cardiovascular screening - university of michigan
TRANSCRIPT
DEPARTMENT OF FAMILY MEDICINE
Cardiovascular Screening
Keri L. Denay, M.DDirector, Primary Care Sports Medicine Fellowship
Assistant ProfessorDepartment of Family Medicine
University of Michigan Medical SchoolTeam Physician, Eastern Michigan University
No disclosures.
DEPARTMENT OF FAMILY MEDICINE
Overview
• Goal of screening• Incidence and Prevalence
– Young vs. “Old”
• Etiology• How to Screen
– Characteristics of a screening test
• Young athlete recommendations• General adult recommendations• Summary and questions
DEPARTMENT OF FAMILY MEDICINE
• Goal: Prevent Sudden Cardiac Death (SCD)

DEPARTMENT OF FAMILY MEDICINE
SCD – Young Incidence and Prevalence– Young athletes (< 35 years of age) 1,2
• High school: 1:50,000-1:80,000 athlete years (AYs)
• College 1:50,000 AYs
– Men 1:37,790 AYs
» incidence rate ratio of 3.2 compared to women
– African American athletes 1:21,491 AYs
» incidence rate ratio of 3.2 compared to Caucasian athletes
– Basketball players 1:8978 AYs
» Division I, male basketball players 1:5200 AYs (1:1300 over a 4-year career)
– Men’s basketball and football account for 50-61% of all identified cases
• Prevalence of cardiac conditions associated with SCD in young athletes = 0.3%
DEPARTMENT OF FAMILY MEDICINE
SCD – “Old” Incidence
• “Old” (> 35 years of age) 3
– Men: 1: 1.5 million episodes of vigorous activity (Physician’s Health Study)
– Women: 1:36.5 million hours of moderate or vigorous activity (Nurse’s Health Study)
DEPARTMENT OF FAMILY MEDICINE
SCD Etiologies - Young
– Honestly. . . we don’t know! 2
• About 44% of athletes with SCD have no structural cardiac abnormalities identified at autopsy!
• Most common causes:– Hypertrophic Cardiomyopathy (HCM): 8-36% of cases– Anomalous coronary arteries– Idiopathic left ventricular hypertrophy– Arrhythmogenic right ventricular cardiomyopathy– Dilated cardiomyopathy– Myocarditis– Long QT syndrome (LQTS)– Wolff–Parkinson–White (WPW)– Aortic dissection– Atherosclerotic coronary artery disease (CAD)

DEPARTMENT OF FAMILY MEDICINE
SCD Etiologies – “Old”
• Atherosclerotic CAD
DEPARTMENT OF FAMILY MEDICINE
Screening
• Young– ???– HCM
• Old– CAD
• Test qualities– Sensitive (rule it out)– Specific (rule it in)– Acceptable to patients– Widely available– Able to alter disease course if detected early– High enough prevalence to justify screening

DEPARTMENT OF FAMILY MEDICINE
Young Screening Options - PPE
• Get a good history!
– Can lead to 88% of medical diagnoses made during PPE 4
– Use resources –PPE monograph 5

DEPARTMENT OF FAMILY MEDICINE
AHA History Recommendations 6
Personal history
• Exertional chest pain or discomfort
• Unexplained syncope/near-syncope
• Excessive exertional and unexplained dyspnea/fatigue
• History of a heart murmur
• Elevated blood pressure
DEPARTMENT OF FAMILY MEDICINE
AHA History Recommendations
Family history
• Premature death (sudden and unexpected) before age 50 years due to heart disease
• Disability from heart disease in a close relative 50 years of age or younger
• Specific knowledge of certain cardiac conditions in family members: hypertrophic or dilated cardiomyopathy, long-QT syndrome or other ion channelopathies, Marfan syndrome, or arrhythmias
DEPARTMENT OF FAMILY MEDICINE
Cardiac Exam
• AHA recommends the following be included in the PPE cardiac exam:
– Listen for murmurs
– Palpate femoral pulses to exclude coarctation
– Examine for physical findings of Marfan Syndrome
– Brachial artery blood pressure in seated position

DEPARTMENT OF FAMILY MEDICINE
Auscultation for murmurs
• Why?
– HCM-associated LV outflow obstruction, AS, MVR, AVI, PVI
• How?
– Supine AND Standing/Valsalva
• HCM murmur louder w/ standing and valsalva due to ↓ venous return
DEPARTMENT OF FAMILY MEDICINE
Auscultation for murmurs (cont.)• What?
–HCM LV outflow obstruction
• Harsh, loud, systolic murmur
• R upper sternal border
• Louder with Valsalva (or squat to stand)
–ANY diastolic murmur is pathologic!
– Systolic ejection or mid-systolic clicks typically abnormal at any age.
DEPARTMENT OF FAMILY MEDICINE
Palpation of Femoral Artery Pulses
• Palpate femoral and brachial pulses simultaneously
• If there is a delay of the femoral pulse compared to the brachial pulse, coarctation must be ruled out

DEPARTMENT OF FAMILY MEDICINE
Marfan Syndrome?
• Kyphoscoliosis
• High-arched palate
• Pectus excavatum
• Arachnodactyly
• Arm span > Height
– ratio >1.05
• Hyperlaxity
• Ghent Criteria
www.glogster.com

DEPARTMENT OF FAMILY MEDICINE
Should we do more to screen our younger athletes?
Add the ECG?

DEPARTMENT OF FAMILY MEDICINE
Hot Topic
• Remember screening test characteristics
– Sensitive (rule it out)
– Specific (rule it in)
– Supportive infrastructure/widely available
– Able to alter disease course if detected early
– High enough prevalence

DEPARTMENT OF FAMILY MEDICINE
ECG Accuracy
• Accuracy 7
– Hard to interpret ECG in athletes• 2013 Seattle and 2014 Refined criteria have improved
this
• Concordance still low
• False positive rate still about 6%
– Some conditions will not have an abnormal ECG (false negatives)• 10% of HCM cases will have normal ECG
• >30% of ARVC cases will have normal ECG
DEPARTMENT OF FAMILY MEDICINE
ECG Logistics
• No infrastructure in US for screening/follow-up testing– Where do the ECG machines come from?
– Who performs and/or interprets?
– What to do with athletes restricted from playing (handling of the true and false positives)?
– Who pays for the testing and potential follow-up testing?• Some cost estimates are $2.5-3.4 billion/year to screen the U.S.
young athletes 7
– What about false negatives and potential consequences?
– How often do we screen?

DEPARTMENT OF FAMILY MEDICINE
ECG Altered disease course/outcome?
• Unclear if treating asymptomatic ECG finding early provides any long-term benefit
• Any treatment available?
• Less active individual other disease outcome?
• Psychological impact
DEPARTMENT OF FAMILY MEDICINE
Young Athlete Recommendations

DEPARTMENT OF FAMILY MEDICINE
• 2016 AMSSM Position Statement on Cardiovascular Preparticpation Screening in Athletes: Current Evidence, Knowledge Gaps, Recommendations, and Future Directions 2
• 2012 AHA Preparticipation Cardiovascular Screening of Young Competitive Athletes: Policy Guidance 8

DEPARTMENT OF FAMILY MEDICINE

DEPARTMENT OF FAMILY MEDICINE
AMSSM 2016
• The lack of clear outcomes-based research precludes AMSSM from endorsing any universal CV screening strategy for athletes.
• Physician autonomy to implement the most appropriate CV screening strategy unique to the athlete population and community resources.

DEPARTMENT OF FAMILY MEDICINE
DEPARTMENT OF FAMILY MEDICINE
AHA 2012
• “At this time, the AHA does not recommend the use of tests such as a 12-lead ECG or echocardiogram in mandatory preparticipation screening programs. Instead, these tests should be used as follow-up if an initial screening raises suspicions about the presence of a cardiovascular disease.”

DEPARTMENT OF FAMILY MEDICINE
BUT OUR ATHLETES GET OLDER. . .
AND THEN WHAT?

DEPARTMENT OF FAMILY MEDICINE
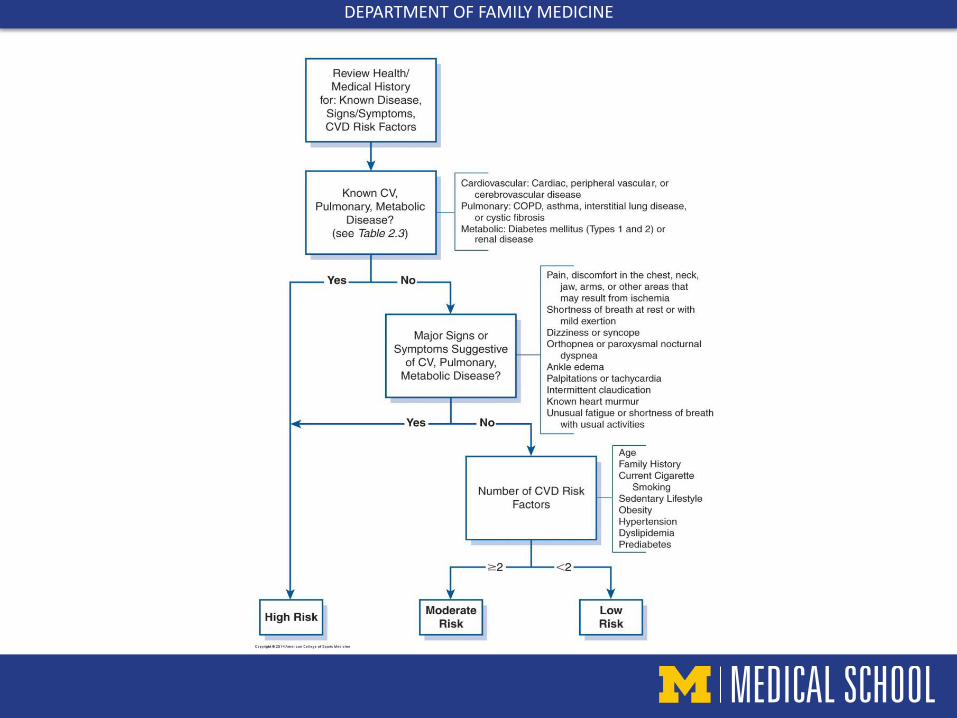
Old ACSM 9
• Individuals classified as low, moderate, or high risk based on the presence or absence of:
– Cardiovascular disease (CVD) risk factors (next slide)
– Signs and symptoms of cardiovascular, pulmonary, renal, or metabolic disease
– Known cardiovascular, pulmonary, renal, or metabolic disease
DEPARTMENT OF FAMILY MEDICINE

DEPARTMENT OF FAMILY MEDICINE

DEPARTMENT OF FAMILY MEDICINE
Why change?
• Complicated
• Exercise is safe for most people
• Absolute risk is low and most have symptoms in the days/weeks prior to incident
• Relative risk increased but improves as people become more physically active
• Predictive value of SCD by risk factor assessment low
• Too many referrals financial burden on healthcare system and barrier to increased physical activity

DEPARTMENT OF FAMILY MEDICINE
What’s different with ACSM 20153?
• No CVD risk factor assessment and classification
• Focuses on:
– Current level of physical activity
– Signs/symptoms of cardiac, metabolic, renal disease
– Desired level of activity

DEPARTMENT OF FAMILY MEDICINE
DEPARTMENT OF FAMILY MEDICINE
Activity Definitions
• Regular exercise = 30 min moderate intensity aerobic exercise at least 3 days/week for at least the last 3 months
• Light intensity = 30 to <40% HRR (HRmax-HRresting) (2 to <3 METs)
• Moderate intensity = 40 to <60% HRR (3 to <6 METs; 64-76% HRmax)
• Vigorous intensity = ≥60% HRR (≥ 6 METs; 77%+ HRmax)

DEPARTMENT OF FAMILY MEDICINE
Disease Definitions
• Cardiac disease: Cardiac, peripheral vascular, and/or cerebrovascular disease
• Metabolic disease: Type I or II diabetes• Symptoms of cardiac, metabolic, or renal disease:
– pain, discomfort in the chest, neck, jaw, arms or other area that may result from ischemia
– shortness of breath at rest or mild exertion– dizziness or syncope– orthopnea or paroxysmal nocturnal dyspnea– ankle edema– palpitations or tachycardia– intermittent claudication– known heart murmur– unusual fatigue or shortness of breath with usual activities

DEPARTMENT OF FAMILY MEDICINE
Last definition
• Medical clearance: “approval from a healthcare professional to engage in exercise”

DEPARTMENT OF FAMILY MEDICINE
ACSM 2015 Summary
• If not already exercising:
– consider “medical clearance” for those with cardiovascular disease, diabetes, or renal disease OR any signs/symptoms of such.
• If already exercising:
– consider “medical clearance” for those with disease and wanting vigorous program OR those with any signs/symptoms.

DEPARTMENT OF FAMILY MEDICINE
USPSTF 201210
Recommends against use of resting or exercise ECG in asymptomatic adults at low risk for CHD events (Grade: D)

DEPARTMENT OF FAMILY MEDICINE
11

DEPARTMENT OF FAMILY MEDICINE
Summary
• There’s still a lot we don’t know about young athlete SCD cases.
• AMSSM and AHA do NOT recommend universal ECG screening as part of PPE.
• “Older” individuals have CAD, and we’re bad at predicting who may suffer SCD as a result.
• Consider “medical clearance” for:1. Those not exercising with cardiac, renal, or metabolic
issues and/or symptoms. 2. If already exercising, only need to be “cleared” if +
disease and want vigorous or symptomatic.

DEPARTMENT OF FAMILY MEDICINE
References
1. Asif I, Harmon K. Incidence and Etiology of Sudden Cardiac Death: New Updates for Athletic Departments. Sports Health. 2017;9(3):268-279.
2. Drezner JA, O’Connor FG, Harmon KG, Fields KB, Asplund CA, Asif IM, et al. AMSSM Position Statement on Cardiovascular Preparticipation Screening in Athletes: Current Evidence, Knowledge Gap, Recommendations, and Future Directions. Clin J Sport Med. 2016; 26(5): 347-361.
3. Riebe D, Franklin BA, Thompson PD, Garber CE, Whitefield GP, Magal M, et al. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015; 47(8): 2473–2479.
4. Chun J, Haney S, DiFiori J. The relative contributions of the history and physical examination in the preparticipation evaluation of collegiate student athletes. Clin J Sport Med. 2006;16(5):437-438.
5. American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports Medicine, American Osteopathic Academy of Sports Medicine. PPE: Preparticipation Physical Evaluation, Fourth Edition. American Academy of Pediatrics. 2010.
6. Maron B et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: a scientific statement from the american heart association council on nutrition, physical activity, and metabolism: endorsed by the american college of cardiology foundation. Circulation 2007;115:1643-1655.
7. Asplund CA, O’Connor FG. The Evidence Against Cardiac Screening Using Electrocardiogram in Athletes. Curr Sports Med Rep. 2016; 15(2): 81-85.
8. American Heart Association and American Stroke Association. Preparticipation Cardiovascular Screening of Young Competitive Athletes: Policy Guidance. 2012. Available at: https://www.heart.org/idc/groups/ahaecc-public/@wcm/@adv/documents/downloadable/ucm_443945.pdf
9. American College of Sports Medicine and American Heart Association. Exercise and Acute Cardiovascular Events: Placing the Risks into Perspective. Med Sci Sports Exerc. 2007; 39(5): 886-897.
10. U.S. Preventive Services Task Force (USPSTF). Screening for Coronary Heart Disease With Electrocardiography: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2012;157:512-518.
11. Freeman J, Froelicher V, Ashley E. The ageing athlete: screening prior to vigorous exertion in asymptomatic adults without known cardiovascular disease. Br J Sports Med. 2009;43:696–701.