care partners in-person training - aims center
TRANSCRIPT

Care Partners In-Person Training
Depression in Late-Life Initiative September 17 & 18, 2015


Site Introductions Vision, Innovation, & Workflow Sharing


Downtown Family Health Center at Connections (DTFHC) Clinic DTFHC resides in the heart of downtown San Diego – home to many of San Diego’s lowest-income seniors – and is co-located within a multi-service residential community designed to help homeless individuals move into permanent housing.
–Margarita Velosa, LCSW, PhD, Care Manager
– Steven Ritter, DO, Primary Care Provider
–Gabrielle Cerda, MD, Psychiatry Consultant
–Myra Buby, LCSW, Project Lead

Serving Seniors- CBO
An independent non-profit focused on improving the health and wellbeing of San Diego’s low-income seniors through the provision of essential services such as food, healthcare, housing, and social services.
–Dennis Dearie, MFT, Case Manager
–Parwin Tahir, MSW, Case Manager

FHCSD/SS: Vision Statement
Our vision is a community which optimizes mind, body, and spirit – one senior at a time.

Family Health Centers of San Diego: Innovation and Workflow Patient’s Workflow Experience • In the course of the primary care visit patients 65 and older
with a positive PHQ-9 screening will be identified and referred to the care manager for further assessment.
• Services will be provided within an integrated approach • Comprehensive multidisciplinary assessment of medical,
functional and psychosocial needs will be provided with ongoing follow-up of patients;
• Coordination across providers • Intensive health education and support for lifestyle
modification; • Monitoring of patients’ progress between office visits • Additional skills provided will include: psycho-education,
positive coping techniques and development of solid self-management skills.

Family Health Centers of San Diego: Innovation and Workflow (continued) Key Points of Workflow • Flexible and innovative integrated services for older adults
• Clarity about responsibilities and accountabilities
Key parts of workflow that have been/are expected to be the most challenging • Patients not wanting to participate in the program
• Identifying patient eligibility
• Fragmented workflow within clinicians and lack of familiarity with the registry
Family Health Centers of San Diego: Innovation and Workflow
Ideas to overcome challenges • Continuous Dissemination of the project to both FHCSD
staff and Serving Seniors staff
• Continued Collaboration between primary care and mental health
• A collaborative phone conference between Serving Seniors and Family Health Centers


Clinic and CBO Introductions
El Sol Neighborhood Educational Center, a community-based organization serving seniors in the city of San Bernardino, California. Team: Oscar S. Bustillos, Alex Fajardo, Angelica Alvarez, Monica Fuentes, and Irma Abaunza
SAC Health System provides comprehensive and low-cost health care services in San Bernardino, California. Team: Tom Bazemore, Adriana Gomez, Jason
Lohr, and Brenda Boyle

Vision Statement
• El Sol and SAC Health System (SACHS) commit to focus on improving care quality and coordination of care among older adults from various racial and ethnic backgrounds in our community with, or at-risk, for depression through Collaborative Care by comprehensive community-based, family-focused, and patient-centered outreach and education.

SACHS & El Sol: Workflow
Participants will be recruited through
• Community outreach events (health fairs, educational presentations held at churches, homes and schools)
• Medical appointments at SACHS (positive score on the PHQ-2)
Potential participants will be asked to complete a screening tool to determine their eligibility
• Each person approached will receive either verbal or written educational information on Depression, General Anxiety Disorder and its symptoms
• Patients will be warmly connected between CHW’s and Care Manager during treatment process.

Workflow & Innovation (cont.) • Enrolled patients can expect follow-up home visits from
Community Health Workers (CHWs) to assess their needs and develop a plan of action to fill them.
• Patients will be referred to a Therapist professional for further care.
• Patients will be educated on Medications (if applicable) during treatment plan.
• CHW’s and Clinic will work closely using CMTS registry as a means of communication and patient evaluation.
• CBO and Clinic staff (Project Lead, CHW’s, Care Manager, Psychiatric Consultant) will have weekly meetings to discuss treatment options and plans.
• After patient has shown signs of improvement, patient will be assessed once more and follow up calls will occur 1-3 months after last home visit.
Workflow & Innovation (cont.) Community Health Workers (CHWs) will:
• Work individually with each patient and be exceptionally involved in providing the best support to eliminate depression and depressive symptoms
• Complete home visits to encourage behavior activation that can counteract the client’s depressive symptoms.
• Provide tools that will bring Empowerment to the Patient and work with them to develop their strengths.
• Provide home-based activities that will vary with each client’s response to the PHQ-9, so that they are tailored to address the areas of the screening where a Patient scored the highest and help improve their score.

Workflow & Innovation-Potential Challenges
Lack of active participation from clinicians (physicians, therapists and psychiatric consults)
• limited availability to participate in meetings or update a client’s “chart” on the CMTS system
Following up with “hard to reach” clients
• Unreliable contact information • Do not want home visits • Partners/caregivers are reluctant to
participate in program

Workflow & Innovation-Overcoming Challenges
Lack of active participation from clinicians • Care Manager and the CHW’s can consult
individually at clinic update clients’ “charts” on CMTS and provide updates at weekly meetings
Following up with “hard to reach” clients
• Collect contact information for participant and several family members/partners in their care
• Follow-up visits can be completed at location outside home that client feels comfortable with and can easily access (El Sol - CBO), during their medical appointment, at their church, etc).
• Follow-up can be completed over the phone/email


Sonoma Care Collaborative Clinic and CBO Introductions • Clinic: Petaluma Health Center - Nurit Licht, M.D., Chief Medical Officer
- Todd Finnemore, Psy.D., Geropsychology
- Ken Weinstock, Psychiatric Consultant - Vicki Rivera, LCSW
• CBO: Sonoma County Human Services Department/Adult & Aging Division
- Anne Percival, Social Work Supervisor
- Diane Camurat, Social Worker/Community Home Visiting Coordinator

Sonoma Care Collaborative Vision Statement
We envision a Sonoma Care Collaborative with a thoughtful, inclusive, and efficient system of care that is focused on delivering whole person care that incorporates medical and social-environmental factors.

Sonoma Care Collaborative: Innovation and Workflow
• Clinic: Petaluma Health Center (PHC)
– Patient Experience: patients will engage in our collaborative in a team-based and supportive environment.

Sonoma Care Collaborative: Innovation and Workflow
• CBO: Sonoma County Human Services Department (HSD)/Adult & Aging Division
- Providers of services to empower, support and protect clients throughout the community
- Experts in delivering coordinated care in older adults’ homes
- Experienced in implementing Healthy IDEAS

Sonoma Care Collaborative: Innovation and Workflow
– Innovations:
• Within PHC, teams are supported by engaged staff and providers, data analytics, and collaborations across family medicine, behavioral health. Multiple avenues exist to engage patients into the program.
• Collaboration continues beyond PHC to our partnering community-based organization, the Division of Adult and Aging; through this collaboration, we are able to provide comprehensive care located both in the medical home (PHC) and the patient’s home.

Sonoma Care Collaborative: Innovation and Workflow
– Challenges:
• Coordinating care and information across team members who are working for different organizations, and making coordination of care seamless for the patient.
• Understanding which patients will benefit most from our innovative and collaborative care model.

Sonoma Care Collaborative: Innovation and Workflow
– Overcoming Challenges:
• Coordinated use of registry, electronic medical record, and meeting time and dedicated support staff to ensure seamless coordination. Patient engagement education and written material to explain the team model and provide consistent contact information to access team members.
• Scheduled consultations with PHC LCSW will allow for stratification of patients and over time provide information as to which patients will benefit most from our collaborative care model.


Clinic and CBO Introductions Primary Care Clinic – LifeLong Medical Care Over 60 Berkeley, CA
– Team Members:
• Program Supervisor: Alex Baker
• PCP: Jennifer Elton
• Psychiatric Consultant: Megan O’Brien
• Care Manager: Jesse Merjil
• Community Health Worker: Alexis Bradley
Community Based Organization – St. Mary’s Center Oakland, CA
– Team Members:
• Carol Johnson
• Karla Salazar

Clinic Name: Vision Statement
Vision Statement LifeLong Over 60
We envision LifeLong Over 60 and St. Mary’s center through Collaborative Care will support the identification,
engagement and treatment of depression among high risk adults 65 plus. We will improve the access of
depression care, which we believe will benefit older adults. Both organizations recognize the importance of
developing trust with older adults who face poverty, isolation and often have distrust of the medical system.
We will form a strong basis for successful screening, enrollment and patient participation in depression care.

LifeLong Medical Care: Innovation and Workflow
• At LifeLong Over 60 and Saint Mary’s we aim to identify and screen between 10-15 patients ages 65+ per week.
• How would a patient experience our workflow?
– Identify and Engage Patients/Establish Diagnosis
– Meet Mr. Johnson! • Mr. Johnson is a 70 year old patient with our Over 60 Health Center
• Scheduled appointment at Over 60 to discuss managing his diabetes.
• Prior to his appointment CHW meets with him and introduces the screening process using PHQ-9.
• Mr. Johnson’s PHQ-9 score was a 13, moderate level depression.
• Receives diagnoses from PCP discuss treatment options.

LifeLong Medical Care: Innovation and Workflow
• How would a patient experience our workflow? – Initiate and provide treatment
• A warm connection made between our PCP and Care Manager/CHW.
• Allow Mr. Johnson to discuss his concerns.
• Our team will educate him about depression, Collaborative Care and the treatment options available.
• Mr. Johnson says no antidepressants!
• But is interested in therapy sessions and community support group at our CBO (Saint Mary’s Center).
– Here a treatment/care plan will be developed and initiated

LifeLong Medical Care: Innovation and Workflow
• How would our patients experience our workflow? – Follow-up Care and Treatment to Target
• CHW does the first two week follow-up call with Mr. Johnson.
• Mr. Johnson has been attending his therapy sessions, but hasn’t wanted to attend the support group at Saint Mary’s.
• Lack of transportation is keeping him from attending the groups.
– Transportation resources are arranged.
• CHW also agrees to meet Mr. Johnson at Saint Mary’s as additional support.
LifeLong Medical Care: Innovation and Workflow
• How would our patients experience our workflow? – Complete Treatment and Relapse Prevention
• Over the course of 12 weeks of treatment Mr. Johnson’s PHQ-9 score has improved from a 13 to a 5.
• He is scheduled a follow-up appointment with our CM to discuss the end of his treatment and plan his RPP.
• He agrees to continue attending his support groups at our CBO and has set goals to ensure no relapse in his symptoms.
• Mr. Johnson is reassured that he has our entire team as a support system as he continues to recover from his depression.

LifeLong Medical Care: Innovation and Workflow • A possible challenge we may face…
– Patients may see treatment as a burden or indication that they are suffering from irregular circumstances.
• Ways to overcome this challenge… – Ensuring patients that we, as a team, will work through their
circumstances to find the best solution for them.
– Helping patients understand that they have a huge support system through the LifeLong and Saint Mary’s Center team.
– Understanding that this treatment will not be a burden but rather an uplifting, progressive movement toward living a happier and healthier life.
As a team LifeLong Medical Care and Saint Mary’s Center aim to successfully treat as many patients as possible and provide each with
healthy and prosperous lives!


UCSF House Calls and Geriatric Clinic, San Francisco, CA • Dr. Helen Kao, UCSF Geriatrics
Clinical Program, Medical Director
• Dr. Meredith Greene, UCSF Geriatrics Clinical Program, Medical Director
• Dr. Daniel Pound, UCSF Center for Geriatric Care
• Marisa Guardado, Clinical Social Worker, UC Care at Home Division of Geriatrics
• Alexis Armenakis, Psychiatric Consultant
Institute on Aging Psychology Department, San Francisco, CA • Karyn Skultety, Ph.D., Vice
President of Health Services
• Carolyn Stead, Psy.D., Project Director, Director of Psychology and Counseling Services
• Clare Farrington, Program Coordinator, Psychological and Counseling Services
• Alyson Madigan, Psy.D. Psychology Post-Doctoral Fellow
• David Shoup, M.A., Psychology Pre-Doctoral Trainee

Vision Statement • The vision of our project is to develop a robust, long-term partnership
between two organizations that strive to increase the quality of life for isolated, homebound adults in our community. Often times homebound elders face significant barriers in accessing adequate mental health services as it is difficult if not impossible for them to leave their homes and very limited, if any services exist to provide affordable treatment in home. We strive to develop an innovative model that addresses the limited access to mental health services for these older adults. This includes the use of Collaborative Care to increase communication between providers, track treatment outcomes, and prevent clients from “falling through the cracks.” Our vision is that through our primary care and psychotherapy collaboration, we will provide effective treatment for homebound elders struggling with depression and create a model that is both replicable and sustainable.

UCSF & Institute on Aging: Innovation and Workflow
Mrs. Anderson has been receiving UCSF primary care services in her home for almost a year now. During a
routine home visit, her doctor recognizes some symptoms of depression and suggests to Mrs. Anderson that she might benefit from having
someone to talk to. Mrs. Anderson agrees and her doctor makes a referral to IOA. The next week, an IOA clinician knocks on Mrs. Anderson’s door to complete
a clinical assessment and discuss next steps.

UCSF & IOA: Innovation and Workflow • Innovation: Patients will be asked by their trusted PCP to
agree to have an additional provider come to them in their home instead of being referred to an outside clinic.
• Challenges: Scheduling “warm connections,” organizing consistent collaboration with non-traditional physical clinic setting and satellite providers.
• Plans to overcome challenges: have PCP state which methods of communication they prefer on referral, scheduling regular consultation meetings that overlap with other staff meetings and have a call-in line available, and consistent collaboration w/supervisors

Clinic and CBO Introductions
• USC Dept of Family Medicine, Los Angeles, CA, Sandra Avila, Jennifer Talbot, Camilo Zaks
• Eisner Pediatrics and Family Medicine: USC-Eisner FMC, Eisner Adult Dept., Los Angeles, CA, Gail Myers, Jose Luevano, Ana Rosas, Eveline Zamora
• St. Barnabas Senior Services, Los Angeles, CA, John Kotick, Maria De Leon

USC/Eisner/SBSS: Vision Statement
• The USC-Eisner-SBSS BALLAD project will improve the treatment of depression in older adults through a collaborative and comprehensive approach to treatment, using a Collaborative Care model plus integration of a Senior services center and training family members to be part of the care team.

USC/Eisner/SBSS: Innovation and Workflow • Eisner First Visit
– Annual depression screening w/ PHQ2PHQ9 – Warm Connection to Case Manager – Case Manager does additional screening (Bipolar, etc.) and does
intake. – Case Manager links to LCSW therapist via EMR – Case Manager links to SBSS by telephone during visit.
• Eisner after First Visit – LCSW contacts patient to set up first session. – LCSW does therapy PST, following protocol.
• SBSS – liaison contacts patient to set up first session. – liaison provides connection to SBSS services. – liaison trains family member to be Caregivers
Innovations in italics and bold.

McClellan Outpatient Clinic Vision & Workflow

• McClellan Outpatient Center
• Sacramento
• Team members
Angela Araneta, Psy.D.
Jane Addagatla, M.D.
Brian Dahmen, Ph.D.
Ladson Hinton, M.D.
Thuc-Nhi Nguyen, Ph.D.
Clinic Introductions

To develop and implement a family-centered model of collaborative depression care to advance outcomes for older veterans
Vision Statement

• Patients screened and engaged in family-centered care during regular primary care visits
• Innovation • Family care partners share in multiple
collaborative care tasks • Using groups to reinforce family-centered care
• Challenges and solutions • Working with PCPs to change practice • Engaging patients and family members • Negotiating confidentiality concerns
Innovation and Workflow

BREAK
Collaborative Care
Jürgen Unützer MD, MA, MPH Professor and Chair Psychiatry & Behavioral Sciences, University of Washington Seattle, Washington

Depression
• More than having a bad day, week, or month
• Pervasive depressed mood/sadness
• Loss of interest/pleasure – Lack of energy, fatigue, poor sleep and appetite, physical slowing or agitation,
poor concentration, physical symptoms (aches and pains), irritability, thoughts of guilt, and thoughts of suicide
• A miserable state that can last for months or even years

What Do Patients Say?
“I am depressed.” “My wife thinks I am depressed.”
or.. “I just don’t feel right … I hurt all over …”
“I just don’t have any energy … it’s all getting me down.”
“I just can’t sleep.”
“I don’t know what hit me …I can’t do anything”
“I am not crazy”
“Isn’t depression just a part of ‘normal aging?”
“Wouldn’t you feel this way if you had lost your spouse?”

Depression is Deadly • One suicide every 14 minutes.
• Older men have the highest rate of suicide.
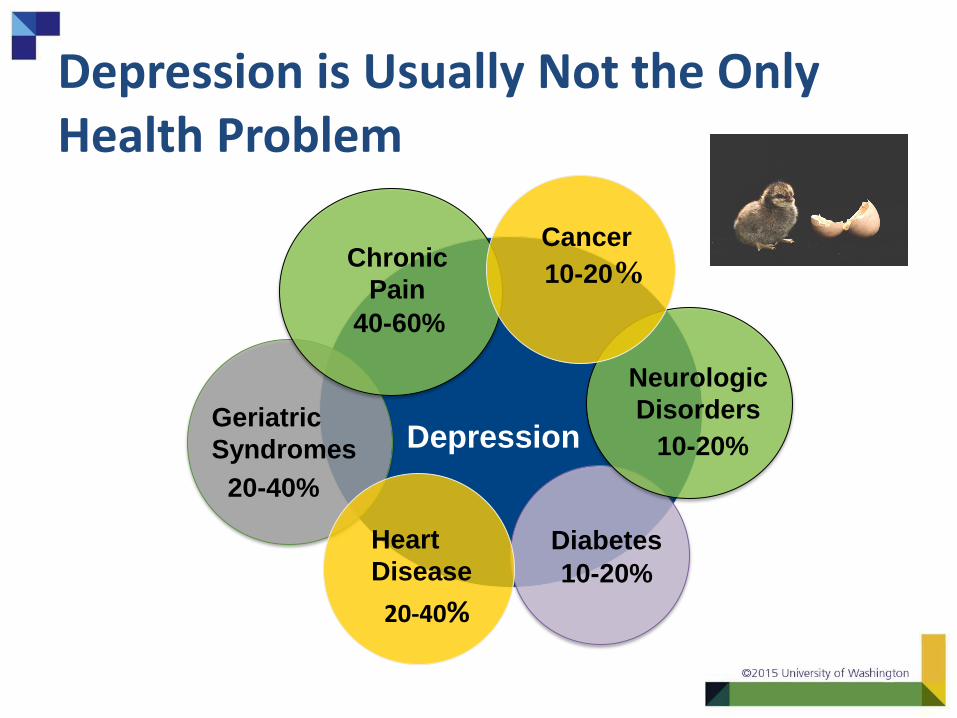
Depression is Usually Not the Only Health Problem
Depression
Neurologic
Disorders Geriatric
Syndromes
Diabetes
20-40%
10-20%
10-20%
Heart
Disease
20-40%
Chronic
Pain
40-60%
10-20%
Cancer

Depression and Diabetes

Effective Treatments for Late-Life Depression • Antidepressant Medications
– Over 25 FDA approved
– All are effective in 40 - 50% of patients if taken correctly
– It often takes several trials to find effective treatment
– Patients need support during this time
• Psychotherapy
– CBT, IPT, BA, PST, etc.
• Other somatic treatments
– Electroconvulsive Treatment (ECT)
• Physical activity/exercise Unützer et al, NEJM 2007

BUT: Few Older Adults Get Effective Depression Treatment
• One in 10 older adults see a psychiatrist – Limited access and concerns related to stigma
• Increasing use of antidepressants in primary care • PCPs prescribe 70 – 90 % of antidepressants
• 10 - 30 % of older adults are on antidepressants (> 4 million)
• But treatment is often not effective
– 30 % drop out of treatment within 4 weeks
– Only 25 % receive adequate follow-up care
– Only about 20 % improve substantially over 12 months
• Limited access to evidence-based psychosocial treatments (psychotherapy)

Bridging the Divide Between Mental Health & Primary Care
• Mental health is part of overall health
• Treat mental health disorders where the patient is/ feels most comfortable receiving care
– Established doctor-patient relationship is an important foundation of trust & helps reach more people in need
– Less stigma
– Better coordination with medical care

IMPACT Study • 1998 – 2003
• 1,801 depressed adults
• 18 primary care clinics – 8 health care organizations in 5 states
• Diverse health care systems – Urban & semi-rural settings
– Capitated (HMO & VA) & fee-for-service
• 450 primary care providers
• Two groups compared: – Usual Care
– Collaborative Care

IMPACT Program
PCP with Care Manager and Patient
Practice Support Registry Consultation Tools & Training Measures

Doubles Effectiveness of Care for Depression
%
Participating Organizations
50 % or greater improvement in depression at 12 months
Unützer et al., JAMA 2002; Psych Clinics North America 2004
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8
Usual Care IMPACT

43%
54%
42%
19% 23%
14%
0%
10%
20%
30%
40%
50%
60%
White Black Latino
IMPACT Care
Care as Usual
Areán et al. Medical Care, 2005
50 % or greater improvement in depression at 12 months
IMPACT Care Benefits Disadvantaged Populations

IMPACT: Summary 1) Improved Outcomes:
— Less depression — Less physical pain — Better functioning — Higher quality of life
2) Greater patient and provider satisfaction
3) More cost-effective
“I got my life back”
THE TRIPLE AIM

Principles of Collaborative Care
Evidence-Based
Population-Based
Treatment to Target
Patient-Centered Team
Accountable

Elizabeth’s Story
https://aims.uw.edu/elizabeths-story

Collaborative Care Delivering Care as a Team

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Collaborative Care Team Approach
New Roles
PCP
Psychiatric Consultant
Patient
© University of Washington
Care Manager
Community Partner
PCC

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Identify and Engage
• Identify people who may need help
• Help patient understand how depression affects them and instill hope
– “You don’t have to feel this way. “
• Identify safety and other concerns
• Introduce Collaborative Care, engage patient in program, and introduce team

PHQ-2 and PHQ-9 as “Vital Signs”
Like screening and monitoring blood pressure!
– Identify that there is a problem
– Need further assessment to understand the cause of the “abnormality”
– Track to measure response to treatment

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Provisional Diagnosis
Provisional diagnosis and
treatment plan
Screen filled out by patient
Assessment by PCP & CM
Psychiatric Consultant
Case Review
71

Common Medical Causes of Depression • Neurological Disorders
– CVA
– Parkinson’s disease
– Huntington’s disease
– Multiple sclerosis
• Cardiovascular disease
– Vascular depression
• Obstructive sleep apnea
• Cancers
– Pancreatic cancer

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Patient Education
• What is depression?
• Instill hope about treatment:
– “You don’t have to feel this way.”
– “We have several good treatment options”
• Discuss concerns and anticipate problems
• Involve significant others
• Systematically assess and follow – Treatment adherence (how are you using the meds?)
– Depressive symptoms (use a scale such as the PHQ-9)

The ‘Cycle of Depression’

Treatment Options
• The treatment that WORKS is the best one
– “One size fits few”
• Medication therapy is not right for everyone; often several trials of medications are needed
• Psychotherapy is not right for everyone; different approaches
• Supporting during treatment is important
– Everyone knows the treatment plan, supports patients, and
can help identify when treatment is not working and
changes should be made.

FDA Approved Antidepressants
• Serotonin Reuptake Inhibitors (SSRIs) – fluoxetine (Prozac), paroxetine (Paxil), citalopram
(Celexa), escitalopram (Lexapro), sertraline (Zoloft), fluvoxamine (Luvox)
• Newer Antidepressants (atypical)
– bupropion (Wellbutrin), mirtazapine (Remeron), venlafaxine XR (Effexor), desvenlafaxine (Pristiq), duloxetine (Cymbalta)
• Tricyclics (TCAs)
– secondary amines: nortriptyline, desipramine
– tertiary amines: imipramine, doxepin, amitriptyline
– Not recommended as 1st line for older adults due to side effects.

Choosing Antidepressants
• All FDA approved antidepressants are equally effective (~ 50 % have a substantial response)
• Considerations in selecting an antidepressant: – Prior treatment history in patient / family members
– Patient preferences
– Expertise of prescribing provider
– Side effect profile (sedating or activating)
– Safety in overdose
– Availability and costs
– Drug-drug interactions

SSRIs: 1st Choice Agents
Starting
Dose/day
Therapeutic
Range/day*
Generic CYP 450
effects
Side-effects
Fluoxetine
(Prozac®)
5-10mg
Qam
10-20mg Y +++ +/++
Sertraline
(Zoloft®)
12.5-25
Qam
50-150 Y ++ ++
Paroxetine
(Paxil®)
10
Qhs
20-30 Y ++ ++
Citalopram
(Celexa®)
10
Qhs
20-40 Y + +
Escitalopram
(Lexapro®)
5-10
Qam
10-20 N ± ±
Espinoza R., Unützer, J. 2013; Mittman 1999; Solai 2001; Sommer 2003; Williams 2000

Assure Adequate Medication Trials
• Follow-up closely to asses progress: – Treatment adherence
• “Are you taking medications?” “How are you taking them?”
• Are you having side effects or concerns?
– Treatment response
• Use a scale such as the PHQ-9 to track symptoms
• Make sure the dose is high enough
– Start low but make sure you achieve therapeutic dose.

Is The Patient at Maximum* Daily Therapeutic Dose?
• Fluoxetine (Prozac) 40 mg
• Paroxetine (Paxil) 50 mg
• Citalopram (Celexa) 20 mg
• Escitalopram (Lexapro) 20 mg
• Sertraline (Zoloft) 200 mg
• Venlafaxine (Effexor) 300 mg
• Desvenlafaxine (Pristiq) 100 mg
• Duloxetine (Cymbalta) 60 mg
• Buproprion (Wellbutrin) 450 mg
• Mirtazapine (Remeron) 45 mg
• Nortriptyline 125 mg (check serum level)
• Desipramine 200 mg (check serum level)
* Start all meds low but go to effective or maximum dose as tolerated over 4-12 wks.

Adverse Effect Profiles
Common – nausea
– loose stools
– restlessness
– akathisia
– insomnia
– headache
– sexual dysfunction
Less common – weight loss / gain
– hyponatremia (SIADH)
– sinus bradycardia
– cardiac arrhythmia
– bleeding (anti-platelet effect)
– Parkinsonism
– Serotonin Syndrome
SSRIs: serotonergic; variably anticholinergic,
antihistaminergic or antidopaminergic

What If Patients Don’t Improve?
Is the diagnosis correct?
? Bipolar depression (manic symptoms: no sleep, excess energy / irritability): use mood stabilizers – not antidepressants: lithium, valproate, lamotrigine, quetiapine
? Psychotic depression: add antipsychotic (e.g., risperidone, olanzapine, quetiapine); consider ECT
? Medical conditions
hypothyroidism, sleep apnea, pain, neurological, neurodegenerative disease, vascular disease, chronic conditions / inflammation, geriatric syndromes
? Medications: steroids, interferon, hormones
? Withdrawal: stimulants, anxiolytics, alcohol, opiates

‘Plan B’ • No response: switch to antidepressant from a different class
– SSRI, SNRI, Bupropion, Mirtazapine, TCA
• Partial response: augment antidepressant
– Other antidepressants (e.g., Bupropion, Nortriptyline)
– Lithium, Thyroid, Stimulants
• Psychotherapy
• Physical Activity / Exercise
• Social Activity
• Electroconvulsive therapy
– Especially if severe, psychotic

“Dual Action” and Atypical Antidepressants
Starting Dosage (mg)
Range*
(mg)
Treatment
Resistance
Drug Interactions Potential SE
Venlafaxine
(Effexor XR®)
37.5 Qam 75-225 Yes Minimal DBP, BP
↓Na, Nausea
Desvenlafaxine
(Pristiq®)
50 Qam 50-100 Unknown Minimal DBP, BP
↓Na, Nausea
Mirtazapine
(Remeron®)
7.5-15 Qhs 30-45 Yes Minimal Sedation, wt
Dry mouth
Duloxetine (Cymbalta®) 20 Qam 20-60 Unknown Minimal DBP, BP
↓Na, Nausea
Nefazodone
(^Serzone®)
50-100 BID 300-600 Unknown Probable
(3A4 inhibition)
liver enzymes?
Sedation
Trazodone
(Desyrel®)
25-50 Qhs 300-600 Unknown Minimal ↓BP, sedation, priapism
Bupropion
(Wellbutrin XL, SR®)
50-75 BID 100-450 Possible Minimal DBP, BP
Seizures
Vilazodone
(Viibryd®)
10 Qam 10-40 Unknown Minimal GI upset, insomnia
Levomilnacipran ER
(Fetzima®)
20 Qam 40-120 Unknown Unlikley GI distress, BP, HR,constipation
Vortioxetine
(Brintellix ®)
5mg Qam 5-20mg Unknown Possible HA, dizziness, GI upset, constipation
* Dosage for Major Depression; ^ Brand not available

Psychotherapy
• Orientation – Cognitive-behavioral
– Interpersonal
– Problem-solving
– Dialectical-behavioral
– Bereavement/Grief Therapy
– Psychodynamic Therapy
– Supportive Therapy
– Reminiscence and life review
– Bibliotherapy
• Modality – Individual
– Couple
– Family
– Group
• Practitioners – Psychiatrists
– Psychologists
– Social Workers
– Nurse therapists
– MFTs

Communication: Care Manager and Primary Care Provider
PCP
Psychiatric Consultant
Patient
Care Manager Role
Community Partner
PCC
GOAL: Efficiently communicate about patient care. • Specific Question or
Request • Brief history of problem • Current treatment
duration, effectiveness, side effects.
• Psychiatric recommendations

Communication: Care Manager and Psychiatric Consultant
PCP
Psychiatric Consultant
Patient
Care Manager Role
Community Partner
PCC
GOAL: Provide psychiatric expertise
to team
• Consultation Scheduled As Needed
• Education Integrated Presentations

Psychiatric Consultation Model Consultation Hour
• Brief check-in – Changes in the clinic – Systems questions
• Identify patients and conduct reviews – Requested by CM – Not improved – Severity of presentation – Disengaged from care
• Wrap-up – Confirm next consultation hour – Send any educational resources discussed

Provider to Provider Communication How and When?
• Consider modality – In person – Staff (MA or nurse) – Phone – Fax – Email (careful with confidential info) – EMR
• Frequency – Scheduled
– As needed

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Comparison of Contacts in Usual Care vs. IMPACT
Usual Care 3.5 PCP Contacts per year*
*Based on HRSA report of average PCP visit rates for FQHCs
20% - 40% treatment response/improvement
12 months 0
= PCP contact

Comparison of Contacts in Usual Care vs. IMPACT
Collaborative Care
50% - 70% treatment response/improvement 12 months 0
= PCP contact (avg. 3.5 contacts per year)
= Case reviews from psychiatric consultant to BHP/CM, PCP (avg. 2 case reviews)
= Contacts with BHP/CM (avg. 10 contacts)

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
System Level Supports

Typical Course of Care Management: Duration
Primary Care Panel
Collaborative Care Caseload
Referral to Specialty Mental
Health
Relapse Prevention

Questions?

Mobilizing Family Support to Advance Collaborative Care for Depression
Ladson Hinton, MD
University of California Davis

Overview
• Defining “family”
• Why involve family?
• Challenges of involving family
• Overview of how family can strengthen depression collaborative care
• Questions/discussion

Who is “Family”?
• Persons in the older adult’s social network who are
– Present in patient’s home or community
– Acceptable/preferred by patient
– Motivated to be part of care team
• Wide range of kin and non-kin
– Spouses, significant others, children, extended family, friends, neighbors, etc…
– Paid in-home caregivers

Why Involve Family?
• Family members are often already involved!
• And patients want them involved
• But they are not well-supported by healthcare systems
• With recognition, support, and skills, family can be valuable depression care partners
• Together we have nice opportunity to advance the field

Common Challenges
• Time
• Confidentiality / privacy issues
• Family impedes treatment
• Elder abuse situations
• Provider comfort in working with family
• Multiple family members involved
• Cultural aspects of family caregiving
• Family unavailable (time, interest, etc..)

Role of Family in Collaborative Care
• Participation in assessment and treatment planning process
• Psychoeducation
• Supporting evidence-based care – Behavioral activation/problem-solving
– Medication management
• Participation in primary care visits
• Facilitating connection to CBO
• Relapse and prevention planning

Partnering with a CBO and Family
PCP
Psychiatric Consultant
Patient (Family)
Care Manager
Community Partner
PCC

Resources
• All of us!
– Discussion of family involvement on calls
– VA workflow document
• Consultation with UC Davis team
– Ongoing NIMH funded study on depression and family engagement
• References

Reflection

LUNCH

Delivering Care as a Team

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat
to Target
Complete Treatment &
Relapse Prevention

Behavioral Health Measures as “Vital Signs”
• Behavioral health measures are like monitoring blood pressure!
– Identify that there is a problem
– Need further assessment to understand the cause of the “abnormality”
– Help with ongoing monitoring to measure response to treatment

Common Measures
• Depression: PHQ-9

Advantages of Using Behavioral Health Measures
• Objective assessment
• Creates common language
• Focuses on function
• Avoids potential stigma of diagnostic terms
• Helps identify patterns of improvement or worsening
• Flexibility of administration

PHQ-9: How to Administer
• In-Person
– Facilitates assessment AND teaching about depression symptoms
– Can be administered orally for low literacy patients
• By phone
– Send a copy home for patient to follow along
• Self-administered
– In clinic or at home

2 8 6 16
PHQ-9: How to Score
Adapted from Kroenke K,
Spitzer RL, Williams JB.
The PHQ-9: Validity of a
brief depression severity
measure. Journal of
General Internal Medicine,
16:606-13, 2001.

Understanding PHQ-9 Score
Score Severity
0 – 4 No Depression
5 – 9 Mild Depression
10 – 14 Moderate Depression
≥ 15 Severe Depression

Practice: PHQ-9
• Each person takes an activity sheet from the envelope.
– One person plays the Care Manager
– One person plays patient
– One person observes (using checklist) and provides feedback to the Care Manager
• We will switch roles so that each person can practice!

Review
• What went well?
• What was challenging?

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat to Target
Complete Treatment & Relapse Prevention
© University of Washington

Introducing Care Partners
PCP
Psychiatric Consultant
Patient (Family)
© University of Washington
Care Manager Role
Community Partner
PCC

Practice
• Step 1: Personalize your Introduction – Use model introduction to get started – Keep it short and simple – Key points
• How shared care works and works well! • Your role and the team • The patient role • Next steps to engage in care
• Step 2: Practice your based on real role on the team – Each person practices introducing Care Partner Program – Each person plays the “patient”
• “Patient” partner provides feedback
– If time, practice twice

Review
• What went well?
• What was challenging?

Collaborative Care Workflow
Identify & Engage
Establish a Diagnosis
Initiate Treatment
Follow-up Care & Treat
to Target
Complete Treatment &
Relapse Prevention
System Level Supports

Provider to Provider Communication: How and When?
Frequency • Scheduled • As needed
Consider modality • In person • Staff (MA or nurse) • Phone • Fax • Email (careful with
confidential info) • EMR • CMTS!
PCP
Psychiatric Consultant
Patient (Family)
Care Manager Role
Community Partner
PCC

Planning Activity!
• Plan YOUR team communication!
• In you clinic group use Team Communication Planning Worksheet
– Consider provider to provider communication
– Consider modality
– Consider frequency
• May need to capture which handoffs need further discussion!

Review
• Which handoffs are ready?
• Which handoffs need some further discussion?

BREAK

Facilitated Reflection in Teams

Brainstorming IdeasGoals Sharing

Day 1 Training Feedback

ADJOURN