cannulation camp: basic needle cannulation training for dialysis staff
TRANSCRIPT
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 1/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Page 1
Deborah J. Brouwer, RN, CNN
Cannulation Camp:
Basic NeedleCannulation Trainingfor Dialysis StaffThis article reviews the basic skills needed by all dialysis staff to correctly cannulate an AV fistula or PTFE graft. Ways to identify the two types of accesses and to determine the direction of bloodflow are described. Access site determination and preparation, needle placement and direction, and various cannulation techniques are explained and supported by illustrations. Complications are examined, as are possible treatments and ways to prevent recurrences.
ow did you learn to cannulate adialysis access? Most practicingnephrology nurses and techni-
cians - myself included - had on-the-jobtraining. We observed our preceptorcannulate different patients who had eithergrafts or fistulas, and then were handedthe needles for our first cannulationattempt.
Very little nursing research and/orliterature is available for a preceptor to use
when teaching the art of needlecannulation. The purpose of this article isto provide current nephrology staff with abasic knowledge of needle cannulation,information which may then be passed onto new staff entering the nephrology field.
Step I: Identify the Typeof Access and Directionof BloodflowThe preferred dialysis access is thearteriovenous (AV) fistula. This is due to itshigh patency rate and the strong ability of
the puncture sites to heal. However, due tovascular limitations, only about 30% of alldialysis patients have working AV fistulas.
1
The most common AV fistula is oneconnecting the radial artery to the cephalicvein, created at the patient's wrist. A fistulacan also be created in the upper arm,connecting the brachial artery with theaxillary vein or another upper arm vein, allof which lead to the subclavian vein. A legfistula can also be created in patients withlimited access options.
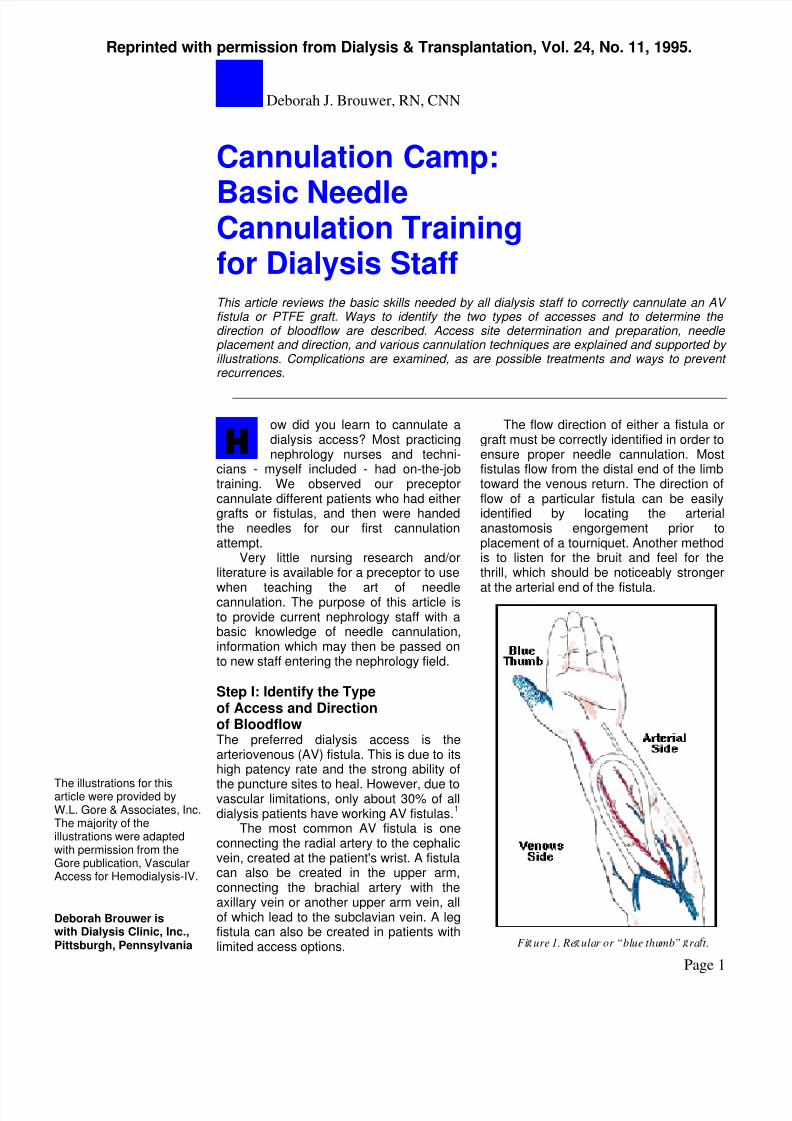
The flow direction of either a fistula orgraft must be correctly identified in order toensure proper needle cannulation. Mostfistulas flow from the distal end of the limbtoward the venous return. The direction offlow of a particular fistula can be easilyidentified by locating the arterialanastomosis engorgement prior toplacement of a tourniquet. Another methodis to listen for the bruit and feel for thethrill, which should be noticeably stronger
at the arterial end of the fistula.
H
The illustrations for thisarticle were provided byW.L. Gore & Associates, Inc.The majority of theillustrations were adaptedwith permission from the Gore publication, VascularAccess for Hemodialysis-IV.
Deborah Brouwer iswith Dialysis Clinic, Inc.,Pittsburgh, Pennsylvania Fi ure 1. Re ular or “blue thumb” ra t.
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 2/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
Page 2
Unfortunately, the flow directionwithin an implanted polytetrafluo-roethylene (PTFE) graft cannot beso easily identified. This is becausea graft can be placed in anylocation where an artery and vein
can be connected. The traditionalgraft sites - i.e., the lower arm (loopgraft) and upper arm (straight graft)- have now been supplemented bystraight or loop grafts in the leg,groin, abdomen, chest, or neck. Assuch, the direction of the bloodflowmay not be apparent by visualinspection alone.
Cooperation with the vascularsurgeon in obtaining a drawing ordescription of the bloodflowdirection is the best way to ensure
proper use of the access. In theabsence of such records, severaltechniques can be used todetermine bloodflow direction. Aspreviously mentioned, the mostcommonly used technique is tolisten to the bruit and feel for thethrill at both ends of the graft; theend with the stronger bruit and thrillis assumed to be the arterial limb.To confirm this assumption, themid-graft area can be lightlycompressed to impede the
bloodflow; again, the end with the
stronger bruit and thrill can beconsidered to be the arterial limb.
Next, the graft can becannulated with two needles andthe blood flashback observed.When the mid-graft area is
compressed, the arterial needleflashback should remain visible,while the venous needle flashbackshould greatly diminish ordisappear.
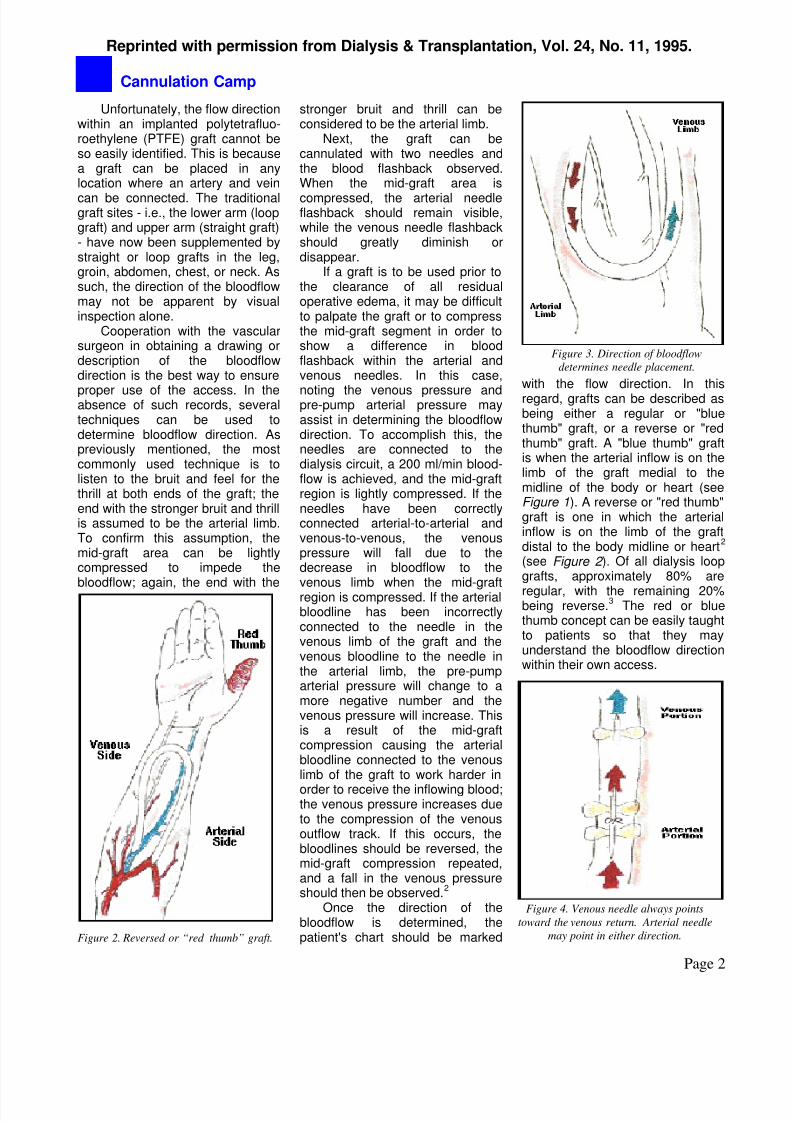
Figure 2. Reversed or “red thumb” graft.
Figure 3. Direction of bloodflow
determines needle placement.
Figure 4. Venous needle always points
toward the venous return. Arterial needle
may point in either direction.
If a graft is to be used prior tothe clearance of all residualoperative edema, it may be difficultto palpate the graft or to compressthe mid-graft segment in order toshow a difference in bloodflashback within the arterial andvenous needles. In this case,
noting the venous pressure andpre-pump arterial pressure mayassist in determining the bloodflowdirection. To accomplish this, theneedles are connected to thedialysis circuit, a 200 ml/min blood-flow is achieved, and the mid-graftregion is lightly compressed. If theneedles have been correctlyconnected arterial-to-arterial andvenous-to-venous, the venouspressure will fall due to thedecrease in bloodflow to the
venous limb when the mid-graftregion is compressed. If the arterialbloodline has been incorrectlyconnected to the needle in thevenous limb of the graft and thevenous bloodline to the needle inthe arterial limb, the pre-pumparterial pressure will change to amore negative number and thevenous pressure will increase. Thisis a result of the mid-graftcompression causing the arterialbloodline connected to the venouslimb of the graft to work harder in
order to receive the inflowing blood;the venous pressure increases dueto the compression of the venousoutflow track. If this occurs, thebloodlines should be reversed, themid-graft compression repeated,and a fall in the venous pressureshould then be observed.
2
Once the direction of thebloodflow is determined, thepatient's chart should be marked
with the flow direction. In thisregard, grafts can be described asbeing either a regular or "bluethumb" graft, or a reverse or "redthumb" graft. A "blue thumb" graftis when the arterial inflow is on thelimb of the graft medial to themidline of the body or heart (seeFigure 1). A reverse or "red thumb"graft is one in which the arterialinflow is on the limb of the graftdistal to the body midline or heart
2
(see Figure 2 ). Of all dialysis loopgrafts, approximately 80% are
regular, with the remaining 20%being reverse.
3The red or blue
thumb concept can be easily taughtto patients so that they mayunderstand the bloodflow directionwithin their own access.
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 3/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
Page 3
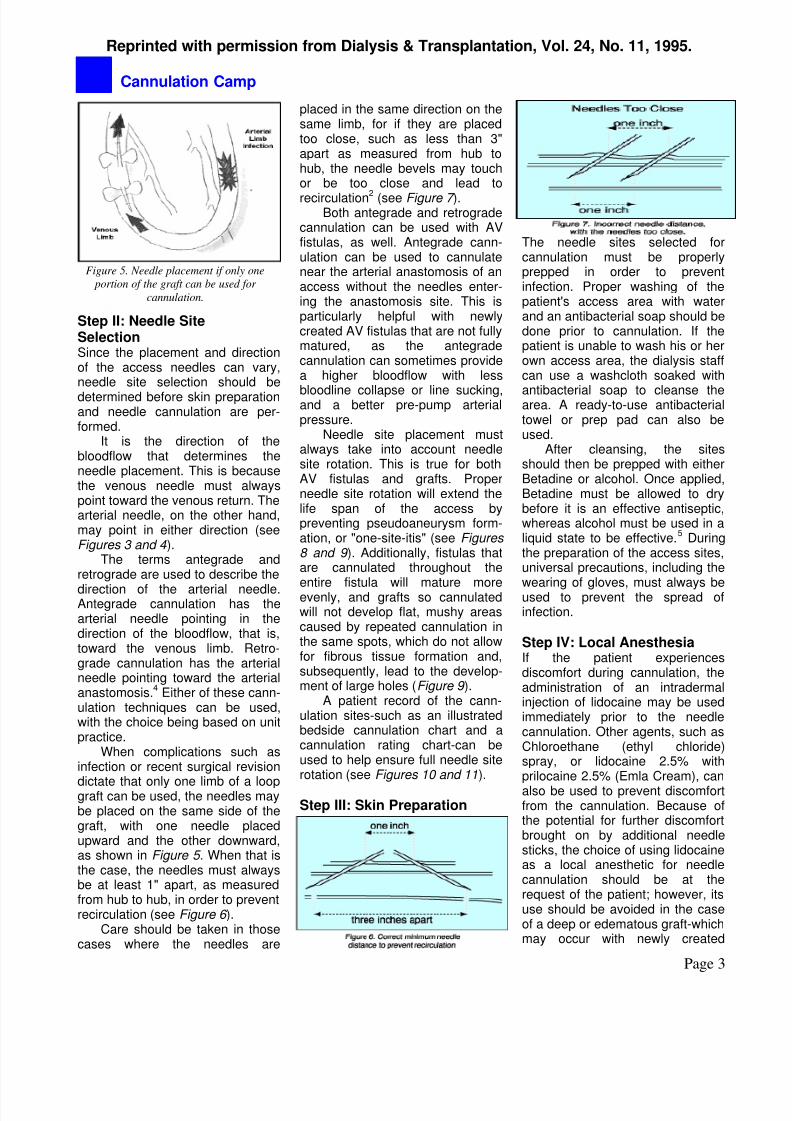
Figure 5. Needle placement if only one
portion of the graft can be used for
cannulation.
Step II: Needle SiteSelectionSince the placement and directionof the access needles can vary,needle site selection should be
determined before skin preparationand needle cannulation are per-formed.
It is the direction of thebloodflow that determines theneedle placement. This is becausethe venous needle must alwayspoint toward the venous return. Thearterial needle, on the other hand,may point in either direction (seeFigures 3 and 4 ).
The terms antegrade andretrograde are used to describe the
direction of the arterial needle.Antegrade cannulation has thearterial needle pointing in thedirection of the bloodflow, that is,toward the venous limb. Retro-grade cannulation has the arterialneedle pointing toward the arterialanastomosis.
4Either of these cann-
ulation techniques can be used,with the choice being based on unitpractice.
When complications such asinfection or recent surgical revision
dictate that only one limb of a loopgraft can be used, the needles maybe placed on the same side of thegraft, with one needle placedupward and the other downward,as shown in Figure 5 . When that isthe case, the needles must alwaysbe at least 1" apart, as measuredfrom hub to hub, in order to preventrecirculation (see Figure 6 ).
Care should be taken in thosecases where the needles are
placed in the same direction on thesame limb, for if they are placedtoo close, such as less than 3"apart as measured from hub tohub, the needle bevels may touchor be too close and lead to
recirculation2 (see Figure 7 ).Both antegrade and retrograde
cannulation can be used with AVfistulas, as well. Antegrade cann-ulation can be used to cannulatenear the arterial anastomosis of anaccess without the needles enter-ing the anastomosis site. This isparticularly helpful with newlycreated AV fistulas that are not fullymatured, as the antegradecannulation can sometimes providea higher bloodflow with less
bloodline collapse or line sucking,and a better pre-pump arterialpressure.
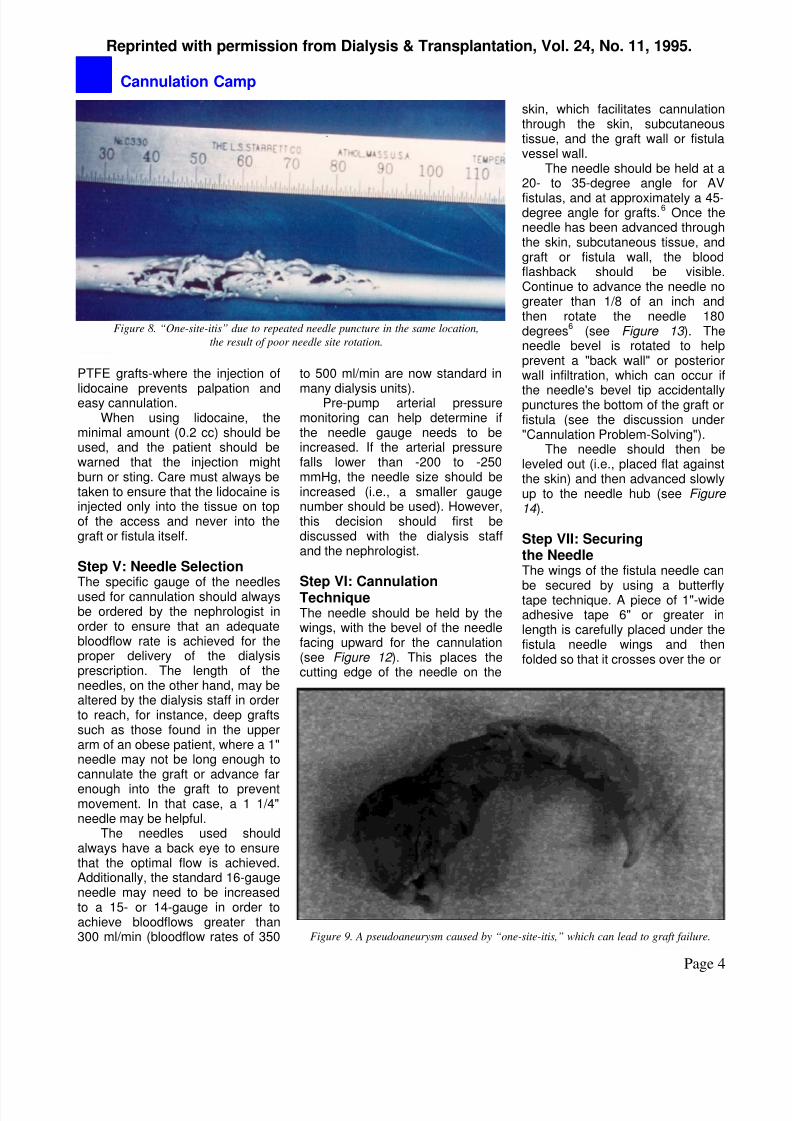
Needle site placement mustalways take into account needlesite rotation. This is true for bothAV fistulas and grafts. Properneedle site rotation will extend thelife span of the access bypreventing pseudoaneurysm form-ation, or "one-site-itis" (see Figures 8 and 9 ). Additionally, fistulas thatare cannulated throughout the
entire fistula will mature moreevenly, and grafts so cannulatedwill not develop flat, mushy areascaused by repeated cannulation inthe same spots, which do not allowfor fibrous tissue formation and,subsequently, lead to the develop-ment of large holes (Figure 9 ).
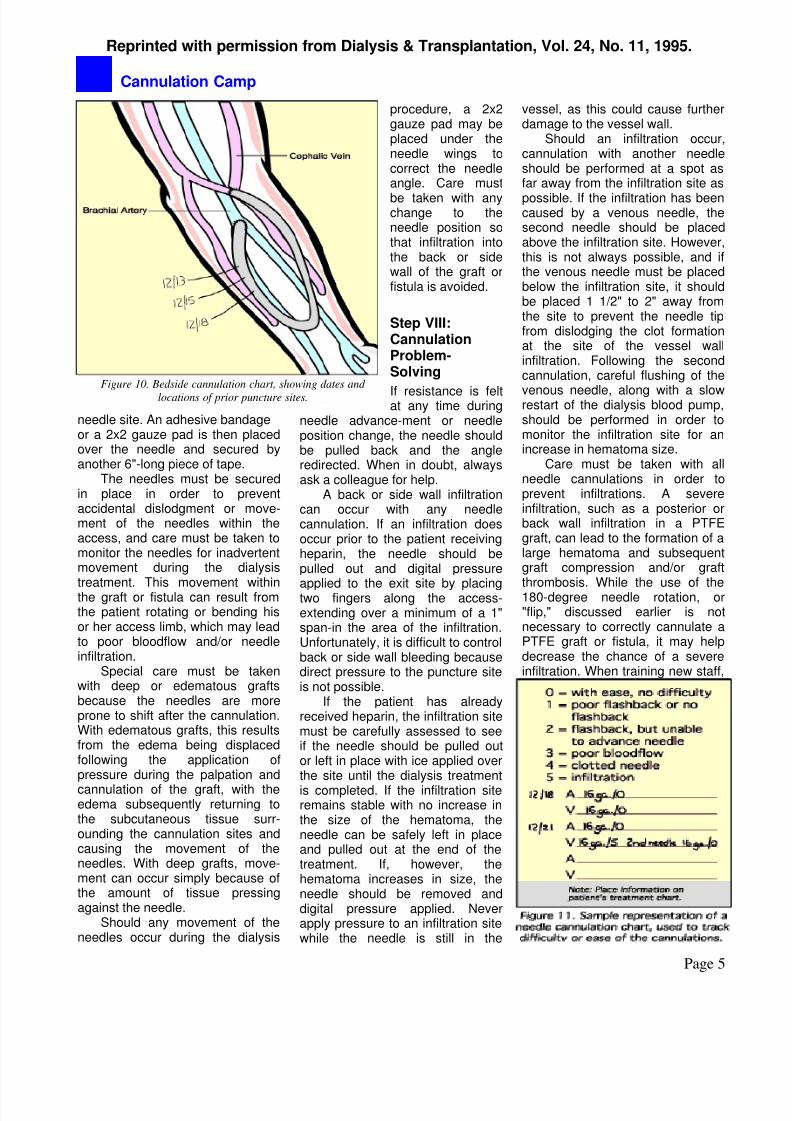
A patient record of the cann-ulation sites-such as an illustratedbedside cannulation chart and acannulation rating chart-can beused to help ensure full needle siterotation (see Figures 10 and 11).
Step III: Skin Preparation
The needle sites selected forcannulation must be properlyprepped in order to preventinfection. Proper washing of thepatient's access area with waterand an antibacterial soap should bedone prior to cannulation. If thepatient is unable to wash his or herown access area, the dialysis staffcan use a washcloth soaked with
antibacterial soap to cleanse thearea. A ready-to-use antibacterialtowel or prep pad can also beused.
After cleansing, the sitesshould then be prepped with eitherBetadine or alcohol. Once applied,Betadine must be allowed to drybefore it is an effective antiseptic,whereas alcohol must be used in aliquid state to be effective.
5During
the preparation of the access sites,universal precautions, including the
wearing of gloves, must always beused to prevent the spread ofinfection.
Step IV: Local AnesthesiaIf the patient experiencesdiscomfort during cannulation, theadministration of an intradermalinjection of lidocaine may be usedimmediately prior to the needlecannulation. Other agents, such asChloroethane (ethyl chloride)spray, or lidocaine 2.5% withprilocaine 2.5% (Emla Cream), canalso be used to prevent discomfortfrom the cannulation. Because ofthe potential for further discomfortbrought on by additional needlesticks, the choice of using lidocaineas a local anesthetic for needlecannulation should be at therequest of the patient; however, itsuse should be avoided in the caseof a deep or edematous graft-whichmay occur with newly created
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 4/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
Page 4
Figure 8. “One-site-itis” due to repeated needle puncture in the same location,
the result of poor needle site rotation.
PTFE grafts-where the injection of
lidocaine prevents palpation andeasy cannulation.When using lidocaine, the
minimal amount (0.2 cc) should beused, and the patient should bewarned that the injection mightburn or sting. Care must always betaken to ensure that the lidocaine isinjected only into the tissue on topof the access and never into thegraft or fistula itself.
Step V: Needle SelectionThe specific gauge of the needlesused for cannulation should alwaysbe ordered by the nephrologist inorder to ensure that an adequatebloodflow rate is achieved for theproper delivery of the dialysisprescription. The length of theneedles, on the other hand, may bealtered by the dialysis staff in orderto reach, for instance, deep graftssuch as those found in the upperarm of an obese patient, where a 1"needle may not be long enough tocannulate the graft or advance far
enough into the graft to preventmovement. In that case, a 1 1/4"needle may be helpful.
Figure 9. A pseudoaneurysm caused by “one-site-itis,” which can lead to graft failure.
The needles used shouldalways have a back eye to ensurethat the optimal flow is achieved.Additionally, the standard 16-gaugeneedle may need to be increasedto a 15- or 14-gauge in order toachieve bloodflows greater than300 ml/min (bloodflow rates of 350
to 500 ml/min are now standard in
many dialysis units).Pre-pump arterial pressuremonitoring can help determine ifthe needle gauge needs to beincreased. If the arterial pressurefalls lower than -200 to -250mmHg, the needle size should beincreased (i.e., a smaller gaugenumber should be used). However,this decision should first bediscussed with the dialysis staffand the nephrologist.
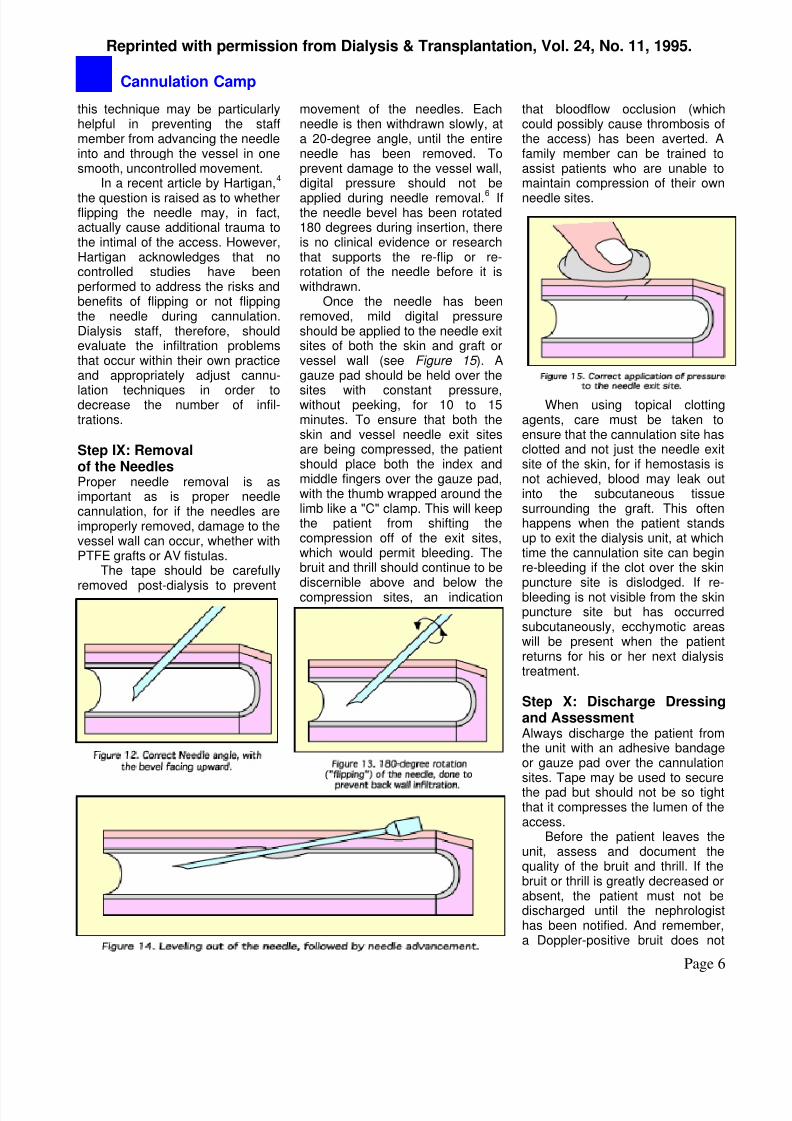
Step VI: CannulationTechniqueThe needle should be held by thewings, with the bevel of the needlefacing upward for the cannulation(see Figure 12 ). This places thecutting edge of the needle on the
skin, which facilitates cannulationthrough the skin, subcutaneoustissue, and the graft wall or fistulavessel wall.
The needle should be held at a20- to 35-degree angle for AV
fistulas, and at approximately a 45-degree angle for grafts.
6Once the
needle has been advanced throughthe skin, subcutaneous tissue, andgraft or fistula wall, the bloodflashback should be visible.Continue to advance the needle nogreater than 1/8 of an inch andthen rotate the needle 180degrees
6(see Figure 13 ). The
needle bevel is rotated to helpprevent a "back wall" or posteriorwall infiltration, which can occur if
the needle's bevel tip accidentallypunctures the bottom of the graft orfistula (see the discussion under"Cannulation Problem-Solving").
The needle should then beleveled out (i.e., placed flat againstthe skin) and then advanced slowlyup to the needle hub (see Figure 14 ).
Step VII: Securingthe NeedleThe wings of the fistula needle can
be secured by using a butterflytape technique. A piece of 1"-wideadhesive tape 6" or greater inlength is carefully placed under thefistula needle wings and thenfolded so that it crosses over the or
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 5/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
Page 5
Figure 10. Bedside cannulation chart, showing dates and
locations of prior puncture sites.
needle site. An adhesive bandageor a 2x2 gauze pad is then placedover the needle and secured byanother 6"-long piece of tape.
The needles must be securedin place in order to preventaccidental dislodgment or move-ment of the needles within theaccess, and care must be taken tomonitor the needles for inadvertentmovement during the dialysis
treatment. This movement withinthe graft or fistula can result fromthe patient rotating or bending hisor her access limb, which may leadto poor bloodflow and/or needleinfiltration.
Special care must be takenwith deep or edematous graftsbecause the needles are moreprone to shift after the cannulation.With edematous grafts, this resultsfrom the edema being displacedfollowing the application ofpressure during the palpation and
cannulation of the graft, with theedema subsequently returning tothe subcutaneous tissue surr-ounding the cannulation sites andcausing the movement of theneedles. With deep grafts, move-ment can occur simply because ofthe amount of tissue pressingagainst the needle.
Should any movement of theneedles occur during the dialysis
procedure, a 2x2gauze pad may beplaced under theneedle wings tocorrect the needleangle. Care must
be taken with anychange to theneedle position sothat infiltration intothe back or sidewall of the graft orfistula is avoided.
Step VIII:CannulationProblem-Solving
If resistance is feltat any time during
needle advance-ment or needleposition change, the needle shouldbe pulled back and the angleredirected. When in doubt, alwaysask a colleague for help.
A back or side wall infiltrationcan occur with any needlecannulation. If an infiltration doesoccur prior to the patient receivingheparin, the needle should bepulled out and digital pressure
applied to the exit site by placingtwo fingers along the access-extending over a minimum of a 1"span-in the area of the infiltration.Unfortunately, it is difficult to controlback or side wall bleeding becausedirect pressure to the puncture siteis not possible.
If the patient has alreadyreceived heparin, the infiltration sitemust be carefully assessed to seeif the needle should be pulled outor left in place with ice applied overthe site until the dialysis treatment
is completed. If the infiltration siteremains stable with no increase inthe size of the hematoma, theneedle can be safely left in placeand pulled out at the end of thetreatment. If, however, thehematoma increases in size, theneedle should be removed anddigital pressure applied. Neverapply pressure to an infiltration sitewhile the needle is still in the
vessel, as this could cause furtherdamage to the vessel wall.
Should an infiltration occur,cannulation with another needleshould be performed at a spot asfar away from the infiltration site as
possible. If the infiltration has beencaused by a venous needle, thesecond needle should be placedabove the infiltration site. However,this is not always possible, and ifthe venous needle must be placedbelow the infiltration site, it shouldbe placed 1 1/2" to 2" away fromthe site to prevent the needle tipfrom dislodging the clot formationat the site of the vessel wallinfiltration. Following the secondcannulation, careful flushing of the
venous needle, along with a slowrestart of the dialysis blood pump,should be performed in order tomonitor the infiltration site for anincrease in hematoma size.
Care must be taken with allneedle cannulations in order toprevent infiltrations. A severeinfiltration, such as a posterior orback wall infiltration in a PTFEgraft, can lead to the formation of alarge hematoma and subsequentgraft compression and/or graft
thrombosis. While the use of the180-degree needle rotation, or"flip," discussed earlier is notnecessary to correctly cannulate aPTFE graft or fistula, it may helpdecrease the chance of a severeinfiltration. When training new staff,
8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 6/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
this technique may be particularlyhelpful in preventing the staffmember from advancing the needleinto and through the vessel in onesmooth, uncontrolled movement.
In a recent article by Hartigan,4
the question is raised as to whetherflipping the needle may, in fact,actually cause additional trauma tothe intimal of the access. However,Hartigan acknowledges that nocontrolled studies have beenperformed to address the risks andbenefits of flipping or not flippingthe needle during cannulation.Dialysis staff, therefore, shouldevaluate the infiltration problemsthat occur within their own practiceand appropriately adjust cannu-
lation techniques in order todecrease the number of infil-trations.
Page 6
Step IX: Removalof the NeedlesProper needle removal is asimportant as is proper needlecannulation, for if the needles areimproperly removed, damage to thevessel wall can occur, whether withPTFE grafts or AV fistulas.
The tape should be carefully
removed post-dialysis to prevent
movement of the needles. Eachneedle is then withdrawn slowly, ata 20-degree angle, until the entireneedle has been removed. Toprevent damage to the vessel wall,digital pressure should not be
applied during needle removal.6 Ifthe needle bevel has been rotated180 degrees during insertion, thereis no clinical evidence or researchthat supports the re-flip or re-rotation of the needle before it iswithdrawn.
Once the needle has beenremoved, mild digital pressureshould be applied to the needle exitsites of both the skin and graft orvessel wall (see Figure 15 ). Agauze pad should be held over the
sites with constant pressure,without peeking, for 10 to 15minutes. To ensure that both theskin and vessel needle exit sitesare being compressed, the patientshould place both the index andmiddle fingers over the gauze pad,with the thumb wrapped around thelimb like a "C" clamp. This will keepthe patient from shifting thecompression off of the exit sites,which would permit bleeding. Thebruit and thrill should continue to be
discernible above and below thecompression sites, an indication
that bloodflow occlusion (whichcould possibly cause thrombosis ofthe access) has been averted. Afamily member can be trained toassist patients who are unable tomaintain compression of their own
needle sites.
When using topical clottingagents, care must be taken toensure that the cannulation site hasclotted and not just the needle exitsite of the skin, for if hemostasis isnot achieved, blood may leak outinto the subcutaneous tissuesurrounding the graft. This oftenhappens when the patient standsup to exit the dialysis unit, at whichtime the cannulation site can beginre-bleeding if the clot over the skin
puncture site is dislodged. If re-bleeding is not visible from the skinpuncture site but has occurredsubcutaneously, ecchymotic areaswill be present when the patientreturns for his or her next dialysistreatment.
Step X: Discharge Dressingand AssessmentAlways discharge the patient fromthe unit with an adhesive bandageor gauze pad over the cannulationsites. Tape may be used to securethe pad but should not be so tightthat it compresses the lumen of theaccess.
Before the patient leaves theunit, assess and document thequality of the bruit and thrill. If thebruit or thrill is greatly decreased orabsent, the patient must not bedischarged until the nephrologisthas been notified. And remember,a Doppler-positive bruit does not

8/14/2019 cannulation camp: basic needle cannulation training for dialysis staff
http://slidepdf.com/reader/full/cannulation-camp-basic-needle-cannulation-training-for-dialysis-staff 7/7
Reprinted with permission from Dialysis & Transplantation, Vol. 24, No. 11, 1995.
Cannulation Camp
Page 7
always equate with a positive bruitand thrill.
CONCLUSIONNursing research is needed tobetter evaluate all cannulation
procedures. Our goal should be tosafely cannulate any accesswithout causing unnecessarydamage to the patient's lifeline. Assuch, the basics of needlecannulation must be openlydiscussed among all patient carestaff members. We must worktoward having all dialysis staffmembers understand and masterthe basics of vascular access.
The fundamental principlesof vascular access should be used
to help train future dialysis staffmembers in order to improve thequality of care that future dialysispatients will receive. We mustcontinue to gain knowledge in thisimportant area through nursingresearch and education.
.
References
1. Fan PY, Schwab S. Vascular access:Concepts for the 1990s. J Am Soc Nephrol3:1, 1992.2. Brouwer D. Hemodialysis: A NursingPerspective. In: Vascular Access forHemodialysis - IV (a W.L. Gore publication).Henry M, Ferguson R (eds.). Chicago, IL:W.L. Gore & Associates, Inc., and PreceptPress, 1992.3. Raja RM. Vascular access forhemodialysis. In: Handbook of Dialysis.Daugirdas JT, Ing TS (eds.). Boston, MA:Little, Brown & Co., 1994.4. Hartigan M. Vascular access andnephrology nursing practice: Existing viewsand rationales for change. Advances inRenal Replacement Therapy 1(2):156-157,
1994.5. Perkins JJ. Principles and Methods ofSterilization in Health Sciences (2nd Ed.).Springfield, IL: Charles C. ThomasPublishers. pp. 337-338, 1969.6. Lancaster LE. Core Curriculum ofNephrology Nursing. Pitman, NJ: AmericanNephrology Nurses' Association, pp. 266,272, 1995