care bundle for women with previous caesarean section at ... after previous cs care bundle... ·...
TRANSCRIPT
Care Bundle for women with previous Caesarean Section at risk of a morbidly adherent placenta
List of Contributors:
Miss Sara Paterson Brown (CHAIR) FRCOG FRCS, Queen Charlotte’s
Hospital London
Dr Sue Catling, Obstetric Anaesthetist, Singleton Hospital, Swansea
Dr Tracey A Johnston MRCOG, Clinical Director, Birmingham Women’s
Hospital, Birmingham
Dr Josephine McHugo,FRCR FRCP FRCPCH Radiologist, Birmingham
Women’s Hospital, Birmingham
Dr Kanchan P Rege, Haematologist, Peterborough District Hospital,
Peterborough
Dr Helen J Scholefield, MRCOG, Liverpool Women’s Hospital, Liverpool
Professor Anthony Watkinson FRCS FRCR, Interventional Radiologist, Royal Devon and Exeter Hospital and Peninsula Medical School, Exeter Devon
Miss Claire Singh, RCOG Research Midwife
Professor James Walker FRCOG, NPSA Clinical Associate
Benedette La Corte RCOG, administrative support
Group members;
Miss Sara Paterson Brown, Dr Helen J Scholefield, Professor Anthony Watkinson, Miss Claire Singh, Dr Sue Catling, Professor James Walker, Dr Tracey A Johnston, Dr. Josephine McHugo, Dr Kanchan P Rege, Ms Emma Boakes, Ms Bridget James, Ms Wendy Martin, Ms Dinah Matthew, Ms Valerie Ann Spalton
1
Contents
Abbreviations
1. Introduction 4
1.1 Patient selection 4
2 Background to Care Bundles 4
3 The Care Bundle in Application 6
4 Antenatal workup 7
4.1 Routine imaging 7
4.2 Consultant review and ongoing consultant input: 7
4.3 Avoid / treat anaemia 7
4.4 Timing of follow-up scan and further imaging 8
5 Gestation of elective delivery 9
6 Multidisciplinary pre-operative workup: 10
6.1 Blood availability 10
6.2 Cell salvage 10
6.3 Interventional radiology 10
6.4 Level 2 critical bed availability on site 11
7 Consent 12
8 Anaesthetic issues 12
9 Surgical procedures 12
a) Routine access to the uterus 12
b) Accessing the uterine cavity deliberately avoiding the placenta 12
10 Postnatal care for those where the placenta has been left in situ 12
10.1 At surgery 13
10.2 Management in the immediate postpartum period 13
10.3 Ongoing care and follow-up 13
References 15
Appendix 1. Placenta Praevia after previous caesarean 19 section-Care Bundle
Appendix 2. Sample specific consent form for surgery 20
2
Abbreviations AAGBI Association of Anaesthetists of Great Britain and Ireland CEMACH Confidential Enquiry in Maternal and Child Health CS caesarean section ERPC Evacuation of retained products of conception ESUR European Society of Urogenital Radiology GMC General Medical Council Hb haemoglobin hCG human chorionic gonadatrophin IHI Institute for Health Improvement IR interventional radiology LSCS lower section caesarean segment MRI magnetic resonance imaging MSBOS Maximum Surgical Blood Ordering Schedule NICE National Institute for Clinical Excellence NPSA National Patient Safety Agency OAA Obstetric Anaesthetists' Association PPH post partum haemorrhage RCOG Royal College of Obstetricians and Gynaecologists
3
1. Introduction A morbidly adherent placenta occurs when the placenta adheres to or invades into or through the myometrium, and can occur when the placenta is located over a previous scar with a deficient decidua basalis. It is increasingly common with increasing numbers of previous caesarean section 1 2 but can also occur following myomectomies, or after a previous manual removal of the placenta from the same placental site. Women with a morbidly adherent placenta (all types grouped together and termed placenta accreta for the purposes of this document) have an increased risk of morbidity and mortality due to massive obstetric haemorrhage at delivery. 1 3 4
This care bundle has been designed by a multidisciplinary expert group to highlight an approach to clinical care, which would reasonably be expected to reduce these risks in a simple, practical and achievable way. They constitute the considered minimum standards of care in this clinical condition. The care bundle comprises 6 criteria which all need to be satisfied for the care bundle to be ‘passed’ and although it focuses on the care of women who have had a previous CS where the placenta is located over the old scar it would be equally pertinent to apply it to other women in whom placenta accreta is suspected and CS is planned. This support document summarises briefly how these decisions were made and provides a reference list for further reading to help inform clinicians 1.1 Patient selection: All women undergoing CS at high risk of placenta accreta should be managed in accordance with this care bundle. This will include:
• Women with one or more previous CS and placenta praevia • Women with a previous scar where imaging of placental localisation
has found the placenta to be lying over the previous scar, even if it is well clear of the internal cervical os.
Routine placental localisation at 20 weeks should have highlighted those women who need a follow-up scan at 32 weeks (Other women at risk of placenta accreta such as women needing CS after previous myomectomies / manual removals could also have the bundle applied to them)
2. Background to care bundles
‘Care bundles’ are a concept that was developed by the Institute for Healthcare Improvement (IHI) in North America; to describe a collection of interventions needed to effectively and safely care for patients. Ideally, a care
4
bundle should be small and straightforward with a set of three to five practices or precautionary steps 5.
Each component of a care bundle is an intervention or practice in its own right, with a solid, sound evidence base. The IHI specify that there should be no controversy surrounding the components of a care bundle, with the focus being on how to deliver the best care, -not what the best care should be 6.
A care bundle does not introduce any new ways of working, but combines these elements of ‘good practice’ into one cohesive bundle, that when applied together improve the quality of care patients receive and aim to improve patient outcomes.
It is crucial that a care bundle contains components that can be applied to a patient in one clinical episode, so that each application of the bundle is self-contained. Each component of a care bundle should be easy to complete, with a tick box response, or a ‘yes’ or ‘no’ answer. For example “Yes-maternal heart rate was monitored,” or “no-this component was not achieved”.
This way the completion of a care bundle is easily monitored. Each care bundle is applied to every patient, every time 7, therefore making the success of each care bundle application assessable with an ‘all or nothing measure’. All components of the bundle need to have been achieved to have successful completion of the care bundle in that application.
Within the UK, care bundles have previously been developed in the areas of critical care nursing, infection control, preventative antibiotics for surgery and medicines safety, and have formed a large part of the work of the Patient Safety Initiative. Obstetric care bundles within the UK have not yet been implemented. The current work of the RCOG and NPSA in this area is therefore pioneering within the field of obstetrics and midwifery.
As with any change implemented within an organisation, staff can be apprehensive about new processes. However with good planning, structured implementation and good communication, teams will be aware of the benefits of care bundles to patient safety and the benefits to their working time.
In summary, care bundles have to be adhered to and signed off. A care bundle is in itself a way to prompt people to act according to best practice.
5
3. The Care Bundle in Application For the purpose of the pilot, the bundle should be applied to women with one or more previous CS and placenta praevia or placenta located over the previous uterine scar.
1. Prior to going to theatre, remove the care bundle (BLUE) sheet from
the back of this document. (Appendix 1)
2. Commence completing the care bundle sheet prior to surgery while the woman is being prepared for theatre.
3. Complete the care bundle during or after the operation once it is clear which staff have been involved
4. Tick the box next to the components that have been achieved.
5. The Doctor completing the care bundle is required to put his/her initials once he/she has completed the care bundle. .
6. Once the surgery has been completed, the outcome box at the bottom of the care bundle must be filled in.
7. Please return the completed care bundle sheet to the Clinical on site lead for the project, whose details are shown below.
If you have any further questions about Care Bundles please contact:
[INSERT STICKER WITH CLINICAL ON SITE LEAD]
or
Claire Singh Research Midwife at the Royal College of Obstetricians and Gynaecologists on 02077726430 or [email protected]
6
4. Antenatal workup The key to good antenatal care in placenta accreta is to recognize the risk of it and make plans accordingly. This requires an index of suspicion, and an antenatal screening process focused on identifying those women with a previous CS whose placenta lies over the old scar. 4.1 Routine Imaging Saving Mother’s Lives recommends “Women who have had a previous caesarean section must have placental localisation in their current pregnancy to exclude placenta praevia, and if present, to enable further investigation to try to identify praevia accreta and the development of safe management strategies” 3.
Women identified at the 20-week scan as having a low or anterior placenta with a history of a previous CS should have a further transabdominal ultrasound scan using the full bladder technique at 32 weeks. This scan aims to identify whether the placenta overlies the old scar and not just to identify the lower edge of the placenta in relation to the internal os. A transvaginal scan can help with assessing the lower edge of the placenta. A suggested ultrasound request / prompt is as follows: ‘Patient at risk of placenta accreta, please rescan at 32 weeks paying particular attention to place of placenta in lower segment around scar site and not just distance from os’.
A low placenta in the midtrimester is likely to persist into the third trimester in 50% of cases and of those still present at around 32 weeks 8, the vast majority will still be a placental praevia at term 9.
4.2. Consultant review and ongoing consultant input: Women who are found to have the placenta lying over the old scar or who have placenta praevia should then see the consultant obstetrician after this second scan (i.e. approx 32 weeks) to discuss the implications for delivery and make plans for antenatal care, further imaging, multidisciplinary preparation for delivery, and the delivery itself. The risk of hysterectomy should also be mentioned and the various different surgical options should be discussed. Since up to 40% of cases are likely to need to be delivered as an emergency, a clear care plan needs to be placed in the case records, including which staff to be called in for an elective or an emergency delivery. 4.3. Avoid / treat anaemia: All women should have their haematinics checked but it is particularly important for those at increased risk of obstetric haemorrhage. (NB it must be borne in mind that serum Vitamin B12 is commonly low despite normal tissue levels in pregnancy). If iron studies indicate iron deficiency, oral iron supplementation should be commenced (the usual rate of Hb rise in iron deficiency is 0.2g/dl/day). Failure to respond to oral iron therapy (in genuine uncomplicated iron deficiency) is commonly due to poor compliance related to
7

side effects. In such cases, the oral iron preparation should be substituted by another oral iron preparation or by parenteral therapy. Iron sucrose may be given intravenously in repeated small doses and iron dextran as a single “total dose” intravenously. Preparations for intramuscular use are also available. Restoration of a normal haemoglobin is speedier using parenteral methods 10. There is no proven role for erythropoietin therapy in this setting for women not in chronic renal failure. 4.4 Timing of follow-up scan and further imaging Complete placenta praevia at 32 weeks gestation is likely to persist in 90 % of cases 11 12, thus as part of good practice a scan should be performed prior to delivery to exclude the 10% of cases where the placenta has migrated. Features of placenta accreta may be looked for at the 32-week scan or at a subsequent specialist follow-up scan depending on local expertise. Ultrasound features consistent with accreta include:
1. Obliteration of the bladder- uterine interface with loss of the normal hypoechogenic retro placental myometrial zone.
2. Adjacent sonolucent spaces
3. Increased vascularity of the bladder wall seen on colour Doppler. Any one of these findings are consistent with abnormal placental invasion sensitivity 0.77 specificity 0.96 positive predictive value 0.65 negative predictive value 0.98 13 although some authors suggest the loss of the hypoechogenic zone between the retroplacenta area and the myometrium can be seen in a normal placenta 14. Patients with inconclusive ultrasound appearances should be considered for MRI. Features of abnormal placentation on precontrast MRI include
1. Thickened dark nodular contour of the placenta – uterine interface with extension of the dark bands within the placenta
2. Mass effect of the placenta causing bulging of the outer margin of the
uterus
3. Heterogenous placenta signal on T2 – weighted Haste with large vessels or placenta lakes
The use of Gadolinium is not licensed for use in pregnancy in the UK but it is widely used in North America and Europe in this clinical setting. Therefore in cases where unenhanced MRI scan remain inconclusive its use should be considered on an individual patient following a risk - benefits analysis 15.
8
The value of MRI is variably reported and local expertise will influence the use and interpretation of it. The definitive diagnosis, however, is never made until surgery, so although it can help inform and raise the index of suspicion, it can never exclude the possibility and preparations for accreta still need to go ahead as a precaution. 5. Gestation of elective delivery It is accepted practice that in cases of placenta praevia where the placenta covers, or the placental edge is less than 2cm from, the internal cervical os, delivery by caesarean section should be offered. Elective caesarean sections should normally be performed at 39 weeks 16 due to the increased risk of neonatal respiratory morbidity compared to delivery after the onset of labour, and the fact that the risk of morbidity is gestational age dependant (approximately 7% at 37 weeks, 4% at 38 weeks and <2% at 39 weeks) 17 However with the increased risks of morbidity due to heavy bleeding with placenta praevia it is accepted that earlier delivery at around 38 weeks is a reasonable compromise 11.
Maternal morbidity and mortality are higher following emergency caesarean section compared to elective caesarean section, and this may be more so in cases of morbidly adherent placenta due to difficulties in arranging optimal operating circumstances out of hours. The later the elective section is planned, the more likely the chance of the woman going into labour or having a significant bleed prior to the date of elective surgery, necessitating ‘emergency’ intervention. Risks of neonatal morbidity therefore need to be balanced against the risks of non-elective surgery in the case of suspected or confirmed placenta accreta. There is little in the literature addressing this problem, therefore members of the expert panel reviewed the timings of elective and emergency caesarean section for placenta praevia (NOT suspected placenta accreta) in over one thousand cases from four major teaching hospitals over a ten-year period. The findings showed that delivery of women with placenta praevia is rarely required prior to 32 weeks but approximately 40% will be delivered as an emergency prior to 38 weeks. This agrees with previous published data on placenta praevia in general 18. Studies have also shown that those requiring emergency delivery are unpredictable.
Elective delivery before 37 weeks cannot therefore be advocated, as to achieve a significant reduction in emergency delivery, it would have to be performed around 32 weeks gestation, which would have a significant impact on neonatal morbidity. Cases should therefore be assessed on an individual basis, taking into account local circumstances and facilities for elective surgery. The maternal and neonatal risks should be weighed up to determine the optimal timing of delivery, but this should not be done electively before 37 weeks.
6. Multidisciplinary pre-operative planning:
9
This should be planned by the consultant obstetrician and co-ordinated by them or a delegated senior member of the team. The multi-disciplinary planning should include all relevant specialities. (e.g anaesthetist, haematologist) 6.1 Blood availability There should be good communication with the Blood Bank to allow cross-matched red cells to be available for delivery as per the hospital’s maximum surgical blood ordering schedule (MSBOS). The blood will need to have been cross-matched within 7 days prior to delivery due to the risk of red-cell allo-immunisation in late pregnancy. All blood banks supplying obstetric units keep stores of red cells, fresh frozen plasma and cryoprecipitate 19.
Platelets, however, are commonly kept off site and although they are rarely needed in obstetric haemorrhage, if needed they will need to be ordered in from the local National Blood Transfusion Centre (again necessitating clear communication between the clinicians and Blood Bank). Recombinant Factor VIIa is being used increasingly in massive obstetric haemorrhage, and local arrangements to procure it rapidly if needed should be considered 19. 6.2 Cell salvage Cell salvage can reduce or eliminate the need for exposure to allogeneic blood, thus reducing patients’ exposure to the well-documented risks of allogeneic blood transfusion 20.
Secondly, in the rare case of severe, uncontrollable haemorrhage, the cell saver can re-circulate the ongoing blood loss and continue to provide red cells for tissue oxygenation even when the loss outstrips the planned provision of the blood bank 21. The use of cell salvage in obstetric haemorrhage is now recommended by CEMACH, NICE, and both AAGBI/OAA and RCOG Guidelines 3 22 23 and the evidence for its safety and effectiveness is extensively examined in 2 recent major Review Articles 24 25 .
In 2005-2006 38% of maternity units in the UK were using cell salvage 26 and there have been no proven complications of the technique reported through the UK Haemovigilance System 20. It is likely that the total number of obstetric cell salvage cases is approaching 1000 24 26 27 28. Experience with the use of and the availability of cell savers in obstetrics is increasing, but it is by no means universally available yet. It is strongly recommended for women who refuse blood products, as it provides the only means of replacing red cells in major haemorrhage 21. For such patients, transfer to a centre providing cell salvage expertise should be considered if this is not available locally. 6.3 Interventionalradiology Interventional Radiology (IR) should be considered in both the elective and emergency management of placenta praevia and placenta accreta. Electively it can be used as a prophylactic measure in known or suspected placenta praevia or accreta. Balloons can be placed via femoral artery punctures in the
10
uterine or internal iliac arteries before delivery. These can be inflated in the event of post partum haemorrhage (PPH). Subsequent embolisation can be performed via the balloon catheters if bleeding continues despite inflation. Even if hysterectomy is required blood loss, blood transfusion and numbers of admissions to intensive care units can be reduced 29 30 31 32. If this facility is not available locally it may be appropriate to transfer the patient at high risk of placenta accreta to a hospital where it is available. It is recommended to consider transfer for Jehovah’s witnesses for either cell saver or access to interventional radiology. In the emergency situation access to a suitably trained radiologist, radiographer and radiology nurse as well as access to high quality imaging are highly desirable. This is preferably in the obstetric unit or if not available in the special procedures unit in the radiology department. In this situation access to the anterior division of the internal iliac arteries via a femoral artery approach (and embolisation with a suitable embolic agent) under image guidance should be considered 29 30 31 32.
There are no randomised controlled trials but numerous observational studies illustrating the value of this technique and an analysis of 46 relevant studies 32 demonstrated success rates for control of major PPH of 90.7% for arterial embolisation, 84% for balloon tamponade, 91.7% for uterine compression sutures and 84.6% for uterine artery ligation. This study concluded that randomised controlled trials are unlikely to be feasible. In the emergency setting compression sutures and balloon tamponade are simple, effective and can be done in all settings. If these fail and IR is available locally its timely use can provide definitive care. If IR is not an option in the emergency setting uterine artery ligation is a reasonable surgical option to try before hysterectomy. NHS Trusts should have in place protocols that include the use of IR in the management of obstetric cases where PPH is likely. In addition NHS trusts should have clear strategies for the management of unpredictable PPH. In hospitals with an IR service treatment algorithms should be drawn up which clearly identify the timing and place of IR in the management of PPH. Where IR services are not available locally or there is no continuous IR on call hospital trusts should ensure that there is an agreed formal arrangement for the provision of these services either with a larger service nearby or through formation of a network with surrounding trusts. 6.4. Level 2 critical bed availability on site Although many women will undergo this surgery and do well some will not, and the unpredictable nature of which ones these are make it imperative that there is the facility to provide level 2 critical care (i.e. a unit or high dependency room that is equipped and has staff competent to provide the support of one organ system) on site if it is needed 33. The availability of a bed in this facility should be confirmed before an elective procedure for this high risk condition 3 34.
11

7. Consent The variety of surgical approaches possible need to be discussed with women by the consultant surgeon pre-operatively so that her preferences regarding blood transfusion, hysterectomy or leaving the placenta in place can be explored. In addition the different procedures, which may be necessary to replace blood and/or control haemorrhage, need to be explained and included in the informed consent. A sample specific consent form is included for reference (Appendix 2). 8. Anaesthetic The high risk nature of these obstetric cases means that a consultant obstetric anaesthetist should be directly involved in the care of these women during surgery. The decision for the type of anaesthetic to be used should be made by the consultant anaesthetist, but regional anaesthesia has been shown to be associated with less blood loss, a reduced need for blood transfusion and a higher post-op Hb than general anaesthesia, and will therefore usually be the safer alternative 35 36 37.
9. Surgical procedures Although good pre-operative planning will have given a guide as to the risk the definitive diagnosis of placenta accreta can only be made at surgery when the placenta either separates or fails to do so, therefore the surgical approach should take this uncertainty into account. The options for surgical approach are as follows: a) Routine access to the uterus This can risk entry through the placenta which if morbidly adherent will then fail to separate cleanly and will bleed. Treatment options in this scenario focus on controlling bleeding and replacing lost volume and as such are damage limiting:
• Blood needs to be replaced in the form of fluids and blood transfusion (cell salvage in this situation is useful in limiting donor blood use).
• Control of bleeding is meanwhile imperative and surgical techniques
such as systemic infusion and local infiltration with uterotonics to maximise uterine tone, under-running the bleeding sinuses in the placenta bed, compression sutures, or even local excision of bleeding myometrial sections can all be useful, as can local pressure applied by a balloon catheter 11 38. Interventional radiology can supplement these manoeuvres in achieving haemostasis if available in theatre, or if the patient is stable enough for transfer to the interventional radiology unit 29 30 31 32 and this can provide definitive treatment while conserving the uterus. In the absence of this facility hysterectomy remains the definitive treatment if performed in a timely fashion.
b) Accessing the uterine cavity deliberately avoiding the placenta
12

This requires a knowledge of the limits of the placental localisation to enable the appropriate skin and uterine incisions to be made, but has the advantage of allowing an assessment of placental adherence without heavy bleeding before a definitive decision is made. Either the placenta separates and the operation continues as normal, or it remains adherent, fails to separate and then the surgical options (previously discussed and agreed with the patient) include:
• Proceed straight to hysterectomy (family complete / woman prefers this to the risk of massive haemorrhage or leaving placenta in situ)
• Leave the placenta in situ and manage it conservatively in the postnatal
period (woman keen to conserve her uterus and understands the follow-up required from this technique and the morbidity and risks associated with it)
10. Postnatal care for those where the placenta has been left in situ This approach to limiting morbidity and preserving the uterus is now recognised through a number of series of case reports describing good outcomes although the practices do vary in the different centres and some women do bleed subsequently requiring hysterectomy as an emergency 39. 10.1 At surgery when the baby is delivered the routine 5 units of slow intravenous syntocinon should be given to make sure the placenta does not separate and is truly adherent. Once clear this is the case the cord should be unclamped and the placenta drained of blood before tying off and dividing it as close to its insertion into the placenta as surgically practicable. The uterus is then closed in the routine way.
10.2 Management in the immediate postpartum period relates to careful postoperative observations especially looking for signs of haemorrhage. When the placenta totally covers the cervical os concealed bleeding within the uterine cavity can occur and vigilance should be high to detect and respond quickly to this with regular assessments of the uterine fundus and vital signs. 10.3 Ongoing care and follow-up recognises the risk of infection and delayed haemorrhage and involves fairly intensive commitment and compliance in terms of hospital visits for clinical checks, blood tests and in some series imaging. Pregnancies have been reported after this approach, but so have cases of delayed haemorrhage and hysterectomy 11.
1. Infection: Antibiotics prophylactically have been used for a few days after delivery, but most important is the postnatal follow-up with prompt recognition and treatment of infection. This has been done with regular hospital visits (as frequent as twice weekly) with clinical review and blood tests for full blood count and C-reactive protein measurements.
13

2. Placental resorption: A baseline measurement of serum beta-HCG should be performed after delivery and then this can be monitored with regular blood tests (twice weekly initially) to check the levels are falling. Methotrexate has been used routinely in some case series, but others reserve it for women in whom the serum beta-HCG stops falling (or rises). Some embolise the placental bed electively and others perform an elective ERPC at 6 weeks.
14
References
1. Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, et al. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol 2006 Jun;107(6):1226–32. 2. Grobman WA, Gersnoviez R, Landon MB, Spong CY, Leveno KJ, Rouse DJ, et al; National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. Obstet Gynecol 2007 Dec;110(6):1249–55. 3. Lewis G, editors. Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer - 2003–2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH; 2007. [http://www.cemach.org.uk/getattachment/8f5c1ed8-fdf3-489b-a182-e53955bec07b/Saving-Mothers--Lives-2003-2005_full.aspx] 4. Knight M; UKOSS. Peripartum hysterectomy in the UK: management and outcomes of the associated haemorrhage. BJOG 2007 Nov;114(11):1380–7. Epub 2007 Sep 17. 5.[www.ihi.org/IHI/Topics?CriticalCare/IntensiveCare/ImprovementStories/WhatIsABundle.htm] 6.[www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/ImprovementStories/WhatIsABundle.htm] 7. [www.ihi.org?IHI/Topics/CriticalCare/IntensiveCare/ImprovementsStories/BundleUpfor Safety.htm] 8. Dashe JS, McIntire DD, Ramus RM, Santos-Ramos R, Twickler DM. Persistence of placenta praevia according to gestational age at ultrasound detection. Obstet Gynecol 2002 May;99(5 Pt 1):692–7. 9. Chama CM, Wanonyi IK, Usman JD. From low-lying implantation to placenta praevia: a longitudinal ultrasonic assessment. J Obstet Gynaecol 2004 Aug;24(5):516–8. 10. Bhandal N, Russell R. Intravenous versus oral therapy for postpartum anaemia. BJOG 2006 Nov;113(11):1248–52. Epub 2006 Sep 27. 11. Royal College of Obstetricians and Gynaecologists. Placenta praevia and placenta praevia accreta: diagnosis and management. Clinical Guideline No. 27. London: RCOG Press; 2005.
15

12. National Institute for Health and Clinical Excellence. Antenatal Care; routine care for the healthy pregnant woman. Clinical Guideline No. 62, developed by the National Collaborating Centre for Women’s and Children’s Health. London: NICE; 2008. 13. Warshak CR, Eskander R, Hull AD, Scioscia AL, Mattrey RF, Benirschke K, at al. Accuracy of ultrasonography and magnetic resonance imaging in the diagnosis of placenta accreta. Obstet Gynecol 2006 Sep;108(3 Pt 1):573–81. 14. Comstock C. The ultrasound diagnosis of placenta accrete Ultrasound 2007; 15(4): 208–14 15. European Society of Urogenital Radiology. Guidelines on Contrast Media Version 4.0. ESUR; 2007[http://www.esur.org/fileadmin/Files/esur_guidelines.pdf] 16. National Collaborating Centre for Women’s and Children’s Health Clinical. Caesarean Section. Clinical Guideline. London: RCOG Press; 2004 17. . Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective caesarean section. BJOG 1995 Feb;102(2):101–6. 18. Love CD, Wallace EM. Pregnancies complicated by placenta praevia: what is appropriate management? BJOG 1996;103(9):864–7. 19. Royal College of Obstetricians and Gynaecologists. Blood Transfusion in Obstetrics. Clinical Guideline No. 49. London: RCOG Press; 2007. 20. Taylor C, Asher D, Knowles S, Tinegate H, Cohen H, Brant L et al. Serious Hazards of Transfusion Annual Report 2006. SHOT; 2007. [http://www.shotuk.org/SHOT_report_2006.pdf] 21. Catling SJ, Freites O, Krishnan S, Gibbs R. Clinical experience with cell salvage in obstetrics: 4 cases from one UK centre. Int J Obstet Anesth 2002 Apr;11(2):128–34. 22. National Institute for Health and Clinical Excellence. Intraoperative blood cell salvage in obstetrics. Interventional Procedure Guidance No. 144. London: NICE; 2005 [http://www.nice.org.uk/nicemedia/pdf/ip/IPG144guidance.pdf] 23. Obstetric Anaesthetists’ Association, The Association of Anaesthetists of Great Britain and Ireland. Guidelines for Obstetric Anaesthetic Services revised edition 2005. London: OAA/AAGBI; 2005 [http://www.aagbi.org/publications/guidelines/docs/obstetric05.pdf]
16

24. Allam J, Cox M, Yentis SM. Cell salvage in obstetrics. Int J Obstet Anesth 2008 Jan;17(1):37–45. 25. Catling S. Blood conservation in obstetrics: a UK perspective. Int J Obstet Anesth 2007 Jul;16(3):241–9. Epub 2007 May 16. 26. Teig M, Clarke V, Catling S. OAA Survey of UK Maternity Units. Poster Presentation. OAA Annual Meeting, Sheffield, July 2007. 27. [http://transfusionguidelines.org.uk/?Publication=BBT&Section=22&pageid=1353] 28. S Catling, personal communication. 29. Pelage JP, Le Dref O, Mateo J, Soyer P, Jacob D, Kardache M, et al. Life-threatening primary postpartum hemorrhage: treatment with emergency selective arterial embolization. Radiology 1998 Aug;208(2):359–62. 30. Hansch E, Chitkara U, McAlpine J, El-Sayed Y, Dake MD, Razavi MK. Pelvic arterial embolization for control of obstetric hemorrhage: a five-year experience. Am J Obstet Gynecol 1999 Jun;180(6 Pt 1):1454–60. 31. Doumouchtsis SK, Papageorghiou AT, Arulkumaran S. Systematic review of conservative management of postpartum hemorrhage: what to do when medical treatment fails. Obstet Gynecol Surv 2007 Aug;62(8):540–7. 32. Boulleret C, Chahid T, Gallot D, Mofid R, Tran Hai D, Ravel A, et al. Hypogastric arterial selective and superselective embolization for severe postpartum hemorrhage: a retrospective review of 36 cases. Cardiovasc Intervent Radiol 2004 Jul-Aug;27(4):344–8. Epub 2004 May 6. 33. Royal College of Anaesthetists, Royal College of Midwives, Royal College of Obstetricians and Gynaecologists, Royal College of Paediatrics and Child Health. Safer Childbirth: Minimum Standards for the Organisation and Delivery of Care in Labour. Working party report. London: RCOG Press; 2007
34. Lewis G, Drife J, editors. Why Mothers Die 2000–2002. The Sixth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. London: RCOG Press; 2004 35. Frederiksen MC, Glassenberg R, Stika CS. Placenta previa: a 22-year analysis. Am J Obstet Gynecol 1999 Jun;180(6 Pt 1):1432–7.
17
18
36. Parekh N, Husaini SW, Russell IF. Caesarean section for placenta praevia: a retrospective study of anaesthetic management. Br J Anaesth 2000 Jun;84(6):725–30. 37. Collis R, Garry M. CSE is the regional anaesthetic technique of choice for placenta praevia. Int J Obstet Anesth 2001 Jul;10(3):252–3. 38. Teo SB, Kanagalingam D, Tan HK, Tan LK. Massive postpartum haemorrhage after uterus-conserving surgery in placenta percreta: the danger of the partial placenta percreta. BJOG 2008 May;115(6):789–92. 39. Brace V, Kernaghan D, Penney G. Learning from adverse clinical outcomes: major obstetric haemorrhage in Scotland, 2003-05. BJOG 2007 Nov;114(11):1388–96. Further reading
• Armstrong CA, Harding S, Dickinson JE Clinical aspects and conservative management of placenta accreta TOG 2004; 6:132-137
• Groom KM and Paterson-Brown S Placenta praevia and placenta praevia accreta - a review of aetiology, diagnosis and management Fetal and Maternal Medicine Review 2001; 12:1 41-66
• Observational study of Jehovah’s witnesses ? author or is this part of the same ref as below??
• Massiah N et al Obstetric care of Jehovah’s witnesses: a 14-year observational study Arch Gynaecology Obstet 2007 276:339-343
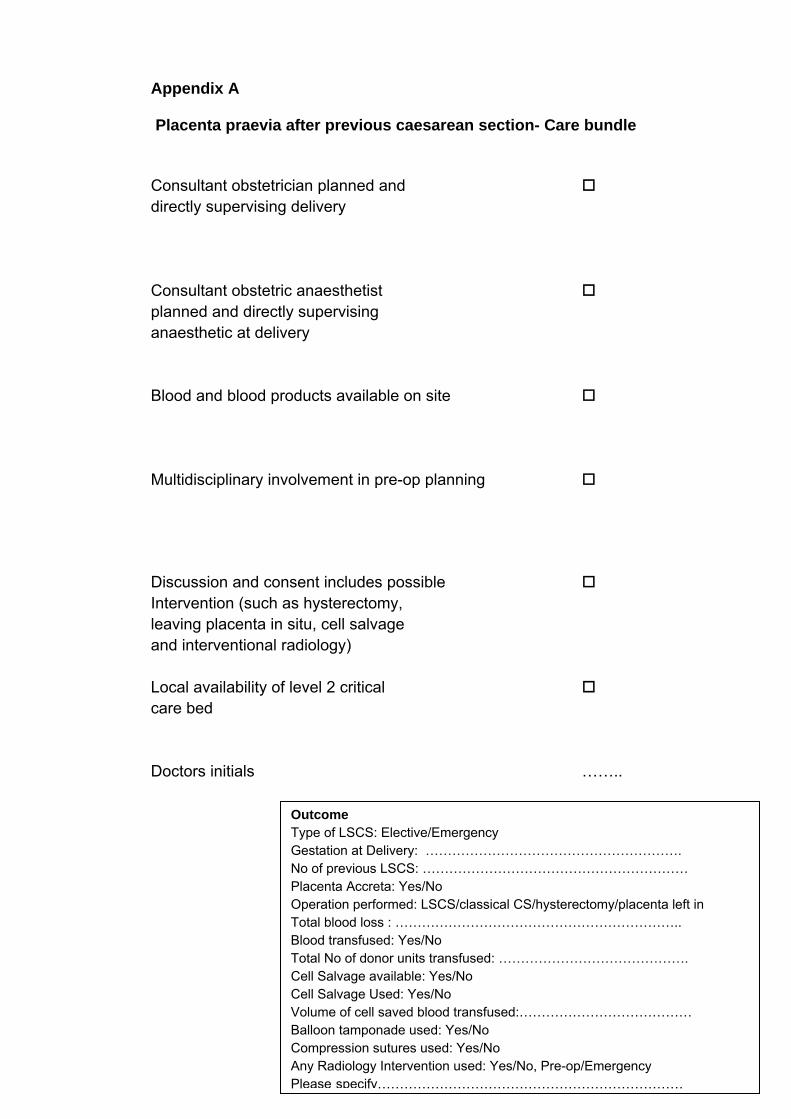
Appendix A Placenta praevia after previous caesarean section- Care bundle
Consultant obstetrician planned and directly supervising delivery Consultant obstetric anaesthetist planned and directly supervising anaesthetic at delivery Blood and blood products available on site Multidisciplinary involvement in pre-op planning Discussion and consent includes possible Intervention (such as hysterectomy, leaving placenta in situ, cell salvage and interventional radiology) Local availability of level 2 critical care bed Doctors initials ……..
Outcome Type of LSCS: Elective/Emergency Gestation at Delivery: …………………………………………………. No of previous LSCS: …………………………………………………… Placenta Accreta: Yes/No Operation performed: LSCS/classical CS/hysterectomy/placenta left in Total blood loss : ……………………………………………………….. Blood transfused: Yes/No Total No of donor units transfused: ……………………………………. Cell Salvage available: Yes/No Cell Salvage Used: Yes/No Volume of cell saved blood transfused:………………………………… Balloon tamponade used: Yes/No Compression sutures used: Yes/No Any Radiology Intervention used: Yes/No, Pre-op/Emergency Please specify……………………………………………………………
Appendix B
consent form 1 Patient agreement to investigation
or treatment
Elective Caesarean Section for placenta praevia in the
presence of a previous Caesarean Section
Patient details (or pre-printed label)
Patient’s surname/family name..………………………….
Patient’s first names .……………………………………….
Date of birth ………………………………………………….
Responsible health professional.…………………………… Job title ……………………………………………………….
NHS number (or other identifier)……………………………..
Male Female Special requirements ……………………………………… (eg other language/other communication method)
To be retained in patient’s notes
20
21
Patient identifier/label Name of proposed procedure or course of treatment (include brief explanation if medical term not clear)
Elective (Planned) Caesarean Section for placenta praevia in the presence of a previous Caesarean Section
Statement of health professional (to be filled in by health professional with appropriate knowledge of proposed procedure, as specified in consent policy) I have explained the procedure to the patient. In particular, I have explained: The intended benefits To avoid risks to yourself and your baby of heavy bleeding which would occur during labour because of the position of your placenta. These would be much greater than the risks of elective caesarean section Serious or frequently occurring risks If the placenta is found to abnormally stuck to the wall of the womb, it may be safer to leave the placenta inside the womb or to do a planned hysterectomy to avoid heavy bleeding. Excessive bleeding may require blood transfusion and other procedures including emergency hysterectomy to control it. Admission to a critical care unit may be necessary. Infection in your wound or bladder, damage to other structures, most commonly your bladder, or blood clots in your legs or chest can occur, the latter two are uncommon. Occasionally your baby may suffer a minor cut during surgery. Any extra procedures which may become necessary during the procedure
blood transfusion or cell salvage (where blood lost is collected, processed and put back into your circulation). The latter reduces the small risk of transmission of infection and transfusion reactions associated with use of donated blood. However there is a theoretical risk of sensitisation to the baby’s blood if that is different to your own and of a rare condition called amniotic fluid embolism. Neither of these have been confirmed in the published research.
other procedure (please specify) Interventional Radiology - blocking the blood vessels to your womb by passing fine tubes through the artery in your groin under x-ray vision. Foam plugs or coils are passed through these tubes to block the vessels to control bleeding. I have also discussed what the procedure is likely to involve, the benefits and risks of any available alternative treatments (including no treatment) and any particular concerns of this patient.
The following leaflet/tape has been provided This procedure will involve:
general and/or regional anaesthesia local anaesthesia sedation Signed:…….…………………………………… Date .. …………………….………. Name (PRINT) ………………………. ……… Job title …….. ………………….… Contact details (if patient wishes to discuss options later) …..……………….…………… Statement of interpreter (where appropriate) I have interpreted the information above to the patient to the best of my ability and in a way in which I believe she can understand. Signed ………………………….……………………. Date ………………..……………. To be retained in patient notes
22
Patient identifier/label Name of proposed procedure or course of treatment (include brief explanation if medical term not clear)
Elective (Planned) Caesarean Section for placenta praevia in the presence of a previous Caesarean Section
Statement of health professional (to be filled in by health professional with appropriate knowledge of proposed procedure, as specified in consent policy) I have explained the procedure to the patient. In particular, I have explained: The intended benefits To avoid risks to yourself and your baby of heavy bleeding which would occur during labour because of the position of your placenta. These would be much greater than the risks of elective caesarean section Serious or frequently occurring risks (Appendix 1) If the placenta is found to abnormally stuck to the wall of the womb, it may be safer to leave the placenta inside the womb or to do a planned hysterectomy to avoid heavy bleeding. Excessive bleeding may require blood transfusion and other procedures including emergency hysterectomy to control it. Admission to a critical care unit may be necessary. Infection in your wound or bladder, damage to other structures, most commonly your bladder, or blood clots in your legs or chest can occur, the latter two are uncommon. Occasionally your baby may suffer a minor cut during surgery. Any extra procedures which may become necessary during the procedure (Appendix 1)
blood transfusion or cell salvage (where blood lost is collected, processed and put back into your circulation). The latter reduces the small risk of transmission of infection and transfusion reactions associated with use of donated blood. However there is a theoretical risk of sensitisation to the baby’s blood if that is different to your own and of a rare condition called amniotic fluid embolism. Neither of these have been confirmed in the published research.
other procedure (please specify) Interventional Radiology - blocking the blood vessels to your womb by passing fine tubes through the artery in your groin under x-ray vision. Foam plugs or coils are passed through these tubes to block the vessels to control bleeding. I have also discussed what the procedure is likely to involve, the benefits and risks of any available alternative treatments (including no treatment) and any particular concerns of this patient.
The following leaflet/tape has been provided This procedure will involve:
general and/or regional anaesthesia local anaesthesia sedation Signed:…….…………………………………… Date .. …………………….………. Name (PRINT) ………………………. ……… Job title …….. ………………….… Contact details (if patient wishes to discuss options later) …..……………….…………… Statement of interpreter (where appropriate) I have interpreted the information above to the patient to the best of my ability and in a way in which I believe she can understand. Signed ………………………….……………………. Date ………………..……………. Copy to be given to patient
23
Statement of patient Patient identifier/label Please read this form carefully. If your treatment has been planned in advance, you should already have your own copy of page 2 which describes the benefits and risks of the proposed treatment. If not, you will be offered a copy now. If you have any further questions, do ask – we are here to help you. You have the right to change your mind at any time, including after you have signed this form. I agree to the procedure or course of treatment described on this form. Elective Caesarean Section for placenta praevia in the presence of previous
Caesarean section I understand that you cannot give me a guarantee that a particular person will perform the procedure. The person will, however, have appropriate experience. I understand that I will have the opportunity to discuss the details of anaesthesia with an anaesthetist before the procedure, unless the urgency of my situation prevents this. (This only applies to patients having general or regional anaesthesia.) I understand that any procedure in addition to those described on this form will only be carried out if it is necessary to save my life or to prevent serious harm to my health. I have been told about additional procedures which may become necessary during my treatment. I have listed below any procedures which I do not wish to be carried out without further discussion. ………………………………………………………………………… ………………………………………………………………………………………………………………… I understand that photographs or video recordings maybe made as a part of my assessment or treatment. If this is going to happen I will be told beforehand or in exceptional circumstances afterwards. These maybe used without my consent within the clinical setting for education or research in a way that I cannot be recognised. Separate information will be provided and my written consent obtained when such material would not form part of my care and when it might be published or used for education or research or where I might be recognised. (Health professionals read notes overleaf) I understand my explicit consent is not necessary for anonymous public health monitoring of removed tissue for the benefit of the nations health. I may opt out of this. I agree to this use of my tissue. Yes No I agree to the use of any tissue which is being removed during this operation being used for research purposes and or teaching if needed. The only tissue removed is placenta unless you have consented separately to participate in research. Patient’s signature ………………………………………….. Date………………………….. Name (PRINT) ……………………………………………………………………………………… A witness should sign below if the patient is unable to sign but has indicated his or her consent. Young people/children may also like a parent to sign here (see notes). Signature …………………………………………… Date ……………………..….……… Name (PRINT) ………………………………………………………………………………….… Confirmation of consent (to be completed by a health professional when the patient is admitted for the procedure, if the patient has signed the form in advance) On behalf of the team treating the patient, I have confirmed with the patient that s/he has no further questions and wishes the procedure to go ahead. Signed:…….…………………………………… Date .. …………………….………. Name (PRINT) ………………………. ……… Job title …….. ………………….… Important notes: (tick if applicable)
See also advance directive/living will (eg Jehovah’s Witness form) Patient has withdrawn consent (ask patient to sign /date here) ……………...……….
24
Guidance to health professionals (to be read in conjunction with consent policy) What a consent form is for This form documents the patient’s agreement to go ahead with the investigation or treatment you have proposed. It is not a legal waiver – if patients, for example, do not receive enough information on which to base their decision, then the consent may not be valid, even though the form has been signed. Patients are also entitled to change their mind after signing the form, if they retain capacity to do so. The form should act as an aide-memoire to health professionals and patients, by providing a check-list of the kind of information patients should be offered, and by enabling the patient to have a written record of the main points discussed. In no way, however, should the written information provided for the patient be regarded as a substitute for face-to-face discussions with the patient. The law on consent See the Department of Health’s Reference guide to consent for examination or treatment for a comprehensive summary of the law on consent (also available at www.doh.gov.uk/consent). Who can give consent Everyone aged 16 or more is presumed to be competent to give consent for themselves, unless the opposite is demonstrated. If a child under the age of 16 has “sufficient understanding and intelligence to enable him or her to understand fully what is proposed”, then he or she will be competent to give consent for himself or herself. Young people aged 16 and 17, and legally ‘competent’ younger children, may therefore sign this form for themselves, but may like a parent to countersign as well. If the child is not able to give consent for himself or herself, some-one with parental responsibility may do so on their behalf and a separate form is available for this purpose. Even where a child is able to give consent for himself or herself, you should always involve those with parental responsibility in the child’s care, unless the child specifically asks you not to do so. If a patient is mentally competent to give consent but is physically unable to sign a form, you should complete this form as usual, and ask an independent witness to confirm that the patient has given consent orally or non-verbally. When NOT to use this form If the patient is 18 or over and is not legally competent to give consent, you should use form 4 (form for adults who are unable to consent to investigation or treatment) instead of this form. A patient will not be legally competent to give consent if: • they are unable to comprehend and retain information material to the decision and/or • they are unable to weigh and use this information in coming to a decision. You should always take all reasonable steps (for example involving more specialist colleagues) to support a patient in making their own decision, before concluding that they are unable to do so. Relatives cannot be asked to sign this form on behalf of an adult who is not legally competent to consent for himself or herself. Information Information about what the treatment will involve, its benefits and risks (including side-effects and complications) and the alternatives to the particular procedure proposed, is crucial for patients when making up their minds. The courts have stated that patients should be told about ‘significant risks which would affect the judgement of a reasonable patient’. ‘Significant’ has not been legally defined, but the GMC requires doctors to tell patients about ‘serious or frequently occurring’ risks. In addition if patients make clear they have particular concerns about certain kinds of risk, you should make sure they are informed about these risks, even if they are very small or rare. You should always answer questions honestly. Sometimes, patients may make it clear that they do not want to have any information about the options, but want you to decide on their behalf. In such circumstances, you should do your best to ensure that the patient receives at least very basic information about what is proposed. Where information is refused, you should document this on page 2 of the form or in the patient’s notes.
25
(Appendix 1) Serious risks include: Maternal Hysterectomy Need for further surgery at a later date, including curettage 0.5 Admission to intensive care unit (highly dependent on reason for 0.9 caesarean section) Bladder injury 0.1 Ureteric injury 0.03 Death (rare/dependent on indication) (n) c. 1/12000 Fetal Fetal injury Lacerations c. 2.0 Future pregnancies Increased risk of uterine rupture during subsequent up to 0.4 pregnancies/deliveries Antepartum stillbirth 0.4 Increased risk in subsequent pregnancies of placenta praevia 0.4–0.8 and placenta accreta Frequent risks include: ● persistent wound and abdominal discomfort in the first few months after surgery ● increased risk of repeat caesarean section for subsequent pregnancies. It is likely that all serious and frequent risks and complications will be more prevalent when a caesarean section is performed in the emergency situation, despite antibiotic cover and thromboprophylaxis, which are now used routinely to minimise the not infrequent and sometimes serious risks of infection and thromboembolism. Any extra procedures that may become necessary during the procedure ● Blood transfusion ● Other procedures: � repair of bladder and bowel damage � surgery on major blood vessels � ovarian cystectomy/oophorectomy in response to unsuspected pathology � hysterectomy If sterilisation is proposed, separate consent must be obtained following specific counselling in the antenatal period. Hysterectomy 0.7–0.8 Need for further surgery at a later date, including curettage 0.5 Admission to intensive care unit (highly dependent on reason for 0.9 caesarean section) Bladder injury 0.1 Ureteric injury 0.03 Death (rare/dependent on indication) (n) c. 1/12000 Fetal injury Lacerations c. 2.0 Future pregnancies Increased risk of uterine rupture during subsequent up to 0.4 pregnancies/deliveries Antepartum stillbirth 0.4 7.1d