cardiovascular pathophysiology - accredited cme … ncvh/5-29-fri/nurse-cath/6 ncvh rci… ·...
TRANSCRIPT

Cardiovascular
Pathophysiology
Thank You To:
AHA/ACC
SICP
Philip B. Adamson, MD
cardiovillage.com

Disclosures
Speaker’s Bureau:
• None
Honorarium:
• None
Consultant:
• None
Stockholder:
• None
Grant/Research Support:
• None
Medical/Scientific Boards:
• None

Outline• Coronary Artery Disease
– Angina
– Acute Coronary Syndrome (UA/NSTEMI, STEMI)
• Heart Failure
– Left and right side
• Valve Disease
– AS, AI, MS, MS
• Cardiomyopathies
– Dilated CMO
– Hypertrophic CMO
• Non-obstructive
• Obstructive
– Restrictive CMO

Coronary Artery Disease
the loss of elasticity of the
blood vessels
is a narrowing of the vessels
due to fatty deposits
Arteriosclerosis Atherosclerosis

Risk Factors For CAD
• Family history
• Advancing age
• Gender is still a factor
• Total cholesterol >200, LDL>100 HDL< 35
• Hypertension
• Smoking
• Overweight/obesity
• Sedentary life-style
• Stress
• Diabetes Mellitus

6

Evolution of Plaque
LDL
Monocyte
endothelium
Cell Adhesion
factors
1
1. LDL enters
2. & Oxidizes
3. Monocytes adhere & 4.
cross intima differentiate
yeilding macrophages
Macrophage
5. Macrophages engulf
LDL yielding Foam
cells
6. muscle cells multiply &
7. Migrate towards intima
8. Muscle cells die
& harden plaque -
Calcium develops
Todd’s Cardiovascular Review Book, 1st Edition, Vol. 3: Hemodynamic Calculations

8
• TWO PROCESSES :
• First the fats:
• Lipid accumulation & oxidation
• Then the vessel deforms:
• Endothelial dysfunction
• Spastic vessels

Manifestations of Coronary Artery Disease
• Predictable
• Unbalanced
Supply &
Demand
• Reduced O₂
• Reduced
Blood Flow
• Responsive to
Medication
• Often related
to occlusive
thrombus &
plaque rupture
• Stasis of flow
• Loss of supply
with increase
in demand
• Irreversible
Myocardial
Damage
Stable Angina Myocardial InfarctUnstable Angina
• Pain which is
unpredicted, new or
occurs at rest
• Unbalanced Supply &
Demand
• Less/Unresponsive to
Medication
• Often related to transient
non-occlusive thrombus

Other Angina TypesPrinzmetals / Variant
• Typically occurs at rest
• Caused by focal spasm of angiographically normal coronary arteries. In the majority of patients there is also atherosclerotic coronary artery obstruction. In cases where there is atherosclerotic obstruction the vasospasm occurs near the stenotic lesion.
Post infarct• Secondary to ischemic tissue around the infarcted area.
Microvascular / Syndrome X• Angina without angiographic evidence of stenosis or disease
• Thought to be microvasculature circulation deficiency

Angina Management
• Lifestyle
• Nitrates
• Statins
• Beta Blockers
• CCB’s
• Aspirin
• PCI (if indicated)
Patient Presentation of the Acute
Myocardial Infarction
• Syncope or near syncope without other cause
• Impairment of cognitive function without other cause
• Chest pain described as a pressure sensation, fullness, or squeezing in the midportion of the thorax
• Radiation of chest pain into the jaw or teeth, shoulder, arm, and/or back
• Associated dyspnea or shortness of breath
• Associated epigastric discomfort with or without nausea and vomiting
• Associated diaphoresis or sweating

13
Thrombus Formation and ACS
UA NQMI STE-MI
Plaque Disruption/Fissure/Erosion
Thrombus Formation
Non-ST-Segment Elevation Acute
Coronary Syndrome (NSTEMI-ACS)ST-Segment
Elevation
Acute
Coronary
Syndrome
(STEMI-ACS)
Old
Terminology:
New
Terminology:

Cardiac Markers• Creatine Kinase- MB
– 4-6 hours after symptom onset
– Normal in 48-72 hours
• Myoglobin
– 2-4 hours after symptom onset
– Normal in 24-36 hours
• Troponins (C, I, T)
– 4-8 hours after symptom onset
– Remain elevated as long as 7-10 days
– I & T specific to cardiac muscle

15
Treatment of Acute Coronary
Syndrome
Initial Treatment of ACS
Long-Term Medical Management
UA/NSTEMI†STEMI*
Thrombolytics PCI or CABG PCI or CABG
Antiplatelet, anti-ischemic, or
anticoagulant therapy
Antiplatelet, anti-ischemic, or
anticoagulant therapy
*Boden WE, et al. N Engl J Med. 2001;344:1939-1942. and Braunwald E, et al. J Am Coll Cardiol. 2000;36:970-1062.

16
ACS Medicine Cabinet
• Aspirin
• Heparin
• Low Molecular Weight Heparin
• GP IIb/IIIa Inhibitors
• Direct Thrombin Inhibitors
• Warfarin
• Statins (HMG Co-A Reductase Inhibitors)
• Early Medical vs Early Invasive therapy
Anticoagulation

17
ACS Medicine Cabinet
• Bed Rest
• Nitroglycerin
• Supplemental O2
• Narcotics (Morphine)
• Beta Blockade
• Ace Inhibitor
• Diuretics
• Anti-arrthymics (PRN)
• Inotropic Agents (PRN)
• IABP (PRN)
• A compassionate listener
Anti-Ischemic Therapy

Complications of MI
• Dysrhythmias
– Heart blocks
– Bundle branch block
– Ventricular
• Heart Failure
• LV Aneurysm
• VSD
• Mitral Regurgitation
Basic Concepts of Heart Failure• Pathophysiological state in which cardiac
function fails to pump blood at a volume
commensurate with venous return to meet
metabolic demands.
• Inadequate forward flow with volume back up
to capillary beds “behind” the failing ventricle
• Can be Left or Right Ventricular in Nature
• RV failure is most commonly due to chronic
LV failure.

Hemodynamic Basis for
Left Sided Heart Failure Symptoms
Philip B. Adamson, MD
Hemodynamics
Increase: LVEDP, LA, PCWP, PAP
Chronic Increase RHP, CVP
Decrease: CO, CI

Etiology of Left Ventricular Failure
Volume Over load: Regurgitate AO valveHigh output status
Pressure Overload: Systemic hypertensionOutflow obstruction (AS)
Loss of Muscle: Post MIChronic ischemiaConnective tissue diseases
Infection
Restricted Filling: Pericardial diseases Restrictive cardiomyopathy
Heart Failure

Hemodynamic Basis for
Left Sided Heart Failure Symptoms
Philip B. Adamson, MD
Hemodynamics
Increase: LVEDP, LA, PCWP, PAP
Chronic Increase RHP, CVP
Decrease: CO, CI

Left Ventricular Dysfunction
Symptoms
Dyspnea on Exertion
Paroxysmal Nocturnal Dyspnea
Tachycardia
Cough
Hemoptysis
Physical Signs
Rales/Crackles
Pulmonary Edema
Pulsus Alternans
S3 Gallop
Pleural Effusion
Cheyne-Stokes Respiration
Clinical Note: Treatment for heart failure is directed at the etiology of failure.
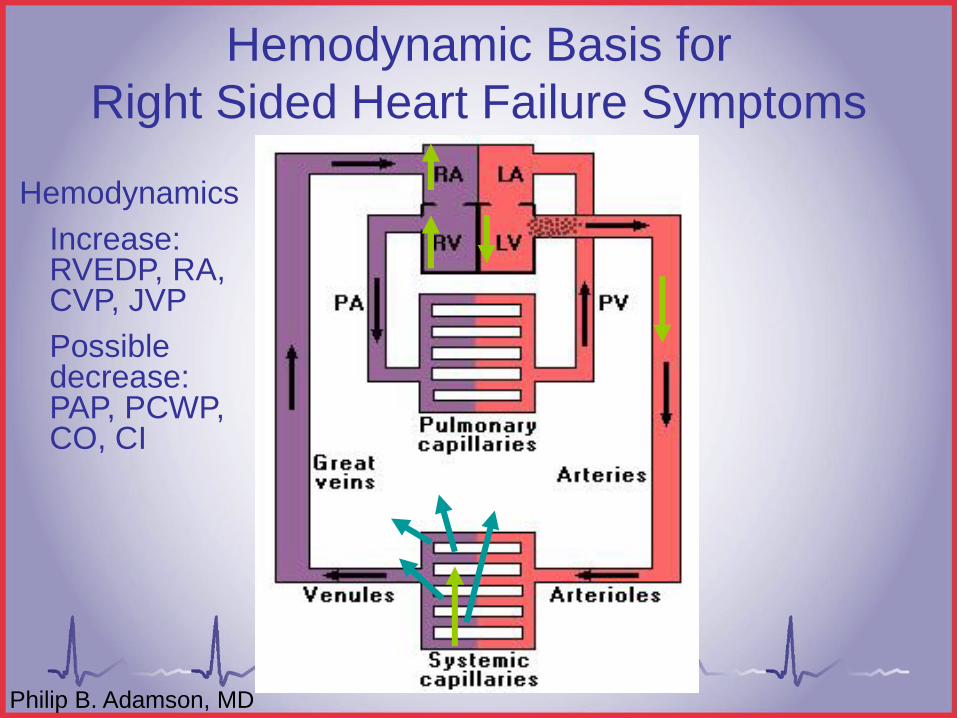
Hemodynamic Basis for
Right Sided Heart Failure Symptoms
Philip B. Adamson, MD
Hemodynamics
Increase: RVEDP, RA, CVP, JVP
Possible decrease: PAP, PCWP, CO, CI

Right Ventricular Dysfunction
Symptoms
Associated with dec. CO
Abdominal Pain
Anorexia
Nausea
Bloating
Swelling
Physical Signs
Peripheral Edema
Jugular Venous Distention
Abdominal-Jugular Reflux
Hepatomegaly
Weight gain
Clinical Note: Treatment for heart failure is directed at the etiology of failure.

Assessing Heart Failure
• ECG Monitor
• O2 Sat Monitor
• Chest X-ray
• Pulmonary Artery Catheter
– SVR / PVR
– CO/CI
– PCWP
– CVP

Functional Classifications
(New York Heart Association)
• Class I: No symptoms with activity.
• Class II: Slight limitations to physical activity, comfortable at rest, physical activity results in fatigue, palpitations, SOB, or angina
• Class III: Marked limitations to physical activity, comfortable at rest, slight physical activity results in fatigue, palpitations, SOB, or angina
• Class IV: Unable to carry out any physical activity without discomfort

29
Pharmacologic/Medical Management• Oxygen
• Digoxin
• Diuretics
• ACE Inhibitors
• Beta-Blockers
• Aldosterone Antagonists
• Angiotensin Receptor Blockers (ARBs)
• Dopamine/Dobutamine
• Intra Aortic Balloon Pump
• Underlying Cause

Heart Failure Summary
• Heart failure is a chronic, progressive disease that is generally not curable, but treatable
• Most recent guidelines promote lifestyle modifications and medical
• It is estimated 15% of all heart failure patients may be candidates for cardiac resynchronization therapy
• Close follow-up of the heart failure patient is essential, with necessary adjustments in medical management


Aortic Stenosis• Normal aortic valve area
is 2.5 to 3.6 cm2
• Critical severe aortic stenosis
less than 0.7 cm2 (can vary)

You can Learn a lot From a Garden Hose
Richard E. Klabunde, PhD -Cardiovascular Physiology Concepts
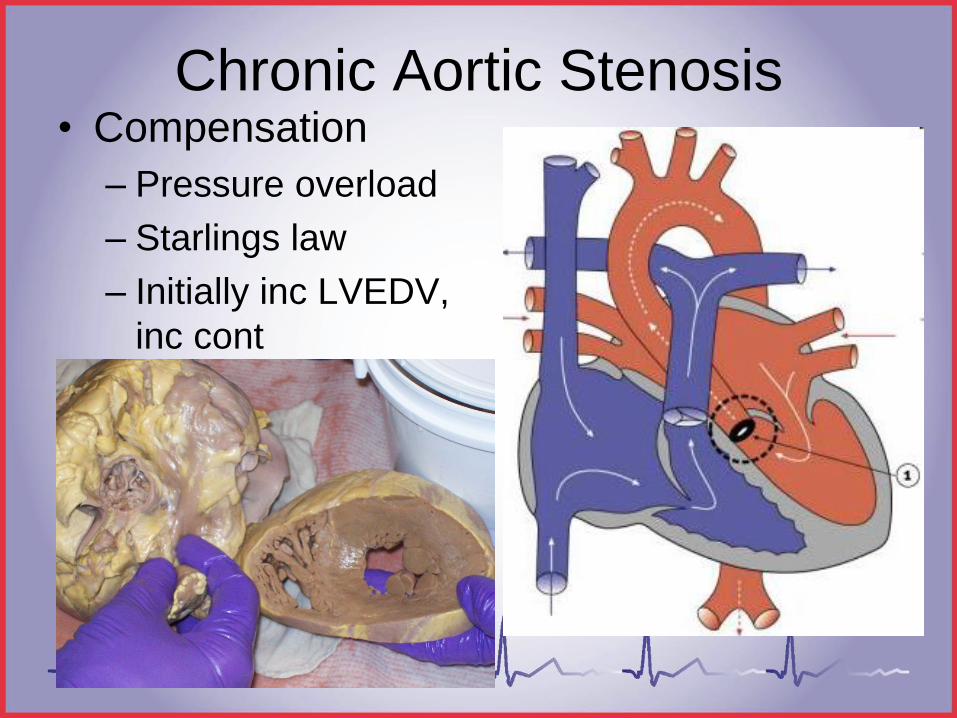
Chronic Aortic Stenosis• Compensation
– Pressure overload
– Starlings law
– Initially inc LVEDV,
inc cont

Aortic Stenosis
• LVOT obstruction
• LVH initially
• Pulsus parvus/tarvus-narrow pulse pressure
• Decreased systemic perfusion
• Inc. LVEDP, LA, PCWP, PA
• Pulmonary congestion
• LV-AO Systolic gradient
• Systolic murmur
• SAD-syncope, angina, dyspnea
Cardiac Self Assessment, Wes Todd, RCIS

Normal Aortic StenosisAO dec systolic
Narrow pulse pressure
LV Inc sys
Inc Dias, LVEDP
Michael Ragosta, MD, www.cardioVillage.com

AS Hemodynamic Manifestations
– AO
• Pulsus Parvous et Tarvus– May be brisk in elderly with non
compliant vessels
– PCWP
• Inc
– PA
• Inc
– SV & CO/CI
• Dec
– LV & AO systolic gradient
– Varies on the severity
Michael Ragosta, MD, www.cardioVillage.com

Aortic Insufficiency
• Leakage of blood
backwards across the
closed aortic valve
during ventricular
diastole

Diagnosis in the Cardiac Cath
Lab• Wide pulse pressure
• LVEDP may normal in
chronic AI, markedly
elevated in acute AI
• No aortic gradient
unless AS is also
present
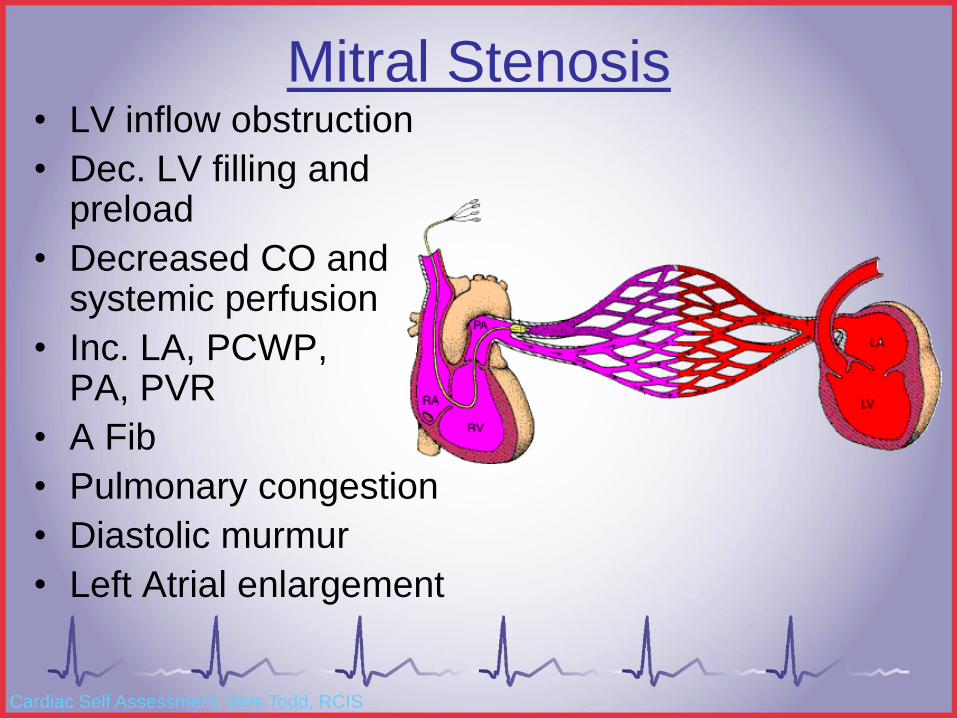
Mitral Stenosis• LV inflow obstruction
• Dec. LV filling and preload
• Decreased CO and systemic perfusion
• Inc. LA, PCWP, PA, PVR
• A Fib
• Pulmonary congestion
• Diastolic murmur
• Left Atrial enlargement
Cardiac Self Assessment, Wes Todd, RCIS

Baim DS, Grossman’s Cardiac Catheterization, Angiography, and Intervention, 7th ed.
Recording a MS Case• Hemodynamics
– PCWP/LA, LV, HR, CO
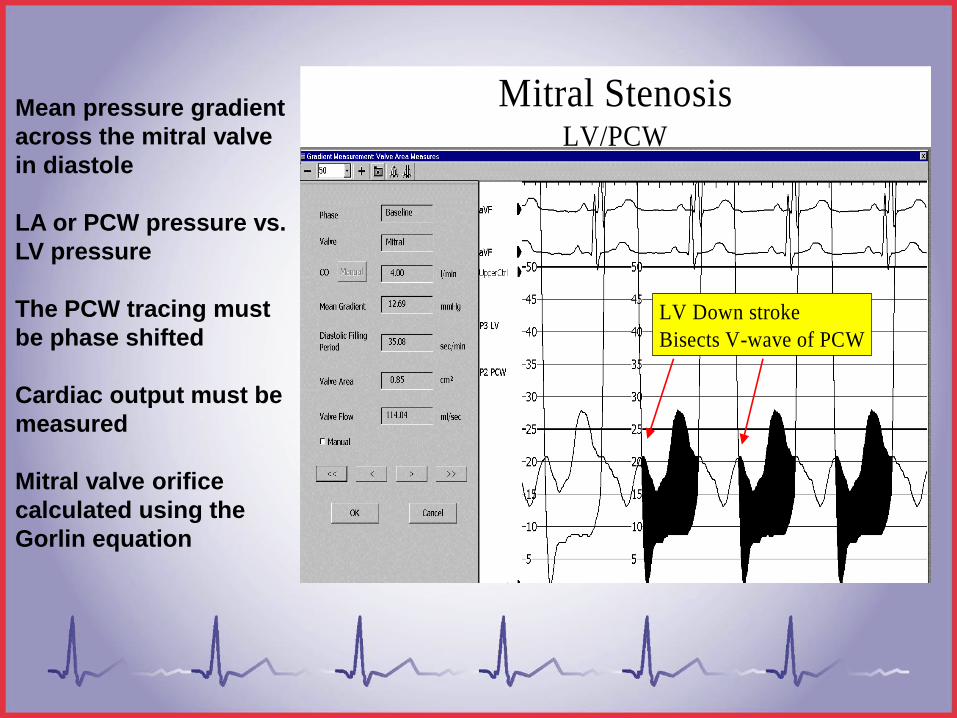
Mitral StenosisLV/PCW
LV Down stroke
Bisects V-wave of PCW
Mean pressure gradient
across the mitral valve
in diastole
LA or PCW pressure vs.
LV pressure
The PCW tracing must
be phase shifted
Cardiac output must be
measured
Mitral valve orifice
calculated using the
Gorlin equation

Mitral Valve Stenosis
A normal mitral valve has an area of 4 – 6 cm2
• Hemodynamically significant changes occur when the valve area is reduced to 2 cm2 or less.
– Other Hemodynamic changes that may occur with significant mitral stenosis:
• Increased a-wave in left atria
• Pulmonary hypertension
• Right heart pressures increase in reaction to pulmonary hypertension, possibly leading to right heart failure.

Mitral Valve Stenosis• Mitral valve stenosis evaluated
hemodynamically by comparing LA or PCWP to LVEDP
– In the normal heart, the mean LA or Wedge pressure should equal the LV EDP.
– If the mean pressure is greater than the LV EDP, this indicates that there is a restriction between the chambers, forcing the atrial pressures to be higher than necessary.
• This is the classic sign of Mitral Stenosis
Note: If LV EDP is higher than the Mean of the LA, your transducers may not be
properly leveled or balanced.

Mitral Stenosis Evaluation
The greater the gradient, the more significant the disease

Mitral Regurgitation
Leakage of blood across a closed mitral valve during ventricular systole
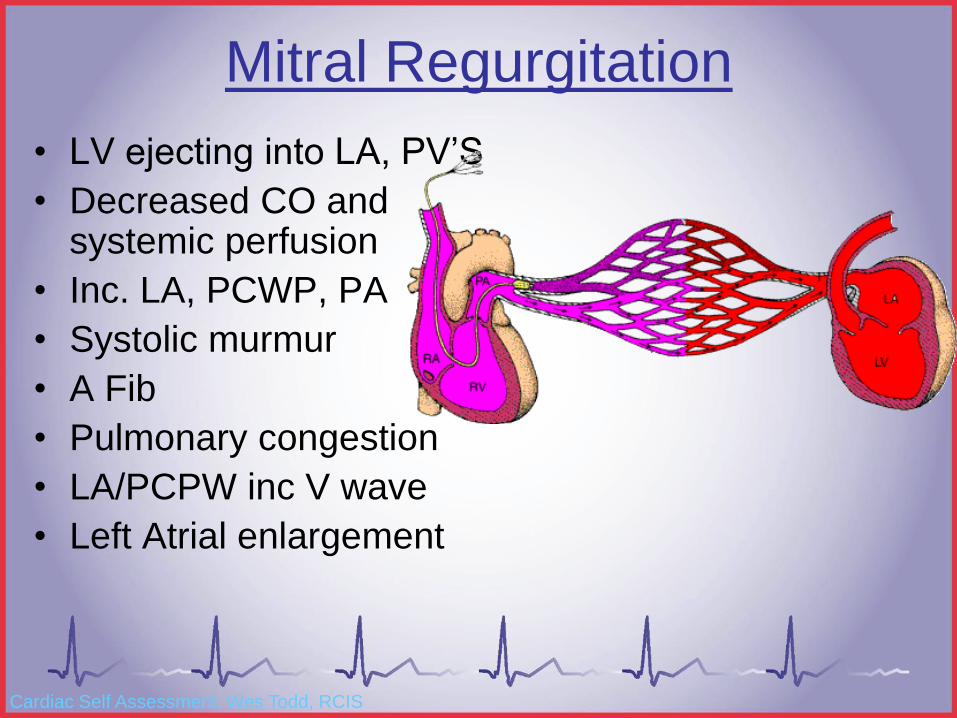
Mitral Regurgitation
• LV ejecting into LA, PV’S
• Decreased CO and systemic perfusion
• Inc. LA, PCWP, PA
• Systolic murmur
• A Fib
• Pulmonary congestion
• LA/PCPW inc V wave
• Left Atrial enlargement
Cardiac Self Assessment, Wes Todd, RCIS
Classification of Mitral Regurgitation
• Classification of Mitral Regurgitation is often performed following Left Ventriculography.
• Classification is based upon the amount of contrast flowing back into the left atrium during ventricular systole.
– Class I+ - Trace amounts of contrast flow into the LA, but it clears during atrial contraction
– Class II+ - Moderate insufficiency; contrast is visible within the entire LA, and does not clear
– Class III+ - Moderately severe MR; contrast opacifies the LA, and becomes more dense with each contraction of the left ventricle
– Class IV+ - Severe regurgitation; wide open MR, contrast completely opacifies the LA during the first contraction of the LV

Mitral Regurgitation
• LA/PCWP inc.
– V wave inc
• PA inc
• CO/CI dec
• S & S pulm edema
Richard E. Klabunde, PhD -Cardiovascular Physiology Concepts

Mitral Valve Regurgitation
• Mitral valve regurgitation is assessed by evaluating the V-wave of the left atrial or pulmonary arterial wedge pressure.
– The V-wave reflects atrial filling following ventricular contraction
– Due to the regurgitant valve, volume will rapidly enter the atrium from the left ventricle in a retrograde fashion, adding to the volume normally received from the right ventricle contraction.

Mitral Valve Regurgitation
Large
V-
wave
LV and Wedge recorded
simultaneously. Notice the very
large V-waves

V Waves

Michael Ragosta, MD, www.cardiovillage.com

Cardiomyopathy
A disease of heart
muscle often in
the absence of a
known etiology
Is a significant
cause of morbidity
and mortality

Cardiomyopathy
• World health organization has classified
the cardiomyopathies into three
categories-
– Dilated cardiomyopathy
– Hypertrophic cardiomyopathy
– Restrictive cardiomyopathy
• Distinctions not always absolute often
overlapping features

Normal Dilated Cardiomyopathy
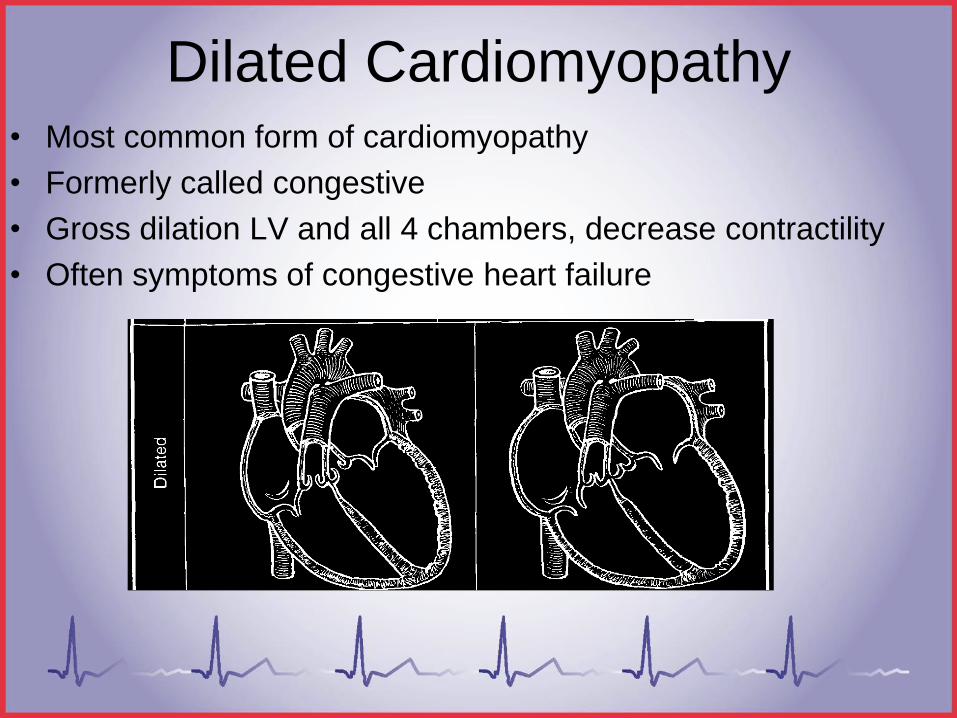
Dilated Cardiomyopathy• Most common form of cardiomyopathy
• Formerly called congestive
• Gross dilation LV and all 4 chambers, decrease contractility
• Often symptoms of congestive heart failure
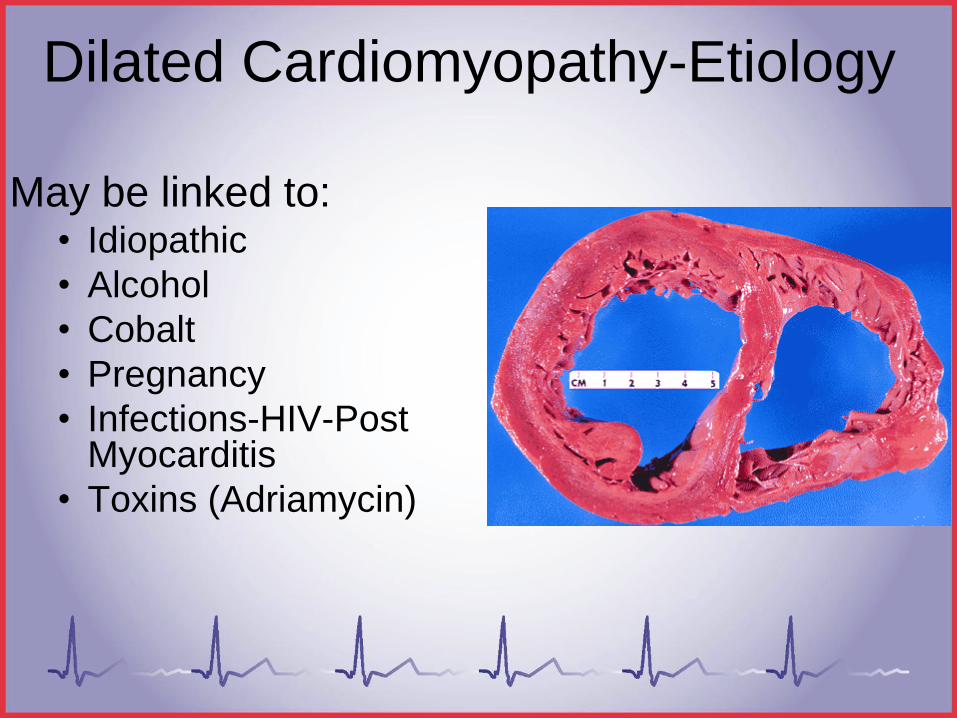
Dilated Cardiomyopathy-Etiology
May be linked to:• Idiopathic
• Alcohol
• Cobalt
• Pregnancy
• Infections-HIV-Post Myocarditis
• Toxins (Adriamycin)

Dilated
Cardiomyopathy
• Gross dilation
• Thin ventricular walls
• Decrease systolic function
• Thrombus formation
• Mitral & Tricuspid regurgitation
• Increase in diastolic and systolic volumes

Dilated Cardiomyopathy-LV Gram

Dilated Cardiomyopathy
LV pressure waveform
Findings in the Cardiac Cath Lab
Hemodynamics
Elevated LVEDP, PCWP, PA
Elevated SVR and PVR
May assess responsiveness to vasodilators for PVR
V-wave on PCWP
Possible increase in right heart pressures
Decreased EF% and CO
Angiographic Evaluation
LV-gram dilated, poorly contractile LV
Global LV hypokineticmovement
Assess coronaries to rule out CAD as a cause of poor contractility
Mitral regurgitation common

Dilated Cardiomyopathy-TreatmentManage Heart Failure
• Digitalis • Diuretics• Ace inhibitors • Beta blockers• Nitrates
Manage Coagulation
• Aspirin• Coumadin
Resynchronization Therapy
If secondary to alcohol-STOP DRINKING

Hypertrophic
Cardiomyopathy

Hypertrophic Cardiomyopathy
• Marked hypertrophy of the heart, especially the interventricular septum without obvious cause (hypertension, aortic stenosis)
• May be diffuse, asymmetrical (IVS) or apical
• With and without obstruction (aprox. 95% without and 5% with obstruction)
• Hypertrophic obstructive cardiomyopathy(HOCM)
• Preserved or enhanced contractile function

Background HOCM
• Prevalence approximately 1:500
• HOCM- #1 killer of young athletes
• More prevalent in men
• Genetically transmitted autosomal dominant with variable expression- Congenital
• May involve all ventricular walls, apex, interventricularseptum
• Acquired hypertrophic cardiomyopathy
– Usually associated with hypertension

HOCMDynamic LVOT obstruction
Gradient increased with reduced
afterload & preload, and increased
contractility
Gradient reduced with increased
preload & afterload, and reduced
contractility
Gradient only occurs in HOCM
with ASH

Hypertrophic Obstructive Cardiomyopathy
Michael Ragosta, MD, www.cardioVillage.com

HOCM
• Hypertrophied septum results in narrowing of LV outflow tract
• Forms obstruction below the aortic valve
• The mitral leaflet that forms lateral wall of LV outflow tract actively involved
• Elevated LVEDP
• Frequent mitral regurgitation
• May have diastolic dysfunction due to stiff non compliant LV
• Pulsus Bisferiens

Cardiac Cath Lab Findings
• Right heart pressures may be normal
• Pressure gradient may not exist at rest
• Provocative maneuvers– Valsalva maneuver (reduces preload)
– Amyl nitrate (reduces afterload)
– Isoproterenol (increases contractility)
• Careful analysis of location of gradient
• Post ectopic beat– Normally would result in increased pulse pressure
– Result in increase in obstruction and reduced stroke volume, “Brockenbrough’s phenomenon”

Pullback in HOCMUse end hole catheter, not a pigtail
Michael Ragosta, MD, www.cardioVillage.com

Michael Ragosta, MD, www.cardioVillage.com

Michael Ragosta, MD, www.cardioVillage.com

Treatment Options
Sigwart U. Non-Surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet 1995;346:211-14.
• AICD for sudden
death
• Surgical•Myotomy/myomectomy with
mitral valve replacement
•Alcohol ablation
• Transplant

Restrictive
Cardiomyopathy

Restrictive Cardiomyopathy
• Least common form of cardiomyopathy
– In western countries, more common in third world
• Impaired diastolic filling
– Rigid ventricular walls
• Systolic function usually preserved
• May result from a variety of local or systemic
diseases or radiation treatments
• Important to differentiate from constrictive
pericarditis

The Restrictive Cardiomyopathies
• Scleroderma• Systemic sclerosis produces fibrotic thickening
• Loeffler’s Endocarditis• Eosinophils lining the endocardium & in the myocardium
• Amyloidosis• Most common in US
• Protein deposits
• Hemochromatosis• Iron deposits
• Sarcoidosis• Granulomatous infiltration

Pathophysiology
• Abnormal diastolic function caused by
infiltration of the endocardium/myocardium
• Excessively rigid stiff ventricular walls
• Decrease in ventricular filling
• Contractility unimpaired
• Normal systolic emptying of ventricles
• Hemodynamically resembles constrictive
pericarditis

Hemodynamics Restrictive Cardiomyopathy
– Preserved Systolic function
– Early rapid ventricular fill associated with decreased ventricular compliance
– Dip and plateau(square root) configuration in LV and RV diastolic pressure wave forms
– RA & LA/PCWP prominent x and y descents-M or W pattern
– LV diastolic ~5mmhg greater than RV diastolic
– With exercise pressure separates further-LV pressure increases more than RV
– Pulmonary hypertension usually exists
Michael Ragosta, MD, www.cardioVillage.com

Clinical Note: RV & LV diastolic pressures will
separate with exercise
Michael Ragosta, MD, www.cardioVillage.com

Michael Ragosta, MD, www.cardioVillage.com

Restrictive Cardiomyopathy S&S
• Gradually worsening shortness of breath
• Chest Pain/Palpatations
• Progressive exercise intolerance
• SOB/Paroxysmal nocturnal dyspnea
• Fatigue
• Abdominal discomfort or liver tenderness
• JVD, Hepatamegaly, Ascites
• Atrial Fibrillation
• Thromboembolic events
• Hemodyamic findings as discussed
• Kussmals Sign
• Distant heart sounds
– S3 or S4 heart sounds possible
• Narrowed pulse pressure
Symptoms Signs

Restrictive Cardiomyopathy &
Constrictive Pericarditis

Restrictive Cardiomyopathy & Constrictive Pericarditis
• Filling occurs in early diastole
• Rapid Y-descent of the atrial pressure tracings
• Rapid early filling waveform in the ventricular pressure
• Square root sign in atrial and ventricular diastolic filling
• Kussmaul’s Sign
Kussmaul’s Sign

Restrictive Cardiomyopathy Management
• Usually poor prognosis
• Optimally treat any systemic disease
process of underlying cause
• Diuretics for systemic and pulmonary
congestion
• Antiarrhythmics

Thank You

Cardiovascular
Pathophysiology
Thank You To:
AHA/ACC
SICP
Philip B. Adamson, MD
cardiovillage.com