care, maintenance and failure of fpds - mohammed...
TRANSCRIPT
Mohammed AlfarsiBDS, MDSc(Pros), PhD
www.DrMohdAlfarsi.comwww.محمدالفارسي.com
Care, Maintenance and Failure of FPDs
Friday, 3 January 14
Care, Maintenance and Failure of FPDsOverview
Friday, 3 January 14
Care, Maintenance and Failure of FPDsOverview
Care
- Prostheses design- Oral hygiene instruction
Maintenance Failure
- Review visits schedule
- Biological- Mechanical
Friday, 3 January 14
Introduction Care, Maintenance and Failure of FPDs
Friday, 3 January 14
Introduction
Proper design
Care, Maintenance and Failure of FPDs
Dentist
mainten
ance
AvoidFailure
Cementing the FPD is not the end of the treatment. Carefully planned recall visits should follow the cementation.
- To monitor the patient’s dental health.- Stimulate proper plaque control habits.- Identify any disease.- Treat any discovered disease.
Patient care
Friday, 3 January 14
Care Plaque Control
Friday, 3 January 14
Care Plaque Control
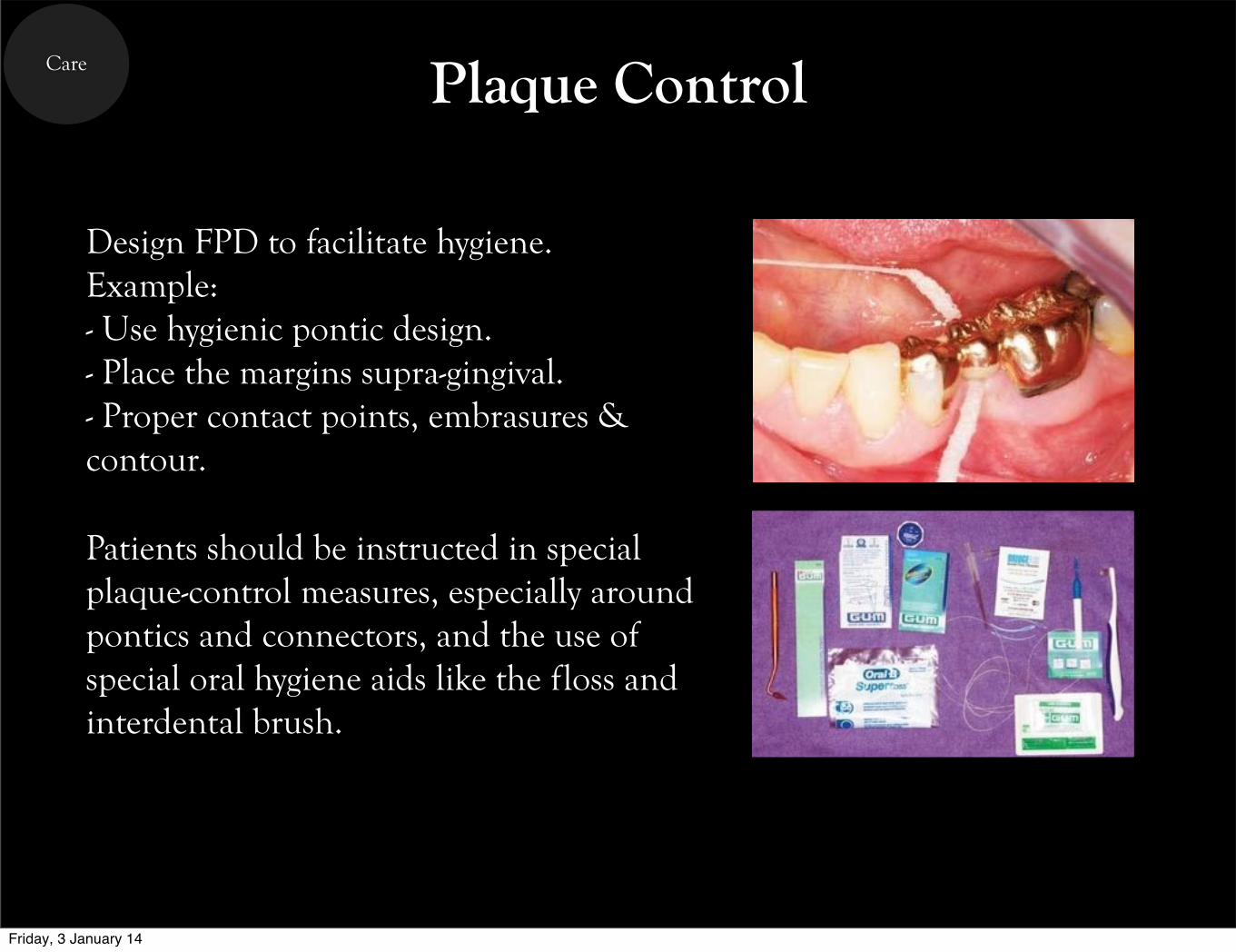
Design FPD to facilitate hygiene.Example:- Use hygienic pontic design.- Place the margins supra-gingival.- Proper contact points, embrasures & contour.
Patients should be instructed in special plaque-control measures, especially around pontics and connectors, and the use of special oral hygiene aids like the floss and interdental brush.
Friday, 3 January 14
Maintenance Post-operative Maintenance Schedule
Friday, 3 January 14
Maintenance Post-operative Maintenance Schedule
- The follow-up visits should be done by the dentists NOT auxiliary staff. Because detecting diseases at the early stage can be difficult yet relatively easy to treat.- The frequency of the follow-up visits depends on the patient oral hygiene attitude and/or the complexity of the FPD. Example: bad oral hygiene ➜ every 3 months, good oral hygiene ➜ every 6 months, and excellent oral hygiene ➜ every 12 months.
Friday, 3 January 14
Maintenance Post-operative Maintenance Schedule
Friday, 3 January 14
Maintenance Post-operative Maintenance Schedule
- First visit should be in 7-10 days.- Look for excess cement.- Re-check the occlusion.- Solve any problems.
Friday, 3 January 14
Maintenance Post-operative Maintenance Schedule
- First visit should be in 7-10 days.- Look for excess cement.- Re-check the occlusion.- Solve any problems.
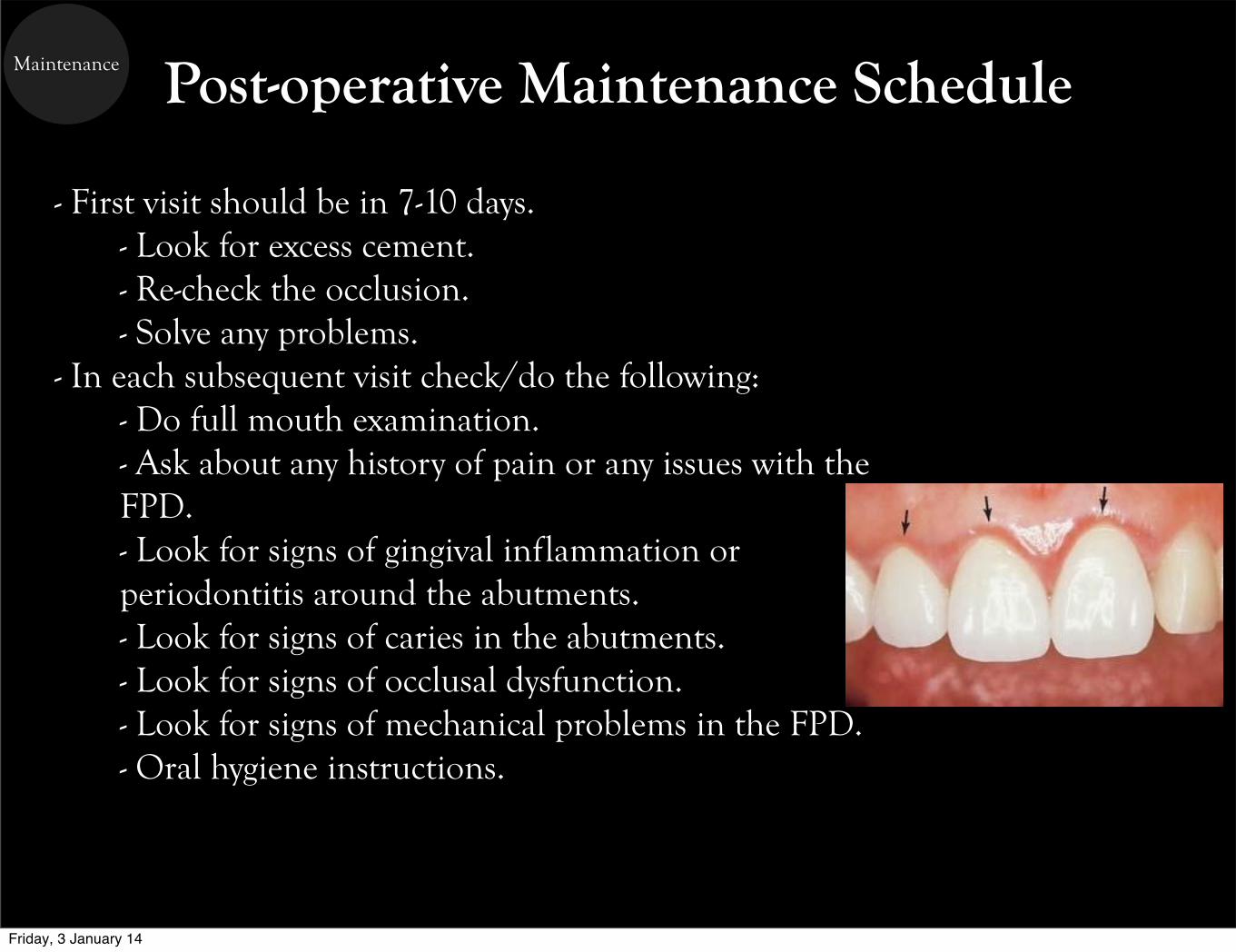
- In each subsequent visit check/do the following:- Do full mouth examination.- Ask about any history of pain or any issues with the FPD.- Look for signs of gingival inflammation or periodontitis around the abutments.- Look for signs of caries in the abutments.- Look for signs of occlusal dysfunction.- Look for signs of mechanical problems in the FPD.- Oral hygiene instructions.
Friday, 3 January 14
Failure Failure of FPD
Friday, 3 January 14
Failure Failure of FPD
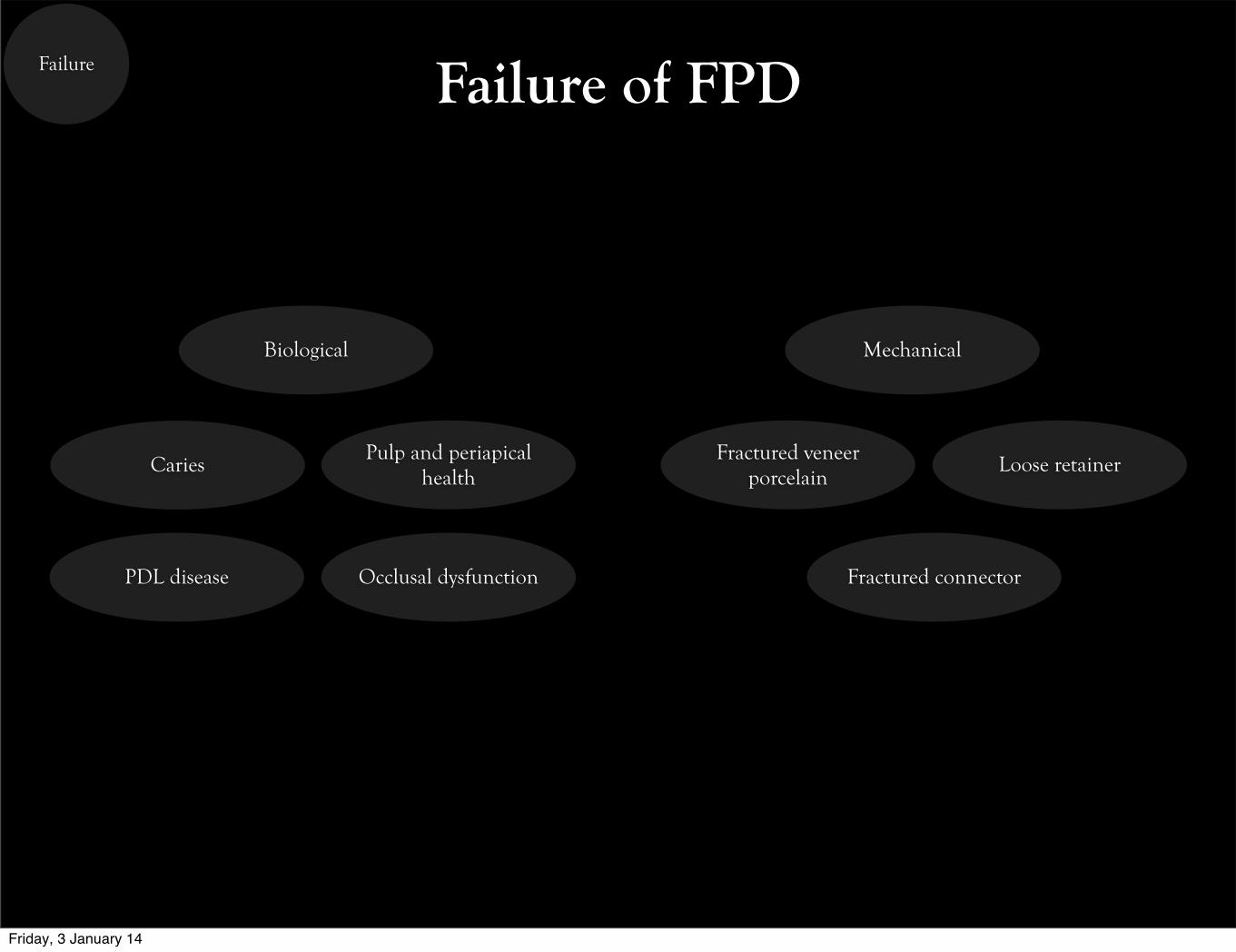
Caries
Biological Mechanical
Occlusal dysfunctionPDL disease
Pulp and periapical health
Fractured connector
Loose retainerFractured veneer porcelain
Friday, 3 January 14
Failure Biological Failure
Friday, 3 January 14
Failure Biological Failure
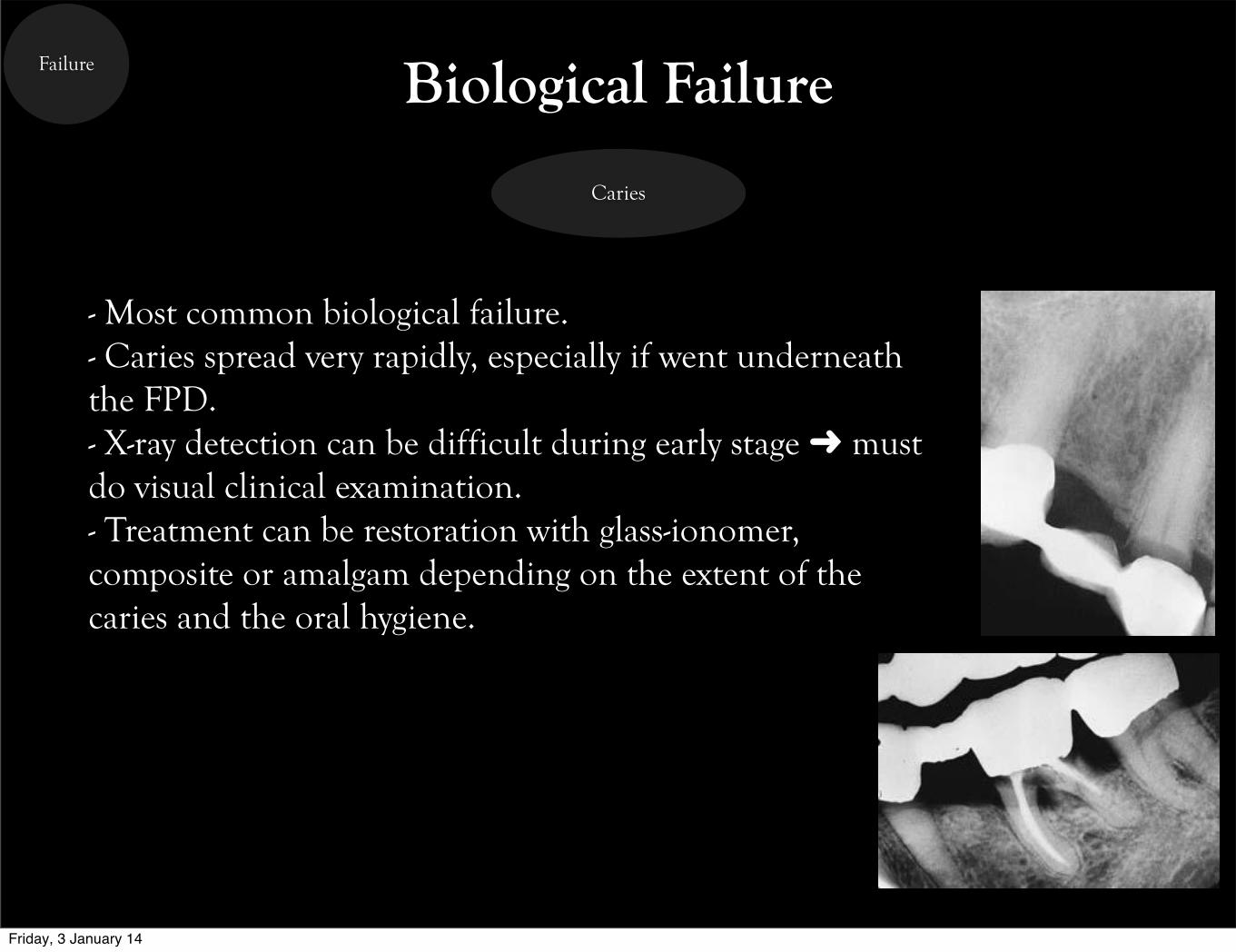
Caries
- Most common biological failure.- Caries spread very rapidly, especially if went underneath the FPD.- X-ray detection can be difficult during early stage ➜ must do visual clinical examination.- Treatment can be restoration with glass-ionomer, composite or amalgam depending on the extent of the caries and the oral hygiene.
Friday, 3 January 14
Failure Biological Failure
Friday, 3 January 14
Failure
Pulp and periapical health
Biological Failure
- Most of oral pain is of pulpal origin.- Causes of loss of pulp vitality after cementation are:
- Preparing the tooth without proper cooling.- Stressed pulp syndrome.- Cracked tooth syndrome, like fractured root with post/core.- Sharp internal line angles that lead to stress accumulation.- Open margins that lead to leakage and decay formation.
- Checking pulp vitality can be challenging for abutments with full coverage retainers.- Periodic x-ray (with a standardized technique) should be taken to monitor the periapical health.- RCT can be done through he crown or by removing the FPD and re-cementing after RCT.
Friday, 3 January 14
Failure Biological Failure
Friday, 3 January 14
Failure
PDL disease
Biological Failure
- Periodontal disease (like gingivitis, periodontitis or pocketing) can occur if:
- Margins are placed subgingivally.- FPD is over/under-contoured.- Bad oral hygiene.
- Signs and symptoms:- Marginal gingivitis- Sulcular hemorrhage.- Plaque/calculus formation around the margins.- Furcation involvement.- Pockets formation around the abutments.
Friday, 3 January 14
Failure Biological Failure
Friday, 3 January 14
Failure
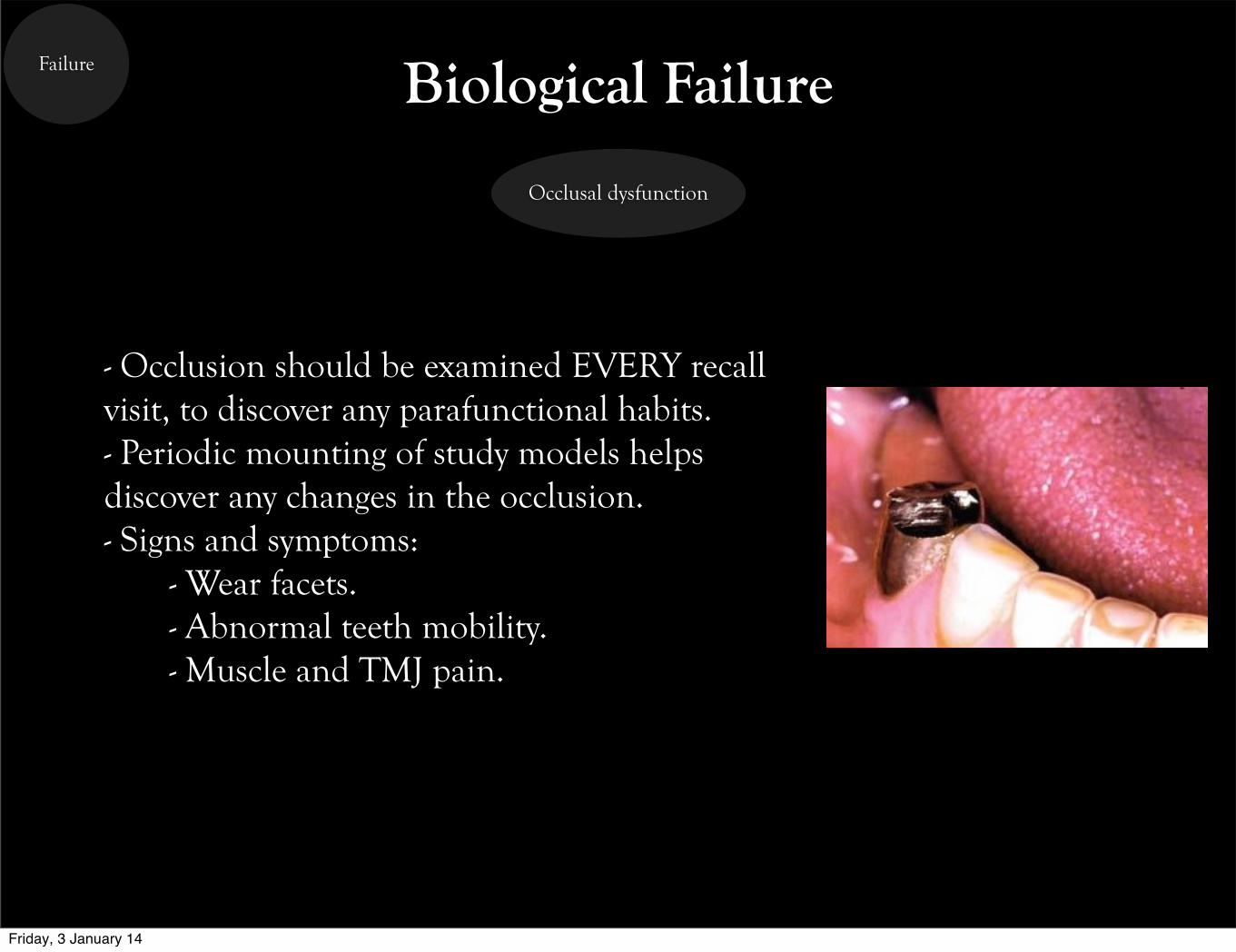
Occlusal dysfunction
Biological Failure
- Occlusion should be examined EVERY recall visit, to discover any parafunctional habits.- Periodic mounting of study models helps discover any changes in the occlusion.- Signs and symptoms:
- Wear facets.- Abnormal teeth mobility.- Muscle and TMJ pain.
Friday, 3 January 14
Failure Mechanical Failure
Friday, 3 January 14
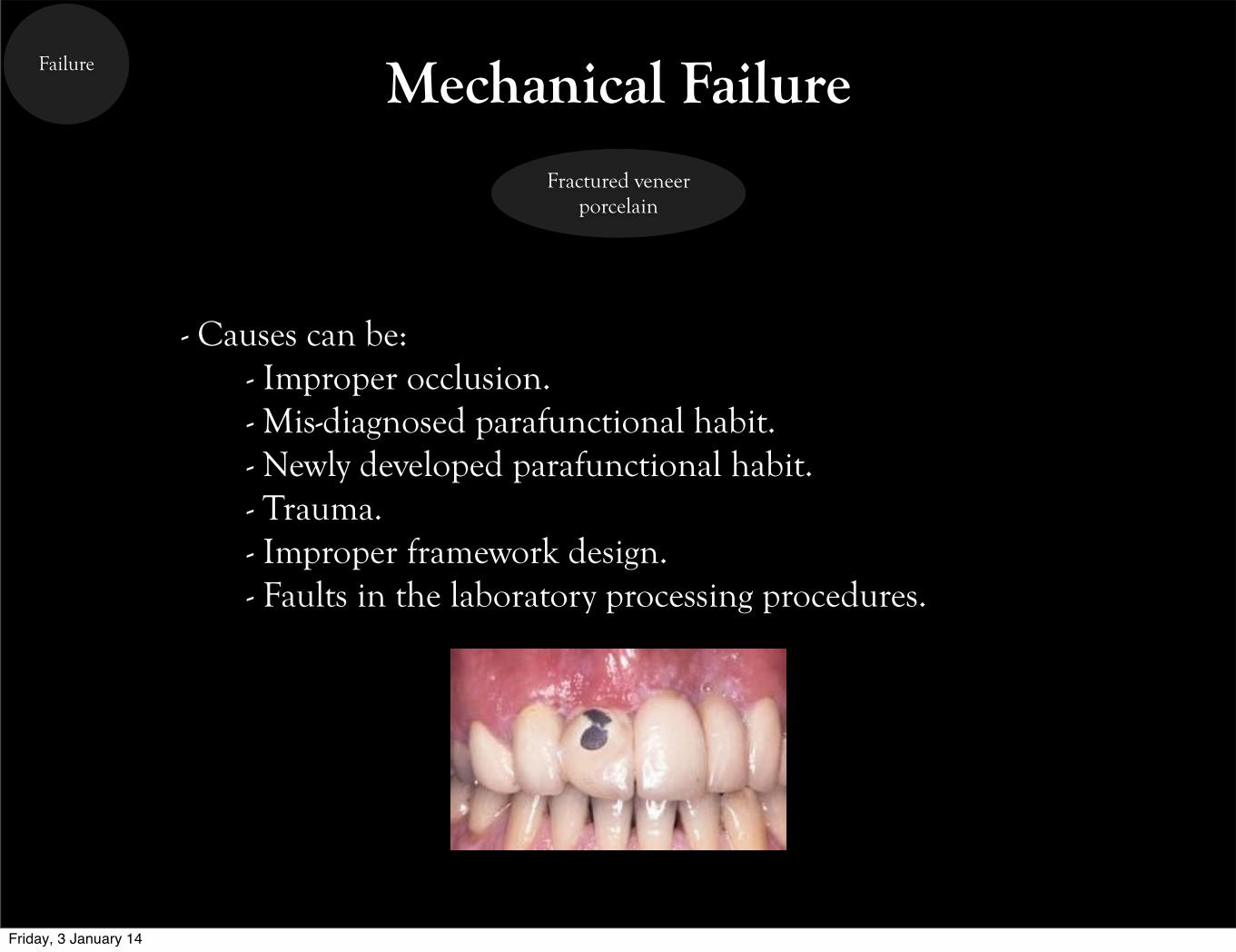
Failure Mechanical FailureFractured veneer
porcelain
- Causes can be:- Improper occlusion.- Mis-diagnosed parafunctional habit.- Newly developed parafunctional habit.- Trauma.- Improper framework design.- Faults in the laboratory processing procedures.
Friday, 3 January 14
Failure Mechanical Failure
Friday, 3 January 14
Failure Mechanical Failure
Loose retainer
- A loose FPD retainer can be difficult to feel by the patient.- Bad smell and/or taste are signs of loose retainers.- Treatment is done by removing the FPD and recemenitng.- If stayed for long time without treatment, decay can form and may lead to the loss of the prothesis.
Friday, 3 January 14
Failure Mechanical Failure
Friday, 3 January 14
Failure Mechanical Failure
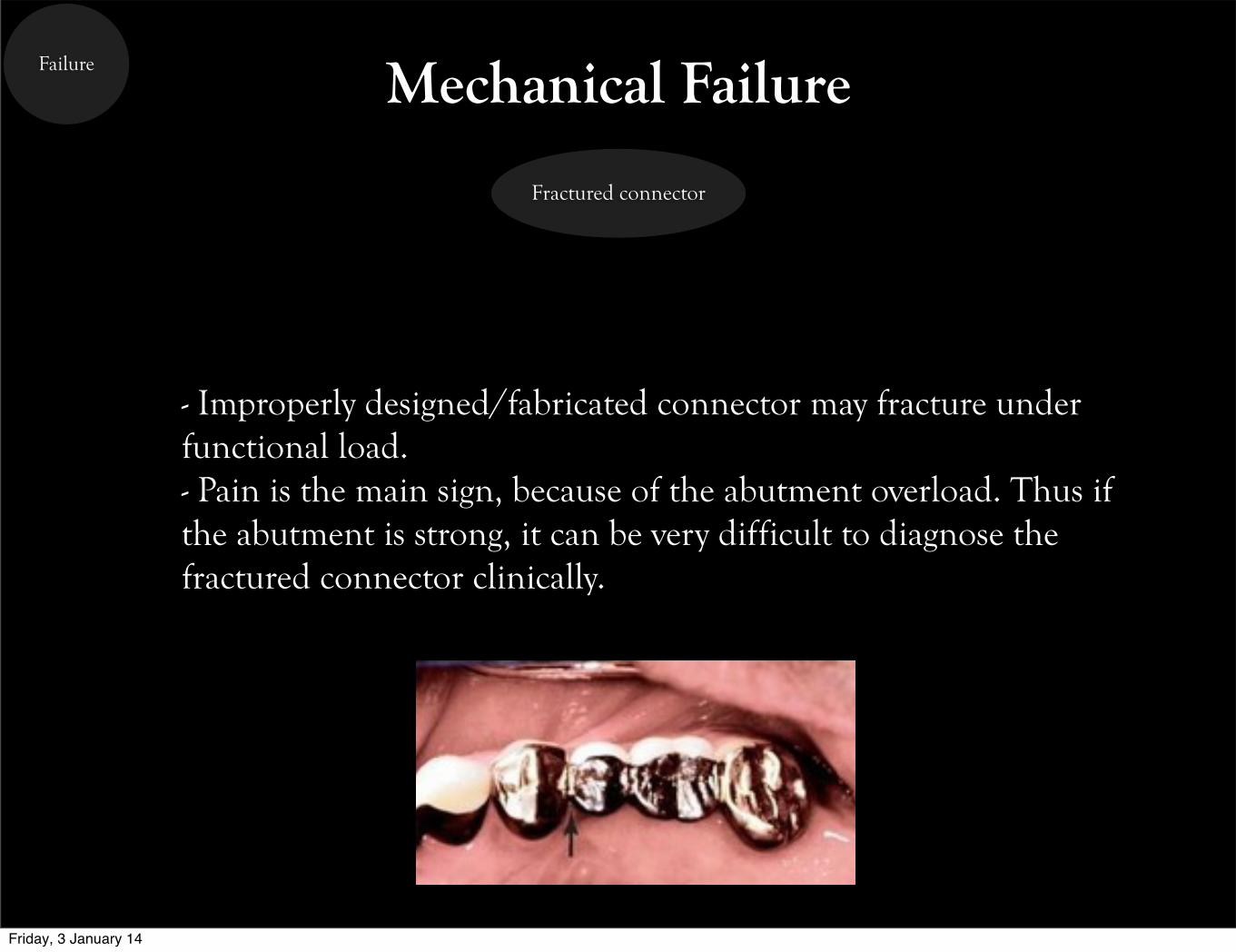
Fractured connector
- Improperly designed/fabricated connector may fracture under functional load.- Pain is the main sign, because of the abutment overload. Thus if the abutment is strong, it can be very difficult to diagnose the fractured connector clinically.
Friday, 3 January 14
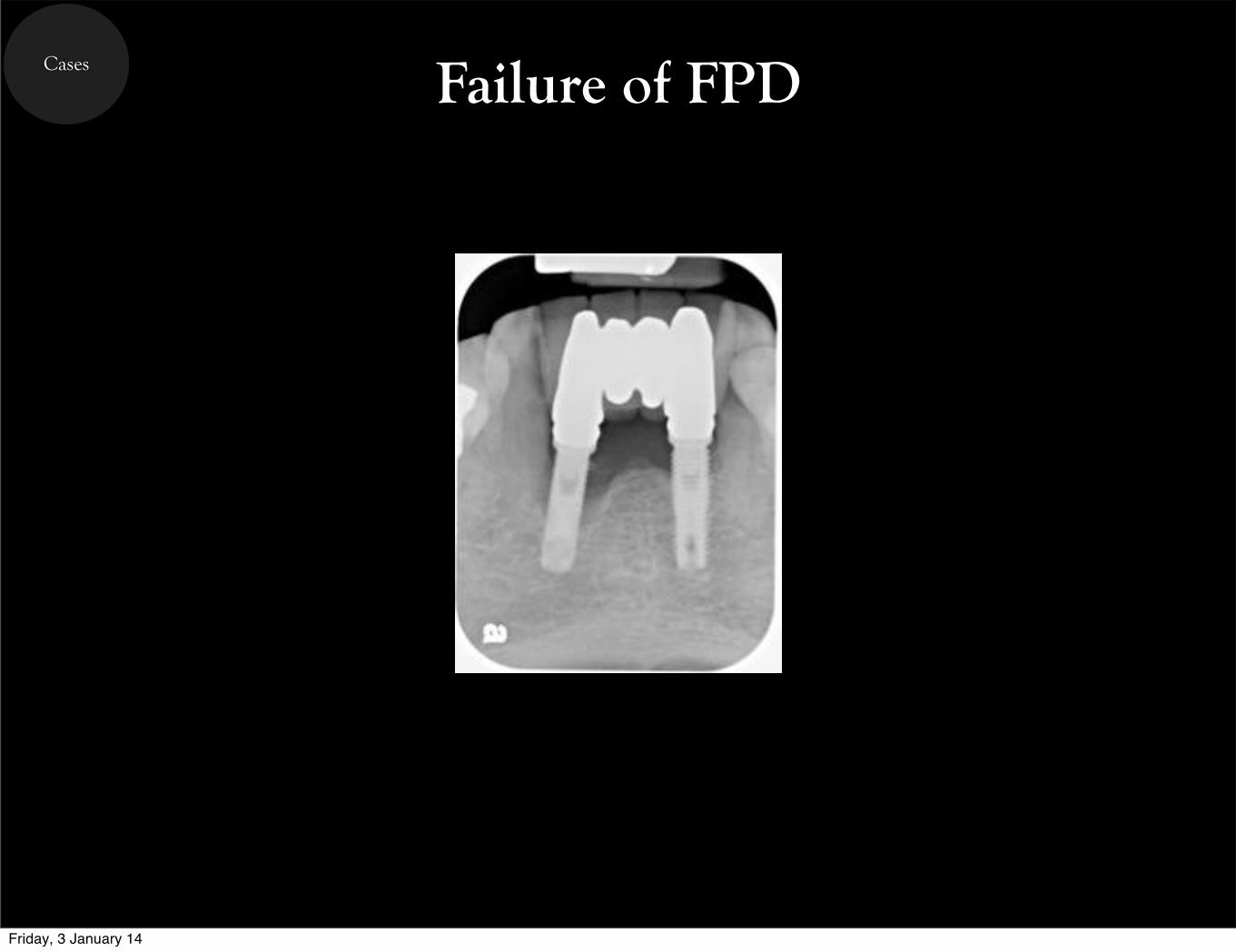
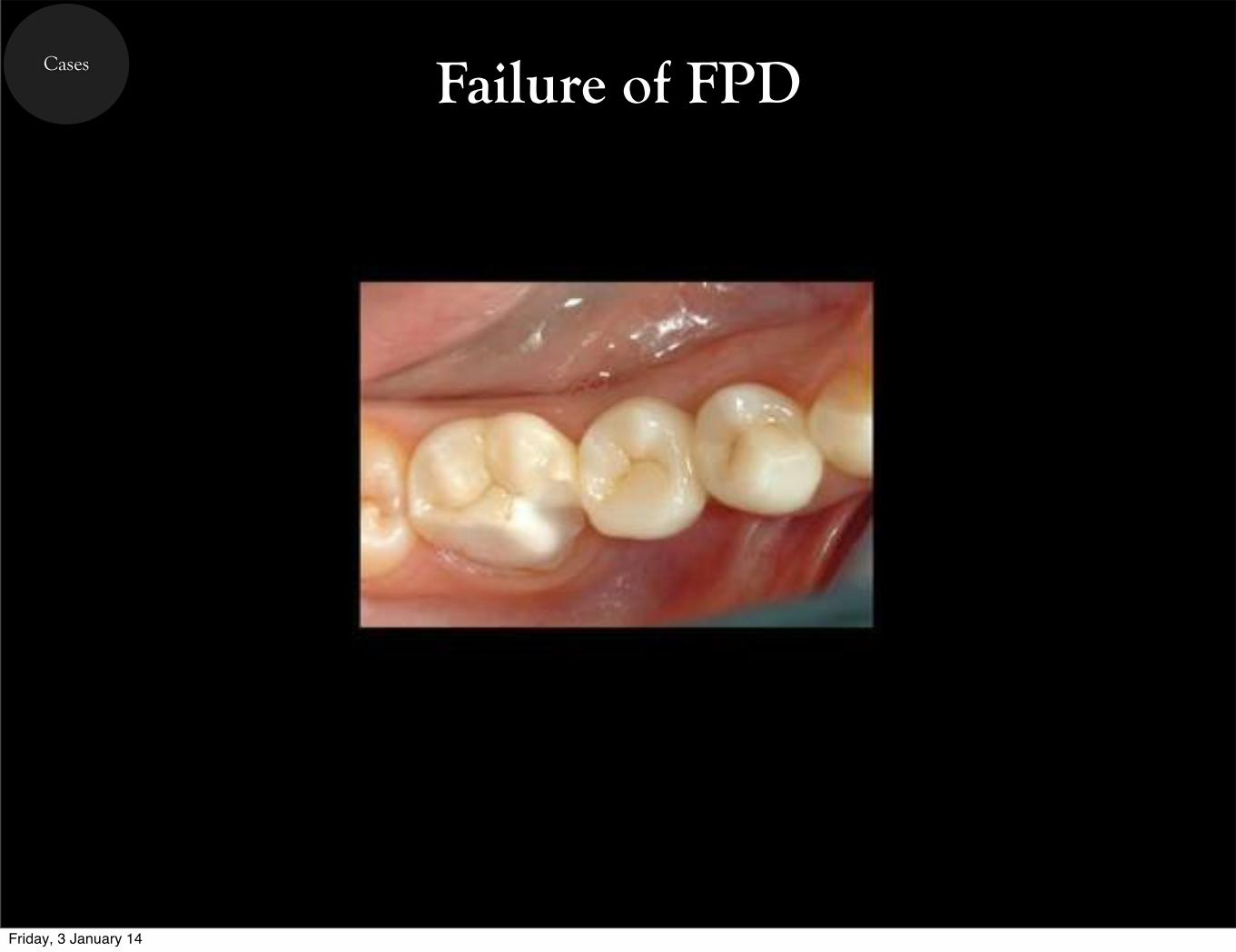
Cases Failure of FPD
Friday, 3 January 14
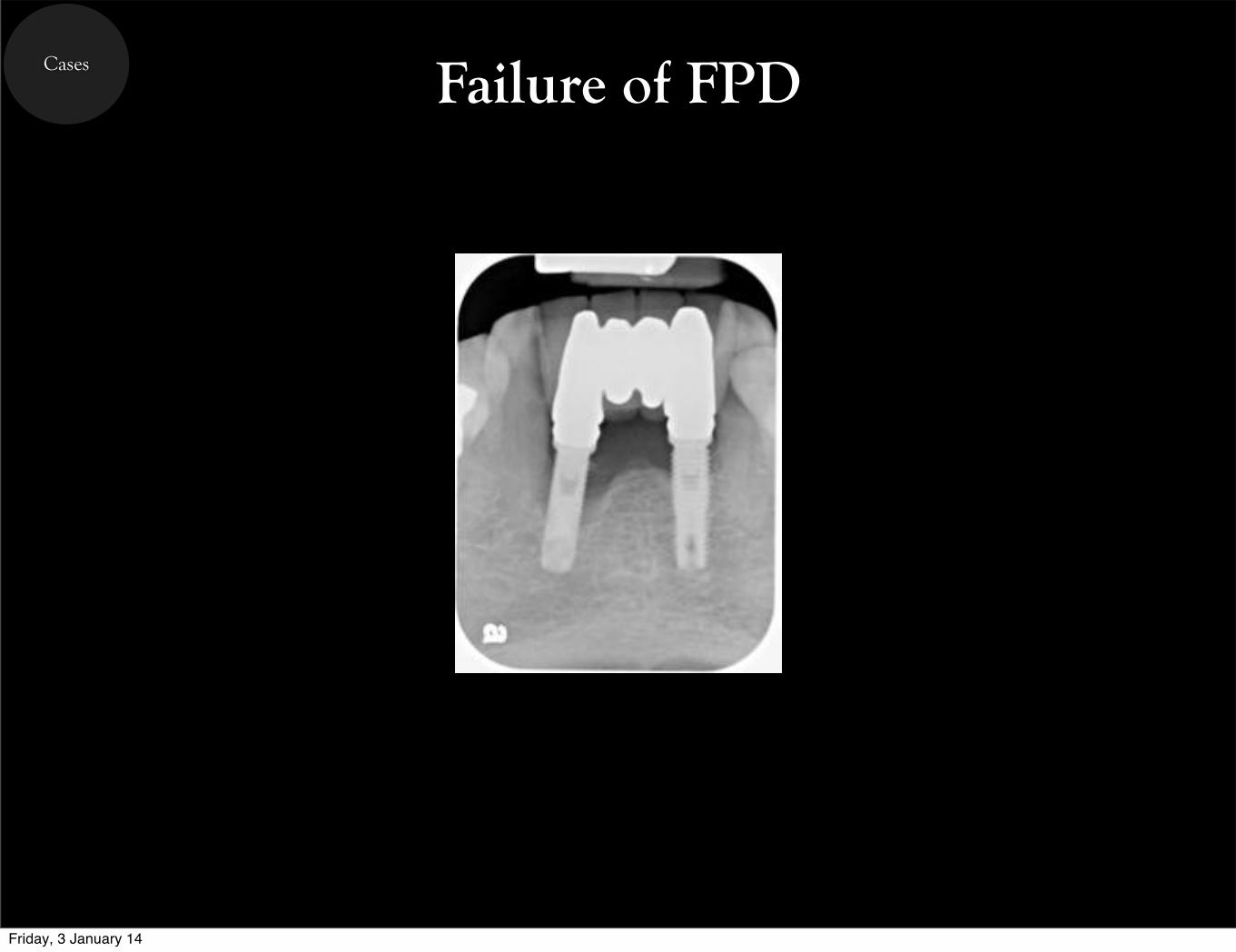
Cases Failure of FPD
Friday, 3 January 14
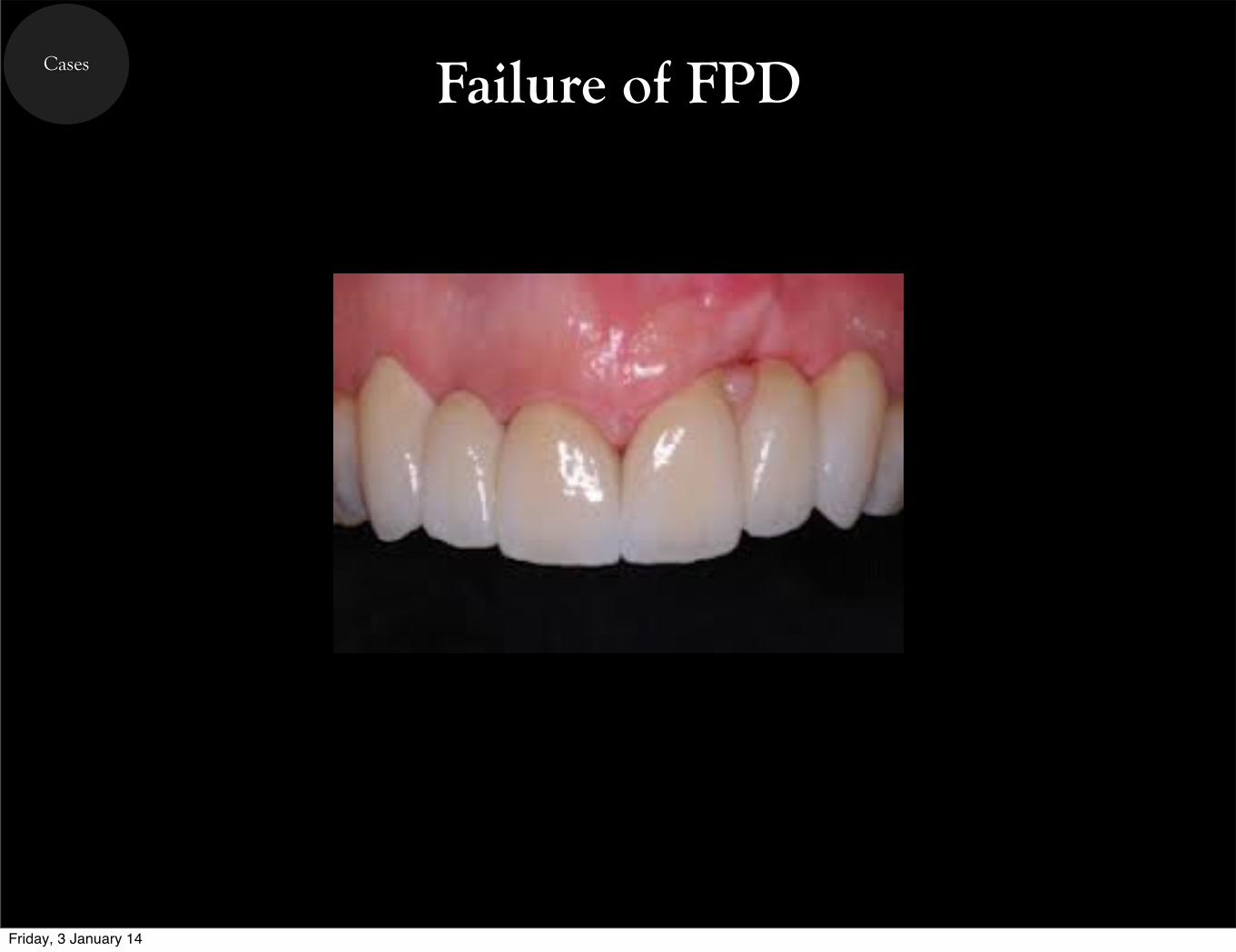
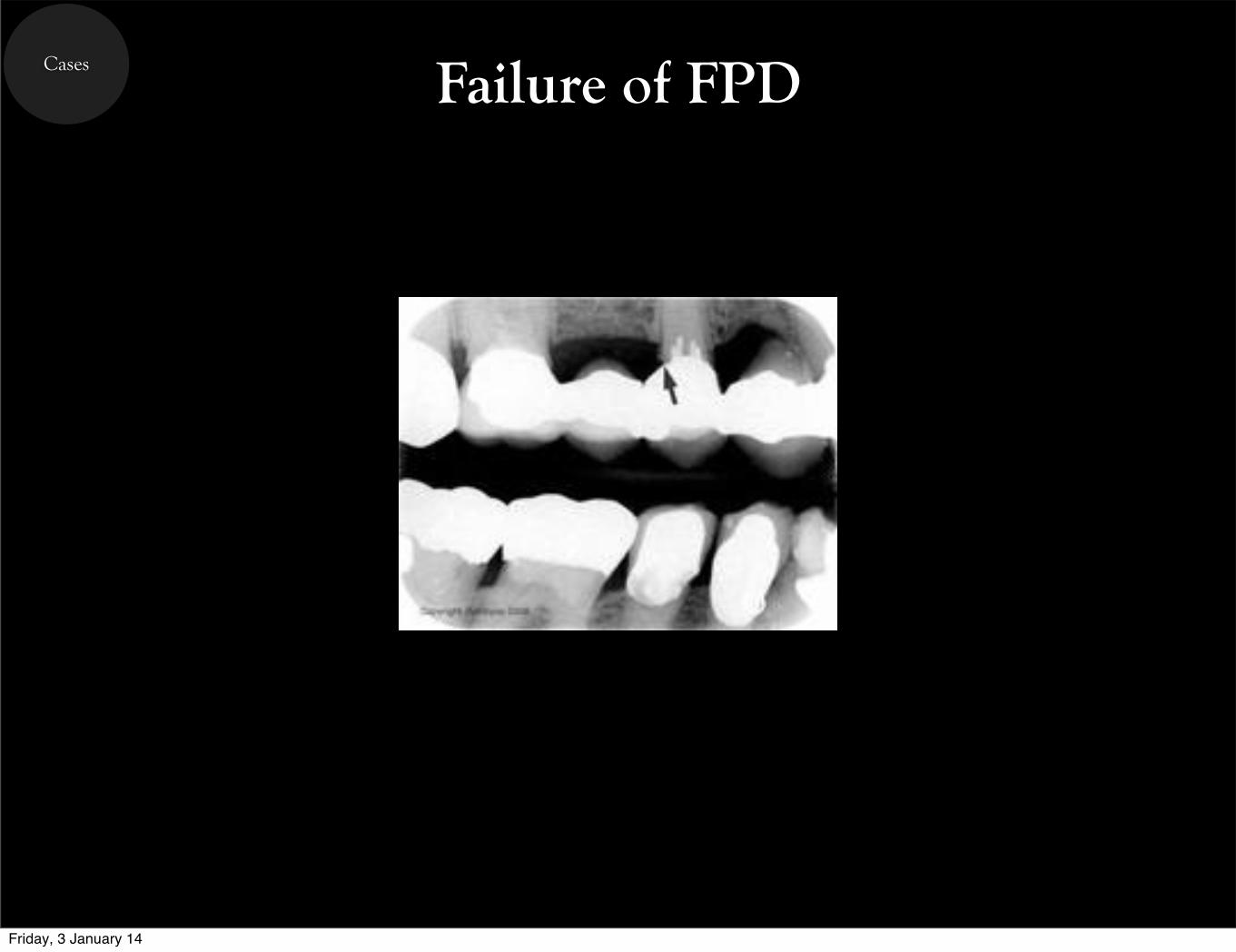
Cases Failure of FPD
Friday, 3 January 14
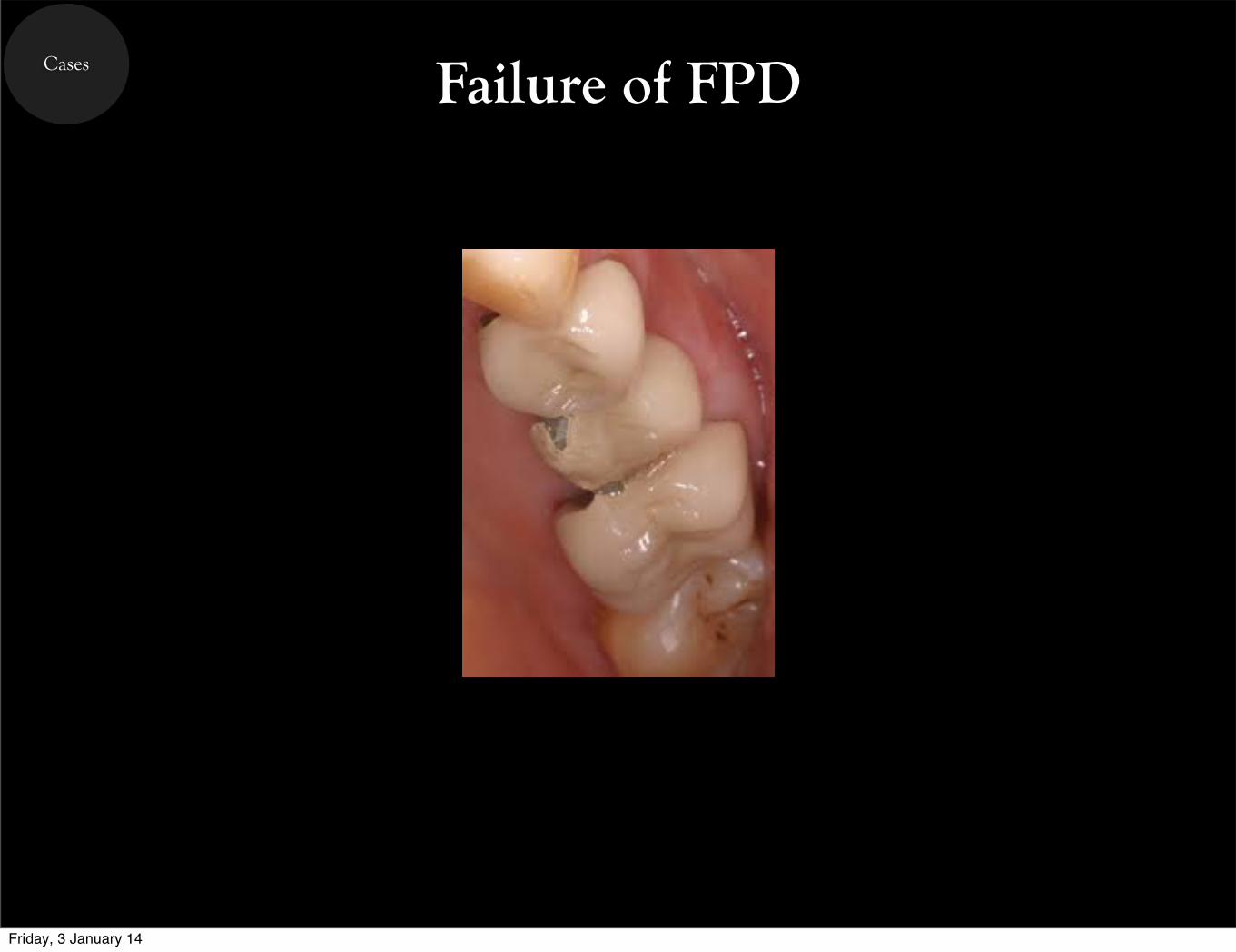
Cases Failure of FPD
Friday, 3 January 14
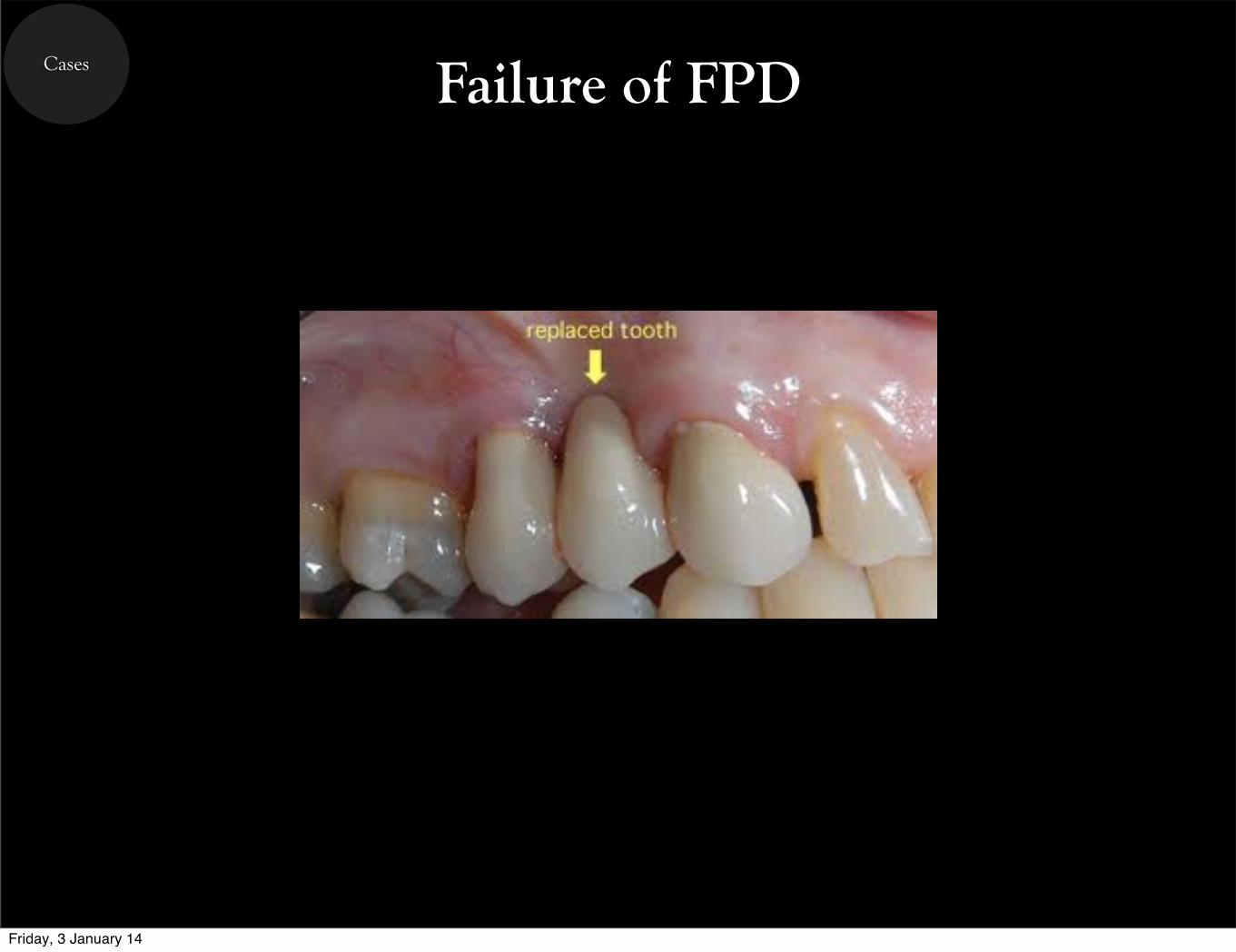
Cases Failure of FPD
Friday, 3 January 14
Cases Failure of FPD
Friday, 3 January 14
Cases Failure of FPD
Friday, 3 January 14
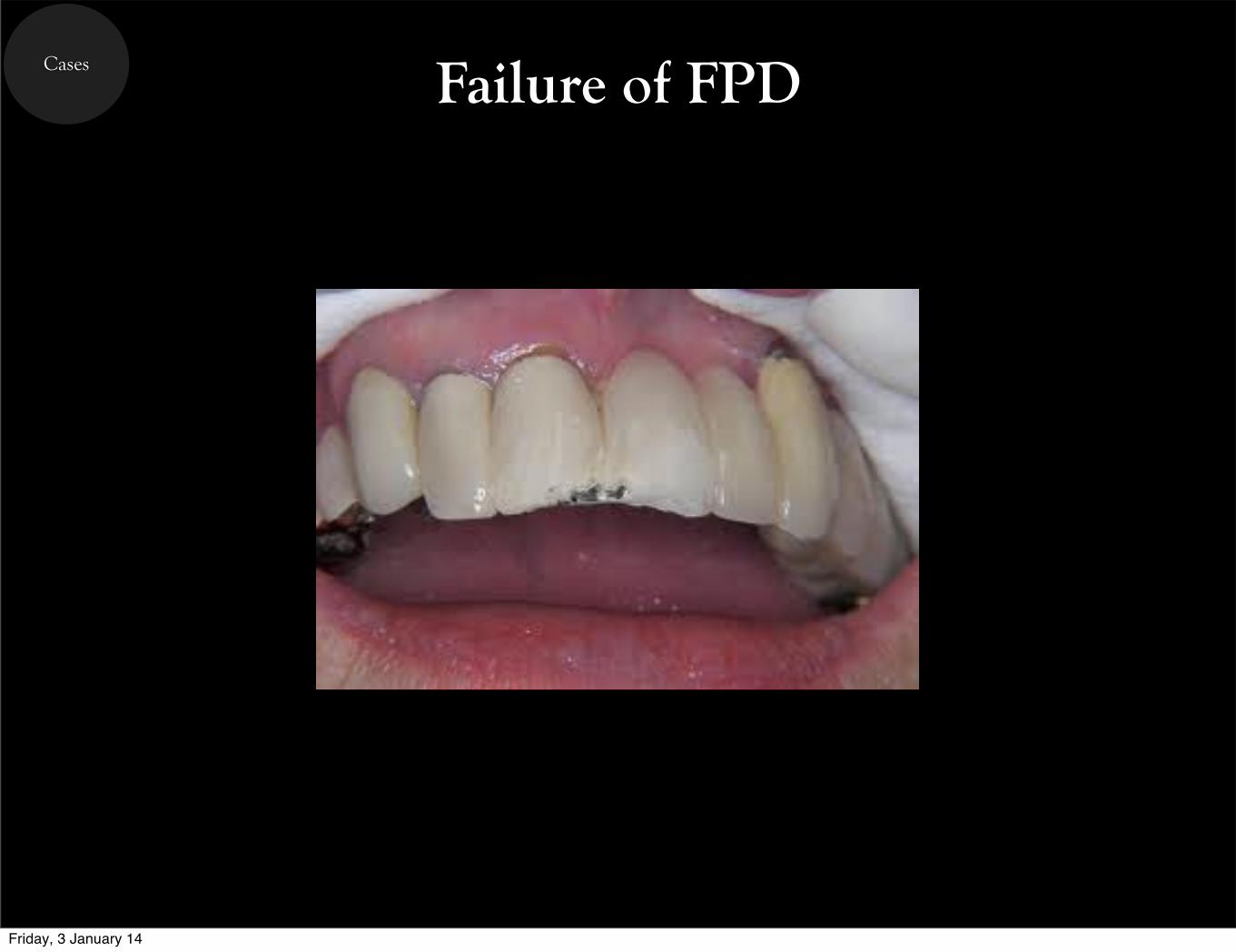
Cases Failure of FPD
Friday, 3 January 14

The End
Friday, 3 January 14
The End
References
Friday, 3 January 14