capecitabine/taxane combination therapy: evolving clinical utility in breast cancer
TRANSCRIPT
IntroductionBreast cancer is the second most frequently diagnosed can-
cer in women, with approximately 213,000 new cases annually, and is responsible for > 40,000 deaths each year.1 Detecting breast cancer at an early stage is critical to success; the 5-year survival rate is 97% when the disease is localized but only 23% when distant metastases are present. Chemotherapy has an important role in the metastatic, adjuvant, and neoadjuvant settings to prolong survival, prevent recurrence, and enable more effective surgical excision of tumors.
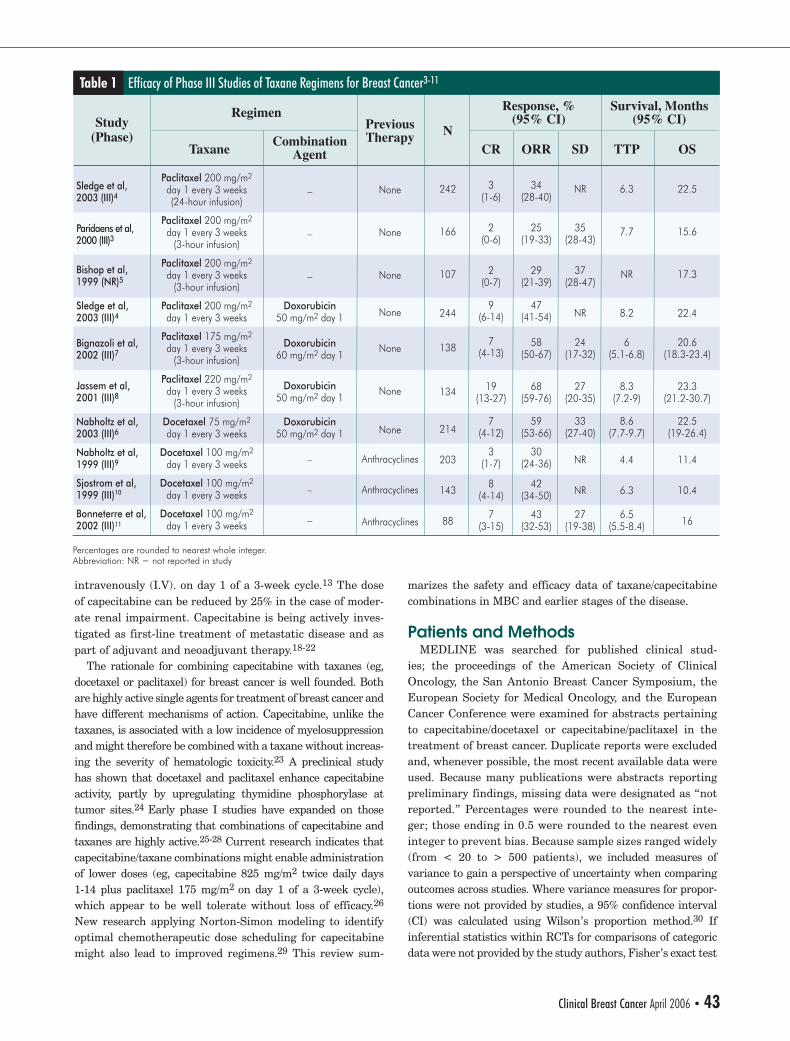
The taxanes docetaxel and paclitaxel have emerged as key agents in the treatment of metastatic and early-stage breast cancer.2 Taxanes enhance microtubule formation and inhibit depolymerization of tubulin, thereby blocking the G2/M phase of the cell cycle. Taxanes are highly active, whether used for first- or second-line metastatic breast can-cer (MBC), when used as a single agent or as part of com-bination therapy. Efficacy (response and survival) results from relevant randomized controlled trials (RCTs) of taxane therapies for metastatic disease are presented in Table 1.3-11 Taxanes are also often associated with moderate to severe
adverse events, including neutropenia, febrile neutropenia, peripheral neuropathy, alopecia, and stomatitis.
Another emerging key agent in the treatment of breast cancer is capecitabine, an orally administered fluoropy-rimidine carbamate that mimics continuous infusion of 5-fluorouracil (5-FU).12 Initially absorbed in the gastroin-testinal tract with excellent oral bioavailability, capecitabine is metabolized (hydrolyzed) in the liver by the enzyme carboxylesterase to 5'-deoxy-5-fluorocytidine, which is then converted by the enzyme cytidine deaminase (also commonly found in tumor tissue) to 5'-deoxy-5-fluorouridine, which in turn, is converted by the enzyme thymidine phosphorylase (found in tumor and normal tissue) to 5-FU.13 Human studies in patients with colorectal cancer have shown that capecitabine therapy leads to substantially greater levels of 5-FU in tumor tissue than in normal colon tissue.14,15
Capecitabine is currently approved by the US Food and Drug Administration (FDA) for the treatment of MBC as monotherapy for patients with disease resistant to paclitax-el and anthracyclines or for those resistant to paclitaxel and for whom further anthracycline therapy is contraindicated; it is also approved as combination therapy with docetaxel for patients after failure of previous anthracycline-con-taining chemotherapy.13 The FDA-approved schedule and dosing of capecitabine for breast cancer are intermittent, ie, at 1250 mg/m2 twice daily orally for 2 weeks followed by a 1-week rest period, whether administered as a single agent16,17 or in combination with docetaxel at 75 mg/m2
Capecitabine/Taxane Combination Therapy: Evolving Clinical Utility in Breast Cancer
Capecitabine is approved as a single agent and in combination with docetaxel for the treatment of metastatic breast cancer. Preclinical and clinical research suggests that the activity of capecitabine is enhanced in combina-tion with taxanes, and several biochemical mechanisms of synergy have been described. Recent data suggest that novel doses and schedules of capecitabine can improve safety without compromising efficacy. More than 50 publications and abstracts describing capecitabine/taxane combination therapy studies were reviewed to evaluate the available data on efficacy, safety, and quality of life for patients with breast cancer. Several ongo-ing randomized adjuvant and neoadjuvant clinical trials are assessing the clinical utility of capecitabine/taxane combinations in early-stage and locally advanced breast cancer.
Clinical Breast Cancer, Vol. 7, No. 1, 42-50, 2006Key words: Docetaxel, Hand-foot syndrome, Neutropenia, Paclitaxel
review
Abstract
comprehensive
Electronic forwarding or copying is a violation of US and International Copyright Laws.Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by CIG Media Group, LP,ISSN #1526-8209, provided the appropriate fee is paid directly to Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923 USA 978-750-8400.
Joyce A. O’Shaughnessy, Joanne L. Blum
Submitted: Jun 9, 2005; Revised: Aug 29, 2005; Accepted: Aug 29, 2005
Address for correspondence: Joanne L. Blum, MD, PhD, Director of Hereditary Cancer Risk Program and Research Site Director, Baylor Charles A. Sammons Cancer Center, 3535 Worth St, Suite 600, Dallas, TX 75246Fax: 214-370-1060; e-mail: [email protected]
Baylor Charles A. Sammons Cancer Center, Dallas, TX
42 • Clinical Breast Cancer April 2006
O'Shaughnessy1 CR1.indd 2 5/4/06 11:53:03 AM
intravenously (I.V). on day 1 of a 3-week cycle.13 The dose of capecitabine can be reduced by 25% in the case of moder-ate renal impairment. Capecitabine is being actively inves-tigated as first-line treatment of metastatic disease and as part of adjuvant and neoadjuvant therapy.18-22
The rationale for combining capecitabine with taxanes (eg, docetaxel or paclitaxel) for breast cancer is well founded. Both are highly active single agents for treatment of breast cancer and have different mechanisms of action. Capecitabine, unlike the taxanes, is associated with a low incidence of myelosuppression and might therefore be combined with a taxane without increas-ing the severity of hematologic toxicity.23 A preclinical study has shown that docetaxel and paclitaxel enhance capecitabine activity, partly by upregulating thymidine phosphorylase at tumor sites.24 Early phase I studies have expanded on those findings, demonstrating that combinations of capecitabine and taxanes are highly active.25-28 Current research indicates that capecitabine/taxane combinations might enable administration of lower doses (eg, capecitabine 825 mg/m2 twice daily days 1-14 plus paclitaxel 175 mg/m2 on day 1 of a 3-week cycle), which appear to be well tolerate without loss of efficacy.26 New research applying Norton-Simon modeling to identify optimal chemotherapeutic dose scheduling for capecitabine might also lead to improved regimens.29 This review sum-
marizes the safety and efficacy data of taxane/capecitabine combinations in MBC and earlier stages of the disease.
Patients and MethodsMEDLINE was searched for published clinical stud-
ies; the proceedings of the American Society of Clinical Oncology, the San Antonio Breast Cancer Symposium, the European Society for Medical Oncology, and the European Cancer Conference were examined for abstracts pertaining to capecitabine/docetaxel or capecitabine/paclitaxel in the treatment of breast cancer. Duplicate reports were excluded and, whenever possible, the most recent available data were used. Because many publications were abstracts reporting preliminary findings, missing data were designated as “not reported.” Percentages were rounded to the nearest inte-ger; those ending in 0.5 were rounded to the nearest even integer to prevent bias. Because sample sizes ranged widely (from < 20 to > 500 patients), we included measures of variance to gain a perspective of uncertainty when comparing outcomes across studies. Where variance measures for propor-tions were not provided by studies, a 95% confidence interval (CI) was calculated using Wilson’s proportion method.30 If inferential statistics within RCTs for comparisons of categoric data were not provided by the study authors, Fisher’s exact test
Efficacy of Phase III Studies of Taxane Regimens for Breast Cancer3-11Table 1
Study(Phase)
Sledge et al,2003 (III)4
Paridaens et al,2000 (III)3
Bishop et al,1999 (NR)5
Sledge et al,2003 (III)4
Bignazoli et al,2002 (III)7
Jassem et al,2001 (III)8
Nabholtz et al,2003 (III)6
Nabholtz et al,1999 (III)9
Sjostrom et al,1999 (III)10
Bonneterre et al,2002 (III)11
Taxane
Regimen Response, %(95% CI)
Survival, Months(95% CI)
Paclitaxel 200 mg/m2
day 1 every 3 weeks(24-hour infusion)
Paclitaxel 200 mg/m2
day 1 every 3 weeks(3-hour infusion)
Paclitaxel 200 mg/m2
day 1 every 3 weeks(3-hour infusion)
Paclitaxel 200 mg/m2
day 1 every 3 weeks
Paclitaxel 175 mg/m2
day 1 every 3 weeks(3-hour infusion)
Paclitaxel 220 mg/m2
day 1 every 3 weeks(3-hour infusion)
Docetaxel 75 mg/m2
day 1 every 3 weeks
Docetaxel 100 mg/m2
day 1 every 3 weeks
Docetaxel 100 mg/m2
day 1 every 3 weeks
Docetaxel 100 mg/m2
day 1 every 3 weeks
CombinationAgent
–
–
–
Doxorubicin50 mg/m2 day 1
Doxorubicin60 mg/m2 day 1
Doxorubicin50 mg/m2 day 1
Doxorubicin50 mg/m2 day 1
–
–
–
PreviousTherapy
None
None
None
None
None
None
None
Anthracyclines
Anthracyclines
Anthracyclines
Percentages are rounded to nearest whole integer.Abbreviation: NR = not reported in study
N
242
166
107
244
138
134
214
203
143
88
CR
3(1-6)
2(0-6)
2(0-7)
9(6-14)
7(4-13)
19(13-27)
7(4-12)
3(1-7)
8(4-14)
7(3-15)
ORR
34(28-40)
25(19-33)
29(21-39)
47(41-54)
58(50-67)
68(59-76)
59(53-66)
30(24-36)
42(34-50)
43(32-53)
SD
NR
35(28-43)
37(28-47)
NR
24(17-32)
27(20-35)
33(27-40)
NR
NR
27(19-38)
TTP
6.3
7.7
NR
8.2
6(5.1-6.8)
8.3(7.2-9)
8.6(7.7-9.7)
4.4
6.3
6.5(5.5-8.4)
OS
22.5
15.6
17.3
22.4
20.6(18.3-23.4)
23.3(21.2-30.7)
22.5(19-26.4)
11.4
10.4
16
Clinical Breast Cancer April 2006 • 43
O'Shaughnessy1 CR1.indd 3 5/4/06 11:53:04 AM
Capecitabine/Taxane Combinations for Breast Cancer
or a 2-sample Z-test for comparing 2 proportions was employed. Significance was set at 5% (α = 0.05) for 2-tailed testing.
Results and DiscussionPhase II Studies
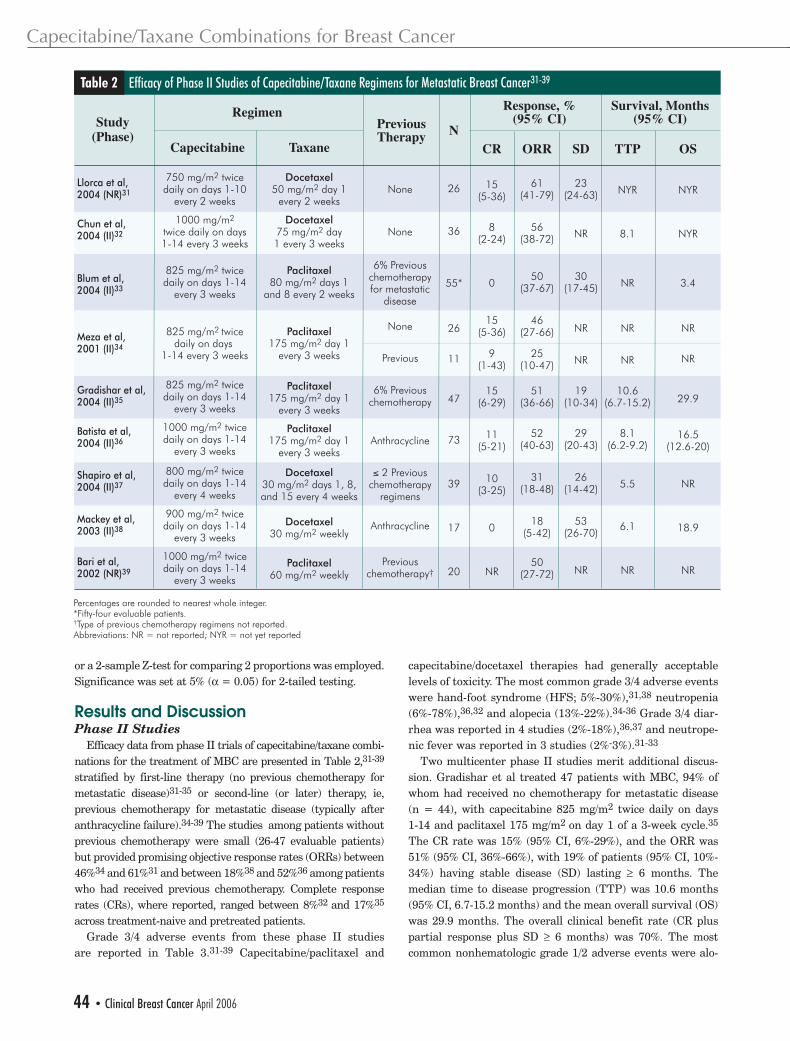
Efficacy data from phase II trials of capecitabine/taxane combi-nations for the treatment of MBC are presented in Table 2,31-39 stratified by first-line therapy (no previous chemotherapy for metastatic disease)31-35 or second-line (or later) therapy, ie, previous chemotherapy for metastatic disease (typically after anthracycline failure).34-39 The studies among patients without previous chemotherapy were small (26-47 evaluable patients) but provided promising objective response rates (ORRs) between 46%34 and 61%31 and between 18%38 and 52%36 among patients who had received previous chemotherapy. Complete response rates (CRs), where reported, ranged between 8%32 and 17%35 across treatment-naive and pretreated patients.
Grade 3/4 adverse events from these phase II studies are reported in Table 3.31-39 Capecitabine/paclitaxel and
capecitabine/docetaxel therapies had generally acceptable levels of toxicity. The most common grade 3/4 adverse events were hand-foot syndrome (HFS; 5%-30%),31,38 neutropenia (6%-78%),36,32 and alopecia (13%-22%).34-36 Grade 3/4 diar-rhea was reported in 4 studies (2%-18%),36,37 and neutrope-nic fever was reported in 3 studies (2%-3%).31-33
Two multicenter phase II studies merit additional discus-sion. Gradishar et al treated 47 patients with MBC, 94% of whom had received no chemotherapy for metastatic disease (n = 44), with capecitabine 825 mg/m2 twice daily on days 1-14 and paclitaxel 175 mg/m2 on day 1 of a 3-week cycle.35 The CR rate was 15% (95% CI, 6%-29%), and the ORR was 51% (95% CI, 36%-66%), with 19% of patients (95% CI, 10%-34%) having stable disease (SD) lasting ≥ 6 months. The median time to disease progression (TTP) was 10.6 months (95% CI, 6.7-15.2 months) and the mean overall survival (OS) was 29.9 months. The overall clinical benefit rate (CR plus partial response plus SD ≥ 6 months) was 70%. The most common nonhematologic grade 1/2 adverse events were alo-
Efficacy of Phase II Studies of Capecitabine/Taxane Regimens for Metastatic Breast Cancer31-39Table 2
Study(Phase)
Llorca et al,2004 (NR)31
Chun et al,2004 (II)32
Blum et al,2004 (II)33
Meza et al,2001 (II)34
Gradishar et al,2004 (II)35
Batista et al,2004 (II)36
Shapiro et al,2004 (II)37
Mackey et al,2003 (II)38
Bari et al,2002 (NR)39
Capecitabine
Regimen Response, %(95% CI)
Survival, Months(95% CI)
750 mg/m2 twicedaily on days 1-10
every 2 weeks
1000 mg/m2
twice daily on days1-14 every 3 weeks
825 mg/m2 twicedaily on days 1-14
every 3 weeks
825 mg/m2 twicedaily on days
1-14 every 3 weeks
825 mg/m2 twicedaily on days 1-14
every 3 weeks
1000 mg/m2 twicedaily on days 1-14
every 3 weeks
800 mg/m2 twicedaily on days 1-14
every 4 weeks
900 mg/m2 twicedaily on days 1-14
every 3 weeks
1000 mg/m2 twicedaily on days 1-14
every 3 weeks
Taxane
Docetaxel50 mg/m2 day 1
every 2 weeks
Docetaxel75 mg/m2 day1 every 3 weeks
Paclitaxel80 mg/m2 days 1
and 8 every 2 weeks
Paclitaxel175 mg/m2 day 1
every 3 weeks
Paclitaxel175 mg/m2 day 1
every 3 weeks
Paclitaxel175 mg/m2 day 1
every 3 weeks
Docetaxel30 mg/m2 days 1, 8,and 15 every 4 weeks
Docetaxel30 mg/m2 weekly
Paclitaxel60 mg/m2 weekly
PreviousTherapy
None
None
6% Previouschemotherapyfor metastatic
disease
None
Previous
6% Previouschemotherapy
Anthracycline
≤ 2 Previouschemotherapy
regimens
Anthracycline
Previouschemotherapy†
Percentages are rounded to nearest whole integer.*Fifty-four evaluable patients. †Type of previous chemotherapy regimens not reported.Abbreviations: NR = not reported; NYR = not yet reported
N
26
36
55*
26
11
47
73
39
17
20
CR
15(5-36)
8(2-24)
0
15(5-36)
9(1-43)
15(6-29)
11(5-21)
10(3-25)
0
NR
ORR
61(41-79)
56(38-72)
50(37-67)
46(27-66)
25(10-47)
51(36-66)
52(40-63)
31(18-48)
18(5-42)
50(27-72)
SD
23(24-63)
NR
30(17-45)
NR
NR
19(10-34)
29(20-43)
26(14-42)
53(26-70)
NR
TTP
NYR
8.1
NR
NR
NR
10.6(6.7-15.2)
8.1(6.2-9.2)
5.5
6.1
NR
OS
NYR
NYR
3.4
NR
NR
29.9
16.5(12.6-20)
NR
18.9
NR
44 • Clinical Breast Cancer April 2006
O'Shaughnessy1 CR1.indd 4 5/4/06 11:53:04 AM
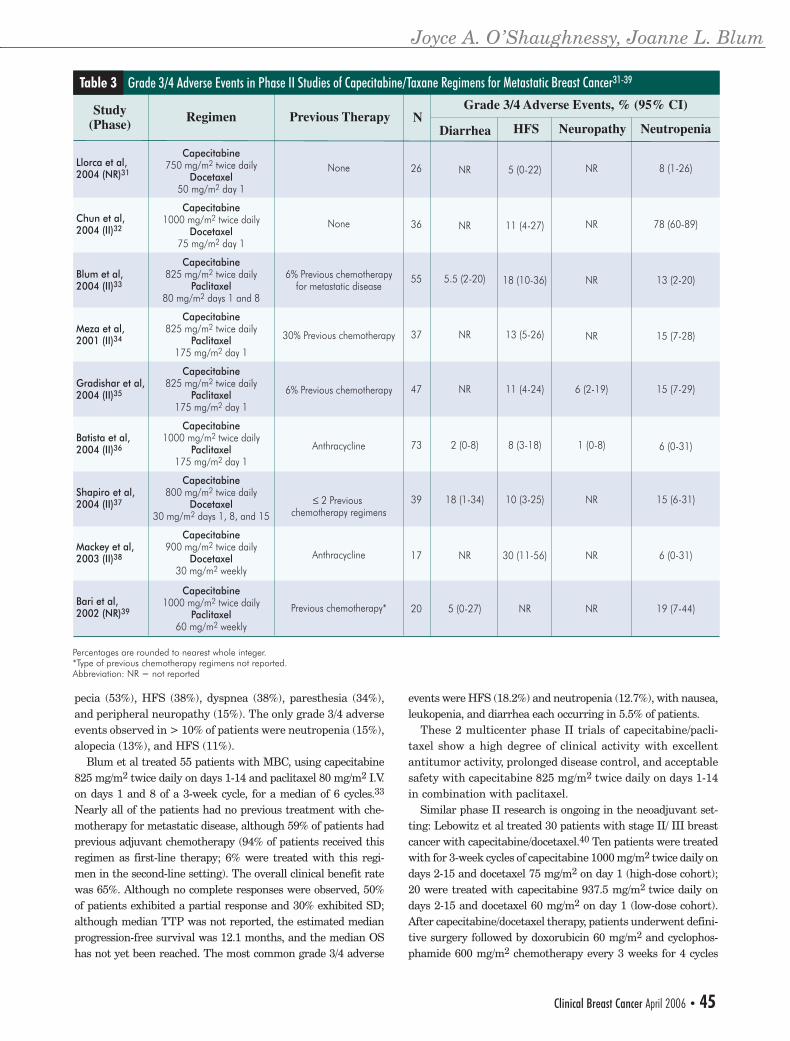
pecia (53%), HFS (38%), dyspnea (38%), paresthesia (34%), and peripheral neuropathy (15%). The only grade 3/4 adverse events observed in > 10% of patients were neutropenia (15%), alopecia (13%), and HFS (11%).
Blum et al treated 55 patients with MBC, using capecitabine 825 mg/m2 twice daily on days 1-14 and paclitaxel 80 mg/m2 I.V. on days 1 and 8 of a 3-week cycle, for a median of 6 cycles.33
Nearly all of the patients had no previous treatment with che-motherapy for metastatic disease, although 59% of patients had previous adjuvant chemotherapy (94% of patients received this regimen as first-line therapy; 6% were treated with this regi-men in the second-line setting). The overall clinical benefit rate was 65%. Although no complete responses were observed, 50% of patients exhibited a partial response and 30% exhibited SD; although median TTP was not reported, the estimated median progression-free survival was 12.1 months, and the median OS has not yet been reached. The most common grade 3/4 adverse
events were HFS (18.2%) and neutropenia (12.7%), with nausea, leukopenia, and diarrhea each occurring in 5.5% of patients.
These 2 multicenter phase II trials of capecitabine/pacli-taxel show a high degree of clinical activity with excellent antitumor activity, prolonged disease control, and acceptable safety with capecitabine 825 mg/m2 twice daily on days 1-14 in combination with paclitaxel.
Similar phase II research is ongoing in the neoadjuvant set-ting: Lebowitz et al treated 30 patients with stage II/ III breast cancer with capecitabine/docetaxel.40 Ten patients were treated with for 3-week cycles of capecitabine 1000 mg/m2 twice daily on days 2-15 and docetaxel 75 mg/m2 on day 1 (high-dose cohort); 20 were treated with capecitabine 937.5 mg/m2 twice daily on days 2-15 and docetaxel 60 mg/m2 on day 1 (low-dose cohort). After capecitabine/docetaxel therapy, patients underwent defini-tive surgery followed by doxorubicin 60 mg/m2 and cyclophos-phamide 600 mg/m2 chemotherapy every 3 weeks for 4 cycles
Grade 3/4 Adverse Events in Phase II Studies of Capecitabine/Taxane Regimens for Metastatic Breast Cancer31-39Table 3
Study(Phase)
Llorca et al,2004 (NR)31
Chun et al,2004 (II)32
Blum et al,2004 (II)33
Meza et al,2001 (II)34
Gradishar et al,2004 (II)35
Batista et al,2004 (II)36
Shapiro et al,2004 (II)37
Mackey et al,2003 (II)38
Bari et al,2002 (NR)39
RegimenGrade 3/4 Adverse Events, % (95% CI)
Capecitabine750 mg/m2 twice daily
Docetaxel50 mg/m2 day 1
Capecitabine1000 mg/m2 twice daily
Docetaxel75 mg/m2 day 1
Capecitabine825 mg/m2 twice daily
Paclitaxel80 mg/m2 days 1 and 8
Capecitabine825 mg/m2 twice daily
Paclitaxel175 mg/m2 day 1
Capecitabine825 mg/m2 twice daily
Paclitaxel175 mg/m2 day 1
Capecitabine1000 mg/m2 twice daily
Paclitaxel175 mg/m2 day 1
Capecitabine800 mg/m2 twice daily
Docetaxel30 mg/m2 days 1, 8, and 15
Capecitabine900 mg/m2 twice daily
Docetaxel30 mg/m2 weekly
Capecitabine1000 mg/m2 twice daily
Paclitaxel60 mg/m2 weekly
Previous Therapy
None
None
6% Previous chemotherapyfor metastatic disease
30% Previous chemotherapy
6% Previous chemotherapy
Anthracycline
≤ 2 Previous chemotherapy regimens
Anthracycline
Previous chemotherapy*
Percentages are rounded to nearest whole integer.*Type of previous chemotherapy regimens not reported. Abbreviation: NR = not reported
N
26
36
55
37
47
73
39
17
20
Diarrhea
NR
NR
5.5 (2-20)
NR
NR
2 (0-8)
18 (1-34)
NR
5 (0-27)
HFS
5 (0-22)
11 (4-27)
18 (10-36)
13 (5-26)
11 (4-24)
8 (3-18)
10 (3-25)
30 (11-56)
NR
Neuropathy
NR
NR
NR
NR
6 (2-19)
1 (0-8)
NR
NR
NR
Neutropenia
8 (1-26)
78 (60-89)
13 (2-20)
15 (7-28)
15 (7-29)
6 (0-31)
15 (6-31)
6 (0-31)
19 (7-44)
Joyce A. O’Shaughnessy, Joanne L. Blum
Clinical Breast Cancer April 2006 • 45
O'Shaughnessy1 CR1.indd 5 5/4/06 11:53:05 AM
Capecitabine/Taxane Combinations for Breast Cancer
or doxorubicin/cyclophosphamide before surgery. Among 29 evaluable patients, the clinical CR rate in the high-dose cohort was 22% (95% CI, 4%-60%) and 35% (95% CI, 16%-59%) in the low-dose group. The ORR was 100% (95% CI, 65%-100%) in the high-dose cohort and 85% (95% CI, 61%-96%) in the low-dose cohort. Based on the safety data with this highly active regimen, the authors recommended a 3-week regimen of capecitabine 800 mg/m2 twice daily on days 2-15 and docetaxel 75 mg/m2 I.V. on day 1 for further study in the preoperative setting.
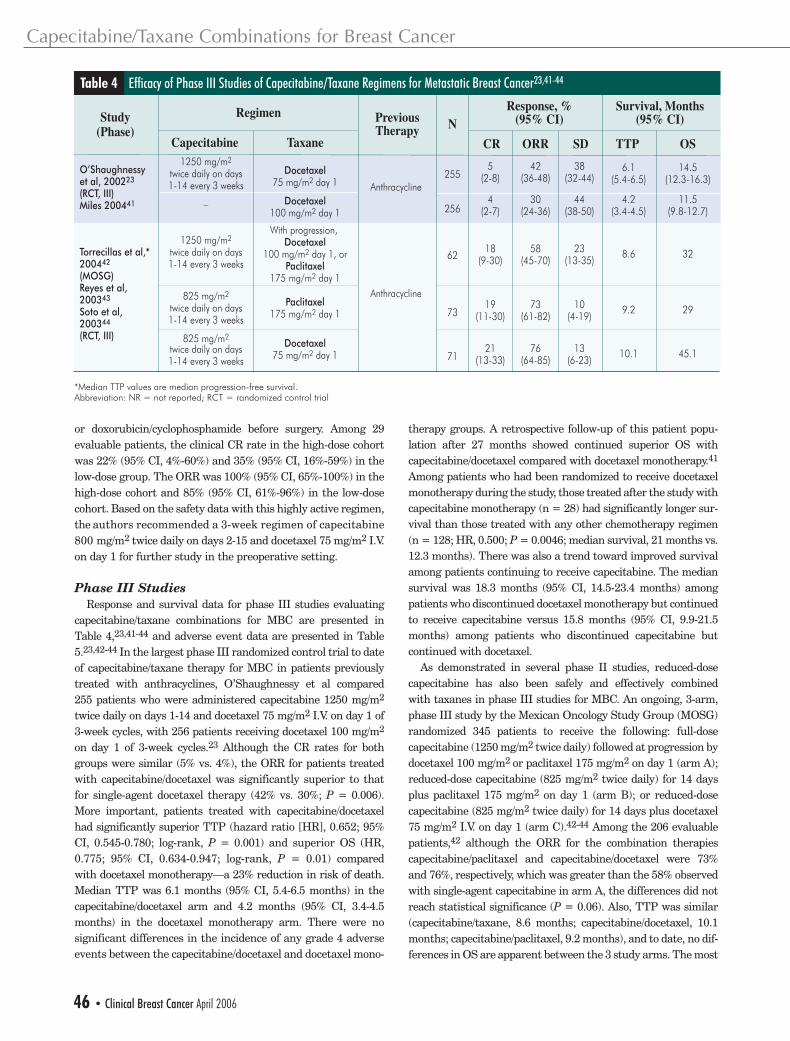
Phase III StudiesResponse and survival data for phase III studies evaluating
capecitabine/taxane combinations for MBC are presented in Table 4,23,41-44 and adverse event data are presented in Table 5.23,42-44 In the largest phase III randomized control trial to date of capecitabine/taxane therapy for MBC in patients previously treated with anthracyclines, O’Shaughnessy et al compared 255 patients who were administered capecitabine 1250 mg/m2 twice daily on days 1-14 and docetaxel 75 mg/m2 I.V. on day 1 of 3-week cycles, with 256 patients receiving docetaxel 100 mg/m2 on day 1 of 3-week cycles.23 Although the CR rates for both groups were similar (5% vs. 4%), the ORR for patients treated with capecitabine/docetaxel was significantly superior to that for single-agent docetaxel therapy (42% vs. 30%; P = 0.006). More important, patients treated with capecitabine/docetaxel had significantly superior TTP (hazard ratio [HR], 0.652; 95% CI, 0.545-0.780; log-rank, P = 0.001) and superior OS (HR, 0.775; 95% CI, 0.634-0.947; log-rank, P = 0.01) compared with docetaxel monotherapy—a 23% reduction in risk of death. Median TTP was 6.1 months (95% CI, 5.4-6.5 months) in the capecitabine/docetaxel arm and 4.2 months (95% CI, 3.4-4.5 months) in the docetaxel monotherapy arm. There were no significant differences in the incidence of any grade 4 adverse events between the capecitabine/docetaxel and docetaxel mono-
therapy groups. A retrospective follow-up of this patient popu-lation after 27 months showed continued superior OS with capecitabine/docetaxel compared with docetaxel monotherapy.41 Among patients who had been randomized to receive docetaxel monotherapy during the study, those treated after the study with capecitabine monotherapy (n = 28) had significantly longer sur-vival than those treated with any other chemotherapy regimen (n = 128; HR, 0.500; P = 0.0046; median survival, 21 months vs. 12.3 months). There was also a trend toward improved survival among patients continuing to receive capecitabine. The median survival was 18.3 months (95% CI, 14.5-23.4 months) among patients who discontinued docetaxel monotherapy but continued to receive capecitabine versus 15.8 months (95% CI, 9.9-21.5 months) among patients who discontinued capecitabine but continued with docetaxel.
As demonstrated in several phase II studies, reduced-dose capecitabine has also been safely and effectively combined with taxanes in phase III studies for MBC. An ongoing, 3-arm, phase III study by the Mexican Oncology Study Group (MOSG) randomized 345 patients to receive the following: full-dose capecitabine (1250 mg/m2 twice daily) followed at progression by docetaxel 100 mg/m2 or paclitaxel 175 mg/m2 on day 1 (arm A); reduced-dose capecitabine (825 mg/m2 twice daily) for 14 days plus paclitaxel 175 mg/m2 on day 1 (arm B); or reduced-dose capecitabine (825 mg/m2 twice daily) for 14 days plus docetaxel 75 mg/m2 I.V. on day 1 (arm C).42-44 Among the 206 evaluable patients,42 although the ORR for the combination therapies capecitabine/paclitaxel and capecitabine/docetaxel were 73% and 76%, respectively, which was greater than the 58% observed with single-agent capecitabine in arm A, the differences did not reach statistical significance (P = 0.06). Also, TTP was similar (capecitabine/taxane, 8.6 months; capecitabine/docetaxel, 10.1 months; capecitabine/paclitaxel, 9.2 months), and to date, no dif-ferences in OS are apparent between the 3 study arms. The most
Efficacy of Phase III Studies of Capecitabine/Taxane Regimens for Metastatic Breast Cancer23,41-44Table 4
Study(Phase)
O’Shaughnessyet al, 200223
(RCT, III)Miles 200441
Torrecillas et al,*200442
(MOSG)Reyes et al,200343
Soto et al, 200344
(RCT, III)
Capecitabine
Regimen Response, %(95% CI)
Survival, Months(95% CI)
1250 mg/m2
twice daily on days1-14 every 3 weeks
–
1250 mg/m2
twice daily on days1-14 every 3 weeks
825 mg/m2
twice daily on days1-14 every 3 weeks
825 mg/m2
twice daily on days1-14 every 3 weeks
Taxane
Docetaxel75 mg/m2 day 1
Docetaxel100 mg/m2 day 1
With progression, Docetaxel
100 mg/m2 day 1, orPaclitaxel
175 mg/m2 day 1
Paclitaxel175 mg/m2 day 1
Docetaxel75 mg/m2 day 1
PreviousTherapy
Anthracycline
Anthracycline
*Median TTP values are median progression-free survival.Abbreviation: NR = not reported; RCT = randomized control trial
N
255
256
62
73
71
CR
5(2-8)
4(2-7)
18(9-30)
19(11-30)
21(13-33)
ORR
42(36-48)
30(24-36)
58(45-70)
73(61-82)
76(64-85)
SD
38(32-44)
44(38-50)
23(13-35)
10(4-19)
13(6-23)
TTP
6.1(5.4-6.5)
4.2(3.4-4.5)
8.6
9.2
10.1
OS
14.5(12.3-16.3)
11.5(9.8-12.7)
32
29
45.1
46 • Clinical Breast Cancer April 2006
O'Shaughnessy1 CR1.indd 6 5/4/06 1:17:15 PM
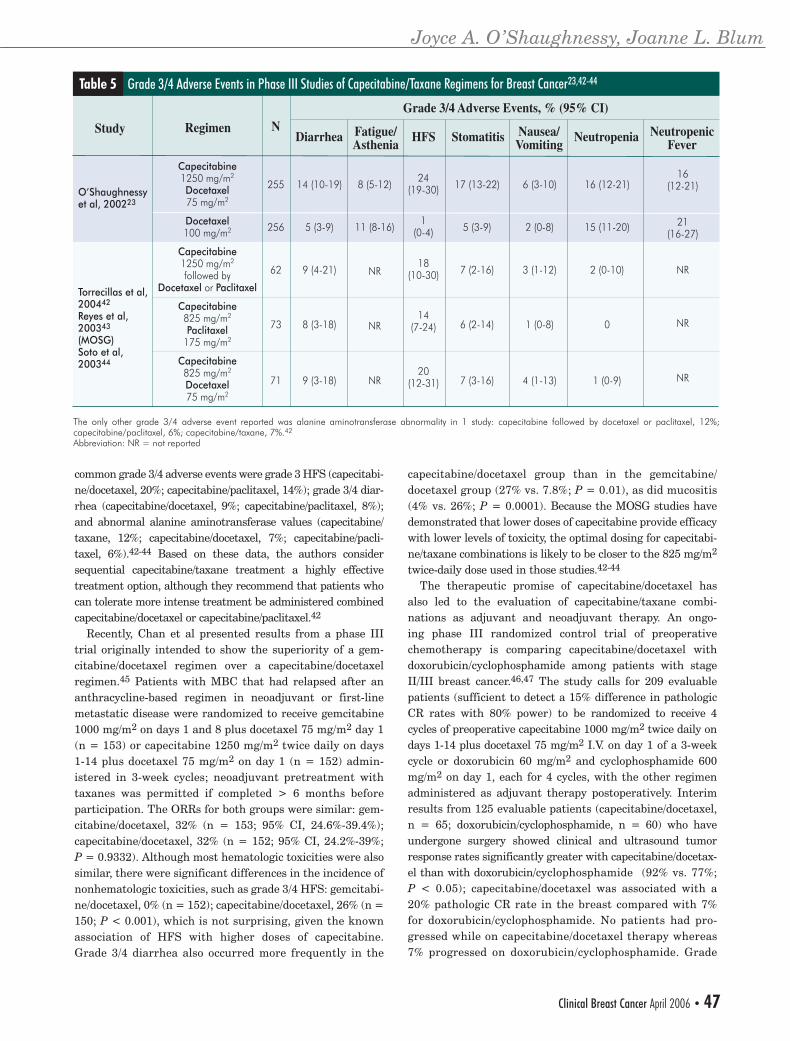
common grade 3/4 adverse events were grade 3 HFS (capecitabi-ne/docetaxel, 20%; capecitabine/paclitaxel, 14%); grade 3/4 diar-rhea (capecitabine/docetaxel, 9%; capecitabine/paclitaxel, 8%); and abnormal alanine aminotransferase values (capecitabine/taxane, 12%; capecitabine/docetaxel, 7%; capecitabine/pacli-taxel, 6%).42-44 Based on these data, the authors consider sequential capecitabine/taxane treatment a highly effective treatment option, although they recommend that patients who can tolerate more intense treatment be administered combined capecitabine/docetaxel or capecitabine/paclitaxel.42
Recently, Chan et al presented results from a phase III trial originally intended to show the superiority of a gem-citabine/docetaxel regimen over a capecitabine/docetaxel regimen.45 Patients with MBC that had relapsed after an anthracycline-based regimen in neoadjuvant or first-line metastatic disease were randomized to receive gemcitabine 1000 mg/m2 on days 1 and 8 plus docetaxel 75 mg/m2 day 1 (n = 153) or capecitabine 1250 mg/m2 twice daily on days 1-14 plus docetaxel 75 mg/m2 on day 1 (n = 152) admin-istered in 3-week cycles; neoadjuvant pretreatment with taxanes was permitted if completed > 6 months before participation. The ORRs for both groups were similar: gem-citabine/docetaxel, 32% (n = 153; 95% CI, 24.6%-39.4%); capecitabine/docetaxel, 32% (n = 152; 95% CI, 24.2%-39%; P = 0.9332). Although most hematologic toxicities were also similar, there were significant differences in the incidence of nonhematologic toxicities, such as grade 3/4 HFS: gemcitabi-ne/docetaxel, 0% (n = 152); capecitabine/docetaxel, 26% (n = 150; P < 0.001), which is not surprising, given the known association of HFS with higher doses of capecitabine. Grade 3/4 diarrhea also occurred more frequently in the
capecitabine/docetaxel group than in the gemcitabine/docetaxel group (27% vs. 7.8%; P = 0.01), as did mucositis (4% vs. 26%; P = 0.0001). Because the MOSG studies have demonstrated that lower doses of capecitabine provide efficacy with lower levels of toxicity, the optimal dosing for capecitabi-ne/taxane combinations is likely to be closer to the 825 mg/m2 twice-daily dose used in those studies.42-44
The therapeutic promise of capecitabine/docetaxel has also led to the evaluation of capecitabine/taxane combi-nations as adjuvant and neoadjuvant therapy. An ongo-ing phase III randomized control trial of preoperative chemotherapy is comparing capecitabine/docetaxel with doxorubicin/cyclophosphamide among patients with stage II/III breast cancer.46,47 The study calls for 209 evaluable patients (sufficient to detect a 15% difference in pathologic CR rates with 80% power) to be randomized to receive 4 cycles of preoperative capecitabine 1000 mg/m2 twice daily on days 1-14 plus docetaxel 75 mg/m2 I.V. on day 1 of a 3-week cycle or doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 on day 1, each for 4 cycles, with the other regimen administered as adjuvant therapy postoperatively. Interim results from 125 evaluable patients (capecitabine/docetaxel, n = 65; doxorubicin/cyclophosphamide, n = 60) who have undergone surgery showed clinical and ultrasound tumor response rates significantly greater with capecitabine/docetax-el than with doxorubicin/cyclophosphamide (92% vs. 77%; P < 0.05); capecitabine/docetaxel was associated with a 20% pathologic CR rate in the breast compared with 7% for doxorubicin/cyclophosphamide. No patients had pro-gressed while on capecitabine/docetaxel therapy whereas 7% progressed on doxorubicin/cyclophosphamide. Grade
Grade 3/4 Adverse Events in Phase III Studies of Capecitabine/Taxane Regimens for Breast Cancer23,42-44Table 5
Study
O’Shaughnessyet al, 200223
Torrecillas et al,200442
Reyes et al,200343
(MOSG)Soto et al,200344
Regimen
Capecitabine1250 mg/m2
Docetaxel75 mg/m2
Docetaxel100 mg/m2
Capecitabine1250 mg/m2
followed byDocetaxel or Paclitaxel
Capecitabine825 mg/m2
Paclitaxel175 mg/m2
Capecitabine825 mg/m2
Docetaxel75 mg/m2
The only other grade 3/4 adverse event reported was alanine aminotransferase abnormality in 1 study: capecitabine followed by docetaxel or paclitaxel, 12%; capecitabine/paclitaxel, 6%; capecitabine/taxane, 7%.42
Abbreviation: NR = not reported
N
255
256
62
73
71
14 (10-19)
5 (3-9)
9 (4-21)
8 (3-18)
9 (3-18)
8 (5-12)
11 (8-16)
NR
NR
NR
24(19-30)
1(0-4)
18(10-30)
14(7-24)
20(12-31)
17 (13-22)
5 (3-9)
7 (2-16)
6 (2-14)
7 (3-16)
6 (3-10)
2 (0-8)
3 (1-12)
1 (0-8)
4 (1-13)
16 (12-21)
15 (11-20)
2 (0-10)
0
1 (0-9)
Diarrhea HFS Stomatitis NeutropeniaFatigue/Asthenia
Nausea/Vomiting
16(12-21)
21(16-27)
NR
NR
NR
NeutropenicFever
Grade 3/4 Adverse Events, % (95% CI)
Joyce A. O’Shaughnessy, Joanne L. Blum
Clinical Breast Cancer April 2006 • 47
O'Shaughnessy1 CR1.indd 7 5/4/06 11:53:06 AM

Capecitabine/Taxane Combinations for Breast Cancer
3 HFS and grade 3/4 stomatitis occurred significantly more frequently with capecitabine/docetaxel than with doxorubicin/cyclophosphamide (23% vs. 0% [P < 0.001] and 11% vs. 0% [P = 0.01], respectively) and grade 3/4 vomiting occurred significantly more frequently with doxo-rubicin/cyclophosphamide (3% vs. 22%; P = 0.001).47 The National Surgical Adjuvant Breast and Bowel Project and the US Oncology Trialist Group are evaluating preoperative capecitabine/docetaxel in larger multicenter trials.
Several studies have reported on quality of life (QOL) with capecitabine/taxane therapy for MBC. Twelves et al compared QOL data among 224 patients who had received capecitabine 1250 mg/m2 twice daily for 14 days and docetaxel 75 mg/m2 I.V. on day 1 in 3-week cycles with 230 patients who had received docetaxel 100 mg/m2 alone on day 1 using the European Organization for Research and Treatment of Cancer QLQ-C30 (ver-sion 2.0) and the Breast Module BR23 questionnaires.48 After 30 weeks, the capecitabine/docetaxel group exhib-ited a trend toward improved overall QOL compared with the docetaxel monotherapy group. More recently, the MOSG group observed that patients treated with oral capecitabine combined with docetaxel or paclitaxel reported that their global health status significantly improved from pretreatment baseline.49
Capecitabine/taxane therapies have also been shown to be cost-effective compared with taxane monotherapy for treatment of MBC. O’Shaughnessy et al showed that, despite a longer mean duration of study treatment for patients treated with capecitabine/docetaxel rather than with single-agent docetaxel, 93% of the acquisition cost of capecitabine was offset by lower costs of docetaxel, leading to a savings of $2500 per life-year gained with capecitabi-ne/docetaxel therapy.50 In a Canadian study of third-line chemotherapy for metastatic disease, the addition of capecitabine to docetaxel compared with single-agent docetaxel yielded a small incremental cost of Can $3691 per life-year gained for the province of Ontario.51 Another Canadian study of capecitabine/docetaxel showed that, if all patients in British Columbia with anthracycline-resistant
MBC received capecitabine/docetaxel combination ther-apy instead of single-agent docetaxel, the overall cost sav-ings for the province would be Can $32,765 (US $25,934) per year, a savings of $2114 per life.52 Similarly, an Australian study of capecitabine/docetax-el using capecitabine at the FDA-recommended therapeu-tic dose reported a cost savings of AUD $158 (US $119) per patient per course compared with docetaxel monotherapy in patients whose disease had
progressed with previous anthracycline therapy.53
Several ongoing phase III studies are evaluating the capecitabine/taxane combination as adjuvant therapy. The US Oncology study 01-062 is a randomized, open-label, mul-ticenter phase III trial investigating the efficacy and safety of capecitabine/docetaxel versus docetaxel monotherapy as adjuvant treatment (Figure 1) in high-risk early-stage breast cancer. Patients are treated initially with four 3-week cycles of doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2
and are then randomized to receive 4 cycles of capecitabine 825 mg/m2 twice daily on days 1-14 plus docetaxel 75 mg/m2 on day 1 of a 3-week cycle or docetaxel 100 mg/m2 alone administered every 3 weeks. Accrual to this study is com-plete, and the combined capecitabine/docetaxel regimen has shown an acceptable safety profile.
Another large, ongoing, randomized, open-label, multi-center phase III trial, study ID01-580 (Figure 2), is inves-tigating the efficacy and safety of capecitabine/docetaxel compared with paclitaxel monotherapy as neoadjuvant therapy for patients with stage IIA-IIIA breast cancer or as an adjuvant therapy for patients with stage I-IIIA breast cancer. A total of 930 patients receive 4 cycles of FEC 100 (5-FU 500 mg/m2 I.V., epirubicin 100 mg/m2 I.V., and cyclo-phosphamide 500 mg/m2 I.V.) on day 1 and are then random-ized to receive combination therapy with oral capecitabine 1000 mg/m2 twice daily on days 1-14 plus docetaxel 75 mg/m2 on day 1 of a 3-week cycle for 4 cycles or paclitaxel 80 mg/m2 I.V. alone weekly for 12 weeks.
DiscussionThere is substantial evidence that regimens combining
capecitabine with a taxane are effective in treating MBC and have manageable toxicities, and data from the MOSG suggest that docetaxel and paclitaxel are equally effective when administered with capecitabine.42-44 A large body of phase II/ III data demonstrates that lowering the dose of capecitabine administered with the taxane improves safety without compromising efficacy. A capecitabine dose of 825 mg/m2 twice daily for 14 days has acceptable toxicity and can be administered with reliable dose intensity in combination
Figure 1 Schematic Design of US Oncology Study 01-062 for Adjuvant Treatment of Breast Cancer
In this randomized, open-label, phase III trial, 2410 patients with high-risk breast cancer, initially treated with four 3-week cycles of doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2 I.V. on day 1 of each cycle, are randomized to four 3-week cycles of oral capecitabine 825 mg/m2 twice daily for days 1-14 plus docetaxel 75 mg/m2 on day 1 or docetaxel 100 mg/m2 I.V. alone on day 1.
Doxorubicin 60 mg/m2
Cyclophosphamide 600 mg/m2 I.V.
D1
2410 Patients with High-Risk Breast Cancer
Adjuvant Chemotherapy
Docetaxel 100 mg/m2 I.V.
Docetaxel 75 mg/m2 I.V.
Capecitabine 825 mg/m2
twice daily
D2
D1
4 Cycles
D14
4 Cycles
D2
D21
D21
D1 D2 D21
RANDOMIZE
3-weekly Doxorubicin/Cyclophosphamide × 4
Rest
Rest
48 • Clinical Breast Cancer April 2006
O'Shaughnessy1 CR1.indd 8 5/4/06 11:53:06 AM

with docetaxel or paclitaxel. Multiple studies that have suc-cessfully used lower doses of capecitabine in taxane combi-nations have shown that prop-er dosing offers patients with MBC a highly effective and tolerable option. The recent phase III study by Chan et al of capecitabine/docetaxel ver-sus gemcitabine/docetaxel for MBC showed equivalent effi-cacy with the 2 regimens but with greater toxicity (especially HFS, diarrhea, and mucositis) with capecitabine/docetaxel.45 However, multiple previous studies showed that 825 mg/m2 twice daily is the ideal dose for capecitabine administered in combination with docetax-el.42-44 The choice of 1250 mg/m2 twice daily in the Chan et al study predisposed patients to predictably high rates of toxicity.45 Because a significant proportion of patients were unable to tolerate this particular capecitabine/docetaxel regimen and stopped therapy, it is not known whether the tolerable capecitabine dose of 825 mg/m2 with docetaxel compared with gemcitabine/docetaxel would result in supe-rior patient outcome. Although the combination of a taxane plus capecitabine is a highly effective treatment option for MBC, patients with small volume, indolent, and asymptom-atic breast cancer might be well served with treatment with capecitabine as a single agent first, followed by a taxane at the time of disease progression.
The success of the capecitabine/taxane combinations has led to studies that use these agents as sequential and weekly therapies and those that explore the addition of agents such as vinorelbine, epirubicin, and erlotinib.20,21,54 Phase III research has shown that weekly dosing for paclitaxel improves tumor response and TTP over the standard regimen (every 3 weeks), as shown by Seidman et al (1124),55 although the reduction in myelosuppression might be offset by an increased likelihood of neurotoxicity. Recently, ABI-007, a nanoparticle albumin-bound (nab) form of paclitaxel, demonstrated a superior response rate and progression-free survival with less grade 4 neutropenia and no significant hypersensitivity reactions (without steroid premedication) than standard paclitaxel formulated with poly-oxyethylene alkyl ethers.56 In addition, ABI-007 has shown considerable efficacy even in patients with taxane-refractory MBC. Plans are under way to conduct phase II studies evalu-ating the combination of nab paclitaxel and capecitabine in patients with MBC.57,58
Several ongoing studies worldwide are investigating the use of capecitabine/taxane combinations as treat-ment for early-stage or locally advanced breast cancer in the neoadjuvant and adjuvant settings.22,59 The next steps include identifying tumor and host factors that predict the likelihood of response and toxicity.
References 1. Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005 [published erra-
tum in CA Cancer J Clin 2005; 55:259]. CA Cancer J Clin 2005; 55:10-30. 2. Crown J, O’Leary M, Ooi WS. Docetaxel and paclitaxel in the treat-
ment of breast cancer: a review of clinical experience. Oncologist 2004; 9(suppl 2):24-32.
3. Paridaens R, Biganzoli L, Bruning P, et al. Paclitaxel versus doxorubicin as first-line single-agent chemotherapy for metastatic breast cancer: a European Organization for Research and Treatment of Cancer Randomized Study with cross-over. J Clin Oncol 2000; 18:724-733.
4. Sledge GW, Neuberg D, Bernardo P, et al. Phase III trial of doxorubi-cin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J Clin Oncol 2003; 21:588-592.
5. Bishop JF, Dewar J, Toner GC, et al. Initial paclitaxel improves out-come compared with CMFP combination chemotherapy as front-line therapy in untreated metastatic breast cancer. J Clin Oncol 1999; 17:2355-2364.
6. Nabholtz JM, Falkson C, Campos D, et al. Docetaxel and doxorubi-cin compared with doxorubicin and cyclophosphamide as first-line chemotherapy for metastatic breast cancer: results of a randomized, multicenter, phase III trial. J Clin Oncol 2003; 21:968-975.
7. Biganzoli L, Cufer T, Bruning P, et al. Doxorubicin and paclitaxel versus doxorubicin and cyclophosphamide as first-line chemotherapy in metastatic breast cancer: the European Organization for Research and Treatment of Cancer 10961 multicenter phase III trial. J Clin Oncol 2002; 20:3114-3121.
8. Jassem J, Pienkowski T, Pluzanska A, et al. Doxorubicin and paclitaxel versus fluorouracil, doxorubicin, and cyclophosphamide as first-line therapy for women with metastatic breast cancer: final results of a ran-domized phase III multicenter trial. J Clin Oncol 2001; 19:1707-1715.
9. Nabholtz JM, Senn HJ, Bezwoda WR, et al. Prospective randomized trial of docetaxel versus mitomycin plus vinblastine in patients with meta-static breast cancer progressing despite previous anthracycline-contain-ing chemotherapy. 304 Study Group. J Clin Oncol 1999; 17:1413-1424.
10. Sjostrom J, Blomqvist C, Mouridsen H, et al. Docetaxel compared with sequential methotrexate and 5-fluorouracil in patients with advanced breast cancer after anthracycline failure: a randomised phase III study with crossover on progression by the Scandinavian Breast Group. Eur J Cancer 1999; 35:1194-1201.
11. Bonneterre J, Roche H, Monnier A, et al. Docetaxel vs 5-fluoroura-cil plus vinorelbine in metastatic breast cancer after anthracycline therapy failure. Br J Cancer 2002; 87:1210-1215.
12. Blum JL. The role of capecitabine, an oral, enzymatically acti-vated fluoropyrimidine, in the treatment of metastatic breast cancer. Oncologist 2001; 6:56-64.
13. Xeloda (capecitabine) tablets prescribing information. Available at: http://www.rocheusa com/products/xeloda. Accessed October 1, 2005.
14. Miwa M, Ura M, Nishida M, et al. Design of a novel oral fluoropy-rimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998; 34:1274-1281.
15. Schuller J, Cassidy J, Dumont E, et al. Preferential activation of capecitabine in tumor following oral administration to colorectal cancer patients. Cancer Chemother Pharmacol 2000; 45:291-297.
16. Blum JL, Jones SE, Buzdar AU, et al. Multicenter phase II study of capecitabine in paclitaxel-refractory metastatic breast cancer. J Clin Oncol 1999; 17:485-493.
Figure 2 Schematic Design of ID01-580 for Neoadjuvant or Adjuvant Treatment of Breast Cancer
In this randomized, open-label, phase III trial, 930 patients with stages I-IIIA breast cancer are initially treated with four 3-week cycles of FEC 100 (5-FU 500 mg/m2 I.V., epirubicin 100 mg/m2 I.V., and cyclophosphamide 500 mg/m2 on day 1) and are then randomized to receive four 3-week cycles of oral capecitabine 1000 mg/m2 twice daily on days 1-14 plus docetaxel 75 mg/m2 I.V. on day 1 or paclitaxel 80 mg/m2 I.V. alone weekly for 12 weeks. Therapy could be in the adjuvant setting for stages I-IIIA or in the neoadjuvant setting for stages IIA-IIIA.
D1
5-FU 500 mg/m2
Epirubicin 100 mg/m2
Cyclophosphamide 500 mg/m2
930 Patients with Operable Breast Cancer
Weekly Paclitaxel 80 mg/m2 for 12 weeks
4 CyclesDocetaxel75 mg/m2
D1 D14
D21
D21
RANDOMIZE
4 Cycles of FEC 100
Rest
Capecitabine 1000 mg/m2 twice daily
Joyce A. O’Shaughnessy, Joanne L. Blum
Clinical Breast Cancer April 2006 • 49
O'Shaughnessy1 CR1.indd 9 5/4/06 11:53:07 AM
17. Blum JL, Dieras V, Lo Russo PM, et al. Multicenter, phase II study of capecitabine in taxane-pretreated metastatic breast carcinoma patients. Cancer 2001; 92:1759-1768.
18. Lara R, Mayordomo JI, Modolell A, et al. Feasibility of adjuvant chemotherapy with doxorubicin plus docetaxel followed by sequential capecitabine in patients with node positive breast cancer. Proc Am Soc Clin Oncol 2004; 23:72.
19. Wenzel C, Hussian D, Bartsch R, et al. Feasibility of docetaxel, epi-rubicin, and capecitabine (TEX) plus pegfilgrastim as neoadjuvant treatment for primary breast cancer: a pilot study. Proc Am Soc Clin Oncol 2004; 23:55.
20. Ghosn M, Chahine G, Kattan J, et al. Phase II study of sequential administration of vinorelbine: capecitabine combination followed by weekly docetaxel as first line chemotherapy for advanced breast cancer. Proc Am Soc Clin Oncol 2004; 23:81 (Abstract #817).
21. Einbeigi Z, Bergstrom D, Malmberg M. Optimizing doses of a first line chemotherapy treatment containing epirubicin, paclitaxel and capecitabi-ne (TEX) in metastatic breast cancer. Presented at: San Antonio Breast Cancer Symposium; December 3-6, 2003; San Antonio, TX.
22. Ahlgren J, Lidbrink E, Lind B, et al. Phase II study of epirubicin, cisplatin and capecitabine as neo-adjuvant chemotherapy in women with locally advanced or inflammatory breast cancer. Proc Am Soc Clin Oncol 2003; 22:27 (Abstract #107).
23. O’Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus docetaxel combination therapy in anthracycline-pretreated patients with advanced breast cancer: phase III trial results. J Clin Oncol 2002; 20:2812-2823.
24. Sawada N, Ishikawa T, Fukase Y, et al. Induction of thymidine phosphor-ylase activity and enhancement of capecitabine efficacy by taxol/taxotere in human cancer xenografts. Clin Cancer Res 1998; 4:1013-1019.
25. Khoury P, Villalona-Calero M, Blum J, et al. Phase I study of capecitabine in combination with the paclitaxel in patients with previously treated metastatic breast cancer. Proc Am Soc Clin Oncol 1998; (Abstract #793).
26. Villalona-Calero MA, Blum JL, Jones SE, et al. A phase I and pharma-cologic study of capecitabine and paclitaxel in breast cancer patients. Ann Oncol 2001; 12:605-614.
27. Tonkin K, Scarfe A, Koski S, et al. Preliminary results of a phase I/II study of weekly docetaxel (Taxotere®) combined with intermittent capecitabine (Xeloda®) for patients with anthracycline pre-treated metastatic breast cancer. Proc Am Soc Clin Oncol 2001; 20:201b (Abstract #2016).
28. Pronk LC, Vasey P, Sparreboom A, et al. A phase I and pharmaco-kinetic study of the combination of capecitabine and docetaxel in patients with advanced solid tumours. Br J Cancer 2000; 83:22-29.
29. Norton L, Dugan L, Hudis CA, et al. Optimizing chemotherapeu-tic dose-schedule (CDS) by Norton-Simon Modeling: capecitabine (Xeloda®). Proc Amer Assoc Cancer Res 2005; 46:5007.
30. Wilson E. Probable inference, the law of succession, and statistical inference. J Am Statistical Assoc 1927; 22:209-212.
31. Llorca C, Mayordomo E, Ardrover I, et al. Activity and safety of biweek-ly docetaxel plus capecitabine as first-line treatment for patients with metastatic breast cancer. J Clin Oncol 2004; 22(14 suppl):73s.
32. Chun JH, Lee HG, Lee ES, et al. Frontline docetaxel (T)/ capecitabine (X) combination therapy in patients (pts) with metastatic breast cancer (MBC): a phase II study. Proc Am Soc Clin Oncol 2004; 22(suppl 14):71s.
33. Blum JL, Dees C, Negron A, et al. A phase II trial of combination therapy with capecitabine (C) and weekly paclitaxel (P) for metastatic breast cancer (MBC): preliminary results in taxane-naive patients. Presented at: San Antonio Breast Cancer Symposium; December 8-11, 2004; San Antonio, TX.
34. Meza L, Amin B, Horsey M, et al. A phase II study of capecitabine in combination with paclitaxel as first or second line therapy in patients with metastatic breast cancer (MBC). Proc Am Soc Clin Oncol 2001; 20:70b (Abstract #2029).
35. Gradishar WJ, Meza LA, Amin B, et al. Capecitabine plus paclitaxel as front-line combination therapy for metastatic breast cancer: a multicenter phase II study. J Clin Oncol 2004; 22:2321-2327.
36. Batista N, Perez-Manga G, Constenla M, et al. Phase II study of capecitabine in combination with paclitaxel in patients with anthra-cycline-pretreated advanced/metastatic breast cancer. Br J Cancer 2004; 90:1740-1746.
37. Shapiro C, Ramaswamy B, Rhoades C, et al. Phase II trial of weekly docetaxel (DOC) and prolonged capecitabine (C) in metastatic breast cancer (MBC) patients (pts). Presented at: San Antonio Breast Cancer Symposium; December 8-11, 2004; San Antonio, TX.
38. Mackey JR, Tonkin K, Scarfe AG, et al. Final results of a phase II clinical trial of weekly docetaxel (T) in combination with capecitabine (X) in anthracycline pre-treated metastatic breast cancer (MBC). Proc Am Soc Clin Oncol 2003; 22:42 (Abstract #167).
39. Bari M, Andrea D, Sartori D, et al. Capecitabine plus weekly paclitax-el (CwP) as 2nd/3rd-line chemotherapy for metastatic breast cancer.
Ann Oncol 2002; 13(suppl 5):69.40. Lebowitz PF, Eng-Wong J, Swain SM, et al. A phase II trial of neoad-
juvant docetaxel and capecitabine for locally advanced breast cancer. Clin Cancer Res 2004; 10:6764-6769.
41. Miles D, Vukelja S, Moiseyenko V, et al. Survival benefit with capecitabine/docetaxel versus docetaxel alone: analysis of therapy in a randomized phase III trial. Clin Breast Cancer 2004; 5:273-278.
42. Torecillas L, Soto C, Cervantes G, et al. Capecitabine (X) and taxanes in patients (pts) with anthracycline-pretreated metastatic breast can-cer (MBC): sequential vs. combined therapy results from the Mexican Oncology Study Group. Presented at: San Antonio Breast Cancer Symposium; December 8-11, 2004; San Antonio, TX.
43. Reyes S, Torrecillas L, Acosta A, et al. Capecitabine and taxanes: combination versus sequential therapy in anthracycline-pretreated metastatic breast cancer (MBC): findings from the Mexican Oncology Study Group (MOSG) phase III trial. Eur J Cancer 2003; 1:S136.
44. Soto C, Reyes S, Delgadillo F, et al. Capecitabine (X) plus docetaxel (T) vs capecitabine plus paclitaxel (P) vs sequential capecitabine then taxane in anthracycline pretreated patients (pts) with metastatic breast cancer: early results. Proc Am Soc Clin Oncol 2004; 22:8.
45. Chan S, Romieu J, Huober T, et al. Gemcitabine plus docetaxel (GD) ver-sus capecitabine plus docetaxel (CD) for anthracycline-pretreated meta-static breast cancer (MBC) patients (pts): results of a European phase III study. Proc Am Soc Clin Oncol 2005; 23(suppl 16):24s (Abstract #581).
46. Lee HG, Lee JJ, Jung KH, et al. Phase III randomized trial of primary chemotherapy with doxorubicin/cyclophosphamide (AC) vs docetaxel/capecitabine (TX) for stage II/III breast cancer (BC): interim analysis. Proc Am Soc Clin Oncol 2004; 23:28 (Abstract #607).
47. Ahn JB, Oh JH, Kwon Y, et al. Interim analysis findings from a phase III randomized trial of docetaxel/capecitabine (TX) vs. doxorubicin/cyclophosphamide (AC) as primary chemotherapy for stage II/III breast cancer (BC). Ann Oncol 2004; 15(suppl 3):iii57 (Abstract #215PD).
48. Twelves C, Fumoleau P, Jones S, et al. Adding Xeloda (capecitabine) to Taxotere (docetaxel) significantly improves survival without com-promising quality of life in patients with metastatic breast cancer. Presented at: San Antonio Breast Cancer Symposium; December 10-13, 2001; San Antonio, TX (Poster #542).
49. Torecillas L, Cortes P, Tokunaga C, et al. Capecitabine monotherapy or combined with taxanes: early results in quality of life in patients with metastatic breast cancer. Proc Am Soc Clin Oncol 2003; 22:749.
50. O’Shaughnessy JA, Blum J, Moiseyenko V, et al. Randomized, open-label, phase II trial of oral capecitabine (Xeloda) vs. a reference arm of intravenous CMF (cyclophosphamide, methotrexate and 5-fluoroura-cil) as first-line therapy for advanced/metastatic breast cancer. Ann Oncol 2001; 12:1247-1254.
51. Verma S, Ilersich AL. Population-based pharmacoeconomic model for adopting capecitabine/docetaxel combination treatment for anthracy-cline-pretreated metastatic breast cancer. Oncologist 2003; 8:232-240.
52. Malfair-Taylor S, Verma S, Barnett J, et al. Cost-effective analysis of capecitabine and docetaxel (DC) versus taxanes alone in the treat-ment of anthracycline resistant metastatic breast cancer (MBC): perspectives from two Canadian provinces. Proc Am Soc Clin Oncol 2003; 22:558 (Abstract #2244).
53. Todd C, Malanos G. Australian economic analysis of Xeloda (capecitabine) in combination with docetaxel for the treatment of patients with advanced breast cancer after failure of prior anthra-cycline-containing chemotherapy. Presented at: San Antonio Breast Cancer Symposium; December 11-14, 2002; San Antonio, TX.
54. Jones R, Trigo F, Derosa F, et al. A phase IB study of erlotinib plus capecitabine and docetaxel in metastatic breast cancer (MBC). Proc Am Soc Clin 2003; 22:45 (Abstract #180).
55. Seidman AD, Berry D, Cirrincione C, et al. CALGB 9840: phase III study of weekly (W) paclitaxel (P) via 1-hour (h) infusion versus standard (S) 3h infusion every third week in the treatment of metastatic breast cancer (MBC), with trastuzumab (T) for HER2 positive MBC and randomized for T inHER2 normal MBC. J Clin Oncol 2004; 22:6 (Abstract #512).
56. O’Shaughnessy J, Tjulandin S, Davidson N, et al. ABI-007 (Abraxane), a nanoparticle albumin-bound (nab) paclitaxel demonstrates superior effi-cacy vs taxol in MBC: a phase III trial. Presented at: San Antonio Breast Cancer Symposium; December 3-6, 2003; San Antonio, TX.
57. Blum JL, Savin M, Edelman J, et al. Long term disease control in tax-ane-refractory metastatic breast cancer treated with nab paclitaxel. Proc Am Soc Clin Oncol 2004; 22:12 (Abstract #543).
58. O’Shaughnessy J, Blum J, Sandbach J, et al. Weekly nanoparticle albumin paclitaxel (Abraxane) results in long-term disease control in patients with taxane-refractory metastatic breast cancer. Presented at: San Antonio Breast Cancer Symposium; December 8-11, 2004; San Antonio, TX.
59. Bellet M, Munoz M, Pelegri A, et al. Phase II study of capecitabine (C) in combination with docetaxel (D) as neoadjuvant treatment in patients with locally advanced breast cancer (IIIA and IIIB stage). Proc Am Soc Clin Oncol 2004; 23:64 (Abstract #752).
Capecitabine/Taxane Combinations for Breast Cancer
50 • Clinical Breast Cancer April 2006
O'Shaughnessy1 CR1.indd 10 5/4/06 11:53:08 AM