can anatomists teach living anatomy using ultrasound as a teaching tool?
TRANSCRIPT
Can Anatomists Teach Living Anatomy Using Ultrasoundas a Teaching Tool?
Rosalyn A. Jurjus,1* Kathryn Dimorier,2 Kirsten Brown,1 Frank Slaby,1 Hamid Shokoohi,2
Keith Boniface,2 Yiju Teresa Liu2
1Department of Anatomy and Regenerative Biology, School of Medicine and Health Sciences,The George Washington University, Washington, Distinct of Columbia2Department of Emergency Medicine, School of Medicine and Health Sciences,The George Washington University, Washington, Distinct of Columbia
The utilization of bedside ultrasound by an increasing number of medical specialties hascreated the need for more ultrasound exposure and teaching in medical school. Althoughthere is a widespread support for more vertical integration of ultrasound teaching through-out the undergraduate curriculum, little is known about whether the quality of ultrasoundteaching differs if performed by anatomists or clinicians. The purpose of this study is tocompare medical students’ evaluation of ultrasound anatomy teaching by clinicians andanatomists. Hands-on interactive ultrasound sessions were scheduled as part of the grossanatomy course following principles of adult learning and instructional design. Seventeachers (three anatomists and four clinicians) taught in each session. Before each session,anatomists were trained in ultrasound by clinicians. Students were divided into groups,rotated teachers between sessions, and completed evaluations. Results indicated studentsperceived the two groups as comparable for all factors except for knowledge organizationand the helpfulness of ultrasound for understanding anatomy (P<0.001). However, resultsfrom unpaired samples t-tests demonstrated a nonstatistically significant difference betweenthe groups within each session for both questions. Moreover, students’ test performancefor both groups was similar. This study demonstrated that anatomists can teach livinganatomy using ultrasound with minimal training as well as clinicians, and encourage theteaching of living anatomy by anatomists in human anatomy courses using ultrasound.Repeating this study at a multicenter level is currently being considered to further validateour conclusion. Anat Sci Educ 00: 000–000. VC 2013 American Association of Anatomists.
Key words: gross anatomy education; medical education; ultrasound education; medicalstudent; ultrasound teaching skills; anatomist
INTRODUCTION
It is believed that expanded training in the use of ultrasoundwill lead to better health care for both individuals and popu-lations (Bahner et al., 2012; Brown et al., 2012). With advan-ces in technology, the utilization of bedside ultrasound by an
increasing number of medical specialties has created the needfor more ultrasound exposure and teaching in medical school.However, medical students typically have minimal to no for-mal teaching in ultrasound use (Brown et al., 2012). There isa widespread support among clinicians for more vertical inte-gration of ultrasound teaching throughout the undergraduatecurriculum, starting with the anatomical sciences (Hoppmannet al., 2011; Bahner et al., 2012). Evidence for this recom-mendation comes from the University of South Carolina,where an integrated ultrasound curriculum (iUSC) was intro-duced and successfully integrated across all four years ofmedical school (Hoppmann et al., 2011).
Teaching anatomy is an innovative field that relies onmodels, imaging, and simulations that consolidate the mas-tery of knowledge (Sugand et al., 2010). The use of ultra-sound as a complementary teaching method has been shownto improve medical students’ skills and understanding of
*Correspondence to: Dr. Rosalyn A. Jurjus, Department of Anatomyand Regenerative Biology, The George Washington University Schoolof Medicine and Health Sciences, 461B Ross Hall, 2300 I Street, NW,Washington, DC 20037, USA. E-mail: [email protected]
Received 6 May 2013; Revised 13 September 2013; Accepted 23September 2013.
Published online 00 Month 2013 in Wiley Online Library(wileyonlinelibrary.com). DOI 10.1002/ase.1417
VC 2013 American Association of Anatomists
Anatomical Sciences Education MONTH 2013 Anat Sci Educ 00:00–00 (2013)
RESEARCH REPORT

living anatomy (Barloon et al., 1998; Wright and Bell, 2008;Ivanusic et al., 2010; Zumwalt et al., 2010; Stringer et al.,2012; Swamy and Searle, 2012). Hands-on ultrasound work-shops performed by medical students have been successfullyintegrated into anatomy courses at institutions in the UnitedStates and Europe (Teichgr€aber et al., 1996; Rao et al., 2008;Sugand et al., 2010). Ultrasonography not only allows forthe visualization complex three-dimensional and living anat-omy but it is also very highly rated by students (Wittichet al., 2002; Stringer et al., 2012). These advancements comeat a time when there is increased support for a stronger linkbetween basic science education and its role in clinical spe-cialties, thereby easing the difficult transition from the pre-clinical to the clinical years with regard to the application ofanatomical knowledge (Waterston and Stewart, 2005; Lazaruset al., 2012).
One of the issues about incorporating ultrasound into medi-cal curriculum concerns the logistics of integration, both interms of (1) when to target students and (2) the availability ofinstructors. Previous research has shown that basic ultrasoundcan be equally taught during short-training sessions to first-and fourth-year medical students (Yoo et al., 2004), suggestingthat first-year medical students are an ideal population to beginintegration of new skills necessary later in their medical careers.Furthermore, ultrasound training complements instruction inphysical examination and radiology clerkships, and improvesstudents’ skills and allows them to better integrate knowledge(Yoo et al., 2004). In an effort to establish a longitudinal inte-gration of anatomical ultrasound teaching throughout medicalschool, changes in the curriculum at the authors’ institutionhave been implemented to enhance the utility of ultrasound.
In the current curriculum, the first-year (Fall semester)anatomy course was chosen as the point of entry for the verti-cal integration of ultrasound into undergraduate medical cur-riculum. Small interactive group sessions were used tointegrate ultrasound, which were tied into relevant gross anat-omy topics. These were designed according to active principlesof adult learning and instructional design (Jurjus et al., 2013).Traditionally, the instructors for these ultrasound sessions havemainly been clinicians or radiologists (Barloon et al., 1998;Butter et al., 2007; Zumwalt et al., 2010). However, cliniciansusually have limited time available for teaching, and thedemand for other educators to step in is increasing.
The objective of this study is to show that anatomists canteach ultrasound with minimal training as well as clinicians.The hypothesis is that medical student’ perceptions of anato-mists teaching ultrasound is similar compared with clinicians.This study assesses teaching with ultrasound by both anato-mists and clinicians, and it explores the issues of humanresource utilization in the assimilation of ultrasound intohuman anatomy curricula.
METHODS
Ethical Approval
This project was approved by the Institutional Review Board(IRB) at The George Washington University, as an exemptstudy (IRB # 071231).
Design of the Study
This is a study conducted to evaluate medical students’ per-ception of ultrasound use for Gross Anatomy teaching by
clinicians and anatomists using both quantitative and qualita-tive approaches. Participants were first-year medical studentsat The George Washington University Medical Schoolenrolled in the Anatomy course (Table 1). This course con-sists of topics in gross anatomy and embryology, extendsover 17 weeks, and is divided into three blocks, correspond-ing to different regions of the body: Upper and lower limbs,thorax, and abdomen; and head and neck; and pelvis andperineum. In total, the course consists of 52 lecture hours(embryology and gross anatomy) and 58 laboratory hours(gross anatomy only). For gross laboratory sessions, the�180 student member class is divided into 15 sets of A andB laboratory groups, with six members in each A and each Blaboratory group pairing, for an overall total of 30 labora-tory groups. Members of the A and B teams alternate theirdissection time every other laboratory, so that at any giventime only half of class is present in laboratory. However,before the start of a new laboratory session, both teams arepresent for a short debriefing period to keep both groups up-to-date on the progress of the dissection. At the end of thirdof the course, the students have both a written and a practi-cal examination. However for third section, the students takethe National Board of Medical ExaminersVR (NBMEVR ) Anat-omy and Embryology Subject Examination in place of theirnormal written examination.
Three hands-on, interactive ultrasound sessions werescheduled as part of the gross anatomy course at the begin-ning of each block and delivered twice, once for the A teams,while B teams were in gross laboratory, and vice versa. Eachsession ran anywhere from three to four hours, dependingupon the concurrent gross laboratory session. Students weredivided into seven groups, by a random combination of twoor three dissection table groups, with each group consistingof 12–14 students. Students rotated teachers from one sessionto another throughout the semester. Sessions were conductedusing resources and space at Clinical Learning and Simula-tion Skills Center (CLASS Center) at the George WashingtonUniversity Hospital. Due to continual use of the CLASS Cen-ter’s resources by other groups, students did not have freeaccess to the ultrasound machines after the sessions. High-quality portable ultrasound machines equipped with a range
Table 1.
Demographics on Study Participants
Students demographics N (%)
Total number of students 178
Gender
Female 98 (55.06)
Male 80 (44.94)
Age distribution
>30 4 (2.25%)
25–30 32 (17.98%)
21–24 142 (79.77%)
2 Jurjus et al.

of transducers were used in this study because they provideimage resolution and larger screens for visualization andsharing in small groups (Stringer et al., 2012; Sweetmanet al., 2013). Ultrasound was performed using one of twoportable ultrasound machines: a Zonare z.one ultra sp ultra-sound system with P4-1c and L8-3 probes (Zonare MedicalSystems, Mountain View, CA) or a Sonosite M-turbo ultra-sound system with L25 and P21 probes (FUJIFILM Sonosite,Bothell, WA). Both low frequency (5–2 MHz) and high fre-quency (13–6 MHz) ultrasound transducers were used,although this varied depending upon the area of the bodyscanned (e.g., low-frequency for abdominal structures, highfrequency for rotator cuff muscles).
Total one-hundred and seventy-eight students in the classwere recruited for each session. All consenting first-year stu-dents completed a survey at the end of each of the three ses-sions. One-hundred and sixty-eight’ students completed thesurvey after the first session, one-hundred and thirty-nine stu-dents completed the survey after the second session and one-hundred and twenty-six students completed the survey afterthe third session. Medical student demographic data isdetailed in Table 1. Seven teachers—three anatomists andfour clinicians—taught each session. Clinical faculty camefrom the subspecialties in emergency medicine, rheumatology,and surgery and all had expertise and used ultrasound regu-larly in their practice. They include residents, fellows, andattending physicians. The clinician instructors were threeboard certified attending physicians in their respective spe-cialties, all ultrasound fellowship trained, with one to morethan four years of ultrasound teaching experience and clinicalpractice experience. The fellow had four years of post-graduate (residency) training in using ultrasound in clinicalpractice and the resident physicians in Emergency Medicineor Surgery, respectively, had more than three years trainingand using ultrasound in clinical practice. Each of the anato-mists had several years of experiences teaching gross anat-omy, varying from 10 to 40 years, but none had any priorultrasound training, except for what was provided to themwithin the context of this study and described below.
The anatomists underwent a two-hour didactic and hands-on training session from the clinicians approximately oneweek before teaching these sessions. The same machines andtransducers were used in these training sessions as in theteaching sessions. These sessions were conducted by a clini-cian sonographer who was a board-certified emergency physi-cian, fellowship trained in emergency ultrasound, and theemergency ultrasound fellowship director at the institution.This physician guided the anatomy faculty through the samesession outline as the one planned for the students. Anoptional one-hour practice session the day before studentteaching was offered to the anatomy faculty. Anatomists’competency in teaching ultrasound was confirmed by the cli-nician sonographer. The clinician competency in teachingultrasound was also confirmed by the clinician sonographer.
Surveys were distributed at the end of the sessions. Stu-dents returned them to a research assistant who collectedand tabulated the anonymous data. The survey data, con-sisting of seven questions rated on a five-point Likert scale(1 5 strongly disagree and 5 5 strongly agree) and one ques-tion rated on yes or no options (Question 5), was gatheredand extrapolated to determine statistical significance andtrends through statistical analysis as detailed below. Quali-tative data, under “comments” were also gathered and ana-lyzed for themes. Triangulation was an important step in
this study to ensure that biases were minimized as much aspossible in the qualitative data analysis (Moustakas, 1994).Concepts and conceptual mapping was done using Lexi-mancer program, version 4.0 (Leximancer, Brisbane,Queensland, Australia), a computer-assisted statistical datasoftware that analyses text. It finds the most commonlyused words and calculates the relevance of other words usedin the text. A colored concept map figure generated usingLeximancer software demonstrates stronger concepts inwarmer colors (red, brown/orange) and more minor, rele-vant concepts in cooler colors (shades of green, blue, andpurple). The size of the circles is a visual representation ofthe concepts. The words within each circle represent the the-saurus of relevant words that were included in the develop-ment of the concept (Sweetman et al., 2013). Facultyassessment of student learning was performed using exami-nation questions at the end of the blocks. Two questionswere put on the first examination and one question in thesecond examination series. Mean, standard deviation andstandard error of the mean, as well as percentages werecalculated for each question.
Design of the Teaching Sessions
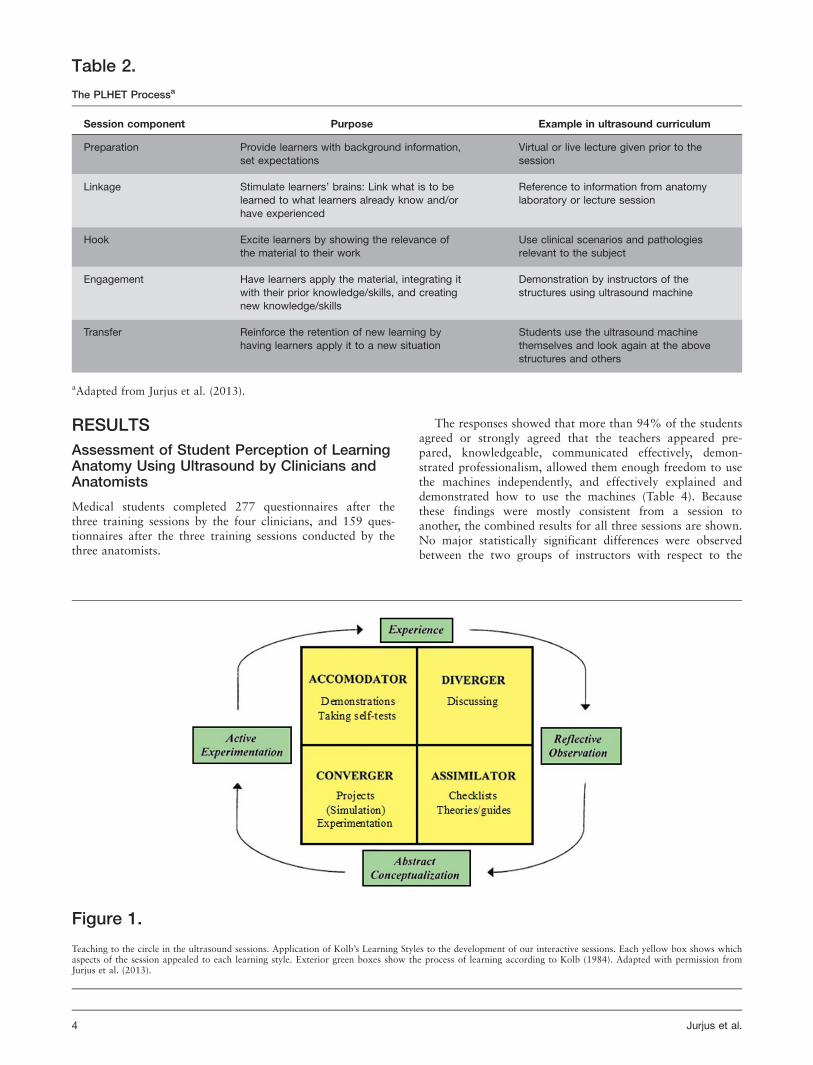
An effective and engaging lecture session (Collins, 2004) con-ducted by the same clinician sonographer that trained theanatomists was first given to the class as an introduction toultrasound, at the beginning of the semester, to orient stu-dents to approach and terminology. Teaching design for theultrasound sessions followed the PLHET model of prepara-tion, linking, hooking, engagement, and transfer describedearlier by Jurjus et al. (2013), (see Table 2). Every effort wasmade to teach to the cycle and ensure all types of learnerswere engaged (Fig. 1). Student handouts given at each ses-sion, which contained clear objectives (Table 3), checklists ofstructures to identify, and theories/guides to ultrasound tech-niques, targeted the Assimilators; demonstrations by faculty-performed ultrasound evaluation of anatomy targeted theAccomodators; discussions on the use of ultrasound inregards to clinical topics targeted the Divergers; extra time toexperiment with ultrasound machines on fellow students tar-geted the Convergers (Kolb, 1984).
The sessions started by having the instructor (clinician oranatomist) going briefly over the anatomical structures on achecklist and demonstrating them to the students usingultrasound.
Then, students were given access to the use of themachine, and under the guidance of the instructor, almost allstudents were given the opportunity to demonstrate a struc-ture or two on themselves, or one of their classmates. Noextra time was available outside of normal class time forextra practice.
Statistical Analysis
Data were subjected to statistical analyses using GraphPadInStat, version 3, software (GraphPad Software, San Diego,CA). Unless otherwise indicated, the differences betweengroups were determined by two-tailed unpaired samplest-tests or an ANOVA (Univariate Analysis of Variance). Sta-tistical significance was set at P� 0.05 for the t-tests andP� 0.001 for the ANOVAs. Bar graphs were generated usingmeans and standard deviation (6SD).
Anatomical Sciences Education MONTH 2013 3
RESULTS
Assessment of Student Perception of LearningAnatomy Using Ultrasound by Clinicians andAnatomists
Medical students completed 277 questionnaires after thethree training sessions by the four clinicians, and 159 ques-tionnaires after the three training sessions conducted by thethree anatomists.
The responses showed that more than 94% of the studentsagreed or strongly agreed that the teachers appeared pre-pared, knowledgeable, communicated effectively, demon-strated professionalism, allowed them enough freedom to usethe machines independently, and effectively explained anddemonstrated how to use the machines (Table 4). Becausethese findings were mostly consistent from a session toanother, the combined results for all three sessions are shown.No major statistically significant differences were observedbetween the two groups of instructors with respect to the
Table 2.
The PLHET Processa
Session component Purpose Example in ultrasound curriculum
Preparation Provide learners with background information,set expectations
Virtual or live lecture given prior to thesession
Linkage Stimulate learners’ brains: Link what is to belearned to what learners already know and/or
have experienced
Reference to information from anatomylaboratory or lecture session
Hook Excite learners by showing the relevance ofthe material to their work
Use clinical scenarios and pathologiesrelevant to the subject
Engagement Have learners apply the material, integrating itwith their prior knowledge/skills, and creating
new knowledge/skills
Demonstration by instructors of thestructures using ultrasound machine
Transfer Reinforce the retention of new learning by
having learners apply it to a new situation
Students use the ultrasound machine
themselves and look again at the abovestructures and others
aAdapted from Jurjus et al. (2013).
Figure 1.
Teaching to the circle in the ultrasound sessions. Application of Kolb’s Learning Styles to the development of our interactive sessions. Each yellow box shows whichaspects of the session appealed to each learning style. Exterior green boxes show the process of learning according to Kolb (1984). Adapted with permission fromJurjus et al. (2013).
4 Jurjus et al.

majority of questions. However, in the combined sessions ofanatomists versus clinicians, two survey questions statisticallyseparated the two groups: Question 3 “Did the teacher pres-ent the information in an organized fashion?” (P� 0.001);Question 8 “Do you feel that ultrasound is helpful withunderstanding the anatomy?” (P� 0.001). An examination ofthe mean student responses to these questions demonstrated aslight increase in positive student responses as the sessionsprogressed for both groups (Fig. 2). Results from unpairedsamples t-tests demonstrated a nonstatistically significant dif-ference between the groups within each session for bothquestions.
Assessment of Students’ Learning Using TestQuestions
After the first ultrasound session, students taught by clini-cians and anatomists had mean scores of 74% and 79%,respectively, on the examination questions that tested thematerial covered in the ultrasound session (Table 5).Unpaired t-test comparing the means of the scores demon-strated this was not statistically significant (P 5 0.376). Simi-larly, after the second ultrasound session, students taught byclinicians and anatomists had mean scores of 89% and 91%,respectively, on the examination question that tested thematerial covered in the ultrasound session (Table 5). A two-tailed unpaired t-test comparing the means of the scores dem-onstrated that this difference is also not statistically signifi-
cant (P 5 0.79). This examination question was illustrated inFigure 3. Finally, student overall performance in the anatomycourse was comparable with the previous year, where theultrasound sessions were only taught by clinicians or even tothe year before, where no ultrasound sessions were given atthat stage (data not shown).
Qualitative Data Analysis
In a nonleading question at the end of the survey, under“Additional comments,” qualitative data obtained from thestudents’ free responses, revealed a clustering under twothemes, both of which were similar between the two teachinggroups.
Students’ Understanding and Perception of theTeaching Improved Over Time
Leximancer extracted the seed concept “Session” (100%),represented in red in the concept map (Fig. 4), and linked itto “helpful” (86%), represented in orange/brown color onthe map. Initially, several students reported being over-whelmed by the amount of information and finding the ses-sions “difficult” (33%), represented in green on the conceptmap. However, as illustrated, the majority of students felt itwas helpful, with one student reporting that, “this was agreat lesson and I hope it gets incorporated more in depthinto the curriculum.” As the sessions progressed, students’comments became more and more positive, as they becamemore interested and understood the clinical and anatomicalrelevance of each session’s content. Students reported thethird sessions was—“the best ultrasound session by far!”—emphasizing not only the students’ preference for later ses-sions, but mainly their increased enthusiasm as they becamemore comfortable with ultrasound.
Student Recommendations on the Method ofTeaching and Timing of the Sessions
Overall, students liked the sessions that were more “hands-on,” where the instructor gave them more “time” (60%) touse the ultrasound machine, as illustrated in dark green onthe concept map. Some students had suggestions on how tomake the sessions “better” (7%) or more “interesting” (3%),as illustrated in the blue shades on the concept map. Severalcomments were geared toward the placement of the ultra-sound session within the curriculum. Student’s favored havingthe sessions later-on in the teaching block of the course,because they found the sessions more interesting after theyalready were exposed to the anatomical topics. Similarly,other students expressed that they “wish these were donelater in the block so we had a better idea of the grossanatomy.” Students also preferred having the sessions later,emphasizing that the ultrasound material “complements thelectures,” highlighting the importance of linking the ultra-sound and lecture content, as means to reinforce the students’overall anatomy learning experience.
DISCUSSION
This study shows that anatomists with focused training canjust as effectively use ultrasound to teach gross anatomy in
Table 3.
Learning Objectives for Ultrasound Session
Session Objectives
Session 1 � To illustrate the difference between varioustissue types (bone, tendon, vessels, muscle,
nerves) on ultrasound.
� To illustrate the 3D anatomy in motion of the
rotator cuff muscles using ultrasound as a tooland its clinical significance.
� To illustrate the 3D anatomy in motion of theknee joint using ultrasound as a tool and itsclinical significance.
Session 2 � To differentiate the 3D anatomy relating tothe major organs/structures in the abdomen,
including the liver, spleen, kidneys.
� To describe the 3D anatomy of the heart and
branches of the aorta.
Session 3 � To illustrate the 3D anatomy of the neck
using ultrasound as a tool and its clinicalsignificance.
� To illustrate the 3D anatomy in motion of theeye using ultrasound as a tool and its clinicalsignificance.
� To employ anatomical landmarks in centralline placement (Seldinger technique) and
ultrasound-guided intravenous (IV) insertions.
Anatomical Sciences Education MONTH 2013 5
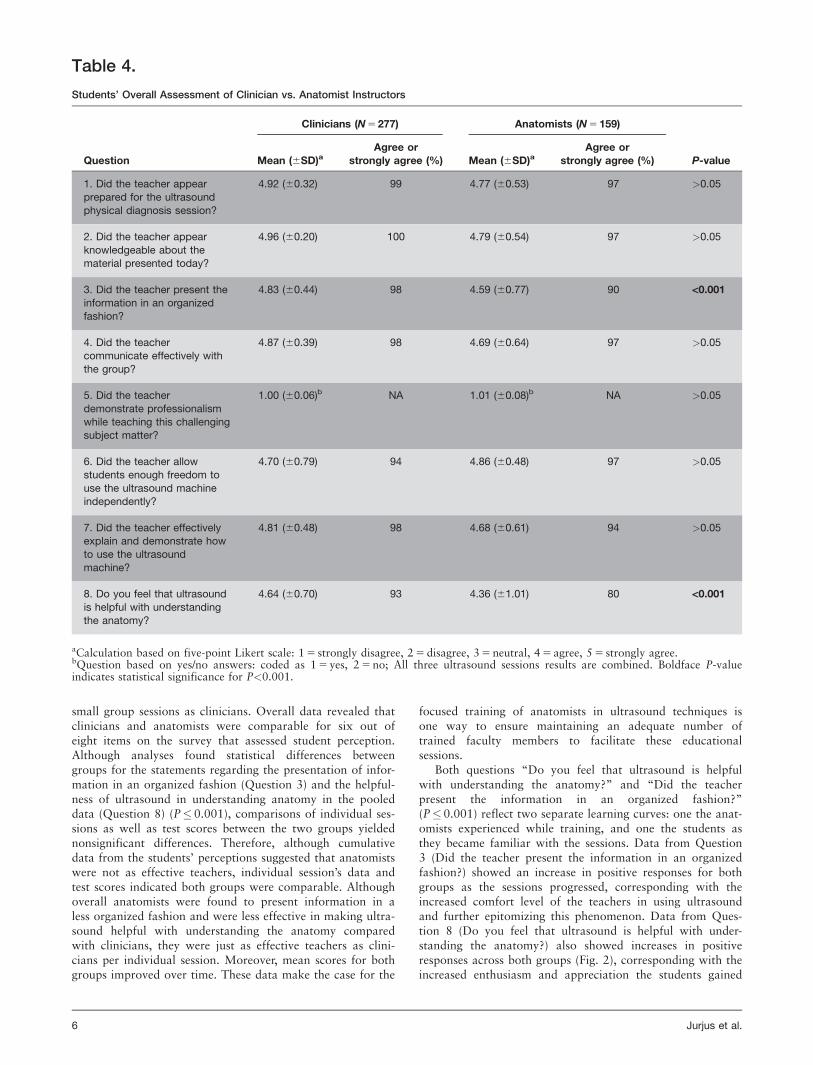
small group sessions as clinicians. Overall data revealed thatclinicians and anatomists were comparable for six out ofeight items on the survey that assessed student perception.Although analyses found statistical differences betweengroups for the statements regarding the presentation of infor-mation in an organized fashion (Question 3) and the helpful-ness of ultrasound in understanding anatomy in the pooleddata (Question 8) (P� 0.001), comparisons of individual ses-sions as well as test scores between the two groups yieldednonsignificant differences. Therefore, although cumulativedata from the students’ perceptions suggested that anatomistswere not as effective teachers, individual session’s data andtest scores indicated both groups were comparable. Althoughoverall anatomists were found to present information in aless organized fashion and were less effective in making ultra-sound helpful with understanding the anatomy comparedwith clinicians, they were just as effective teachers as clini-cians per individual session. Moreover, mean scores for bothgroups improved over time. These data make the case for the
focused training of anatomists in ultrasound techniques isone way to ensure maintaining an adequate number oftrained faculty members to facilitate these educationalsessions.
Both questions “Do you feel that ultrasound is helpfulwith understanding the anatomy?” and “Did the teacherpresent the information in an organized fashion?”(P� 0.001) reflect two separate learning curves: one the anat-omists experienced while training, and one the students asthey became familiar with the sessions. Data from Question3 (Did the teacher present the information in an organizedfashion?) showed an increase in positive responses for bothgroups as the sessions progressed, corresponding with theincreased comfort level of the teachers in using ultrasoundand further epitomizing this phenomenon. Data from Ques-tion 8 (Do you feel that ultrasound is helpful with under-standing the anatomy?) also showed increases in positiveresponses across both groups (Fig. 2), corresponding with theincreased enthusiasm and appreciation the students gained
Table 4.
Students’ Overall Assessment of Clinician vs. Anatomist Instructors
Question
Clinicians (N 5 277) Anatomists (N 5 159)
P-valueMean (6SD)aAgree or
strongly agree (%) Mean (6SD)aAgree or
strongly agree (%)
1. Did the teacher appearprepared for the ultrasound
physical diagnosis session?
4.92 (60.32) 99 4.77 (60.53) 97 >0.05
2. Did the teacher appear
knowledgeable about thematerial presented today?
4.96 (60.20) 100 4.79 (60.54) 97 >0.05
3. Did the teacher present theinformation in an organizedfashion?
4.83 (60.44) 98 4.59 (60.77) 90 <0.001
4. Did the teachercommunicate effectively with
the group?
4.87 (60.39) 98 4.69 (60.64) 97 >0.05
5. Did the teacher
demonstrate professionalismwhile teaching this challengingsubject matter?
1.00 (60.06)b NA 1.01 (60.08)b NA >0.05
6. Did the teacher allowstudents enough freedom to
use the ultrasound machineindependently?
4.70 (60.79) 94 4.86 (60.48) 97 >0.05
7. Did the teacher effectivelyexplain and demonstrate howto use the ultrasound
machine?
4.81 (60.48) 98 4.68 (60.61) 94 >0.05
8. Do you feel that ultrasound
is helpful with understandingthe anatomy?
4.64 (60.70) 93 4.36 (61.01) 80 <0.001
aCalculation based on five-point Likert scale: 1 5 strongly disagree, 2 5 disagree, 3 5 neutral, 4 5 agree, 5 5 strongly agree.bQuestion based on yes/no answers: coded as 1 5 yes, 2 5 no; All three ultrasound sessions results are combined. Boldface P-valueindicates statistical significance for P<0.001.
6 Jurjus et al.

over time for the relevance of ultrasound to the anatomicalor clinical sciences. This phenomenon is further reinforced bythe qualitative data, as evidenced by the linking of “helpful”and “session” in the concept map (Fig. 4). A learning curvereflects improvement over time and shows the potential andthe process that training anatomists to teach using ultrasoundis a good investment.
In this study, learning was evaluated primarily and ini-tially, by asking students to what extent the session hasimproved their understanding of anatomy (Stringer et al.,2012), which addressed Kirkpatricks’ first level of learning,or effective reaction (Kirkpatrick and Kirkpatrick, 2005). Sec-ondarily, learning was evaluated by incorporating, test ques-tions in the examinations for the first two sessions,addressing his second level of learning. One the most impor-tant results from these sets of analyses was the finding thatthere was increased student agreement in the question regard-ing ultrasound’s helpfulness in understanding the anatomyand an increase in scores on the anatomical ultrasound testquestions as the sessions progressed. Students began to enjoythe ultrasound sessions more and appreciate their relevanceto anatomy after the second session as they became morefamiliar with both the ultrasound technique and anatomicalcontent. Correspondingly, scores on the anatomical ultra-sound test questions were also higher after the second ses-sion. These results are consistent with previously publisheddata from Wayne State University School of Medicine thatfound both high student satisfaction for ultrasound educationand high mean class scores on technical assessments (Raoet al., 2008), suggesting that a greater familiarity in ultra-sound may have facilitated anatomical learning. However,the comparisons with overall class scores in years pasts, dem-onstrated no significant differences or improvement in learn-ing, consistent with what others have found (Sweetman et al.,2013).
Ultrasound and similar imaging tools complement the dis-section experience in the gross anatomy laboratory (Griksaitiset al., 2012). Dissection remains an important central teach-ing modality in anatomical education. However, anatomistscontinue to innovate and favor change in the curriculum andbroader learning opportunities (Patel and Moxham, 2006;
Figure 2.
Student mean response to questions: (A) Question #3 “Did the teacher presentthe information in an organized fashion?” and (B) Question #8 “Do you feelthat ultrasound is helpful with understanding the anatomy?” per session whentaught by anatomists or clinicians. As the sessions progressed, there was anincrease in student perception of the helpfulness of ultrasound, regardless ofwhether the session was anatomist or clinician taught. Unpaired samples t-testsdid not exhibit significant differences in mean responses for the individualsessions.
Table 5.
Scores on Examination Questions That Tested the Material Presented in Two Ultrasound Sessions Taught by Clinicians andAnatomists
Examinationquestions scores
SEM
Examinationquestions scores
SEM P-valueMean (6SD) % (6SD)
Session 1 (2 questions)
Anatomist-taught 1.58 (60.30) 0.088 79.20 (615.35) 4.432 0.376
Clinician-taught 1.48 (60.29) 0.065 74.32 (614.62) 3.270
Session 2 (1 question)
Anatomist-taught 0.91 (60.12) 0.035 91.00 (612.88) 3.570 0.790
Clinician-taught 0.89 (60.12) 0.030 89.78 (612.90) 3.042
Anatomical Sciences Education MONTH 2013 7

Drake et al., 2009; Kerby et al., 2011; Johnson et al., 2012).The introduction of an ultrasound curriculum that goes intandem with the anatomical sciences is an opportunity toimprove vertical integration of the anatomical disciplinethroughout the undergraduate medical curriculum. Longitudi-nal integration of the anatomical sciences in the curriculum iswidely supported by clinicians from all disciplines (Waterstonand Stewart, 2005; Zumwalt et al., 2010). However, assimi-lation of knowledge and improved learning may be betterfacilitated by increasing number of sessions and repetition ofthe material (Sweetman et al., 2013). Therefore, withincreases in both of these, the training of anatomists in teach-ing ultrasound would be essential for such improvements.The main focus here was to train the anatomy faculty andshow they can equally teach using ultrasound, because theywill be the ones to champion and guide the endeavor’s suc-cess (Hoppmann et al., 2011). The strength of these sessionslies in well-prepared and enthusiastic instructors (Wright andBell, 2008).
LIMITATIONS
This study is limited by several factors. Whereas only threeanatomists were available for training and teaching for allsessions, the clinicians came from a larger, more variablepool and this could have introduced some variability in ourstudy. Specialties and teaching experience of the instructorsmay play an influencing role in using ultrasound to teachanatomical science. Analysis of the data by the specialties ofour clinician instructors may be an important factor to con-sider in the future (Brown et al., 2012). Students were alsomore familiar with anatomy faculty, which could have influ-enced their perception. Finally, this study was performed at asingle medical school with one class of students, limiting theextrapolation of the results to other institutions. Repeatingthis study at a multicenter level is currently being consideredto further validate the conclusion. The positive wording ofthe questionnaire and the enthusiasm of the faculty teaching
may have introduced a bias toward favorable responses. Thecontent of the third session is different from first two becauseit has a component of interventional ultrasound that not onlymay be a major confounding variable to explain our findings,but also may be a more appropriate topic for the later clini-cal years. However, the aim of the third session was to focuson the anatomical landmarks needed to be identified viaultrasound to perform such a technique and not the tech-nique itself. Because it is believed that ultrasound sessionswill increase medical student comfort with future clinical sit-uations (Brown et al., 2012), an end of the semester surveyalong the lines of preparation for real-life scenarios may beappropriate. Moreover, the hands-on component reinforcesfurther ease with ultrasound skills later in the students’ medi-cal trajectories. Additionally, no test question was includedon the examination for the third part of the course for logis-tical reasons with timing of the NBME examination, limitingthe ability to associate perception with actual learningthroughout all three sessions. Finally, the authors acknowl-edge that a real assessment of learning outcomes would haveto consist of more than few examination questions.
Figure 3.
Assessment of learning anatomical relationships using ultrasound. Test ques-tions pertaining to the ultrasound sessions were added to anatomy examina-tions. Illustrated here is an example of the question from Examination II,pointing at the splenic artery branching from the celiac trunk.
Figure 4.
Concept map figure. A colored concept map figure generated using Leximancersoftware program shows the strongest concept in warmer colors (red, brown/orange) and the less relevant concepts in cooler colors (shades of green, blue,and purple here). The size of the circles is a visual representation of the con-cepts. The words within each circle represent the thesaurus of relevant wordsthat were included in the development of the concept.
8 Jurjus et al.

CONCLUSIONS
This study demonstrated that overall anatomists were foundto present information in a less organized fashion and wereless effective in making ultrasound helpful with understand-ing the anatomy compared with clinicians. However, theywere just as effective teachers as clinicians per individual ses-sion and mean scores for both groups improved over time.Scores from examination questions yielded nonsignificant dif-ference between the two groups, demonstrating that anato-mists are just as effective ultrasound teachers from a grossanatomy standpoint. A learning curve was observed for bothteachers and students, where the former grew more comforta-ble with teaching over time, while the latter grew comforta-ble with the material and a gained a greater appreciation forultrasound in anatomy, resulting in a more positive percep-tion of ultrasound. Based on these results, training anatomiststo teach clinically relevant anatomy using ultrasound is apromising and feasible educational approach to train futurephysicians.
ACKNOWLEDGMENTS
The authors would like to acknowledge the generous support ofthe GWU CLASS center for providing educational ultrasoundmachines and instructional spaces. We are in debt to the follow-ing individuals for their time and quality teaching: Drs. Kat Cal-abrese, Mandana Hashefi, Hope Jackson, and MohammadSalimian. They also thank Ms. Gisela Butera for her help withthe referencing, formatting of this manuscript, and acquiringthe student demographic data and Mr. Steve Harrison for hishelp in summarizing the quantitative examination questionsdata.
NOTES ON CONTRIBUTORS
ROSALYN A. JURJUS, M.D., Ph.D., is an assistant professorin the Department of Anatomy and Regenerative Biology atthe George Washington University School of Medicine andHealth Sciences, Washington, DC. She teaches the anatomicaldisciplines, gross anatomy, and microscopic anatomy to first-year medical students and other graduate and undergraduatestudents.
KATHRYN DIMORIER, B.S., is a patient care technicianand clinical scribe in the Department of Emergency Medicineat the George Washington University Hospital, Washington,DC. She has a Bachelor’s of Science in Chemistry from theGeorge Washington University.
KIRSTEN BROWN, Ph.D., is a lecturer in the Depart-ment of Anatomy and Regenerative Biology at the GeorgeWashington University School of Medicine and Health Scien-ces, Washington, DC. She teaches the anatomical disciplines,gross anatomy, and neuroanatomy to first-year medical stu-dents and other graduate and undergraduate students.
FRANK SLABY, Ph.D., is a professor in the Departmentof Anatomy and Regenerative Biology at the George Wash-ington University School of Medicine and Health Sciences,Washington, D.C. He is director of the gross anatomy coursefor first-year medical students, director of the anatomycourse for physician assistant students, and lecturer in thegross anatomy course for undergraduate students.
HAMID SHOKOOHI, M.D., M.P.H., R.D.M.S., is anassistant professor of emergency medicine in the Departmentof Emergency Medicine at the George Washington University
School of Medicine and Health Sciences, Washington, DC.He is the Director of Research for Emergency Ultrasound sec-tion and is well published in the clinical and educationalapplications of point-of-care ultrasound. He teaches ultra-sound to physicians, fellows, residents, and students and hehas been heavily involved with the integration and efficiencyof pre-clinical medical student ultrasound education.
KEITH BONIFACE, M.D., R.D.M.S., is an associate pro-fessor of emergency medicine in the Department of Emer-gency Medicine at George Washington University School ofMedicine and Health Sciences. He is the Chief of EmergencyUltrasound in the Department of Emergency Medicine andhas been active in ultrasound education and research.
YIJU TERESA LIU, M.D., is an assistant professor ofemergency medicine in the Department of Emergency Medi-cine at the George Washington University School of Medicineand Health Sciences, Washington, DC. She is the fellowshipdirector for Emergency Ultrasound section, the clerkshipdirector for the bedside ultrasound elective, and teaches bed-side ultrasound internationally and nationally to physicians,basic scientists, and physician trainees of various disciplines.
LITERATURE CITEDBahner DP, Jasne A, Boore S, Mueller A, Cortez E. 2012. The ultrasound chal-lenge: A novel approach to medical student ultrasound education. J UltrasoundMed 31:2013–2016.
Barloon TJ, Brown BP, Abu-Yousef MM, Ferguson KJ, Schweiger GD,Erkonen WE, Schuldt SS. 1998. Teaching physical examination of the adultliver with use or real-time sonography. Acad Radiol 5:101–103.
Brown B, Adhikari S, Marx J, Lander L, Todd GL. 2012. Introduction ofultrasound into gross anatomy curriculum: Perceptions of medical students. JEmerg Med 43:1098–1102.
Butter J, Grant TH, Egan M, Kaye M, Wayne DB, Carri�on-Carire V,McGaghie WC. 2007. Does ultrasound training boost year 1 medical studentcompetence and confidence when learning abdominal examination? Med Educ41:843–848.
Collins J. 2004. Education techniques for lifelong learning: Giving a Power-Point presentation: The art of communicating effectively. Radiographics 24:1185–1192.
Drake RL, McBride JM, Lachman N, Pawlina W. 2009. Medical education inthe anatomical sciences: The winds of change continue to blow. Anat Sci Educ2:253–259.
Griksaitis MJ, Sawdon MA, Finn GM. 2012. Ultrasound and cadaveric prosec-tions as methods for teaching cardiac anatomy: A comparative study. Anat SciEduc 5:20–26.
Hoppmann RA, Rao VV, Poston MB, Howe DB, Hunt PS, Fowler SD,Paulman LE, Wells JR, Richeson NA, Catalana PV, et al. 2011. An integratedultrasound curriculum (iUSC) for medical students: 4-Year experience. CritUltrasound J 3:1–12.
Ivanusic J, Cowie B, Barrington M. 2010. Undergraduate student perceptionsof the use of ultrasonography in the study of “living anatomy”. Anat Sci Educ3:318–322.
Johnson EO, Charchanti AV, Troupis TG. 2012. Modernization of an anatomyclass: From conceptualization to implementation. A case for integratedmultimodal-multidisciplinary teaching. Anat Sci Educ 5:354–366.
Jurjus RA, Krum J, Goldman EF. 2013. Design for learning: Adapting themicroscopic anatomy laboratory to adult learners. Anat Sci Educ 6:177–181.
Kerby J, Shukur ZN, Shalhoub J. 2011. The relationships between learningoutcomes and methods of teaching anatomy as perceived by medical students.Clin Anat 24:489–497.
Kirkpatrick DL, Kirkpatrick JD. 2005. Transferring Learning to Behavior:Using the Four Levels to Improve Performance. 1st Ed. San Francisco, CA:Berrett-Koehler Publishers Inc. 220 p.
Kolb DA. 1984. Experiential Learning: Experiences as the Source of Learningand Development. 1st Ed. Upper Saddle River, NJ: Prentice Hall. 256 p.
Lazarus MD, Chinchilli VM, Leong SL, Kauffman GL Jr. 2012. Perceptions ofanatomy: Critical components in the clinical setting. Anat Sci Educ 5:187–199.
Moustakas CE. 1994. Phenomenological Research Methods. 1st Ed. ThousandOaks, CA: Sage Publications Inc. 208 p.
Patel KM, Moxham BJ. 2006. Attitudes of professional anatomists to curricu-lar change. Clin Anat 19:132–141.
Rao S, Van Holsbeeck L, Musial JL, Parker A, Bouffard JA, Bridge P, JacksonM, Dulchavsky SA. 2008. A pilot study of comprehensive ultrasound
Anatomical Sciences Education MONTH 2013 9

education at the Wayne State University School of Medicine: A pioneer yearreview. J Ultrasound Med 27:745–749.
Stringer MD, Duncan LJ, Samalia L. 2012. Using real-time ultrasound to teachliving anatomy: An alternative model for large classes. N Z Med J 125:37–45.
Sugand K, Abrahams P, Khurana A. 2010. The anatomy of anatomy: A reviewfor its modernization. Anat Sci Educ 3:83–93.
Swamy M, Searle RF. 2012. Anatomy teaching with portable ultrasound tomedical students. BMC Med Educ 12:99.
Sweetman GM, Crawford G, Hird K, Fear MW. 2013. The benefits and limita-tions of using ultrasonography to supplement anatomical understanding. AnatSci Educ 6:141–148.
Teichgr€aber UK, Meyer JM, Poulsen Nautrup C, von Rautenfeld DB. 1996.Ultrasound anatomy: A practical teaching system in human gross anatomy.Med Educ 30:296–298.
Waterston SW, Stewart IJ. 2005. Survey of clinicians’ attitudes to the anatomi-cal teaching and knowledge of medical students. Clin Anat 18:380–384.
Wittich CM, Montgomery SC, Neben MA, Palmer BA, Callahan MJ, SewardJB, Pawlina W, Bruce CJ. 2002. Teaching cardiovascular anatomy to medicalstudents by using a handheld ultrasound device. JAMA 288:1062–1063.
Wright SA, Bell AL. 2008. Enhancement of undergraduate rheumatologyteaching through the use of musculoskeletal ultrasound. Rheumatology(Oxford) 47:1564–1566.
Yoo MC, Villegas L, Jones DB. 2004. Basic ultrasound curriculum for medicalstudents: Validation of content and phantom. J Laparoendosc Adv Surg TechA 14:374–379.
Zumwalt AC, Luefler RS, Monteiro J, Shaffer K. 2010. Building the body:Active learning laboratories that emphasize practical aspects of anatomy andintegration with radiology. Anat Sci Educ 3:134–140.
10 Jurjus et al.