capsular bag shrinkage after implantation of a capsular bending or capsular tension ring
TRANSCRIPT
Capsular bag shrinkage after implantation
of a capsular bending or capsular tension ring
Sabine Kurz, MD, Frank Krummenauer, PhD, Philipp Hacker, MS, N. Pfeiffer, MD, H. Burkhard Dick, MD
PURPOSE: To evaluate the influence of a capsular bending ring (CBR) or tension ring (CTR) on capsularbag shrinkage.
SETTING: Department of Ophthalmology, Johannes Gutenberg-University, and Department of Med-ical Biometry, Epidemiology and Informatics, University of Mainz, Mainz, Germany.
METHODS: In 92 eyes of 92 patients, a capsular measuring ring (CMR) was implanted after phacoemul-sification to measure capsular bag size in vivo. Patients were randomized into 3 groups: The first re-ceived a CMR and CBR, the second received a CMR and CTR, and the third received a CMR alone.Measurements were performed preoperatively, intraoperatively, during the first 3 postoperativedays, and after 1 and 3 months. Preoperative biometric characteristics such as axial length (AL) andanterior chamber depth were determined. Primary clinical end points were capsular bag size and cap-sulorhexis diameter measured intraoperatively and by means of slitlamp biomicroscopy and retroillu-mination photography postoperatively.
RESULTS: There were no clinically relevant group differences in AL, anterior chamber depth, or cap-sulorhexis diameter. Eyes implanted with the CBR showed shrinkage of the capsular bag from 10.6 to10.4 mm after a median of 3 months (sign test; PZ .023); eyes with a CTR showed comparable mediancapsular bag shrinkage from 10.5 to 10.2 mm (P<.001), whereas eyes without a CTR showed a medianshrinkage from 10.5 to 10.0 mm (P<.001). Intraindividual shrinkage was of a similar, although signifi-cantly different, order among these groups (median shrinkage 0.15 versus 0.23 and 0.38 mm, respec-tively; all pairwise Wilcoxon test; P Z .050, P Z .020, P<.001, respectively).
CONCLUSIONS: Capsular shrinkage can be inhibited by a CBR and, to lesser extent, a CTR; the gain inshrinkage prevention is limited when compared with a CMR, however. This conclusion can be drawnonly for the specific CBR or CTR and hydrophobic acrylic intraocular lens (IOL) used in this study.Reduction of capsular bag shrinkage after CTR implantation may reduce IOL dislocation and tilt andhelp to maintain postoperative visual acuity.
J Cataract Refract Surg 2005; 31:1915–1920 Q 2005 ASCRS and ESCRS
J CATARACT REFRACT SURG - VOL 31, OCTOBER 2005
Shrinkage of the capsular bag and capsulorhexis opening
occurs frequently after cataract surgery. These complica-
tions can lead to intraocular lens (IOL) decentration, defor-
mation, and tilting, resulting in reduced or double vision.1
These problems can be severe, especially with multifocal
and toric lenses. Capsular bag shrinkage usually desists
after 3 to 6 months.2
Capsular tension rings (CTRs) have proved valuable
for an increasing variety of applications during the past
13 years, including for use in cases of zonular weakness
and dialysis, pseudoexfoliation, lens colobomas, phaco-
donesis, and severe nystagmus in complicated anteriorsegment surgery.3–7 Furthermore, CTRs can be used to
prevent lens decentration, for example, under conditions
of nonideal capsulorhexis and implantation of a multifocal
or aspheric IOL.8,9 Other indications include the reduction
Q 2005 ASCRS and ESCRS
Published by Elsevier Inc.
of posterior capsule opacification (PCO)10,11 in cases with
a potential for IOL exchange, relief of primary posterior
capsulorhexis, and iris defects.11–14 The aim of this pro-
spective randomized study was to evaluate the influenceof the implantation of a capsular bending ring (CBR) or
a CTR on capsular bag shrinkage.
PATIENTS AND METHODS
Included in the study were 92 eyes of 92 patients (median age78 years; range 37 to 93 years). Inclusion criteria were otherwisehealthy eyes with cataract and an axial length (AL) between21 mm and 26.5 mm. Other inclusion criteria were intact zonularapparatus and intact capsular bag. Exclusion criteria were intra-operative complications (ie, zonulysis, capsule tears), priorintraocular surgery, lenticular pseudoexfoliation, proliferative di-abetic retinopathy, uveitis, corneal diseases, trauma, vitrectomy,
0886-3350/05/$-see front matterdoi:10.1016/j.jcrs.2005.06.046
1915

CAPSULAR BAG SHRINKAGE AFTER CAPSULAR RING IMPLANTATION
neoplasm of the eye, and pupils!8.0mm after medical mydriasis.Each patient signed informed consent forms. Preoperatively, slit-lamp examination of the anterior and posterior eye segmentswas performed in mydriasis with tropicamide. Biometric charac-teristics such as AL and the anterior chamber depth were deter-mined by means of the Zeiss IOLMaster. Following uneventfulphacoemulsification, a capsular measuring ring (CMR) was im-planted into all eyes. On the day of cataract surgery, eyes were ran-domized into 3 groups: The first group received a CMR and a CBR,the second group received a CMR and a CTR, and the third groupserved as a control sample and received only a measuring CMR.
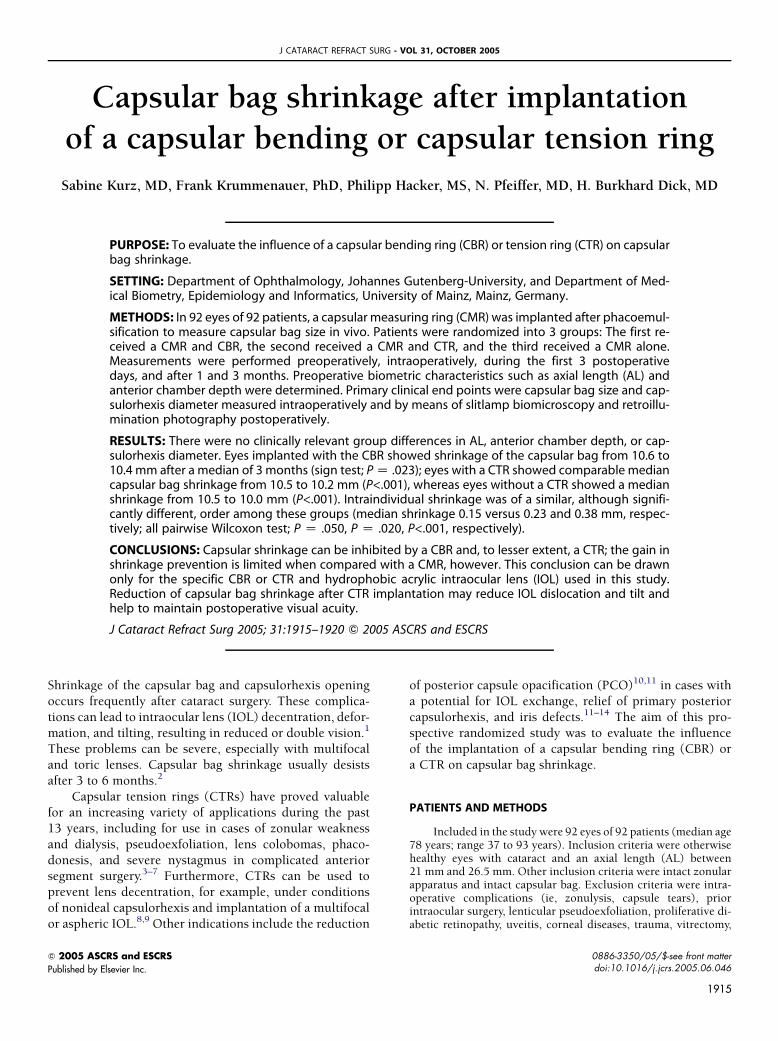
The CMR first introduced by H.R. Koch (MicroPlex KMR 12,HumanOptics) is composed of soft and thin poly(methyl methac-rylate) (PMMA) with round edges. It allows determination of thecapsular bag in vivo (Figure 1).2 In its relaxed state, the CMR isa ring with a diameter of 12.0 mm, possessing measuring exten-sions at both ends instead of eyelets. Determining the relative po-sitions of these extensions via slitlamp biomicroscopy allows forcalculation of the diameter of the capsular bag. The measuring
Figure 1. In vivo slitlamp photograph of the CMR (type KMR12, Human-
Optics). The rectangular end passed the other end due to capsular bag
shrinkage. Both ends lie on the other; the actual capsular bag diameter
is 10.0 mm.
Accepted for publication June 16, 2005.
From the Department of Ophthalmology (Kurz, Hacker, Pfeiffer,Dick), Johannes Gutenberg-University, and Department of Medi-cal Biometry (Krummenauer), Epidemiology and Informatics, Uni-versity of Mainz, Mainz, Germany.
Presented in part at the ASCRS Symposium on Cataract, IOL andRefractive Surgery, San Francisco, California, USA, April 2003, andat the XXst Congress of the European Society for Cataract & Re-fractive Surgeons, Munich, Germany, September 2003.
No author has a financial or proprietary interest in any materialand method mentioned.
Reprint requests to Sabine Kurz, MD, Department of Ophthal-mology, Johannes Gutenberg-University, Langenbeckstrasse 1,55101 Mainz, Germany. E-mail: [email protected].
J CATARACT REFRACT SURG -1916
extensions are 0.2 mm thick; 1 of the 2 extensions has a 1.0 mmlong transverse extension and represents an intraocular referencedistance (Figures 2 and 3). The distance between the extensionscan thereby be measured accurately. By using a conversion table,the current capsular bag diameter can be determined.2 Whenthe capsular bag shrinks, the ends of the CMR move above eachother. The CBR (Ø 11.0 mm, Nishi/Menapace 1E, Morcher) isan advancement over the CTR with a lateral height of 0.7 mmand a sharp-edged design. It is made of PMMA and has a diameterof 11.0 mm. A CTR made of PMMA and 11.0 mm in diameter wasimplanted (SR11, Acritec).
After ring implantation, a hydrophobic acrylic OptiEdge IOL(AR40e, AMO) was implanted in all eyes. The same surgeon(H.B.D.) performed all surgeries in this study. The following mea-surements were performed in all eyes: The capsular bag size andthe horizontal and vertical capsulorhexis diameters were mea-sured intraoperatively. The capsular bag diameter was assessedat the end of surgery when the CMR and the CBR or CTR andthe IOL were in the bag, after complete removal of viscoelasticsubstance and after the chamber was filled with balanced salt so-lution (BSS). Intraocular pressure (IOP) after the anterior cham-ber was filled with BSS did not influence capsular bag diameterwithin a range of 5 to 35 mm Hg. The capsular bag diameterwas measured after an IOP of 15 to 20 mm Hg was achieved. Atvisit 1 (1 to 3 days postoperatively), capsular bag size and capsu-lorhexis diameter were measured again after mydriasis by meansof slitlamp biomicroscopy. Additionally, in all eyes, retroillumina-tion photography was performed to confirm the slitlamp resultsby measuring with a ruler the distance between the measuringends of the CMR and the capsulorhexis diameter. At visit 2 (1month postoperatively) and visit 3 (3 months postoperatively),these parameters were measured again.
Primary Clinical End Point
The primary clinical end point of this investigation was intra-individiual difference (in millimeters) in capsular bag diameter on
Figure 2. Scanning electron microscopy of the 2 ends of the CMR. One
end measures exactly 0.2 mm in width, and the second rectangular end
is 1.0 mm in width, acting as an intraocular measuring reference.
VOL 31, OCTOBER 2005
CAPSULAR BAG SHRINKAGE AFTER CAPSULAR RING IMPLANTATION
the day of surgery versus visit 3 (3 months after implantation). Aclinically relevant shrinkage of capsular bag diameter was definedas a reduction of 0.3 mm or more in the statistical analysis plan ofthis investigation. This benchmark was introduced into samplesize calculation, which affords predetermination of clinically rel-evant changes due to the intervention under consideration. Re-garding the results of previous pivotal trials, a median shrinkageof 0.3 mm was expected and also corresponded to clinically rele-vant changes in capsular bag shrinkage (the latter indicating pos-sible loss in clinical benefit after surgery). Clinical relevance wastherefore defined before the start of the investigation.
Study Design
Ninety-two eyes of 92 patients were included to achievea group size of more than 30 patients per subsample (CMR,CTRCCMR, CBRCCMR). Patients were randomized withoutstratification for possible confounders; random numbers weregenerated using SPSS software (release 10.0 for Windows). Thesample size (n Z 33) was chosen to achieve a statistical powerof 80% or more in pairwise group comparisons along this investi-gation’s primary clinical end point. A multiple significance level of5% (ie, a pairwise comparison level of 1.7%)was determined in thestatistical analysis plan to reveal a group difference R0.3 mm inthe clinical end point as statistically significant in pairwisecomparisons. The Independent Ethics Committee (Landesarzte-kammer Rheinland-Pfalz) approved this study design in March2003.
diameter: 12 mm
compressed to 10.0 mm
Figure 3. The CMR at different compression stages (distance between the
ends 2.0 mm in relaxed state and 1.7 mm in compressed state) and the
resulting capsular bag diameter (12.0 mm versus 10 mm).
J CATARACT REFRACT SURG -
Statistical Analysis
Data description was based onmedians and quartiles for con-tinuous end points and on absolute and relative frequencies forcategorical end points. Comparisons of repeated measurementsin continuous end points were evaluated bymeans of intraindivid-ual differences and ratios. Graphic representation of continuousdata was based on nonparametric box whisker plots, accordingly.
For significance comparisons in continuous repeated mea-surements, the sign test was applied, and the 2-sample Wilcoxontest was applied for group comparisons along continuous endpoints. Results of these tests were summarized with P values forwhich the evaluation of the primary clinical end point was dueto a multiple significance level of 5%. Bonferroni correction wasapplied to the P values, which arose from pairwise comparisonalong the primary clinical end point. P values derived by analysisof secondary end points were not adjusted for multiplicity andtherefore indicate local statistical significance.
RESULTS
Preoperatively, no statistically significant differences
were found between groups in the AL (pooled median
23.3 mm, range 21.4 to 26.8 mm) and in the ACD (me-
dian 3.1 mm, range 2.8 to 3.4 mm). Postoperatively, no
statistically significant differences were found in the cap-
sulorhexis diameter within groups (intraindividual com-
parison by means of sign tests: group 1, P Z .06; group 2,P Z.56; group 3, P Z.19) and between groups (interindi-
vidual comparison by means of 2-sample Wilcoxon tests,
pooled median 5.5 to 5.6 mm, range 4.4 to 6.8 mm). The
eyes implanted with the CBR (group 1) showed small but
statistically significant shrinkage of the median capsular
bag from 10.55 mm (range 9.85 to 11.4 mm) to 10.4 mm
(range 9.7 to 11.6mm) after 3months (sign test, PZ .023).
The eyes with a CTR (group 2) showed a statistically signif-icant shrinkage of the median capsular bag from 10.45 mm
(range 9.95 to 11.25 mm) to 10.25 mm (range 9.15 to
10.85 mm) (P!.001). The largest shrinkage from a median
of 10.45 mm (range 9.8 to 11.55 mm) to 10.03 mm (range
8.0 to 11.1 mm) was found in the control group (CMR
alone, group 3, P!.001) (Table 1 and Figure 4).
For interindividual comparison between groups 1 and
3, a significantly larger shrinkage of the capsular bag wasfound in group 3 within the first 3 postoperative days
(P Z .01), after 1 month (P!.001), and after 3 months
(P!.001). Comparing groups 2 and 3, no locally statisti-
cally significant differences were found within the first 3
postoperative days (P Z .663) but was seen after 1 month
(P Z.008) and 3 months (P Z.020). The latter group dif-
ference did not remain statistically significant after Bonfer-
roni correction for multiplicity and was therefore due tolocal statistical significance. The median changes in the
capsular bag diameter between groups are displayed in
Figure 5.
VOL 31, OCTOBER 2005 1917

CAPSULAR BAG SHRINKAGE AFTER CAPSULAR RING IMPLANTATION
DISCUSSION
Capsular tension rings are frequently used for the man-
agement of intraoperative complications such as zonuloly-
sis. A CTR is able to reduce folds of the posterior lens
capsule after IOL implantation and therefore helps to re-
store quality of vision. Moreover, it can be useful to support
optimal centration of the IOL. The CBR is more rigid with
a higher spring constant15 and is implanted to reduce PCObecause of its sharp, OptiEdge design.16,17 Capsule opacifi-
cation and capsular bag shrinkage may lead to IOL decen-
tration and tilt. These complications can cause a decrease in
222927323531252825N =CMRCTR + CMRCBR + CMR
intra
indi
vidu
al s
hrin
kage
pre
- po
st [m
m]
2,01,81,61,41,21,0,8,6,4,2,0
-,2-,4-,6-,8
-1,0
Figure 4. Nonparametric box plots for the capsular bag shrinkage distri-
bution 1 to 3 days and 1 and 3 months postoperatively (pre-post; mm) in
groups 1 (CBRCCMR), 2 (CTRCCMR), and 3 (CMR). Horizontals indicate
medians and quartiles (minimum andmaximum values), which do not ex-
ceed a deviation from the quartiles of more than 1.5 times the interquar-
tile ranges. B Z statistical outliers with deviation from the quartiles of
more than 1.5 times the interquartile range. *Z statistical extreme values
with deviation from the quartile of more than 3 times the interquartile
range.
Table 1. Medians and quartiles for capsular bag diameter distribution and
intraoperative and 3-month postoperative measurements.*
Capsular Bag Size (mm)
GroupIntraoperativeMedian (Q1–Q3)
3-Month PostopMedian (Q1–Q3)
CBR C CMR 10.6 (10.3–10.9) 10.4 (10.1–10.8)CTR C CMR 10.5 (10.3–10.9) 10.2 (10.0–10.6)CMR 10.5 (10.3–10.8) 10.0 (9.8–10.3)
CBRZ capsular bag ring; CMRZ capsular measuring ring; CTRZ capsu-
lar tension ring; Q Z quartile
*The least shrinkagewas found in group 1 (CBRCCMR, sign test PZ .023);
the greatest was found in the control group (CMR alone, sign test
P!.001).
J CATARACT REFRACT SURG -1918
visual acuity. Resistance to lens decentration and tilt and
the occurrence of capsule opacification greatly depend on
the design and the material of the IOL.18–20 The latter
also influence the clinical presentation of capsular shrink-
age.19 Particularly for toric IOLs, rotational stability and
centering are necessary to achieve the desired refractivecorrection. Additionally, optimal centration is needed in
aspheric as well as multifocal IOLs.
The goal of this prospective randomized masked
study was to find out whether a CTR or a more rigid CBR
is able to inhibit the forces of capsular bag shrinkage under
normal circumstances. To our knowledge, this is the first
report that analyzed the influence of a CTR compared
with a CBR on capsular bag shrinkage. The influence ofa CBR or CTR on capsular bag shrinkage over a 3-month
follow-up was quantified. Shrinkage prevention of the cap-
sular bag by the CBR, and to a lesser extent by the CTR,
over 3 months was evaluated. The most shrinkage occurred
between the first postoperative day and the first postopera-
tive month. During a multivariate reanalysis of the data by
means of multiple logistic regression modeling, no signifi-
cant association was observed between the preoperativebiometric characteristics (ie, AL, anterior chamber depth),
capsulorhexis diameter, and capsular bag shrinkage. The
differences in capsular bag shrinkage among groups
(CBRCCMR, CTRCCMR, CMR only) were statistically
223225 293528 273125N = CMRCTR + CMRCBR + CMR
rela
tive
shrin
kage
[pos
t / p
re]
1,10
1,05
1,00
,95
,90
,85
,80
Figure 5. Nonparametric box plots for the relative shrinkage (post/pre) of
the capsular bag diameter in groups 1 (CBRCCMR), 2 (CTRCCMR), and 3
(CMR). Horizontals indicate medians and quartiles (minimum and maxi-
mum values), which do not exceed a deviation from the quartiles of
more than 1.5 times the interquartile ranges. B Z statistical outliers
with deviation from the quartiles of more than 1.5 times the interquartile
range. * Z statistical extreme values with deviation from the quartile of
more than 3 times the interquartile range.
VOL 31, OCTOBER 2005

CAPSULAR BAG SHRINKAGE AFTER CAPSULAR RING IMPLANTATION
significant but not clinically relevant in terms of the prespe-
cified order of 0.3 mm. However, the median differences
supported the expected tendency toward a preventive na-
ture of CBRs and, to a somewhat lesser extent, of CTRs.
The CBR group showed few cases of capsular expan-
sion within the first 3 postoperative months. This may berelated to baseline being the intraoperative measurement,
whereas postoperative examinations were performed at
the slitlamp.
One limitation of this conclusion is that it can only be
drawn for the specific types of CBRs, CTRs, and hydropho-
bic acrylic IOLs used in the study. Another point of view
must be considered concerning the control sample: The
CMR was used as a reference to determine the capsularbag size. Although it is made of a soft acrylic material, we
do not know exactly how much capsular bag shrinkage is
prevented by the CMR. In this case, one would expect
even larger differences among treatment groups. At pres-
ent, the CMR is used solely for clinical research purposes.
In another study,15 we compared the elastic boundaries
of 14 commercially available CTRs. We found great differ-
ences in the spring constants among the various types anddesigns, ranging from 0.82 to 4.55 mN/mm. However,
CTRs of the same model had comparable mechanical
properties.
To date, exact measurement of the capsular bag diam-
eter in vivo remains a challenge. Vass et al.21 measured the
distance between the ends of a CTR through a gonioscopy
lens by adjusting the slit height. This distance was added to
the known length of the CTR to calculate the capsular bagcircumference and from this, the capsular bag diameter by
means of a regression formula. However, magnification of
the cornea by 3-mirror contact glass and material depend-
ing magnification constrain the measuring results.
The method used in this study was first introduced by
Tehrani et al.,2 who found, using a CMR, capsular bag
shrinkage of almost 14% in 55 patients, from a mean of
10.53 mm at the time of surgery to 9.07 mm after 3 months.Capsular bag shrinkage in our control group (in which only
a measuring ring was implanted) was only about 5%. Teh-
rani et al.2 found an increase in the capsular bag shrinkage
with eyes of greater length. Therefore, only eyes with an AL
of 21.5 to 26.5 mm were included in our study.
Nishi et al.16 investigated the inhibitory effect of a CTR
on migrating lens epithelial cells (LECs) in rabbit eyes.
These authors used a CTR with a 14.0 mm diameter(1.0 mm wide and 0.2 mm thick). After cataract surgery,
a PMMA IOL was implanted in the capsular bag in 5 rabbit
eyes. The authors found an accumulation of LECs at the
equatorial corner outside the haptic or ring, showing the
inhibition of LEC migration. The control group showed
markedly less inhibition of LEC migration on macroscopic
and microscopic observations.16
J CATARACT REFRACT SURG -
Nishi and coauthors17 examined the effect of an equa-
torial PMMA CBR in another study. They performed a pro-
spective randomized trial of 100 patients requiring bilateral
cataract surgery. Each patient received a Hydroview hydro-
gel IOL (Storz Ophthalmics) with a CBR in 1 eye and a Hy-
droview IOL without the CBR in the fellow eye. After 6months, there was significantly less PCO in the eyes with
the CBR, with no constriction of the anterior capsule open-
ing and fewer capsule folds.17
Lee and coauthors8 examined the effect of a CTR on
the tilting and decentration of IOLs after cataract surgery
in 40 eyes of 20 patients. They performed an intraindivid-
ual comparison; 1 eye received a hydrophobic IOL and
a CTR, and the fellow eye received only the IOL. The post-operative IOL position was measured with a Scheimpflug
camera anterior eye segment analysis system. The eyes
with both an IOL and a CTR had significantly less IOL de-
centration and tilting than eyes with an IOL only. Lee and
coauthors concluded that a CTR seemed effective in pre-
serving capsule integrity and IOL position.
Strenn and coauthors9 described 19 eyes (13 patients)
that had clear corneal cataract surgery with implantation ofa foldable, open-loop, silicone posterior chamber IOL. At
the same time, an open PMMA CTR (Morcher type 14 or
14A) was inserted to allow measurement of capsular bag
circumference and diameter. They measured the distance
between the ends of the 2 eyelets of the CTR gonioscopi-
cally at the slitlamp by adjusting the slit height to the dis-
tance in between as described by Vass et al.21 The authors
found a significant decrease in the capsular bag circumfer-ence of 2% G 1.5% within a 3-month follow-up. These re-
sults are similar to our results of capsular bag shrinkage
with the CTR. We found a shrinkage of 2.9% in this group.
Strenn and coauthors further reported that although the de-
crease in the capsule bag circumference was similar with
both ring types from 1 week to 1 month, capsule contrac-
tion continued for 2 months with the smaller ring (type
14 Z 10.0 mm in diameter) but ceased with the largerring (12.0 mm in diameter). These authors concluded
that the diameter of the capsular bag could be calculated
in the living eye and that the influence of the CTR itself
on capsular bag shrinkage remained to be established.
In conclusion, capsular bag shrinkage can be inhibited
by a CBR and, to a lesser extent, by a CTR. The effect of
a CTR on capsular bag shrinkage in a normal eye is depen-
dent on the design and the diameter of the CTR. It is prob-ably further dependent on the type, diameter, and material
of the IOL. Larger eyes ofO27.0 mm respond with greater
capsular bag shrinkage.2 Therefore, in these eyes, a larger
CTR diameter is preferred. Further study is necessary to
evaluate the influence of other CTR designs on capsular
bag shrinkage. The reduction in the capsular bag shrink-
age after CTR implantation may reduce the incidence of
VOL 31, OCTOBER 2005 1919

CAPSULAR BAG SHRINKAGE AFTER CAPSULAR RING IMPLANTATION
IOL dislocation and tilt, helping to maintain postoperative
visual acuity.
REFERENCES
1. Apple DJ, Solomon KD, Tetz MR, et al. Posterior capsule opacification.
Surv Ophthalmol 1992; 37:73–116
2. Tehrani M, Dick HB, Krummenauer F, Pfirrmann G, et al. Capsule mea-
suring ring to predict capsular bag diameter and follow its course after
foldable intraocular lens implantation. J Cataract Refract Surg 2003;
29:2127–2134
3. Cionni RJ, Osher RH. Endocapsular ring approach to the subluxated
cataractous lens. J Cataract Refract Surg 1995; 21:245–249
4. Cionni RJ, Osher RH. Management of profound zonular dialysis or
weakness with a new endocapsular ring designed for scleral fixation.
J Cataract Refract Surg 1998; 24:1299–1306
5. Cross HE, Jensen AD. Ocular manifestations in the Marfan syndrome
and homocystinuria. Am J Ophthalmol 1973; 75:405–420
6. Gimbel HV, Sun R, Heston JP. Management of zonular dialysis in pha-
coemulsification and IOL implantation using the capsular tension ring.
Ophthalmic Surg Lasers 1997; 28:273–281
7. Sun R, Gimbel HV. In vitro evaluation of the efficacy of the capsular
tension ring for managing zonular dialysis in cataract surgery. Oph-
thalmic Surg Lasers 1998; 29:502–505
8. Lee DH, Shin SC, Joo CK. Effect of a capsular tension ring on intraocular
lens decentration and tilting after cataract surgery. J Cataract Refract
Surg 2002; 28:843–846
9. Strenn K, Menapace R, Vass C. Capsular bag shrinkage after implanta-
tion of an open-loop silicone lens and a poly(methylmethacrylate)
capsule tension ring. J Cataract Refract Surg 1997; 23:1543–1547
10. Dick HB, Augustin AJ. Lens implant selection with absence of capsular
support. Curr Opin Ophthalmol 2001; 12:47–57
J CATARACT REFRACT SURG1920
11. Nishi O, Nishi K, Menapace R, Akura J. Capsular bending ring to pre-
vent posterior capsule opacification: 2 year follow-up. J Cataract Re-
fract Surg 2001; 27:1359–1365
12. Dick HB, Schwenn O, Pfeiffer N. Implantation of the modified en-
docapsular bending ring in pediatric cataract surgery using a vis-
coadaptive visoelastic agent. J Cataract Refract Surg 1999; 25:
1432–1436
13. Menapace R, Findl O, Georgopoulos M. The capsular tension ring: de-
signs, applications and techniques. J Cataract Refract Surg 2000;
26:898–912
14. Dick HB, Schwenn O. Der Kapselknickring. Ophthalmologe 1999;
96:114–119
15. Kurz S, Dick HB. Spring constants of capsular tension rings. J Cataract
Refract Surg 2004; 30:1993–1997
16. Nishi O, Nishi K, Mano C, et al. The inhibition of lens epithelial cell mi-
gration by a discontinuous capsular band created by a band-shaped
circular loop or a capsule-bending ring. Ophthalmic Surg Lasers 1998;
29:119–125
17. Nishi O, Nishi K, Menapace R. Capsule bending ring for the prevention
of capsular opacification: a preliminary report. Ophthalmic Surg La-
sers 1998; 29:749–753
18. Nishi O. New posterior chamber lens with open circular haptic for
a small capsular opening: preliminary report. J Cataract Refract Surg
1990; 16:640–643
19. Werner L, Pandey SK, Apple DJ, et al. Anterior capsule opacification;
correlation of pathologic findings with clinical sequelae. Ophthalmol-
ogy 2001; 9:1675–1681
20. Dahlhauser MD,Wroblewski KJ, Mader T. Anterior capsule contraction
with foldable silicone intraocular lenses. J Cataract Refract Surg 1998;
24:1216–1219
21. Vass C, Menapace R, Schmetterer K, et al. Prediction of pseudophakic
capsular bag diameter based on biometric variables. J Cataract Refract
Surg 1999; 25:1376–1381
- VOL 31, OCTOBER 2005