cardiotoxicity of chemotherrapy
TRANSCRIPT
CARDIAC TOXICITY OF CHEMOTHERAPIES
JOYDEEP GHOSH
Introduction…
• With the improvement in cancer care- the concern for toxicity comes into play
• Cells which are rapidly dividing– bear the brunt of major toxicities
• Cardiac myocytes have limited regenerative capacity
• So, they are susceptible to permanent side effects
Drugs…
• Anthracyclins , anthraquinones
• Bleomycin, mitomycin C
• Etoposide
• Alkylating agents
• Antimicrotubule agents
• Antimetabolites
• ATRA, arsenic
• Targeted therapy agents, esp herceptin
Anthracyclins..
• Once developed, carries poor prognosis and often fatal
• Types:
– Acute and subacute
– Chronic
Acute…
• Develops in 2-3 days , can be prolonged uptoweeks in subacute variety
• Incidence– 11%
• C/o: chest pain, palpitations
• Patho: myopericarditis, due to edema of myofibrils and pericardial mesothelium
• ECG: PSVT, sinus tachy, premature atrial and vent complexes
• Acute LVF: very rare but usually reversible
Chronic..
• Incidence much lower: 1.3%
• It is usually evident within 30 days of administration of its last dose, but it may occur even after 6–10 years after its administration
• Risk factors:– other cardiotoxic agents, mediastinal RT
– Extremes of age
– Prior CV morbidity
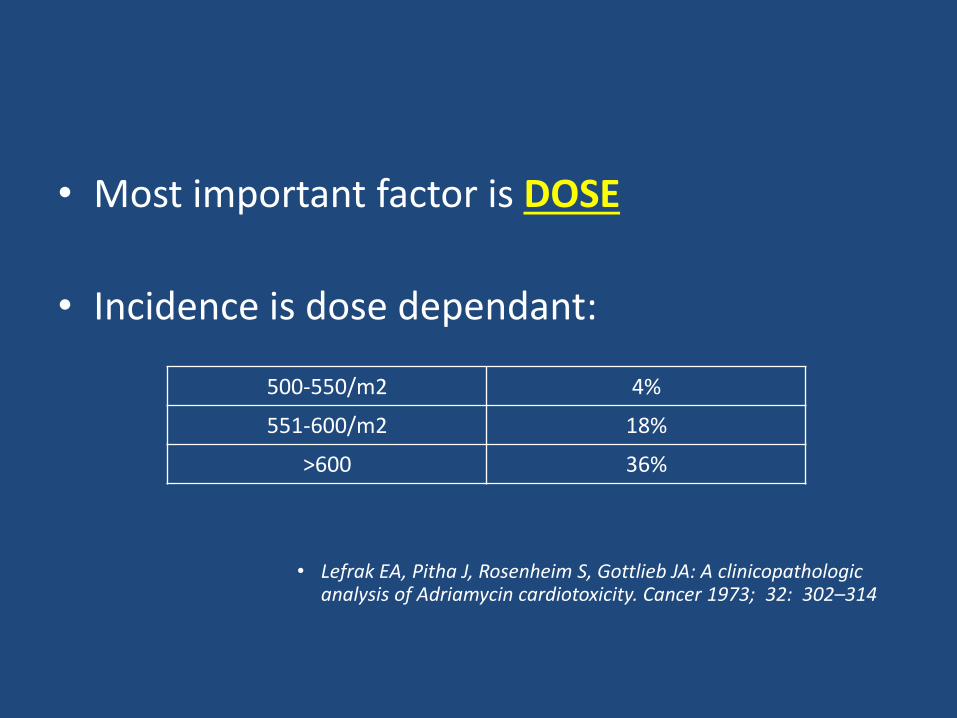
• Most important factor is DOSE
• Incidence is dose dependant:
• Lefrak EA, Pitha J, Rosenheim S, Gottlieb JA: A clinicopathologicanalysis of Adriamycin cardiotoxicity. Cancer 1973; 32: 302–314
500-550/m2 4%
551-600/m2 18%
>600 36%
Morphology and functional changes
• Similar to those of dilated cardiomyopathy
• All 4 chambers are usually dilated
• LVEF and inotropy is reduced
• Concomitant elevation of LVEDP due to diastolic failure
• Wall stress is increased as there is no significant hypertrophy
• Mural thrombi may be present
Histopathology…
• Patchy myocardial interstitial fibrosis with scattered vacuolated myocytes – ADRIA cells
• Fibroblastic proliferation and histiocyticinfiltration
• Partial / total loss of myofibrils and vacuolar degeneration is essential
• Distension of sarcoplasmic reticulum
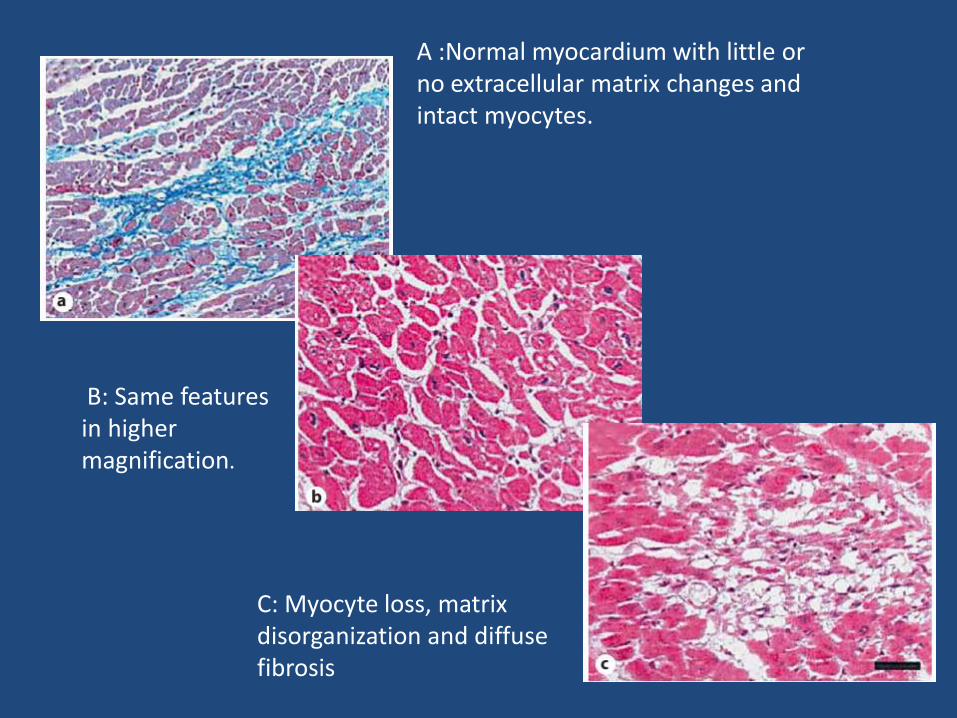
A :Normal myocardium with little or no extracellular matrix changes and intact myocytes.
B: Same features in higher magnification.
C: Myocyte loss, matrix disorganization and diffuse fibrosis
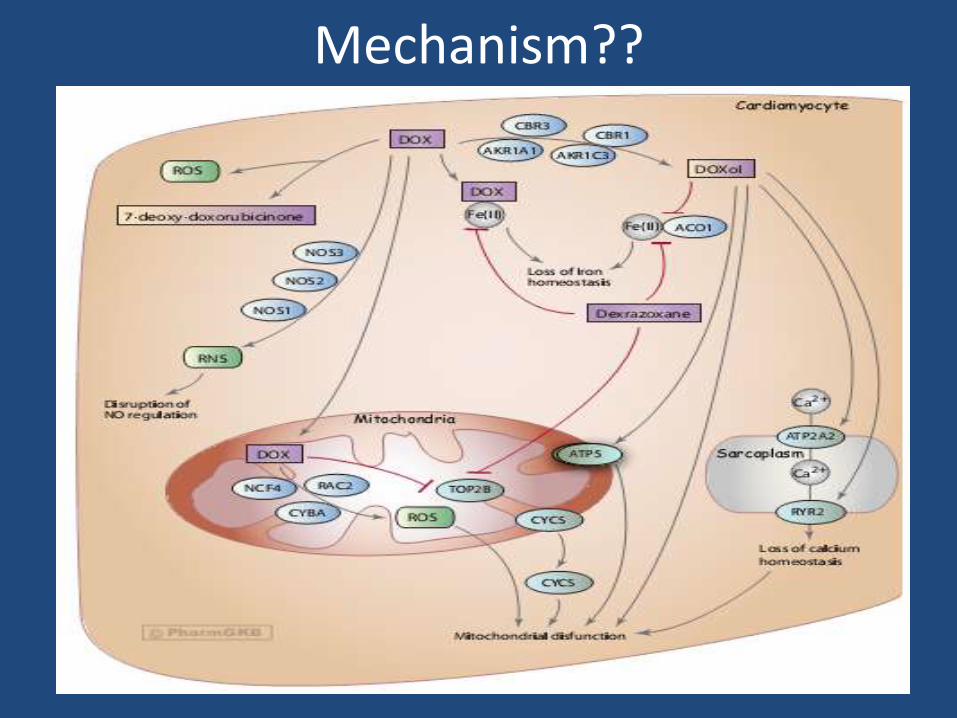
Mechanism??
DIAGNOSIS
• History and physical examination– Elevated JVP
– S3 gallop
• ECG: nonspecific ST-T changes with low voltage QRS complexes
• CXR, echo
• Radionuclide ventriculography has been used to assess LV systolic and diastolic function– Impaired glucose and fatty acid metabolism has been
observed in doxorubicin cardiomyopathy
• Antimyosin antibody study with the use of 111 In-labeled monoclonal antimyosin antibody is used for the diagnosis of myocarditis and has also been employed for the diagnosis of doxorubicin cardiomyopathy
• Highly sensitive
• Annexin V, which has high affinity for membrane -bound phosphatidylserine, has been used to detect apoptosis induced by doxorubicin
• In case of CHF, cardiac troponins and BNP are useful
• The endomyocardial biopsy may reveal characteristic diagnostic features of doxorubicin cardiomyopathy.
• Required for diagnosis are:– loss of myofibrils,
– distention of sarcoplasmic reticulum
– vacuolization of the cytoplasm
Doxorubicin in lymphoma ..
Total 141 ptsAverage dose 250 – 550 /m2Results: Clinical CHF: only 1 ptSubclinical decline in LVEF <25% of baseline: 28%Risk factor analysis: AGE and MALE SEX to be the most significant factor
Management..
• No specific therapy
• Metoprolol is safe and effective
• ACEI, diuretics when HF develops
• ICD – in case of arrythmia and LVEF <40 with NYHA 3-4 symptomatology
Prevention..
• Major emphasis has been to limit the cumulative dose of doxorubicin to <450 mg/m2
• continuous slow infusion
• Most of the pharmacologic agents that have been tested to reduce or prevent doxorubicin cardiotoxicity have the potential to reduce oxidative stress
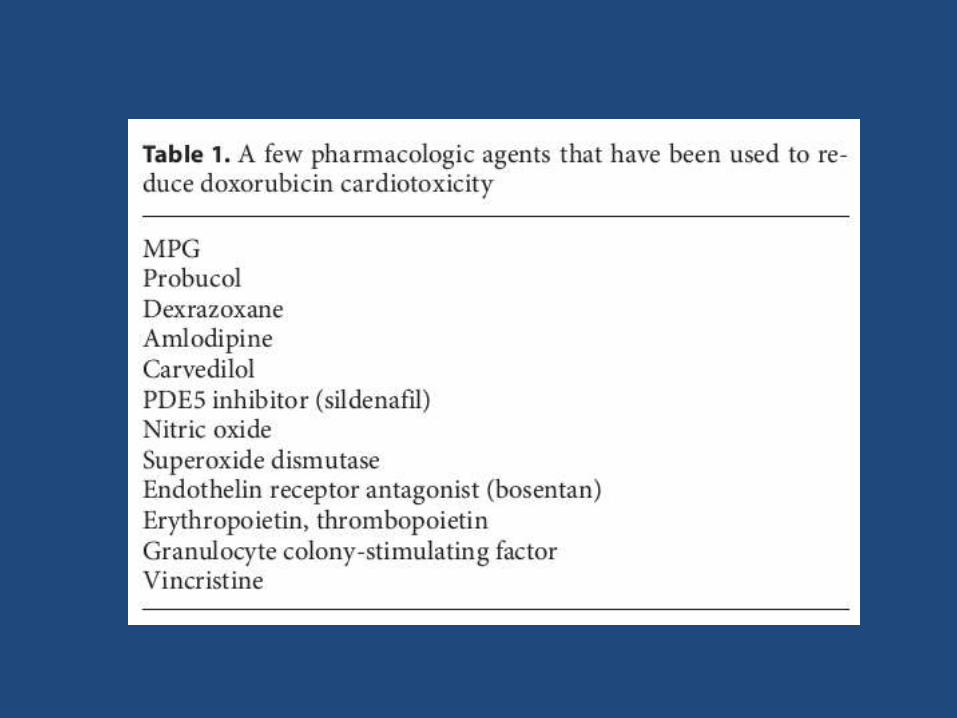
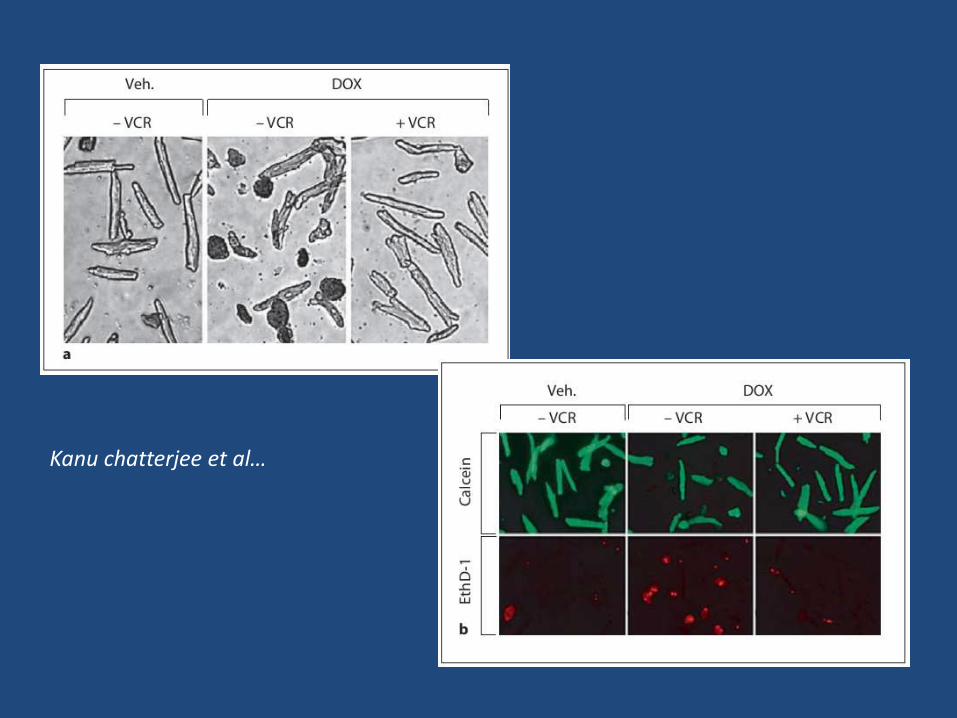
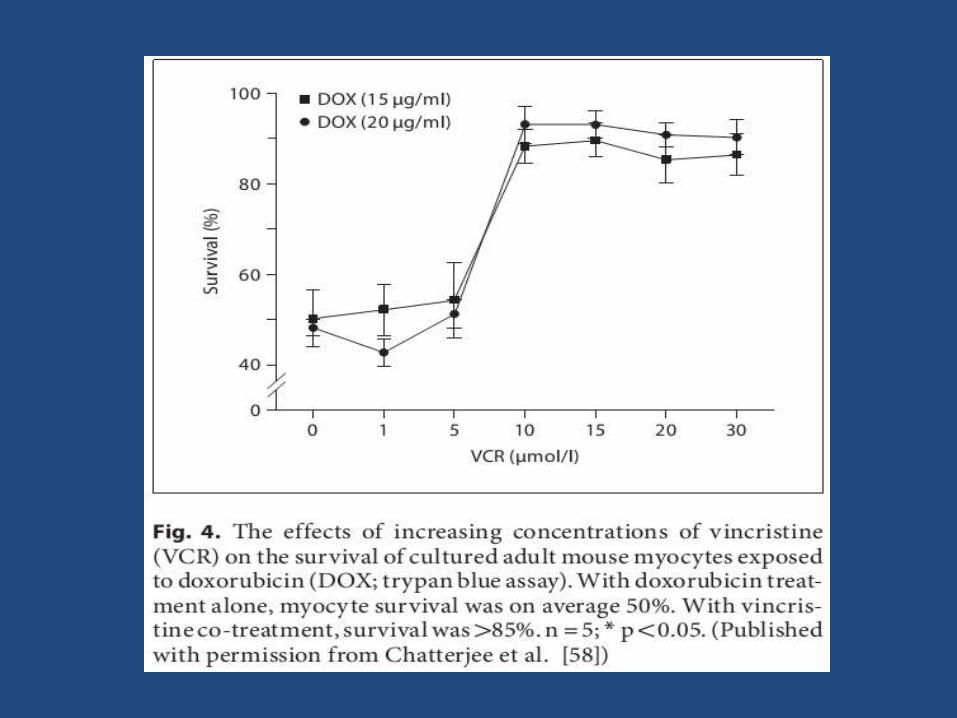
Kanu chatterjee et al…
Dexrazoxane..
• Used successfully to reduce cardiac toxicity in patients receiving anthracycline-based chemotherapy for cancer (predominantly women with advanced breast cancer)
• MOA: iron chelation in the cells.
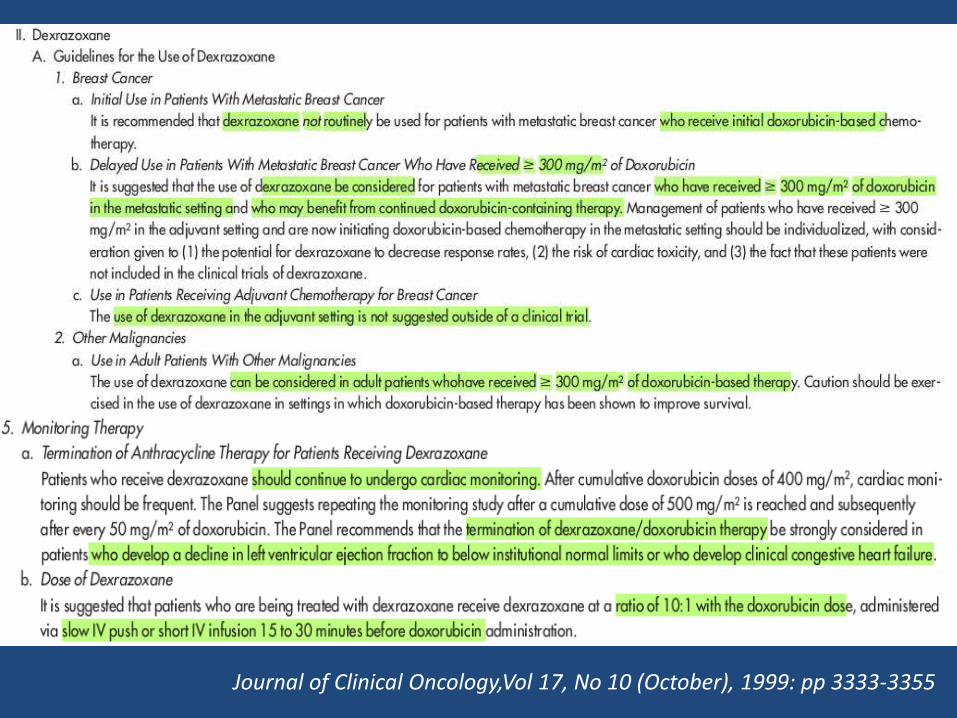
Journal of Clinical Oncology,Vol 17, No 10 (October), 1999: pp 3333-3355
• 101 pts in doxo alone arm/ 105 pts in doxo+dexra arm• Median cumulative dose of doxo: 300mg/m2• Method: serial monitoring of Trop t in both the groups• Results:
– Trop T elevation in 35%pts– Elevated trop T levels (50% vs 21%, P<0.001)– extremely elevated troponin T levels (32 percent vs. 10 percent, P<0.001)– Median follow up is 2.5 yrs– Rate of event-free survival at 2.5 years was 83 percent– in both groups (P=0.87 by the log-rank test)
Anthraquinones…
• Mitoxantrone is an anthraquinone designed to yield broad spectrum antitumor activity similar to the anthracyclines
• Phase I and phase II studies -- dose-related cardiac failure and arrhythmias
• Doses greater than 160/ mg/m2
• Incidence:• Subclinical mod to severe decline: 13%
• Overt cardiac failure: 2.3%
Other drugs..
• Vinca alkaloids:
– Hypertension, myocardial ischemia, myocardial infarction, and other vaso-occlusive complications have been implicated with the use of these drugs
– Most common agent is vinblastine
» Harris AL, Wong C. Myocardial ischaemia, radiotherapy, and vinblastine. Lancet 1988;8223:787
» Mandel E, Lewinski U, Djaldetti M. Vincristine-induced myocardial infarction. Cancer 1975;36:1979-1982
Mitomycin C, Bleomycin
• Mito C: cumulative doses greater than 30 mg per m2
• In one report, 5 of 15 patients treated with mitomycin C had myocardial changes that histologically resembled radiation-induced cardiac injury
• Ravry MJ. Cardiotoxicity of mitomycin C in man and animals. Cancer Treat Rep 1979;63:555
Bleomycin
• Pericarditis is an uncommon, but potentially serious, cardiotoxicity
• An acute chest pain syndrome • incidence is less than 3%
• sudden substernal chest pain
• treatment is supportive and discontinuation of the drug is not needed
• May also cause • CAD
• ACS
Topoisomerase II inhibitors
• Etoposide:
– myocardial infarction and vasospastic angina• Schwarzer S, Eber B, Greinix H, et al. Eur Heart J
1991;12:748-750
• Additionally, etoposide is often a part of bleomycin- and cisplatin-based regimens that have been associated with cardiac toxicity
ALKYLATING AGENTS
• At low doses, cyclophosphamide has not been reported to be associated with cardiotoxicity
• Acute cardiac toxicity - doses of 120 to 170 mg per kg over 1 to 7 days as in high dose conditioning regimens for BMT
• Manifestations:– Low voltage QRS
– Nonspecific ST-T changes
– Tachyarrythmia
– CHB
• Acute onset fulminant CHF is seen in 29% cases of high dose therapy
• Mx:
– diuretics,
– ACEI,
– Beta blockers,
– inotropic medications
• Other complications:– Hemorrhagic myopericarditis
• Pathophysiology: endothelial injury
• Onset: usually 1st week of therapy
• Fortunately, most of the effusions can be treated with corticosteroids and analgesics without serious sequelae
Paclitaxel– cardiac arrhythmias, including an asymptomatic
bradycardia that is reversible
– In one phase II study of 45 patients, 13 of the patients treated with paclitaxel developed bradycardia and 2 patients progressed to a higher grade heart block
– It has been suggested that the maximum cumulative doxorubicin dose should be decreased to less than 380/ mg/m2 when it is used in combination with paclitaxel
– Albumin-bound paclitaxel appears to have the same cardiac toxicity as nonalbumin-bound paclitaxel
Docetaxel..
• Conduction abnormalities, cardiovascular collapse, and angina
• Evidence does exist for a potentiating effect of anthracycline cardiomyopathy
Antimetabolites.
• Since then, 5-FU has become the most widely investigated antineoplastic agent known to cause myocardial ischemia
• Ischemic events are more common when this agent is administered in combination with cisplatin
• In a large study of 1140 pts, incidence was 3.1%
• 50% of all patients treated with 5-FU have nonspecific changes on ECG, and
– up to 16% of patients demonstrate ST-T changes
• Precordial chest pain, both anginal and noncardiac, has been reported in patients during continuous drug infusion.
• Rhythm disturbances: vent ectopy, AF
• Mostly occur during 2nd or subsequent infusion
• Symptoms improve with
– Termination of infusion
– Nitrates/CCB
• Prophylactic use of CCB is helpful in prevention
Differentiating agents..
• ATRA:– Approximately 10% to 15% of patients develop a
retinoic acid syndrome (RAS), manifested by fever, dyspnea, pleural effusions, pericardial effusions (with potential for cardiac tamponade), pulmonary infiltrates, peripheral edema, and myocardial ischemia/infarction
• ATO: – prolongation of the QT interval in as high as 63% of
patients and
– Torsades de pointes
• Arsenic induced tachyarrythmia is often drug resistant
• Treatment with parenteral potassium and magnesium, maintaining high normal levels, may be beneficial( K- 4meq/L, Mg- 2mg/dl)
• Specifically, electrolyte and ECG with QT measurement must be obtained before initiating therapy and once or twice weekly during treatment
• Pretreatment QTc should be <500ms
• Arsenic should be discontinued and corrective measures to be started
• If QTc does not correct to <460ms, treatment should be withheld with arsenic

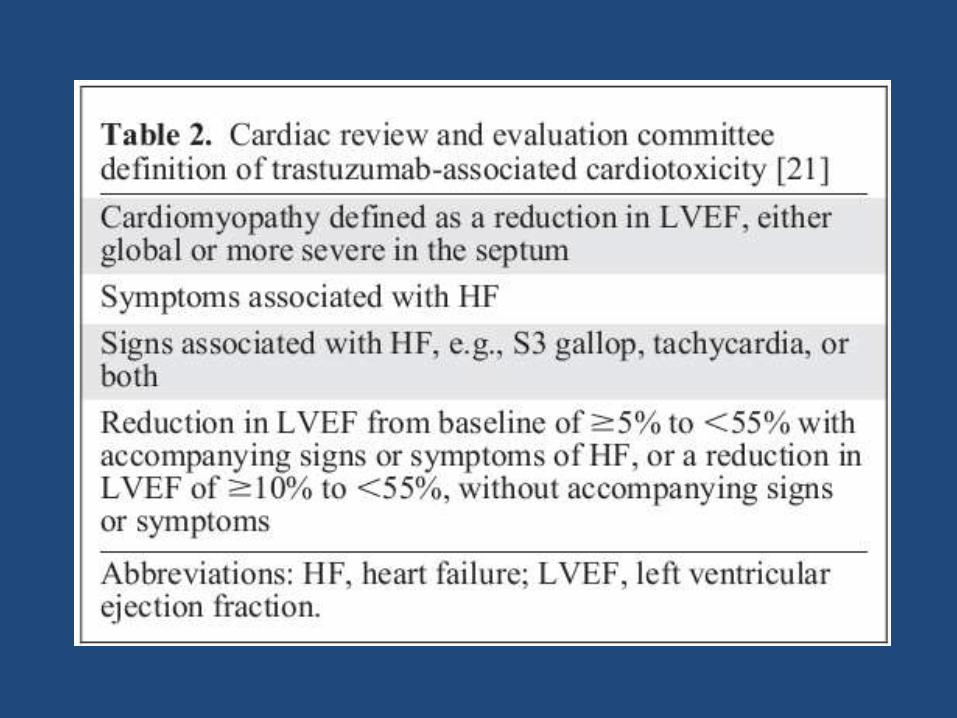
Trastuzumab..
• The incidence rates were
– 2% sincle agent
– 13% + paclitaxel
– 27% + anthracycline
How different from other cardiotoxicities??
• Is not dose-dependent,
• Its clinical manifestations vary between patients,
• It may be reversible, and
• It apparently does not cause ultrastructuralalterations within the myocardium
Management..
• If asymptomatic decline in LVEF:
– ACEI/ARBs/beta blockers stop herceptin
• If symptomatic
– Diuretics add on
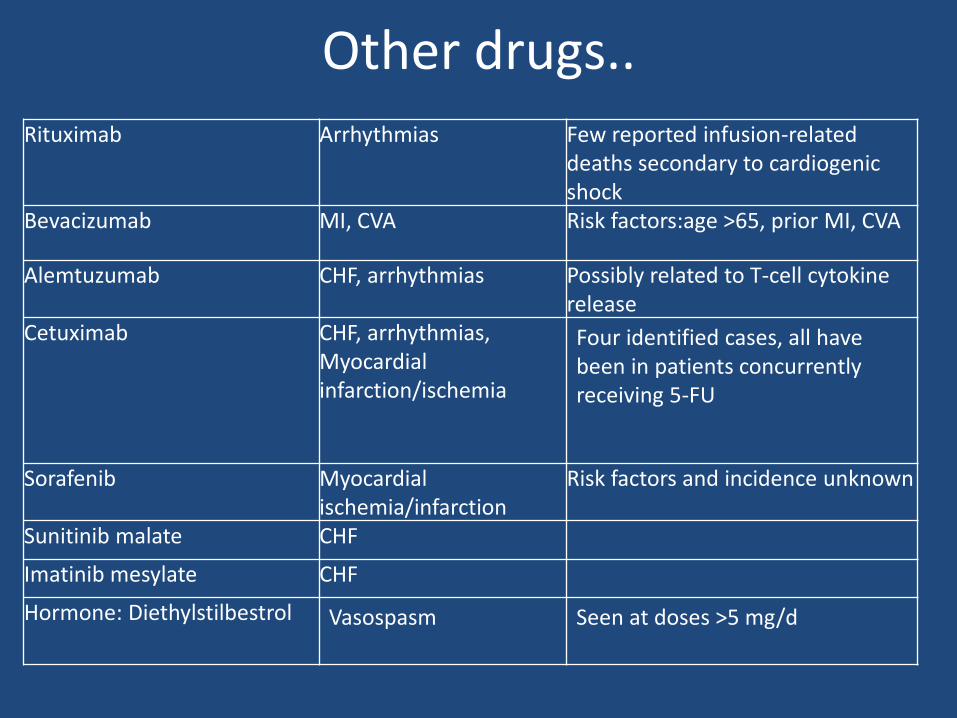
Other drugs..Rituximab Arrhythmias Few reported infusion-related
deaths secondary to cardiogenic shock
Bevacizumab MI, CVA Risk factors:age >65, prior MI, CVA
Alemtuzumab CHF, arrhythmias Possibly related to T-cell cytokine release
Cetuximab CHF, arrhythmias, Myocardial infarction/ischemia
Four identified cases, all have been in patients concurrently receiving 5-FU
Sorafenib Myocardial ischemia/infarction
Risk factors and incidence unknown
Sunitinib malate CHF
Imatinib mesylate CHF
Hormone: Diethylstilbestrol Vasospasm Seen at doses >5 mg/d