cancer contributions to qipp dr janet williamson national director, nhs improvement the beeches...
TRANSCRIPT
Cancer Contributions to QIPP
Dr Janet WilliamsonNational Director, NHS Improvement
The Beeches Conference Centre, Birmingham 4 November 2010

“We must keep a relentless focus on improving quality and productivity. The
QIPP programme and the need to achieve £15 - £20 Billion inefficiency savings by
20/03/14 are now more pressing than ever. We need to build on the excellent planning
work you have all done”.
Sir David Nicholson, NHS Chief Executive 2010
Political Context for Cancer• Election Campaign (April 2010) – cancer featured
prominently in Leader’s debate• Coalition Government agreement (May 2010)• White Paper: Equity and Excellence – Liberating
the NHS (July 2010)• Announcement of Cancer Reform Strategy
‘Refresh’ – To be completed by Winter 2010– Emphasis on improving outcomes

Equity and Excellence: Liberating the NHS
• Key messages– Information and choice: ‘No decision about me without
me’– Emphasis on outcome measures, not process targets– Commissioning: NHS Commission Board and GP
consortia– Ring fenced public health budget
Aims of ‘Refreshing’ the Cancer Reform Strategy
• To align cancer strategy with the White Paper• To set the direction for the next 5 years –
taking account of progress since 2007• To show how outcomes can be improved
despite the cold financial climate

Last 15 years: Huge investment in quality, equipment, manpower and redesign in
cancer • Prevention: screening• Care: cancer waits, access, centralisation
surgery new drugs• Clinical infrastructure – MDTs networks, clinical
teams, facilities
Mortality reduces by 2% pa under 75s

Gap in service provision remains … • Early Diagnosis
– 10,000 avoidable deaths p.a.
• Survivorship– Over 3 million survivors– Service provision based in OPD
• Inpatient – increasing emergency admissions (52%)
• 14,000 occupied bed (60% non elective• Inequalities – variations UK wide

• How many trips to the GP before diagnosis?
• Why do 40% blood samples have defects?
• Why does a woman needing breast surgery for cancer stay in hospital for 6 days when 23 hours is available?
• Over 12 weeks from smear to result in hand for a test that takes 5 hours to process.
Where the difference can be made

Rationale
• Patients do not wish to be in hospital more often or longer than necessary
• Bed utilisation in England for cancer patients is higher than elsewhere
• Inpatient care accounts for around half of all cancer expenditure
• Inpatient bed utilisation varies widely between PCTs (even when cancer incidence has been accounted for)
• We need to improve productivity if we are to introduce new life saving technologies

If all cancer services adopted the winning principles &the key improvements this can save a million bed days
Unscheduled (emergency patients) should be assessed prior to the decision to admit. Emergency admission should be the exception not the norm.
Patients should be on a defined inpatient pathways based on their tumour type and reasons for admission.
Clinical decisions should be made on a daily basis to promote proactive case management.
Patient and carers need to know about their condition and symptoms to encourage self-management and to know who to contact when needed
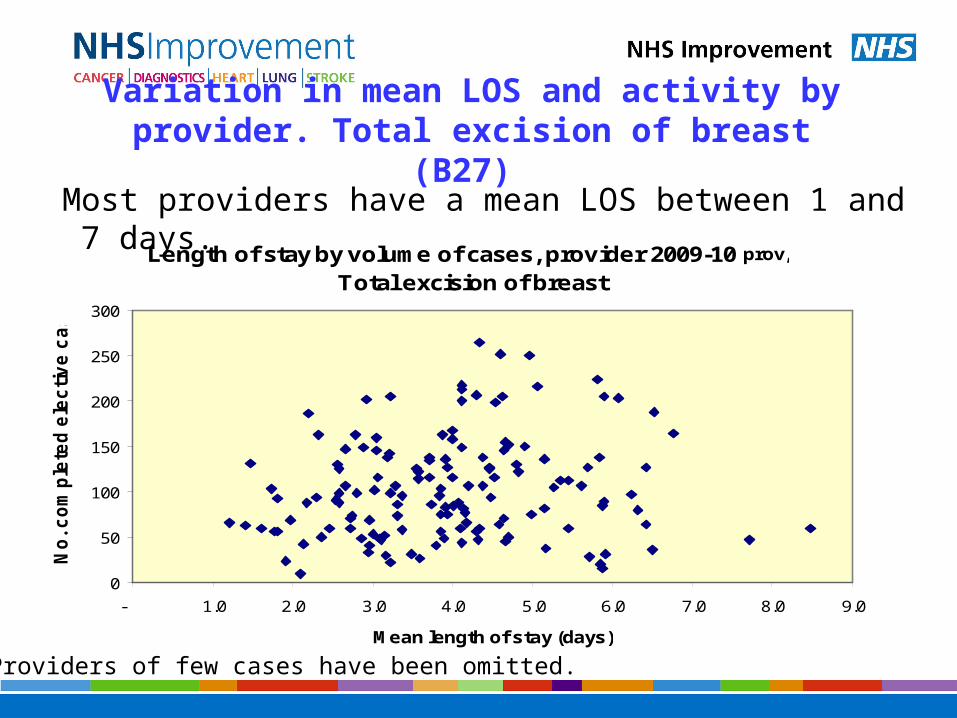
Variation in mean LOS and activity by provider. Total excision of breast (B27)
Most providers have a mean LOS between 1 and 7 days.
Length of stay by volume of cases, provider 2009-10 prov,
Total excision of breast
0
50
100
150
200
250
300
- 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0 9.0
Mean length of stay (days)
No
. c
om
ple
ted
ele
cti
ve
ca
se
s
Providers of few cases have been omitted.

**Pre-operative surgical assessment • Full clinical & risk assessment eg thrombolysis prophylaxis• Default booking as day case – overnight booking as the exception not the rule• Specialist advice… anaesthetic/co-morbidity management• Check patient informed surgical consent• Inform patient of admission time, length of stay & discharge date• Patient education: self management e.g. arm mobility exercises - physiotherapist/nurse/DVD• Prosthesis advice/fitting• Prescribe TTO’s• Plan theatre scheduling and timing
Intra-operative• Drains the exception not the norm • Anaesthetics: short acting/ local anaesthetic• Analgesia: non steroidal/non opiate • Minimal intra operative fluids• *Sentinel node Biopsy
Post-operative• Analgesia: avoid PCA/opiates• Provide nutrition and mobilise• Nurse led discharge • Patient discharge summary with 24/7 contact information and wound care advise• Discharge day case (85% of patients)• 23 hour discharge (1 night stay, 15% of patients)• GP discharge summary• Drain management information (if required)• Fitting permanent prosthesis• Dispense TTO’s
Surgical follow-up options• No follow up required• Patient activated e.g. telephone call/questionnaire• Pro-active follow up call• Outpatients appointment• GP follow-up• Open Access: seromas/drain management and complications• Joint clinic: e.g. further treatment options: chemotherapy/radiotherapy• Palliative care
*Intra-operative - Sentinel Node Biopsy: In centres where adequate training has been provided. Extra theatre time e.g. 40mins is required for this procedure
Primary care – optimising pre- operative health• Blood pressure • BMI, diabetes etc.• Lifestyle advice• Patient choice • Patient information
Diagnosis (Triple Assessment Clinic) • Full clinical assessment• Mammogram/ultrasound/ +/-MRI +Chest X-ray • Core/fine needle biopsy • Bloods• Discuss informed consent• Pathology reportingOutcomes• Discuss results• Involve patient in choice of treatments/trials/reconstruction• Obtain patient informed surgical consent• Confirm treatment/surgery date ** Pre-operative assessment• Provide patient information prescription, hand held record/care plan/patient diary• Inform patient of next steps• Inform GP positive results within 24 hours/negative within 10 working days
Admission (Day Unit, Treatment Centre, Surgical Ward)• Admit day of surgery• Starvation – the ‘2 and 6’ rule fasting time 6 hours for food and clear fluids 2 hours prior to surgery (consider carbohydrate drink)• No pre med• Pre-op analgesia (paracetamol/ non steroidals)
‘Patient involvement & Choice Guarantee’ ‘Professional & Patient Outcome Audits’
Continuing care for cancer patients• Continuing cancer care assessment care plan (including referral as appropriate to AHPs)• Education – self care management programme• Palliative care
Day Case/23 Hour Breast Surgical Pathway
Patient informed decision making
**Pre-operative - Surgical assessment at diagnosis clinic or minimum 7 days prior to surgery
7/10/2010

Transferring the lessons from Birmingham
An exemplar in improvement
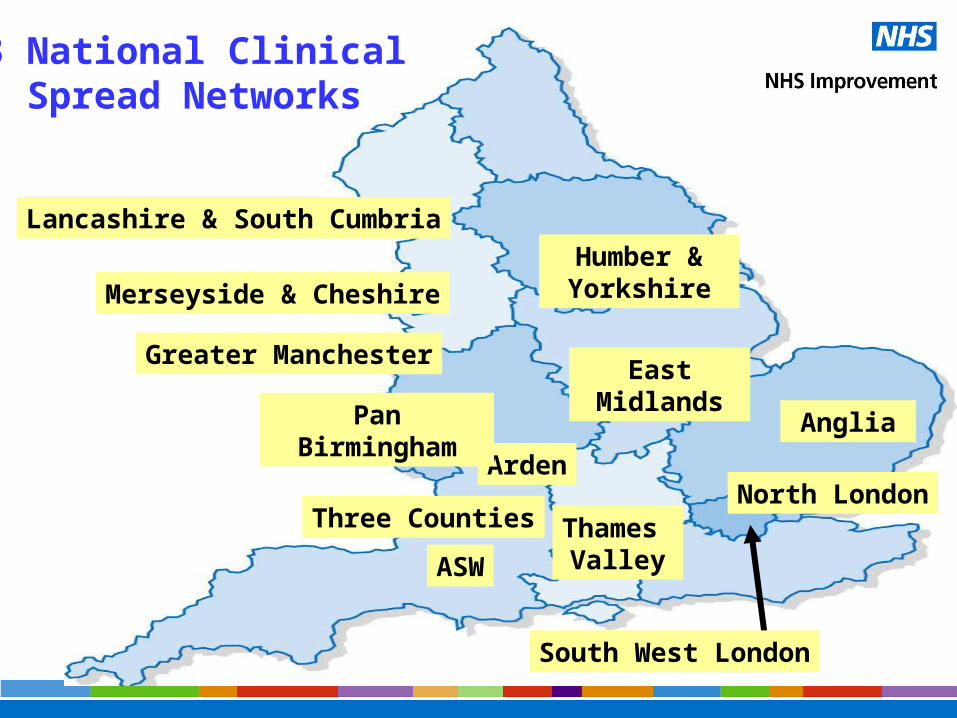
13 National Clinical Spread Networks
Thames Valley
Merseyside & Cheshire
Lancashire & South Cumbria
Greater Manchester
Humber & Yorkshire
East Midlands
Anglia
Arden
South West London
Pan Birmingham
North LondonThree Counties
ASW

Potential for Breast Day Case/23 Hour Model
• National average Los 2.8 days (HES 09)= 95,200 bed days
• Approx 34,000 new case registered per annum
• 1 day stay = 34,000 bed days

Cytology screening
• 14 day standard delivery by end 2010 (baseline 12 weeks+)
• Delivery of standard requires:– Understanding of process and redesign
– First in, first out principles
– Single queues
– Small batches
– Daily problem resolution

The Result (QIPP) across 10 pilots
• Q. 100% delivery of
the 14 day standard– 80% in 7 days
• I. New processes • P. £100K savings per
site– 14% re-work eliminated
• National impact £18million per annum
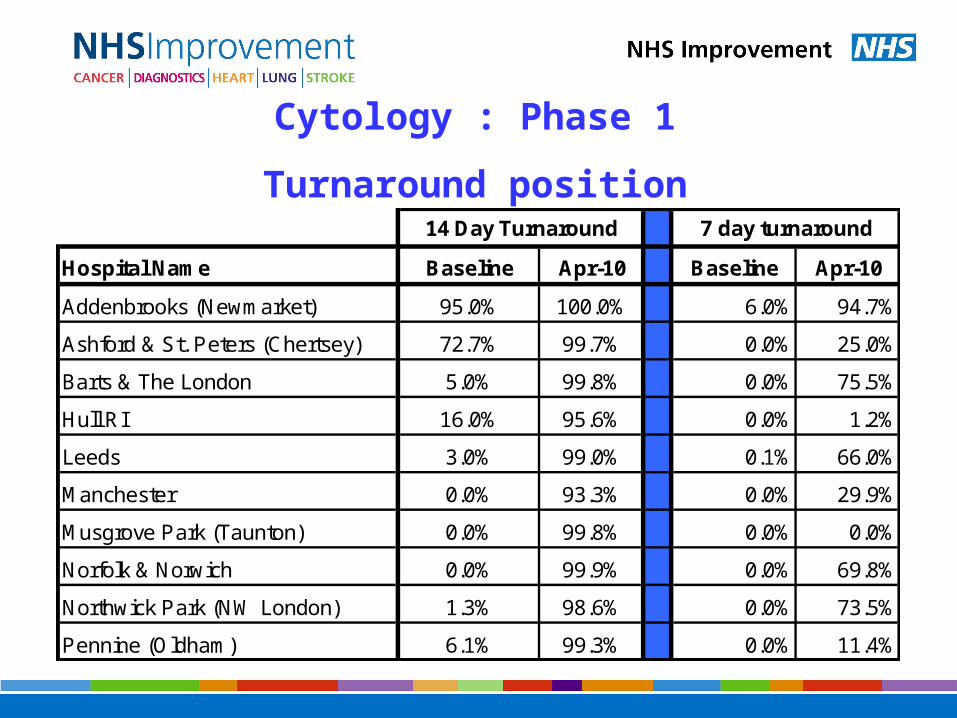
Hospital Name Baseline Apr-10 Baseline Apr-10
Addenbrooks (Newmarket) 95.0% 100.0% 6.0% 94.7%
Ashford & St. Peters (Chertsey) 72.7% 99.7% 0.0% 25.0%
Barts & The London 5.0% 99.8% 0.0% 75.5%
Hull RI 16.0% 95.6% 0.0% 1.2%
Leeds 3.0% 99.0% 0.1% 66.0%
Manchester 0.0% 93.3% 0.0% 29.9%
Musgrove Park (Taunton) 0.0% 99.8% 0.0% 0.0%
Norfolk & Norwich 0.0% 99.9% 0.0% 69.8%
Northwick Park (NW London) 1.3% 98.6% 0.0% 73.5%
Pennine (Oldham) 6.1% 99.3% 0.0% 11.4%
14 Day Turnaround 7 day turnaround
Cytology : Phase 1
Turnaround position
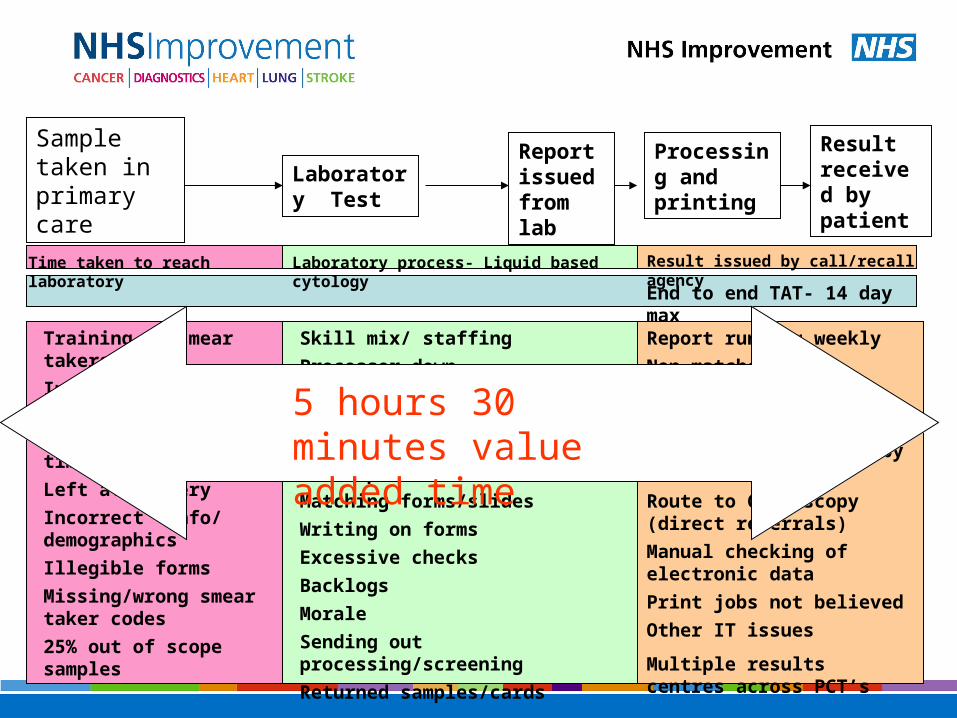
Sample taken in primary care
Laboratory Test
Report issued from lab
Result received by patient
End to end TAT- 14 day max
Laboratory process- Liquid based cytology Time taken to reach laboratory Result issued by call/recall agency
Training of smear takers
Inconsistent use of NHS numbers
Transport-delivery times/ routes
Left at surgery
Incorrect info/ demographics
Illegible forms
Missing/wrong smear taker codes
25% out of scope samples
Skill mix/ staffing
Processor down
Data entry issues
Over- printing labels
Double look-up/ printing from open-exeter
Matching forms/slides
Writing on forms
Excessive checks
Backlogs
Morale
Sending out processing/screening
Returned samples/cards
Report running weekly
Non-matches
Enveloping- leaflets
Postage
‘Abnormals’ sent out by GP
Route to Colposcopy (direct referrals)
Manual checking of electronic data
Print jobs not believed
Other IT issues
Multiple results centres across PCT’s
Processing and printing
5 hours 30 minutes value added time


Innovation
• Diffusion of innovation is critical• ‘Adaption’ not adoption is central
– Open networks not closed alliances– No need to totally reinvent wheel
• Define in terms of value added• Headspace for innovation• Defining ‘What to do’ and ‘How’
‘The best way to improve services is through healthy plagiarism’. National Clinical Lead, Heart

• ‘Not invented here’• ‘We don’t work like that’• ‘It’s easy for them. They have 6 nurse specialists and a
couple of GPwSI.’• ‘We can’t do more work without more staff/ equipment’• ‘Jumping straight to solutions’• ‘Not taking time to understand the process’
The biggest enemies of improvement are:
Source National Clinical Leads NHS Improvement

The big opportunities
• Early diagnosis and prevention
• New models of care– Long term conditions– Self and supportive care
• Transforming ‘inpatients’
• Diagnostics
