cardiac rehab
TRANSCRIPT

REHABILITASI JANTUNG MELALUI PROGRAM LATIHAN PADA PENDERITA PENYAKIT JANTUNG KORONER
- Uswa Malik*, Muzakkir -
CARDIOVASCULAR DEPARTMENTMEDICAL FACULTY HASANUDDIN UNIVERSITY

INTRODUCTION

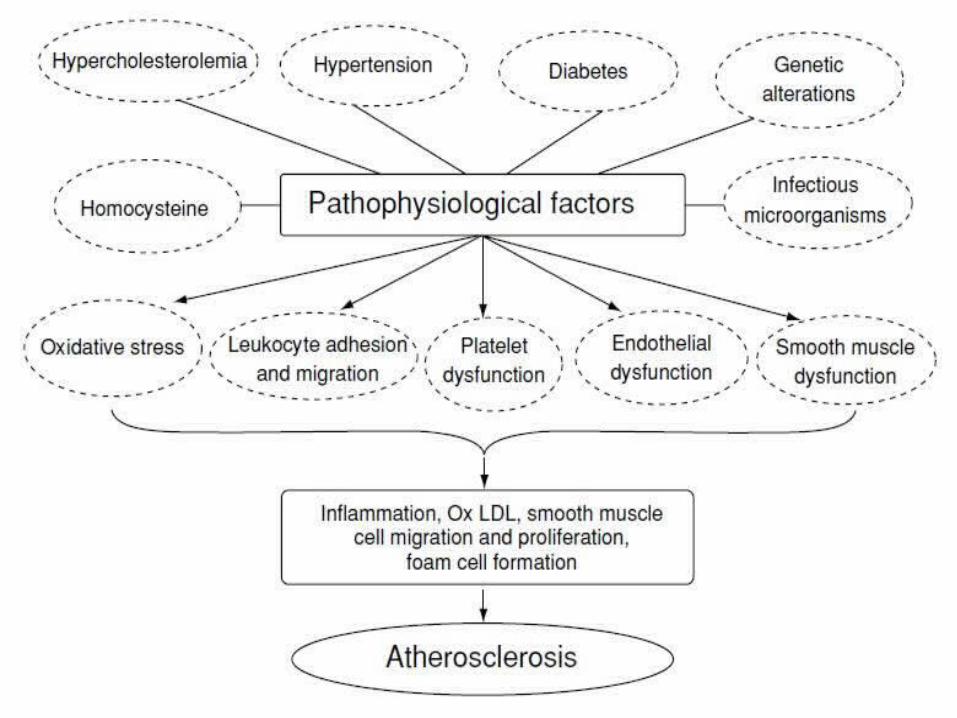
Atherosclerosis

Definition of CR
• Coordinated, multifaceted interventions designed to optimize a cardiac patient’s physicial, psychological, and social functioning, in addition to stabilizing, slowing or even reversing the progression of the underlying atherosclerotic process, thereby reducing morbidity and mortality
AHA Scientific Statement, Circ 2005;111:369-76

The History of Cardiac Rehabilitation (US)1912 Herrick J.B. Association of American Physicians Modern Concept of coronary thrombosis and
myocardial infarction (MI)1912 – 1950 Lewis T
Absolute bed rest 6-8 wks with total nursing care to prevent further ischemic, LV aneurysm, ventricular
rupture, arrhythmia, recurrent MI, sudden cardiac death1951 Levine SA & Lown B
Encourage pt to sit 1-2 hours from D1 of MI to avoid deconditioning
1951-1960s Practices varies Bed rest 1day – 4 weeks
Hospitalization 2-6 weeks1964 WHO: Rehabilitation of Patients with Cardiovascular
Diseases. (Technical report Series No 270) Geneva1971 Wenger NK, Gilbert C., Skoropa M.; Cardiac conditioning after
myocardial infarction. An early intervention program. J. Card. Rehabil2:17, 1971
Benefits of CR
• Limit the adverse physiologic effects of cardiac illness
• Limit the adverse psychological effects of cardiac illness
• Reduce the risk of sudden death or reinfarction• Control cardiac symptoms
• Stabilize or reduce atherosclerosis
• Improve functional capacity• Enhance psycho-social and vocational status


Phases of Cardiac Rehabilitation
• Phase I : Inpatient
• Phase II: Outpatient EKG monitored
• Phase III: Outpatient with decreasing monitoring
• Phase IV: Community based, independent exercise

Inpatient Cardiac Rehabilitation Principles
• Goals– normal cardiovascular response to changes in position and ADLs
– reach 3-4 MET activity level by discharge
• Activity--Slow progression of activity intensity (increase by 1 MET/day)
Initiating Inpatient Cardiac Rehab
• Post-MI, Post-surgery, Post-stent (no MI), CHF, heart transplant
• Patient may begin if:– No chest discomfort (8 hours)– No new signs of decompensated heart failure
– No abnormal EKG changes (8 hours)
Cardiac Rehab Phase II
• Supervised outpatient program 6-8 wks• Exercise test performed prior to rehab• EKG monitoring every session• Goals - increase exercise capacity to 5 METS• Patient education on HR, exercise, symptoms
Phase III Outcomes
• Functional capacity goals > 8 METS or 2x energy requirements of work
• Training effects expected• No cardiac symptoms• EKG monitoring happens occasionally, or when
increasing activity parameters
• Patients learn self-monitoring of HR and symptoms
Cardiac Rehab Phase IV
• Unsupervised program
• Community Based

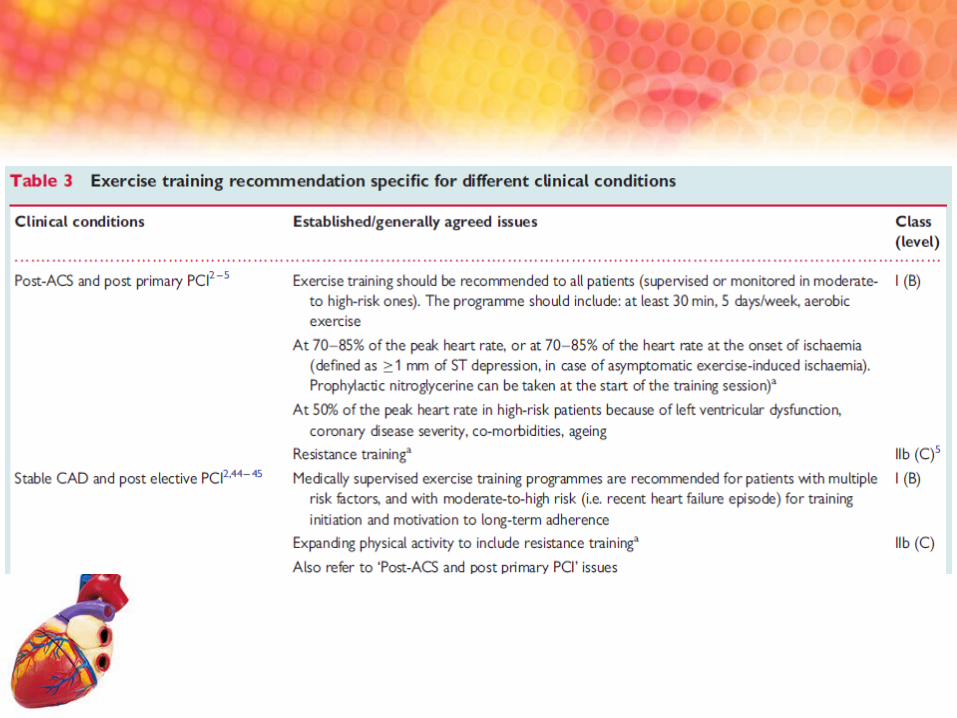
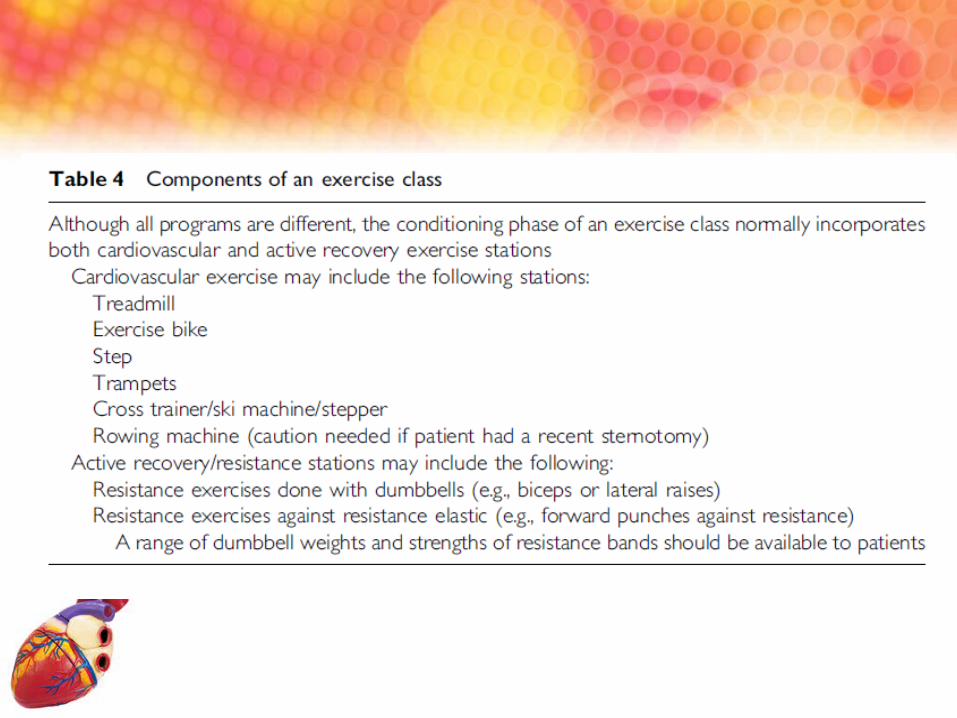
Exercise training programme
• Exercise training is defined as a sub-category of physical activity in which planned, structured, and repetitive bodily movements are performed to maintain or improve one or more attributes of physical fitness and thus it is a structured intervention over a defined period of time.
The Benefits of Exercise Primary Prevention
• Brisk walking, 30mins/day, 5 times/week– 30% ↓vascular events in 3.5 years follow-up1
• 3 hours of brisk walking/week = 1.5 hours of vigorous exercise per week2
• Resistance exercise and weight training were also beneficial3
1. Manson JE, Greenland P, LaCroix AZ, et al: Walking compared with vigorous exercise for the prevention of cardiovascular events in women N Eng J. Med 347;716, 2002
2. Manson JE, Hu FB, Rich Edward JW , et al: a prospective study of walking as compared with vigouous exercise in the prevention of coronary artery disease in women. N Eng J. Med 341:650, 1999
3. Tanasescu M, Leitzmann MF, Rimm EB, et al: Exercise type and intensity in relation to coronary heart disease in men. JAMA 288:1994, 2002

The Benefits of Exercise Secondary Prevention
Physical activity with 1000kcal/wk – 20-30% ↓ all cause mortality1
For patients without revascularization– Exercise training improves SBP, angina symptoms and
exercise tolerance2
For patients with revascularization– Improvement in exercise tolerance– ↓29% cardiac events – ↓re-admissions (18.6 vs 46%)3
1. Lee I-M, Skerett PJ: Physical activity and all-cause mortality—What is the dose response relation? Med. Sci Sports exerc33(6Suppl):S459,2001
2. Hambrecht R. Wolf A, Gielen S, et al: Effects of exercise on coronary endoothelial function in patients wwith coronary artery disease. Am J Cadriol 90:124, 2002
3. Belardinelli R, Paolini I, Cianci G, et al: Exercise training intervention after coronary angioplasty: The ETICA trial. J Am Coll Cardiol 37:1891, 2001
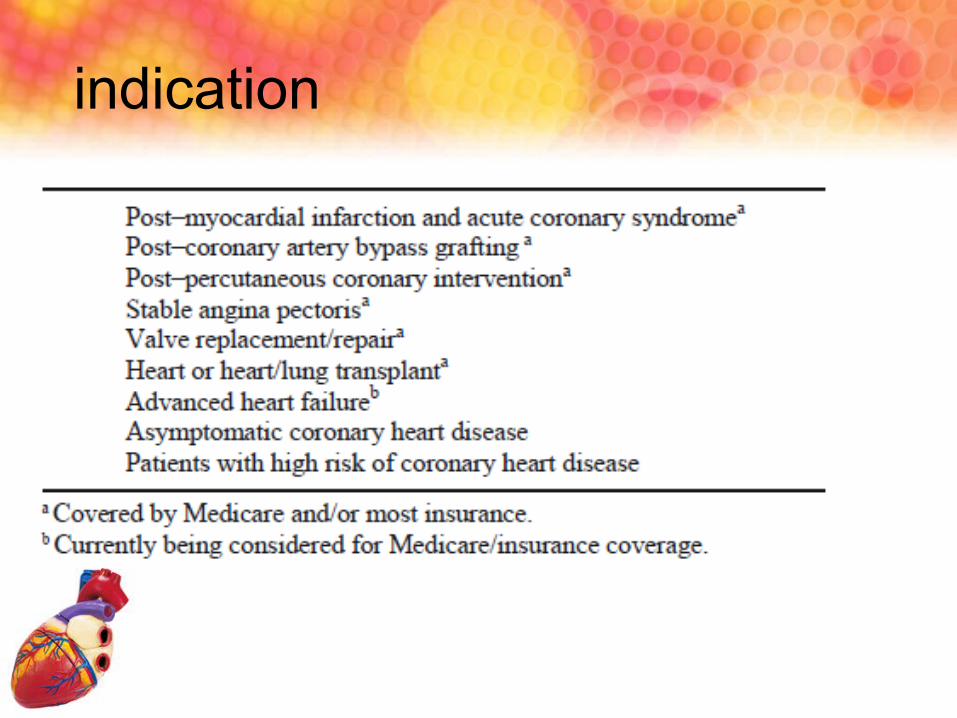
indication

Absolute Acute myocardial infarction (within two days) Unstable angina Uncontrolled cardiac arrhythmias causing symptoms or homodynamic
compromise Symptomatic severe aortic stenosis Uncontrolled symptomatic heart failure Acute pulmonary embolus or pulmonary infarction Acute myocarditis or pericarditis Active endocarditis Acute aortic dissection Acute noncardiac disorder that may affect exercise performance or be
aggravated by exercise Inability to obtain consent
Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation 2001; 104:1694

Left main coronary stenosis or its equivalent Moderate stenotic valvular heart disease Electrolyte abnormalities Severe hypertension (systolic 200 mmHg and/or diastolic 110 mmHg) Tachyarrhythmias or bradyarrhythmias, including atrial fibrillation with
uncontrolled ventricular rate Hypertrophic cardiomyopathy and other forms of outflow tract
obstruction Mental or physical impairment leading to inability to cooperate High-degree atrioventricular block
Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation 2001; 104:1694;

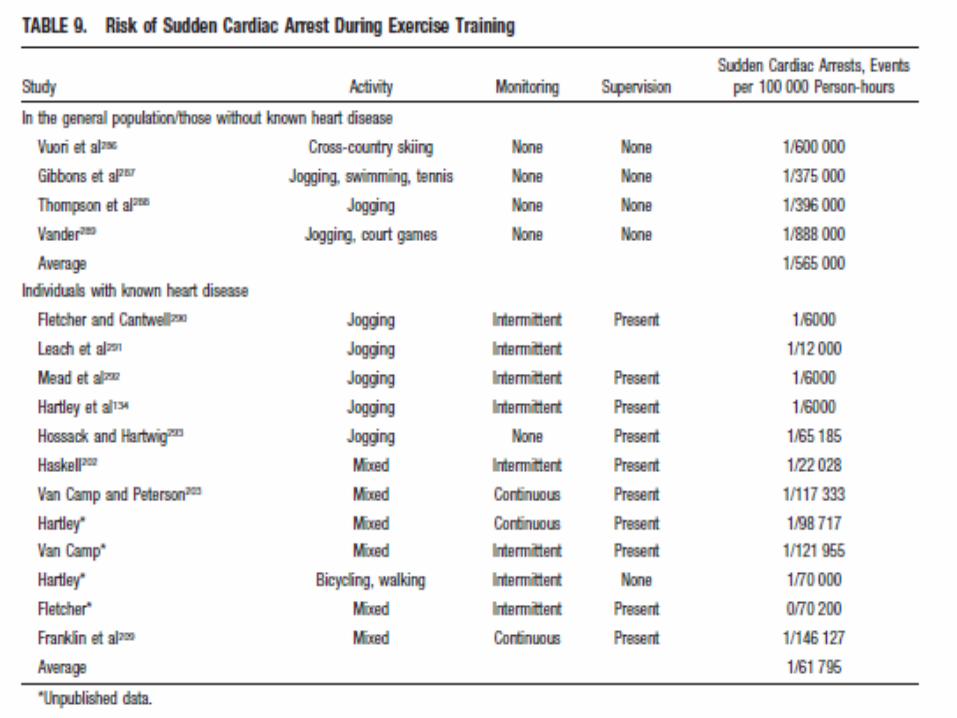
Safety of Exercise
Exercise without medical advice:– Sudden Cardiac Arrest: 1 per 60,000 pt. hours1
Supervised Programs:– Cardiac events: 8.9 per 1,000,000 pt. hours– Myocardial Infarction: 3.4 per 1,000,000 pt. hours– Mortality: 1.3 per 1,000,000 pt.hours 2
1. Fletcher GF, Balady GJ, Amsterdam EA, et al: Exercise standards for testing and training: A statement for healthcarecare professionals from the American Heart Association. Circulation 104:1694, 2001
2. Ades PA: Cardiac rehabilitation and secondary prevention of coronary heart disease. N Eng J Med 345:892, 2001

25
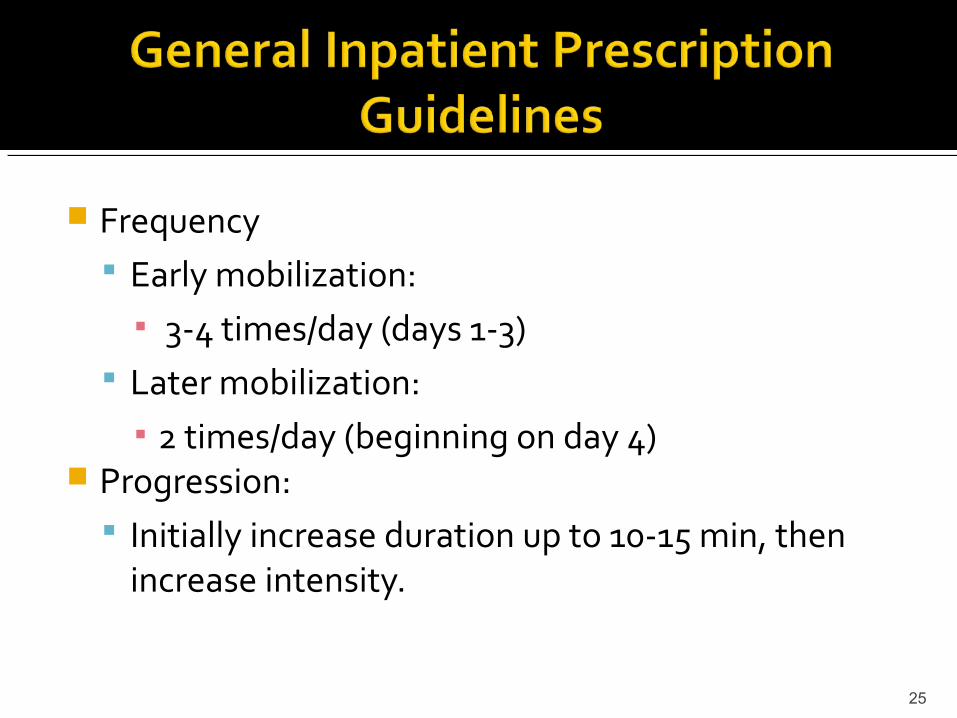
Frequency Early mobilization:
▪ 3-4 times/day (days 1-3) Later mobilization:
▪ 2 times/day (beginning on day 4) Progression:
Initially increase duration up to 10-15 min, then increase intensity.

26
Selected moderate to high risk patients should be encouraged to participate in outpatient cardiac rehabilitation programs &/or
Manage their discharge rehabilitation plan and report any cardiovascular symptoms promptly (should they occur).

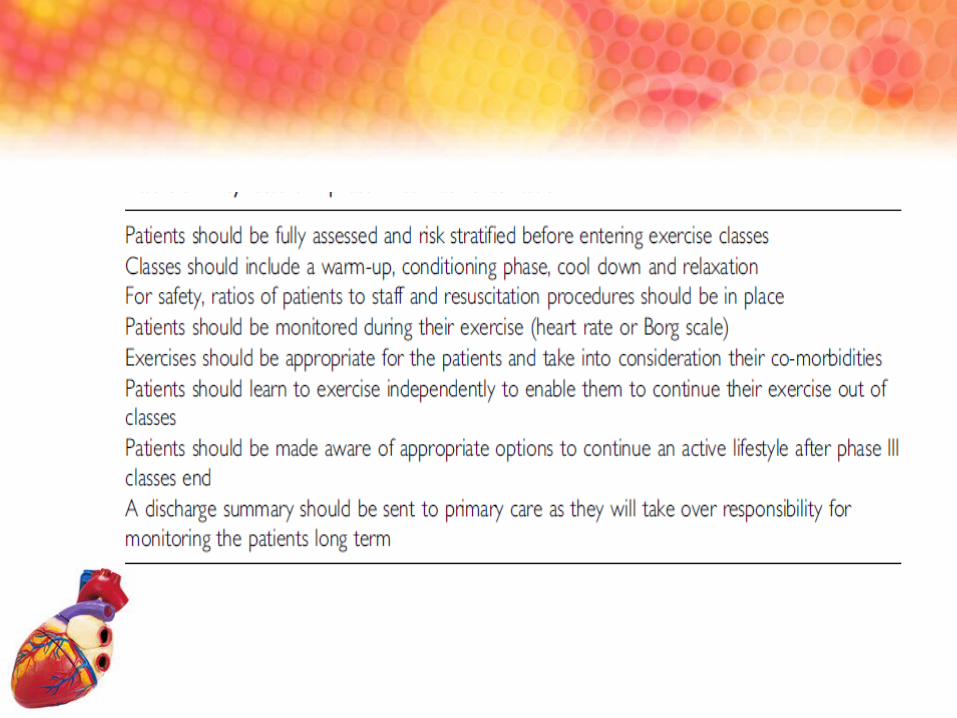
Risk stratification

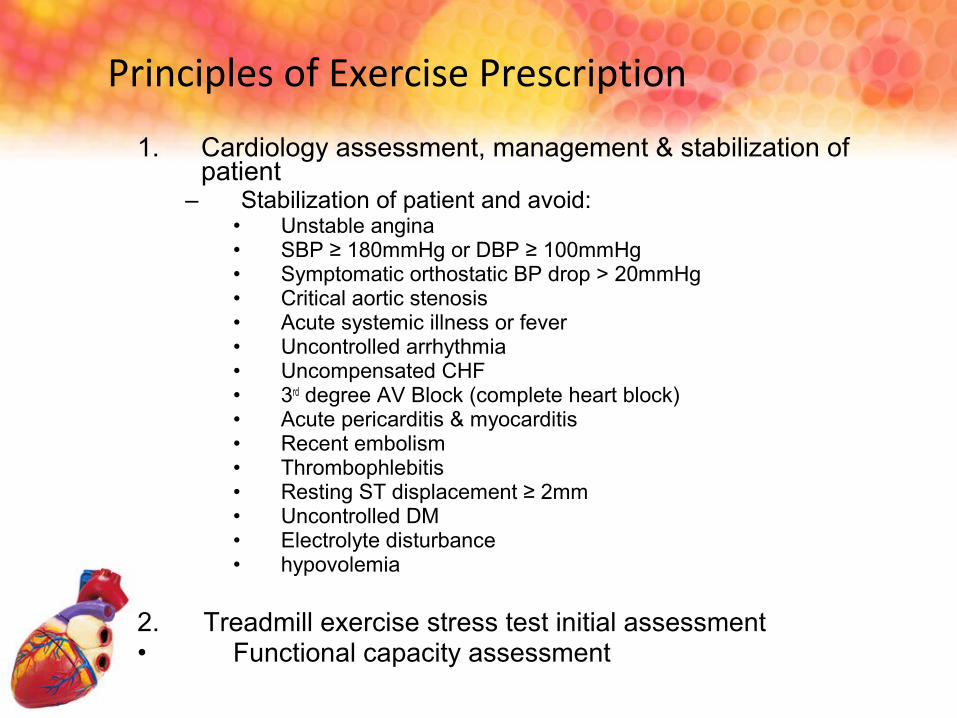
1. Cardiology assessment, management & stabilization of patient
– Stabilization of patient and avoid:• Unstable angina• SBP ≥ 180mmHg or DBP ≥ 100mmHg• Symptomatic orthostatic BP drop > 20mmHg• Critical aortic stenosis• Acute systemic illness or fever• Uncontrolled arrhythmia• Uncompensated CHF• 3rd degree AV Block (complete heart block)• Acute pericarditis & myocarditis• Recent embolism• Thrombophlebitis• Resting ST displacement ≥ 2mm• Uncontrolled DM• Electrolyte disturbance• hypovolemia
2. Treadmill exercise stress test initial assessment• Functional capacity assessment
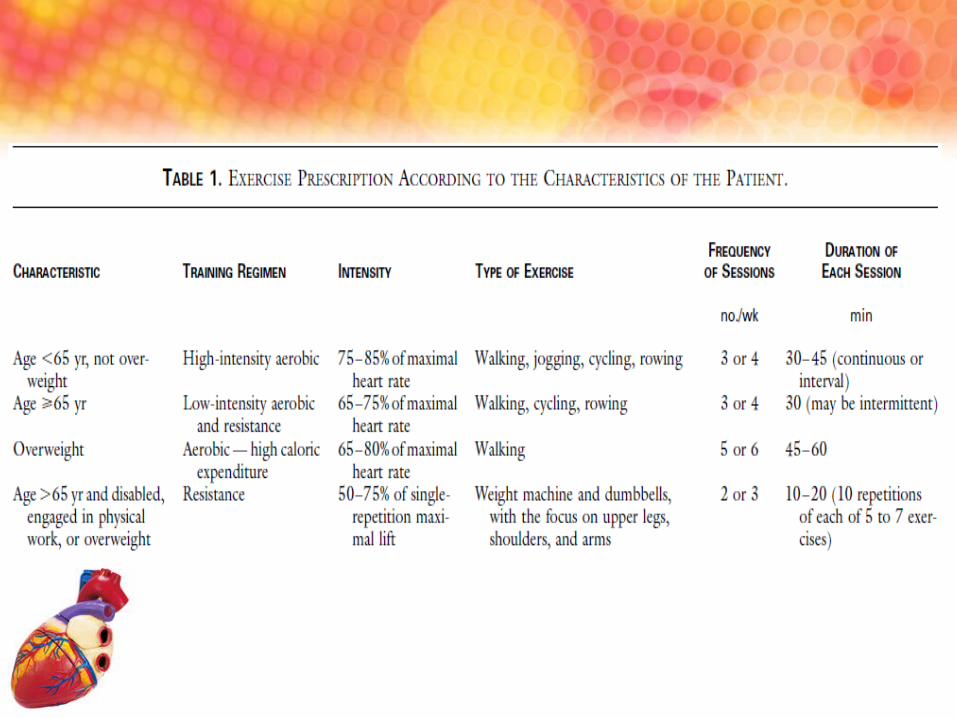
Principles of Exercise Prescription

3. Tips on Exercise prescription

4.Regular clinical follow-up for exercise progress and symptoms reassessment– To assess the cardiovascular status
• Chest pain, dizziness, palpitation, dypsnoea, appetite, resting BP & P.
– To assess the progress of exercise tolerance– Advancing the prescription according to
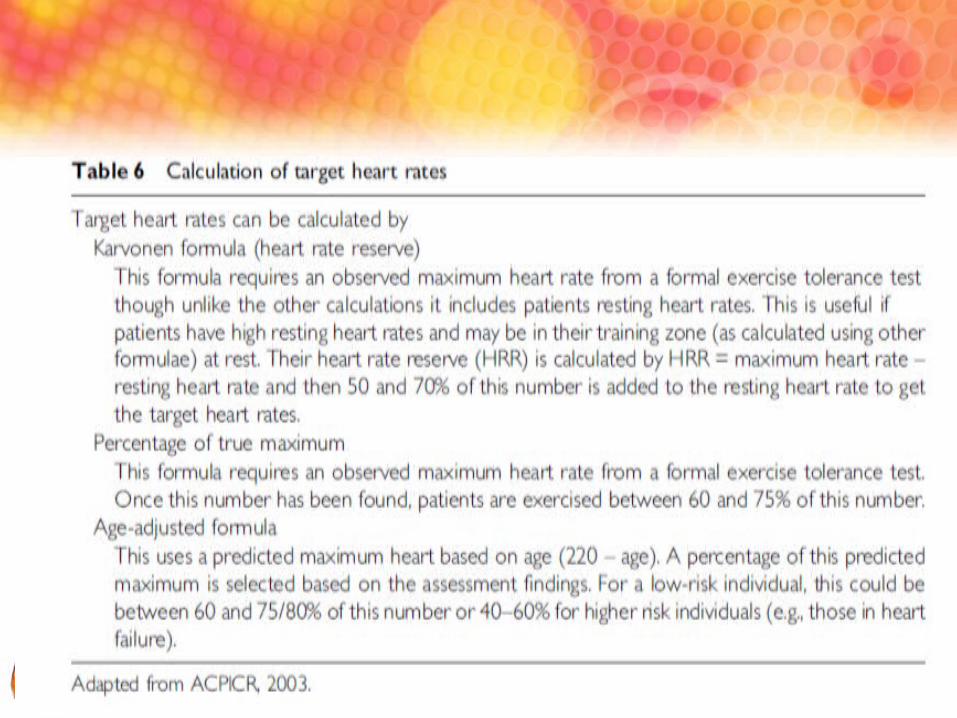
• The improvement in fitness• To increase in steps of 5 – 10% of max. heart rate• To maintain ~ 85% of max. heart rate during the whole
exercise session

Exercise stress test after MI