canadian forces flight safety investigation report...
TRANSCRIPT

CANADIAN FORCES FLIGHT SAFETY INVESTIGATION REPORT (FSIR)
FINAL REPORT
FILE NUMBER: 1010-12438 (DFS 2-2) DATE OF REPORT: 30 January 2008 AIRCRAFT TYPE: CH124A Sea King DATE/TIME: 02 1932Z February 2006 LOCATION: HMCS ATHABASKAN 56048N 011011E
(30 NM E Aalborg, Denmark) CATEGORY: "A" Category Accident
This report was produced under authority of the Minister of National Defence (MND) pursuant to section 4.2 of the Aeronautics Act, and in accordance with
A-GA-135-001/AA-001, Flight Safety for the Canadian Forces.
With the exception of Part 1, the contents of this report shall only be used for the purpose of accident prevention. This report was released to the public under the authority of the
Director of Flight Safety (DFS), National Defence Headquarters, pursuant to powers delegated to him by the MND as the Airworthiness Investigative Authority (AIA) of the
Canadian Forces.
SYNOPSIS
After completing night circuit training at Aarhus Denmark, the five crewmembers onboard the Sea King helicopter were returning to Her Majesty’s Canadian Ship (HMCS) ATHABASKAN when the accident occurred. On completion of one radar controlled approach to the ATHABASKAN, the crew commenced an overshoot and entered the visual circuit to land. On short final, at approximately 30 meters off of the ATHABASKAN’s port quarter, the helicopter’s rear fuselage and tail rotor contacted the water. The helicopter pitched forward, became airborne again, and began to yaw to the right. The helicopter then impacted the water in a near level attitude and, while still yawing right, rolled left. Water flooded the helicopter almost immediately as it rolled inverted. All five crewmembers then egressed and were recovered to the ATHABASKAN, by Zodiac, within approximately 15 minutes. One crewmember received minor injuries. The aircraft remained afloat for approximately one hour, and then sank in 16 meters of water.
i

TABLE OF CONTENTS 1 FACTUAL INFORMATION ....................................................................................... 1
1.1 HISTORY OF THE FLIGHT........................................................................................ 1 1.2 INJURIES TO PERSONNEL....................................................................................... 2 1.3 DAMAGE TO AIRCRAFT........................................................................................... 2 1.4 COLLATERAL DAMAGE ........................................................................................... 3 1.5 PERSONNEL INFORMATION .................................................................................... 3 1.6 AIRCRAFT INFORMATION ........................................................................................ 4 1.7 METEOROLOGICAL INFORMATION .......................................................................... 4 1.8 AIDS TO NAVIGATION ............................................................................................. 4 1.9 COMMUNICATIONS ................................................................................................. 4 1.10 AERODROME INFORMATION ................................................................................... 5 1.11 FLIGHT RECORDERS .............................................................................................. 5 1.12 WRECKAGE AND IMPACT INFORMATION ................................................................ 5 1.13 MEDICAL................................................................................................................. 6 1.14 FIRE, EXPLOSIVES DEVICES, AND MUNITIONS ...................................................... 6 1.15 SURVIVAL ASPECTS ............................................................................................... 6 1.16 TEST AND RESEARCH ACTIVITIES.......................................................................... 9 1.17 ORGANIZATIONAL AND MANAGEMENT INFORMATION.......................................... 10 1.18 ADDITIONAL INFORMATION- AIRCRAFT RECOVERY ............................................. 10 1.19 USEFUL OR EFFECTIVE INVESTIGATION TECHNIQUES ........................................ 11
2 ANALYSIS ................................................................................................................. 12
2.1 THE ACCIDENT ..................................................................................................... 12 2.2 MARITIME HELICOPTER APPROACH PROCEDURES............................................. 14 2.3 INADVERTENT DESCENT ...................................................................................... 16 2.4 PHYSIOLOGICAL EFFECTS ................................................................................... 17 2.5 AIRCREW CURRENCY REQUIREMENTS................................................................ 19 2.6 IPVMS ANALYSIS ................................................................................................ 25 2.7 ANALYSIS OF AVIATION LIFE SUPPORT EQUIPMENT ........................................... 27 2.8 SHIP’S FLIGHT DECK CAMERA............................................................................. 31 2.9 NIGHT VISION GOGGLES...................................................................................... 32
3 CONCLUSIONS ........................................................................................................ 33
3.1 FINDINGS .............................................................................................................. 33 3.2 CAUSE(S) AND CONTRIBUTING FACTOR(S) ......................................................... 35 3.3 CONTRIBUTING CAUSE FACTORS ........................................................................ 35
4 PREVENTIVE MEASURES .................................................................................... 36
4.1 PREVENTIVE MEASURES TAKEN.......................................................................... 36 4.2 PREVENTIVE MEASURES RECOMMENDED........................................................... 36 4.3 OTHER SAFETY CONCERNS ................................................................................ 38 4.4 DFS REMARKS .................................................................................................... 39
Annex A: Abbreviations………………….……………………………………………A-1 Annex B: Photographs ……………………………………………………………….B-1 Annex C: Figures………………………………………………………………………C-1
ii
1 FACTUAL INFORMATION
GENERAL
The Sea King helicopter was embarked on HMCS ATHABASKAN, the Standing NATO Maritime Group 1 (SNMG 1) flagship. The Helicopter Air Detachment (HELAIRDET) was from 423 Maritime Helicopter (MH) Squadron. The Sea King helicopter was crewed by five personnel; the MH Captain (MHC), was seated in the left seat, the MH Co-Pilot (MHCP) in the right seat, the Tactical Co-ordinator (TACCO), and the Airborne Electronic Sensor Operator (AESOP) with a second MH Co-Pilot (MHCP1) who was seated in the rear cabin of the aircraft. All times are Universal Time Coordinated (Z); local time was Z plus one hour.
1.1 History of the Flight
On 02 February 2006, the ATHABASKAN was sailing in the Baltic Sea in company with the SNMG 1 fleet, east of Denmark.
At 1656Z, the aircraft departed the ship to conduct a night pilot training mission at the local airfield in Aarhus, Denmark. For the first half of the flight, MHCP1 was seated in the right cockpit seat. On completion of his training sequences, the MHCP replaced him in the right cockpit seat and MHCP1 moved to the centre troop seat in the rear cabin of the aircraft. The airfield training then continued until the aircraft returned to the ATHABASKAN to prepare for deck landing practice. With a ceiling of approximately 700 feet, visibility of six nautical miles (NM), the aircraft commenced a radar controlled approach (RCA) at 1915Z. The helicopter continued to approach the ship, when at 0.6 NM on short-final, the Ship’s Air Controller (SAC) monitoring internal communications between the Landing Signals Officer (LSO) and the Flying Coordinator (FLYCO) perceived an indication that the flight deck landing lights were not at the correct intensity settings. The SAC then directed the helicopter crew to commence an overshoot and to contact the LSO for control in order to allow time to confirm that the flight deck lighting was correctly set. The crew complied with the SAC’s direction and climbed to 200 feet while proceeding upwind to conduct a visual circuit and approach for landing. With the MHC still at the controls, flying on instruments, the MHCP provided lateral spacing information to allow the MHC to turn onto final between one to two NM behind the ship. By about one NM, the aircraft commenced a descent to 100 feet and a deceleration to between 60 to 70 knots prior to reaching one-half NM. Once inside one-half NM, the MHCP then asked the MHC to descend further to 80 feet. The MHCP then called visual with the ship and took control of the aircraft to fly the approach using visual references. The MHCP began the transition to the hover. As the aircraft descended through 20 feet, the MHC came onto the controls and raised the collective in an effort to prevent contact with the sea surface. The aircrew then felt a solid bump as the aircraft contacted the water. The helicopter quickly became airborne again and began to yaw to the right. The MHC then lowered the collective and applied right cyclic, allowing the aircraft to land on the surface in a near-level attitude as it
1/39

continued to yaw right, while simultaneously starting to roll left. The aircraft rolled over onto its left side and the main rotor blades contacted the water’s surface. The crash sequence occurred about 30 meters from the flight deck, on the ATHABASKAN’s port quarter.
Water quickly entered the aircraft cabin as the aircraft continued to roll to an inverted position floating on the surface (Photograph 1). The ATHABASKAN immediately came to Emergency Flying Stations and commenced a turn back to the crash site. As the aircrew surfaced after conducting an underwater emergency egress from the aircraft, they attempted to signal the ship using their strobe lights, helmet-mounted lip lights, a night flare, and a chemical light stick. Meanwhile the ship’s searchlight was trained on them. The ATHABASKAN’s rescue diver approached in a Zodiac and recovered all five crewmembers within nine minutes post-crash. By 1948Z all five aircrew were recovered onboard the ATHABASKAN. At 2042Z the aircraft sank in 16 meters of water in position 56.48.58N 011.11.96E.
1.2 Injuries to Personnel
Injuries Crew Passengers Others Fatal 0 0 0
Serious 0 0 0 Minor 1 0 0
Table 1: Injuries to Personnel
1.3 Damage to Aircraft
The aircraft was submerged in 16 metres of seawater for approximately 25 hours, resulting in severe corrosion to the avionics equipment and electrical wiring. Moderate corrosion to the airframe was also observed throughout the aircraft. After recovery to a salvage barge (Photograph 2), the aircraft was rinsed with fresh water and corrosion control measures were initiated to minimise further material degradation.
Much of the helicopter’s damage was restricted to the rotor system, the main gearbox (MGB) and accessory sections such as the radome, oil cooler, and generators. Two main rotor blades wrapped around the main rotor head while the remaining three fractured and were not recovered (Photograph 3). Numerous gouges and severed hydraulic and lubrication lines were observed on the MGB. As a result, the MGB lost most of its lubricating oil and filled up with seawater. MGB oil samples indicated a large number of metallic particles, indicative of significant internal deterioration of MGB components as a result of the sudden main rotor blade stoppage.
The number one engine’s sudden stoppage, caused by the water ingestion, resulted in significant internal damage to the compressor blades. Corrosion on the compressor blades was also identified after the aircraft was recovered. The
2/39
fibreglass constructed foreign object deflector shed pieces when it hit the water. Debris entered the number two engine, which caused significant damage to the compressor blades.
The upper left portion of the cabin fuselage suffered a main rotor blade strike just above the middle troop seat. The upper tail pylon area was also severely damaged as a result of a tail rotor blade strike. Three of the tail rotor blades were bent and two were completely sheared off (Photograph 4). The main landing gear was up at the time of the impact. The sponsons suffered compression skin damage while the tail pylon showed skin buckling.
The Aircraft Damage Level is categorized as “damaged beyond economical repair.”
1.4 Collateral Damage
A site survey conducted by the Royal Danish Air Force accident investigator, who was part of the Flight Safety Investigation Team, assessed that negligible environmental impact was incurred as a result of the accident.
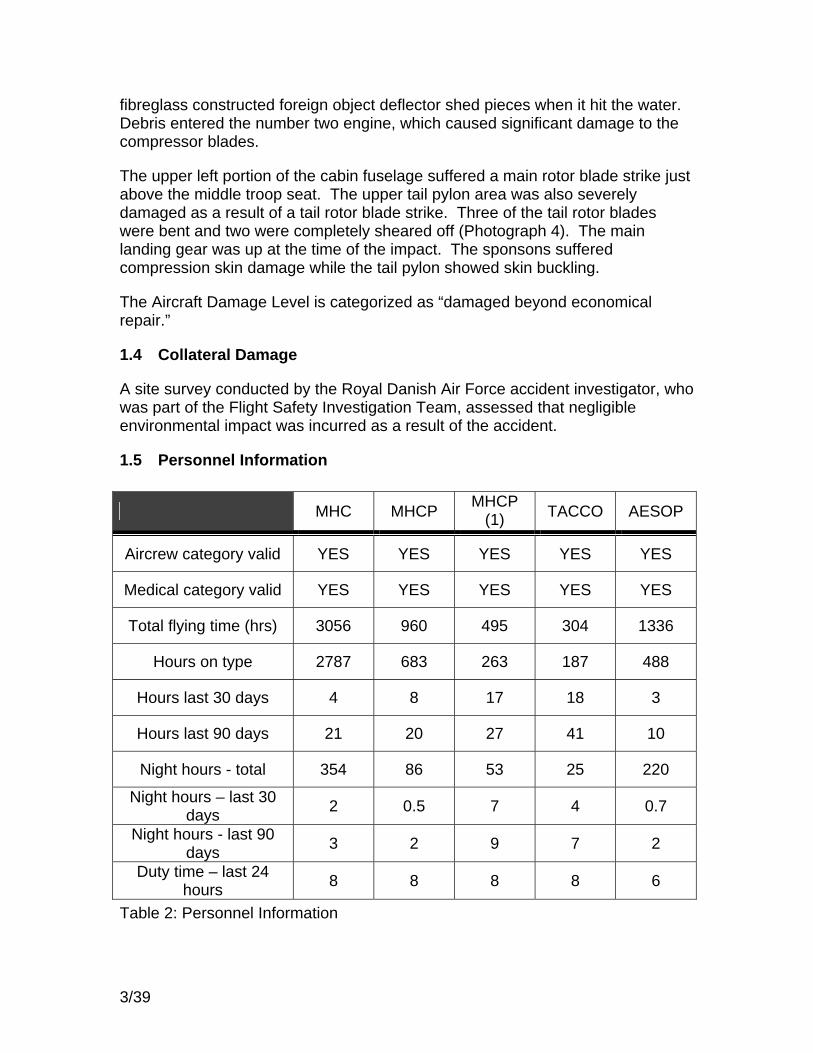
1.5 Personnel Information
MHC MHCP MHCP (1) TACCO AESOP
Aircrew category valid YES YES YES YES YES
Medical category valid YES YES YES YES YES
Total flying time (hrs) 3056 960 495 304 1336
Hours on type 2787 683 263 187 488
Hours last 30 days 4 8 17 18 3
Hours last 90 days 21 20 27 41 10
Night hours - total 354 86 53 25 220
Night hours – last 30 days 2 0.5 7 4 0.7
Night hours - last 90 days 3 2 9 7 2
Duty time – last 24 hours 8 8 8 8 6
Table 2: Personnel Information
3/39

1.6 Aircraft Information
CH12438 embarked HMCS ATHABASKAN on 11 January 2006. The aircraft was a Mk III model with T58-GE-100 engines and a 24000 series MGB. It was declared fully serviceable at the time of embarkation and when it launched for the final flight.
On 21 January 2006, the right engine was changed after suffering a compressor stall. The aircraft was successfully test flown and declared serviceable on 31 January 2006.
1.7 Meteorological Information
The following information was taken from the ATHABASKAN’s Ship Meteorological Log for 02 1930 Z February 2006, the approximate time of the accident.
Wind light and variable, visibility 6 statute miles with mist. Clouds SCT 004 OVC 007, SF4ST4 Temperature 2.3° Celsius Dew point 1.0° Altimeter 30.00 Sea state 1, height 1 foot, period 4 Sea temperature 2.0° Celsius METAR - CYWM 021700Z 29008KT 6SM BR SCT004 OVC007 3/1 A29.99 TAF - CYWM 021730Z 021806 24009KT 6SM BR SCT004 OVC007 SUNSET: 1537Z EVENING TWILIGHT: 1617Z
1.8 Aids to Navigation
N/A.
1.9 Communications
During normal flying operations, four departments onboard the ATHABASKAN are on the internal communications system (ICS): the SAC, who controls aircraft via radar; the LSO, who controls the aircraft visually within the ship’s control zone and over the flight deck; the FLYCO, who controls flight deck lighting, damage control, and fire fighting measures; and the Second Officer of the Watch, who liaises between the LSO and the Officer of the Watch to execute flying operations. Each department monitors all communications on the ICS when the ship is at flying stations.
Radio communications between the aircraft and the ship are through either the SAC or LSO, depending on the phase of flight.
4/39

1.10 Aerodrome Information
HMCS ATHABASKAN is a Guided Missile Area Air Defence Destroyer (DDH) from the 280 Iroquois Class. It has a hangar and flight deck located just aft of amidships. The landing deck of the ship is approximately 30 feet above the water. The ship has hangar capacity for two CH124 or similar aircraft, however it only carried one helicopter during this deployment.
Flying operations on the flight deck are controlled by the LSO from the Howdah position. The Howdah is a small cut out position in the forward starboard flight deck area. FLYCO controls flight deck fire/rescue operations from his control room, which is elevated above the flight deck in the aft port hangar section.
On a normal radar controlled approach, SAC controls the helicopter via radar until the helicopter is within one half nautical mile of the ship. At that point, the pilots take over visually. As the helicopter approaches the ship, the deck lights will be changed to “two mile lighting” and “one mile lighting”. In the two mile configuration, the large Horizon Bars and Centre Line lights are on. The ship’s Strobe lights may also be used if required in poor weather. In the one mile light configuration the Centre line and Strobe lights are turned off and the Hangar Face, Hangar Top and Dustpan lights (located around the perimeter of the flight deck), are turned on. This change in lighting is done by the FLYCO when the pilots change the aircraft lighting, turning the navigation lights and side position lights off and the probe lights on.
Normally, the helicopter conducts an approach to hover on either the port or starboard side of the ship. Upon receiving clearance from the LSO, the helicopter slides over the flight deck to the high hover position of 15 to 17 feet. When the ship’s motion has steadied, the helicopter descends to the low hover and lands when cleared to by the LSO.
1.11 Flight Recorders
The CH124 fleet is not fitted with cockpit voice recorders or flight data recorders. The aircraft was equipped with an Instrument Panel Video Monitoring System (IPVMS). The IPVMS is an onboard video recorder that records images from four separate cameras, three focused on the instrument panels and one providing a generic overview of the aircraft cockpit. The IPVMS is not designed to be crash survivable.
All Canadian flight deck-equipped warships have a flight deck video monitoring and recording system. The ATHABASKAN’s flight deck video did not record the accident.
1.12 Wreckage and Impact Information
At 1932Z the helicopter impacted the water at position 56. 48N 011.11E. The impact and subsequent roll over caused several tail rotor blades and sections of
5/39

the main rotor blades to depart the aircraft. The aircraft came to rest inverted, and remained afloat for approximately one hour. During that time, the sea current carried the inverted, floating wreckage approximately one NM. The airframe body remained mostly intact throughout this time. At 2042Z the aircraft sank at position 56.49N 011.12E. The helicopter was recovered approximately 25 hours later. Small debris from the helicopter, and some personal effects, were strewn about the seabed and were not recovered.
1.13 Medical
The five aircrew members were immediately tended to by the ship’s medical personnel. Due to an insufficient supply of sampling kits onboard the ATHABASKAN, only four toxicological samples were taken by the ship's Flight Surgeon for analysis. Several of these toxicology sampling kits were found to be time expired. Additionally, one crewmember was permitted to ingest a cola soft drink immediately prior to providing samples. Procedural difficulties onboard the ATHABASKAN resulted in a delay of shipping the toxicology samples to the Armed Forces Institute of Pathology in Bethesda, Maryland, USA. Toxicology results were negative.
All crewmembers reported prolonged numbness in their fingers as a result of exposure to the 2°Celcius water. For several members this sensation remained up to two days post-accident. Only one crewmember received minor injuries as a result of squeezing through the right cockpit window.
1.14 Fire, Explosives Devices, and Munitions
At the time of accident, the aircraft was armed with three sonobuoys, six C2A1 smoke markers and three electronic sound signalling devices (ESUS). The smoke markers and sonobuoys were not recovered. The three ESUS were still on the helicopter and had been activated by salt-water immersion. Although equipped with a self-defence suite, no chaff or flares were onboard. There was no post-crash fire or detonation. The aircraft also had explosive cartridges incorporated into various systems, such as the emergency hoist cable cutting system and the fire bottles. These cartridges were removed from the aircraft and handed over to the Royal Danish Navy for disposal.
1.15 Survival Aspects
1.15.1 Crash Survivability and Emergency Egress
The crash was survivable. The cockpit and all crew positions within the airframe maintained survivable volumes. The deceleration forces were small and well within the tolerance level of the human body. The floating helicopter rolled inverted soon after impacting the water and rapidly filled with cold water. This, combined with the almost total darkness, greatly exacerbated the difficulty of the aircrew’s escape. The following descriptions detail the egress actions completed by the aircrew in their probable order of leaving the helicopter:
6/39
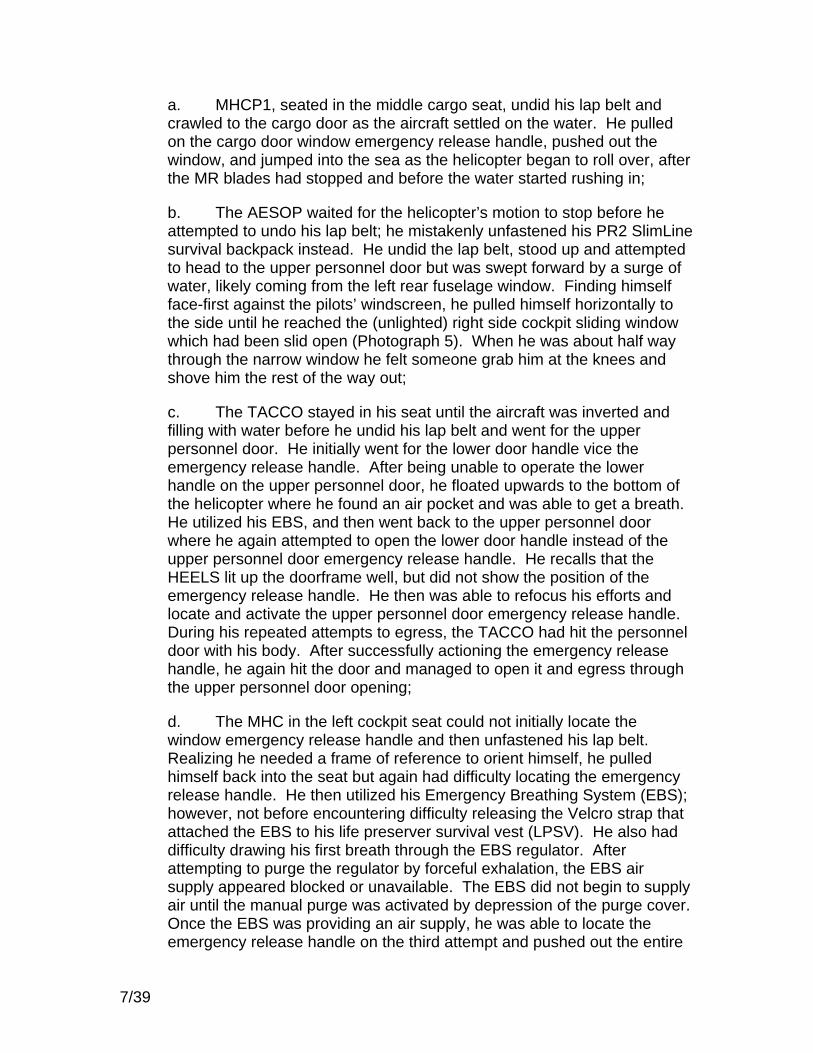
a. MHCP1, seated in the middle cargo seat, undid his lap belt and crawled to the cargo door as the aircraft settled on the water. He pulled on the cargo door window emergency release handle, pushed out the window, and jumped into the sea as the helicopter began to roll over, after the MR blades had stopped and before the water started rushing in;
b. The AESOP waited for the helicopter’s motion to stop before he attempted to undo his lap belt; he mistakenly unfastened his PR2 SlimLine survival backpack instead. He undid the lap belt, stood up and attempted to head to the upper personnel door but was swept forward by a surge of water, likely coming from the left rear fuselage window. Finding himself face-first against the pilots’ windscreen, he pulled himself horizontally to the side until he reached the (unlighted) right side cockpit sliding window which had been slid open (Photograph 5). When he was about half way through the narrow window he felt someone grab him at the knees and shove him the rest of the way out;
c. The TACCO stayed in his seat until the aircraft was inverted and filling with water before he undid his lap belt and went for the upper personnel door. He initially went for the lower door handle vice the emergency release handle. After being unable to operate the lower handle on the upper personnel door, he floated upwards to the bottom of the helicopter where he found an air pocket and was able to get a breath. He utilized his EBS, and then went back to the upper personnel door where he again attempted to open the lower door handle instead of the upper personnel door emergency release handle. He recalls that the HEELS lit up the doorframe well, but did not show the position of the emergency release handle. He then was able to refocus his efforts and locate and activate the upper personnel door emergency release handle. During his repeated attempts to egress, the TACCO had hit the personnel door with his body. After successfully actioning the emergency release handle, he again hit the door and managed to open it and egress through the upper personnel door opening;
d. The MHC in the left cockpit seat could not initially locate the window emergency release handle and then unfastened his lap belt. Realizing he needed a frame of reference to orient himself, he pulled himself back into the seat but again had difficulty locating the emergency release handle. He then utilized his Emergency Breathing System (EBS); however, not before encountering difficulty releasing the Velcro strap that attached the EBS to his life preserver survival vest (LPSV). He also had difficulty drawing his first breath through the EBS regulator. After attempting to purge the regulator by forceful exhalation, the EBS air supply appeared blocked or unavailable. The EBS did not begin to supply air until the manual purge was activated by depression of the purge cover. Once the EBS was providing an air supply, he was able to locate the emergency release handle on the third attempt and pushed out the entire
7/39
window (Photograph 6). He then egressed through the window and ascended nine feet to the surface; and
e. The MHCP in the right cockpit seat grabbed his EBS and placed it in his mouth as the aircraft rolled over. Despite repeated attempts, he could not locate the window emergency release handle though he was able to effortlessly move the sliding part of the window fully aft. During his struggles, the MHCP perceived a crewmember beside and in front of him in the cockpit, attempting to exit. The MHCP then grabbed the crewmember’s legs and assisted him out of the right window. He again tried to locate the emergency release handle, but without success, and undid his lap belt. He attempted to fit through the window but became jammed and returned to his seat position. He tried to undo his PR2 SlimLine survival backpack but, although he found the buckle, he could not undo it. He again attempted to exit through the window and again got stuck at chest level so he exhaled his breath and started to kick. His feet then found a solid purchase from which he could push and he egressed through the sliding window opening.
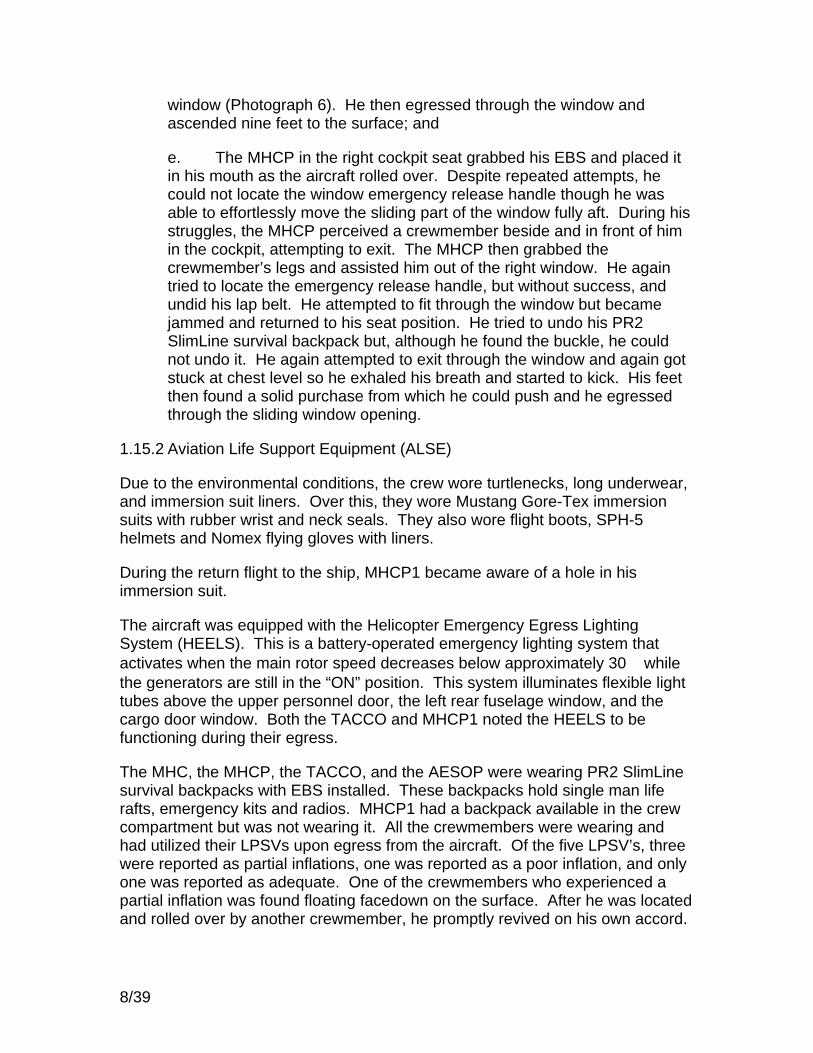
1.15.2 Aviation Life Support Equipment (ALSE)
Due to the environmental conditions, the crew wore turtlenecks, long underwear, and immersion suit liners. Over this, they wore Mustang Gore-Tex immersion suits with rubber wrist and neck seals. They also wore flight boots, SPH-5 helmets and Nomex flying gloves with liners.
During the return flight to the ship, MHCP1 became aware of a hole in his immersion suit.
The aircraft was equipped with the Helicopter Emergency Egress Lighting System (HEELS). This is a battery-operated emergency lighting system that activates when the main rotor speed decreases below approximately 30 while the generators are still in the “ON” position. This system illuminates flexible light tubes above the upper personnel door, the left rear fuselage window, and the cargo door window. Both the TACCO and MHCP1 noted the HEELS to be functioning during their egress.
The MHC, the MHCP, the TACCO, and the AESOP were wearing PR2 SlimLine survival backpacks with EBS installed. These backpacks hold single man life rafts, emergency kits and radios. MHCP1 had a backpack available in the crew compartment but was not wearing it. All the crewmembers were wearing and had utilized their LPSVs upon egress from the aircraft. Of the five LPSV’s, three were reported as partial inflations, one was reported as a poor inflation, and only one was reported as adequate. One of the crewmembers who experienced a partial inflation was found floating facedown on the surface. After he was located and rolled over by another crewmember, he promptly revived on his own accord.
8/39

All five aircrew had extreme difficulty accessing and/or utilizing the items in the LPSVs. With a water temperature of 2 Celsius, the aircrew reported that their fingers were numb within two to three minutes, making the Velcro-sealed pockets extremely difficult or impossible to open. Consequently the aircrew were incapable of performing simple survival tasks. Only one aircrew member attempted to inflate his backpack’s liferaft; however, he reached to the backpack’s left shoulder strap for the activation lanyard instead of the right shoulder strap where the lanyard is located.
Although each LPSV housed an emergency strobe light in a front pocket, only two of the aircrew were able to access it. Due to a loss of manual dexterity from the exposure to the cold, the remaining three aircrew could not open the Velcro-sealed pockets. Those that were able to open the Velcro secured pockets found the strobe light operating switches taped in the “OFF” position and they were unable to remove the tape. A functional check was carried out post-accident and three of the five strobe lights were non-operable and showed signs of water ingress.
One aircrew member managed with some difficulty to get a Day/Night flare out of his LPSV. When he pulled the activation tab on the night flare, the tab pulled off of the flare without activating it. He then illuminated a chemical light-stick.
Although they are not considered ALSE, two of the aircrew utilized their “lip-lights” to signal the ship. These are small battery powered green lights installed on the helmet’s microphone boom.
All aircrew had reflective tape strips attached to the top and back of their helmets. Rescuers reported that these strips were effective in helping to spot the aircrew in the water.
The LPSVs also carried sea dye markers and whistles. None of the aircrew attempted to utilize these items.
1.15.3 Emergency Transmitters
The AN/URT 506 (V) Crash Position Indicator (CPI) was ejected on impact by activation of the frangible switch and functioned properly. It was later recovered by a boat from the ATHABASKAN. An aviation Emergency Locator Transmitter (ELT) is also carried on board. It is standard for the ELT to remain in the unarmed position until required as a backup to the CPI. The PR2 SlimLine backpacks also hold PRQ 501 emergency radios.
1.16 Test and Research Activities
The helicopter was recovered from the sea floor and transported by barge to Aarhus, Denmark. It was then moved to a hangar in the harbour where an in-depth analysis of all mechanical and flight control systems of the Sea King was conducted. Both aircraft and ship’s fuel and hydraulic samples were recovered
9/39

and sent to the Royal Danish Air Force Material Command laboratories for analysis. Fuel samples from the ship’s aviation fuel supply were analyzed and released from quarantine on 11 Feb 2006.
Divers from the ATHABASKAN recovered the IPVMS from the helicopter while it was still on the seabed. The tape remained in the recorder and was brought to the surface. It was then flushed with fresh water, packaged, and hand delivered to the National Research Council (NRC) Flight Data Recorder Playback Centre in Ottawa.
1.17 Organizational and Management Information
The occurrence aircraft and crew were from 12 Wing, 423 (MH) Squadron, Shearwater, NS. They embarked HMCS ATHABASKAN and were in the Baltic Sea in support of Standing NATO Maritime Group 1. The aircraft and crew were under Operational Control of CO HMCS ATHABASKAN. Operational Command, except for Flight Safety and Airworthiness, had been transferred from Comd 1 Cdn Air Div to Comd CEFCOM when the aircrew and aircraft embarked.
1.18 Additional Information- Aircraft Recovery
With the ATHABASKAN at anchor and the large salvage vessel “SAMSON” on site, a reconnaissance dive was conducted to determine the helicopter’s position in order to formulate a recovery plan. The helicopter was found to be inverted and partially resting on its left side, making a lift from normal hoisting point on the main rotor head impossible. The main rotor blades had been broken off or wrapped around the mast so were not a factor in the recovery process, making a lift from the right side high tie down points (rated for 18000 lbs each) the best option for recovery.
A second dive was carried out to secure loose equipment inside the cabin, attach lifting straps to the high tie down points and to ensure the area was clear prior to commencing the lift. The helicopter was lifted approximately 15 feet off the bottom, at which point hoisting was paused to ensure the high tie down points would hold the weight due to the uncertainty of damage sustained during the crash. After 15 minutes, lifting re-commenced and the helicopter was winched the rest of the way out of the water, at which time the barge was brought in and positioned under the helicopter. The helicopter was lowered to approximately five feet above the barge so a second lifting strap could be secured to the left side high tie down points to level the helicopter. It was then lowered onto the crash cradles and secured to the barge with chains.
Following the recovery a diver was sent down to survey the resting area for debris, but due to the poor visibility and strong currents, no wreckage debris was located. The barge was floated to a pier in Aarhus harbour where the helicopter was hoisted off the barge by a wheeled crane. It was then moved into a port
10/39

building for purposes of the investigation and afterwards to prepare the helicopter for shipment back to Canada.
At the time of accident, the aircraft was armed with sonobuoys, C2A1 smoke markers and electronic sound signalling devices (ESUS). When the aircraft was relocated to the building, three ESUS were found. Recovery workers reported that all of the remaining internal armament stores had been removed, and it was assumed the sonobouys and C2A1s had been lost in the ocean. Months later, when the aircraft was being prepared for use as a technical training aid, two C2A1’s were discovered in the internal stores chutes. The chutes where the C2A1s were found are labelled “ESUS”. Since the ESUS had been accounted for, it is suspected that this may be why these chutes were not confirmed as being empty. Regardless, this was a serious safety breach as the helicopter was shipped by sea container from Aarhus to Shearwater with C2A1s on board.
On 18 June 2006, a fisherman recovered large pieces of a main rotor blade near Varberg, Sweden, over 75 kms from the accident site. Pictures were relayed through the Royal Danish Air Force to the investigation team and the parts were verified as being from CH12438. Swedish authorities disposed of the blades locally.
1.19 Useful or Effective Investigation Techniques
The crew of HMCS ATHABASKAN conducted an extremely thorough and well documented evidence gathering exercise. This greatly enhanced the speed and efficiency of the investigating team in consolidating all the relevant facts concerning the accident. During the course of the investigation, all efforts were made by the ship’s crew to accommodate any requests for tools, space and equipment made by the Flight Safety Investigation Team. As well, the HELAIRDET technicians worked long hours to assist the investigation team’s acquisition of relevant mechanical data from the wreckage and to prepare the aircraft for return to Canada. The SNMG 1 staff photographer onboard the ATHABASKAN provided the investigation team with excellent photographic support.
An investigator from the Flight Safety Branch of the Royal Danish Air Force Tactical Air Command proved to be a valuable addition to the investigation team, providing excellent liaison service with the Royal Danish Navy, the Port Agent, and with the civilian salvage company that recovered the helicopter. Additionally, he provided a great deal of video and still imagery of the recovery effort.
Finally, the Royal Danish Navy generously provided the team with a number of invaluable services including office space, Information Technology support, tools and equipment, and disposal of both hazardous and explosive material.
11/39

2 ANALYSIS
2.1 The Accident
The helicopter was conducting a radar controlled approach and when it was at about 1.75 NM from the ship, the LSO asked the FLYCO to turn the flight deck lighting on to the “two mile” configuration. The two mile light configuration is utilized at night when the approaching aircraft is at two or more NM until it reaches one NM. In this configuration, the large Horizon Bars and Centre Line lights are on. The ship’s Strobe lights may also be used if required in poor weather. However, those latter lights were not utilized on the night of the accident. After the aircraft reported to be at one NM from the ship, the LSO asked the FLYCO to switch the flight deck lighting to the “one mile” configuration in order to provide adequate visual references to the pilots when they transitioned from the instrument approach to a visual approach. The FLYCO set the lighting levels to those normally used for night flying operations. In the “one mile” light configuration the Centre line and Strobe lights are turned off and the Hangar Face, Hangar Top and Dustpan lights (located around the perimeter of the flight deck), are turned on. Before reaching the RCA minimums of one half NM and 100 feet above sea level, the pilots were visual with the ATHABASKAN and anticipated clearance to proceed to land at the scheduled time of 1930Z. The helicopter continued to approach the ship, when at 0.6 NM on short-final, the SAC perceived internal communications between the LSO and the FLYCO indicating that the flight deck landing lights were not at the correct intensity settings. The SAC then directed the helicopter crew to commence an overshoot and to contact the LSO for control in order to allow time to confirm that the flight deck lighting was correctly set. The crew complied with the SAC’s direction and climbed to 200 feet while proceeding upwind to conduct a visual circuit and approach for landing. The LSO then cleared the aircraft to come across the flight deck in anticipation of a free deck landing.
The aircraft opened from the ATHABASKAN at 90 knots to one NM before turning downwind and the crew confirmed that pre-landing checks were complete. With the MHC still at the controls flying on instruments, the MHCP provided lateral spacing information to allow the MHC to turn onto final between one to two NM. The flight deck lighting remained at the “one mile” configuration. The MHC briefly looked up from the instruments and noted that the aircraft’s line- up with the ship was consistent with a normal approach profile. By about one NM, the aircraft commenced a descent to 100 feet and a deceleration to between 60 to 70 knots prior to reaching one-half NM. Once inside one-half NM, the MHCP then asked the MHC to descend further to 80 feet. The MHCP told the MHC initially that he was coming onto the controls, and then declared, “I have control,” soon followed by “back me up.” The MHCP later stated that at this point he thought the helicopter was high and fast. The MHC fully relinquished aircraft control to the MHCP and began to monitor the aircraft’s altitude and airspeed. As the aircraft continued to close the ship, the MHCP believed the hangar face lighting to be somewhat darker than ideal, and he considered having the MHC
12/39

radio the LSO. The MHCP began the transition to the hover. Then, as the aircraft’s height and airspeed rapidly decreased, the MHC told the MHCP that the aircraft’s altitude was descending through 30 feet, and then 20 feet before telling him to pull up; the LSO simultaneously radioed the aircraft to pull up as the aircraft descended below the flight deck and out of his field of view. The MHCP recalls as he pulled the stick back to slow down the MHC “shouted 20 feet, pull up, pull up!” He felt a solid “bump” and thought the aircraft had “bellied.”
When he called through 20 feet, the MHC came onto the controls and raised the collective in an effort to prevent contact with the sea surface. The other aircrew reported feeling a solid impact as the aircraft contacted the water. This is assessed as the helicopter’s rear fuselage and the tail rotor blades hitting the sea surface, causing damage that eliminated the anti-torque capability of the tail rotor, precluding yaw control. The aft end of the “boat-hull” fuselage, the area around the rear jacking point and the tail wheel, are also assessed as having hit the water. This area is of robust construction and did not incur significant damage. The helicopter quickly became airborne again, momentarily maintaining a level attitude as both pilots raised the collective. Then the aircraft began to yaw quickly to the right and the MHC lowered the collective and applied right cyclic allowing the aircraft to land on the water surface in a near-level attitude as it continued to yaw right to about 130º from the aircraft’s original approach heading, while simultaneously starting to roll left. The immediate action taken after the tail rotor strike is in accordance with Aircraft Operating Instructions (AOI) and prevented the yaw from increasing and a more violent, potentially catastrophic, impact with the water. The aircraft rolled over onto its left side and the main rotor blades then contacted the water’s surface. Two of the main rotor blades folded around the rotor head mast while the remaining three fractured and separated from the rotor system. There were a few MR blade strikes to the fuselage and tail pylon, which created some perforations to the airframe but did not cause any injuries. The crash sequence occurred about 30 meters from the flight deck on the ATHABASKAN’s port quarter.
Water quickly entered the aircraft cabin as the aircraft continued to roll to an inverted position floating on the surface (Photograph 1). The ATHABASKAN immediately came to Emergency Flying Stations and commenced a turn back to the crash site. As the aircrew surfaced, following their underwater emergency egress from the aircraft, they attempted to signal the ship using their strobe lights, helmet-mounted lip lights, a night flare, and a chemical light. Meanwhile, the ship’s searchlight was trained on them. The reflective tape on the aircrew helmets greatly assisted the searchlight operator in aiming the light. The ATHABASKAN’s rescue diver approached in a Zodiac and recovered all five crewmembers within nine minutes of the crash. A second Zodiac was launched and some of the crewmembers transferred to it in order to be hoisted aboard the ATHABASKAN by means of the torpedo loading cranes. By 1948Z all five aircrew were recovered onboard the ATHABASKAN where they were met by the ship’s surgeon and the medical team. At 2042Z the aircraft sank in 16 meters of water.
13/39

The actions taken by the ship’s company were prompt and effective in rescuing the aircrew and are to be commended.
2.2 Maritime Helicopter Approach Procedures
2.2.1 VFR Flight At Night.
The Shipborne Helicopter Operating Procedures (C-12-124-AOO/MB-002) (SHOPS) manual, which incorporates Fleet Operational Flight Procedures (FLOPS) as an annex, is a joint Maritime Command / 1 Canadian Air Division document. FLOPS, Chapter 3, Visual Flight Rules (VFR) at paragraph 306, states: “Night: The two authorized methods of VFR night recovery are an instrument approach and a visual approach. Because most night over-water flights require the pilot to fly primarily by reference to aircraft instruments, an instrument approach should be the preferred method even though visual meteorological conditions may exist. A visual approach may be conducted subject to the concurrence of the aircraft captain.” The accident aircrew initially flew an IFR approach to the ship, but the MHC opted to conduct a visual approach after the overshoot. A visual circuit is shorter than an instrument approach and would expedite their return to the ship in order to begin flight deck evolutions on schedule. This was permitted by the regulations and it is normal to incorporate several different procedures into a pilot training flight.
The minimum weather required for VFR flight in rotary-wing aircraft given in the B-GA-100-001/AA-000 (National Defence Flying Orders) for uncontrolled airspace is a flight visibility 1 mile (day), 3 miles (night) and the aircraft must remain clear of cloud. The VFR limits given in 1 Cdn Air Div Orders and FLOPS are a ceiling of 300 feet, flight visibility 2 miles with no differences for day or night operations.
The weather as recorded by the ship and detailed in section 1.7 gives the ceiling as being 700 feet with a prevailing visibility of 6 statue miles.
2.2.2 Pilot Monitored Approaches
The pilot monitored approach (PMA) procedure outlined in the Instrument Flying chapter in the Standard Manoeuvre Guide (C-12-124-A000/MB-001) (SMG) is for one pilot (called the Instrument Pilot) to fly the approach on instruments at specified altitudes, vectors and airspeeds while the other pilot (the Monitor Pilot) provides heading changes required to line the aircraft up with the desired flying course. The section is re-printed below:
“At minimums, if in visual contact with the runway environment and in a position to carry out a normal landing, the Monitor Pilot will take control and carry out the landing. The Instrument Pilot will remain on instruments throughout the approach.
14/39

Aircraft control shall initially be passed to the Instrument Pilot in sufficient time to permit the Monitor Pilot to complete the pre-landing check before reaching final approach. In addition to monitoring the approach, the Monitor Pilot will tune and monitor navigation aids and carry out communications as briefed by the Instrument Pilot.”
This procedure is further modified in the Night Operations chapter of the SMG as follows:
For recovery, the pilot shall carry out a standard approach for landing as described in FLOPs using the Pilot Monitored Approach (PMA). The shipborne PMA procedures are as follows: a. The PMA procedure shall be used during all night and instrument approaches to ships. Some changes to the basic PMA are necessary and are described in the following paragraphs. b. The approach briefing and the pre-landing check with the exception of the landing gear will be completed prior to arrival at the Final Approach Fix. (FAF). The helicopter will be flown at 200 feet at 90 knots. c. At the FAF, the Instrument Pilot will reduce speed to 70 knots and will descend to 100 feet by 1 NM from the ship. The Monitor Pilot will call 150 feet and 100 feet. Starting at 1 NM and before 0.5 NM, the Instrument Pilot will reduce speed to the higher of relative wind speed plus 30 knots or the safe single engine speed. d. The Monitor Pilot may take control at 0.5 NM, if fully oriented with the visual references on the ship. After passing control to the Monitor Pilot, the Instrument Pilot shall remain on instruments and call altitudes and airspeed respectively until the Monitor Pilot tells the Instrument Pilot to cease. e. At 0.5 NM if the Monitor Pilot does not have the ship visual, the Monitor Pilot will call “overshoot”. The Instrument Pilot will commence an immediate climb to 200 feet and turn to the missed approach heading. If there is no visible horizon, the pilot should concentrate on the lighted horizon bars in the final stages of the approach to avoid disorientation.
The investigation found that this is the procedure the aircrew utilized on the approach prior to the accident with no substantial deviations. As stated, this shipborne PMA procedure found in the SMG is to be used for all night approaches, regardless of actual weather conditions. It is to be used under instrument conditions as well as visual night conditions. On the accident flight,
15/39

the Monitor Pilot (MHCP) had the ship visual for the entire straight in portion of the approach. Therefore, there was no “visual” call at 0.5 NM, just a transfer of control when the Monitor Pilot was satisfied with the positioning of the aircraft relative to the ship. 100 feet is the Minimum Descent Altitude if the approach is being flown IMC. Having the Instrument Pilot fly lower than this altitude, as the MHCP did when he “stepped” the aircraft further down to 80 feet, is not addressed in any publications. It can not be assessed as an appropriate procedure as the CH124 SMG directs that “At minimums, if in visual contact with the runway environment and in a position to carry out a normal landing, the Monitor Pilot will take control and carry out the landing.” and in an other section the SMG provides some changes to the basic PMA and directs that “The Monitor Pilot may take control at 0.5 NM, if fully oriented with the visual references on the ship.” Other MH pilots were questioned on this action, and the consensus was that there is nothing wrong in having the instrument pilot descend further as it is a visual procedure. Other than the excerpts presented above from the SMG, which is a combined and general procedure for IFR and Night VFR recovery, there is no detailed direction on how to fly a pilot monitored approach for either visual or IMC approaches. As well, there is no night visual approach currency requirement in 1 Canadian Air Division orders.
The SMG states that “the pilot shall carry out a standard approach for landing as described in FLOPS.” However, FLOPS only vaguely describe approaches, giving airspeeds and altitudes, but no direction or techniques, and there is no mention of PMAs. FLOPS also reference MAGORDs, a set of documents retired prior to 2000.
2.3 Inadvertent Descent
The final approach segment is a difficult phase of flight as the pilots make the transition from instruments to outside visual references. The workload on the pilot is increased, as the pilot has to slow the aircraft, add power to enter the hover and anticipate the control inputs required to counter-act pitch and yaw forces. In the case of the PMA, the MHCP had been looking outside of the aircraft for visual cues in order to verbally direct the MHC to position the aircraft. There was no perceptible horizon, and the only light sources in the area came from the ship. The MHCP’s attention had been focused on the ship and his statements indicate he perceived the hangar face lighting to be less than ideal as the distance closed. Already dealing with a high workload, this may have served as a momentary distraction. The MHCP stated that when he took control he thought he was high and fast, so his corrective action was to pull on the cyclic to flare the aircraft and begin to transition to the hover. This is an ingrained action for helicopter pilots, but without any horizon he would have had to look at the attitude indicator to determine how far up the nose of the aircraft had risen. Since he had previously been focusing his attention outside the aircraft, he may have omitted a crosscheck of the flight instruments at a crucial time. It is assessed that the flying pilot lost situational awareness and did not perceive the rapidly increasing nose-up pitch attitude, which in turn, in the absence of a rapid
16/39

power increase, generated a high rate of descent. In the section on Water Operations, the CH124 AOI (page 3-20-1) includes the caution “Nose up attitudes in excess of 5 degrees below 10 feet may result in tail rotor damage from contact with the water.” The distance from the pilot’s position in the cockpit to the tail rotor is approximately 50 feet. With 15 degrees nose up, as the investigation revealed, the tail rotor would strike the water with an instrument altitude reading well above 10 feet. (Figure 1) The pilot’s objective was to enter a 60 foot hover in a position 30 yards abeam the ship, which would equate to about 30 feet above the ship’s flight deck. However, as the nose came up the helicopter descended out of 80 feet rapidly. The MHC stated he called out altitude warnings starting at 40 feet, and the Radar Altitude Warning System would have emitted a warning at 30 +/- 5 feet. The MHC did not take action quickly enough to either verbally warn the MHCP or physically take over control of the helicopter when the aircraft began its rapid descent. The LSO also transmitted “Pull-Up” on the radio, but the pilots were unable to halt the descent prior to contacting the water.
2.4 Physiological Effects
2.4.1 Visual Illusions
An illusion is an erroneous perception of reality due to limitations of sensory receptors or the manner in which information is presented or interpreted. Vision, supported by the other senses, allows a pilot to maintain orientation. At night or during periods of reduced visibility, the supporting senses can conflict with what is actually seen. This situation can leave a pilot vulnerable to spatial disorientation. Spatial disorientation is defined as the failure to achieve accurate orientation with respect to the earth’s surface. In this case it could refer to separation from the sea surface as well. The following excerpt obtained from the USAF Instrument Flight Center describes the first of three types of spatial disorientation:
Type 1. This is unrecognized spatial disorientation; the pilot is unaware that anything is wrong and controls the aircraft in accordance with, and in response to, false sensations of attitude and motion. This involves a strong anomaly of attention, which dominates the pilot’s conscious mind for some length of time. Although this time internally may not seem excessive to the pilot, it may be longer than he thinks: the phenomenon of temporal distortion. It has been demonstrated that a pilot’s eyes can be away from his instrument cross-check 15 to 90 seconds while he is busy attending to another task. At night or in weather, distractions for this amount of time may have fatal results, especially at low altitudes. If the pilot does not experience some sensory input that the aircraft has entered an unusual or dangerous attitude, he may assume subconsciously that things are all right. This is the most common type of spatial disorientation involved in aircraft mishaps.
17/39

It is plausible that as the MHCP took over control of the aircraft, this physiological influence may have affected his behaviour.
The “black-hole approach” is another documented illusion, which occurs when darkness, absence of visual cues and few lights distort the pilot’s perception of altitude, attitude or both. When an aircraft is on approach to a runway and all is dark below the approach path with only the distant runway, or ship’s lighting providing visual stimulus, an illusory or false sense of height and/or altitude may be perceived. Flying over unlighted terrain or water with no horizon, the runway environment (or in this case the ship) is not sufficient for determining where the actual horizon would be. Deprived of peripheral visual cues to provide spatial orientation, the pilot may feel steady, but perceives the runway to move or be out of position. The pilot interprets the horizontal plane of the landing surface incorrectly and overestimates the altitude, which may lead to flying a shallower than desired approach. This arcing below the desired flight path may lead to landing short of the intended touchdown site.
Although the preconditions for this phenomenon were present, it is unlikely it affected the approach flown. The MHC stated that he had checked the MHCP’s sight picture prior to relinquishing control and felt no cause for alarm, meaning he perceived that the aircraft was correctly positioned in relation to the ship. 2.4.2 Vestibular Illusions
There are four systems in the human body, which provide information for determining orientation. They are the visual, auditory, somatosensory (muscle preceptors) and the vestibular system. The vestibular system is the non-auditory portion of inner ear that senses motion and gravity. The main sensory organs involved are the semicircular ducts and the two otolith organs. The semicircular ducts contain sensory hair cells which measure angular motion by the amount of displacement of the hair caused by the flow of fluid in the ducts. Similarly, the otolith organs are affected by straight line or linear forces and gravity.
The complex motions induced by flight can generate inaccurate responses in the vestibular system. With a lack of visual references, the human mind will revert back to this potentially erroneous information. Illusions created by the vestibular system are subdivided into those caused by the semicircular canals and those caused by the otoliths.
One of the three types of illusion caused by the otolith organs is the “Illusion of Pitch Attitude Change.” This phenomenon may occur when an aircraft accelerates or decelerates quickly. Inertia from linear acceleration causes the otolith organs to sense a nose high attitude during acceleration and a nose low attitude during deceleration. When a nose-low attitude is perceived during decreasing velocity, there is a tendency to pull the nose up. Usually this illusion does not occur if adequate outside visual references are available.
18/39
The MHCP did not have the benefit of any visual aids other than the ship’s lighting. After sensing that he was high and fast, the MHCP attempted to promptly reduce the perceived excess airspeed. Raising the aircraft nose and the accompanying deceleration may have induced this illusion of pitch attitude change generating a sense of being nose-low, or under-interpreting the degree to which the nose had risen. This is further supported by the MHCP’s comments that he thought the aircraft had initially “bellied”, vice striking the tail, indicating he had sensed the aircraft at a near level attitude. This nose high attitude moved the lift vector of the main rotor disc rearwards, permitting the helicopter to further decelerate and increase its rate of descent.
2.4.3 Mitigation Of Physiological Effects
The main defences against disorientation and the perception effects discussed above are awareness and training. CF student aircrew undergo training at the Canadian Forces School of Survival and Aerospace Training (CFSSAT). The course is intended to educate students regarding the existence of these phenomena and their effects. The aim is to create awareness and anticipation of these effects to help aircrew deal with their onset when they are exposed later in their careers.
The other aspect is the training and overall experience which influences a pilot’s capabilities. The recency of the training is extremely important. An instrument cross-check is another tool to lessen physiological effects. A good instrument cross-check is a skill that can erode over time. Pilots with little instrument time are particularly susceptible to disorientation. However, as stated in the Canadian Forces Manual of Instrument Flying, “Total flying time does not protect an experienced pilot from spatial disorientation. More important is currency and recency of experience.”
2.5 Aircrew Currency Requirements
2.5.1 Orders
The MH orders regulating aircrew currency requirements are defined in the B-GA-100 (National Defence Flying Orders), the 1 Cdn Air Div Orders, 12 Wing Orders, and the Unit Flying Orders. The 1 Cdn Air Div Orders Vol 5, 5-504 states the specific currency requirements required for MH pilots to maintain currency. The orders state the restrictions imposed if an item becomes expired, and they also state what the pilot must do in order to rectify the deficiency. For most lapsed items, in order to resume normal flying duties, the pilot must conduct a Dedicated Proficiency Flight (DPF). When a DPF is required, it shall be flown with a current MHC. As a minimum, the DPF shall include all currency sequences in which the pilot is deficient. A DPF may be conducted in conjunction with another flight, provided adequate time is allocated to rectify the currency deficiencies. A DPF may be conducted for two consecutive months. If a pilot is deficient for a third consecutive month, the pilot will be restricted from
19/39
flying duties and will require a Supervised Training Flight (STF). A STF shall be flown with a Standards Check Pilot, Flying Training Officer, or MH Flight Instructor. As a minimum the STF shall include all deficient currency sequences and an evaluation of overall proficiency shall be conducted.
2.5.2 Maritime Helicopter Captain (MHC) Currency
On the day of the accident, the MHC was current in accordance with the Flying Currency requirements stated in the 1 Cdn Air Div Orders. The occurrence MHC’s role on the ATHABASKAN HELAIRDET was to fulfill the duties of Aircraft Captain and Crew Commander of one of the two crews. As Aircraft Captain, the pilot is responsible for all decisions regarding the safety of flight as well as monitoring and ensuring the progress of the crew. As a Crew Commander, the pilot is also responsible for all tactical decisions regarding the mission; as well he is responsible for supervising the TACCO and the AESOP.
The MHC was recently posted from 12 Wing Helicopter Operational Test and Evaluation Facility (HOTEF) to 423 Sqn in September 2005. As a member of HOTEF, the pilot was not required to deploy to HMC Ships, nor was he expected to maintain any currency with respect to destroyer deck landings (DDLs), approaches to ships, or landing signals officer (LSO). In September 2005, he was attach-posted to HMCS ATHABASKAN and he embarked the ship as a co-pilot for two weeks to obtain his DDL and LSO qualifications. He also completed one week of Work-ups training on the ship in Jan 2006. (A Work-up is a voyage or cruise in which various trials and exercises are held in order to bring the crew and ship’s systems to the required operational readiness level.) Prior to these short sailings, the MHC’s last deployment on a ship was in 1990, 16 years earlier. In Jan 2006, with only three weeks of recent ship borne experience, he embarked as both the Aircraft Captain and the Crew Commander of his crew.
During the previous six months, the MHC flew a total of 35 missions and he was the Aircraft Captain on nine of those trips. The nine trips where he was the Aircraft Captain were flown within the 90 days previous to the accident. The MHC flew six out of the seven missions as Aircraft Captain during the 30 days prior to the accident, as he was now the designated MHC and MHCC for his crew on the air detachment. Even though this MHC is a highly experienced Sea King pilot, three-quarters of his missions during the last six months ashore were flown as a co-pilot. Again, this was the first time in 16 years that the pilot was flying as an MHC or MHCC while deployed at sea.
Analysis of the MHC’s 2005 flying hour summary reveals that the 1Cdn Air Div monthly requirements (10 hrs total, 1 hr night, 1 hr low level over-water (LLOW)) were met in only two months during that year (March and June).
In the four months prior to the accident, the MHC did not meet the 1 Cdn Air Div requirements for minimum night flying hours (1 hr/month or 3 hr/3 months) in three out of the four months.
20/39

The MHC was current in night flying on the day of the accident; he had 2.7 night hrs in the last month and had 3.4 hrs in the last 3 months, which satisfies the requirements of the orders. However, further analysis reveals that the MHC had only 4.7 hrs night in the last six months and only 10.9 hrs night in the previous 12 months. In the previous year, the pilot had been restricted from night flying as an Aircraft Captain on four different occasions. Six days prior to embarking the ATHABASKAN, the MHC flew a night DPF that included 2.0 hrs of night. Prior to this DPF mission, the pilot had flown only 0.8 hrs night in the previous three months. The DPF mission rendered the pilot “current” to fly as an aircraft captain when he embarked as an MHCC on 11 January, however the low number of night flying hours the pilot flew in the previous year brings into question his proficiency to operate over-water and carry out approaches to ships in night time conditions.
LLOW is considered to be any over-water flight at or below 500 ft in actual or simulated IFR conditions. The 1 Cdn Air Div Orders state that pilots must fly 1 hr LLOW/month or 3 hr LLOW/3 months. The MHC did not meet the minimum 1 Cdn Air Div requirements for LLOW on two occasions during the previous year.
2.5.3 Co-pilot (MHCP) Currency
The MHCP was a qualified Aircraft Captain who had recently embarked with the HELAIRDET to fly as a co-pilot. He had upgraded to MHC in January 2005 and flew missions as the MHC on numerous occasions. The MHCP embarked on the ship two weeks after the remainder of the HELAIRDET personnel. He joined the ship in Germany, and his first flight from the ship was flown on 31 January, two days prior to the accident. Upon joining the ship, he was expired for DDLs, LSO qualifications, and night hours. The occurrence mission was being flown as a DPF.
Analysis of the MHCP’s 2005 flying hour summary reveals that the 1Cdn Air Div monthly requirements (10 hrs total, 1 hr night, 1 hr LLOW) were met in only one month during that year (May). In the month previous to the accident, the MHCP did not meet the requirements for total flying hours (10 hr/month or 30 hr/3 month) or the minimum night flying hours (1 hr/month or 3 hr/3 months). He rectified the total hour deficiency, however he did not rectify his night hour deficiency prior to embarking. He flew 1.6 hrs of LLOW during the previous 30 days and 3.0 hrs during the previous 90 days satisfying the currency requirements of the 1 Cdn Air Div Orders.
During the three months prior to embarking, the co-pilot flew only 10 missions, accumulating 17.4 day hrs and 2.1 night hrs. This is well below the minimum requirements. (10 hrs/month or 30 hrs 3/months total, 1 hr/month or 3 hrs/3 months night). The pilot was unable to rectify his night hour deficiency prior to embarking, however the accident flight was intended to have rectified his night hour deficiency.
21/39

The MHCP last conducted night DDLs on 31 Aug 05 and had expired for night DDLs on 31 Dec 05. If a period of four months elapses since a pilot last conducted a night deck landing, the pilot’s night DL qualification is expired. In order to re-qualify, the pilot must complete six night landings under the supervision of a current night DL qualified pilot. One of the purposes of the accident flight was to re-qualify the pilot on this deficiency. It can be assumed that because the co-pilot has not completed night DDLs in the previous five months, he had also not flown any night approaches to a ship. There is no currency requirement for night or instrument approaches to ships. Despite his 683 Sea King hours, the MHCP stated he could not remember the last time, if ever, that he had flown a night visual approach to a ship. This is a very challenging manoeuvre requiring significant concentration by the pilot and supervision by the non-flying pilot.
2.5.4 Force Generation Process
Force Generation (FG) is the process of organizing, training and equipping forces for force employment. The “Maritime Helicopter Combat Training Directive” (CTD) is a 1 Cdn Air Div document, the aim of which is to describe how MH Combat Readiness is to be developed, maintained and reported. The CTD outlines the relationship between the Air Division, MARLANT, MARPAC and 12 Wing concerning 12 Wing’s response to operational tasking, commitments and sustainment status. The Commander 12 Wing is responsible to the Commander 1 Cdn Air Div for the generation of HELAIRDETS. In turn, the Squadron Commanding Officers are responsible to the Comd 12 Wing for the force generation of helicopters, aircrew and maintenance personnel to support the operational HELAIRDETS commitments. The CTD delineates the various levels of Combat Readiness, the resource requirements and the currency requirements to achieve the levels.
The FSI team attempted to determine the reason why the pilots were not able to meet the monthly flying requirements on a regular basis and why the pilots did not embark the ship with at least the minimum currency requirements. It was assessed that there are significant systemic training deficiencies throughout the MH community as a result of reduced flying rates. The main impediment to crew training has been the non-availability of serviceable aircraft. This is due to a number of factors, perhaps the greatest of which is the low level of experience amongst the CH124 maintenance technicians. This situation could be traced back to previous years when recruiting levels were at zero or near zero levels. Further aggravating the challenge of providing serviceable aircraft is the age of the fleet. Increased age has led to more extensive corrosion that necessitates more frequent and more comprehensive repairs. The age of the aircraft also makes it more difficult to establish contracts for the manufacturer and supply of replacement parts.
The difficulty in providing serviceable aircraft for FG missions has been recognized by the chain of command for some time. Numerous programs have
22/39

been investigated and implemented to mitigate the effects of reduced flying rates. Despite the best efforts expended, there is only so much return available within the systemic constraints facing the Sea King fleet. In October of 2006, a Flight Safety survey of 12 Wing indicated that most aircrew felt proficiency was a significant concern when not deployed to sea. This concern was evident by the fact that most aircrew are averaging only ten hours per month. See Figure 2.
Compounding 12 Wing’s FG challenge is the reduced availability of HMC Ships to provide training evolutions. Reduced sailing rates and long-term operational commitments (Op Apollo, Op Altair) have resulted in a decrease in opportunities to practice DDLs and night operations.
Because of the lack of resources available to MH aircrew for maintaining currency, it has become the norm in the MH community to provide DPF flights to aircrew. While useful for ensuring that the pilot who occasionally does not achieve his or her minimum hours is still considered safe to fly, the aim of DPF flights is not to provide adequate practice over the long term, or to ensure pilots remain proficient on such things as sight pictures over a ship on a dark night. However, these flights are now considered a normal procedure. The shortage of serviceable aircraft assets and the resultant currency deficiencies have resulted in the generation of a monthly “pumpkin list” of pilots who have not achieved their minimum hours and have been removed from active flying status. These pilots then require a DPF flight to “re-set” their currency. During January of 2006, less than one- third of the pilots at 12 Wing were fully current. Although the CTD defines HELAIRDET proficiency, it contains no requirement for aircrew to be current before deploying.
Data from the 12 Wing Flying Schedule shows that in the four months previous to the accident, the MHC flew 20 out of the 32 scheduled missions, (63%). This does not include the scheduling statistics from the flying program while embarked. On seven occasions the cause of a mission not being flown was given as aircraft serviceability, and five times the reason was cited as “OPS,” meaning the Wing Operations Cell had cancelled the flight.
The MHCP flew 16 out of the 23 scheduled missions (70%) during the 4 months prior to the accident. Four of these missions were called off by Operations, three were not flown due to aircraft serviceability, and bad weather precluded the final two.
Both pilots flew approximately 65% of their scheduled missions. The remaining 35% of the missions were cancelled due to scheduling conflicts, aircraft unserviceabilities, or weather. This success rate with CH124 scheduling is considered normal within the Sea King community.
The Sea King Operational Flight Tactical Trainer (OFTT) is an older technology flight simulator with motion. In accordance with Transport Canada definitions, it is a “Flight Training Device”. It does not have a visual system and the cockpit
23/39

windows are opaque glass so all evolutions are done on instruments. As such, it does not provide the fidelity or realism that would be required to offset actual training flights. Some fleets have modern, high fidelity simulators that provide a near replication of actual flight experiences to such a degree that check rides can be performed in the simulator. Although the OFTT can provide valuable training, it cannot replace FG hours flown on the aircraft.
2.5.5 Pilot’s Aircrew Proficiency Conclusions
The Oxford dictionary defines proficiency as: “Skillfulness in the command of fundamentals deriving from practice and familiarity, synonyms: technique.” An occurrence involving a performance discrepancy in proficiency can therefore be related to skill retention, which is a capability one would expect to correlate well with opportunity to practice, i.e.: flying hour availability.
John Patrick1 is cited in several aviation investigation reports in view of his work on task/skill analysis and skill retention. He states that skill retention degrades with time following training and the amount of degradation is related to the following:
a) The level of retention is positively related to the level of learning at the end of the training;
b) The skill retention gets worse, the longer the retention interval: and
c) The rehearsal of skill mitigates against skill loss.
A Canadian Transportation Safety Board report2 captures well the conundrum of skill retention: “In essence, skills can be expected to be most effectively maintained when they are well mastered during training, retrained on a regular basis, and rehearsed regularly between training sessions. This cycle of retraining is most critical for procedural tasks, which consist of a number of discrete steps (for example, responding to an in-flight emergency such as an engine failure), since these types of tasks have been shown to degrade the most over time. Conversely, continuous tasks, which are more automatic and for which cues are provided by the environment (for example, manually flying an aircraft on a visual approach), show minimal degradation over time.”
Regular and repeated practice is required to maintain proficiency. Maintaining minimum currency may be acceptable for a short time but, if allowed to persist and become the norm, proficiency will degrade. The actual amount of degradation will depend somewhat on an individual’s experience and personal abilities.
1 Training: Research and Practice, J. Patrick, May 12, 1992 ISBN-10: 0125466609 2 Transportation Safety Board of Canada (TSB) report number A05O0147, released on 22 February 2006.
24/39

This particular front-end crew was comprised of an experienced MHC and MHCC as the aircraft captain and an experienced co-pilot. Analysis of the previous flying hour statistics of both crewmembers indicate that although they legally met the minimum currency requirements, both pilots were at or below minimum proficiency levels required for ship borne operations. The aircraft captain had just recently been posted to the operational unit from HOTEF, and it had been 16 years since he had embarked as part of a HELAIRDET. He had only three weeks of sea time to prepare himself for the responsibilities of both an aircraft captain and crew commander of a Sea King crew while at sea. His co-pilot was an experienced Sea King pilot who could relieve significant workload and pressure from the MHC; however, it had also been a long period of time since this co-pilot had operated from a ship. The co-pilot had expired for DDL requirements, LSO requirements, total hours and night hours upon embarking the ship. This front-end crew had flown only two trips together during this deployment prior to the accident flight: a test flight and a day DPF. Although legally current by virtue of this DPF, the MHCP reported that his last night deck landing was to the ATHABASKAN on 31 Aug 2005. Thus, the MHCP’s proficiency at night deck landings can be assessed as weak.
12 Wing has been having difficulty in recent years ensuring its pilots receive the minimum number of day and night hours required to remain current. This has been due to the decrease in Force Generation flying rates caused by the difficulties in providing serviceable aircraft at 12 Wing. This situation has been deleterious for Sea King pilot proficiency in general.
2.6 IPVMS Analysis
The aircraft was equipped with an Instrument Panel Video Monitoring System (IPVMS) that records images from four separate cameras, three focused on the instrument panels and one providing a generic overview of the aircraft cockpit. The images are recorded on a commercial-grade VHS recorder. The IPVMS, which has no audio function, was introduced to the CH124 in 2003 in order to capture data for analysis of the “Sudden Uncommanded Transient Loss of Torque” phenomenon that affected the fleet at that time. The IPVMS is not designed to be crash survivable.
Divers recovered the IPVMS tape while the helicopter was still on the sea floor. It was packaged appropriately and sent by courier to the National Research Council’s Flight Recorder Playback Centre located in Ottawa. (NRC)
The tape had been soaked in seawater overnight, and the final few frames of the recording, approximately three seconds worth, became bonded to the recording device. NRC was able to provide imagery of the final moments of the flight up to this un-recoverable section. The tape is black and white, grainy, and is of the quality that can be expected from a night recording on a helicopter flight deck.
25/39

Although difficult to read, the “triple tach” (tachometer), showing rotor speed and the freewheeling turbine speeds for engines one and two, is in view. Also visible are the Ng1 and Ng2 gauges, depicting the gas producing turbine speeds, and the torque indicators for both engines. The engine temperatures are also shown, and a portion of the attitude indicator is visible. Camera #4, which should capture an overview of the cockpit area, was partially out of alignment and mostly aimed at the back of the MHC’s helmet (left seat.) It does capture a portion of the MHC’s body, occasionally the left hand of the MHCP (right seat pilot), a portion of the centre console, and the lower and central portion of the main instrument panel but without sufficient resolution to precisely read instruments. No altitude information is available on the recording.
Analysis of the last five minutes of the tape corroborates statements made by the aircrew. There is no indication of any mechanical problems leading to the accident; all engine and Main Gearbox (MGB) instrument indications are consistent with normal operations.
The last 14-second time frame is assessed as when the MHC relinquished control to the MHCP. Shortly after this the attitude indicator shows the nose of the helicopter rising to more than 15° above the horizon. At the same time, the engine gauges indicate a power application; of which the exact magnitude is not discernible. It is not known if this was the normal increase in power required to enter the hover or if this was part of the attempted recovery. Five seconds before the end of the recording, the MHC rocks sideways in his harness and the images become more blurred indicating the time when the tail rotor contacted the water.
The #4 camera mount is susceptible to being bumped by aircrew as they enter or leave the cockpit. There are tools available and procedures in place for technicians to verify the alignment of the cameras before flight. However, even if this verification is conducted, there is no guarantee the cameras will remain aligned after the aircrew have strapped in.
NRC Flight Data Recorder Playback Centre (FDRPC) has indicated that a voice recording capability on the CH124 IPVMS would have provided very valuable information. If this had been in place, significant Human Factors information would have been available to the FS Investigation team such as; sequence of events, change of pilot in command, reaction of the crew, and crew communication. Aircraft noises can also provide valuable information. Additionally, it is easier to recover audio data files from a damaged VHS tape than video images.
26/39

2.7 Analysis of Aviation Life Support Equipment
Defence Research and Development Canada (DRDC) Toronto provided technical expertise for the analysis of the ALSE. Some of the equipment was hand carried back to Toronto by the DRDC member of the field investigation. The remainder was shipped at the end of the field investigation in February 2006 and did not reach DRDC until 20 July 2006. All recovered ALSE and flight clothing was contaminated from exposure to the salt water and Petroleum Oil and Lubricants. The CO2 cylinders were removed from both the LPSVs and the liferafts before shipping.
All flares from the LPSVs and survival kits were left with the ship’s ALSE technician for disposal. The CF363- Aircraft Support Equipment Record Sets (Log Books) did not arrive at DRDC Toronto until the end of Jul 2006. With the exceptions noted throughout this section, the logbook entries were accurate and up to date. No ALSE was found to have expired inspection dates.
2.7.1. Immersion Suits
The immersion suits were all worn over long underwear, turtle neck shirts and immersion suit liners. All the immersion suits had the mitts, hood and survival knife attached. The immersion suits were in good condition except one had a 3/8” hole on the back of the upper right leg. This suit was worn by MHCP1 and he had noticed the hole after moving to the cargo compartment, prior to the accident. It was his intent to don a spare suit when the crew commenced DDLs. The investigation revealed a protruding fastener with a broken vinyl retainer on the front horizontal tube of the 3-man troop seat that likely caused this hole. (Photograph 7) This hole later allowed a small amount of water to enter the suit.
2.7.2 Helmets
Four of the crew wore SPH-5CF helmets fitted with padded chinstraps. These had numerous scrapes and scratches but were in generally good condition with the exception of one that had a deep scratch, approximately 2” long on top of the shell. The shell did not appear to be cracked. The remaining aircrew wore a HGU-56P helmet with padded chinstrap that was specially fitted by DRDC in Dec 03. There was a crack, approximately 2.5” long, along the back of the left ear cup of the shell. This crack may have happened post crash during recovery, handling or shipping. (Photograph 8)
The helmets had strips of highly reflective tape that aided the ATHABASKAN’s crew in locating the survivors in the water with searchlights. Surprisingly, the aircrew reported their lip lights still functioned after being submerged in salt water and they used these small LED lights to signal rescuers.
27/39

2.7.3 LPSVs
The overall condition of the LPSVs was good, and all the CO2 cylinders and gaskets appear to have been properly installed. When inflated after egress, four of the vests failed to evenly inflate due to restrictions caused by the failure of the collar zipper to completely separate. The failures occurred on different sides of the individual vests and were reported as “partial inflations” by the crew. This failure mode has the potential of having very serious consequences. Quality Engineering Test Establishment (QETE) was tasked to investigate the inflation times of the LPSVs at cold temperature and to recommend possible alternate configurations. Based upon QETE findings, the TAA issued a modification to all Helicopter and Transport aircraft LPSVs. These modifications are to provide a complete bladder deployment on inflation.
Analysis also revealed that modification C-22-521-000/CF-016, “Installation of Exterior Pocket Closure Flap Extension”, dated 25-02-11, was not carried out on any of the LPSVs. This fact, along with the cold, wet hands of the crew in the water, made it almost impossible for them to open vest pockets and access survival items.
2.7.4 SlimLine Backpack and EBS
There were five SlimLine backpacks on board the helicopter. Each backpack assembly included a one-man liferaft; an emergency breathing system (EBS); an AN/PRQ-501 beacon radio set; and emergency survival items; all packed in the backpack container. None of the SlimLine backpack liferafts were deployed in the accident, although one crewmember tried to activate his raft but failed to find the lanyard. He recalled later that he had reached to the backpack’s left shoulder strap for the activation lanyard instead of the right shoulder strap where the lanyard is located. Four of the liferafts were later tested and found to be serviceable.
One SlimLine backpack was left in the rear compartment of the helicopter and the AESOP’s was left at his station. The SlimLine backpacks are not individually issued but are installed on the helicopter. The backpacks are serial numbered locally, but there is no annotation in the logbooks indicating their position in the helicopter. The letter designation in the serial number is A,B,C, & D. The backpacks are normally installed in the following manner; A-pilot, B-co-pilot, C-TACCO and D-AESOP but this is not always the case. A spare backpack is installed when required. The logbooks for the EBS do not identify their location. The logbooks for the backpacks had the wrong NATO Stock Number entered on the Data Record sheet.
28/39

1 Cdn Air Div Orders Vol 2, 2-007state;
37. Rotary Wing Aircraft. Crewmember LPSV should be equipped with Emergency Breathing System (EBS) as dictated by mission requirements.
52. Maritime Helicopter. Backpack dinghies shall be available in the aircraft for all crewmembers (including, but not limited to, Standards personnel, OTU Instructors, fifth crewman for Helicopter Towed Array System (HELTAS)/SAR, etc) when flying overwater. The backpack shall be worn whenever the crewmembers are seated at their station while flying overwater.
MHCP1 seated in the troop seat in the rear of the helicopter was not wearing a SlimLine backpack. There was one available to him hanging on the sidewall. The above order may have been interpreted that the backpack did not have to be worn depending on how “their station” is construed. However, without the backpack this crewmember did not have ready access to an EBS bottle.
2.7.5 Flying Gloves
The gloves and liners are provided primarily for flash fire protection, while retaining dexterity and control feel. The liners are made of Nomex while the flying gloves are of Nomex and leather. Their construction is neither warm nor robust enough for outside winter wear. They are not waterproof, and offer no thermal protection when wet. Because the sea surface temperature was 2° Celsius, the crew lost the dexterity of their fingers very rapidly. The immersion suits carry mitts in an external pocket, but none of the survivors accessed them. All crew members reported difficulty conducting basic manual tasks.
2.7.6 Strobe Lights
The crewmembers had problems trying to activate the strobe lights because of unauthorized tape installed to prevent the switch from being inadvertently turned on. One strobe light switch was in the ON position when inspected approximately 48 hours after the crash. It did not work until new batteries were installed. Only two of the strobes worked at that time.
The MS-2000(M) version of the strobe light is designed to operate in water as deep as 15 meters. Three of the strobes involved in this accident leaked even though the depth of submersion was approximately three meters. Some had indications of moisture in the battery compartment and one had moisture in the lens compartment. The three units also leaked in two feet of water in lab testing at DRDC Toronto. The CFTO for the Distress Light Marker does not specify any inspection of the battery compartment O-ring for condition or deterioration. The strobe lights were issued to individuals and carried in their LPSVs; the serial numbers of the strobe lights were not recorded in logbooks for tracking
29/39

ownership or location. The strobe light battery changes were recorded in the LPSV logbooks. The four strobe lights were sent to QETE in Dec 2006 for further analysis. Although the final report has not been concluded, it appears pinched or deteriorated O-rings permitted water to enter the cases.
2.7.7 Emergency Escape Handles and HEELS
MHCP1 and the TACCO noted the HEELS to be functioning during their escape from the darkened aircraft. (The MHCP1 at the cargo door, and the TACCO at the personnel door.) However, both pilots in the cockpit encountered difficulty locating the window emergency release handles. The MHC located the handle on his third attempt after utilizing his EBS, while the MHCP never did find his. When the pilots are seated normally at the controls, the handles are adjacent to their outboard hand and would appear to be readily utilized. But being upside down, in complete darkness, deprived of gravitational references and dealing with changing buoyancy forces acting on their bodies, generated changes in pilots’ positions relative to the seats and made locating the unlighted handles problematic.
2.7.8 Flares/Chemical Light Sticks
One crewman was able to remove a flare from his LPSV, but it did not operate when he pulled the firing ring. It is not known if the flare failed due to a defect, or improper operation by the user. He then activated a chemical light stick, which he had elected to keep in his LPSV. Chemical light sticks are not part of the required contents of the LPSV. Chemical light sticks (glow sticks) are far less bright than pyrotechnic flares, and do not have a day capability. But they are also extremely easy to operate and even small ones provide light for hours. Ship’s personnel carry them attached to their outer garments when they work out of cover. The Navy uses a holder that allows the sticks to be activated using one hand.
2.7.9 Rotary Wing Under Water Escape Training (RUET)
To remain current, MH aircrew must undergo egress and ditching drills, dinghy drills, as well as RUET. Egress and ditching drills are to be conducted annually and include at least one ditching scenario. The drills are supervised by qualified personnel who instruct on the proper procedures and use of emergency equipment. Dinghy drills are conducted annually in a swimming pool or other suitable body of water and include survival swimming and the proper use of survival equipment.
RUET and EBS training shall be conducted in accordance with 1 Cdn Air Div orders and is valid for a period of five years. Current RUET/EBS training is required for all dedicated overwater flights. A civilian company under contract with DND provides this training, near 12 Wing Shearwater. The accident aircrew
30/39

had met all the currency requirements for dinghy, egress, and ditching drills, as well as their ALSE review and RUET.
Analysis has shown that most fatalities caused by drowning following aircraft ditching are due to:
-Disorientation;
-Unfamiliarity with escape handles/hatches;
-Premature un-strapping prior to settling of the aircraft;
-Head injury caused by improper use of helmet (unfastened or poorly fitted); and
-Non-availability of personal floatation devices.
RUET provides a controlled atmosphere in which to expose aircrew to the first three of these survival threats. As a result of this training, aircrew are more cognizant of the challenges they face in extracting themselves from a submerged aircraft.
Although the crew in this situation were able to egress from the aircraft following the accident, all five reported escape actions that diverged by some degree from established, and taught, egress procedures. One of the crewmembers accidentally unfastened his backpack while intending to undo his lap belt. Two aircrew undid their lap belts before the aircraft’s motion ceased. Both pilots and the TACCO had difficulty locating and utilizing escape hatch handles. One of the crew could not locate the activation lanyard for his liferaft.
All five of the survivors stated that RUET had been paramount in their ability to escape the aircraft. Given the difficulties encountered by the aircrew despite being current for RUET, the investigation team believes RUET should be carried out more frequently.
2.8 Ship’s Flight Deck Camera
Following the accident of Sea King 12424 in October of 1996, one of the safety measures promulgated was to record on video all helicopter deck evolutions. To this end, video cameras with recorders were installed on all HMC Ships with flight decks. Although the ATHABASKAN’s camera was turned on and pointed at the helicopter as per standard operating procedures, the recording device was not set to record from the Landing Deck Camera, but rather to an empty channel. Therefore, an opportunity to provide valuable investigative information was missed. This imagery would not have prevented the accident, but it’s existence would have been crucial to the investigation had the aircrew not been able to successfully exit the aircraft.
31/39

2.9 Night Vision Goggles
Night Vision Goggles (NVGs) are electro-optical devices that intensify (or amplify) existing light. This ambient light comes from the stars, moon or sky glow, or from distant manmade sources. The user’s field of view is reduced from about 190° to approximately 40° eliminating peripheral vision, and depth perception is significantly compromised. NVGs display the world in only one colour (green) and under good circumstances may provide acuity approximating 20/25 to 20/45 vision.
To be compatible with NVG use, significant modifications have to be made to cockpit lighting and instrumentation. Aircrew have to undergo training on their use, and NVGs are susceptible to operator error. However, their use provides visual flight operations in circumstances where it otherwise would not be possible.
NVGs are utilized on other CF aircraft fleets including Tactical Helicopters and Search and Rescue Helicopters. Other military forces use them for shipborne operations. Information from the Ship’s Meteorological Log on the luminosity reading at the time of the accident indicates fair conditions for the use of NVGs existed. They may not have prevented this accident from occurring, but NVGs would provide MH aircrews with improved situational awareness and reduce the probability of vestibular illusion.
32/39
3 CONCLUSIONS
3.1 Findings
3.1.1 The aircraft was serviceable at the time of the accident.
3.1.2 The aircraft technical documentation and maintenance work were completed in accordance with orders and accomplished by qualified personnel.
3.1.3 The weather was within limits for Night VFR Flight.
3.1.4 The prevailing environmental conditions, other than the darkness, were not contributory to the accident.
3.1.5 The crew was qualified with respect to 1 Cdn Air Div currency requirements to perform the mission. However, the pilots were at a low level of proficiency.
3.1.6 The MHCP had recently embarked with the HELAIRDET. Upon joining the ship he was expired for DDLs, LSO currency and night hours.
3.1.7 At the time of the accident, there was no night visual approach procedure published in the SMG for recovery to Navy ships.
3.1.8 At the time of the accident, the SMG was lacking in specifics on how night approaches are to be flown and what techniques are appropriate to the situation.
3.1.9 1 Cdn Air Div Orders, Vol 5, 5-504, Annex B, Appendix 1, para 36 states “If a period of four months elapses since a pilot last conducted a night deck landing, the pilot’s night DL qualification is expired.” But there is no currency requirement for night or instrument approaches to ships.
3.1.10 There is no night visual approach currency requirement in 1 Canadian Air Division orders.
3.1.11 The MHCP at the controls became momentarily disoriented and lost visual and situational awareness in the final stages of the approach.
3.1.12 The main defences against disorientation and the perception effects are awareness and training.
3.1.13 The MHC did not take action quickly enough to either verbally warn the MHCP or physically take over control of the helicopter when the aircraft began its rapid descent.
33/39

3.1.14 The helicopter’s rear fuselage and tail rotor struck the water first, causing severe damage to the tail rotor system.
3.1.15 After water contact, the helicopter became airborne again, but as it began to yaw out of control the MHC lowered the collective control and applied right cyclic, allowing the helicopter to settle in a near-level attitude onto the sea surface.
3.1.16 The helicopter immediately rolled inverted but remained afloat for approximately one hour following the accident.
3.1.17 The HEELS lighting system functioned as it was intended to do.
3.1.18 The IPVMS #4 camera mount is susceptible to being misaligned. The #4 camera was out of proper alignment.
3.1.19 Although feasible, there is no voice recording capability on the CH124 IPVMS.
3.1.20 MH aircrews are receiving fewer opportunities to practice DDLs than in past years due to reduced availability levels of HMC Ships for training evolutions.
3.1.21 MH pilots are routinely not meeting 1 Cdn Air Div minimum flying currency requirements.
3.1.22 A survey of 12 Wing in October of 2006 found most aircrew interviewed indicated that proficiency was a significant concern when not deployed to sea.
3.1.23 The CH124 simulator is not of sufficient quality or fidelity to authentically replicate flying conditions. MH pilots do not have access to a simulator that provides realistic enough training to make up for reduced flying rates.
3.1.24 The CH124 simulator does not have a visual system, so night approaches cannot be effectively simulated.
3.1.25 The logbooks for the SlimLine backpacks and EBS assemblies do not identify their location in the aircraft.
3.1.26 The crewmember seated in the rear of the aircraft was not wearing a SlimLine backpack.
3.1.27 Flying gloves worn by MH aircrew provide no thermal protection when wet.
3.1.28 Three of the five emergency strobe lights involved in this accident leaked when exposed to seawater.
34/39
3.1.29 The serial numbers of the strobe lights were not recorded in logbooks for tracking ownership or location.
3.1.30 The emergency strobe lights had been the subject of an unauthorized modification that resulted in tape being placed over the ON/OFF switches.
3.1.31 One crewmember was able to remove a flare from his LPSV, but it did not operate when he pulled the firing ring. He was then able to activate a chemical light stick, which he had elected to keep in his LPSV, to signal the ship’s company.
3.1.32 Some of the LPSV bladders did not fully inflate when activated.
3.1.33 One pilot had difficulty locating the window emergency release handle. The other pilot was unsuccessful at locating the emergency release handle.
3.1.34 The window emergency release handles in the cockpit are unlighted.
3.1.35 All five aircrew were current for underwater escape training (RUET).
3.1.36 RUET increased the crew’s ability to egress a submerged helicopter.
3.1.37 The ship’s flight deck video camera system was improperly configured.
3.1.38 CH124 crews are not issued or trained in the use of NVGs. CH124 cockpits are not compatible with NVG use.
3.1.39 The actions taken by the ship’s company were prompt and effective in rescuing the aircrew from the sea.
3.2 Cause Factor
The accident occurred when the MHCP became momentarily disoriented and lost visual and situational awareness during a critical phase of flight. The MHC did not take action soon enough to prevent the tail rotor from striking the water.
3.3 Contributing Factor
Contributory to these causes was the lowered level of proficiency that the aircrew were maintaining due to the systemic reduction in training opportunities within the MH community.
35/39

4 PREVENTIVE MEASURES
4.1 Preventive Measures Taken
4.1.1 12 Wing initiated remedial egress and ditching drill training based on the egress difficulties encountered by this crew. This training was required for all MH aircrew prior to conducting overwater flight operations.
4.1.2 A Special Inspection of all similar CF strobe lights was conducted to remove any unauthorized tape that had been installed. Another means of securing the switch in the “OFF” position has been developed and is being implemented.
4.1.3 The TAA has mandated IPVMS camera alignment checks be carried out prior to daily flight operations.
4.1.4 Modification C-22-521-000/CF-016, “Installation of Exterior Closure Flap Extension” has been completed on LPSVs.
4.1.5 The partial inflation malfunction of the LP/SV is being addressed through a modification to the bladder cover and a replacement of the manual inflation device. Following trial and evaluation, a modification has been approved by the TAA and modifications to the LP/SVs will begin in the first quarter of 2008.
4.1.6 The OAA has developed a specific night visual approach procedure for use when helicopters recover to ships, including specific guidance concerning the transition from an instrument or night visual approach from one-half nautical mile to the Delta Hover Astern position. This procedure was added to the SMG, effective Change 7.
4.1.7 In order to ensure video recording of all flight deck evolutions onboard Canadian warships, an Engineering Change was approved for fleet wide installation of a more capable, user friendly, closed circuit TV and recording system. Approval was granted in November 2006, and installation is forecast to be completed within 24 months.
4.2 Preventive Measures Recommended
4.2.1 It is recommended that the TAA add voice-recording capability to the CH124 IPVMS.
4.2.2 The IPVMS number four camera mount (overview of cockpit area) is prone to inadvertent misalignment due to impact with the aircrew’s helmets. It is recommended that the TAA ensure this mount is modified.
36/39

4.2.3 It is recommended that the TAA investigate the issue of improving the visibility of cockpit emergency escape release handles and incorporating improvements in the CH124.
4.2.4 It is recommended that the TAA conduct an investigation into the water resistant suitability of the current issue strobe lights and modify them in order to meet the CF operational needs.
4.2.5 It is recommended 1 Cdn Air Div ensure the contractor responsible for providing CH-124 RUET incorporate the lessons learned from this aircraft ditching into current egress training provided to Canadian Forces personnel.
4.2.6 It is recommended that the OAA shorten the five year validity period of the required RUET (Rotary Wing Under Water Escape Training) and validate the annual recurrent egress training for helicopter aircrew.
4.2.7 It is recommended that the TAA/OAA incorporate an NVG capability to MH operations.
4.2.8 Because of the systemic reduction in CH124 training opportunities, it is recommended that the CF procure, or provide access to, a flight simulator with realistic night and instrument ship approach training capability for MH pilots.
4.2.9 It is recommended that the OAA amend CH124 pilot currency requirements to include visual and instrument approach currency to HMC or other Navy Ships.
4.2.10 It is recommended that Canadian Forces School of Survival and Aerospace Training (CFSSAT) use the lessons learned from this accident to increase awareness and reemphasize the effects of disorientation and perception to CF student aircrew.
4.2.11 It is recommended that the CMS increase the availability of HMC Ships for 12 Wing aircrew DDL and night approach training.
4.2.12 It is recommended that the OAA investigate the procurement of improved flying gloves that afford better thermal protection when wet.
4.2.13 It is recommended that the OAA ensure all CH124 crewmembers wear SlimLine backpacks at all times while flying overwater.
4.2.14 It is recommended that the OAA modify procedures so the logbooks for both the SlimLine backpacks and the EBS assemblies are annotated to show the location of each item in the helicopter.
37/39

4.2.15 It is recommended the OAA modify the contents of the LPSVs to ensure appropriate day/night signalling devices are available to aircrew.
4.3 Other Safety Concerns
Nil.
38/39

4.4 DFS Remarks One has to go back to 1967 to find another accident where a serviceable Canadian Forces’ Sea King flew into the water at night, and even so, that accident happened during cruise flight and not during the approach phase. So, given the long history of safe night approaches to the decks of ships, this investigation needed to inquire into what factors led to this particular night approach being unsuccessful after so many years of safe operations. The answers point to an insidious combination of circumstances that led to a lowering of aircrew proficiency within the Sea King community. Low aircraft serviceability coupled with fewer decks being available for night evolutions led to a situation where it became the norm for pilots to achieve only the absolute minimum levels of currency, vice the levels of proficiency commensurate with safe and effective flight operations. The situation was made more complicated in that it was, and remains, very difficult for the Air Force to objectively measure aircrew proficiency with the tools currently available. In former years the kind of specific guidance found wanting today in the Standard Manoeuvre Manual was probably thought unnecessary when flying hours and decks were more plentiful and aircraft were available for honing perishable skills such as night approaches to ships. Likewise, the limited capabilities of the flight simulator were likely offset by the greater amount of flying time available to the crews in the past. Unfortunately, flying hours, aircraft and decks have not been so available in the last few years, and while there has been an improvement in aircraft availability recently, the number of available decks may continue to be constrained by other factors such as frigate modernization. As the Sea King will continue in service for several years before its replacement is operational, the proposed preventive measures consider any practical means of enhancing aircrew proficiency and safety, notwithstanding that implementation of an NVG capability and simulator enhancements would be very challenging.
An accident such as this also offers an unsought but useful opportunity to examine the safety aspects of aircrew equipment, egress from the aircraft and emergency response plans. Deficiencies that might otherwise remain hidden come to light, and as a result several preventive measures have been proposed to improve the prospects for individual survival should another such crash occur. C.R. Shelley Colonel Director of Flight Safety
39/39

Annex A to 1010-CH12438 Dated 30 Jan 08 ANNEX A: ABBREVIATIONS AESOP Airborne Electronic Sensor Operator ALSE Aircrew Life Support Equipment AOI Aircraft Operating Instructions CF Canadian Forces CFTO Canadian Forces Technical Order CMS Chief of the Maritime Staff CPI Crash Position Indicator CTD Maritime Helicopter Combat Training Directive DPF Dedicated Proficiency Flight DDL Destroyer Deck Landing DFS Director of Flight Safety EBS Emergency Breathing System ELT Emergency Locator Transmitter ESUS Electronic Sound Underwater Signaling Device FAF Final Approach Fix FLYCO Flying Coordinator FSIR Flight Safety Investigation Report HEELS Helicopter Emergency Egress Lighting System HELAIRDET Helicopter Air Detachment HMCS Her Majesty's Canadian Ship ICS Intercom Systems IPVMS Instrument Panel Video Monitoring System LLOW Low Level Over Water LSO Landing Signals Officer MGB Main Gear Box MH Maritime Helicopter MHC Maritime Helicopter Pilot MHCC Maritime Helicopter Crew Commander MHCP Maritime Helicopter Co-pilot MND Minister of National Defense NM Nautical Mile NRC National Research Council PMA Pilot Monitored Approach RCA Radar Controlled Approach RUET Rotary-Wing Underwater Escape Training SAC Ships Air Controller SOP Standard Operating Procedures SMG Standard Manoeuvre Guide SNMG 1 Standing NATO Maritime Group 1 TACCO Tactical Coordinator TBD To Be Determined VHS Video Home System VFR Visual Flight Rules
A-1/1

Annex B To 1010-CH12438 (DFS 2-2) Dated 30 Jan 08
ANNEX B: PHOTOGRAPHS
Photograph 1: Sea King inverted and floating.
Photograph 2: Recovery from the seabed.
B-1/5

Annex B To 1010-CH12438 (DFS 2-2) Dated 30 Jan 08
Photograph 3: Main rotor head.
Photograph 4: Tail rotor.
B-2/5

Annex B To 1010-CH12438 (DFS 2-2) Dated 30 Jan 08
Photograph 5: Right Side on barge.
Photograph 6: Left Side on barge.
B-3/5
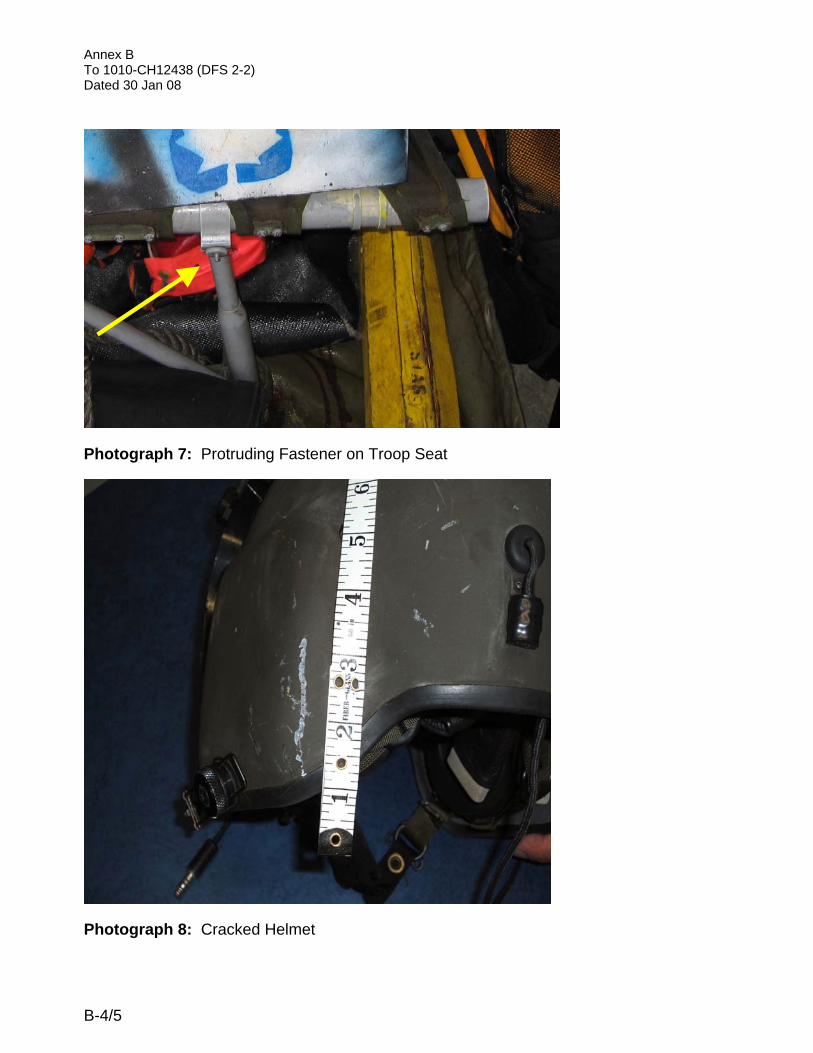
Annex B To 1010-CH12438 (DFS 2-2) Dated 30 Jan 08
Photograph 7: Protruding Fastener on Troop Seat
Photograph 8: Cracked Helmet
B-4/5

Annex C To 1010-CH12438 (DFS 2-2) Dated 30 Jan 08
Figure 1: Sea King at +15° attitude
P ilo t A v a ila b ility
36 3741
22
4449
53
14 1210
8
6
5
925 24
42
23 16
10
14 14 1314 14
15 12
23
0
10
20
30
40
50
60
70
80
90
100
O c t-05 N ov-05 D ec -05 Jan-06 F eb-06 M ar-06 A pr-06
G rounded
E x p ired
Day O nly
Current
Figure 2: 12 Wing Pilot Status, October 05 to April 06.
B-5/5