care of patient with stroke dr. belal hijji, rn, phd november 19 & 23, 2011
TRANSCRIPT
Care of Patient With Stroke
Dr. Belal Hijji, RN, PhD
November 19 & 23, 2011
2
Learning Outcomes
At the end of this and next lecture, students will be able to:
• Describe stroke and identify its classifications.
• Describe ischemic stroke, the risk factors predisposing to it, its pathophysiology, assessment and diagnostic findings, and its medical management.
• Describe subarachnoid hemorrhage, its clinical manifestations, classifications, diagnosis, and medical management modalities.
• Describe intracerebral hemorrhage, its etiology, assessment and diagnosis, and medical management.
• Discuss the nursing management of a patient with stroke.
3
Description of Stroke
• Stroke describes a sudden onset of acute neurologic deficit persisting for more than 24 hours and caused by interruption of blood flow to the brain.
• Stroke is either ischemic or hemorrhagic. Both conditions will be discussed next.

4
Ischemic Stroke• Description: Ischemic stroke results from reduction or
obstruction (thrombotic or embolic) of blood flow to the brain. Thrombosis can form in large or small vessels. Embolic sources include the heart and atherosclerotic plaques in the bifurcation of the common carotid artery.
A blood clot (thrombus) may form in the body, break-off, and travel to the brain
through a carotid artery. .

5
The blood clot may block the passage of blood through a brain artery, depriving nearby tissue of oxygen and nutrients. The result is
a stroke. .
6
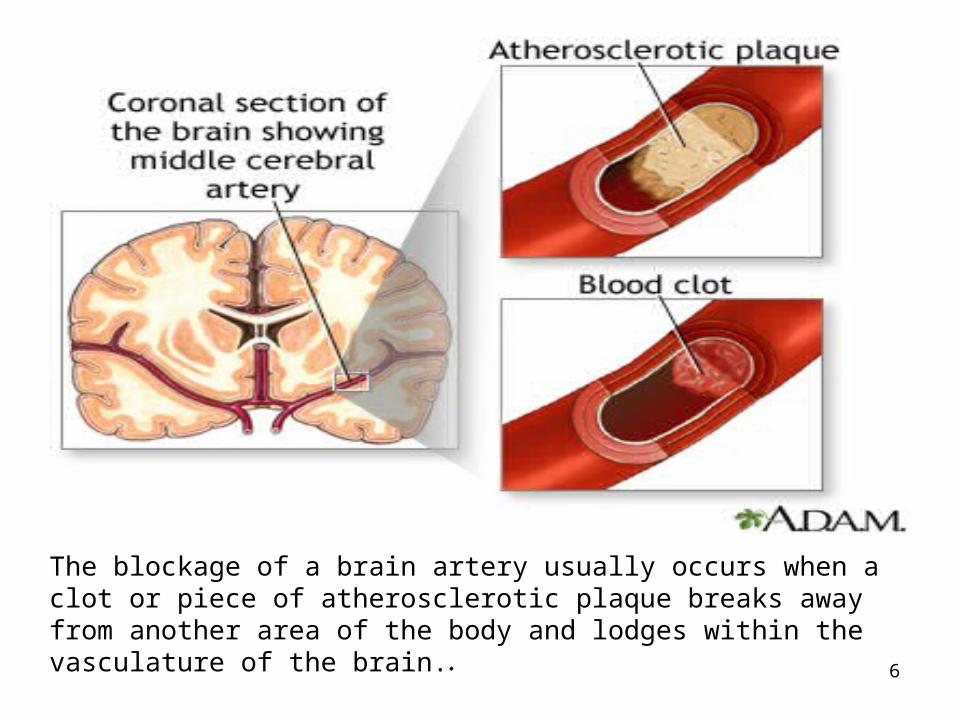
The blockage of a brain artery usually occurs when a clot or piece of atherosclerotic plaque breaks away from another area of the body and lodges within the vasculature of the brain..

7
Ischemic Stroke (Continued…)
• Risk factors: Hypertension, dyslipidemia, diabetes, smoking, and carotid atherosclerotic disease.
• Pathophysiology: Ischemic injury occurs when cerebral blood flow is reduced to a level insufficient to maintain neuronal viability. In focal stroke, an area of hypoperfused tissue, the
ischemic penumbra, surrounds a core of ischemic cells.
Penumbra: Occlusion of the left middle cerebral artery (MCA) with irreversibly dead tissue in black and tissue at risk or penumbra in red.

8
Ischemic Stroke (Continued…)
• Assessment and Diagnosis.– Hemiparesis, aphasia, and hemianopia [blindness in one half of
the visual field of one or both eyes] are common. Changes in the level of consciousness [coma, confusion, and agitation “اهتياج”] are usual.
– Noncontrast CT scanning is the most important diagnostic tool that can differentiate between ischemic and hemorrhagic stroke.
– MRI can demonstrate infarction in the cerebral tissue earlier than the CT but is less useful in the emergent differential diagnosis.

9
Ischemic Stroke (Continued…)• Medical Management.
– Thrombolytic therapy with IV recombinant tissue plasminogen activator (rtPA) is recommended to patients older than 18 years within 3 to 4.5 hours of onset of confirmed ischemic stroke. The dose is 0.9 mg/kg (maximum dose is 90 mg). Ten percent of the dose is given as IV bolus, and the remaining 90% is administered by intravenous infusion over 1 hour. Contraindications for thrombolysis are evidence of intracranial hemorrhage, suspicion of subarachnoid hemorrhage, recent stroke, recent serious head trauma (past 3 months), uncontrolled hypertension at the time of treatment, seizure, internal bleeding, and intracranial tumor.
– Airway protection and ventilatory support to maintain adequate tissue perfusion.
– For non thrombolysed patients (next slide), antihypertensive therapy is indicated only if DBP is > 120 mmHg or SBP > 220 mmHg.

10
Blood Pressure Management For Nonthrombolytic Candidates Blood Pressure
TreatmentDBP > 140 mm Hg
SBP > 220 mm Hg, DBP 121 – 140 mm Hg.
SBP < 220 mm Hg, DBP = 120 mm Hg.
Sodium nitroprusside (0.5 mcg/kg/min)
10-20 mg of labetalol given by IVP over 1-2 minutes; may repeat every 20 minutes.
Emergency antihypertensive therapy is deferred in the absence of acute MI, severe congestive heart failure, or hypertensive encephalopathy.

11
• Medical Management (Continued…).– Treatment of cerebral edema or seizure activity.
– Surgical decompression if a large cerebellar infarction compresses the brainstem.

12
Subarachnoid Hemorrhage (SAH)
• Description & Clinical Manifestations. SAH is bleeding into the subarachnoid space, which is caused by rupture of a blood vessel outside the brain. The space rapidly fills with blood, and the patient may have a sudden, intense headache, neck pain, and nausea or vomiting. The sudden buildup of pressure outside the brain may also cause coma or death.

13
Subarachnoid Hemorrhage (Continued…)
• Classifications. – Grade 1: asymptomatic or mild headache and slight nuchal
rigidity.
– Grade 2: moderate to severe headache, nuchal rigidity.
– Grade 3: drowsiness, confusion, or mild focal deficit.
– Grade 4: stupor and moderate to severe hemiparesis.
– Grade 5: deep coma and decerberate rigidity.

14
Subarachnoid Hemorrhage (Continued …)
• Diagnosis. Diagnosis of SAH is based on:– clinical presentation
– noncontrast CT findings
– lumbar puncture results. If CT finding is negative, CSF after SAH appears bloody and has a red blood cells count of > 1000/ mm3.Normally, CSF has no RBCs.
• Medical Management. SAH is a medical emergency and time is so critical. Medical management includes:– Surgical clipping or endovascular coiling of aneurysms (next two
slides): This is a definitive treatment for the prevention of re-bleeding.
– Embolisation: This procedure is indicated when an aneurysm is surgically inaccessible due to size, location, medical instability of the patient. It is performed under fluoroscopy guidance where microcatheters are inserted into the aneurysm and embolic material (like glue) is placed endovascularly.

15
Aneurysm clipping
Surgical clipping aims to isolate an aneurysm from the normal circulation. Under general anesthesia, craniotomy is performed. A small clip is placed across the base, or neck, of the aneurysm to block the normal blood flow from entering. Clips are made of titanium and remain on the artery permanently.

16
The goal of coiling is to isolate an aneurysm from the normal circulation. A flexible catheter enters through the large femoral artery and is advanced to one of the arteries in the neck that leads to the brain. Once the catheter reaches the aneurysm, a very thin platinum wire is inserted, which coils up and is then detached. Multiple coils are packed inside the dome. Over time, a clot forms inside the aneurysm, effectively removing the risk of aneurysm rupture.
Most aneurysms are balloon-like, with a narrow neck at the origin and a large expanding dome.
Coiling

17
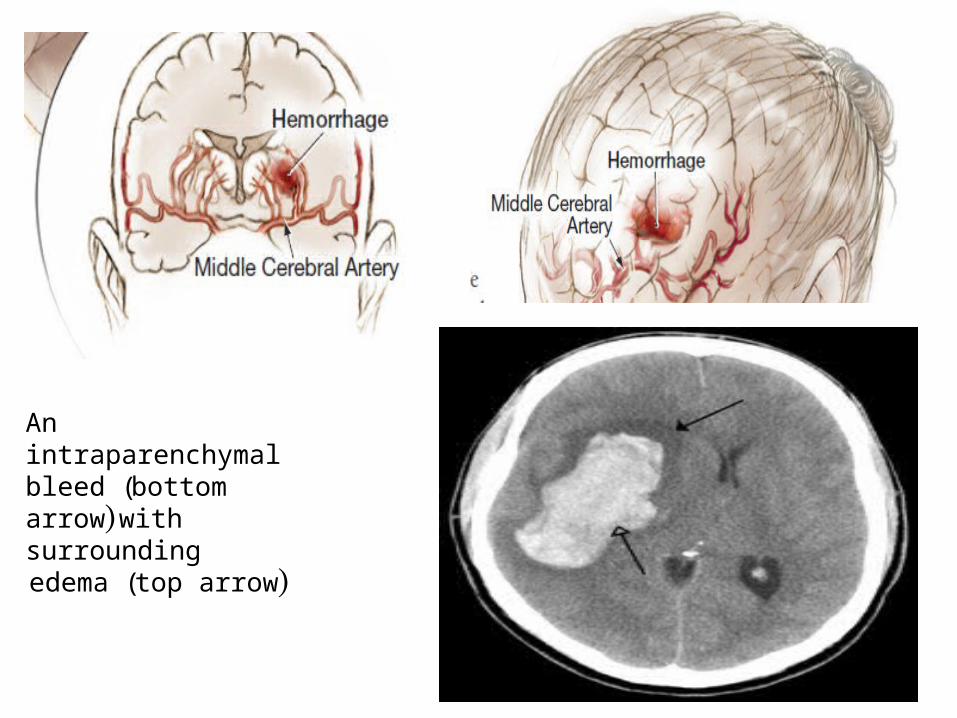
Intracerebral Hemorrhage (ICH)
• Description and etiology: ICH is bleeding directly into the cerebral tissue destroying it, causing cerebral edema, and increasing intracranial pressure. The most common cause of ICH is hypertension. Other possible causes are thrombolytic therapy, coagulation disorders, drug abuse, and bleeding into cerebral infarct or tumor.
• Assessment and diagnosis. The patient is often unconscious requiring (50% of patients) ventilatory assistance. The patient’s relatives describe sudden focal deficit (left face, right arm, tongue) accompanied by nausea, vomiting, and severe headache. Patients have severe elevation of blood pressure (200/100 to 250/150 mm Hg) and increased ICP. Diagnosis is established by CT brain scanning.
18
An intraparenchymal bleed (bottom arrow) with surrounding edema (top arrow)
19
Intracerebral Hemorrhage (Continued…)
• Medical Management. As ICH is a medical emergency:– attention must be given to airway, breathing, and circulation.– Intubation is usually necessary.– Blood pressure management is individualised. Careful reduction
of BP is required to decrease ongoing bleeding. However, too rapid or too much lowering of BP may compromise cerebral perfusion pressure (CPP) especially in patient with increased ICP. CPP must be maintained above 70 mm Hg.
– Increased ICP is managed through mannitol, hyperventilation, sedation.
– Fluid management to maintain pulmonary artery occlusion pressure of 10-14 mm Hg.
– Body temperature is kept < 38.5, and blood glucose level of < 140 mg/dL without inducing hypoglycemia.
20
Nursing Management of Stroke
• Performing Frequent Assessments. Nurses:– Should closely monitor of the patient’s neurologic signs and
vital signs.
– Should use automatic noninvasive devices such as blood pressure cough and pulse oximeter.
– Must identify seizure activity and report to physician for immediate management.
• Maintaining Surveillance For Complications. Nurses should:– Closely monitor the patient for bleeding, vasospasm, and
increased ICP.