care and treatment of chronic hbv and hcv€¦ · care and treatment of chronic hbv and hcv...
TRANSCRIPT

CARE AND TREATMENT
OF CHRONIC HBV AND HCV - D e c e m b e r 20 1 8 -
GEORGE PAPATHEODORIDIS, MD
PROFESSOR IN MEDICINE AND GASTROENTEROLOGY ATHENS UNIVERSITY MEDICAL SCHOOL
HARRY JANSSEN, MD PROFESSOR OF MEDICINE, TORONTO WESTERN AND TORONTO GENERAL HOSPITAL,
UNIVERSITY HEALTH NETWORK, TORONTO, CANADA
ANGELOS HATZAKIS, MD PROFESSOR OF EPIDEMIOLOGY AND PREVENTIVE MEDICINE
ATHENS UNIVERSITY MEDICAL SCHOOL

Contents
Care and Treatment of Chronic Hepatitis B
Care and Treatment of Chronic Hepatitis C

Chronic HBV and HCV are treatable or curable
Current HBV treatment options Current HCV treatment options
Lamivudine Ribavirin
Adefovir dipivoxil Sofosbuvir
Peginterferon alfa-2a Simeprevir
Peginterferon alfa-2b Daclatasvir
Entecavir Sofosbuvir/Ledipasvir
Telbivudine Paritaprevir/ritonavir/Ombitasvir ± Dasabuvir
Tenofovir disoproxil fumarate Sofosbuvir/Velpatasvir
Tenofovir alafenamide Elbasvir/Grazoprevir
Glecaprevir/Pibrentasvir
Sofosbuvir/Velpatasvir/Voxilaprevir
Agents in bold are those mostly used

CARE AND TREATMENT OF CHRONIC HEPATITIS B

• Induction of long-term suppression of HBV DNA:
the main endpoint of all current treatment strategies.
• Induction of HBeAg loss, with or without anti-HBe seroconversion,
in HBeAg-positive CHB patients: valuable endpoint, often
representing partial immune control of the chronic HBV infection.
• Biochemical response (ALT normalization): additional endpoint
achieved in most patients with long-term suppression of HBV
replication.
• HBsAg loss, with or without anti-HBs seroconversion:
optimal endpoint indicating profound suppression of HBV
replication and viral protein expression.
End-points of therapy
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

Indications for treatment
• Patients should be considered for treatment if
– HBV DNA >2,000 IU/ml and
– ALT >ULN (40 IU/L) and/or
– At least moderate necroinflammation and/or at least moderate
fibrosis by liver biopsy [or liver stiffness >9 or >12 kPa if ALT ≤ULN or
>ULN (<5xULN)]
• Patients with compensated or decompensated cirrhosis need treatment, with any detectable HBV DNA level and regardless of ALT levels
• Indications for treatment may also take into account
age, health status, comorbidities, family history of HCC or cirrhosis and
extrahepatic manifestations
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

Treatment indications/Management in HBeAg-pos. CHB patients
ALT >ULN & HBV DNA >2,000 & Biopsy ≥A2/F2
A. HBeAg-pos. chronic HBV infection (previously immunotolerant phase):
Persistently ALT ≤ULN
• No Biopsy – No therapy – Follow-up if age ≤30
• Treatment if age >30 or family history of HCC, cirrhosis, stiffness >9 kPa
B. Obviously active CHB: ALT >2xULN & HBV DNA >20,000 IU/ml
• Therapy – Biopsy optional
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

ALT >ULN & HBV DNA >2,000 & Biopsy ≥A2/F2
A. HBeAg-ve patients with persistently ALT ≤ULN
(ALT every 3 months for at least 12 months) &
- HBV DNA <2000: No biopsy, No therapy, Follow-up
- HBV DNA 2,000-20,000 & no evidence of advanced liver disease:
No Biopsy, No therapy, Follow-up (close for another 2 years)
- HBV DNA >20,000 & no evidence of advanced liver disease: individualize
- HBV DNA >2000 & evidence of advanced liver disease
(including stiffness >9 kPa): therapy
B. Obviously active CHB: ALT >2xULN & HBV DNA >20,000
• Therapy – Biopsy optional
Treatment indications/Management in HBeAg-neg. CHB patients
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.
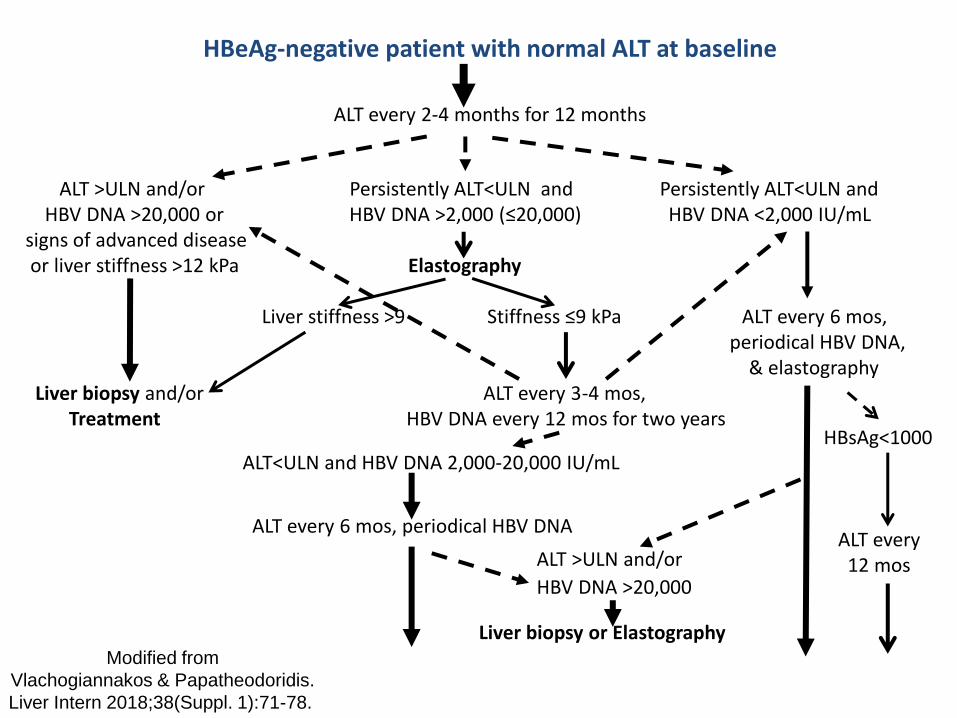
HBeAg-negative patient with normal ALT at baseline
ALT every 2-4 months for 12 months
ALT >ULN and/or Persistently ALT<ULN and Persistently ALT<ULN and HBV DNA >20,000 or HBV DNA >2,000 (≤20,000) HBV DNA <2,000 IU/mL signs of advanced disease or liver stiffness >12 kPa Elastography Liver stiffness >9 Stiffness ≤9 kPa ALT every 6 mos, periodical HBV DNA, & elastography Liver biopsy and/or ALT every 3-4 mos, Treatment HBV DNA every 12 mos for two years
ALT<ULN and HBV DNA 2,000-20,000 IU/mL ALT every 6 mos, periodical HBV DNA
ALT >ULN and/or
HBV DNA >20,000
Liver biopsy or Elastography
HBsAg<1000 ALT every 12 mos
Modified from
Vlachogiannakos & Papatheodoridis.
Liver Intern 2018;38(Suppl. 1):71-78.
Additional indications of treatment/prophylaxis
for chronic HBV patients
• Liver transplantation
• HBV-HIV co-infection
• HDV-HBV co-infection with ongoing HBV replication
• HBV-HCV co-infection during and for 12 weeks after DAAs
• Last trimester of pregnancy and up to 12 weeks after delivery if HBV DNA
>200,000 IU/ml or HBsAg >4 log10 IU/ml
• During and for 12 months after immunosuppressive therapy or
chemotherapy
• Healthcare workers performing exposure prone procedures with serum HBV
DNA >200 IU/ml
• Extrahepatic manifestations and replicative HBV infection
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

HBV-RELATED CHRONIC LIVER DISEASE
Groups of treatment options
Peg-interferon-alfa
(PegIFNa)
(antiviral+
immunomodulator)
Entecavir (ETV)1, Tenofovir disoproxil
fumarate (TDF)1, tenofovir alafenamide (TAF)1
Telbivudine (TBV)2, Lamivudine (LAM)2,
Adefovir (ADV)2 (pure antivirals)
Subcutaneous injections (one weekly) Tablets (one daily)
1High barrier to resistance 2Low barrier to resistance

EFFICACY OF 48-WEEKS OF PegIFNa IN CHB: End of therapy (EOT) & Sustained off-therapy responses
Pts, %
Lau G et al, NEJM 2005; Marcellin P et al, NEJM 2004
HBeAg(+)CHB HBeAg(-)CHB
EOT 6-mos FUP EOT 6-mos FUP HBeAg to anti-HBe seroconversion HBV DNA <400 cp/ml

Cumulative incidence of HBV resistance for NA in
pivotal trials in nucleos(t)ide-naïve patients with CHB
Collation of currently available data – not from head-to head studies
Note: No evidence of resistance has been shown after 8 years of TDF treatment.
Preferred regimens
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398. NA: nucleos(t)ide analogue(s)

Resistance to ETV or TDF in CHB with LAM resistance P
atie
nts
wit
h r
esi
stan
ce (
%)
6 0 0 0 0
Years 1 2 3 4 5 6 1 2 3 4
Entecavir (ETV) Tenofovir (TDF)
These trials included different populations, different exclusion criteria and different endpoints
15
31
47 51
Although licensed, ETV (1.0 mg) is not recommended for patients with LAM resistance by almost all guidelines
57
Tenney D et al. EASL 2009, Abstr. 20; Van Bommel F et al. Hepatology 2010, 51: 73-80

Indications for selecting ETV or TAF over TDF*
* TAF should be preferred to ETV in patients with previous exposure to nucleoside analogues.
** ETV dose needs to be adjusted if eGFR <50 ml/min; no dose adjustment of TAF is required in adults or adolescents (aged at least 12 years and of ≥35 kg body weight) with estimated creatinine clearance (CrCl) ≥15 ml/min or in patients with CrCl <15 ml/min receiving haemodialysis.
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

Han S et al. AASLD 2008. Shouval et al. AASLD 2008.
Pat
ien
ts w
ith
HB
V D
NA
<3
00
cp
/mL
(%)
55%
Year 1
83%
Year 2
89%
Year 3
67%
n/ N
236/ 354
Year 4
91%
80/ 146
116/ 140
116/ 131
98/ 108
Year 5
88/ 94
94%
Year 1
ETV-022
0
20
40
60
80
100
ETV-901
Long-term ETV therapy in naive HBeAg(+)/(-) CHB
HBeAg(+) HBeAg(-)
Year 1
91%
Year 2 95%
Year 3
94%
93/99 84/90
67/74 54/57
93%
Year 1
ETV-027
0
20
40
60
80
100
ETV-901

Marcellin P et al. AASLD 2011, 2012
HBeAg(-): 5 year - 6 years
ΙΤΤ: 83%- 81%
Per protocol*: 99%- 100%
HBeAg(+): 5 years - 6 years
ΙΤΤ: 65%- 62%
Per protocol*: 97%- 99%
Patients with HBV DNA <400 cp/mL at 5-6 years under TDF
*missing = exclusion

Antiviral Efficacy of TAF and TDF at Week 96
Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
*Adjusted for baseline HBV DNA level and oral antiviral treatment status strata M=F: Missing =Failure
Agarwal K et al. J Hepatol 2018;68:672-81.
HBeAg+
Rates of Viral Suppression (ITT; M=F) HBV DNA <29 IU/mL
No resistance was detected through 96 weeks Similar HBV DNA suppression rates for TAF compared to TDF through
Week 96
HBeAg-
73%
75%
P=0.47*
90%
91%
P=0.84*
TAF
TDF
94%
93% 64%
67%
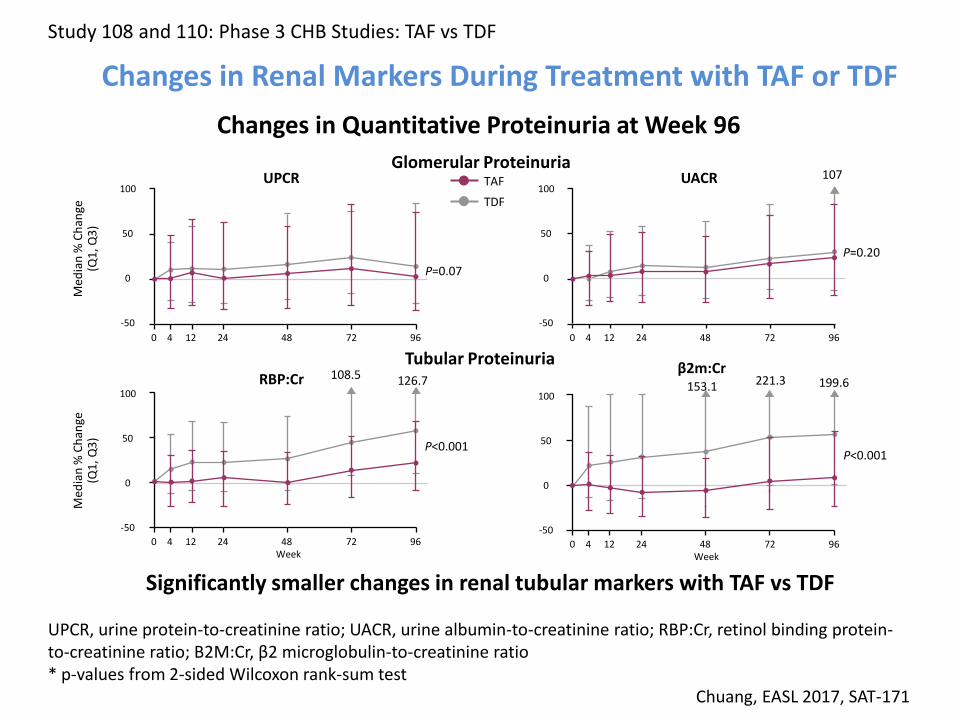
Changes in Renal Markers During Treatment with TAF or TDF
Study 108 and 110: Phase 3 CHB Studies: TAF vs TDF
Changes in Quantitative Proteinuria at Week 96
Significantly smaller changes in renal tubular markers with TAF vs TDF
UPCR, urine protein-to-creatinine ratio; UACR, urine albumin-to-creatinine ratio; RBP:Cr, retinol binding protein-to-creatinine ratio; B2M:Cr, β2 microglobulin-to-creatinine ratio * p-values from 2-sided Wilcoxon rank-sum test
Chuang, EASL 2017, SAT-171
Glomerular Proteinuria
Tubular Proteinuria
UPCR UACR
RBP:Cr β2m:Cr
Med
ian
% C
han
ge
(Q1
, Q3
) M
edia
n %
Ch
ange
(Q
1, Q
3)
100
50
0
-50
0 4 12 24 48 72 96
100
50
0
-50
100
50
0
-50
100
50
0
-50
0 4 12 24 48 72 96
0 4 12 24 48 72 96 0 4 12 24 48 72 96
P=0.07
P=0.20
P<0.001 P<0.001
Week Week
TAF
TDF
107
108.5 126.7 221.3 199.6 153.1

Monitoring of patients treated with ETV, TDF or TAF
1) All patients treated with NA should be followed with periodical assessments
including ALT (every 3-4 months during year 1 & then every 6 months) and
serum HBV DNA (every 3-4 months during year 1 & then every 6-12
months) (and HBeAg/anti-HBe every 6 months for HBeAg-pos. patients
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.
2) Patients at risk of renal disease treated with any NA should undergo
periodical* renal monitoring with eGFR and all patients regardless of
renal risk treated with TDF should undergo periodical* renal monitoring
with at least eGFR and serum phosphate levels.
(*periodical: every 3 months during year 1 & then every 6 months)
3) Patients on TDF at risk of development and/or with underlying renal or
bone disease should be considered for a switch to ETV or TAF, depending
on previous LAM exposure.

Ishak Fibrosis Scores
Pe
rce
nta
ge o
f p
atie
nts
0
10
20
30
40
50
60
70
80
90
100
Baseline Year 1 Year 5
39%
38%
12%
P < 0.001
P < 0.001
63%
0
10
20
30
40
50
60
70
80
90
100
Baseline Year 1 Year 5
39%
38%
12%
P < 0.001
P < 0.001
63%
6
5
4
3
2
1
0
6
5
4
3
2
1
0
Patients with cirrhosis (Ishak score ≥5): 28% at baseline, 8% at year 5
Fibrosis Is Reversible Liver Fibrosis Regression over 5 Yrs of Tenofovir Therapy
Marcellin P et al. Lancet 2013
348 patients with paired biopsies at baseline & year 5

Long-term outcome during NA therapy
1) Patients under effective long-term NA therapy should
remain under surveillance for HCC.
(Evidence level II-2, grade of recommendation 1)
2) HCC surveillance is mandatory for all patients with
cirrhosis as well as those with moderate or high HCC
risk scores at the onset of NA therapy.
(Evidence level II-2, grade of recommendation 1)
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

HCC in CHB patients under LAM
Patients with HCC,
%
LAM Untreated
Patients n: 779 534
HBeAg(-) 49% 54%
Comp. Ci: 29% 39%
FUP (mos): 32-90 32-108
• Liaw et al, NEJM 2004
• Papatheodoridis et al, HEP 2005
• Yuen et al, AVT 2007
P=0.003
P=0.015
P=0.016
All VR BR/BTH Untreated pts LAM treated pts N 779 353 426 534
Papatheodoridis GV et al. J Hepatol 2010;53:348-56

0,5%
1,0%
0,7%
0,1%
0,5%
0,0%
0,5%
1,0%
1,5%
2,0%
Tx-naive Tx-naive and/or tx-experienced Tx-naive
Papathe- odoridis N=212
Yang N=202
Wong N=984
Wong N=813
Yang N=314
Hosaka N=237
Lampe- rtico
N=213
Arends N=580
An
nu
al H
CC
In
cid
en
ce
Lim N=878
Cho N=933
Wu N=18748
Lampe- rtico
N=243
Papathe- odoridis N=1231
ETV TDF ETV or TDF
Yamada N=402
Prior exposure
NR
Tx-naive and/or tx-experienced
Asians Caucasians
ETV or TDF for non-cirrhotic CHB patients
HCC rates per year
Papatheodoridis GV et al. J Hepatol 2015;62:956-67

1,4%
2,8%
5,4%
2,0%
4,1%
3,3%
0,9%
5,4%
2,6%
5,1%
2,2%
4,5%
3,9%
0,0%
1,0%
2,0%
3,0%
4,0%
5,0%
6,0%
Yang N=121
Wong N=482
Wong
N=247
Hosaka N=79
Chen
N=239
Kim
N=324
Yang
N=152
Chen N=143
Papa theo- dori dis
N=69
Lamp- etico
N=155
Are- nds
N=164
Koklü N=77
2,8%
4,2%
1,8%
3,3%
2,5%
5,2%
1,5%
0,0%
1,0%
2,0%
3,0%
4,0%
5,0%
6,0%
Lim N=860
Cho
N=445
Su N=666
Wu N=2847
Lamp- ertico
N=131
Papa theo- dori dis
N=1231
Koklü N=72
Yama- da
N=94
ETV or TDF for cirrhotic CHB patients HCC rates per year
ETV TDF ETV or TDF
Tx-naive Tx-naive and/or tx-experienced Tx-naive
Prior exposure
NR
Tx-naive and/or tx-experienced
Asians Caucasians
Papatheodoridis GV et al. J Hepatol 2015;62:956-67

PAGE-B represents a simple to use HCC risk score for the first 5 years of ETV/TDF in Caucasian CHB patients
Construction of the PAGE-B risk score for HCC
Age (years) Gender Platelets
(/mm3)
16–29: 0 Female:
0 ≥200,000: 0
30–39: 2 Male: 6 100,000–
199,999: 6
40–49: 4 <100,000: 9
50–59: 6
60–69: 8
≥70: 10
Papatheodoridis GV et al. J Hepatol 2016;64:800-6
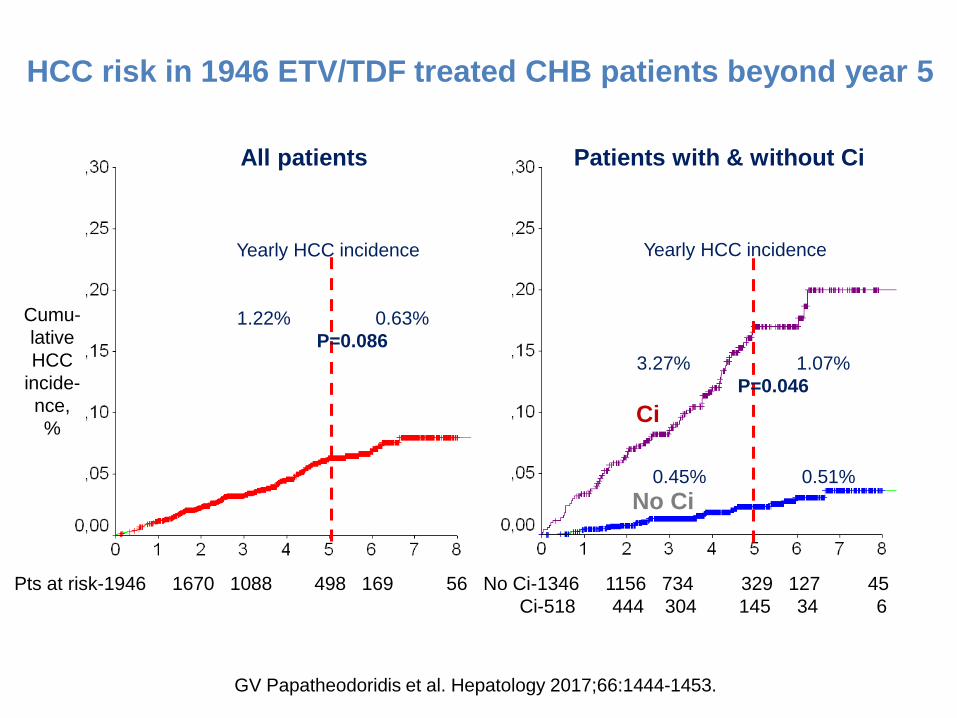
HCC risk in 1946 ETV/TDF treated CHB patients beyond year 5
GV Papatheodoridis et al. Hepatology 2017;66:1444-1453.
Ci
No Ci
All patients Patients with & without Ci
Yearly HCC incidence
1.22% 0.63%
P=0.086
Yearly HCC incidence
3.27% 1.07%
P=0.046
0.45% 0.51%
Cumu-
lative
HCC
incide-
nce,
%
Pts at risk-1946 1670 1088 498 169 56 No Ci-1346 1156 734 329 127 45
Ci-518 444 304 145 34 6

1) NAs should be discontinued after confirmed HBsAg loss, with or without anti-HBs seroconversion. (Evidence level II-2, grade of recommendation 1).
2) NAs can be discontinued in non-cirrhotic HBeAg positive CHB
patients who achieve stable HBeAg seroconversion and undetectable HBV DNA and who complete at least 12 months of consolidation therapy. Close post-NA monitoring is warranted. (Evidence level II-2, grade of recommendation 2)
3) Discontinuation of NAs in selected non-cirrhotic HBeAg-
negative patients who have achieved long-term (3 years) virological suppression under NA(s) may be considered if close post-NA monitoring can be guaranteed. (Evidence level II-2, grade of recommendation 2)
NA discontinuation
EASL 2017 CPG HBV, J Hepatol 2017;67:370-398.

Patients with
durable HBeAg
serocon- version,
%
At 6 12 24 months after NA(s) discontinuation
GV Papatheodoridis et al. Hepatology 2016; 63:1481-92.
Rates of durable HBeAg seroconversion after NAs discontinuation Systematic review: 6 studies, 289 initially HBeAg+ patients

Patients with
HBV DNA <20,000 IU/mL,
%
At 6 12 24 36 months after NA(s) discontinuation
Rates of virological remission after NAs discontinuation 14 studies, 733 initially HBeAg+ patients
Pooled HBsAg loss: 1%; Durable biochemical remission: 76%
GV Papatheodoridis et al. Hepatology 2016; 63:1481-92.

Patients with
HBV DNA <20,000 IU/mL,
%
At 6 12 24 36 months after NA(s) discontinuation
Rates of virological remission after NAs discontinuation 17 studies, 967 HBeAg- patients
Pooled HBsAg loss: 1.7%; Durable biochemical remission: 57%
GV Papatheodoridis et al. Hepatology 2016; 63:1481-92.

Patients with VR
at 12 mos after NAs
discontin., %
Rates of virological remission at 12 mos after NAs discontinuation in HBeAg-neg. CHB patients in relation to several factors
VR: virological remission
HBV DNA (IU/mL) <200 <2,000 <20,000 <12 12-24 >24 mos
VR definition Duration of on-NAs VR
P=0.513 P=0.017
GV Papatheodoridis et al. Hepatology 2016; 63:1481-92.

HBV treatment modifies the outcome of the disease
Sustained response after pegIFNa or long-term ETV/TDF/TAF monotherapy
Improvement/Stabilization of liver disease in practically all patients
Often regression of histological cirrhosis
Improvement/Disappearance of portal hypertension and liver decompensation
No need for liver transplantation due to liver failure
Reduction but not elimination of HCC risk
Improved survival

CARE AND TREATMENT OF CHRONIC HEPATITIS C

1992 1996 1998 2001 2011 2013 2014
SVR, %
>
Standard IFNa
RBV
PegIFNa
BOC/TPV
New DAAs
Evolution in efficacy of CHC treatment
IFN: interferon-alfa, R: ribavirin, PR: pegylated IFN+R, PI: protease inhibitor, BOC:boceprevir, TPV: telaprevir, DAA(s): direcr acting antiviral(s)

SOVALDI®
Sofosbuvir NS5B polymerase
Inhibitor Gilead
OLYSIO® Simeprevir
NS3/4A protease Inhibitor Janssen
DAKLINZA® Daclatasvir
NS5A Inhibitor
BMS
400 mg/24h
Genotypes 1-6
High genetic barrier
150 mg/24h with food
Genotypes 1,4
Low genetic barrier
60 mg/24h
Genotypes 1,2,3,4
Low genetic barrier
January 17, 2014 May 16, 2014 August 28, 2014 November 18, 2014
90+400 mg/24h
Genotypes 1,3,4
High genetic barrier
HARVONI® Ledipasvir
NS5A inhibitor +Sofosbuvir
NS5B polymerase Inhibitor Gilead
Anti-HCV agents approved by ΕMA in 2014

VIEKIRAX® Ombitasvir
NS5A inhibitor +Paritaprevir
NS3/4A protease inhibitor/ Ritonavir
EXVIERA® Dasabuvir
Non-nucleos(t)ide NS5B polymerase
inhibitor
[75/50+12.5 mg] x2 /24h with food
Genotypes 1, 4
Genetic barrier dependent on genotype
250 mg/12h
Genotype 1
Low genetic barrier
January 16, 2015
Anti-HCV agents approved by ΕMA in 2015
Abbvie

EPCLUSA® Velpatasvir
NS5A inhibitor +Sofosbuvir
NS5B polymerase Inhibitor Gilead
100+400 mg/24h
Genotypes 1-6
High genetic barrier
July 8, 2016
ZEPATIER®
Elbasvir NS5A inhibitor +Grazoprevir
NS3/4A protease inhibitor
MSD
50+100 mg /24h
Genotypes 1, 4
Genetic barrier dependent on genotype
July 28, 2016
Anti-HCV agents approved by ΕMA in 2016

VOSEVI® Velpatasvir
NS5A inhibitor +Sofosbuvir
NS5B polymerase Inhibitor
+Voxilaprevir NS3/4A protease
inhibitor Gilead
MAVIRET® Glecaprevir
NS3/4A protease inhibitor
+Pibrentasvir NS5A inhibitor
Abbvie
• [100/40 mg] x3 /24h with food
Genotypes 1-6
High genetic barrierγμός
• 100/400/100 mg /24h
Genotypes 1-6
High genetic barrier
Anti-HCV agents approved by ΕMA in 2017
July 26, 2017 July 26, 2017

Sofosbuvir + Daclatasvir (±Ribavirin)
Current IFNa-free regimens for genotype 1,4
Sofosbuvir/Ledipasvir* (±Ribavirin)
Paritaprevir/r/Ombitasvir + Dasabuvir (±Ribavirin)
Sofosbuvir/Velpatasvir*
Grazoprevir/Elbasvir (±Ribavirin)
Glecaprevir/Pibrentasvir*
Sofosbuvir/Velpatasvir/Voxilaprevir*
Sofosbuvir + Daclatasvir, Paritaprevir/r/Ombitasvir + Dasabuvir: not used in most countries; Sofosbuvir/Velpatasvir/Voxilaprevir: mostly used in DAA failures
*Also for GT5,6

Sofosbuvir + Daclatasvir +/- RBV for G1 patients (phase IIb study)
100
80
60
40
20
0
SVR12 (%)
100
29/ 29
100
14/ 15
S/D S/D/R
24 wks
100
21/ 21
S/D
19/ 20
95
S/D/R
24 wks
100
41/ 41
95
39/ 41
12 wks S/D S/D/R
Naive Prior PI (BOC/TPV) failures
• 20% cirrhotics • Almost all cured – 12 weeks adequate, RBV unnecessary
Sulkowski M et al. N Engl J Med 2014;370:211-21

ALLY-1: Advanced cirrhosis cohort
Total: n = 60; any GT; Baseline MELD score range 8–27 GT-1: n=45; GT-1/CP-B: 53%, GT-1/CP-C: 22%
Safety: Discontinuations due to adverse events, n = 1
SVR rates with SOF+DCV+RBV x12 weeks in HCV GT1 patients with advanced cirrhosis
Poordad F et al. Hepatology 2016;63:1493-505.
8291
76
92100
50
0
20
40
60
80
100
N=45 N=34 N=11 N=11 N=24 N=10
All GT1a GT1b CP-A CP-B CP-C
SVR12, %
CP: Child-Pugh

HEPATHER: SOF+DCV ±RBV x12 or 24 wks in GT1 pts
SVR4, %
SOF+DCV SOF+DCV+RBV SOF+DCV SOF+DCV+RBV x12 wks x12 wks x24 wks x24 wks
409 patients, 318 cirrhotics, 306 failures to PR±TPV/BOC
No cirrhosis Cirrhosis
S Pol et al. EASL 2015, Abstr. LB 03

SVR
12
(%
)
n N
141 142
143 143
143 143
211 212
66 66
211 211
67 67
212 214
66 68
Overall GT1a GT1b
141 141
215 215
71 71
Subgroup results do not include patients who withdrew consent or who were lost to follow-up.
Error bars: 95% CI.
ION-1: SOF/LDV ± RBV in GT1 treatment-naive patients – SVR12
Afdhal N et al. New Engl J Med 2014;70:1889-98.

ION-1: SVR rates* in GT1 treatment-naive cirrhotic patients (subgroup analysis)
* Subgroup results do not include patients who withdrew consent or were lost to follow-up.
No cirrhosis Cirrhosis
179 179
32 33
178 178
33 33
181 182
31 32
179 179
36 36
n N
SVR
12
(%
)
Afdhal N et al. New Engl J Med 2014;70:1889-98.

One patient achieved SVR12, but was not subgenotyped.
Error bars: 95% CI.
SVR
12
(%
)
n N
159 171
159 172
163 172
202 215
42 43
201 216
42 44
206 216
43 44
Overall GT1a GT1b
ION-3: Phase III SOF/LDV ± RBV in GT1 naive, non-cirrhotic patients – SVR12
Kowdley KV et al. New Engl J Med 2014;370:1879-88.

Predictors of relapse in ION-3 trial: SOF/LDV±RBV for 8 vs 12 wks in GT1 naive, non-cirrhotic patients
Patients with
relapse*, %
*Patients lost to follow-up or who withdraw
consent excluded CC non-CC <6 ≥6 MIU/ml IL28B genotype Baseline HCV RNA n/N 2/56 0/57 0/54 9/157 9/153 3/157 2/121 3/136 2/128 9/92 6/74 1/83
SOF/LDV x8wks SOF/LDV+RBV x8wks SOF/LDV x12wks
P=0.034
P=0.088
P=0.141
Kowdley KV et al. New Engl J Med 2014;370:1879-88.

SVR
12
(%
)
n N
82 86
84 88
84 85
102 109
20 23
107 111
23 23
108 109
24 24
Overall GT1a GT1b
87 88
110 111
23 23
Error bars: 95% CI.
One patient achieved SVR12, but was not subgenotyped.
ION-2: SOF/LDV ± RBV in GT1 treatment-experienced patients
Afdhal N et al. New Engl J Med 2014;370:1483-93.

ION-2: SVR rates in GT1 treatment-experienced cirrhotic patients (subgroup analysis)
No cirrhosis Cirrhosis
83 87
19 22
89 89
18 22
86 87
22 22
88 89
22 22
n N
Error bars: 95% CI.
SVR
12
(%
)
Afdhal N et al. New Engl J Med 2014;370:1483-93.

LDV/SOF Efficacy in Cirrhotics According to Treatment Experience, Duration, RBV
100
80
60
40
20
0
Total Treatment Naive
92 96 98 100
SV
R1
2 (
%)
118 204 133 58
96 98 97
47 45 33 36
100
Treatment Experienced
90
96 98
71 159 100 22
100
12 wks of LDV/SOF
12 wks of LDV/SOF + RBV
24 wks of LDV/SOF
24 wks of LDV/SOF + RBV
n =
Reddy KR et al. Hepatology 2015;62:79-86.

SYNERGY Trial: LDV/SOF for 12 wks in patients with G4
• Single-center, open-label phase 2a trial
• 38% of patients were TE; all were naive to DAAs; 33% had cirrhosis
• No deaths, SAEs, or grade 4 laboratory events; 1 D/C
GT4 HCV (N=21)
SOF/LDV
12 wks SVR12, %
95
Kapoor R et al. AASLD 2014, Abstract #240
French cohort
GT4 HCV (N=44)
SOF/LDV
12 wks SVR12, %
93
Abergel A et al. EASL 2015, Abstr. O56
Experienced: 22 (50%), Cirrhosis: 10 (23%)

ASTRAL-1: SOF/VEL STR for 12 Weeks in GT1 Patients
Feld JJ et al. N Engl J Med. 2015;373:2599-607.
323/328 206/210 117/118
SVR12, %

ASTRAL-1: SOF/VEL STR for 12 Weeks in GT4, GT5, GT6 Patients
Feld JJ et al. N Engl J Med. 2015;373:2599-607.
116/116 34/35 41/41
SVR12, %
SV
R1
2 (
%)
299/316 144/157 129/131 n/N =
Overall GT1a GT1b
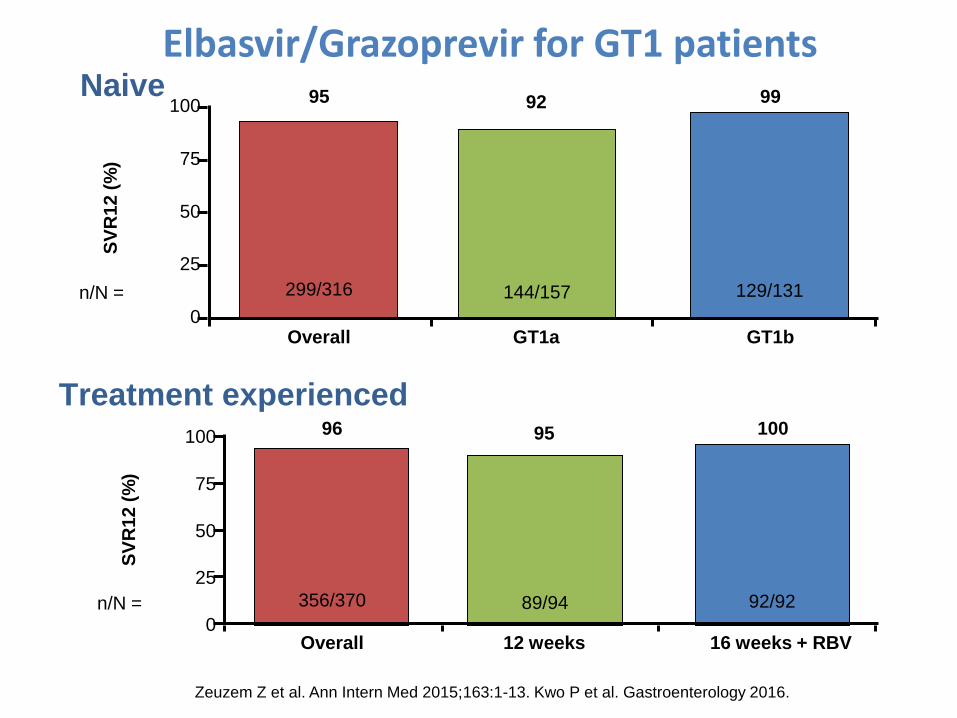
95 92 99 100
75
50
25
0
SV
R1
2 (
%)
356/370 89/94 92/92 n/N =
Overall 12 weeks 16 weeks + RBV
96 95 100 100
75
50
25
0
Naive
Treatment experienced
Elbasvir/Grazoprevir for GT1 patients
Zeuzem Z et al. Ann Intern Med 2015;163:1-13. Kwo P et al. Gastroenterology 2016.

SV
R1
2 (
%)
18/18 n/N =
GT 4
100% 100
75
50
25
0
SV
R1
2 (
%)
32/37 7/9 8/8 n/N =
Overall 12 weeks 16 weeks + RBV
87 79 100 100
75
50
25
0
Elbasvir/Grazoprevir for GT4 patients
Zeuzem Z et al. Ann Intern Med 2015;163:1-13. Kwo P et al. Gastroenterology 2016.
Naive
Treatment experienced
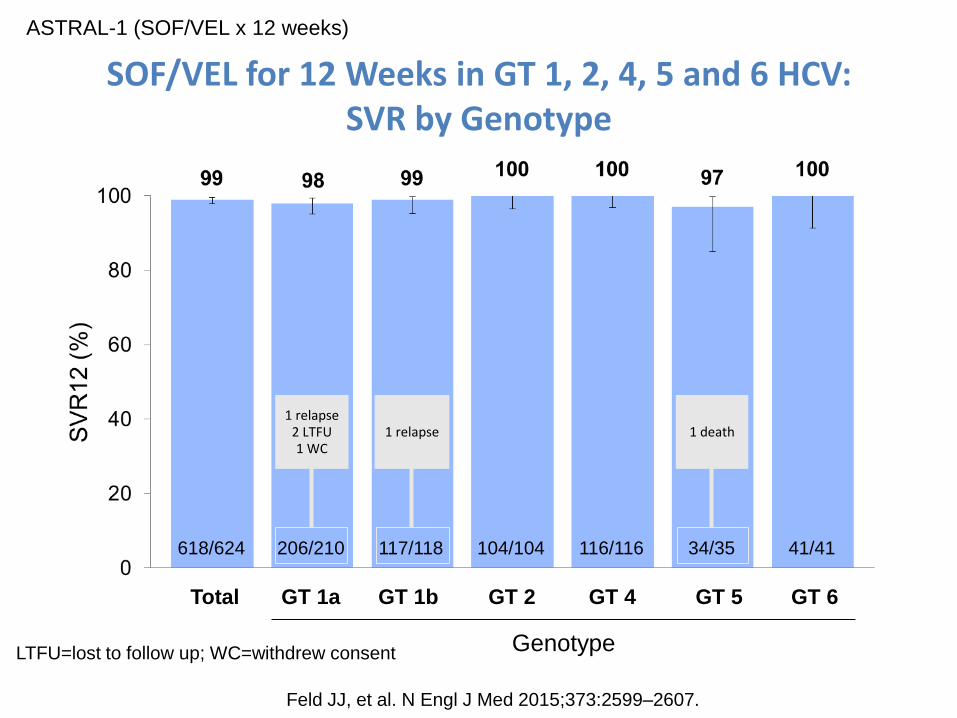
SOF/VEL for 12 Weeks in GT 1, 2, 4, 5 and 6 HCV: SVR by Genotype
ASTRAL-1 (SOF/VEL x 12 weeks)
618/624
Total
206/210 117/118 104/104 116/116 34/35 41/41
GT 1a GT 1b GT 2 GT 4 GT 5 GT 6
Genotype LTFU=lost to follow up; WC=withdrew consent
1 death 1 relapse 1 relapse
2 LTFU 1 WC
Feld JJ, et al. N Engl J Med 2015;373:2599–2607.

ENDURANCE-1: 8- vs 12-week treatment with G/P in non-cirrhotic naive or PR/SOF experienced patients with GT1
(Primary Efficacy)
Zeuzem S, et al. NEJM 2018;378:354-369.
PR: Peginterferon+Ribavirin; SOF: sofosbuvir; VF, virologic failure; ITT, all patients receiving study drug.
331
332
332
335 332
332
8 weeks
12 weeks
1 LTFU
331
331
ITT population, excluding
HIV co-infected and SOF-
experienced patients
ITT-PS population excluding patients
with premature D/C or virologic failure
prior to week 8, and missing data in the
SVR12 window
1 d/c
1 VF
1 LTFU

ENDURANCE-4: 12-week G/P in naive or PR/SOF experienced HCV patients with GT4–6 (Efficacy)
mITT population is ITT population excluding patients who did not achieve SVR12 for non-virologic reasons.
120
121
75
76
26
26 19
19
120
120
75
75
26
26 19
19
The patient who did not achieve SVR12 discontinued on day 12 due to a SAE (transient ischemic attack with a reasonable possibility of being related to study drug)
1 D/C
Overall GT4 GT5 GT6
1 D/C
Asselah T, et al. Clin Gastroenterol Hepatol 2018;16:417-426
PR: Peginterferon+Ribavirin; SOF: sofosbuvir.

SURVEYOR-II (Part 4): 8-week G/P in Naive or PR/SOF-Experienced Patients with GT2, 4–6 without Cirrhosis (Efficacy – ITT)
LLOQ, lower limit of quantification; TE, treatment emergent; * All patients had HCV RNA <LLOQ at last visit; † Patient had a medical history of gastric bypass. Exposure of GLE on Day 1 and Week 4 was >75% lower than the mean in patients in the same treatment arm; exposure of PIB was comparable to the other patients in the cohort.
97% (196/203, ITT) of GT2, 4, 5, or 6-infected patients without cirrhosis
achieved SVR12 following 8 weeks of G/P
In DAA-naive patients with GT2 infection, 8-week treatment was non-inferior to the historical 95%
SVR12 rate achieved with 12 weeks SOF + RBV
2 relapses
2 D/C
3 missing
SVR12 data*
196
203
2 relapses
1 D/C
1 D/C
2 missing
SVR12 data
1 missing
SVR12 data
142
145
43
46
2
2
9
10
Sequence Analysis
Patient A† Non-cirrhotic
(relapse)
Patient B Non-cirrhotic
(relapse))
NS3 Baseline None None
TE substitutions at failure None None
NS5A Baseline L31M L31M
TE substitutions at failure None None
GT2-infected patients
Asselah T, et al. Clin Gastroenterol Hepatol 2018;16:417-426

EXPEDITION-I: 12-week G/P for of Chronic HCV GT1, 2, 4, 5 or 6 Infection in Adults with Compensated Cirrhosis (Efficacy)
Forns X, et al. Lancet ID 2017; 17:1062–1068.
d/c, discontinuation; PTW, post-treatment Week; RAS, resistance-associated substitution. * SVR12 ITT and mITT are the same.
145
146
89
90
31
31
16
16
2
2
7
7
1 GT1a patient
relapsed at PTW8
n
N
G/P treatment achieved high SVR rates regardless of baseline patient or viral characteristics
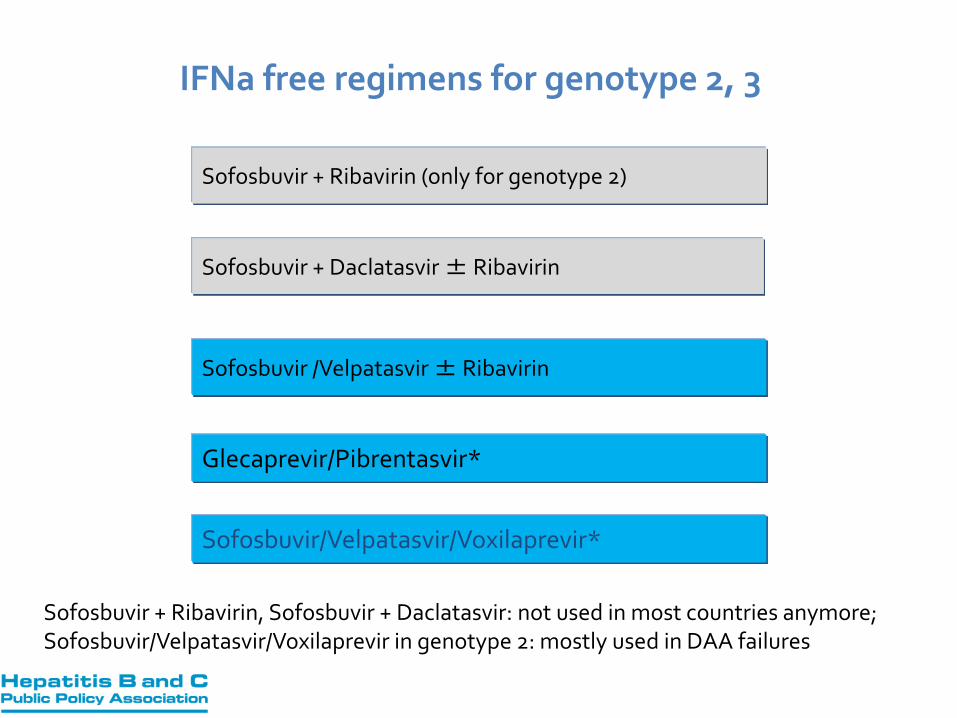
Sofosbuvir + Ribavirin (only for genotype 2)
IFNa free regimens for genotype 2, 3
Sofosbuvir + Daclatasvir ± Ribavirin
Sofosbuvir /Velpatasvir ± Ribavirin
Glecaprevir/Pibrentasvir*
Sofosbuvir + Ribavirin, Sofosbuvir + Daclatasvir: not used in most countries anymore; Sofosbuvir/Velpatasvir/Voxilaprevir in genotype 2: mostly used in DAA failures
Sofosbuvir/Velpatasvir/Voxilaprevir*

ASTRAL-2: SOF/VEL STR for 12 Weeks in GT2 Patients
133/134 124/132
SOF/VEL SOF + RBV P=0.018*
Foster GR et al. N Engl J Med 2015;373:2608-17.
104/104
Feld JJ et al. N Engl J Med. 2015;373:2599-607.

SVR
12
(%
)
264/277 221/275
P<0.001*
12 Weeks 24 Weeks
ASTRAL-3: Open-Label Trial - SVR12, Safety With Sofosbuvir/Velpatasvir in GT3 HCV
Foster GR et al. N Engl J Med 2015;373:2608-17.

100
ASTRAL-3: Open-Label Trial - SVR12, Safety With Sofosbuvir/Velpatasvir in GT3 HCV
Foster GR et al. N Engl J Med 2015;373:2608-17.
n/N =
SVR
12
(%
)
80
60
40
20
0
264/277
221/275
191/197
163/187
73/ 80
55/ 83
200/ 206
176/ 204
64/ 71
45/ 71
95
80
63
90 97 97 87
91
66
86
All Pts No Yes Naive Experienced
Cirrhosis
P < .001 (superiority)
SOF/VEL 12 wks
SOF + RBV 24 wks
Treatment History
SV
R1
2, %
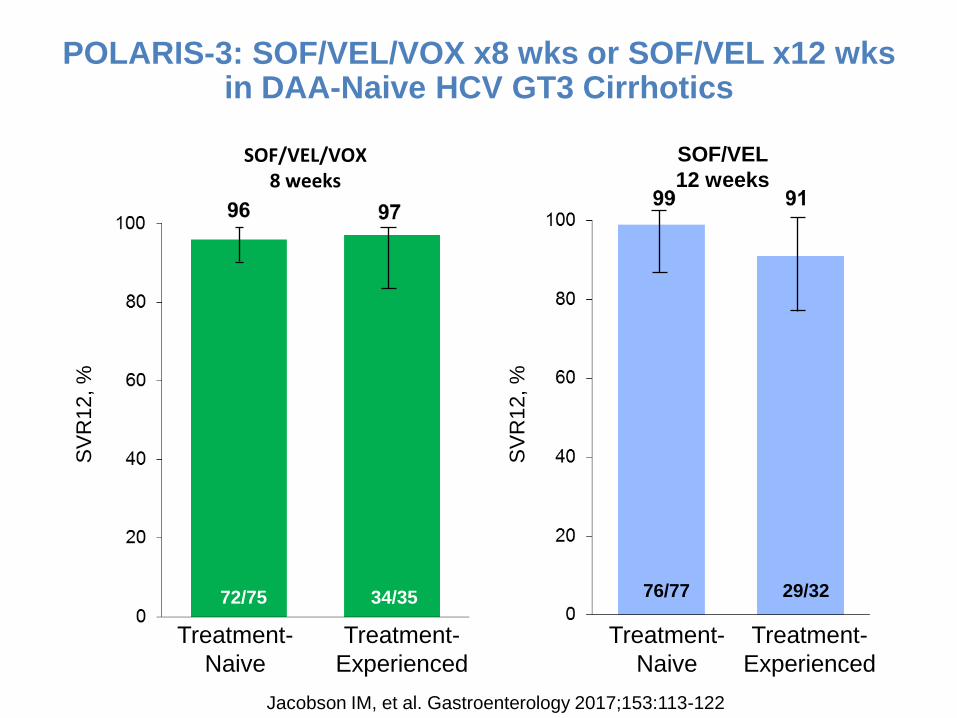
29/32 72/75 76/77
SOF/VEL
12 weeks
SOF/VEL/VOX 8 weeks
34/35
Treatment-
Naive
Treatment-
Experienced
Treatment-
Naive
Treatment-
Experienced
SV
R1
2, %
POLARIS-3: SOF/VEL/VOX x8 wks or SOF/VEL x12 wks in DAA-Naive HCV GT3 Cirrhotics
Jacobson IM, et al. Gastroenterology 2017;153:113-122

ENDURANCE-3: 8- or 12-week G/P vs 12-week SOF+DCV in naive non-cirrhotic HCV patients with GT3 (Efficacy)
BT, breakthrough; non-VF, non-virologic failure; RAS, resistance-associated substitution.
149
157
111
115
222
233
12 weeks 12 weeks 8 weeks
1 BT 3 relapses 7 non-VF
0 BT 1 relapses 3 non-VF
1 BT 5 relapses 2 non-VF
G/P is non-inferior to 12-week SOF+DCV
G/P 8 weeks is non-inferior to G/P 12 weeks
n
N
149
155
111
112
222
226 n
N
12 weeks 12 weeks 8 weeks
Zeuzem S, et al. NEJM 2018;378:354-369.

SURVEYOR-II (Part 3): Patients with HCV GT3 Infection with Prior Treatment Experience and/or Cirrhosis (Efficacy – ITT)
Wyles DL, et al. Hepatology 2017 Sep 19, [Epub ahead of print]
• Substitutions detected by next- • generation sequencing at 15% • detection threshold
(NS3: 36, 43, 54, 55, 56, 80, • 155, 156, 166, and 168;
NS5A: 24, 28, 29, 30, 31, • 32, 58, 92, and 93)
TE
Non-cirrhotic
12 weeks
TE
Non-cirrhotic
16 weeks
TN
Cirrhotic
12 weeks
TE
Cirrhotic
16 weeks
2 relapses 1 relapse 1 LTFU
1 breakthrough
1 relapse
20
22 21
22
39
40
45
47
Sequence Analysis*
Patient A Non-cirrhotic
12 weeks (relapse)
Patient B Non-cirrhotic
12 weeks (relapse))
Patient C Non-cirrhotic
16 weeks (relapse)
Patient D Cirrhotic 16 weeks (relapse)
Patient E Cirrhotic 16 weeks
(breakthrough)
NS3 Baseline None None None None A166S
Failure None None Y56H, Q168R None A156G, A166S
NS5A Baseline Y93H A30K A30K None None
Failure Y93H A30K, Y93H A30K, Y93H L31F, Y93H A30K, Y93H
4 of 5 patients with virologic failure had treatment-emergent
substitutions

Treatment recommendations for TN and TE* patients without cirrhosis SOF/VEL GLE/PIB
SOF/VEL/ VOX
LDV/SOF GZR/EBR OBV/PTV/r+
DSV
GT1a
TN 12 wk 8 wk No 8-12 wk 12 wk
(HCV RNA ≤800,000 IU/ml) No
TE 12 wk 8 wk No No 12 wk
(HCV RNA ≤800,000 IU/ml) No
GT1b TN 12 wk 8 wk No 8-12 wk
8 wk (F0-F2) 12 wk (F3)
8 wk (F0-F2) 12 wk (F3)
TE 12 wk 8 wk No 12 wk 12 wk 12 wk
GT2 TN 12 wk 8 wk No No No No
TE 12 wk 8 wk No No No No
GT3 TN 12 wk 8 wk No No No No
TE 12 wk 12 wk No No No No
GT4 TN 12 wk 8 wk No 12 wk
12 wk (HCV RNA ≤800,000 IU/ml)
No
TE 12 wk 8 wk No No No No
GT5 TN 12 wk 8 wk No 12 wk No No
TE 12 wk 8 wk No No No No
GT6 TN 12 wk 8 wk No 12 wk No No
TE 12 wk 8 wk No No No No
EASL 2018 Recommendations on Treatment of Hepatitis C 2018, J Hepatol 2018

Treatment recommendations for TN and TE patients with compensated cirrhosis
SOF/VEL GLE/PIB SOF/VEL/VOX LDV/SOF GZR/EBR OBV/PTV/r+DSV
GT1a
TN 12 wk 12 wk No 12 wk 12 wk
(HCV RNA ≤800,000 IU/ml) No
TE 12 wk 12 wk No No 12 wk
(HCV RNA ≤800,000 IU/ml) No
GT1b TN 12 wk 12 wk No 12 wk 12 wk 12 wk
TE 12 wk 12 wk No 12 wk 12 wk 12 wk
GT2 TN 12 wk 12 wk No No No No
TE 12 wk 12 wk No No No No
GT3 TN No 12 wk 12 wk No No No
TE No 16 wk 12 wk No No No
GT4 TN 12 wk 12 wk No 12 wk
12 wk (HCV RNA ≤800,000 IU/ml)
No
TE 12 wk 12 wk No No No No
GT5 TN 12 wk 12 wk No 12 wk No No
TE 12 wk 12 wk No No No No
GT6 TN 12 wk 12 wk No 12 wk No No
TE 12 wk 12 wk No No No No
EASL 2018 Recommendations on Treatment of Hepatitis C 2018, J Hepatol 2018

GT
DAA
Naive
no cirrhosis
PR/SOF exper.
no cirrhosis
Naive
cirrhosis
PR/SOF exper.
cirrhosis
1,2,
4,5,
6
SOF/VEL x12 weeks
GLE/PIB x8 weeks x12 weeks
3
SOF/VEL x12 weeks x12 weeks + RBV (or SOF/VEL/VOX)
GLE/PIB x8 weeks x12 weeks x16 weeks
Synopsis of treatment recommendations for pangenotypic regimens for TN and TE patients without or with compensated cirrhosis
PR: PegIFNa+RBV

• Protease inhibitors are contraindicated
• SOF/LDV, SOF/VEL: the only DAA options
• Addition of RBV increases the SVR rates
Treatment recommendations for HCV patients with decompensated cirrhosis
EASL 2018 Recommendations on Treatment of Hepatitis C 2018, J Hepatol 2018

SOLAR-1: SVR12 and safety according to CTP score in decompensated cirrhosis
100
80
60
40
20
0
SVR
12
(%
)
Overall CTP B CTP C
LDV/SOF + RBV 12 wks LDV/SOF + RBV 24 wks
87 89
45/52 42/47
87 89 86 90
26/30 24/27 19/22 18/20
3 relapses 1 death 1 relapse
2 deaths
1 relapse 1 death 1 LTFU 1 relapse
1 death
Patients n (%)
CTP B CTP C
12 Wks
(n=30)
24 Wks
(n=29)
12 Wks
(n=23)
24 Wks
(n=26)
AE 29 (97) 27 (93) 23 (100) 26 (100)
SAE 3 (10) 10 (34) 6 (26) 11 (42)
Treatment-emergent, -related
SAEs 2 (7) 0 0 2 (8)
Treatment D/C due to AEs 0 1 (3) 0 2 (8)
Charlton M et al. Gastroenterology 2015;149:649-59.

SOLAR-2: SOF/LDV+RBV in HCV decompensated cirrhotics and transplant patients
M Manns et al. Lancet Infect Dis 2016;16:685-97.

SOLAR-2: SOF/LDV+RBV in HCV decompensated cirrhotics and transplant patients
MELD score change from baseline to follow-up week-4
M Manns et al. Lancet Infect Dis 2016;16:685-97.

ASTRAL-4: SOF/VEL ± RBV in HCV Patients with Decompensated Liver Disease
75/90 82/87 77/90 60/68 65/68 65/71 7/14 11/13 6/12 GT2 4/4 GT4 4/4
GT2 4/4 GT4 2/2
GT2 3/4 GT4 2/2 GT6 1/1
Curry MP et al. N Engl J Med 2015;373:2618-28.
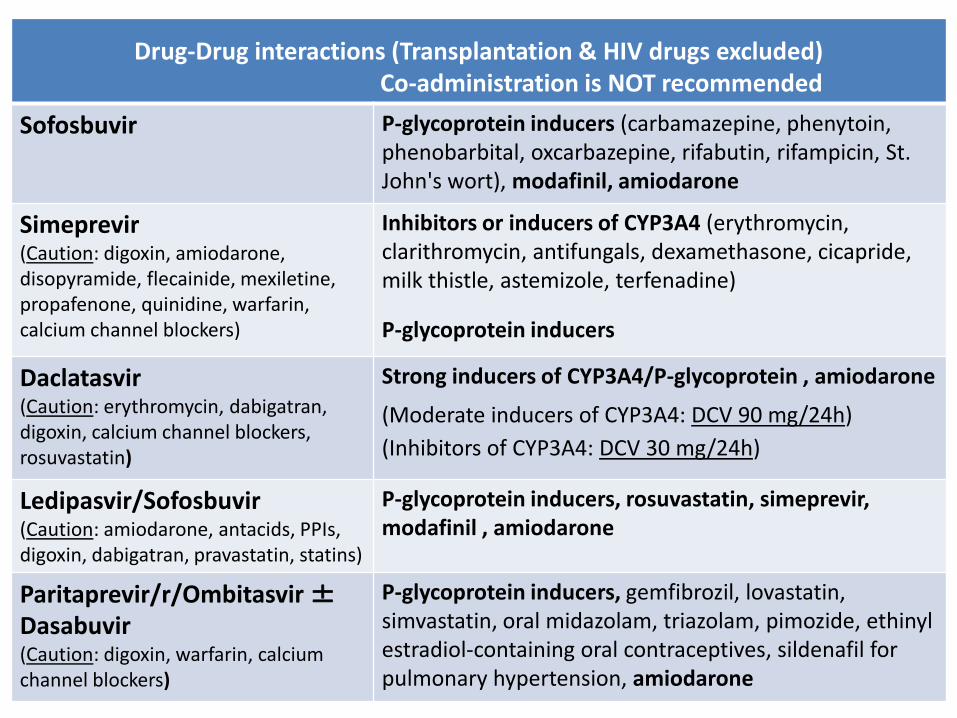
Drug-Drug interactions (Transplantation & HIV drugs excluded) Co-administration is NOT recommended
Sofosbuvir P-glycoprotein inducers (carbamazepine, phenytoin, phenobarbital, oxcarbazepine, rifabutin, rifampicin, St. John's wort), modafinil, amiodarone
Simeprevir (Caution: digoxin, amiodarone, disopyramide, flecainide, mexiletine, propafenone, quinidine, warfarin, calcium channel blockers)
Inhibitors or inducers of CYP3A4 (erythromycin, clarithromycin, antifungals, dexamethasone, cicapride, milk thistle, astemizole, terfenadine)
P-glycoprotein inducers
Daclatasvir (Caution: erythromycin, dabigatran, digoxin, calcium channel blockers, rosuvastatin)
Strong inducers of CYP3A4/P-glycoprotein , amiodarone
(Moderate inducers of CYP3A4: DCV 90 mg/24h)
(Inhibitors of CYP3A4: DCV 30 mg/24h)
Ledipasvir/Sofosbuvir (Caution: amiodarone, antacids, PPIs, digoxin, dabigatran, pravastatin, statins)
P-glycoprotein inducers, rosuvastatin, simeprevir, modafinil , amiodarone
Paritaprevir/r/Ombitasvir ± Dasabuvir (Caution: digoxin, warfarin, calcium channel blockers)
P-glycoprotein inducers, gemfibrozil, lovastatin, simvastatin, oral midazolam, triazolam, pimozide, ethinyl estradiol-containing oral contraceptives, sildenafil for pulmonary hypertension, amiodarone
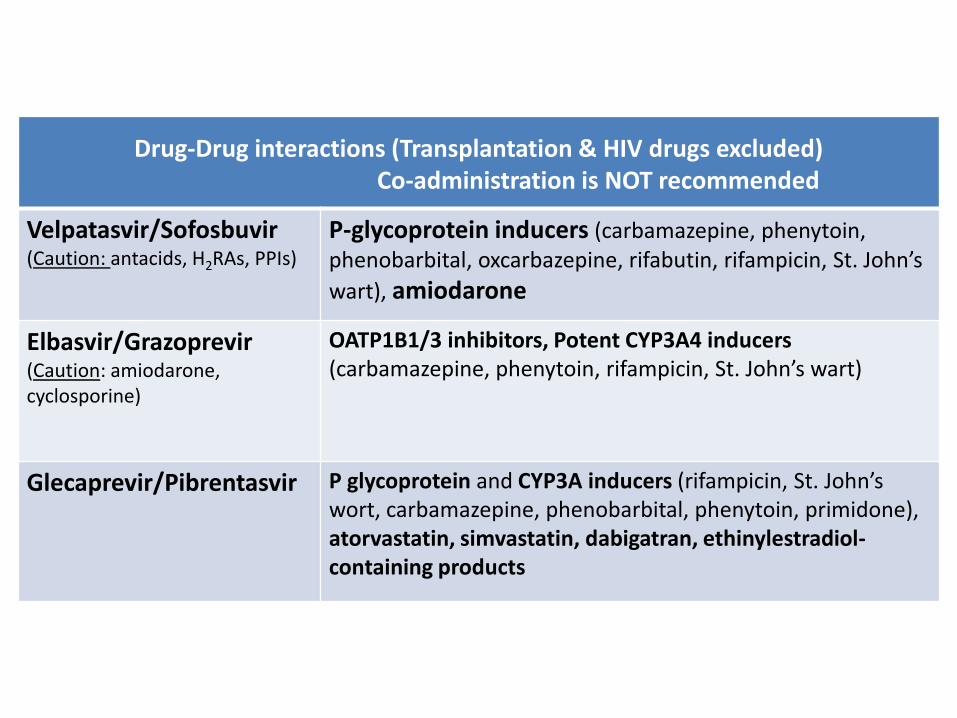
Drug-Drug interactions (Transplantation & HIV drugs excluded) Co-administration is NOT recommended
Velpatasvir/Sofosbuvir (Caution: antacids, H2RAs, PPIs)
P-glycoprotein inducers (carbamazepine, phenytoin, phenobarbital, oxcarbazepine, rifabutin, rifampicin, St. John’s
wart), amiodarone
Elbasvir/Grazoprevir (Caution: amiodarone, cyclosporine)
OATP1B1/3 inhibitors, Potent CYP3A4 inducers (carbamazepine, phenytoin, rifampicin, St. John’s wart)
Glecaprevir/Pibrentasvir P glycoprotein and CYP3A inducers (rifampicin, St. John’s wort, carbamazepine, phenobarbital, phenytoin, primidone), atorvastatin, simvastatin, dabigatran, ethinylestradiol-containing products
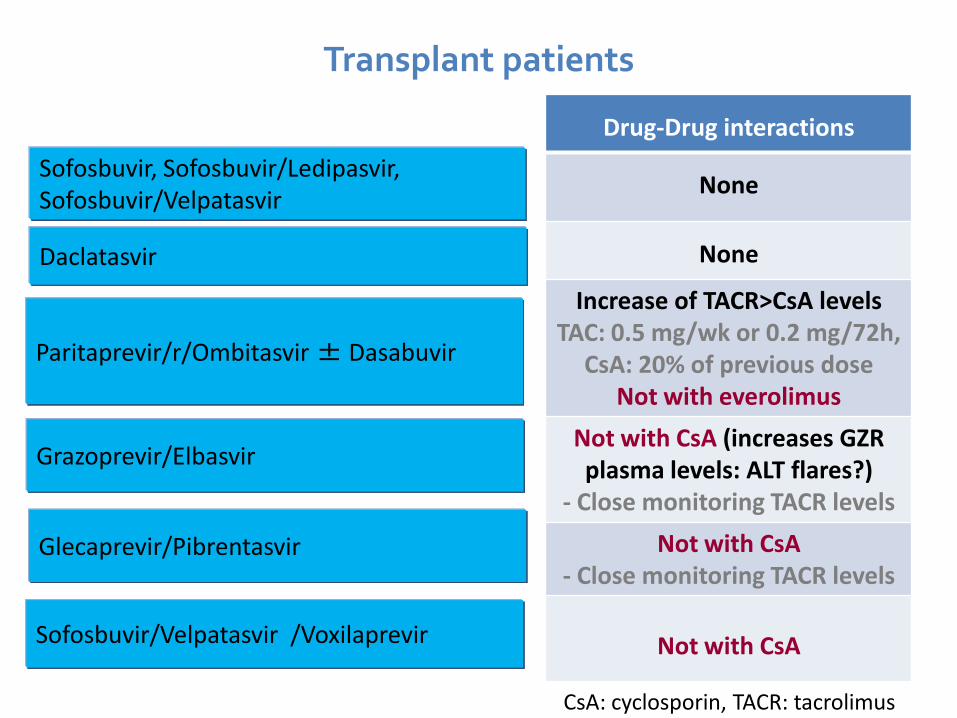
Sofosbuvir, Sofosbuvir/Ledipasvir, Sofosbuvir/Velpatasvir
Daclatasvir
Paritaprevir/r/Ombitasvir ± Dasabuvir
Drug-Drug interactions
None
None
Increase of TACR>CsA levels TAC: 0.5 mg/wk or 0.2 mg/72h,
CsA: 20% of previous dose Not with everolimus
Not with CsA (increases GZR plasma levels: ALT flares?)
- Close monitoring TACR levels
Not with CsA - Close monitoring TACR levels
Not with CsA
Glecaprevir/Pibrentasvir
Grazoprevir/Elbasvir
Transplant patients
Sofosbuvir/Velpatasvir /Voxilaprevir
CsA: cyclosporin, TACR: tacrolimus

Drug-Drug interactions with HIV drugs
None
Not with darunavir, lopinavir, etravirine ή nevirapine - DCV 30 mg with atazanavir/r, DCV 90 mg with efavirenz
Not with cobicistat*, tripanavir/r
Not with efavirenz, rilpivirine ή lopinavir
Not with efavirenz (closer follow-up for TDF AEs)
Not with efavirenz (closer ALT fup with atazanavir, darunavir, lopinavir, saquinavir, tripanavir)
Not with atazanavir, darunavir, efavirenz, lopinavir, etravirine, nevirapine
Not with atazanavir, efavirenz, lopinavir, etravirine, nevirapine (closer follow-up for TDF AEs) *cobicistat: elvitegravir + cobicistat + emtricitabine + tenofovir
Sofosbuvir
Daclatasvir
Sofosbuvir/Ledipasvir
Paritaprevir/r/Ombitasvir ± Dasabuvir
Sofosbuvir/Velpatasvir
Grazoprevir/Elbasvir
HCV & HIV coinfection IFNa-free regimens similar efficacy to HCV monoinfected patients
Glecaprevir/Pibrentasvir
Sofosbuvir/Velpatasvir /Voxilaprevir
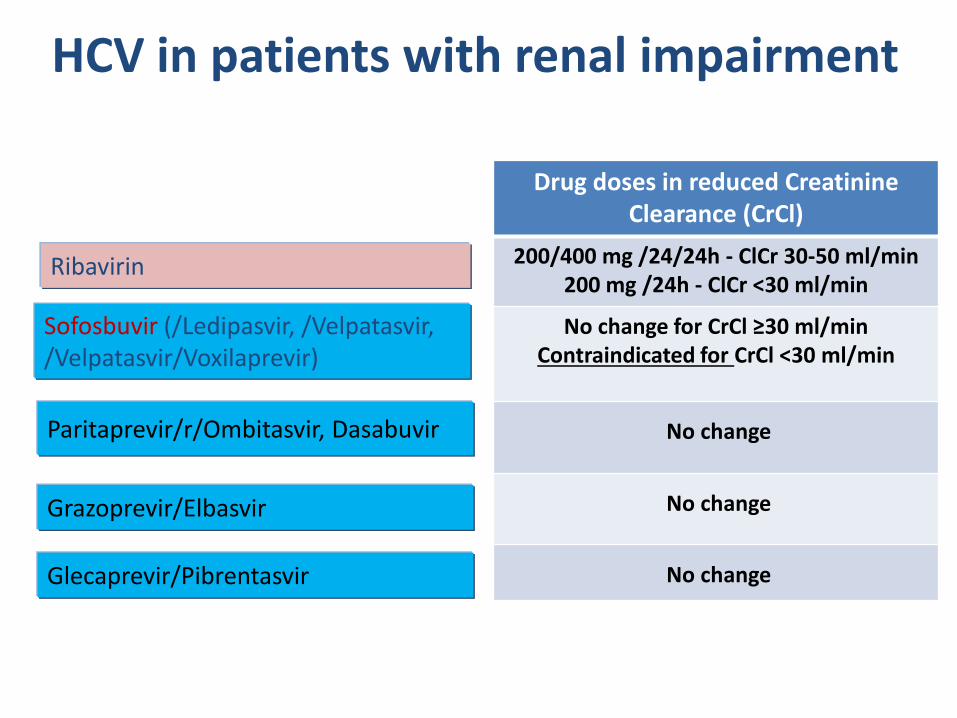
Sofosbuvir (/Ledipasvir, /Velpatasvir, /Velpatasvir/Voxilaprevir)
Paritaprevir/r/Ombitasvir, Dasabuvir
HCV in patients with renal impairment
Drug doses in reduced Creatinine Clearance (CrCl)
200/400 mg /24/24h - ClCr 30-50 ml/min 200 mg /24h - ClCr <30 ml/min
No change for CrCl ≥30 ml/min Contraindicated for CrCl <30 ml/min
No change
No change
No change
Ribavirin
Grazoprevir/Elbasvir
Glecaprevir/Pibrentasvir

New DAAs - Conclusions
Increasing number of licensed agents for patients with HCV
-Availability and accessibility vary among countries
Shortening of treatment duration to 8 weeks is possible in some non-cirrhotic
patients, with no loss of efficacy
Treatment options available irrespective of cirrhosis status
The proportion of patients failing to respond to DAAs is small and re-
treatment options are available for most patients
-NS5A inhibitor failures remain a treatment challenge
The availability of DAAs means that HCV cure is now a reality for most patients