced 28 9.8Widowed 20 7.0
Education< high school 18 6.4High school 66 23.2College/University 200 70.4
Employment StatusUnemployed 37 13.0On disability 55 19.3Employed 69 24.2Retired 124 43.5
Household Income<$14,999 6 2.1$15,000 – 29,999 24 8.4$30,000 – 59,999 50 17.5>$60,000 102 35.8Not answered 103 36.2
EthnicityEuropean 237 83.2Non-European 48 16.8

85
Table 2. Medical characteristics of participants (n=285)
Characteristic N %
Primary tumor siteGastrointestinal 79 27.7Genitourinary 61 21.4Gynecology 51 17.9Lung 48 16.8Breast 46 16.1
Performance Status (ECOG)0 96 33.71 173 60.72 16 5.6
Cancer treatment statusReceiving treatment Chemotherapy 197 69.1 Chemotherapy and radiation 4 1.4 Hormonal agents 15 5.3Chemotherapy stopped 4 1.4On surveillance 26 9.1Awaiting new treatment 39 13.7
Charlson Comorbidity Index 0 202 70.91 53 18.62 30 10.5
Survival after completion of measuresAlive 125 43.9>24 to 30 months 6 2.1>18 to 24 months 17 6.0>12 to 18 months 34 11.9>6 to 12 months 42 14.70 to 6 months 61 21.4Number of months deceased Mean (SD) 10.2 6.8 Median (range) 8 1-28
Abbreviations: ECOG, Eastern Cooperative Oncology Group performance status
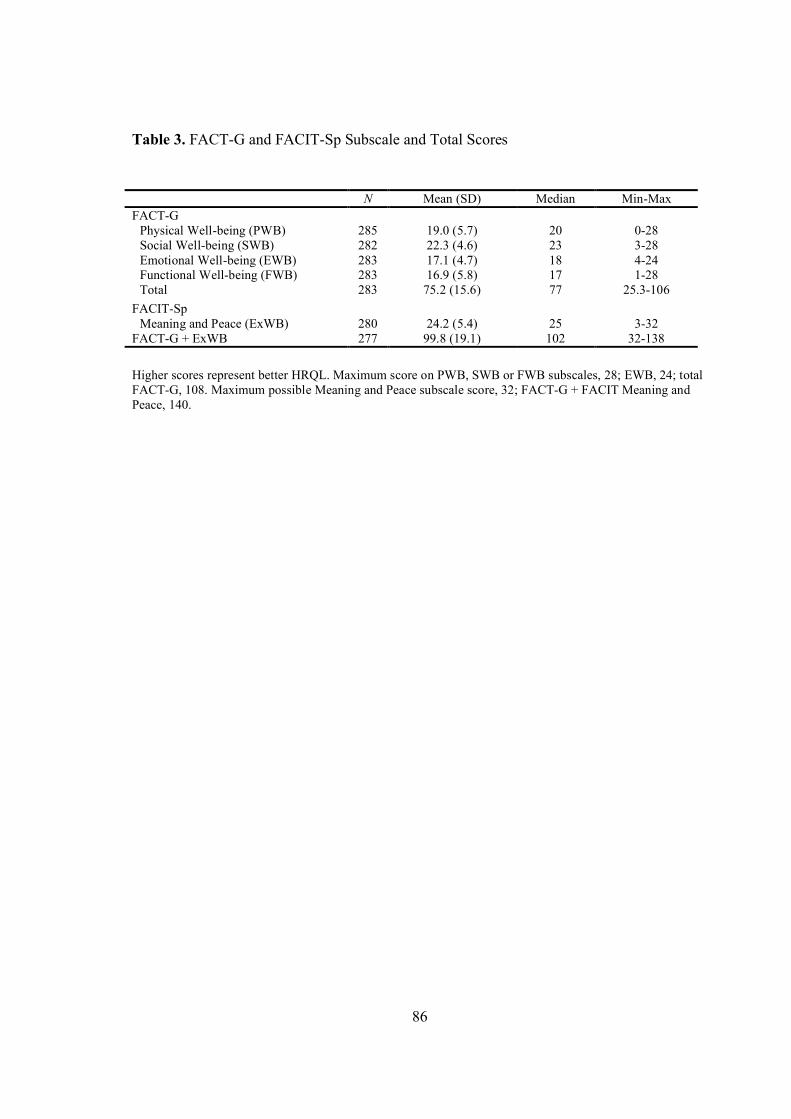
86
Table 3. FACT-G and FACIT-Sp Subscale and Total Scores
N Mean (SD) Median Min-MaxFACT-G
Physical Well-being (PWB) 285 19.0 (5.7) 20 0-28Social Well-being (SWB) 282 22.3 (4.6) 23 3-28Emotional Well-being (EWB) 283 17.1 (4.7) 18 4-24Functional Well-being (FWB) 283 16.9 (5.8) 17 1-28Total 283 75.2 (15.6) 77 25.3-106
FACIT-SpMeaning and Peace (ExWB) 280 24.2 (5.4) 25 3-32
FACT-G + ExWB 277 99.8 (19.1) 102 32-138
Higher scores represent better HRQL. Maximum score on PWB, SWB or FWB subscales, 28; EWB, 24; total FACT-G, 108. Maximum possible Meaning and Peace subscale score, 32; FACT-G + FACIT Meaning and Peace, 140.

Table 4. Comparisons of FACT-G and FACIT-Sp domains by demographic and medical characteristics of participants (means and standard deviations are indicated)
Variable PWB SWB EWB FWB ExWB
Male 20.2 (5.2) 2* 22.1 (4.5) 18.3 (4.3) 3* 17.2 (5.9) 24.5 (5.2)SexFemale 17.2 (5.9) 22.4 (4.6) 16.3 (4.8) 16.6 (5.8) 23.9 (5.6)
< 60 yrs 17.9 (6.0) 3* 22.2 (4.3) 16.3 (4.7) 2 16.3 (5.8) 23.8 (4.8)Age≥ 60 yrs 20.1 (5.2) 22.4 (4.8) 17.9 (4.5) 17.4 (5.8) 24.4 (5.9)
Ethnicity Non-European 16.9 (7.0) 1* 22.7 (4.8) 17.8 (4.8) 16.0 (6.3) 24.6 (4.7)
European 19.5 (5.3) 22.2 (4.5) 17.0 (4.6) 17.1 (5.7) 24.1 (5.5)
Employment Status Employed 20.2 (4.8) 3* 22.6 (4.0) 17.4 (4.7) 1 18.6 (5.4) 3* 24.6 (4.9)Unemployed 16.9 (7.1) 22.8 (4.7) 16.2 (5.0) 15.6 (7.4) 24.1 (5.7)On disability 16.3 (5.9) 21.4 (4.2) 15.7 (4.8) 14.7 (4.9) 23.1 (5.0)Retired 20.3 (5.0) 22.4 (4.9) 17.9 (4.3) 17.3 (5.5) 24.4 (5.7)
Income ≥$60,000 19.3 (5.8) 23.3 (3.8) 2 16.7 (4.8) 17.3 (5.5) 24.0 (5.5)$30,000 – $59,999 18.7 (5.2) 22.2 (4.2) 18.2 (4.7) 17.2 (6.2) 25.0 (5.0)$15,000 – $29,999 18.3 (4.8) 19.5 (6.5) 16.7 (4.8) 16.0 (6.3) 22.4 (6.5)
<$14,999 19.3 (6.0) 22.6 (4.1) 19.3 (3.3) 19.5 (5.0) 26.3 (6.3)
Survival time Survived > 6 months/alive 19.6 (5.5) 3* 22.2 (4.5) 17.4 (4.4) 17.6 (5.5) 3* 24.6 (4.9) 1
Survived ≤ 6 months 17.0 (5.9) 22.5 (4.8) 16.2 (5.4) 14.5 (6.4) 22.7 (6.8)
0 21.1 (4.8) 3* 22.8 (4.3) 18.2 (4.0) 2* 19.2 (5.5) 3* 25.6 (4.5) 3*
1 18.5 (5.5) 22.2 (4.4) 16.7 (4.8) 16.0 (5.5) 23.6 (5.4)ECOG
2 12.8 (7.0) 20.6 (6.8) 14.9 (5.4) 12.3 (6.7) 20.5 (7.2)
Breast 18.7 (6.7) 1* 22.1 (4.7) 15.8 (5.1) 2* 17.5 (7.0) 24.3 (5.5)GI 19.9 (4.6) 22.5 (4.2) 18.4 (4.2) 17.2 (5.5) 24.2 (5.2)GU 20.2 (5.5) 22.3 (4.3) 17.7 (4.4) 17.8 (5.4) 24.8 (4.7)GYNE 18.0 (5.5) 22.1 (4.7) 16.0 (5.1) 16.9 (5.5) 24.2 (5.7)
Primary tumor
Lung 17.4 (6.3) 22.5 (5.2) 16.9 (4.3) 14.8 (5.5) 23.1 (6.1)
Receiving treatment 19.0 (5.8) 22.4 (4.4) 17.2 (4.6) 17.1 (5.6) 24.3 (4.9)No cancer treatment 18.5 (5.3) 22.5 (4.4) 17.8 (4.0) 15.8 (6.6) 22.2 (7.3)
Cancer treatment status
Awaiting new treatment 19.4 (5.6) 21.6 (5.7) 16.1 (5.3) 16.9 (6.0) 24.8 (6.0)
1p≤0.05 for overall comparison; 2p≤0.01 for overall comparison; 3p≤0.001 for overall comparison; *clinically significant. PWB, physical well-being; SWB, social well-being; EWB, emotional well-being; FWB, functional well-being; ExWB, existential well-being.

88
Table 5. Multivariate determinants of Health-Related Quality of Life
Estimates for individual factors within modelOutcome Variable
(model R2)Factors contributing to the
modelβ Coefficient SE P-value
FACT-G/FACIT domain
Physical well-being Sex -1.6 0.8 0.04(0.22) Age 0.1 0.03 <0.001
ECOG -3.0 0.7 <0.001Survived ≤ 6 months -2.7 0.9 0.003
Social well-being Age 0.06 0.03 0.05(0.08) Income ≥ $60K 2.1 0.7 0.002
CCI score -0.8 0.4 0.05
Emotional well-being Sex -1.7 0.7 0.01(0.22) Age 0.12 0.03 <0.001
ECOG -1.6 0.6 0.007Awaiting new treatment -3.2 0.9 <0.001Survived ≤ 6 months -1.9 0.8 0.02
Functional well-being Age 0.09 0.04 0.01(0.16) ECOG -2.8 0.7 <0.001
Survived ≤ 6 months -3.1 1.0 0.002
Existential well-being (ExWB) Age 0.07 0.03 0.04(0.13) ECOG -2.1 0.7 0.003
No cancer treatment -2.9 1.3 0.03Survived ≤ 6 months -2.8 1.0 0.004
FACT-G Total Age 0.4 0.1 <0.001(0.24) ECOG -8.6 1.9 <0.001
Awaiting new treatment -6.9 2.9 0.02Survived ≤ 6 months -7.8 2.5 0.002
FACT-G and ExWB Age 0.5 0.1 <0.001(0.22) ECOG -10.9 2.4 <0.001
Awaiting new treatment -7.5 3.7 0.05Survived ≤ 6 months -10.5 3.2 0.001
Abbreviations: ECOG, Eastern Cooperative Oncology Group performance status

89
Chapter Eight
Summary of findings

90
SUMMARY OF FINDINGS
This chapter will summarize briefly the findings from the research in this thesis. In the next
chapter, I will present what I have learned about conducting such research and offer
recommendations for those conducting similar studies.
Our systematic review of the effectiveness of specialized palliative care examined
the existing research on the impact of specialized palliative care teams on quality of life,
satisfaction with care and economic cost. Of 22 randomized controlled trials (RCTs)
included in the analysis, only four of 13 studies assessing quality of life and one of 14
assessing symptoms showed a significant benefit of the intervention. Evidence of cost
savings was found in one of seven studies and improvement of family satisfaction with care
in seven of 10 studies. Methodological problems were evident in all the trials reviewed,
including contamination of the control group, failure to account for clustering in cluster
randomized trials, and difficulties with recruitment, attrition and adherence. We concluded
that there was most evidence of benefit for improvement of family satisfaction with care,
and that further carefully planned trials with attention to appropriate methodology were
needed.
We proceeded to plan an RCT assessing the effectiveness of early involvement of
specialized palliative care for patients with metastatic cancer, and conducted a phase II
study to assess the efficacy of our proposed intervention. Our phase II study found that there
was improvement of symptom control and patient satisfaction one week and one month
after consultation with a palliative care team. We achieved a 74% recruitment rate; non-
participants were older than participants (median age 67 vs 60, p=0.07), but had similar
91
symptom distress (ESAS distress score 42.8 vs 39.5, p=0.25). Retention of participants was
82% (123 of 150 patients) at one week and 58% (88 of 150 patients) at one month.
However, those who did not complete measures at one week had less severe symptom
distress at baseline than those continuing in the study, suggesting that attrition was not due
to clinical deterioration but due to less perceived relevance of such a study to patients who
had few symptoms. This study established the efficacy of the intervention and the feasibility
of recruitment in a population with advanced cancer. The high attrition rates at one month
demonstrated the necessity of establishing inclusion criteria that assured adequate follow-up
for the completion of the primary endpoint.
For the phase II trial we used two outcome measures, the ESAS and the FAMCARE.
Although both measures have been validated,34,35,37 the latter measure is generally
administered to family members one month after the death of the patient, rather than being
administered prospectively to patients, as we did in this trial. We used this measure (after
modification of questions for patient use) because it was designed specifically to evaluate
satisfaction with palliative cancer care, and had face validity for use prospectively and with
patients. Indeed it had already been used in this way in previous studies,38,58,59 due to the
lack of other measures specific for use in the palliative cancer setting. We subsequently
published a paper describing preliminary psychometric testing of our modified FAMCARE
measure, (which we called the FAMCARE-Patient Version) using the population of the
phase II trial (see Appendix 1).202 Factor analysis of the satisfaction measure revealed a one-
factor structure and suggested the removal of one non-loading item, producing a 16-item
scale (FAMCARE-P16) with high internal reliability.
We further validated the FAMCARE-Patient measure by analyzing data from 315
outpatients with advanced cancer participating in our randomized controlled trial of early

92
palliative care intervention versus routine oncology care, and their caregivers. (see
Appendix 2). A reduced 13-item version of our measure (FAMCARE-P13) possessed a one-
factor structure with high reliability. Patient satisfaction was correlated in predicted
directions with physical distress, communication and relationship with healthcare providers,
and caregiver satisfaction. To assess responsiveness to change, we repeated paired t-test
analyses on the 13-item scale for the 150 patients participating in our phase II trial of
palliative care effectiveness, in which the FAMCARE-P had been administered at baseline,
one week and one month after an outpatient palliative care intervention. There were
statistically significant increases in patient satisfaction at one week (p<0.0001) and one
month (p<0.001). This instrument may be useful to oncology clinicians, researchers, and
other health professionals seeking to evaluate satisfaction with care in settings where
patients have advanced and progressive disease. Due to its responsiveness to change, it may
be particularly useful for clinical trials assessing satisfaction with oncology palliative care.
We also used data from the phase II trial of palliative care efficacy to examine
predictors of symptom severity and response in patients with advanced cancer, and baseline
data from our ongoing RCT of the effectiveness of early palliative care to determine
predictors of health-related quality of life (HRQL) in this population. In the former study,
we found that symptoms at baseline were more severe in women, (particularly anxiety and
appetite) and in those with worse performance status. Symptom improvement was more
pronounced in women and in those with worse symptoms at baseline. We concluded that
performance status, gender and baseline symptom severity should be accounted for in trials
of palliative care interventions, and that inclusion criteria based on symptom severity should
be considered.
93
In the study of determinants of HRQL in patients with advanced cancer, we found
that good performance status (p<0.001) was again a strong predictor of HRQL, and male
gender predicted better emotional and physical well-being. Survival time >6 months was
also an independent determinant and age strongly predicted overall HRQL, particularly in
the physical and emotional domains. Treatment status also had an impact, in that those who
were awaiting a new line of chemotherapy had worse emotional well-being and those who
were not receiving cancer treatment had worse existential well-being. We concluded that
age, performance status, treatment status and gender should be accounted for in clinical
trials of palliative care interventions, and that interventions are needed to improve emotional
and existential distress associated with changing or stopping chemotherapy.
These studies have all informed the planning and development of our ongoing RCT
of effectiveness of early involvement of specialized palliative care in patients with
metastatic cancer. After conducting the systematic review and the subsequent empirical
studies, I have developed recommendations for those planning a randomized controlled trial
for patients with advanced cancer. These will be presented in the following chapter.

94
Chapter Nine
General Discussion
In preparation for publication as:
Zimmermann, C. et al. Designing randomized
controlled trials in palliative care populations

95
GENERAL DISCUSSION
Randomized controlled trials (RCTs) are considered to represent the highest level of
evidence for assessing the effectiveness of treatments203 and of health services.20 However,
they may also be difficult to design, particularly in populations with advanced disease and
limited prognosis. Guidelines have been developed for the reporting of individually and
cluster randomized trials,204,205 and for the reporting of the abstracts of such trials.206
Systematic reviews have also highlighted methodological difficulties in trials conducted in
palliative care populations.18,29 Due to the clinical status of participants, these studies are
particularly prone to problems that may occur in any clinical trial, including difficulties with
recruitment, attrition, contamination of the control group and adherence to the study
protocol. However, with careful planning, such RCTs can be conducted successfully.
Here we review the basic steps involved in the design of an RCT in a palliative care
population. The examples used are from RCTs reviewed in our systematic review, and from
our own studies presented in this thesis. Although all of these examples are from palliative
care trials, the principles presented may be applied more broadly to any randomized
controlled study.
(1) Start with a clinically relevant research question
The best research questions are practical, have clinical relevance and can be adequately
answered. The question should be carefully selected, clearly defined and stated in advance
in the form of a hypothesis.169 It is important that the researcher is interested in the outcome,
but not so invested in proving it that a negative result is not considered acceptable. In this
vein, it is also essential that there is clinical equipoise: that is, “genuine uncertainty within

96
the expert medical community - not necessarily on the part of the individual investigator -
about the preferred treatment”.207
There exists an abundance of unanswered research questions in palliative care.
However, not all of these questions will be answerable with an RCT, and it is important that
the methodology matches the research question.208 It may also be the case that although the
question of interest is best answered by an RCT, such a study is not feasible in the setting in
which the investigator is working. It is therefore essential to consider carefully feasibility
concerns early in the process of the study, and if necessary, to expand the study to other
centres. Indeed, although the research question guides subsequent planning for the RCT, all
of the steps below should be considered before the question and hypothesis are finalized.
(2) Choose a suitable study population
The study population should be selected with attention to the impact this will have on study
design, recruitment, adherence to the protocol, attrition, and generalizability. In trials of
palliative care interventions, problems with recruitment and attrition are particularly
common, given the clinical status of the participants. In order to ensure that the participants
will be well enough to complete the trial, clear inclusion criteria should be developed that
include predictors of survival such as clinical prognosis and performance status.29,123 To
maximize participation and assure a representative sample, recruitment should include a
comprehensive screening strategy to identify potential cases, rather than relying on patient
referrals.29 As well, nonparticipants should be evaluated if possible, to judge generalizability
of trial results.
Our RCT includes inclusion criteria of ECOG 0-2 and clinical impression of the
treating oncologist of a prognosis greater than 6 months. Although physicians tend to

97
overestimate survival, their predictions are still highly correlated with survival209 and
oncologists’ estimates may be more accurate than those of other health care professionals.126
According to data from patients who completed the study as of September 2008, attrition for
our study at our primary endpoint is 20%, which is substantially lower than the median of
40% for previous studies assessing quality of life and satisfaction after a specialized
palliative care intervention. We have also conducted recruitment by systematic screening of
participating oncology clinics, and offered participants who declined participation to
complete baseline measures. By the end of the trial we should have a sufficient number to
compare the HRQL of those participating to those consenting to complete only baseline
measures. In addition, we will compare the demographics of those participating in the trial
to those declining, as we did in our pilot study,210 and has been done for other studies.211
(3) Specify and maintain the contrast between intervention and control groups
Both the intervention and control groups must be clearly defined, and the contrast between
them clearly described in the methods, and maintained throughout the course of the trial. A
palliative care team is a complex intervention, with several interacting components; it is
therefore important to delineate the different components of the intervention and how they
vary among recipients or between research sites.212 Description of the intervention can be
divided into two main categories: the core intervention, which is required in all patients
randomized to the treatment group; and additional interventions, which are an extension of
the core intervention, but are conditional on the situation of the individual patient.29 In
addition there can be unforeseen cointerventions that are necessary in the comprehensive
care of the individual patient, but which are not part of the planned intervention. These can
98
cause problems for interpretation if they occur in differing frequencies in the control and
intervention groups.
In our pilot study,210 the comprehensive assessment and follow-up by a palliative
care physician and nurse constituted the core intervention, while additional interventions
included referrals to social workers or psychiatrists, and involvement of home care and
hospice services. Both the core and additional interventions were described in detail in the
Methods section, and the number of patients who received additional interventions was
documented in the Results.210 In our analysis of baseline data for our ongoing RCT, we
found that the treatment status of the patient was an important cointervention that influenced
HRQL in patients with advanced cancer (see Chapter 7). We will therefore include
treatment status as a covariate for the analysis of our RCT.
In RCTs of health services interventions, description of the control group is as
important as description of the intervention. In our systematic review, the core intervention
was well described in all studies, but less than half described the control group or the
contrast between intervention and control. It is not sufficient to state that the control arm
received usual care, because there may be wide variations among care centres in what care
is standard, leading to problems with generalizability. Jordhoy et al explicitly tabulated the
differences between the intervention and control arm for each component of their palliative
care intervention.62 We have done this as well on in describing our intervention (see Chapter
6, page 101).
The contrast between intervention and control arms must not only be described at
the outset, but also must be monitored and maintained throughout the course of the trial.
Due to the possibility of rapid changes in clinical status in patients with advanced disease,
palliative care trials are susceptible not only to unplanned cointerventions, but also to actual

99
crossover from the control to the intervention arm. This was the case for several studies in
our systematic review,63,105,110 and generally occurred because patients, families or
clinicians, requested a specialized palliative care referral or palliative care unit admission
due to a decline in clinical status. Such occurrences illustrate the difficulty of carrying out
health services research in settings where there may already be established patterns of care,
with or without supporting evidence. Cross-over in our study has been rare, with only 6% of
controls transferring to the intervention group. This low cross-over rate is likely due to the
inclusion of prognostic criteria for entry into the trial, and because our research question
specifically focuses on the effectiveness of early palliative care intervention - which is not
regular clinical practice at our centre – rather than on palliative care intervention at the end
of life, which occurs fairly routinely.
Also common but more difficult to document is contamination of the control group.
This is particularly a problem in individually randomized palliative care trials, where there
is interaction between control and intervention groups for patients and their professional
caregivers. In this situation, physicians may change their palliative care practices for control
patients based on their experience with intervention patients, and control and intervention
patients may discuss their experiences in the waiting room. For this reason, cluster
randomization is increasingly being used in health care interventions, but presents further
challenges, which are discussed below.
(4) Choose an appropriate randomization process and plan analyses accordingly
An important decision in conducting an RCT of a palliative care intervention is whether to
randomize groups (clusters) or individuals. Cluster randomized trials have become
increasingly popular to evaluate the effectiveness of health care interventions, including in

100
palliative care. When the intervention is a change on the organizational or community level,
randomization of individuals may not be possible. Randomization of groups can also avoid
contamination of the control group, which may occur in individually randomized studies
when the intervention is being carried out by clinicians who are also caring for control
patients, or when intervention patients and controls are sharing the same waiting room.
Lastly, individual randomization may not be acceptable to patients if it involves an
intervention such as palliative care, about which patients and clinicians may have
preconceived biases. To overcome the latter obstacle, randomized consent designs, where
individual randomization occurs before consent, are another option, but have been shown to
be less acceptable to patients in a palliative care setting than cluster randomized designs,
resulting in inferior recruitment rates.213
The decision of individual versus cluster randomization should be carefully
considered, and justified in the description of the methods for the trial. Although cluster
randomization has the methodological advantages above, its main disadvantage is selection
bias, which occurs when randomization of clusters occurs before consent at the individual
level. Because clinicians and patients know in advance to which arm they have been
assigned, characteristics of those who consent to participate may differ according to whether
or not they or their physicians consider the intervention or control to be acceptable.
Selection bias occurred in a previous cluster randomized trial of palliative care214 and was
also apparent in the preliminary baseline analyses for our RCT (see Chapter 6, page 98). We
considered this possibility in planning our trial, but felt that despite this disadvantage,
cluster randomization would be preferable, again for reasons of patient and oncologist
preference. We considered that patients would not consider it acceptable to be individually
randomized to an intervention about which they might have strong preferences, which

101
would lead to poor recruitment. We regarded the risk of an underpowered trial to be more
severe than that of selection bias; we plan to offset this bias by including baseline measures
as covariates.
Cluster randomization trials that have been most successful at avoiding selection
bias are those where it was considered acceptable not to obtain individual consent. This was
the case, for example, in a trial where hospitals were randomized to routine offering (or not)
of influenza vaccine to staff, and the outcome was measured by examining patient mortality
data.215 Because both intervention and control sites adopted their trial arm as standard
practice, and the outcome was obtained by hospital records, consent was not considered
necessary for treatment or for collection of data. However, consent to treatment is generally
required for palliative care interventions, and if data is collected in the form of
questionnaires, then consent for collection of data is necessary for both arms of the trial.
In palliative care, units of randomization for cluster RCTs have included
communities,62 physician specialty groups,112 practices,106 or clinics.9 However, these trials
have not always considered the implications of cluster randomization for the design and
analysis of such trials.18 For a cluster RCT, the sample size will need to be considerably
larger than for an individually randomized trial addressing the same question.131 This is
because, unlike for an individually randomized study, the outcome for each patient cannot
be assumed to be independent from that of other patients: patients within clusters are more
likely to have similar outcomes. The degree of similarity among responses within a cluster
is measured by the intracluster correlation coefficient, which must be taken into account
when calculating the sample size for a cluster-randomized trial (see below). As well, if the
unit of analysis is the patient rather than the cluster, standard statistical methods for
measuring outcomes of RCTs are not appropriate, since these assume that data are

102
independent. Failure to account for clustering in the sample size calculation can lead to type
2 error, while lack of consideration of clustering in the analysis leads to type 1 error.
Analyses that account for clustering include an adjusted two-sample t-test or a mixed effects
linear regression model;132 we will use the latter for our analyses.
(5) Select appropriate outcome measures
Outcome measures for a palliative care study need to be clinically relevant, sensitive to the
benefit of the intervention, and easy to measure or observe. Relevant endpoints for palliative
care include clinical outcomes such as symptoms, quality of life and satisfaction with care;
administrative outcomes such as place of death, acute care admissions and emergency
department visits; and economic outcomes such as cost effectiveness or cost utility.
Clinical outcome measures in palliative care trials are generally in the form of
subjective questionnaires rather than objective clinical events such as death or disease
progression. It is preferable to use measures that have been validated previously and have
demonstrated sensitivity to change. This may be difficult given the lack of measures in
palliative care that have undergone rigorous development and testing.216 When nonvalidated
measures look promising, these can be validated during the course of the trial as long as
validated measures are also included; however, the primary outcome should be a validated
measure. For our trial we modified the FAMCARE for patient use to measure patient
satisfaction with care, because it had good face validity for this purpose.210 We were
subsequently able to validate the patient version of this measure, by comparing it with other
complementary measures we used in our pilot study and RCT, including family caregiver
satisfaction, symptom control, quality of life and performance status.202

103
During the planning stage of an RCT, it should be specified which is the primary
outcome, and other outcomes should be labelled as secondary. The primary outcome should
be the one used to calculate the sample size, and should be directly influenced by the
intervention. While the latter is self-evident in trials of pharmacologic agents, for health
services interventions this may be more difficult. For example, one trial included in our
systematic review of palliative care team effectiveness used pain and nausea as the primary
outcomes.105 Although validated measures were chosen to assess these outcomes, they may
not have been sensitive to the benefits of the palliative care service. There was no specific
protocol for the treatment of pain or nausea, and entry criteria were not based on prevalence
or severity of these symptoms. As well, these symptoms tend to fluctuate in patients with
advanced cancer, with crises and remissions that can occur within days. Because the
measures were administered at monthly intervals, any change in pain or nausea that
occurred in between these intervals would not be recorded.
Trials assessing improvement in specific symptoms should be constructed
specifically with that symptom in mind. Specifically, they should have entry criteria that
require the presence of the symptom; a standardized intervention specifically targeted at its
improvement; and endpoints measured after a time interval sufficient for its relief. For trials
assessing more general benefits of palliative care teams, HRQL or satisfaction with care are
reasonable outcomes.
(6) Perform a sample size calculation and address feasibility concerns
In order to perform a sample size calculation for an RCT one needs to estimate the standard
deviation and the minimally important difference for the primary outcome measure for the
trial. This is done by referring to previous literature in a similar population. In addition, the

104
sample size calculation needs to take into account attrition, lack of completion of
questionnaires, and potential limited penetration of the intervention. In individually
randomized trials, contamination of the control group should be taken into consideration,
whereas in cluster randomization studies the intracluster correlation coefficient and cluster
size need to be accounted for.
The failure to conduct a proper sample size calculation can result in underpowered
studies, resulting in type II error. This was a difficulty in many of the trials reviewed for our
systematic review: of 18 studies using individual randomization, only nine described a
formal sample size calculation and of these only six attained their intended sample size.
Only one of four cluster randomization studies acknowledged that the cluster size and
within-cluster correlation should be accounted for, and even this trial did not use these to
calculate the sample size.62 Although practical considerations including those of economics
and time often influence the sample size calculation, both money and time are ultimately
wasted if the primary question cannot be answered due to lack of statistical power. If many
such underpowered studies are conducted, this can in time give the impression that the
intervention itself is not effective, leading to the discarding of potentially beneficial
interventions.
It should be kept in mind that sample size calculations are estimates, based on
parameters gleaned from studies in similar populations to the one being examined. The best
estimate will be obtained using data from a pilot study in the population that will participate
in the trial. We recalculated our sample size half way through recruitment, and found that
the estimate of our intra-cluster correlation was slightly larger (0.04 vs. 0.03) and our
standard deviation slightly smaller (15.4 vs. 15.9) than those used for our original sample
size calculation before the study began. We were also able to estimate more accurately

105
drop-out, completion of questionnaires, and drop-in to the intervention from the control
based on the current figures from the trial. Our recalculated sample size was 450 (225
patients per group), compared to our original estimate of 380, resulting in a lengthening of
recruitment time, for which we obtained additional funding.
(7) Take measures to minimize bias
Although blinding of both the participants and investigators to the intervention assignment
is a hallmark of a well-designed RCTs evaluating effectiveness in pharmaceutical trials, this
may be difficult or impossible to achieve in randomized clinical trials of health services
interventions. In palliative care trials where the intervention is a multidisciplinary team, it
will be evident to both investigators and participants to which group they have been
assigned. However there are still aspects of the trial that can be concealed from patients and
investigators, to avoid bias in implementing of the trial and interpreting the results.
In cluster randomized studies it may be possible to achieve blinding to the existence of the
trial for both groups, and blinding to the existence of an intervention, for the control group.
This was done in the study by Jordhoy et al62 as well as in our own RCT (see Chapter 6).
When possible, those assessing and recording the outcome measures should also be blinded
to group assignment.
As much as possible, aspects of the trial which could normally be carried out by the
investigators should be performed independently to avoid bias. For example, the
randomization sequence should be generated by a statistician rather than directly by the
investigators, using a random numbers table or computer program. A coin toss has been
used to assign groups in cluster randomized studies with small numbers of clusters,9 but is
particularly susceptible to bias if implemented by the investigators. For individually

106
randomized trials randomization should be implemented by calling a central number, rather
than by sealed envelopes which are vulnerable to bias.217 Lastly, there should always be an
independent data and symptom monitoring board to monitor the trial for benefit and harm.
Conclusion
Randomized controlled trials provide high-grade evidence about the effectiveness of
pharmacologic and non-pharmacologic interventions; however, this is only the case if such
trials are properly designed and achieve sufficient power. Although such trials are
particularly challenging to conduct in palliative care populations, there have been well
designed trials that have shown that this is possible,103,111 and pilot trials indicating that
further research is underway.13,210 Although patients with advanced cancer constitute a
vulnerable population, and there are valid concerns about the ethical conduct of research in
this group,218 it is perhaps even more unethical to administer a treatment to the terminally ill
or any other population without sound evidence for its efficacy219 - something that due to
lack of research studies occurs all to often in palliative care. We hope that this paper will
provide encouragement and guidance to those planning RCTs in palliative care or related
disciplines.

107
Chapter Ten
Conclusions
108
CONCLUSIONS
My aim with this thesis has been to make a contribution towards the rigorous evaluation of
evidence for the effectiveness of palliative care in the treatment of patients with advanced
cancer. Under the supervision of my committee and together with my research team, I have
systematically reviewed the literature and identified areas for improvement of RCTs
assessing palliative care effectiveness. We have also successfully completed a phase II trial
of palliative care effectiveness, which has shown effectiveness of our intervention for
symptom control and patient satisfaction at one week and one month. In addition, we have
identified predictors of symptom control and of quality of life, which need to be taken into
account in the design or analysis phase of RCTs assessing palliative care effectiveness. We
have validated a measure of patient satisfaction with palliative care, which is sensitive to
change and can be used in clinical trials in outpatients with advanced cancer. Using
information from all of these studies, we have developed recommendations for those
planning RCTs in palliative care populations.
Currently there is insufficient evidence for the benefit from specialized care for
quality of life and satisfaction with care. However, studies have lacked methodological
rigour, limiting the conclusions that can be made. Health services research in this area is
highly needed and although RCTs in this setting are challenging to plan and carry out, the
increasing quality of studies in recent years is encouraging. In addition to well-designed
trials, further research is needed regarding the development of appropriate validated
outcome measures and of interventions representing various models of care delivery.
Specific directions for further research by our research team will be discussed in the next
chapter.

109
Chapter Eleven
Future Directions

110
FUTURE DIRECTIONS
This thesis has provided a starting point for further studies regarding health services
research in palliative care. Future directions for this research include completing the
ongoing RCT, assessing barriers to palliative care referral as perceived by referring
oncologists, developing palliative care research in other populations, and developing
measures to adequately assess palliative care interventions.
My foremost goal will be to complete the ongoing cluster randomized trial. We will
use the information from the phase II trial and analyses of baseline data to inform the
completion of the study and the analyses of the data. We have also added a qualitative
component to the randomized trial, which will be completed by patients and caregivers at
study-end and will complement the quantitative findings. Although it has been
acknowledged that qualitative methods are valuable in providing information that cannot be
retrieved using quantitative measures,220-222 and that mixed methods are likely to produce
the most comprehensive picture of the effects of a palliative care intervention or service,223
only one trial of a palliative care team has used such methods to complement its quantitative
findings.224 We will conduct open-ended individual qualitative interviews in a subset of
approximately 80 subjects (20 patients and 20 caregivers from both the intervention and the
control groups) at the end of the 4-month follow-up period. Patients and caregivers will be
selected using a quota sampling method225 so that approximately equal numbers in each
group will consist of younger and older men and women and will have low and high scores
on the quality of life measures (FACT-G measure for patients; SF-36 for caregivers). A
grounded theory approach will be used,226,227 and theoretical sampling will be used to

111
determine the sample size at saturation (i.e. when no new themes are recognized).227,228 The
qualitative component will enrich the findings, by addressing aspects of quality of life
and/of quality of care that may not have been covered by the questionnaires, and by
obtaining opinions of patients about the appropriateness of early palliative care referral.
I am also planning a survey of Canadian oncologists to better understand availability
of palliative care services, referral practices to specialized palliative care, and barriers to
referral earlier in the disease course. The survey will be sent to members of the Canadian
Association of Medical Oncologists, Canadian Association of Radiation Oncologists,
Canadian Haematological Society, and the Canadian Society of Surgical Oncology. We
have created a survey instrument to identify Palliative Care referral practices, attitudes and
important physician characteristics (see Appendix); no such previous validated instrument
exists. The survey was designed to assess the domains of (1) physician demographics,
training, and nature of oncology practice; (2) availability and nature of palliative care
services; (3) palliative care referral practices; and (4) opinions about palliative care services.
Results from this survey will be used to understand gaps that exist in the current method of
palliative care provision in Canada, and to improve coordination of care for patients with
incurable cancer.
Another population that would benefit from palliative care is patients with
haematological malignancies. Patients with leukemia are typically referred to palliative care
services less frequently and later in the disease course than patients with solid tumours, and
there has been scant palliative care research in this population. In collaboration with Dr.
Gary Rodin, I am conducting a prospective longitudinal study (C. Zimmermann, Gary
Rodin, co-PI’s, CIHR) to evaluate the palliative care and psychosocial oncology needs of
patients with acute myelogenous leukemia (AML), which has a median life expectancy of

112
11 months from diagnosis. We are monitoring traumatic stress reactions, depression and
physical symptoms in patients with AML and to what extent they are related to discrete
events in the disease course. We are recruiting 400 patients from outpatient haematology
clinics over a 36-month period, who will be followed every 1-3 months for 18 months or
until death. We are also conducting qualitative interviews to assess the patient’s experience
of communication with their health care providers. The aim of this study is to evaluate
prospectively physical and psychological distress in patients with AML, using both
qualitative and quantitative methods, and to identify factors which contribute to or mitigate
their suffering. The longitudinal design will allow us to test a causal model and identify
targets for proactive palliative care intervention, which will lead to both clinical practice
recommendations and funded randomized clinical trials for patients with acute leukemia.
Other longer-term goals include the creation and validation of additional measures
for palliative care. We have validated the FAMCARE-P measure of patient satisfaction with
outpatient oncology palliative care; we are currently in the process of developing a measure
of satisfaction with inpatient palliative care to be used in palliative care units. This will be
done using qualitative interviews with patients and their caregivers, as well as focus groups
with health care providers.
Palliative care is a rapidly developing field both clinically and in terms of research.
To date, the clinical development has been more rapid than the corresponding evidence
base. With this thesis I am hoping to make a contribution towards the latter.

113
Appendix 1
Preliminary validation of the FAMCARE-Patient scale
Published previously as:
Lo, C., Burman, D., Rodin, G., and Zimmermann, C. Measuring patient satisfaction in
oncology palliative care: Psychometric properties of the FAMCARE-Patient scale.
Qual Life Res. 2009 Aug;18(6):747-52
Contributions: For this paper I conceived the idea for the study, supervised data analyses,
wrote the Introduction and Discussion sections, and edited the final version.

114
ABSTRACT
Purpose: We provide preliminary psychometric results concerning the use of a modified
FAMCARE scale, adapted for patient use, to assess satisfaction with outpatient care in
advanced stage cancer patients.
Methods: Participants were 145 outpatients with advanced cancer who were participating in
a phase II trial of an outpatient palliative care intervention. Patients completed our modified
FAMCARE measure of patient satisfaction and the Edmonton Symptom Assessment Scale,
a measure of symptom burden. Individuals were also assessed for performance status using
the Eastern Cooperative Oncology Group scale. We conducted an exploratory factor
analysis of the patient satisfaction measure, and report correlations of satisfaction with
symptom burden as well as with performance status.
Results: Factor analysis of the satisfaction measure revealed a one-factor structure and
suggested the removal of one non-loading item, producing a 16-item scale (FAMCARE-
P16) with high internal reliability. Patient satisfaction was not correlated with performance
status, but was inversely associated with symptom burden, particularly with depression and
anxiety.
Conclusions: The FAMCARE-P16 may be used to assess satisfaction with outpatient
palliative care interventions of patients with advanced stage cancer in both clinical settings
and prospective trials.

115
Introduction
Satisfaction of patients and caregivers is an important indicator of quality of care,
and may be particularly relevant for patients whose disease is not curable.57,229 Satisfaction
with palliative care is related to other constructs such as quality of life52 and quality of
death,53 but is a distinct concept that includes accessibility, coordination and
personalization of care, symptom management, communication and education, emotional
support, and support of decision-making.54 Although patient satisfaction with care has
been shown to be amenable to change with palliative care interventions,18 there is a lack of
instruments specific to the context of palliative care, resulting in reliance on unvalidated
measures or measures not specific for pallaitive care settings.18,54
The FAMCARE scale34 is a 20-item self-report measure that was developed to
measure family satisfaction with palliative cancer care.230,231 Validation of the measure has
shown that 19 of the 20 items load onto a single factor assessing family satisfaction.37 The
FAMCARE is generally administered to family members one month after the death of the
patient.55,56 However, limitations of such retrospective evaluations include the risk of
recall bias,57 the potential influence of grief on perceptions,54 difficulty contacting grieving
families, and the absence of the patient’s perception in the evaluation. Although in some
studies the FAMCARE has been administered prospectively,58,59 and to patients,38 the
measure has not previously been validated for this purpose. Given the paucity of validated
measures of patient satisfaction with palliative oncology care, we developed and tested a
new measure of patient satisfaction, which we generated by selectively modifying the
original FAMCARE items.

116
We report an exploratory psychometric analysis of our FAMCARE-Patient
(FAMCARE-P) scale, which we administered to a sample of advanced cancer outpatients
receiving palliative care in a phase II trial [16].210 We hypothesized that the FAMCARE-P
would: (1) possess a one-factor structure, consistent with Ringdal et al.'s (2003) findings
for the original FAMCARE; and (2) negatively correlate with measures of symptom
burden and functional disability.
Methods
Patient Selection and Study Procedures
The sample consisted of patients participating in a phase II study evaluating the
efficacy of an outpatient palliative care intervention in metastatic cancer.210 Between July
2006 and April 2007, 204 patients were approached upon initial referral to the Oncology
Palliative Care Clinic (OPCC) at Princess Margaret Hospital, Toronto, Canada; 150 agreed
to participate; of those who declined, 31 were not interested, 18 were too ill, and 5 stated
they had insufficient time. Eligible outpatients had metastatic cancer, were at least 18
years old, and were fluent in English. Although cognitive status was not specifically
measured, patients were sufficiently cognitively intact to provide informed consent.
Patients were interviewed by research staff who evaluated the Eastern Cooperative
Oncology Group performance status. Patients completed the Edmonton Symptom
Assessment Scale and FAMCARE-P scales at baseline, and one week and one month after
their OPCC consultation. All analyses for this study were conducted on baseline measures,
which were completed in the clinic waiting room, before any contact with the palliative
care team. Study approval was granted from the University Health Network Research

117
Ethics Board, and patients provided written, informed consent. Table 1 shows the baseline
characteristics of the sample.
The FAMCARE-Patient Scale
We modified the original 20-item FAMCARE scale by rewording relevant items to
assess the patient’s satisfaction with care rather than that of the family member (e.g., “the
patient’s pain relief” was changed to “your pain relief”). The original scale contained the
following items: “availability of doctors to the family,” “availability of nurses to the
family,” and “availability of the doctor to patient.” In our modified scale, we rephrased
these to read: “availability of doctors to answer your questions,” “availability of nurses to
answer your questions,” and “availability of the doctor to your family.” We excluded the
following items: item 14, “time required to make a diagnosis;” item 6, “availability of a
hospital bed;” and item 7, “family conferences held to discuss the patient’s illness.” Item
14 was excluded because Ringdal et al. (2003) found in their psychometric analyses of the
original FAMCARE scale that this item did not cohere with other FAMCARE items.
Items 6 and 7 were dropped because they were not considered to be as relevant in a
prospective outpatient setting, and family inclusion in decision-making was already
assessed in item 15, “the way the family is included in treatment and care decisions.”
These changes resulted in an initial FAMCARE-Patient satisfaction scale with 17 items.
Each item was rated from 1 (very dissatisfied) to 5 (very satisfied).
118
Other Measures
The Eastern Cooperative Oncology Group (ECOG) scale is a 6-point measure
ranging between 5 (dead) and 0 (fully active) that assesses the patient's ability for self-care
and ambulation.32
The Edmonton Symptom Assessment System (ESAS) is a validated, self-
administered instrument to measure the severity of common symptoms in patients with
advanced incurable illness.35 The scale ranges between 0 (best) and 10 (worst), and
assesses 9 main symptoms (pain, fatigue, drowsiness, nausea, anxiety, depression,
appetite, dyspnea, sense of well-being) and one “other” symptom.33 For this study, the
“other” symptom item was replaced by two items rating insomnia and constipation, which
were graded using the same 0-10 scale. Since no time window is stipulated on the ESAS
form, we added instructions that symptoms were to be rated based on the previous 24-hour
period.210 The ESAS Distress Score (EDS) was calculated by summing the ratings on the 9
main symptoms (excluding insomnia and constipation), multiplying by nine (the number
of possible items), and dividing by the total number of items completed.33
Statistical Analyses
Analyses were conducted in SAS 9.1. Individuals with more than 25% missing
items on the FAMCARE-P were removed from further study, leaving a sample of 145
participants, of whom 32 had missed one item, 15 had missed two items, 8 had missed
three items and 5 had missed four items. Missing values were multiply imputed by the
Markov Chain Monte Carlo method with PROC MI.232 For simplicity, we only report the
results from a single imputation because the pattern of results was the same across multiple

119
imputations. The findings did not substantively change when analyzing individuals with
only complete data. There were no missing ECOG data and negligible missing ESAS data
(4 individuals had missed one item and 2 had missed two items).
An exploratory factor analysis (EFA) with principal axis factoring was conducted
on the 17 items to determine their factor structure. Items loading poorly on a factor (i.e.,
loadings <0.40) were dropped from further analysis. Factor-based scores were calculated
by summing relevant items. Correlations were calculated between factor-based scores and
measures of performance status and symptom burden.
Results
The scree plot and eigenvalue ≥1 criterion indicated the presence of a single
dominant factor, which explained 80% of the variance in the 17 items. Table 2 shows the
loadings on this single satisfaction factor. Item 1 loaded poorly and was dropped,
producing a 16-item scale, the FAMCARE-P16. The FAMCARE-P16 items were summed
and descriptive statistics for this variable, including internal reliability and percentage of
generally satisfied individuals, are shown in Table 1. Consistent with previous
approaches,37 we identified individuals scoring ≥64 as generally satisfied because this cut-
off value is associated with rating 4 (satisfied) on all 16 items. The FAMCARE-P16 was
uncorrelated with ECOG but was inversely correlated with ESAS, r= -0.19, p=0.02.
Correlations between the FAMCARE-P16 and individual ESAS symptoms indicated that
satisfaction was significantly, inversely associated with depression, r= -.18, p=0.03, and
anxiety, r= -0.20, p=0.01, and marginally, inversely associated with fatigue, r= -.16,
p=0.06, and appetite, r= -0.15, p=0.07.

120
Discussion
We have reported preliminary results concerning a modified FAMCARE scale for
assessing patient satisfaction with care in advanced stage cancer outpatients. Consistent
with our hypotheses, we found that the items of the FAMCARE-P cohered into a single
patient satisfaction factor, except for one item concerning satisfaction with pain relief. Of
note, the latter is the sole item that relates to the outcome rather than the structure and
process of care.57 We dropped the pain relief item and the resulting 16-item scale
demonstrated high internal reliability. Although the resulting scale does not measure the
outcome of care delivery to patients with advanced cancer, improvement in pain and other
symptoms can perhaps best be assessed directly with specific measures,33,233,234 rather than
indirectly by measuring satisfaction with these outcomes. Patient satisfaction was
inversely associated with symptom burden on the ESAS, particularly with lower
depression and anxiety, suggesting that these psychological symptoms may have the
greatest impact on patient satisfaction. The directionality of the relationship between
psychological distress and patient satisfaction cannot be determined in a cross-sectional
study of this kind and deserves further exploration.
Assessment of satisfaction can be problematic, due to ceiling effects, subjective
variability in defining satisfactory care, reluctance of patients to criticize their care
providers, and the possibility of satisfaction with care that is suboptimal according to
established standards.235,236 However, in this study only 55% of patients expressed general
satisfaction with care at baseline, allowing for the possibility of improvement. Indeed, in
our phase II study using this measure, there was improvement in satisfaction one week

121
after an outpatient palliative care clinic intervention in 12 of the 16 items, with a
statistically significant improvement in the overall score, demonstrating sensitivity of this
scale to change.210
A limitation of the present study is that our approach towards scale construction
and revision, although expedient, may not be as rigorous as other methods (e.g., generating
and testing new items based on cognitive interviews with patients). As such, there are
aspects of palliative care interventions (e.g., psychosocial and spiritual care) relevant to
patient satisfaction which are not assessed by the current instrument. Therefore, depending
on the palliative care outcome of interest, further patient satisfaction instruments may be
necessary to address these domains. As well, when used clinically, we recommend that the
scale be accompanied by direct measures of psychological and physical symptom relief.
The FAMCARE-P specifically measures patient satisfaction with palliative care
and can be used in palliative care outpatient settings both clinically and for research
studies. Although several measures exist for measuring patient quality of life145,237 and
quality of death238 in palliative care settings, these constructs are distinct from the
construct of patient satisfaction with care.53,54 As well, although there are existing
instruments for measurement of satisfaction with oncology inpatient and outpatient
care,239-241 and for care in intensive care unit settings,242 these are not suitable for use by
palliative care physicians in palliative care clinic settings. Similar to the FAMCARE, the
FAMCARE-P is specifically indicated for measurement of satisfaction with palliative
cancer care, and includes items that are considered to be important for measuring patient
satisfaction, including accessibility, coordination of care, symptom management,
communication and education, and support of decision-making.54 In view of the increasing

122
interest in palliative outpatient care,6,8,9,13 and in intervention studies with specialized
palliative care as an intervention,18 a validated and specific measure of patient satisfaction
with palliative care, such as the FAMCARE-P, is needed and has potential to improve
methodologic rigour in this field.
In conclusion, we are providing preliminary results of psychometric properties for
a new patient satisfaction measure that may be used to assess satisfaction with outpatient
palliative care interventions in patients with advanced cancer. Future research should
consider further scale validation.

123
Table 1: Baseline characteristics of participants (N=145)
Characteristic N (%) Min-Max α
SexFemale 72 (49.7)Male 73 (50.3)
Age Mean (SD) 61 (13) 31-90
Married/common-law 99 (75.0)
Disease siteGastrointestinal 48 (33.1)Breast 26 (17.9)Lung 22 (15.2)Gynecological 7 (4.8)Genitourinary 7 (4.8)Other 35 (24.1)
Performance status (ECOG) Mean (SD) 1.8 (0.92) 0-4
ESAS Distress Score Mean (SD) 40 (18) 2-79 0.83
FAMCARE-P16 Score Mean (SD) 63 (23) 23-80 0.94
FAMCARE-P16 Score ≥ 64 79 (54.5)
α = Cronbach’s alpha; maximum possible score for EDS = 90; maximum possible score for FAMCARE-P16 =
80.

124
Table 2: Factor loadings for the initial pool of 17 items.
Item Loading
1. Your pain relief 0.30
2. Doctor’s attention to your description of symptoms 0.72*
3. How thoroughly the doctor assesses your symptoms 0.76*
4. Information given about how to manage pain 0.64*
5. Information given about side effects 0.75*
6. Speed with which symptoms are treated 0.76*
7. Information given about your tests 0.69*
8. The way tests and treatments are performed 0.61*
9. The way tests and treatments are followed up by the doctor 0.73*
10. Information provided about your prognosis 0.80*
11. Answers from health professionals 0.79*
12. Referrals to specialists 0.68*
13. The availability of doctors to answer your questions 0.76*
14. The availability of nurses to answer your questions 0.59*
15. The way the family is included in treatment and care decisions 0.65*
16. Coordination of care 0.70*
17. The availability of the doctor to your family 0.80*
Note. Factor loadings ≥ .40 are marked with an asterisk.

125
Appendix 2
Confirmatory validation of the FAMCARE-Patient scale
Published previously as:
Lo, C., Burman, D., Hales, S., Swami, N., Rodin, G., Zimmermann, C. The FAMCARE-
Patient scale: measuring satisfaction with care of outpatients with advanced cancer.
Eur J Cancer. 2009 Sep 26 [epub ahead of print]
Contributions: For this paper I conceived the idea for the study, supervised data analyses,
wrote the Introduction and Discussion sections, and edited the final version of the paper.

126
ABSTRACT
Objective: To provide confirmatory results concerning the psychometric properties of a
measure of satisfaction with oncology care for use with advanced stage cancer patients, and
test its sensitivity to change.
Methods: We analyzed data from 315 outpatients with advanced cancer participating in a
randomized controlled trial of early palliative care intervention versus routine oncology
care, and their caregivers. Patients completed a 16-item measure of patient satisfaction
(FAMCARE-P16), based on the FAMCARE measure of family satisfaction with cancer
care, and measures assessing communication and relationship with healthcare providers,
performance status and symptom burden. Caregivers completed the original FAMCARE
measure. We used confirmatory factor analysis to test the patient satisfaction measure for a
single factor structure. To determine construct validity, we assessed correlations between
patient satisfaction and the other patient and caregiver measures. To assess responsiveness
to change, we repeated paired t-test analyses on the 13-item scale and 16-item scale for 150
patients participating in a phase II trial of palliative care effectiveness, in which the
FAMCARE-P had been measured at baseline, one week and one month after an outpatient
palliative care intervention.
Results: A reduced 13-item version of our measure (FAMCARE-P13) possessed a one-
factor structure with high reliability. Patient satisfaction was correlated in predicted
directions with physical distress, communication and relationship with healthcare providers,
and caregiver satisfaction. There were statistically significant increases in patient
satisfaction at one week (p<0.0001) and one month (p<0.001).

127
Conclusions: We recommend the use of the FAMCARE-P13 to assess satisfaction with
outpatient palliative care interventions of patients with advanced stage cancer.

128
INTRODUCTION
Effectiveness of oncology care has traditionally been measured in terms of
biomedical outcomes, such as survival and disease-free survival. However, the importance
of patient and family-reported outcomes for clinical trials in oncology is increasingly
acknowledged, and such outcomes are increasingly incorporated into cancer clinical
trials.243,244 Subjective outcomes are particularly important in the palliative setting, where
the focus is explicitly on quality of life for the patient and family.97
In studies assessing the effectiveness of palliative care interventions, relevant patient
outcomes include symptom control, quality of life, quality of death and satisfaction with
care.18,33,53,54 The most consistent improvement has been shown for satisfaction with care,18
which is a distinct concept encompassing symptom management, emotional support,
communication, accessibility and coordination of care, and support of patients’ decision-
making.54 However, a hindrance in the assessment of satisfaction with palliative cancer care
has been the lack of measures that are validated specifically for patients with advanced
cancer.216
In a previous study,202 we explored the psychometrics of the FAMCARE-Patient
(FAMCARE-P) scale, a measure of patient satisfaction which we constructed based on the
20-item FAMCARE measure for family satisfaction with care.34 We selectively modified
the FAMCARE items for patient use, and found that 16 items formed a scale with a single-
factor structure and high internal reliability. The FAMCARE-P was used in a phase II trial
of an outpatient palliative care clinic intervention, and was responsive to change,
demonstrating a significant improvement in patient satisfaction at both one week and one
month.210

129
The purpose of the current study was to take a confirmatory approach towards
assessing the factor structure of the FAMCARE-P, and to examine in detail its construct
validity in a sample of outpatients with advanced cancer and their primary caregivers. We
hypothesized that the FAMCARE-P would: (1) show a single factor structure; (2) correlate
negatively with measures of symptom burden and functional disability; (3) correlate
positively with measures assessing the quality of communication and quality of
relationships with healthcare providers; and (4) correlate positively with caregiver
satisfaction with oncology care.
PATIENTS AND METHODS
Participants and Procedure
The sample for this study is comprised of patients with advanced cancer and their primary
caregivers participating in an ongoing cluster randomized controlled trial of early palliative
care intervention versus routine oncology care. Patients with advanced cancer were
recruited from 24 outpatient oncology clinics at Princess Margaret Hospital, Toronto, and
randomized either to immediate consultation and follow-up by a palliative care team, or to
conventional cancer care. Inclusion criteria were metastatic gastrointestinal, genitourinary,
breast, lung or gynecological cancer (for lung cancer, Stage IIIA and B were included), age
≥18 years, Eastern Cooperative Oncology Group (ECOG) performance status from 0 to 2,
and a prognosis of 6 months to 2 years (estimated by the primary oncologist). Patients with
metastatic breast or prostate cancer were also refractory to hormonal therapy; patients with
locally advanced pancreatic cancer were included. Exclusion criteria were insufficient
English literacy to complete the questionnaires, and inability to pass the cognitive screening
test (Short Orientation-Memory-Concentration Test (SOMC) score <20 or >10 errors).143
130
Approval for this study was granted from the University Health Network Research
Ethics Board. Patients completed measures of quality of life, symptom burden, and
satisfaction with care monthly for 4 months. Primary caregivers of consenting patients were
also approached for participation, and were asked to complete measures of their own quality
of life and satisfaction with the patient's care. Between 1-Dec-2006 and 30-Apr-2009, 678
patients were approached, 465 consented to participate, and 331 completed baseline
questionnaires. During the same time interval, 262 caregivers were approached, 209
consented and 140 completed baseline questionnaires.
Patient Measures
The FAMCARE-P16 is a self-report scale assessing patient satisfaction with outpatient
oncology care, which is composed of 16 items rated from 1 (very dissatisfied) to 5 (very
satisfied). The items are not specific for a particular tumour type or symptom, but are
broadly relevant for outpatients with advanced cancer; the summed items produce a single
satisfaction score. A preliminary analysis indicated that the measure had good psychometric
properties when used with advanced cancer patients in an outpatient palliative care clinic.202
The Edmonton Symptom Assessment System (ESAS) is a validated, self-
administered tool to measure the severity of common symptoms in patients with advanced
illness.35 The numerical scale ranges from 0 (best) to 10 (worst), and assesses 9 main
symptoms: pain, fatigue, drowsiness, nausea, anxiety, depression, appetite, dyspnea, and
sense of well-being and one “other” symptom.33 We replaced the “other” symptom item by
two items rating insomnia and constipation, which were graded using the same 0-10 scale.
Because no time window is stipulated on the ESAS form, we added instructions that

131
symptoms were to be rated based on the previous 24-hour period.210 The ESAS Distress
Score (EDS) is the prorated sum of the 9 main symptom ratings.
The Communication with Health Care Providers (CARES) Medical Interaction
Subscale is an 11-item subscale derived from the Cancer Rehabilitation Evaluation
System.150 It assesses whether or not patients experience problems in their interactions with
their nurses and doctors, including problems related to information seeking and active
participation in medical care.
The QUAL-E is a 26-item validated self-report measure of quality of life at the end
of life, which contains items in four domains: life completion, symptoms impact,
relationship with health provider and preparation for end of life.145 We used the 5-item
relationship with healthcare provider subscale, which assesses the degree to which
individuals feel that they have access to information about their illness and can participate in
treatment decisions.
The Eastern Cooperative Oncology Group (ECOG) scale is a 6-point measure
ranging between 5 (dead) and 0 (fully active) that assesses the patient's ability for self-care
and level of ambulation.32
Caregiver Measures
Caregivers were asked to fill out 19 items from the original 20-item FAMCARE scale34 to
assess their satisfaction with oncology care. We dropped the item “time required to make a
diagnosis” because Ringdal et al. found this item to be poorly associated with the other
FAMCARE items in their validation study.37 We refer to this measure as the FAMCARE-
C19.

132
Statistical Analyses
We conducted our analysis of the baseline measures in SAS 9.1 (SAS Institute,
Cary, NC). Individuals with more than 25% missing items on the FAMCARE-P16 were
removed from analysis, leaving a final sample of 315 participants. Missing values were
multiply imputed by the Markov Chain Monte Carlo method with PROC MI.232 We only
report the results from a single imputation because the pattern of results was the same across
multiple imputations. The findings did not change substantively when analyzing patients
with only complete data. Satisfaction scores were calculated for 136 of the 140 caregivers (4
were excluded due to greater than 50% missing items).
A confirmatory factor analysis (CFA) was used to test for the presence of a single
factor in the FAMCARE-P16. The fit of a single factor structure to the data was evaluated
using goodness of fit indices. A good fit is indicated by a Comparative Fit Index (CFI)
greater than 0.95, a Non-Normed Fit Index (NNFI) greater than 0.95, and a Root Mean
Square Error of Approximation (RMSEA) less than 0.06. An acceptable fit is indicated by
CFI and NNFI between 0.90 and 0.95, and RMSEA between 0.06 and 0.10.245 When there
was poor fit, modification indices were consulted and items displaying problematic local
dependencies were identified.246,247 Selected items were dropped or allowed to have
correlated error terms. This produced a 13-item scale, which was re-tested for a one factor
structure using CFA. Summed patient satisfaction scores were computed for the 13-item and
16-item scales, and correlations were calculated with measures of performance status,
symptom burden, communication and relationship with healthcare providers, and caregiver
satisfaction.
To assess the responsiveness of the scale to change, we reexamined data from the
phase II trial of palliative care effectiveness210 in which the FAMCARE-P had been

133
measured on three occasions: at baseline, and at one week and one month after an outpatient
palliative care intervention. We repeated our paired t-test analyses and report on the changes
in the 13-item scale and 16-item scale from baseline to one week and from baseline to one
month.
RESULTS
Table 1 reports the characteristics of the patient and caregiver samples. The CFA indicated
that a one factor structure had a poor fit to the FAMCARE-P16, with CFI=0.88, NNFI=0.86
and RMSEA=0.11, despite all items having significant loadings on the common factor.
Modification indices revealed that the lack of fit was attributable to certain items having
correlated error terms; that is, certain pairs or clusters of items continued to exhibit
associations with each other, beyond what could be accounted for by an overall common
factor, and yet these associations were not strong enough to produce separate factors. Such
local item dependencies can occur when pairs or groups of items are highly similar in
content, target or topic.247
We examined the ten most problematic item pairs. Item 15 (Coordination of care)
and item 16 (The availability of doctors to your family) exhibited multiple dependencies
with other items, and were excluded from further analysis. However, the three most
problematic item pairs remained unaddressed. Item 1 (Doctor’s attention to your description
of symptoms) and item 2 (How thoroughly the doctor assesses your symptoms) were overly
redundant. Item 1 was dropped because the thoroughness of the doctor’s symptom
assessment subsumes the issue of the doctor’s attending to the description of symptoms.
Item-pair 3 (Information given about how to manage pain) and 4 (Information given about
side effects) was also problematic, as was item-pair 9 (Information provided about your

134
prognosis) and 10 (Answers from health professionals), but it was unclear which item in
each pair should be dropped. We therefore kept these items and specified correlated error
terms within each pair. With these changes, a one factor model had acceptable fit to the
remaining 13 items, CFI=0.95, NNFI=0.94, RMSEA=0.076. Table 2 presents the
standardized factor weights for each item. We refer to this reduced scale as the FAMCARE-
P13 (see Appendix). Internal reliabilities for the 16-item and 13-item scales were high, with
Cronbach’s alpha 0.94 and 0.93, respectively.
We calculated summed scores for the FAMCARE-P16 and FAMCARE-P13, and
correlated them with ECOG, EDS, individual ESAS items, CARES Medical Interaction
subscale, QUAL-E relationship with healthcare provider subscale, and FAMCARE-C19
(see Table 3). All correlations were significant and in the predicted directions. Greater
patient satisfaction was associated with better communication and relationship with
healthcare providers, higher performance status, lower symptom burden (especially anxiety
and well-being), and greater caregiver satisfaction with oncology care. Finally, we identified
patients scoring ≥64 on the FAMCARE-P16 as generally satisfied, because this cut-off
value is associated with rating 4 (satisfied) on all 16 items: 62% of patients were
categorized as generally satisfied. We similarly identified patients scoring ≥52 on the
FAMCARE-P13 as generally satisfied: 63% were categorized as generally satisfied.
To assess the responsiveness of the 13-item scale to change, we reanalyzed the data
from our phase II trial of palliative care effectiveness.210 Relative to baseline, we found
statistically significant increases in the 13-item scale at one week, M=4.4, CI.95 (2.5, 6.3),
p<0.0001, and at one month, M = 3.6, CI.95 (1.5, 5.8), p=.0009. We also found significant
increases in the 16-item scale at one week, M = 5.7, CI.95 (3.4, 8.0), p<0.0001, and at one
month, M=4.7, CI.95 (2.1, 7.2), p=0.0004.

135
DISCUSSION
This study was a confirmatory analysis of the factor structure and validity of a new measure
of patient satisfaction in a sample of cancer outpatients with advanced cancer. We examined
the functioning of the FAMCARE-P and found that a reduced 13-item version fit the
hypothesized one factor model. Both the 13-item and the 16-item scales were associated in
hypothesized directions with related constructs, including symptom severity, satisfaction
with communication, caregiver satisfaction, and patient quality of life as determined by
relationships with healthcare providers. We recommend use of the 13-item scale (see
Appendix) due to its brevity and stronger one-factor structure; however, both scales are
appropriate in clinical and research settings to measure the effectiveness of outpatient
oncology palliative care.
The present study revealed stronger relationships between patient satisfaction and
symptom burden, and between patient satisfaction and functional disability than our initial
exploratory study of the FAMCARE-P16 in patients with advanced cancer.202 This may be
due in part to the fact that the sample size for the current study was more than twice the size
of that in the preliminary study. It is also noteworthy that patients in the present study had
less advanced disease than patients in the earlier study. In another study measuring
satisfaction with care in medical inpatients at the end of life, it was similarly found that
satisfaction was not related to depression or anxiety and only weakly associated with
symptom severity.248 When patients with advanced cancer are being treated relatively early
in the disease course, their satisfaction with care may depend more on the effectiveness of
treatment to reduce physical distress. However, when such patients are treated later in the
136
disease trajectory, when progressive physical deterioration can be expected, individuals may
begin to evaluate their quality of care based less on their actual physical health.
It is important to distinguish satisfaction with care from related constructs of quality
of life, quality of death and quality of care. Quality of life is measured subjectively, and
includes the domains of physical, psychological, social and functional well-being. In
palliative care, spiritual and existential well-being has been described as an additional
domain of importance.137,146 Quality of death is generally measured by the family member
after the death of the patient, and encompasses physical, psychological, social, and spiritual
experiences; the nature of health care, life closure and death preparation; and the
circumstances of death.53 Satisfaction with care assesses the fulfillment of individual needs
and expectations of those receiving care by means of indirect or direct questions about the
quality of care provided.235 Quality of care includes not only aspects of care relevant at the
individual level, but also concepts such as equity, which are important at the societal
level.249 For this reason and for others, such as individual differences in perception of
satisfaction and reluctance of patients to criticize health care providers, satisfaction with
care is an incomplete indicator of the quality of care of a particular health service.
Nonetheless it is an important measure of whether a particular service meets the needs and
expectations of patients and/or families under its care.
Validated measures exist to measure quality of life for patients with cancer122,250
including in palliative care,145,251 and for measuring quality of death238 but these are not
appropriate for directly measuring satisfaction with care. A measure has also been
developed to measure quality of care at the end of life.252 However quality of care is not
defined in this paper, and the 16-item measure includes items such as “Have you a close
relationship with your family?”, “Have you spent a lot of time with your family?”, “Have

137
you felt that you life is meaningful and valuable” and “Have you been dealing well with
finishing touch on your life?”, which are similar to items usually used for quality of life
measures, and do not link quality of life specifically to care from the medical team.
Although there are existing measures of patient satisfaction with oncology care,
none are specific for the palliative care outpatient setting. Some validated measures of
satisfaction with palliative care are designed for use by family members rather than by
patients.34,253 The QUEST (Quality of End-of-life care and satisfaction with treatment scale)
measures patient satisfaction with care by physicians and nurses, but was designed and
validated specifically for inpatient use at the end of life.248 Several scales measure patient
satisfaction with outpatient oncology care, but one refers only to care as it relates to
treatment by physicians,254 one is very long, with 60 items in total,255 one is intended to
evaluate patients’ experiences when taking anticancer therapy,256 and none are specifically
for patients in palliative outpatient settings.254-256 In a recent systematic review of studies
assessing satisfaction with care at the end of life,54 only one study used a measure designed
for the end of life, which was a retrospective measure of family satisfaction with care (an
item from the Toolkit Afterdeath Survey).111 Thus this validation of the FAMCARE-P will
provide a measure for outpatient oncology palliative care, which was previously not
available.
A limitation of our study is that this scale was developed from a previously existing
scale for that was designed for retrospective use by family members after the death of the
patient, rather than from direct interviews with patients. However the FAMCARE has face
value for use prospectively and with patients, and has been used previously in this
way.38,58,59 Our finding that the scale is sensitive to change after care provided by a
palliative care team indicates that it is useful for assessing patient satisfaction in trials of

138
palliative care interventions. As previously noted, Ringdal et al. found that the one
FAMCARE item assessing satisfaction with the time required to make a diagnosis did not
relate well with other FAMCARE items,37 and this item was removed when we constructed
the initial FAMCARE P-16 scale. This omission is perhaps appropriate from a clinical
intervention perspective, in that interventions by the current clinical team are unlikely to
change satisfaction with diagnostic issues that occurred earlier in the cancer trajectory.
Issues of communication of diagnosis and prognosis are nonetheless important, and there is
an existing measure that specifically assesses satisfaction with care and communication at
the time of the diagnosis of advanced cancer and initiation of cancer-directed treatment.239
In conclusion, we have developed and validated a brief measure of patient
satisfaction. This instrument may be useful to oncology clinicians, researchers, and other
health professionals seeking to evaluate quality of care in settings where patients have
advanced and progressive disease. Because the FAMCARE-P measure does not contain
items specific to any one nation of healthcare system, it is likely relevant internationally,
similar to the original FAMCARE measure.34,37,58 Due to its responsiveness to change, it
may be particularly useful for clinical trials assessing satisfaction with oncology palliative
care.
Acknowledgement
We are grateful to all the patients who participated in this study, and to the clinical and
research staff of the Oncology Palliative Care Clinic and medical oncology clinics.
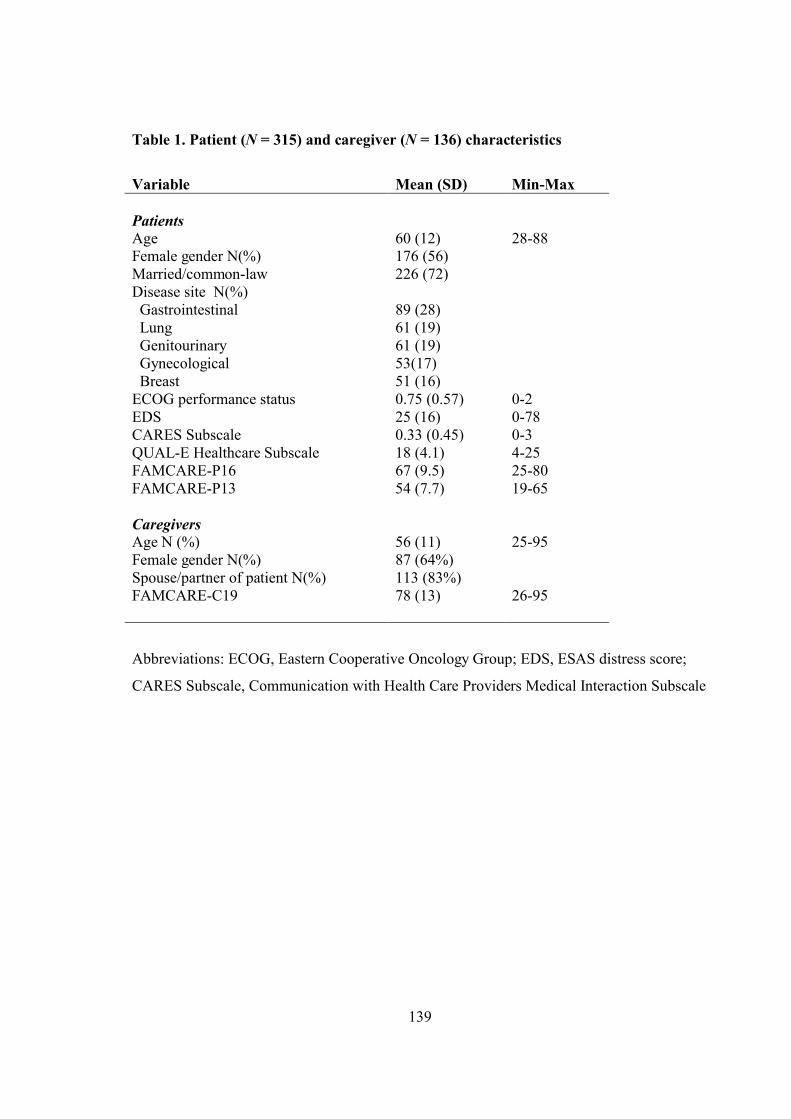
139
Table 1. Patient (N = 315) and caregiver (N = 136) characteristics
Variable Mean (SD) Min-Max
PatientsAge 60 (12) 28-88Female gender N(%) 176 (56)Married/common-law 226 (72)Disease site N(%) Gastrointestinal 89 (28) Lung 61 (19) Genitourinary 61 (19) Gynecological 53(17) Breast 51 (16)ECOG performance status 0.75 (0.57) 0-2EDS 25 (16) 0-78CARES Subscale 0.33 (0.45) 0-3QUAL-E Healthcare Subscale 18 (4.1) 4-25FAMCARE-P16 67 (9.5) 25-80FAMCARE-P13 54 (7.7) 19-65
CaregiversAge N (%) 56 (11) 25-95Female gender N(%) 87 (64%)Spouse/partner of patient N(%) 113 (83%)FAMCARE-C19 78 (13) 26-95
Abbreviations: ECOG, Eastern Cooperative Oncology Group; EDS, ESAS distress score;
CARES Subscale, Communication with Health Care Providers Medical Interaction Subscale

140
Table 2. Standardized factor weights for the items of the FAMCARE-P13
Item Weight
2. How thoroughly the doctor assesses your symptoms 0.81
3. Information given about how to manage pain 0.67
4. Information given about side effects 0.64
5. Speed with which symptoms are treated 0.69
6. Information given about your tests 0.69
7. The way tests and treatments are performed 0.55
8. The way tests and treatments are followed up by the doctor 0.78
9. Information provided about your prognosis 0.69
10. Answers from health professionals 0.85
11. Referrals to specialists 0.66
12. The availability of doctors to answer your questions 0.81
13. The availability of nurses to answer your questions 0.66
14. The way the family is included in treatment and care decisions 0.66
Note. Items 1 (Doctor’s attention to your description of symptoms), 15 (Coordination of
care) and 16 (The availability of doctors to your family) were dropped from the 13-item
reduced scale. Error terms for items 3 and 4 were correlated at 0.29. Error terms for items 9
and 10 were correlated at 0.24.

141
Table 3. Correlations with the FAMCARE-P16 and FAMCARE-P13 scales
FAMCARE-P16 FAMCARE-P13
ECOG -0.14* -0.15*
EDS -0.34** -0.36**
Individual ESAS items
Pain -0.16* -0.17*
Fatigue -0.25** -0.25**
Nausea -0.17* -0.18*
Depression -0.25** -0.25**
Anxiety -0.31** -0.32**
Drowsiness -0.24** -0.24**
Appetite -0.23** -0.24**
Wellbeing -0.33** -0.34**
Dyspnea -0.16* -0.18*
Constipation -0.12* -0.12*
Insomnia -0.12* -0.13*
CARES Medical Interaction -0.49** -0.50**
QUAL-E relationship with
healthcare provider 0.55** 0.55**
FAMCARE-C19 0.55** 0.54**
Note. Correlations with the FAMCARE-C19 were based on data from the 136 caregiver and
patient pairs. All other correlations were based on data from the 315 patients.
*p < .05. **p < .001.

142
Appendix. The 13-item FAMCARE-Patient scale (FAMCARE-P13)
1 = Very Dissatisfied, 2 = Dissatisfied, 3 = Undecided, 4 = Satisfied, 5 = Very Satisfied
How satisfied are you with:
1. How thoroughly the doctor assesses your symptoms
2. Information given about how to manage pain
3. The availability of nurses to answer your questions
4. Information provided about your prognosis
5. Speed with which symptoms are treated
6. Information given about your tests
7. The way tests and treatments are performed
8. The availability of doctors to answer your questions
9. Answers from health professionals
10. Referrals to specialists
11. The way tests and treatments are followed up by the doctor
12. Information given about side effects
13. The way the family is included in treatment and care decisions

143
References

144
References
1. Teunissen SC, Wesker W, Kruitwagen C, de Haes HC, Voest EE, de Graeff A. Symptom prevalence in patients with incurable cancer: a systematic review. J Pain Symptom Manage 2007; 34(1):94-104.
2. Lidstone V, Butters E, Seed PT, Sinnott C, Beynon T, Richards M. Symptoms and concerns amongst cancer outpatients: identifying the need for specialist palliative care. Palliat Med 2003; 17(7):588-595.
3. Whitmer KM, Pruemer JM, Nahleh ZA, Jazieh AR. Symptom management needs of oncology outpatients. J Palliat Med 2006; 9(3):628-630.
4. Saunders C. The moment of truth: care of the dying person. In: Pearson L, editor. Death and dying: Current Issues in the Treatment of the Dying Person. Cleveland: Case Western Reserve University Press; 1969: 49-78.
5. Mount BM. The problem of caring for the dying in a general hospital; the palliative care unit as a possible solution. Can Med Assoc J 1976; 115(2):119-121.
6. Strasser F, Sweeney C, Willey J, Benisch-Tolley S, Palmer JL, Bruera E. Impact of a half-day multidisciplinary symptom control and palliative care outpatient clinic in a comprehensive cancer center on recommendations, symptom intensity, and patient satisfaction: a retrospective descriptive study. J Pain Symptom Manage 2004; 27(6):481-491.
7. Bruera E, Michaud M, Vigano A, Neumann CM, Watanabe S, Hanson J. Multidisciplinary symptom control clinic in a cancer center: a retrospective study. Support Care Cancer 2001; 9(3):162-168.
8. Casarett DJ, Hirschman KB, Coffey JF, Pierre L. Does a palliative care clinic have a role in improving end-of-life care? Results of a pilot program. J Palliat Med 2002; 5(3):387-396.
9. Rabow MW, Dibble SL, Pantilat SZ, McPhee SJ. The comprehensive care team: a controlled trial of outpatient palliative medicine consultation. Arch Intern Med 2004; 164(1):83-91.
10. Moore S, Corner J, Haviland J, Wells M, Salmon E, Normand C et al. Nurse led follow up and conventional medical follow up in management of patients with lung cancer: randomised trial. BMJ 2002; 325(7373):1145.
11. Rummans TA, Clark MM, Sloan JA, Frost MH, Bostwick JM, Atherton PJ et al. Impacting quality of life for patients with advanced cancer with a structured multidisciplinary intervention: a randomized controlled trial. J Clin Oncol 2006; 24(4):635-642.
12. von Plessen C, Aslaksen A. Improving the quality of palliative care for ambulatory patients with lung cancer. BMJ 2005; 330(7503):1309-1313.

145
13. Temel JS, Jackson VA, Billings JA, Dahlin C, Block SD, Buss MK et al. Phase II study: integrated palliative care in newly diagnosed advanced non-small-cell lung cancer patients. J Clin Oncol 2007; 25(17):2377-2382.
14. Garcia-Perez L, Linertova R, Martin-Olivera R, Serrano-Aguilar P, Benitez-Rosario MA. A systematic review of specialised palliative care for terminal patients: which model is better? Palliat Med 2009; 23(1):17-22.
15. Greer DS, Mor V, Sherwood S, Morris JN, Birnbaum H. National hospice study analysis plan. J Chronic Dis 1983; 36(11):737-780.
16. Greer DS, Mor V, Morris JN, Sherwood S, Kidder D, Birnbaum H. An alternative in terminal care: results of the National Hospice Study. J Chronic Dis 1986; 39(1):9-26.
17. Kane RL, Wales J, Bernstein L, Leibowitz A, Kaplan S. A randomised controlled trial of hospice care. Lancet 1984; 1(8382):890-894.
18. Zimmermann C, Riechelmann R, Krzyzanowska M, Rodin G, Tannock I. Effectiveness of Specialized Palliative Care: A Systematic Review. JAMA 2008; 299(14):1698-1709.
19. Paes P. A pilot study to assess the effectiveness of a palliative care clinic in improving the quality of life for patients with severe heart failure. Palliat Med 2005; 19(6):505-506.
20. Eccles M, Grimshaw J, Campbell M, Ramsay C. Research designs for studies evaluating the effectiveness of change and improvement strategies. Qual Saf Health Care 2003; 12(1):47-52.
21. Bruera E, Sweeney C. The development of palliative care at the University of Texas M.D. Anderson Cancer Center. Support Care Cancer 2001; 9(5):330-334.
22. Zhukovsky DS. A model of palliative care: the palliative medicine program of the Cleveland Clinic Foundation. A World Health Organization Demonstrations Project. Support Care Cancer 2000; 8(4):268-277.
23. Zimmermann C, Seccareccia D, Clarke A, Warr D, Rodin G. Bringing palliative care to a Canadian cancer center: the palliative care program at Princess Margaret Hospital. Support Care Cancer 2006; 14(10):982-987.
24. Strohscheer I, Verebes J, Samonigg H. Implementation of a palliative care team in an Austrian university hospital. Support Care Cancer 2006; 14(8):795-801.
25. Sepulveda C, Marlin A, Yoshida T, Ullrich A. Palliative Care: the World Health Organization's global perspective. J Pain Symptom Manage 2002; 24(2):91-96.
26. Choi YS, Billings JA. Changing perspectives on palliative care. Oncology (Williston Park) 2002; 16(4):515-522.

146
27. Higginson IJ, Finlay I, Goodwin DM, Cook AM, Hood K, Edwards AG et al. Do hospital-based palliative teams improve care for patients or families at the end of life? J Pain Symptom Manage 2002; 23(2):96-106.
28. Higginson IJ, Finlay IG, Goodwin DM, Hood K, Edwards AG, Cook A et al. Is there evidence that palliative care teams alter end-of-life experiences of patients and their caregivers? J Pain Symptom Manage 2003; 25(2):150-168.
29. Rinck GC, van den Bos GA, Kleijnen J, de Haes HJ, Schade E, Veenhof CH. Methodologic issues in effectiveness research on palliative cancer care: a systematic review. J Clin Oncol 1997; 15(4):1697-1707.
30. Hughes SL, Weaver FM, Giobbie-Hurder A, Manheim L, Henderson W, Kubal JD et al. Effectiveness of team-managed home-based primary care: a randomized multicenter trial. JAMA 2000; 284(22):2877-2885.
31. Riechelmann RP, Krzyzanowska MK, O'carroll A, Zimmermann C. Symptom and medication profiles among cancer patients attending a palliative care clinic. Support Care Cancer 2007; 15(12):1407-1412.
32. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982; 5(6):649-655.
33. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care 1991; 7(2):6-9.
34. Kristjanson LJ. Validity and reliability testing of the FAMCARE Scale: measuring family satisfaction with advanced cancer care. Soc Sci Med 1993; 36(5):693-701.
35. Chang VT, Hwang SS, Feuerman M. Validation of the Edmonton Symptom Assessment Scale. Cancer 2000; 88(9):2164-2171.
36. Philip J, Smith WB, Craft P, Lickiss N. Concurrent validity of the modified Edmonton Symptom Assessment System with the Rotterdam Symptom Checklist and the Brief Pain Inventory. Support Care Cancer 1998; 6(6):539-541.
37. Ringdal GI, Jordhoy MS, Kaasa S. Measuring quality of palliative care: psychometric properties of the FAMCARE Scale. Qual Life Res 2003; 12(2):167-176.
38. Dudgeon DJ, Knott C, Eichholz M, Gerlach JL, Chapman C, Viola R et al. Palliative Care Integration Project (PCIP) Quality Improvement Strategy Evaluation. J Pain Symptom Manage 2008; 35(6):573-582.
39. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40(5):373-383.
147
40. Extermann M. Measuring comorbidity in older cancer patients. Eur J Cancer 2000; 36(4):453-471.
41. Cheung WY, Barmala N, Zarinehbaf S, Rodin R, Le LW, Zimmermann C. Association of physical and psychological symptom burden with time to death in palliative care outpatients. J Pain Symptom Manage. 2008 May; 35(5):535-43.
42. Osoba D. A taxonomy of the uses of health-related quality-of-life instruments in cancer care and the clinical meaningfulness of the results. Med Care 2002; 40(6 Suppl):III31-III38.
43. Ringash J, O'Sullivan B, Bezjak A, Redelmeier DA. Interpreting clinically significant changes in patient-reported outcomes. Cancer 2007; 110(1):196-202.
44. Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol 1998; 16(1):139-144.
45. Barrett B, Brown D, Mundt M, Brown R. Sufficiently important difference: expanding the framework of clinical significance. Med Decis Making 2005; 25(3):250-261.
46. Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes 2003; 1(1):79.
47. Fayers PM, Aaronson NK, Bjordal K, Groenvold M, Curran D, Bottomley A. EORTC QLQ-C30 scoring manual (3rd edn). Brussels, Belgium: EORTC Quality of Life Group; 2001.
48. Osoba D, Slamon DJ, Burchmore M, Murphy M. Effects on quality of life of combined trastuzumab and chemotherapy in women with metastatic breast cancer. J Clin Oncol 2002; 20(14):3106-3113.
49. Joly F, Vardy J, Pintilie M, Tannock IF. Quality of life and/or symptom control in randomized clinical trials for patients with advanced cancer. Ann Oncol 2007; 18(12):1935-1942.
50. Guyatt GH, Osoba D, Wu AW, Wyrwich KW, Norman GR. Methods to explain the clinical significance of health status measures. Mayo Clin Proc 2002; 77(4):371-383.
51. Modonesi C, Scarpi E, Maltoni M, Derni S, Fabbri L, Martini F et al. Impact of palliative care unit admission on symptom control evaluated by the edmonton symptom assessment system. J Pain Symptom Manage 2005; 30(4):367-373.
52. Kaasa S, Loge JH. Quality of life in palliative care: principles and practice. Palliat Med 2003; 17(1):11-20.
53. Hales S, Zimmermann C, Rodin G. The quality of dying and death. Arch Intern Med2008; 168(9):912-918.

148
54. Dy SM, Shugarman LR, Lorenz KA, Mularski RA, Lynn J. A systematic review of satisfaction with care at the end of life. J Am Geriatr Soc 2008; 56(1):124-129.
55. Ringdal GI, Jordhoy MS, Kaasa S. Family satisfaction with end-of-life care for cancer patients in a cluster randomized trial. J Pain Symptom Manage 2002; 24(1):53-63.
56. Kristjanson LJ, Leis A, Koop PM, Carriere KC, Mueller B. Family members' care expectations, care perceptions, and satisfaction with advanced cancer care: results of a multi-site pilot study. J Palliat Care 1997; 13(4):5-13.
57. Morrison RS, Siu AL, Leipzig RM, Cassel CK, Meier DE. The hard task of improving the quality of care at the end of life. Arch Intern Med 2000; 160(6):743-747.
58. Hwang SS, Chang VT, Alejandro Y, Osenenko P, Davis C, Cogswell J et al. Caregiver unmet needs, burden, and satisfaction in symptomatic advanced cancer patients at a Veterans Affairs (VA) medical center. Palliat Support Care 2003; 1(4):319-329.
59. Grunfeld E, Coyle D, Whelan T, Clinch J, Reyno L, Earle CC et al. Family caregiver burden: results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ 2004; 170(12):1795-1801.
60. Stromgren AS, Goldschmidt D, Groenvold M, Petersen MA, Jensen PT, Pedersen L et al. Self-assessment in cancer patients referred to palliative care: a study of feasibility and symptom epidemiology. Cancer 2002; 94(2):512-520.
61. Stromgren AS, Sjogren P, Goldschmidt D, Petersen MA, Pedersen L, Hoermann L et al. A longitudinal study of palliative care: patient-evaluated outcome and impact of attrition. Cancer 2005; 103(8):1747-1755.
62. Jordhoy MS, Fayers P, Loge JH, Ahlner-Elmqvist M, Kaasa S. Quality of life in palliative cancer care: results from a cluster randomized trial. J Clin Oncol 2001; 19(18):3884-3894.
63. Hanks GW, Robbins M, Sharp D, Forbes K, Done K, Peters TJ et al. The imPaCT study: a randomised controlled trial to evaluate a hospital palliative care team. Br J Cancer 2002; 87(7):733-739.
64. Stromgren AS, Groenvold M, Petersen MA, Goldschmidt D, Pedersen L, Spile M et al. Pain characteristics and treatment outcome for advanced cancer patients during the first week of specialized palliative care. J Pain Symptom Manage 2004; 27(2):104-113.
65. Jordhoy MS, Fayers P, Loge JH, Saltnes T, Ahlner-Elmqvist M, Kaasa S. Quality of life in advanced cancer patients: the impact of sociodemographic and medical characteristics. Br J Cancer 2001; 85(10):1478-1485.
149
66. Walsh D, Donnelly S, Rybicki L. The symptoms of advanced cancer: relationship to age, gender, and performance status in 1,000 patients. Support Care Cancer 2000; 8(3):175-179.
67. Husain AF, Stewart K, Arseneault R, Moineddin R, Cellarius V, Librach SL et al. Women experience higher levels of fatigue than men at the end of life: a longitudinal home palliative care study. J Pain Symptom Manage 2007; 33(4):389-397.
68. Follwell M, Burman D, Le LW, Wakimoto K, Seccareccia D, Bryson J et al. Phase II study of an outpatient palliative care intervention in patients with metastatic cancer. Journal of Clinical Oncology (in press) 2008.
69. Philip J, Smith WB, Craft P, Lickiss N. Concurrent validity of the modified Edmonton Symptom Assessment System with the Rotterdam Symptom Checklist and the Brief Pain Inventory. Support Care Cancer 1998; 6(6):539-541.
70. Paul SM, Zelman DC, Smith M, Miaskowski C. Categorizing the severity of cancer pain: further exploration of the establishment of cutpoints. Pain 2005; 113(1-2):37-44.
71. Perneger TV. What's wrong with Bonferroni adjustments. BMJ 1998; 316(7139):1236-1238.
72. Bradley N, Davis L, Chow E. Symptom distress in patients attending an outpatient palliative radiotherapy clinic. J Pain Symptom Manage 2005; 30(2):123-131.
73. Cheung WY, Barmala N, Zarinehbaf S, Rodin G, Le LW, Zimmermann C. The Association of Physical and Psychological Symptom Burden with Time to Death Among Palliative Cancer Outpatients. J Pain Symptom Manage 2008.
74. Chow E, Fung K, Panzarella T, Bezjak A, Danjoux C, Tannock I. A predictive model for survival in metastatic cancer patients attending an outpatient palliative radiotherapy clinic. Int J Radiat Oncol Biol Phys 2002; 53(5):1291-1302.
75. Hjermstad MJ, Fayers PM, Bjordal K, Kaasa S. Health-related quality of life in the general Norwegian population assessed by the European Organization for Research and Treatment of Cancer Core Quality-of-Life Questionnaire: the QLQ=C30 (+ 3). J Clin Oncol 1998; 16(3):1188-1196.
76. Holzner B, Kemmler G, Cella D, De Paoli C, Meraner V, Kopp M et al. Normative data for functional assessment of cancer therapy--general scale and its use for the interpretation of quality of life scores in cancer survivors. Acta Oncol 2004; 43(2):153-160.
77. Ciaramella A, Poli P. Assessment of depression among cancer patients: the role of pain, cancer type and treatment. Psychooncology 2001; 10(2):156-165.
78. Miaskowski C. Gender differences in pain, fatigue, and depression in patients with cancer. J Natl Cancer Inst Monogr 2004;(32):139-143.

150
79. Given CW, Given BA, Stommel M. The impact of age, treatment, and symptoms on the physical and mental health of cancer patients. A longitudinal perspective. Cancer1994; 74(7 Suppl):2128-2138.
80. Aass N, Fossa SD, Dahl AA, Moe TJ. Prevalence of anxiety and depression in cancer patients seen at the Norwegian Radium Hospital. Eur J Cancer 1997; 33(10):1597-1604.
81. Hopwood P, Stephens RJ. Depression in patients with lung cancer: prevalence and risk factors derived from quality-of-life data. J Clin Oncol 2000; 18(4):893-903.
82. De Leeuw JR, de Graeff A, Ros WJ, Blijham GH, Hordijk GJ, Winnubst JA. Prediction of depression 6 months to 3 years after treatment of head and neck cancer. Head Neck 2001; 23(10):892-898.
83. Carlson LE, Angen M, Cullum J, Goodey E, Koopmans J, Lamont L et al. High levels of untreated distress and fatigue in cancer patients. Br J Cancer 2004; 90(12):2297-2304.
84. Strong V, Waters R, Hibberd C, Rush R, Cargill A, Storey D et al. Emotional distress in cancer patients: the Edinburgh Cancer Centre symptom study. Br J Cancer 2007; 96(6):868-874.
85. Pascoe S, Edelman S, Kidman A. Prevalence of psychological distress and use of support services by cancer patients at Sydney hospitals. Aust N Z J Psychiatry 2000; 34(5):785-791.
86. Stone P, Hardy J, Broadley K, Tookman AJ, Kurowska A, A'Hern R. Fatigue in advanced cancer: a prospective controlled cross-sectional study. Br J Cancer 1999; 79(9-10):1479-1486.
87. Akechi T, Kugaya A, Okamura H, Yamawaki S, Uchitomi Y. Fatigue and its associated factors in ambulatory cancer patients: a preliminary study. J Pain Symptom Manage 1999; 17(1):42-48.
88. Redeker NS, Lev EL, Ruggiero J. Insomnia, fatigue, anxiety, depression, and quality of life of cancer patients undergoing chemotherapy. Sch Inq Nurs Pract 2000; 14(4):275-290.
89. Pater JL, Zee B, Palmer M, Johnston D, Osoba D. Fatigue in patients with cancer: results with National Cancer Institute of Canada Clinical Trials Group studies employing the EORTC QLQ-C30. Support Care Cancer 1997; 5(5):410-413.
90. Grigoriadis S, Robinson GE. Gender issues in depression. Ann Clin Psychiatry 2007; 19(4):247-255.
91. Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site. Psychooncology 2001; 10(1):19-28.
151
92. Lundh HC, Seiger A, Furst CJ. Quality of life in terminal care--with special reference to age, gender and marital status. Support Care Cancer 2006; 14(4):320-328.
93. van Wijk CM, Kolk AM. Sex differences in physical symptoms: the contribution of symptom perception theory. Soc Sci Med 1997; 45(2):231-246.
94. Barsky AJ, Peekna HM, Borus JF. Somatic symptom reporting in women and men. J Gen Intern Med 2001; 16(4):266-275.
95. National Cancer Institute of Canada. Canadian Cancer Statistics 2008. 2008. Toronto, Canada.
96. Rodin G, Zimmermann C, Rydall A, Jones J, Shepherd FA, Moore M et al. The desire for hastened death in patients with metastatic cancer. J Pain Symptom Manage 2007; 33(6):661-675.
97. World Health Organization. WHO definition of palliative care. www.who.int/cancer/palliative/definition/en . 2002. Accessed Sept 17, 2007.
98. Ferris FD, Balfour HM, Bowen K, Fraley J, Hardwick M, Lamontagne C et al. A model to guide hospice palliative care: based on national principles and norms of practice. Ottawa, Canada: Canadian Hospice Palliative Care Association; 2002.
99. Costantini M, Toscani F, Gallucci M, Brunelli C, Miccinesi G, Tamburini M et al. Terminal cancer patients and timing of referral to palliative care: a multicenter prospective cohort study. Italian Cooperative Research Group on Palliative Medicine. J Pain Symptom Manage 1999; 18(4):243-252.
100. Lamont EB, Christakis NA. Physician factors in the timing of cancer patient referral to hospice palliative care. Cancer 2002; 94(10):2733-2737.
101. Cowan JD, Walsh D, Homsi J. Palliative medicine in a United States cancer center: a prospective study. Am J Hosp Palliat Care 2002; 19(4):240-250.
102. Osta BE, Palmer JL, Paraskevopoulos T, Pei BL, Roberts LE, Poulter VA et al. Interval between first palliative care consult and death in patients diagnosed with advanced cancer at a comprehensive cancer center. J Palliat Med 2008; 11(1):51-57.
103. Jordhoy MS, Fayers P, Saltnes T, Ahlner-Elmqvist M, Jannert M, Kaasa S. A palliative-care intervention and death at home: a cluster randomised trial. Lancet2000; 356(9233):888-893.
104. Hughes SL, Cummings J, Weaver F, Manheim L, Braun B, Conrad K. A randomized trial of the cost effectiveness of VA hospital-based home care for the terminally ill. Health Serv Res 1992; 26(6):801-817.
105. McWhinney IR, Bass MJ, Donner A. Evaluation of a palliative care service: problems and pitfalls. BMJ 1994; 309(6965):1340-1342.

152
106. Addington-Hall JM, MacDonald LD, Anderson HR, Chamberlain J, Freeling P, Bland JM et al. Randomised controlled trial of effects of coordinating care for terminally ill cancer patients. BMJ 1992; 305(6865):1317-1322.
107. McCorkle R, Benoliel JQ, Donaldson G, Georgiadou F, Moinpour C, Goodell B. A randomized clinical trial of home nursing care for lung cancer patients. Cancer1989; 64(6):1375-1382.
108. McMillan SC, Small BJ. Using the COPE intervention for family caregivers to improve symptoms of hospice homecare patients: a clinical trial. Oncol Nurs Forum2007; 34(2):313-321.
109. Toseland RW, Blanchard CG, McCallion P. A problem solving intervention for caregivers of cancer patients. Soc Sci Med 1995; 40(4):517-528.
110. Engelhardt JB, McClive-Reed KP, Toseland RW, Smith TL, Larson DG, Tobin DR. Effects of a program for coordinated care of advanced illness on patients, surrogates, and healthcare costs: a randomized trial. Am J Manag Care 2006; 12(2):93-100.
111. Casarett D, Karlawish J, Morales K, Crowley R, Mirsch T, Asch DA. Improving the use of hospice services in nursing homes: a randomized controlled trial. JAMA 2005; 294(2):211-217.
112. A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA 1995; 274(20):1591-1598.
113. Grande GE, Todd CJ, Barclay SI, Farquhar MC. A randomized controlled trial of a hospital at home service for the terminally ill. Palliat Med 2000; 14(5):375-385.
114. Miller DK, Chibnall JT, Videen SD, Duckro PN. Supportive-affective group experience for persons with life-threatening illness: reducing spiritual, psychological, and death-related distress in dying patients. J Palliat Med 2005; 8(2):333-343.
115. Aiken LS, Butner J, Lockhart CA, Volk-Craft BE, Hamilton G, Williams FG. Outcome evaluation of a randomized trial of the PhoenixCare intervention: program of case management and coordinated care for the seriously chronically ill. J Palliat Med 2006; 9(1):111-126.
116. Brumley R, Enguidanos S, Jamison P, Seitz R, Morgenstern N, Saito S et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc 2007; 55(7):993-1000.
117. Zimmer JG, Groth-Juncker A, McCusker J. A randomized controlled study of a home health care team. Am J Public Health 1985; 75(2):134-141.

153
118. Ringdal GI, Jordhoy MS, Kaasa S. Family satisfaction with end-of life care for cancer patients in a cluster randomized trial. Journal of Pain and Symptom Management 2002; 24(1):53-63.
119. Smeenk FW, van Haastregt JC, de Witte LP, Crebolder HF. Effectiveness of home care programmes for patients with incurable cancer on their quality of life and time spent in hospital: systematic review. BMJ 1998; 316(7149):1939-1944.
120. Salisbury C, Bosanquet N, Wilkinson EK, Franks PJ, Kite S, Lorentzon M et al. The impact of different models of specialist palliative care on patients' quality of life: a systematic literature review. Palliat Med 1999; 13(1):3-17.
121. Meyers FJ, Linder J, Beckett L, Christensen S, Blais J, Gandara DR. Simultaneous care: a model approach to the perceived conflict between investigational therapy and palliative care. J Pain Symptom Manage 2004; 28(6):548-556.
122. Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol 1993; 11(3):570-579.
123. Jordhoy MS, Kaasa S, Fayers P, Ovreness T, Underland G, Ahlner-Elmqvist M. Challenges in palliative care research; recruitment, attrition and compliance: experience from a randomized controlled trial. Palliat Med 1999; 13(4):299-310.
124. Forster LE, Lynn J. Predicting life span for applicants to inpatient hospice. Archives of Internal Medicine 1988; 148:2540-2543.
125. Christakis NA, Lamont EB. Extent and determinants of error in doctors' prognoses in terminally ill patients prospective cohort study. British Medical Journal 2000; 320(469):472.
126. Llobera J, Esteva M, Rifa J, Benito E, Terrasa J, Rojas C et al. Terminal cancer. duration and prediction of survival time. Eur J Cancer 2000; 36(16):2036-2043.
127. Glare P, Virik K, Jones M, Hudson M, Eychmuller S, Simes J et al. A systematic review of physicians' survival predictions in terminally ill cancer patients. BMJ2003; 327(7408):195.
128. Fairhurst K, Dowrick C. Problems with recruitment in a randomized controlled trial of counselling in general practice: causes and implications. J Health Serv Res Policy1996; 1(2):77-80.
129. Gilbody S, Whitty P. Improving the delivery and organisation of mental health services: beyond the conventional randomised controlled trial. Br J Psychiatry 2002; 180:13-18.
130. Puffer S, Torgerson D, Watson J. Evidence for risk of bias in cluster randomised trials: review of recent trials published in three general medical journals. BMJ 2003; 327(7418):785-789.

154
131. Torgerson DJ. Contamination in trials: is cluster randomisation the answer? BMJ2001; 322(7282):355-357.
132. Donner A, Klar N. Design and Analysis of Cluster Randomization Trials in Health Research. London, UK: Arnold; 2000.
133. Donner A, Klar N. Pitfalls of and controversies in cluster randomization trials. Am J Public Health 2004; 94(3):416-422.
134. Morrison RS, Meier DE. Clinical practice. Palliative care. N Engl J Med 2004; 350(25):2582-2590.
135. Fisch MJ, Titzer ML, Kristeller JL, Shen J, Loehrer PJ, Jung SH et al. Assessment of quality of life in outpatients with advanced cancer: the accuracy of clinician estimations and the relevance of spiritual well-being--a Hoosier Oncology Group Study. J Clin Oncol 2003; 21(14):2754-2759.
136. Brady MJ, Peterman AH, Fitchett G, Mo M, Cella D. A case for including spirituality in quality of life measurement in oncology. Psychooncology 1999; 8(5):417-428.
137. Cohen SR, Mount BM, Tomas JJ, Mount LF. Existential well-being is an important determinant of quality of life. Evidence from the McGill Quality of Life Questionnaire. Cancer 1996; 77(3):576-586.
138. Weitzner MA, McMillan SC, Jacobsen PB. Family caregiver quality of life: differences between curative and palliative cancer treatment settings. J Pain Symptom Manage 1999; 17(6):418-428.
139. Weitzner MA, McMillan SC. The Caregiver Quality of Life Index-Cancer (CQOLC) Scale: revalidation in a home hospice setting. J Palliat Care 1999; 15(2):13-20.
140. Braun M, Mikulincer M, Rydall A, Walsh A, Rodin G. Hidden morbidity in cancer: spouse caregivers. J Clin Oncol 2007; 25(30):4829-4834.
141. Rigby A, Krzyzanowska M, Le LW, Coe G, Swami N, Moore M et al. Impact of opening a palliative care unit on administrative outcomes on a general oncology ward. Cancer 2008; (in press).
142. KFL&A Palliative Care Integration Project. Symptom Management Guidelines. Kingston: Queen's University; 2003.
143. Katzman R, Brown T, Fuld P, Peck A, Schechter R, Schimmel H. Validation of a short Orientation-Memory-Concentration Test of cognitive impairment. Am J Psychiatry 1983; 140(6):734-739.
144. Steinhauser KE, Bosworth HB, Clipp EC, McNeilly M, Christakis NA, Parker J et al. Initial assessment of a new instrument to measure quality of life at the end of life. J Palliat Med 2002; 5(6):829-841.

155
145. Steinhauser KE, Clipp EC, Bosworth HB, McNeilly M, Christakis NA, Voils CI et al. Measuring quality of life at the end of life: validation of the QUAL-E. Palliat Support Care 2004; 2(1):3-14.
146. Peterman AH, Fitchett G, Brady MJ, Hernandez L, Cella D. Measuring spiritual well-being in people with cancer: the functional assessment of chronic illness therapy--Spiritual Well-being Scale (FACIT-Sp). Ann Behav Med 2002; 24(1):49-58.
147. McClain CS, Rosenfeld B, Breitbart W. Effect of spiritual well-being on end-of-life despair in terminally-ill cancer patients. Lancet 2003; 361(9369):1603-1607.
148. Nelson CJ, Rosenfeld B, Breitbart W, Galietta M. Spirituality, religion, and depression in the terminally ill. Psychosomatics 2002; 43(3):213-220.
149. Breitbart W. Spirituality and meaning in supportive care: spirituality- and meaning-centered group psychotherapy interventions in advanced cancer. Support Care Cancer 2002; 10(4):272-280.
150. Schag CA, Heinrich RL, Aadland RL, Ganz PA. Assessing problems of cancer patients: psychometric properties of the cancer inventory of problem situations. Health Psychol 1990; 9(1):83-102.
151. Han WT, Collie K, Koopman C, Azarow J, Classen C, Morrow GR et al. Breast cancer and problems with medical interactions: relationships with traumatic stress, emotional self-efficacy, and social support. Psychooncology 2005; 14(4):318-330.
152. Weitzner MA, Jacobsen PB, Wagner H, Jr., Friedland J, Cox C. The Caregiver Quality of Life Index-Cancer (CQOLC) scale: development and validation of an instrument to measure quality of life of the family caregiver of patients with cancer. Qual Life Res 1999; 8(1-2):55-63.
153. Weitzner MA, Meyers CA, Steinbruecker S, Saleeba AK, Sandifer SD. Developing a care giver quality-of-life instrument. Preliminary steps. Cancer Pract 1997; 5(1):25-31.
154. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 Health Survey Manual and Interpretation Guide. Boston, MA: New England Medical Center,The Health Institute; 1993.
155. McHorney CA, Ware JE, Jr., Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care 1993; 31(3):247-263.
156. McHorney CA, Ware JE, Jr., Lu JF, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care 1994; 32(1):40-66.

156
157. Ware JE, Jr., Kosinski M, Gandek B, Aaronson NK, Apolone G, Bech P et al. The factor structure of the SF-36 Health Survey in 10 countries: results from the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol 1998; 51(11):1159-1165.
158. Ringdal GI, Ringdal K, Jordhoy MS, Ahlner-Elmqvist M, Jannert M, Kaasa S. Health-related quality of life (HRQOL) in family members of cancer victims: results from a longitudinal intervention study in Norway and Sweden. Palliat Med 2004; 18(2):108-120.
159. Donner A, Piaggio G, Villar J, Pinol A, Al Mazrou Y, Ba'aqeel H et al. Methodological considerations in the design of the WHO Antenatal Care Randomised Controlled Trial. Paediatr Perinat Epidemiol 1998; 12 Suppl 2:59-74.
160. Villar J, Bakketeig L, Donner A, Al Mazrou Y, Ba'aqeel H, Belizan JM et al. The WHO antenatal care randomised controlled trial: rationale and study design. Paediatr Perinat Epidemiol 1998; 12 Suppl 2:27-58.
161. Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sondergaard O. Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet 1996; 348(9040):1467-1471.
162. Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, Amar SS, Balfour TW et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 1996; 348(9040):1472-1477.
163. Meinert CL. Clinical Trials: Design, Conduct and Analysis. Oxford: Oxford University Press; 1986.
164. Cella D, Hahn EA, Dineen K. Meaningful change in cancer-specific quality of life scores: differences between improvement and worsening. Qual Life Res 2002; 11(3):207-221.
165. Cella D, Nowinski CJ. Measuring quality of life in chronic illness: the functional assessment of chronic illness therapy measurement system. Arch Phys Med Rehabil2002; 83(12 Suppl 2):S10-S17.
166. Patrick DL, Gagnon DD, Zagari MJ, Mathijs R, Sweetenham J. Assessing the clinical significance of health-related quality of life (HrQOL) improvements in anaemic cancer patients receiving epoetin alfa. Eur J Cancer 2003; 39(3):335-345.
167. Osoba D. What has been learned from measuring health-related quality of life in clinical oncology. Eur J Cancer 1999; 35(11):1565-1570.
168. Cella D, Eton DT, Lai JS, Peterman AH, Merkel DE. Combining anchor and distribution-based methods to derive minimal clinically important differences on the Functional Assessment of Cancer Therapy (FACT) anemia and fatigue scales. J Pain Symptom Manage 2002; 24(6):547-561.
157
169. Friedman LM, Furberg CD, DeMets DL. Fundamentals of Clinical Trials. New York: Springer-Verlag; 1998.
170. Lachin JM. Introduction to sample size determination and power analysis for clinical trials. Control Clin Trials 1981; 2(2):93-113.
171. Klar N, Donner A. Current and future challenges in the design and analysis of cluster randomization trials. Stat Med 2001; 20(24):3729-3740.
172. Klar N, Darlington G. Methods for modelling change in cluster randomization trials. Stat Med 2004; 23(15):2341-2357.
173. Campbell MK, Mollison J, Steen N, Grimshaw JM, Eccles M. Analysis of cluster randomized trials in primary care: a practical approach. Fam Pract 2000; 17(2):192-196.
174. SAS Institute Inc. What's new in SAS 9.0, 9.1, 9.1.2 and 9.1.3. Cary, NC: SAS Institute, 2004.
175. Bernhard J, Cella DF, Coates AS, Fallowfield L, Ganz PA, Moinpour CM et al. Missing quality of life data in cancer clinical trials: serious problems and challenges. Stat Med 1998; 17(5-7):517-532.
176. Fairclough DL. Design and Analysis of Quality of Life Studies in Clinical Trials. Boca Raton, FL: Chapman & Hall/CRC; 2002.
177. Fairclough DL, Cella DF. Functional Assessment of Cancer Therapy (FACT-G): non-response to individual questions. Qual Life Res 1996; 5(3):321-329.
178. Davis D, Evans M, Jadad A, Perrier L, Rath D, Ryan D et al. The case for knowledge translation: shortening the journey from evidence to effect. BMJ 2003; 327(7405):33-35.
179. Murray DM, Rooney BL, Hannan PJ, Peterson AV, Ary DV, Biglan A et al. Intraclass correlation among common measures of adolescent smoking: estimates, correlates, and applications in smoking prevention studies. Am J Epidemiol 1994; 140(11):1038-1050.
180. Parker DR, Evangelou E, Eaton CB. Intraclass correlation coefficients for cluster randomized trials in primary care: the cholesterol education and research trial (CEART). Contemp Clin Trials 2005; 26(2):260-267.
181. Killip S, Mahfoud Z, Pearce K. What is an intracluster correlation coefficient? Crucial concepts for primary care researchers. Ann Fam Med 2004; 2(3):204-208.
182. Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000; 284(19):2476-2482.

158
183. Wilson KG, Chochinov HM, McPherson CJ, LeMay K, Allard P, Chary S et al. Suffering with advanced cancer. J Clin Oncol 2007; 25(13):1691-1697.
184. Whitford HS, Olver IN, Peterson MJ. Spirituality as a core domain in the assessment of quality of life in oncology. Psychooncology 2008; 17(11):1121-1128.
185. Janda M, Disipio T, Hurst C, Cella D, Newman B. The Queensland cancer risk study: general population norms for the functional assessment of cancer therapy-general (FACT-G). Psychooncology 2008.
186. Schwarz R, Hinz A. Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur J Cancer 2001; 37(11):1345-1351.
187. Fossa SD, Hess SL, Dahl AA, Hjermstad MJ, Veenstra M. Stability of health-related quality of life in the Norwegian general population and impact of chronic morbidity in individuals with and without a cancer diagnosis. Acta Oncol 2007; 46(4):452-461.
188. Brucker PS, Yost K, Cashy J, Webster K, Cella D. General population and cancer patient norms for the Functional Assessment of Cancer Therapy-General (FACT-G). Eval Health Prof 2005; 28(2):192-211.
189. Yost KJ, Eton DT. Combining distribution- and anchor-based approaches to determine minimally important differences: the FACIT experience. Eval Health Prof2005; 28(2):172-191.
190. Edmondson D, Park CL, Blank TO, Fenster JR, Mills MA. Deconstructing spiritual well-being: existential well-being and HRQOL in cancer survivors. Psychooncology2008; 17(2):161-169.
191. Statistics Canada. Ethnic Origin. http://www12.statcan.ca/english/census01/Products/Reference/dict/pop040.htm . Accessed October 4, 2009.
192. Feinstein AR. Multivariable Analysis: An Introduction. New Haven: Yale University Press; 1996.
193. Hjermstad MJ, Fayers PM, Bjordal K, Kaasa S. Using reference data on quality of life--the importance of adjusting for age and gender, exemplified by the EORTC QLQ-C30 (+3). Eur J Cancer 1998; 34(9):1381-1389.
194. Exley C, Letherby G. Managing a disrupted lifecourse: issues of identity and emotion work. Health 2009; 5(1):112-132.
195. Rauch PK, Muriel AC. The importance of parenting concerns among patients with cancer. Crit Rev Oncol Hematol 2004; 49(1):37-42.
196. Mor V, Allen S, Malin M. The psychosocial impact of cancer on older versus younger patients and their families. Cancer 1994; 74(7 Suppl):2118-2127.

159
197. Chow E, Abdolell M, Panzarella T, Harris K, Bezjak A, Warde P et al. Predictive model for survival in patients with advanced cancer. J Clin Oncol 2008; 26(36):5863-5869.
198. Ando M, Morita T, Okamoto T, Ninosaka Y. One-week Short-Term Life Review interview can improve spiritual well-being of terminally ill cancer patients. Psychooncology 2008; 17(9):885-890.
199. Harrington SE, Smith TJ. The role of chemotherapy at the end of life: "when is enough, enough?". JAMA 2008; 299(22):2667-2678.
200. Wan GJ, Counte MA, Cella DF, Hernandez L, Deasy S, Shiomoto G. An analysis of the impact of demographic, clinical, and social factors on health-related quality of life. Value Health 1999; 2(4):308-318.
201. Jordhoy MS, Inger RG, Helbostad JL, Oldervoll L, Loge JH, Kaasa S. Assessing physical functioning: a systematic review of quality of life measures developed for use in palliative care. Palliat Med 2007; 21(8):673-682.
202. Lo C, Burman D, Rodin G, Zimmermann C. Measuring patient satisfaction in oncology palliative care: psychometric properties of the FAMCARE-patient scale. Qual Life Res 2009.
203. Preventive Services Task Force. Guide to clinical preventive services: report of the U.S. Preventive Services Task Force. 2nd ed. ed. Baltimore: Willians & Wilkins; 1996.
204. Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet 2001; 357(9263):1191-1194.
205. Campbell MK, Elbourne DR, Altman DG. CONSORT statement: extension to cluster randomised trials. BMJ 2004; 328(7441):702-708.
206. Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG et al. CONSORT for reporting randomized controlled trials in journal and conference abstracts: explanation and elaboration. PLoS Med 2008; 5(1):e20.
207. Freedman B. Equipoise and the ethics of clinical research. N Engl J Med 1987; 317(3):141-145.
208. Parfrey P, Ravani P. On framing the research question and choosing the appropriate research design. Methods Mol Biol 2009; 473:1-17.
209. Glare P, Virik K, Jones M, Hudson M, Eychmuller S, Simes J et al. A systematic review of physicians' survival predictions in terminally ill cancer patients. BMJ2003; 327(7408):195.

160
210. Follwell M, Burman D, Le LW, Wakimoto K, Seccareccia D, Bryson J et al. Phase II study of an outpatient palliative care intervention in patients with metastatic cancer. J Clin Oncol 2009; 27(2):206-213.
211. Balboni TA, Vanderwerker LC, Block SD, Paulk ME, Lathan CS, Peteet JR et al. Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. J Clin Oncol 2007; 25(5):555-560.
212. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing andevaluating complex interventions: the new Medical Research Council guidance. BMJ 2008; 337:a1655.
213. Fowell A, Johnstone R, Finlay IG, Russell D, Russell IT. Design of trials with dying patients: a feasibility study of cluster randomisation versus randomised consent. Palliat Med 2006; 20(8):799-804.
214. Jordhoy MS, Fayers PM, Ahlner-Elmqvist M, Kaasa S. Lack of concealment may lead to selection bias in cluster randomized trials of palliative care. Palliat Med2002; 16(1):43-49.
215. Carman WF, Elder AG, Wallace LA, McAulay K, Walker A, Murray GD et al. Effects of influenza vaccination of health-care workers on mortality of elderly people in long-term care: a randomised controlled trial. Lancet 2000; 355(9198):93-97.
216. Mularski RA, Dy SM, Shugarman LR, Wilkinson AM, Lynn J, Shekelle PG et al. A systematic review of measures of end-of-life care and its outcomes. Health Serv Res2007; 42(5):1848-1870.
217. Peto R. Failure of randomisation by "sealed" envelope. Lancet 1999; 354(9172):73.
218. Koffman J, Morgan M, Edmonds P, Speck P, Higginson IJ. Vulnerability in palliative care research: findings from a qualitative study of black Caribbean and white British patients with advanced cancer. J Med Ethics 2009; 35(7):440-444.
219. Chochinov HM. The culture of research in palliative care: you probably think this song is about you. J Palliat Med 2009; 12(3):215-217.
220. Flemming K, Adamson J, Atkin K. Improving the effectiveness of interventions in palliative care: the potential role of qualitative research in enhancing evidence from randomized controlled trials. Palliat Med 2008; 22(2):123-131.
221. Pope C, Mays N. Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research. BMJ 1995; 311(6996):42-45.

161
222. Payne SM. Qualitative methods of data collection and analysis. In: Addington-Hall J, Bruera E, Higginson I, Payne SM, editors. Research Methods in Palliative Care. Oxford: Oxford University Press; 2007: 139-161.
223. Ingleton C, Davies S. Mixed methods for evaluation research. In: Addington-Hall J, Bruera E, Higginson I, Payne S, editors. Research Methods in Palliative Care. Oxford: Oxford University Press; 2007: 191-209.
224. Rabow MW, Schanche K, Petersen J, Dibble SL, McPhee SJ. Patient perceptions of an outpatient palliative care intervention: "It had been on my mind before, but I did not know how to start talking about death...". J Pain Symptom Manage 2003; 26(5):1010-1015.
225. Kish L. Survey Sampling. New York: 1965.
226. Strauss A, Corbin J. Basics of Qualitative Research. Newbury Park: Sage; 1990.
227. Charmaz C. Grounded theory: Objectivist and constructivist methods. In: Denzin NK, Lincoln YS, editors. Handbook of Qualitative Research. Thousand Oaks: Sage; 2000: 509-535.
228. Kuzel AJ. Sampling in Qualitative Inquiry. In: Crabtree BF, Miller WL, editors. Doing Qualitative Research. Newbury Park: Sage; 1992: 31-44.
229. Lynn J. Measuring quality of care at the end of life: a statement of principles. J Am Geriatr Soc 1997; 45(4):526-527.
230. Kristjanson LJ. Indicators of quality of palliative care from a family perspective. J Palliat Care 1986; 1(2):8-17.
231. Kristjanson LJ. Quality of terminal care: salient indicators identified by families. J Palliat Care 1989; 5(1):21-30.
232. SAS Institute. The MI Procedure: SAS/STAT User's Guide: SAS OnlineDoc 9.1 . 2003. 16-6-2009.
Ref Type: Electronic Citation
233. Portenoy RK, Thaler HT, Kornblith AB, Lepore JM, Friedlander-Klar H, Kiyasu E et al. The Memorial Symptom Assessment Scale: an instrument for the evaluation of symptom prevalence, characteristics and distress. Eur J Cancer 1994; 30A(9):1326-1336.
234. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 1994; 23(2):129-138.
235. Aspinal F, Addington-Hall J, Hughes R, Higginson IJ. Using satisfaction to measure the quality of palliative care: a review of the literature. J Adv Nurs 2003; 42(4):324-339.

162
236. Wilkinson EK, Salisbury C, Bosanquet N, Franks PJ, Kite S, Lorentzon M et al. Patient and carer preference for, and satisfaction with, specialist models of palliative care: a systematic literature review. Palliat Med 1999; 13(3):197-216.
237. Cohen SR, Mount BM, Strobel MG, Bui F. The McGill Quality of Life Questionnaire: a measure of quality of life appropriate for people with advanced disease. A preliminary study of validity and acceptability. Palliat Med 1995; 9(3):207-219.
238. Curtis JR, Patrick DL, Engelberg RA, Norris K, Asp C, Byock I. A measure of the quality of dying and death. Initial validation using after-death interviews with family members. J Pain Symptom Manage 2002; 24(1):17-31.
239. Teno JM, Lima JC, Lyons KD. Cancer patient assessment and reports of excellence: reliability and validity of advanced cancer patient perceptions of the quality of care. J Clin Oncol 2009; 27(10):1621-1626.
240. Bredart A, Bottomley A, Blazeby JM, Conroy T, Coens C, D'haese S et al. An international prospective study of the EORTC cancer in-patient satisfaction with care measure (EORTC IN-PATSAT32). Eur J Cancer 2005; 41(14):2120-2131.
241. Radwin L, Alster K, Rubin KM. Development and testing of the Oncology Patients' Perceptions of the Quality of Nursing Care Scale. Oncol Nurs Forum 2003; 30(2):283-290.
242. Wall RJ, Engelberg RA, Downey L, Heyland DK, Curtis JR. Refinement, scoring, and validation of the Family Satisfaction in the Intensive Care Unit (FS-ICU) survey. Crit Care Med 2007; 35(1):271-279.
243. Lipscomb J, Reeve BB, Clauser SB, Abrams JS, Bruner DW, Burke LB et al. Patient-reported outcomes assessment in cancer trials: taking stock, moving forward. J Clin Oncol 2007; 25(32):5133-5140.
244. Garcia SF, Cella D, Clauser SB, Flynn KE, Lad T, Lai JS et al. Standardizing patient-reported outcomes assessment in cancer clinical trials: a patient-reported outcomes measurement information system initiative. J Clin Oncol 2007; 25(32):5106-5112.
245. Im KS, Grover V. The use of structural equation models in IS research: review and recommendations. In: Whitman ME, Woszcznyski A, editors. The Handbook of Information Systems Research. Idea Group; 2004: 44-65.
246. Hatcher L. A Step-by-Step Approach to Using the SAS System for Factor Analysis and Structural Equation Modeling. Cary, NC: SAS Institute; 1998.
247. Yen WM. Scaling performance assessments: strategies for managing local item dependence. J Educ Meas 1993; 30:187-213.

163
248. Sulmasy DP, McIlvane JM, Pasley PM, Rahn M. A scale for measuring patient perceptions of the quality of end-of-life care and satisfaction with treatment: the reliability and validity of QUEST. J Pain Symptom Manage 2002; 23(6):458-470.
249. Donabedian A. The definition of quality and approaches to its assessment. Michigan: 1980.
250. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85(5):365-376.
251. Cohen SR, Mount BM. Quality of life in terminal illness: defining and measuring subjective well-being in the dying. J Palliat Care 1992; 8(3):40-45.
252. Yun YH, Kim SH, Lee KM, Park SM, Lee CG, Choi YS et al. Patient-reported assessment of quality care at end of life: development and validation of Quality Care Questionnaire-End of Life (QCQ-EOL). Eur J Cancer 2006; 42(14):2310-2317.
253. Morita T, Hirai K, Sakaguchi Y, Maeyama E, Tsuneto S, Shima Y. Measuring the quality of structure and process in end-of-life care from the bereaved family perspective. J Pain Symptom Manage 2004; 27(6):492-501.
254. Loblaw DA, Bezjak A, Bunston T. Development and testing of a visit-specific patient satisfaction questionnaire: the Princess Margaret Hospital Satisfaction With Doctor Questionnaire. J Clin Oncol 1999; 17(6):1931-1938.
255. Wiggers JH, Donovan KO, Redman S, Sanson-Fisher RW. Cancer patient satisfaction with care. Cancer 1990; 66(3):610-616.
256. Trask PC, Tellefsen C, Espindle D, Getter C, Hsu MA. Psychometric Validation of the Cancer Therapy Satisfaction Questionnaire. Value Health 2008.