cancer pain พระนั่งเกล้า2
TRANSCRIPT

แนวทางเวชปฏบต
การดแลรกษาผปวยปวดจากมะเรง
พญ.ฉนทนา หมอกเจรญพงศ
กลมงานเวชศาสตรประคบประคอง
สถาบนมะเรงแหงชาต
กรมการแพทย กระทรวงสาธารณสข

ความปวด ***** PAIN
An unpleasant sensory and emotional
experience associated with actual or potential
tissue damage, or described in terms of such damage
ประสบการณทไมสบายกาย ไมสบายใจ ทเกดจากการ
บาดเจบของเนอเยอหรอศกยภาพทจะท าใหมการบาดเจบของ
เนอเยอ หรอประหนงวามการบาดเจบ
FACTS ABOUT CANCER PAIN
Frequency of occurrence varies with ;
• stage of the disease• primary site of the tumor
Moderate or severe pain occurs in 30 - 40%
of the patients at the time of diagnosis and 60 - 100% with advanced cancer
Most cancer patients have more than one pain

ความปวดทพบในผปวยมะเรง
เกดจากหลายสาเหต

CAUSES OF PAIN
1. Due to tumor involvement 78%
• bone, nerve, soft tissue, viscera
2. Associated with treatment 19%
• diagnosis and staging procedures
• surgery
• chemotherapy; mucositis, phlebitis,
tissue necrosis, myalgia, arthralagia
• radiotherapy; mucositis, neuropathy,
myelopathy
CAUSES OF PAIN
3. Due to general illness but not cancer (10%)• constipation
• pressure
• gastric distention
• reflux esophagitis
• bladder spasm (with catheterization)
• musculoskeletal pain
• thrombosis and embolism
• mucositis
• post herpetic neuralgia
4. Unrelated to cancer or its treatment(10%)

ความปวดจากมะเรงมผลเสยทางดานความเปนอย จตใจ
อารมณ สงคม ของผปวยและผใกลชด

ASSESSMENT: REVIEW OF THE SYSTEMS
1. Systemic/constitutional• anorexia เบออาหาร
• weight loss น าหนกลด
• cachectic ผอมหนงหมกระดก
• fatigue/weakness ความลา / ออนแรง
• insomnia นอนไมหลบ
2. Neurologic• sedation งวงซม
• confusion มนงง สบสน
• hallucination ประสาทหลอน
• headache ปวดศรษะ
• motor weakness กลามเนอออนแรง
• altered sensation การรบความรสกเปลยนแปลง
• incontinence กล นไมอย
ASSESSMENT: REVIEW OF THE SYSTEMS
3. Respiratory• dyspnea, cough, hiccough
4. Gastrointestinal• dysphagia - dehydration
• nausea/vomiting - constipation/diarrhea
5. Psychological• irritability - depression
• anxiety - dementia
6. Integument• decubitus
• dry, sore mouth

Physical
well-beingPsychological
well-being
Social
well-beingSpiritual
well-being
Quality of life for cancer patients in pain

Pain
Total suffering
Psychological problems
Physical symptoms
Spiritual concerns
Cultural factors
Social difficulties
GETTING TO KNOW CANCER PAIN
• Acute pain – Chronic pain
• Nociceptive – Neuropathic
• Somatic – Visceral
• Basal – Breakthrough – Incidental pain
• Biopsychosocial impact

Nociceptive pain
Inflammatory
pain
Neuropathic pain
Visceral pain
Bone pain
Existing suffering
Cancer pain

KEY TO SUCCESSFUL PAIN MANAGEMENT
• Comprehensive pain assessment and diagnosis
• Formulate treatment plan
• View the treatment as a dynamic process
• Explanation
• Rx of the underlying cause
• Elevation of the pain threshold
• Interruption/destruction/stimulation of the pain pathways
• Change of life style

KEY TO SUCCESSFUL PAIN MANAGEMENT
• WHO guidelines are the mainstay • But !!! Not the only solution
• Talk to the patient and care-givers will• Reinforce patient autonomy
• Increase pain tolerance
• Improve coping skills
• Allay misconceptions
HOW TO ACHIEVE MAXIMUM BENEFIT FROM ANALGESIC LADDER
• Choose the drug according to severity of pain
• Only one drug in a class
• Combine one drug from each of different classes
• Multimodal analgesia – polypharmacy
• Use coanalgesics or adjuvants
HOW TO ACHIEVE MAXIMUM BENEFIT FROM OPIOIDS
• For opioid naive patient with moderate pain
• Codeine 90-120 mg/day
• Tramadol 150-200 mg/day
• Morphine 15-20 mg/day
• Oxycodone 10 mg/day
• Titration for patient with severe pain
• Morphine immediate release (MIR)
• Morphine sustained release (MST)
• Big dose tramadol?
• Fentanyl TTS

HOW TO ACHIEVE MAXIMUM BENEFIT FROM OPIOIDS
• Start with any appropriate route of administration
• Oral MIR 10 mg q 6 h (60 mg/day)
• IV bolus titration
• IV PCA
• Rescue dose 16% of total daily dose
• Increase dose by 33-50% or rescue dose + in
suitable interval
• Switch to oral dose of MST or Fentanyl TTS
BREAKTHROUGH PAIN, INCIDENTAL PAIN AND RESCUE ANALGESIC
• Incidence 19-95%
• Medications:
• MIR: MSS, tablet
• Tramadol
• Dose 10-15% of total daily dose
• Mismatch between breakthrough pain profile and opioid
pharmacokinetics:
• Methadone
• Various routes of administration; IV, nasal, sublingual,
effervescent morphine, oral transmucosal fentanyl

HOW TO ACHIEVE MAXIMUM BENEFIT FROM OPIOIDS
• Aware of the inter- and intra-individual response to
opioids
• Problematic start!!!!
• Sedation
• Nausea
• Patients with excruciating pain
• Fast titration
• Test dose IV morphine
• Re-evaluate the pain syndrome

HOW TO ACHIEVE MAXIMUM BENEFIT FROM OPIOIDS
• Patients with poor respond;
• Wider opening therapeutic
window by aggressive side
effects treatment
• Opioid rotation
• Coanalgesics or adjuvants
• Non-pharmacological
approaches

การประเมนความปวด

PAIN ASSESSMENT
• Location of all the pain
• How the pain feels
• Intensity of the pain
• When, frequency, duration
• What ease the pain, what worsen
the pain
• Medications taking
• Side effects of pain medications
• Quality of life issues
•Pain diary!

PAIN ASSESSMENT
• Chronicity: Acute vs Chronic pain • Pain intensity
• Pathophysiology:
somatic vs. visceral
nociceptive vs. neuropathic
• Course of the disease: continuous,
breakthrough, incident pain.
• Pain syndrome: brain metastasis,
bone pain
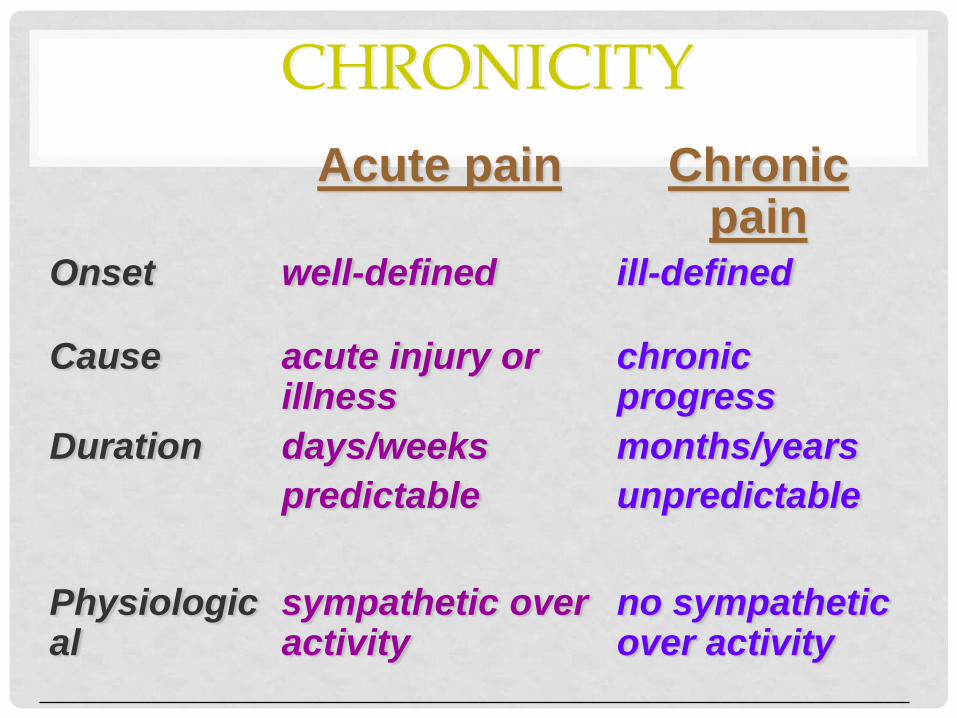
CHRONICITY
Acute pain Chronic pain
Onset well-defined ill-defined
Cause acute injury or illness
chronic progress
Duration days/weeks
predictable
months/years
unpredictable
Physiological
sympathetic over activity
no sympathetic over activity

Acute pain Chronic pain
Affective anxiety depression
Cognitive meaningful meaningless
Behavioral inactivity until recovery
changes in life style
changes in functional ability
withdrawn
Treatment cause
temporary analgesics
supportive
regular analgesics

CATEGORAL SCALES
• Verbal rating scale (VRS)
(verbal descriptor scale)
• 2 – 7 words
None Mild Moderate Severe
• Pain relief
None Slight Moderate Good Complete
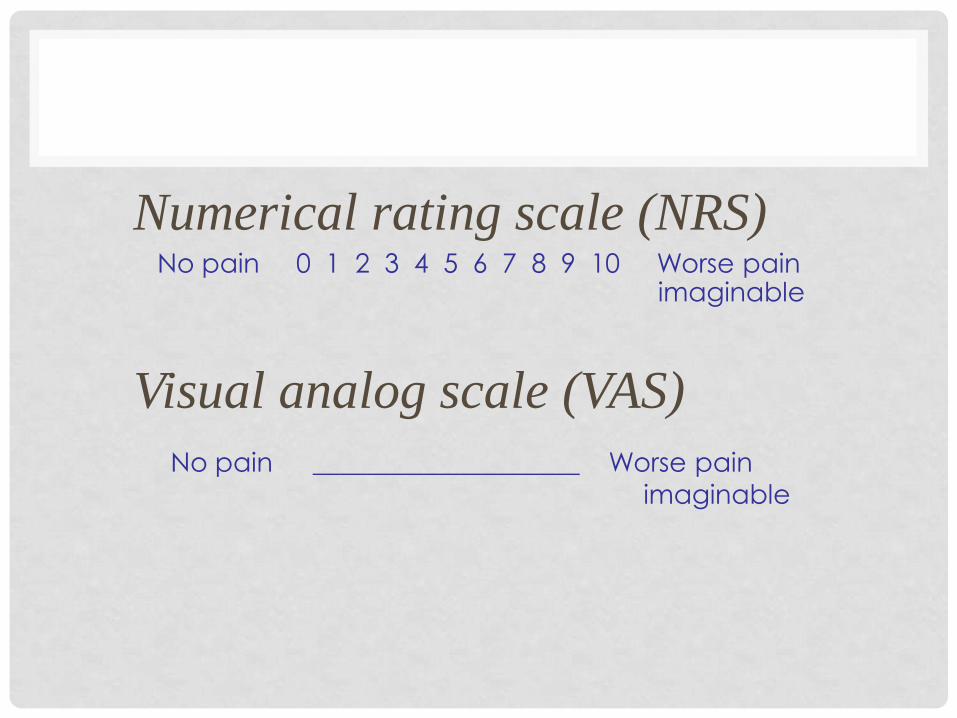
Numerical rating scale (NRS)No pain 0 1 2 3 4 5 6 7 8 9 10 Worse pain
imaginable
Visual analog scale (VAS)
No pain ____________________ Worse pain
imaginable

HAPPY/SAD FACES.
PAIN ASSESSMENT
• Chronicity: Acute vs Chronic pain
• Pain intensity
• Pathophysiology:
somatic vs. visceral
nociceptive vs. neuropathic
• Course of the disease: continuous,
breakthrough, incident pain.
• Pain syndrome: brain metastasis,
bone pain
• รปตกตา pain
• ไฟล pdf cheop scales

PATHOPHYSIOLOGY
• Nociceptive ( somatic and visceral )
• constant and well localized
• aching, throbbing, gnawing
• vague in distribution and quality, deep, dull, aching, dragging, squeezing, pressure-like
• Neuropathic
• may be constant, steady, and spontaneously maintained, intermittent, shock-like, shooting, lancinating, electrical, burning, tingling, numbing, pressing, squeezing, and itching
• dysesthesia, hyperalgesia, allodynia, hyperesthesia, hyperpathia
NEUROPATHIC PAIN
• Hardest mechanism to treat
• Diagnose straightforward: nerve or
dermatome distribution, no local tenderness
but referred
• Two types
• Mixed: nociceptive/neuropathic due to tumor
invasion or compression of nerve pathway;
brachial, lumbosacral plexus, chest wall invasion,
spinal cord compression
• Pure (Deafferentation): no nociceptive element;
PHN, post-thoracotomy syndrome, phantom pain




BONE PAIN
• Most common cause of pain in advanced
cancer
• Most common malignancies metastasize to
bone: breast, prostate, lung, kidney, thyroid
• Common problems: chronic bone pain, pathologic
fracture, hypercalcemia
• Treatment includes: NSAIDs, opioids, radiotherapy,
Strontium-89, bisphosphonate, corticosteroids, calcitonin.
• Early Orthopedic consultation and treatment is
important
PATTERN OF PAIN
Constant pain
Breakthrough and
incident pain
Intermittent pain

หลกการระงบปวดในผปวยมะเรง
PRINCIPLE OF ANALGESIC USE
• Define the nature of pain
• Maximize the current regimen
• Understand the drug Pharmacology
• Speed of onset and duration of action
• Management of side effects
• Beware of the drug interactions
• Emphasize patient education

CANCER PAIN MANAGEMENT
• Pharmacologic
treatment
• Non-
Pharmacologic treatment
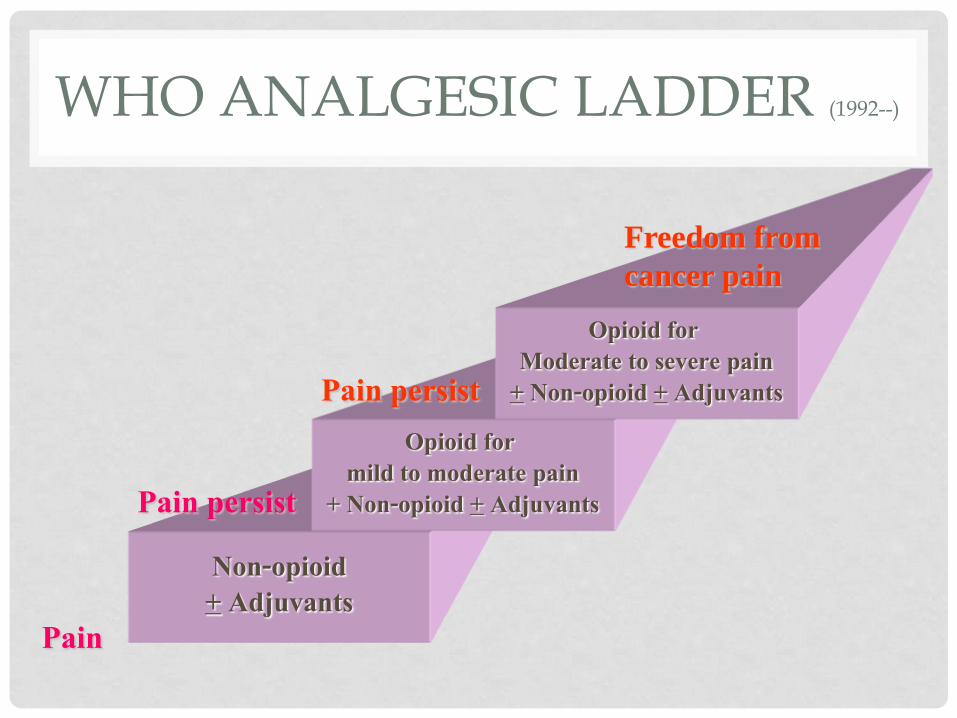
WHO ANALGESIC LADDER (1992--)
Non-opioid+ Adjuvants
Opioid for mild to moderate pain
+ Non-opioid + Adjuvants
Opioid for Moderate to severe pain
+ Non-opioid + Adjuvants
Pain
Pain persist
Pain persist
Freedom from
cancer pain

MORPHINE เปนยาแกปวดรนแรงทดทสดในปจจบน
ใชกนไดสะดวก
บรหารไดหลายวธ

ESSENTIAL CONCEPTS IN THE WHO APPROACH TO DRUG THERAPY
•By the mouth
•By the clock
•By the ladder
• For the
individual
•With attention to detail
PRINCIPLES OF ANALGESIC USED
•Administer on strict schedule to
prevent pain, not PRN
•Give instructions for treatment of
breakthrough pain
• Following analgesic ladder
•Review & assess
GENERAL RECOMMENDATIONS
• Oral medications should be used as the first line approach.
• Any proposed systemic regimen must be individualized.
• There is no predetermined maximum dose of an opioid.
• Dose titration may be required periodically.

ADVERSE DRUG EFFECTS FROM OPIOID THERAPY
• Tolerance
• Physical dependence
• Addiction
• Constipation
• Sedation
• Nausea-vomiting
• Mental clouding
• Myoclonus, pruritus, urinary retention
• respiratory depression

NAUSEA
• Moderate to severe 8.3 – 18.3%
• Direct effect of opioids on CTZ
• Decrease quality of life, limit food
intake
• Other underlying conditions; electrolyte imbalance, dehydration, brain metastasis, intestinal obstruction, ileus, chemotherapy, tumor of the GI, constipation, infection, blood poisoning, kidney problems, anxiety, etc.

NAUSEA
• Usually subside within few days
• Treatment;
• Metoclopramide ( block in GI tract and CTZ)
• Butyrophenones (haloperidol, droperidol) (at CTZ)
• Phenothiazine (CTZ, GI, vestibular)
• Antihistamine (dramamine,hydroxyzine) (H1 blockade and VC)
• Hyoscine, scopolamine (VC and GI)
• Ondansetron (5HT3 in GI and CTZ)• Benzodiazepine (lorazepam) GABA agonist

CONSTIPATION
• The most troublesome, almost everyone is involved,
will not develop tolerance

TREATMENT OF CONSTIPATION
• Stimulant laxatives• Senokot 1 tab hs – 4 tab tid orally
• Dulcolax 1 tab hs – 3 tab tid orally
• Bulk-forming laxatives• Metamucil 1 tsp in 8 oz water OD – tid
• Bran
• Saline or osmotic cathartics• MOM 15 – 40 ml OD – bid
• Magnesium citrate solution 240 ml OD
CNS EFFECTS
• Aggravating factors;
• High doses opioid
• Psychoactive drugs
• Renal failure
• Slow down of cognitive function, sedation,
hallucination and delirium, fluctuation of
consciousness, change in sleep-wake cycle,
agitation, myoclonus.
• Improve spontaneously
CNS EFFECTS
• Role of M-3-G
• Management;• Opioid rotation
• Dose reduction
• Circadian modulation
• Hydration
• Psychostimulants
• Other drugs; haloperidol, midazolam, baclofen, clonazepam,clonidine
ADJUVANTS
• Antidepressants : tricyclic antidepressant (amitriptyline), SSRI (Fluoxitine)
• Anticonvulsants : Carbamazepine (tegretol), Hydantion (dilantin), Gabapentin (Neurontin)
• Sedatives, hypnotics, tranquilizers
• Steriod
• Muscle relaxants

ADJUVANTS
DRUGS
- Anticonvulsants
- Antidepressants
- Local anesthetics
- Corticosteroids
- Antihistaminics
- Muscle relaxants
- Psychostimulants
- Drug action on bone
INDICATIONS
- neuropathic pain
- neuropathic pain
- neuropathic pain
- multiple
- coanalgesic, antiemetic
- muscle spasm
- opioid sedation
- bone pain

ANTIDEPRESSANTS
• Used in neuropathic pain ; several studies in
Diabetic neuropathy, Post-herpetic neuralgia,
phantom limb pain, migraine headache
• Reduce insomnia and anxiety
• 1-2 weeks lag time for clinical effects
• Start 10-20 mg hs
• Escalated 4-5 day intervals to doses 100- 150
mg
• Abrupt escalation not recommended

TCA USES LIMITED BY SIDE EFFECTS
•Anticholinergic : dry mouth, visual changes, constipation, tachycardia, urinary retention, reduced gastric motility, worsen narrow angle glaucoma
•Antihistamine : sedation
•Alpha adrenergic blockade :orthoststic hypotension
• Sodium channel blockade :prolonged QT and QRS
สรปแนวทางการระงบปวดผปวยโรคมะเรง
•มะเรงเปนโรคทมผลรายตอชวต มะเรงระยะทายท าให ผปวยจ านวนมากมความปวด
•ความปวดทพบในผปวยมะเรงมหลายสาเหต รกษาตามความเหมาะสมของแตละสาเหต
•การประเมนความปวดมท งทางกายและทางใจ
•ปรมาณความปวดดไดจาก VAS ฯ

สรปแนวทางการระงบปวดผปวยโรคมะเรง
•การระงบปวดใชยาเปนหลก
•ใหยาระงบปวดตามความรนแรง ตามเวลาอยางตอเนอง
เสรมเมอตองการเพม และประเมนผลการรกษาบอยๆ
•ยงมการระงบปวดโดยไมใชยาอกหลายวธ
•ดแลคณภาพชวตของผปวย

Thank you

การดแลผปวยตอเนองทบาน
•บรการทตองส ารวจ ประเมน และสรปความตองการการดแลสขภาพทแทจรงของผปวย
• เพอใหบรการปองกน แกไขปญหาสขภาพ ปองกนการปวยซ าดวยโรคเดม และแกไขปญหาอน ๆ ทเกยวของกบ
ปญหาสขภาพ
•โดยก าหนดแผนการดแลรวมกบผปวย ครอบครว และทมสขภาพ ในขณะด าเนนการวางแผนจ าหนายในหอผปวย
หรอเปนแบบผปวยนอก

• การดแลผปวยทบานทมประสทธภาพจะชวยใหผปวย และครอบครว
พฒนาความสามารถในการดแลตนเองไดเรวขน
เกณฑในการรบผปวยเพอการดแลตอเนองทบาน
1. ผปวยทสงปรกษาจากแพทยเจาของไข หรอพยาบาล ซงเปน
ผปวยทตองการดแลยงยากซบซอนเปนรายกรณ และทจ าเปน
ตองการการดแลตอเนองทบาน ท งผปวยในและผปวยนอก
2. ผปวยทสงปรกษามาเพอตองการใชอปกรณ หรอเครองมอพเศษ
เมอกลบบาน เชน เครองชวยหายใจ เครองพนยาเปนตน

ขนตอน/กจกรรมการดแลตอเนองทบาน
• กอนการเยยม
1. เตรยมความพรอมของครอบครวในการชวยเหลอ ใหการดแล หรอ
จดการการดแลผปวยทบาน
2. ก าหนดเปาหมายและวางแผนการดแลผปวยตามปญหาทก าหนด
รวมกบครอบครวและ ทมแพทย พยาบาล
3. นดหมายการเยยมบาน ภายใน 1 สปดาห หลงการจ าหนาย
4. ประชมปรกษากอนการเยยมดแลทบาน
ขนตอน/กจกรรมการดแลตอเนองทบาน
• ขณะเยยม
1. ปฏบตการดแลผปวยทบานรวมกบครอบครว
2. ประเมนผลการดแลผปวยรวมกบครอบครว
3. นดหมายการเยยมครงตอไป ตามผลการประเมนหลงการเยยม
หรอตามแผนทวางไว
ขนตอน/กจกรรมการดแลตอเนองทบาน
•หลงการเยยม
1. การบนทก และรายงานผลการดแลตามแผนและเปาหมายทวาง
ไว
2. การวางแผนจ าหนายและการประสานสงตอสถานบรการสขภาพ
ใกลบานเมอครอบครวสามารถจดการการดแลผปวยทบานได

บทบาทหนาทของพยาบาลเยยมบาน
• 1. ศกษาขอมลผปวยจากแบบสงปรกษาตอผปวยกบเกณฑการ
รบผปวย โทรศพทสอบถามขอมลเพมเตม
จากพยาบาลประจ าหอผปวย
• 2. แนะน าตนเอง สรางสมพนธภาพ และบอกวตถประสงคใน
การดแลผปวย แกผปวยและครอบครว
• 3. ชวยเหลอ เปนทปรกษาในการวางแผนดแลผปวยในรายท
พบปญหา หรอรายทมความซบซอนในการดแล

บทบาทหนาทของพยาบาลเยยมบาน
• 4. วางแผนและจดการการดแลรวมกบครอบครว โดยใชกระบวนการ
พยาบาลเพอใหเกดกระบวนการดแล โดยครอบครวในการ
ดแลผปวยตลอด 24 ช วโมง จนกระท งจ าหนายเมอครอบครวสามารถ
จดการการดแลไดดวยตนเอง
• 5. นดหมายการเยยมผปวยและครอบครว
• 6. วางแผนการจ าหนายผปวยรวมกบพยาบาลประจ าหอผปวย และ
ครอบครว เพอชวยใหครอบครวสามารถ ดแลผปวยไดอยางตอเนอง

บทบาทหนาทของพยาบาลเยยมบาน
• 7. ประสานงานทมสขภาพท งใน และนอกหนวยงาน เพอใหผปวย
ไดรบการดแลตอเนอง
• 8. บนทกการพยาบาลในแบบบนทกตามกระบวนการพยาบาลอยาง
ตอเนองทกข นตอน
• 9. ปรบเปลยนแผนการดแลใหสอดคลองกบปญหาและความตองการ
การดแลของผปวย
เอกสารทใชประกอบการปฏบต
• 1. แบบบนทกการรบผปวย (HC. 01)
•2. แบบบนทกการดแลทบาน (HC. 02)
•3. แบบสงตอเพอการดแลตอเนองทบาน
เกณฑในการเยยมผปวยเพอการดแลตอเนองทบาน
• 1. ผปวยทอยในเขตกรงเทพมหานครและปรมณฑล
• 2. ผปวยทตองพงพาอปกรณทางการแพทยทตองใชทกษะใน
การดแล เชน เครองดดเสมหะ ออกซเจนชนดแทงค หรอเปน
เครองผลตออกซเจน เปนตน
• ตาราง HC บนทก แผนทบ






เกณฑในการเยยมผปวยเพอการดแลตอเนองทบาน
• 3. ผปวยมความจ าเปนทตองดแลตอเนองทบาน มปญหาสขภาพทซบซอน
ไดแก ผปวย Palliative cares หรอ ผปวยมะเรงระยะสดทายท
ชวยเหลอตนเองไมได ผปวยทตองมการจดการเรองความเจบปวด (Pain
Management) ผปวยทมแผลมะเรง หรอแผลจากการท าหตถการทยงยากซงผดแลไมม นใจวาจะสามารถดแลผปวยทบานได
• 4. ผปวยทมปญหายงยากซบซอนในการดแลท งทางรางกาย อารมณ สงคม จต
วญญาณ

เกณฑในการเยยมผปวยเพอการดแลตอเนองทบาน
1.ในผปวยมะเรงระยะสดทายทมคะแนน PPS v2 0%-30%
การด าเนนของโรค 3 ระดบ โดยใชการประเมน PPS Score ไดแก
1.ระยะคงท คะแนน PPS v2 70%-100%
2.ระยะเปลยนผาน คะแนน PPS v2 40%-60%
3.ระยะวาระสดทาย คะแนน PPS v2 0%-30%
PLEA OF A
PATIENTWhen I come to you in pain
’This for comfort and not for gain
Should I need a narcotic
Lebel me not a drug addict
And when the pain is phenomenal
Don’t forget the non-steroidal
With the H2 blocker
or anti-ulcer
PLEA (ค าขอรอง)OF A
PATIENT
And if it’s time for the adjuvants
Do remember the antidepressants
Seek the cause of my pain
And ponder not if I feign
So when the pain fills me with dread(นากลว)
Please don’t say it is in my head
When it’s time for eternity
Allow me to leave with dignity